Paeds · acute-care-resuscitation-and-toxicology
Rapid sequence intubation in children
Also known as Paediatric RSI · Drug-assisted intubation in children · Crash airway management in children · Emergency endotracheal intubation in children
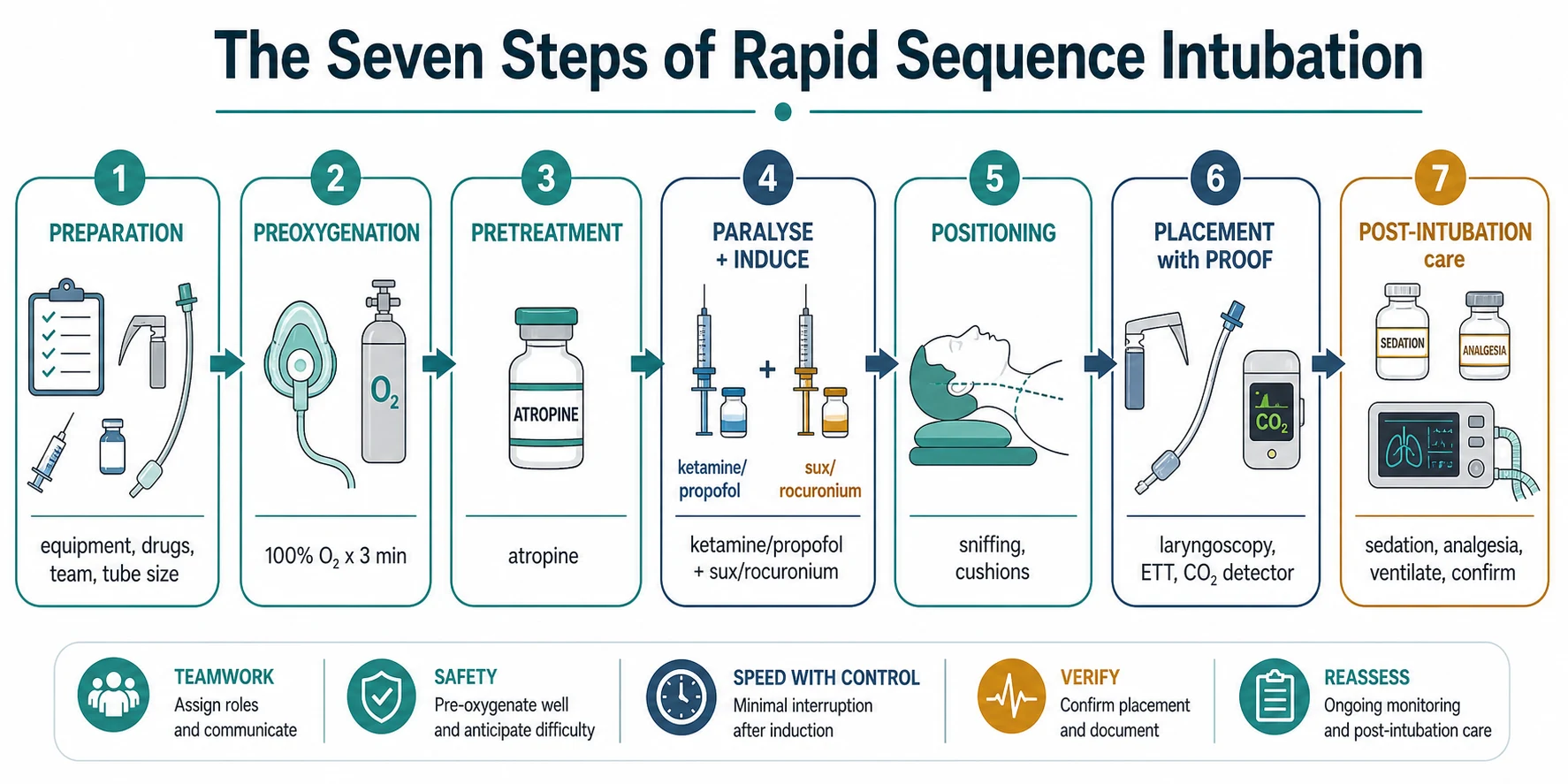
A fellowship approach to rapid sequence intubation in children: prepare a team and equipment, preoxygenate to a child's shorter safe apnoea time, give a weight-based induction agent and neuromuscular blocker in rapid succession, size the endotracheal tube by the age formulae (uncuffed equals age over four plus four; cuffed equals age over four plus 3.5), confirm placement with exhaled carbon dioxide, and avoid the pitfalls of desaturation, bradycardia and cardiovascular collapse.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A 3-year-old with severe pneumonia is grunting, retracting hard, and now drowsy with saturations of 86 per cent on high-flow oxygen. You have decided she needs a definitive airway. The next ten minutes are where children are made safe or harmed, because a child's oxygen reserve is small, the doses are weight-based and unforgiving, and the difference between a calm first pass and a frantic third attempt is preparation. This page teaches the whole sequence — the drugs, the tube sizes, the blade choices, and what to do when it goes wrong. [1] [6]
The seven P sequence
Overview & Definition
Imagine you must put a breathing tube into a sick child in the next two minutes. The child has not fasted, so stomach contents could come up the oesophagus and go down the lungs the moment they lose consciousness. Rapid sequence intubation is the technique built to beat that risk. You give an induction drug to make the brain unconscious and a neuromuscular blocker to stop breathing and muscle tone almost at the same moment, then pass the tube as quickly as possible without squeezing the bag in between, because bagging pushes air into the stomach and forces regurgitation. [1]
The word "rapid" refers to the sequencing of the two drugs and the deliberate omission of mask ventilation — not to a reckless hurry. Every step is prepared in advance so that the apnoeic interval between loss of consciousness and tube placement is as short as you can make it. Sagarin and colleagues framed RSI for the paediatric emergency setting as a structured, drug-assisted intubation that an emergency team can perform reliably under pressure. [1]
The key idea a candidate must hold is the buffer. In an elective anaesthetic intubation you preoxygenate, paralyse, and if the view is poor you mask-ventilate the patient while you get a better look, because the patient is fasted and you have time. In RSI you give up that mask-ventilation safety net on purpose, in exchange for protecting the lungs from aspirated gastric contents. That trade only works if you have done the preparation that lets you pass the tube quickly and confirm it, and if you have a back-up plan for the moment the tube will not go in. [3]
Classification
Sort intubation in children by how much physiological reserve the child has, because that drives your speed and your drug choice. [1] [6]
The first sort is by urgency. An emergency or "crash" airway is the child who is peri-arrest or already in arrest, in whom you intubate immediately, often without time for full preparation, and you accept that you may have to ventilate. An urgent RSI is the child who needs an airway but still has a pulse and some minutes of reserve, so you can prepare equipment, draw up drugs, and assemble the team. The distinction matters because the urgent case is where the full RSI sequence and its preparation pay off, while the crash case is survival-driven and forgiving of short cuts. [6]
The second sort is by the difficulty you predict. Most children have a straightforward anatomy for laryngoscopy, but a child with a small jaw, a short neck, blood or secretions, or a known syndrome carries a difficult airway label. For these you call senior anaesthetic help early, prepare a video laryngoscope, a supraglottic airway and a front-of-neck back-up, and you rehearse the failed-airway plan before you give the paralyser. The sister page on the difficult paediatric airway and emergency front-of-neck access carries the full failed-airway algorithm. [3]
A useful refinement is the contrast with delayed sequence intubation, in which a calm but agitated child is first sedated enough to accept preoxygenation (often with ketamine) before the full paralytic dose. This is occasionally used in older cooperative-enough children to improve the preoxygenation buffer, but it is not standard emergency RSI and should only be done by experienced operators. [3]
Epidemiology & Risk Factors
Paediatric RSI fails on the first attempt more often than adult RSI, and adverse events are common — and that single fact should change how a candidate thinks about the procedure. Kerrey and colleagues used video review of emergency intubations and found a higher frequency of failed attempts and adverse events in children than is acceptable in adult practice, with desaturation, oesophageal intubation and bradycardia recurring as the dominant complications. The youngest and the sickest carry the highest risk. [6]
Age and acuity are the two strongest risk multipliers. Infants fail first attempts more often than older children because their anatomy is harder, their oxygen reserve is smaller, and they desaturate faster. A child who is already in cardiac arrest, profound shock, or deep hypoxaemia when you start has almost no buffer and little margin for a slow attempt. Goto and colleagues showed that the factors most strongly associated with first-pass success in the emergency department were operator experience and the conditions surrounding the attempt, not the child's diagnosis alone. [8]
Who performs the intubation changes the outcome. Kim and colleagues, in a four-centre acute-care study, confirmed that the intubator's training level is independently associated with first-pass success. The practical reading is direct: the most experienced available operator should perform or directly supervise every paediatric RSI, and a learner should not attempt an emergency airway unsupervised. In retrieval and small units, this is the argument for calling the retrieval team early rather than persisting with repeated attempts. [9]
System factors matter too. A child in a quiet rural emergency department at night, with a single junior doctor and no senior anaesthetist on site, faces a higher risk than the same child in a paediatric centre with an airway team. Recognising that mismatch early — and either calling help or retrieving the child to a centre that can manage the airway — is a mark of safe practice, not a sign of weakness. [6]
Pathophysiology
Children fall off their oxygen cliff much faster than adults during the apnoeic period of RSI, and the reasons are mechanical. A child has a small functional residual capacity — the store of oxygen held in the lungs at the end of a breath out — relative to a high metabolic oxygen consumption per kilogram. When breathing stops, that small store is drained quickly, so the time from apnoea to dangerous desaturation can be only a fraction of an adult's. [1] [3]
The chest wall works against the intubator too. A young child's ribs are soft and cartilaginous, so the chest is compliant and the closing capacity (the lung volume at which small airways begin to collapse) sits close to or below the resting lung volume. This means oxygen is not only scarce but also harder to hold onto, and any preoxygenation is more easily undone by a few wasted seconds. [3]
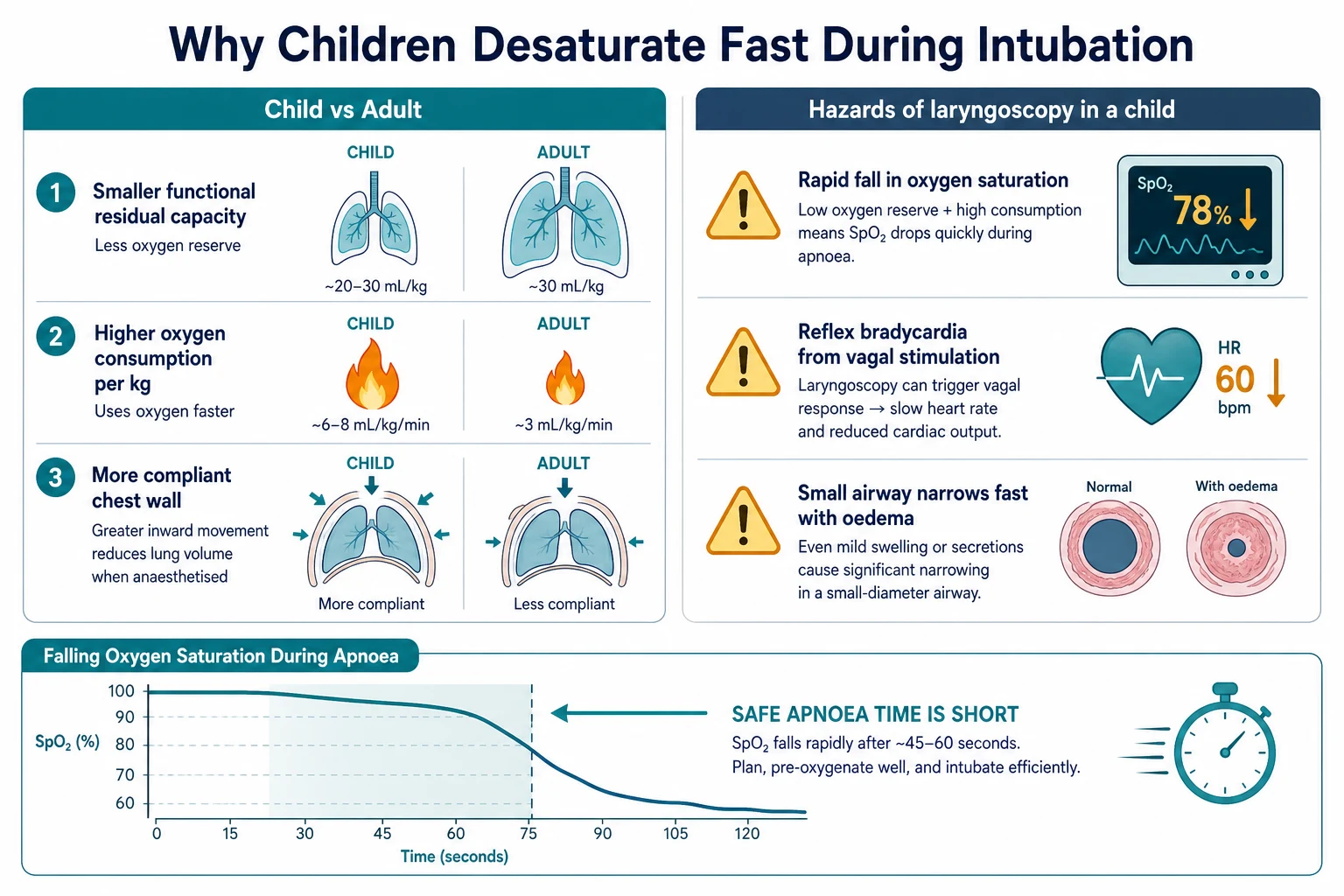
The second danger is cardiovascular, not respiratory. Stimulation of the child's airway during laryngoscopy is powerfully vagal, and suxamethonium itself can trigger bradycardia, especially in infants. A child who is already hypoxaemic is primed for a brisk vagal response, so a falling heart rate during laryngoscopy is often the first warning that oxygenation has been lost. This is the physiological basis for atropine premedication in the youngest children. [5] [10]
Finally, the full-stomassumption is the whole reason the sequence exists. A child who loses tone at induction loses the tone of the lower oesophageal sphincter at the same moment. If you mask-ventilate before the tube is in, you inflate the stomach, raise gastric pressure, and invite passive regurgitation of acidic contents into the airway — aspiration. RSI's defining feature, the avoidance of mask ventilation, is engineered precisely to keep that pressure gradient from building. [1]
The paediatric airway is not a smaller adult airway; its shape is different. The larynx sits higher and more anterior in the neck, the epiglottis is longer and stiffer, and the narrowest point is below the cords at the cricoid ring rather than at the vocal cords. These facts change technique — you use a straight blade and a different lift in an infant — but they do not make the airway impossible, only unforgiving of an adult-style approach. [3]
Clinical Presentation
The child who needs RSI does not always look the same, because the indication can be respiratory, neurological, or both. Read the bedside picture to decide both whether to intubate and how to do it safely. [1] [6]
The classic respiratory indication is the child who cannot oxygenate or ventilate despite maximal support — the tiring infant in bronchiolitis, the silent chest in severe asthma, the shunting lung in pneumonia or paediatric ARDS. You see exhaustion, a falling respiratory rate, reducing effort with no improvement, and hypoxaemia that no longer responds to oxygen. These children are failing the work of breathing, and the tube takes over that work. [6]
The neurological indications look different. A child in coma from a toxic ingestion, a prolonged seizure, or a raised intracranial pressure cannot protect their own airway, even if the lungs are healthy. The tube is placed to protect the airway from aspiration and to control carbon dioxide, not because the lungs have failed. The bedside clue is a child who does not protect their airway — absent gag, pooling secretions, or a Glasgow Coma Score low enough to lose airway reflexes. [1]
A third, exam-favoured indication is anticipated deterioration — the child who does not need a tube this minute but clearly will, and in whom waiting until they are crashing makes the intubation harder and more dangerous. Examples are the evolving upper-airway obstruction, the child being transferred to intensive care, or the septic child whose shock is deepening. [3]
The shocked child needs special recognition. Cold peripheries, weak pulses, prolonged capillary refill, and a narrow pulse pressure tell you the circulation is failing, and that matters for drug choice — a full dose of propofol or thiopentone here can collapse the blood pressure the moment consciousness is lost. Spot shock before you draw up the drugs, and choose an agent and dose that will not drop the pressure further. [3]
Differential Diagnosis
Before committing to RSI, ask whether a less invasive step would buy the time you need, or whether a different airway entirely is the answer. The differential here is not a list of diseases but a list of airway strategies. [1] [3]
Non-invasive support is the first alternative. Heated humidified high-flow nasal cannula, continuous positive airway pressure (CPAP), or bilevel support can reverse moderate respiratory distress and avoid intubation altogether in the right child. The decision turns on whether the child is failing despite non-invasive support or has never had an adequate trial of it. If the child is tiring or losing consciousness, non-invasive support is no longer enough — but apnoeic oxygenation via nasal cannula during the attempt can still extend the safe apnoea time. [1]
The front-of-neck airway is the other end of the differential. When the tube will not pass and oxygenation is failing, the question shifts from "how do I get the tube in" to "how do I oxygenate now." The answer is a supraglottic airway as a bridge, and, if that fails, an emergency surgical airway. In small children the surgical option is a needle cricothyroidotomy with jet ventilation rather than the open surgical cricothyroidotomy used in adults, because the cricothyroid membrane is tiny. This pathway lives on the difficult paediatric airway sister page. [3]
Reversible causes deserve a final thought before the paralyser. A tension pneumothensiothorax, a severe asthma attack, anaphylaxis, or an inhaled foreign body can masquerade as "needs intubation" when the real answer is a needle decompression, bronchodilators, adrenaline, or removal of the obstruction. RSI does not treat these — it supports the child while you do. [1]
Clinical & Bedside Assessment
The bedside assessment for RSI is almost entirely about preparation, because the procedure is won or lost before the first drug is given. Work through equipment, drugs, sizing, and roles as a checklist. [1] [3]
Start with the airway trolley. You need working suction with a Yankauer tip, high-flow oxygen connected to a bag-mask, a laryngoscope with the correct blade and a checked light, a second laryngoscope as a spare, the endotracheal tube plus a half-size above and below, a bougie or stylet, tape or a securing device, a supraglottic airway, and an exhaled carbon dioxide detector. Checking the laryngoscope light and connecting the suction are the two steps most often skipped and most often regretted. [1]
Endotracheal tube size — the age formulae
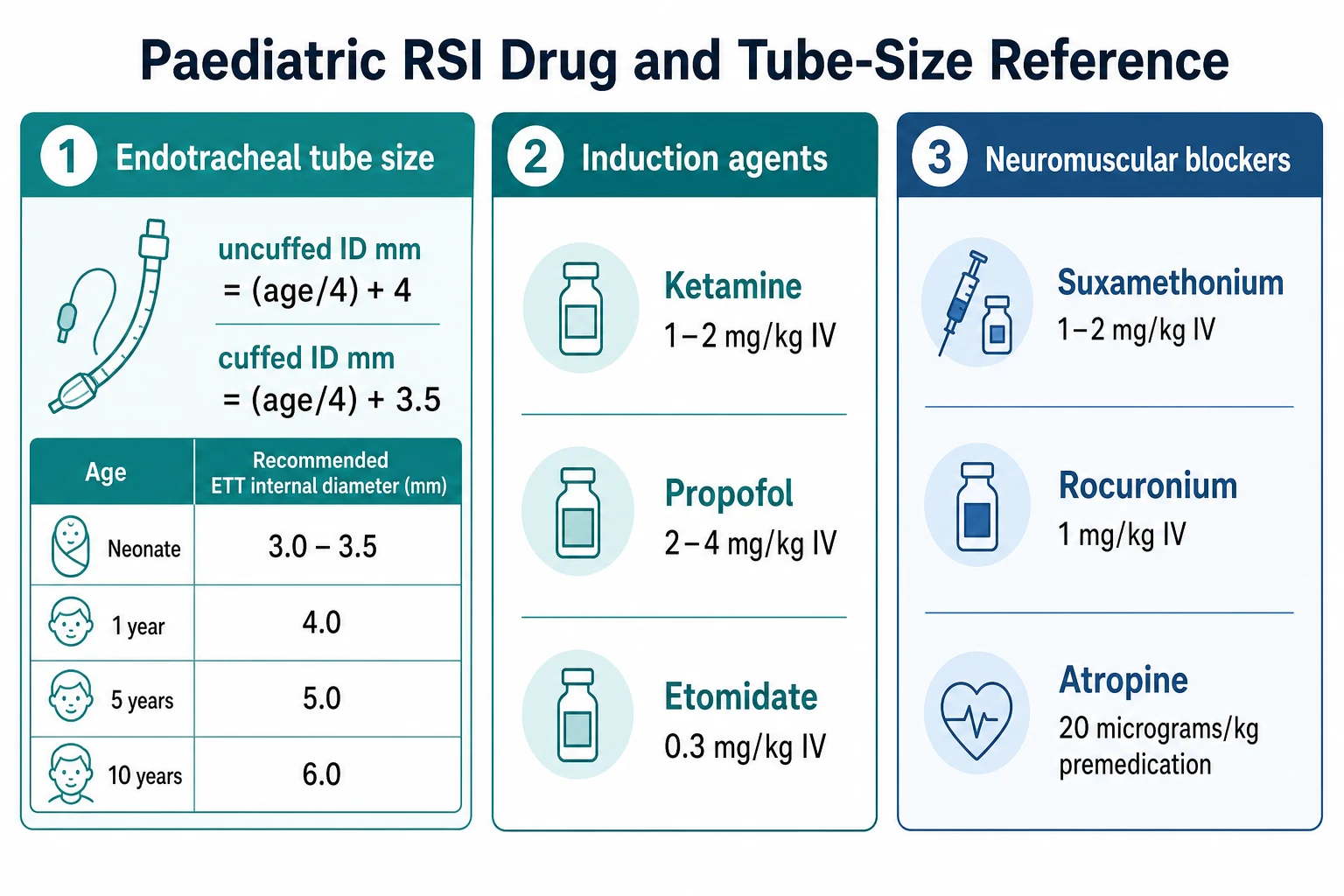
Sizing the tube is the single most testable calculation in this topic. For a child over two years, the uncuffed tube internal diameter in millimetres equals the age in years divided by four, plus four. The cuffed tube is smaller — age over four plus three and a half — because the cuff adds bulk. No formula is perfect, so you always confirm at the cords and have the adjacent sizes to hand. The cuffed-versus-uncuffed question is covered in the evidence section below. [2] [7]
The laryngoscope blade is chosen by age, not by habit. Neonates and infants need a straight blade (Miller) — size 0 for the preterm or small neonate, size 1 for the term infant and older infant — because a straight blade directly lifts the long, stiff, omega-shaped infant epiglottis. Young children from about two to eight years take a curved Macintosh size 2, and older children and adolescents take a Macintosh 3, approaching adult practice. [3]
Preoxygenation is the next bedside step and it must be done well, because it is the only buffer you have. Give 100 per cent oxygen for three minutes, or eight effective tidal-volume breaths through a tight-fitting mask, before the first drug. In the agitated or crying child this is hard, and you may have to accept a partial preoxygenation; in the apnoeic child you begin bag-mask ventilation as the preparation itself, accepting that this child is already a crash airway. [1]
Confirmation at the bedside is mandatory and is not optional. The gold standard is exhaled carbon dioxide — ideally continuous capnography, or a colorimetric detector if capnography is unavailable. A colour change or a capnography trace confirms the tube is in the trachea within a few breaths. Add chest rise and fall, bilateral air entry on auscultation, condensation in the tube, and a rise in oxygen saturation, but treat carbon dioxide as the definitive check. [3]
Pre-intubation bedside checklist
Suction on and within reach; oxygen flowing to a bag-mask
Laryngoscope light checked; correct blade by age; spare laryngoscope ready
Endotracheal tube sized by formula plus a half-size above and below; bougie or stylet ready
Supraglottic airway sized to the child on the trolley; carbon dioxide detector ready
Drugs drawn up, labelled, double-checked: induction agent, neuromuscular blocker, atropine
Roles assigned: intubator, assistant to hold cricoid or pass tube, drugs, timer, scribe
Difficult-airway plan stated aloud and back-up equipment confirmed
Investigations
Most investigations must not delay RSI. The only mandatory "test" before you start is the child's weight, or a best estimate of it, because every drug dose is weight-based and a wrong weight means a wrong dose. Weigh the child, use a length-based tape (such as a Broselow-type tape) if the weight is unknown, and have the doses pre-calculated or use the tape's dosing guide. [1]
A few bedside tests change the plan. A blood gas taken before induction tells you the baseline carbon dioxide and pH, which helps you set the ventilator and judge how sick the child is, but it must never delay a child who needs a tube now. An electrolyte panel matters specifically when you are considering suxamethonium, because a child with a high potassium — renal failure, a burn more than a day old, a neuromuscular disease, or a crush injury — may suffer a lethal potassium rise with suxamethonium and should receive rocuronium instead. [4]
After intubation, a chest radiograph confirms the tube tip lies above the carina (to avoid right mainstem intubation) and excludes a pneumothorax from the positive-pressure ventilation that often follows. Capnography then becomes continuous monitoring rather than a one-off check, because a tube can migrate or dislodge at any point during transfer and ventilation. [3]
Management — Resuscitation
The resuscitation phase is the moment of the procedure itself. As soon as the decision to intubate is made, call for help, assemble the team and equipment, and allocate roles. State the plan aloud so every team member knows who is intubating, who is giving drugs, who is holding cricoid pressure if it is used, and who is timing. A short team brief turns a frantic attempt into a coordinated one. [1]
Preoxygenate fully, as described above. Then give the induction agent and the neuromuscular blocker in rapid succession — ideally within seconds of each other — without waiting to observe the effect of the induction agent first. The whole point of the sequence is that the paralyser follows the induction drug immediately, so that the period between loss of consciousness and loss of airway reflexes is bridged without mask ventilation. [1]
Position the child for the best laryngoscopic view. The infant's occiput is large, so the sniffing position is achieved with a small shoulder roll and a headrest, not by flexing the neck as you would in an adult. The older child takes the classic sniffing position of neck flexion and head extension. In a suspected cervical spine injury, an assistant holds in-line manual stabilisation throughout and you make no head movement. [3]
Cricoid pressure deserves a careful word. It was once a fixed step of RSI, applied to compress the oesophagus against the vertebral column and prevent regurgitation. Modern paediatric practice has largely moved away from routine cricoid pressure, because in small children it can distort the laryngeal view and there is little evidence it prevents aspiration. If it is used, it is light, applied only after induction, and released immediately if it worsens the view. [3]
The single most important resuscitation rule during the attempt is this: if the child desaturates, stop and ventilate. Return to bag-mask oxygenation, reposition, suction if needed, and reattempt — do not persist with a blind or prolonged laryngoscopy while the child goes blue. Bag-mask ventilation during a desaturation is correct and safe even in RSI, because a hypoxic cardiac arrest is a far worse outcome than a theoretical aspiration risk. [6]
Management — Definitive & Stepwise
The definitive management is the full seven-step sequence executed well, with the right drugs for the right child. State the induction agent and the paralyser by name, dose, and reason. [1] [3]
Induction agents — choose by haemodynamics
These induction doses follow APLS and current paediatric emergency practice. [3] [4]
The induction agent is chosen to the child's circulation. Ketamine is the workhorse for the unstable child because it preserves sympathetic tone and bronchodilates, making it the default for shock and for severe asthma. Etomidate is haemodynamically the most stable and suits the unstable child in whom you most fear a pressure drop, with the caveat that it suppresses the adrenal axis. Propofol and thiopentone both lower blood pressure and should be reserved for the cardiovascularly stable child or used at a reduced dose. [3] [4]
Neuromuscular blockers and atropine
These paralyser and atropine doses follow APLS, with atropine guidance drawn from Fastle and Kovacich. [4] [5] [10]
The paralyser is chosen between suxamethonium and rocuronium. Suxamethonium has the fastest onset and shortest duration, which is ideal if you expect difficulty and want the child breathing again within minutes, but it risks hyperkalaemia in susceptible children and can trigger malignant hyperthermia. Rocuronium at 1 mg/kg has a rapid onset without the hyperkalaemia risk and is the alternative when suxamethonium is contraindicated, with the longer duration now reversible by sugammadex where available. The recent emergency-department comparison of the two agents informs this choice rather than mandating one over the other. [4] [12]
Atropine premedication prevents the vagal bradycardia that laryngoscopy and suxamethonium provoke. Give 20 micrograms/kg intravenously (with a minimum of 100 micrograms) to infants under one year, and to children receiving suxamethonium up to about five years. The evidence is mixed on routine use for all children, but the youngest are clearly at greatest risk of bradycardia, which Fastle and Kovacich both documented in emergency practice. [5] [10]
After the tube is placed and confirmed by carbon dioxide, the post-intubation phase is mandatory and is where candidates often stop too early. Secure the tube to prevent dislodgement, start lung-protective mechanical ventilation, and — critically — give ongoing sedation and analgesia. A child who is paralysed but not sedated is conscious, in pain, and unable to move; this is both inhumane and dangerous, because an aware child will fight the ventilator. Fentanyl for analgesia and a sedative such as midazolam, started once the tube is confirmed, are the minimum. Arrange intensive-care admission and a confirmatory chest radiograph. [3]
Specific Subtypes & Scenarios
Different children need a tailored RSI, and the exam rewards the candidate who can match the drug and the technique to the scenario. [3]
The neonate is the most demanding scenario. Tube sizes are tiny (3.0 to 3.5 mm), the straight Miller blade is essential, drug volumes are small and easily mis-drawn, and the bradycardia risk is highest, so atropine is strongly considered. The neonate also has a rapidly falling saturation tolerance, and the resuscitation context may be a delivery-room or neonatal unit rather than an emergency department. [3]
The child in septic shock is the scenario where the wrong induction agent kills. The circulation is catecholamine-depleted, so a full dose of propofol or thiopentone can collapse the blood pressure at induction and precipitate arrest. Use a reduced dose of ketamine, have a fluid bolus and a vasoactive infusion ready to run, and warn the team that the pressure may drop. This is the scenario to rehearse aloud before giving the drug. [3]
Drug choices follow APLS and current emergency-department evidence. [3] [4]
In severe asthma, the goal is to place the tube without provoking cardiovascular collapse from dynamic hyperinflation. Ketamine is preferred for its bronchodilator effect, and the ventilator is set to a slower rate with a long expiratory time to allow trapped gas to escape. Beware the child who obstructs on induction and the one who becomes hypotensive once positive pressure is applied. [3]
The child with a suspected cervical spine injury needs in-line manual stabilisation throughout, no head extension, the most experienced operator, and a low threshold for a video-assisted approach. The risk is that a poorly controlled intubation worsens an unstable spinal injury, so technique and teamwork matter more than speed. [3]
In raised intracranial pressure, the aim is to secure the airway without a cough, buck, or blood-pressure surge that would raise intracranial pressure further, and without hypotension that would drop cerebral perfusion. Thiopentone or propofol (in the stable child) blunts the intracranial response, a generous dose of paralyser prevents coughing, and careful attention to oxygenation and carbon dioxide target protects the brain. [3]
Complications & Pitfalls
Complications in paediatric RSI are common and cluster around a few predictable failures. Knowing them in advance is how you avoid them. [6]
Desaturation is the most frequent adverse event and the most dangerous, because a child's oxygen buffer is short. The defence is thorough preoxygenation, a back-up of bag-mask ventilation the instant saturations fall, and a refusal to prolong a blind laryngoscopy. Bradycardia follows closely, driven by vagal stimulation and suxamethonium in the young child, and is prevented by atropine premedication and treated by stopping the stimulus, ventilating with oxygen, and, if needed, giving adrenaline. [5] [10]
Oesophageal intubation is the catastrophic pitfall that carbon dioxide confirmation exists to prevent. A tube in the oesophagus gives no carbon dioxide trace, no improvement in saturations, and no condensation — but in the heat of the moment these can be misread. Treat a missing carbon dioxide trace as an oesophageal intubation until proven otherwise, remove the tube, ventilate with bag-mask, and reattempt. [6]
D.O.P.E. — when the intubated child deteriorates
Right mainstem intubation is more common in small children because the trachea is short. The tube advances past the carina into the right main bronchus, giving asymmetric chest movement, reduced left-sided air entry, and sometimes low saturations. Correct it by slowly withdrawing the tube while watching capnography and chest rise until breath sounds are equal, then re-secure and confirm with a chest radiograph. [3]
Cardiovascular collapse after induction is the pitfall most tied to drug choice. Giving a full dose of propofol or thiopentone to a shocked child can drop the pressure to a cardiac arrest. The defence is recognising shock beforehand, choosing ketamine or a reduced dose, and having fluid and vasoactive support ready. Finally, the paralysed-without-sedation error — leaving a child under neuromuscular blockade but without analgesia or sedation — is both a humane failure and a patient-safety incident, and it is prevented by a post-intubation sedation plan stated before the tube goes in. [3]
Prognosis & Disposition
Every child who undergoes RSI is admitted to paediatric intensive care, or to a retrieval service if intensive care is not on site. A ward or a general area is not a safe place for an intubated, ventilated child, because the monitoring, the ventilator expertise, and the ability to manage a dislodged tube all sit in intensive care. If the child is in a smaller hospital, the retrieval team is called before, not after, the intubation. [3]
The number of attempts matters for outcome. Each additional laryngoscopy attempt multiplies the risk of desaturation, bradycardia, oesophageal intubation, and trauma, which is why first-pass success is treated as a quality target and a marker of a well-prepared team. The studies by Kerrey, Goto, and Kim all point to the same conclusion: preparation and operator experience are the modifiable factors that protect the child. [6] [8] [9]
After RSI, ongoing monitoring is continuous. Capnography, pulse oximetry, electrocardiography, and blood pressure are monitored throughout, and arterial or capillary gases guide ventilation and perfusion. The ventilator, the sedation, and the tube position are reviewed regularly, and the child is weaned from support only when the underlying condition allows, with a plan for safe extubation and a plan for what happens if reintubation is needed. [3]
It is worth saying plainly to a family that the long-term outcome depends far more on why the child needed the tube than on the intubation itself. The tube is a life-support bridge, not a treatment; the treatment is of the underlying illness. Owning the procedure's risks — desaturation, a second attempt, a need for intensive care — while framing it as the step that lets the real treatment happen is honest and steadying communication. [1]
Special Populations
Some children carry an airway risk that changes the RSI from the first phone call, and recognising them early is the mark of safe practice. [3]
The technology-dependent child — one with a tracheostomy, a home ventilator, or a known difficult airway from a chronic condition — should have a pre-existing airway plan documented in their records and, ideally, on their person. Find that plan, involve the teams who know the child, use the tube size and technique that has worked before, and have senior anaesthesia present. These children are often the hardest airways in the hospital, and routine approaches fail them. [3]
A child with a neuromuscular disease turns the paralyser choice into a safety decision. Suxamethonium can cause a dangerous hyperkalaemia and rhabdomyolysis in conditions such as Duchenne muscular dystrophy and spinal muscular atrophy, so rocuronium is preferred. Knowing this single fact before the drug is drawn up can prevent a cardiac arrest. [4]
The immunocompromised or oncology child may have mucositis that makes the airway friable and bleeds easily, or a coagulopathy that raises the risk of any airway trauma. Anticipate bleeding, use gentle technique, and have suction ready. [3]
A child with developmental disability or autism benefits, when time allows, from a calm, parent-involved preparation, a quiet environment, and clear simple communication. The emergency may not allow this, but where a few minutes of preparation can buy cooperation and a better preoxygenation, they are well spent. [3]
In remote and retrieval settings, the question is often who should intubate and where. A small unit with a single junior doctor and no paediatric airway expertise faces a high-risk intubation; the safer answer may be to support the child with bag-mask ventilation and call a retrieval team that can perform the RSI in a controlled way. The retrieval team's first-pass success, including with videolaryngoscopy, is part of why moving the skill to the child is often safer than moving the child to repeated attempts. [9] [11]
Evidence, Guidelines & Regional Differences
The guidelines that anchor paediatric RSI — APLS, the RCH Melbourne guidelines, the Difficult Airway Society paediatric guidelines, and PALS — agree on the seven-step structure and on most drug doses, but a few evidence questions are live and worth knowing for the exam. [1] [3]
The cuffed-versus-uncuffed question is the clearest example of evidence changing practice. For decades, uncuffed tubes were standard in children under about eight years, on the theory that the cricoid is the narrowest point and a cuff would cause post-extubation stridor. Khine's 1997 study challenged this, showing that cuffed tubes in infants and young children did not increase stridor when cuff pressure was controlled, and the 2017 Cochrane review found no clear difference in complications between cuffed and uncuffed tubes in children aged eight years and under. Cuffed tubes are now acceptable across ages, including in young children, provided the cuff pressure is kept below about 20 to 25 cm of water. The practical advantage is fewer tube exchanges for a poor fit and a better seal. [2] [7]
Atropine premedication is a more contested area. The classical teaching gives atropine to prevent the bradycardia of laryngoscopy and suxamethonium, and Fastle documented the reflex bradycardia in paediatric emergency intubation. More recent work, including Kovacich's emergency-department study, has questioned whether routine atropine prevents clinically important bradycardia or hypoxaemia in all children. The current pragmatic position is selective: atropine is recommended for infants under one year and for young children receiving suxamethonium, where the bradycardia risk is highest. [5] [10]
Cricoid pressure has been largely de-emphasised in modern paediatric RSI. The theoretical protection against aspiration is not well supported in children, and cricoid pressure can worsen the laryngeal view in small infants, so routine use is no longer advised in many ANZ and UK settings. If an operator uses it, it is light and released if the view is poor. [3]
The suxamethonium-versus-rocuronium debate continues to be informed by emergency-department data. Ching reviewed the case for etomidate and rocuronium as newer agents, and Mendez's recent comparison of succinylcholine and rocuronium for paediatric RSI adds to a picture in which both agents are acceptable, with the choice driven by the contraindications and the availability of sugammadex reversal for rocuronium. [4] [12]
Videolaryngoscopy is an emerging evidence strand. Abid and colleagues showed improved intubation success with videolaryngoscopy in a paediatric and neonatal critical-care transport team, supporting its use both in retrieval and as a first-line or rescue device in predicted difficulty. It does not replace sound direct laryngoscopy skills, but it is increasingly part of the modern armamentarium. [11]
Exam Pearls
The exam will test three things above all: the tube-size formulae, the drug doses, and the recognition of when RSI is going wrong. Have these ready to say aloud. [1] [3]
State the formulae precisely: uncuffed tube internal diameter in millimetres equals age in years divided by four plus four; cuffed equals age over four plus three and a half. For a 6-year-old, that is an uncuffed 5.5 mm and a cuffed 5.0 mm. Always add that you would have a half-size above and below ready, and that neonates use weight- and gestation-based sizing rather than the formula. [2]
Know the doses cold: ketamine 1 to 2 mg/kg IV, propofol 2 to 4 mg/kg IV, etomidate 0.3 mg/kg IV, thiopentone 3 to 5 mg/kg IV, suxamethonium 1 to 2 mg/kg IV, rocuronium 1 mg/kg IV, atropine 20 micrograms/kg IV (minimum 100 micrograms). Pair the induction agent to the haemodynamics — ketamine for shock and asthma, etomidate for instability, propofol only when stable — and never give a full induction dose of propofol to a shocked child. [3] [4]
Know the preoxygenation target: 100 per cent oxygen for three minutes, or eight effective breaths, and be ready to explain why a child's safe apnoea time is shorter than an adult's. Know the blade by age — Miller 0 or 1 for neonate and infant, Macintosh 2 for the young child, Macintosh 3 for the older child — and know that exhaled carbon dioxide is mandatory for confirming placement. [1]
Finally, have the DOPE sequence and the seven P sequence on the tip of your tongue, and be able to talk through what you do when the child desaturates during laryngoscopy: stop, ventilate with oxygen, reposition, and reattempt — never persist with a blind attempt. The candidate who can describe the calm, prepared, back-up-ready approach is the one who passes this topic. [6]
References
- [1]Sagarin MJ Rapid sequence intubation for pediatric emergency airway management. Pediatr Emerg Care, 2002.PMID 12488834
- [2]Khine HH Comparison of cuffed and uncuffed endotracheal tubes in young children during general anesthesia. Anesthesiology, 1997.PMID 9066329
- [3]Zelicof-Paul A Controversies in rapid sequence intubation in children. Curr Opin Pediatr, 2005.PMID 15891426
- [4]Ching KY Newer agents for rapid sequence intubation: etomidate and rocuronium. Pediatr Emerg Care, 2009.PMID 19287283
- [5]Fastle RK Pediatric rapid sequence intubation: incidence of reflex bradycardia and effects of pretreatment with atropine. Pediatr Emerg Care, 2004.PMID 15454737
- [6]Kerrey BT Rapid sequence intubation for pediatric emergency patients: higher frequency of failed attempts and adverse effects found by video review. Ann Emerg Med, 2012.PMID 22424653
- [7]De Orange FA Cuffed versus uncuffed endotracheal tubes for general anaesthesia in children aged eight years and under. Cochrane Database Syst Rev, 2017.PMID 29149469
- [8]Goto T Factors Associated with First-Pass Success in Pediatric Intubation in the Emergency Department. West J Emerg Med, 2016.PMID 26973736
- [9]Kim JH Impact of Intubator's Training Level on First-Pass Success of Endotracheal Intubation in Acute Care Settings: A Four-Center Retrospective Study. Children (Basel), 2022.PMID 35883944
- [10]Kovacich NJ Incidence of Bradycardia and the Use of Atropine in Pediatric Rapid Sequence Intubation in the Emergency Department. Pediatr Emerg Care, 2022.PMID 34009889
- [11]Abid ES The Impact of Videolaryngoscopy on Endotracheal Intubation Success by a Pediatric/Neonatal Critical Care Transport Team. Prehosp Emerg Care, 2021.PMID 32347776
- [12]Mendez D Succinylcholine Versus Rocuronium for Pediatric Rapid Sequence Intubation in the Emergency Department. Pediatr Emerg Care, 2026.PMID 41489184