Paeds · acute-care-resuscitation-and-toxicology
Retrieval, transport and interfacility stabilisation
Also known as Paediatric critical care retrieval · Interfacility transport of the critically ill child · Specialist retrieval team and stabilisation · Neonatal and paediatric transport medicine · Pre-transport stabilisation and safe transfer
A fellowship approach to moving a critically ill or injured child between facilities. Treat retrieval as a system that brings intensive care to the child before the child is moved, stabilise the airway, breathing and circulation in full before departure, run a structured referral and handover, choose the right mode of transport and escort for the child and the weather, manage the hostile physics of altitude, vibration and cold, monitor continuously, and rehearse the contingency for deterioration in flight.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Retrieval is the organised process of bringing specialist intensive care to a critically ill child at a referring hospital and then moving that child to a centre that can deliver definitive care. Transport is the act of moving the child between those places. Interfacility stabilisation is the work done at the bedside before, during and after the move to keep the physiology controlled. The three are inseparable, and the candidate who thinks of them as one linked system will answer well. [1] [8]
The single most important idea is that you bring the intensive care to the patient, and then move the patient through the intensive care. The retrieval is not an ambulance ride, and it is not a holding pattern until the child reaches the definitive centre. The standard of monitoring, airway control, ventilation, circulatory support and vigilance on the trolley at the referring hospital is the same standard that travels with the child, and it is the same standard that hands over at the receiving door. [4] [11]
A second idea follows from the first. The dangerous moment in retrieval is the move itself, because the environment deteriorates sharply the moment the child leaves a controlled bed space. The cabin or ambulance is cramped, noisy, vibrating, poorly lit, cold and hard to work in. Adverse events are common when transport is added to critical illness, and most of them are preventable by completing resuscitation first and by using a specialist retrieval team. [2] [3]
[1] [4]The bedside clinician sits in the middle of this system. You receive the referral, you resuscitate and stabilise, you communicate with the retrieval service and the receiving unit, you prepare the child for the move, you hand over in a structured way, and you build a contingency for the journey. You do not have to perform the transport yourself to own it: your decisions at the referring hospital decide whether the journey is safe. [6] [1]
The retrieval sequence, from referral to handover
Referral and accept
Take a structured referral, agree the receiving unit and bed, and call the retrieval service in parallel with resuscitation.
Stabilise before moving
Control the airway, breathing and circulation in full at the referring hospital, secure every tube and line, and document a pre-transport checklist.
Prepare for the mode
Decide road, rotary-wing or fixed-wing for the child, the distance and the weather; manage the physics of altitude, vibration and cold.
Transport and monitor
Move with continuous monitoring, a defined escort and a rehearsed contingency for deterioration en route.
Hand over and close the loop
Give a structured handover at the receiving door, confirm acceptance of care, and feed the case back into the system for learning.
Classification
Classify every retrieval by the axis that drives the decision to move, the team that moves the child, and the mode by which the child travels. The first axis is urgency and purpose: time-critical transfer, where a definitive intervention such as neurosurgery, extracorporeal support or a cardiac procedure cannot wait; specialist-care transfer, where the child needs a higher level of ongoing intensive care than the referring hospital can sustain; and repatriation or elective transfer, where the child is stable and the move is logistical. [4] [8]
The second axis is the retrieval team model. A specialist paediatric retrieval team is physician-led, paediatric intensive-care trained, and carries its own equipment and drugs; it is the model associated with the lowest adverse-event rates. A primary-response or referring-hospital team moves the child with the staff and kit available locally. The distinction matters because moving a critically ill child without the right skills and equipment is the leading cause of preventable transport harm. [1] [11]
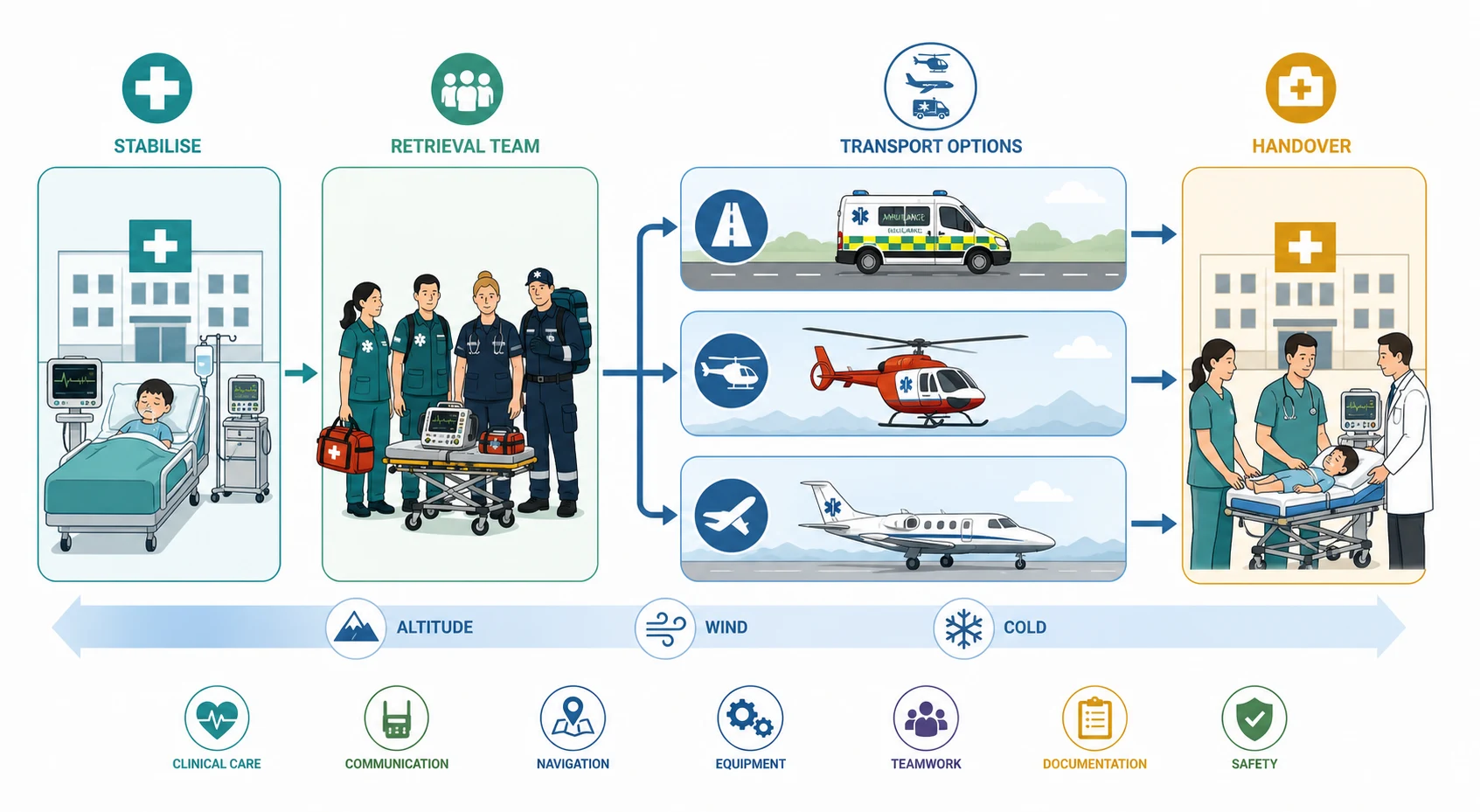
The third axis is mode of transport: road ambulance, rotary-wing helicopter, and fixed-wing aircraft. Road suits short distances, stable children and poor weather. Rotary-wing bridges medium distances quickly but is limited by range, weather, cabin size and vibration. Fixed-wing serves long-distance, international and island-to-mainland retrievals, with a pressurised cabin that softens altitude effects but adds ground-transfer legs at each end. The choice balances speed against the physiological and logistical cost of the mode. [4] [7]
| Mode | Best for | Limitations | Altitude or cabin issue |
|---|---|---|---|
| Road ambulance | Short to medium distance, stable child, all weather | Slower over distance, road conditions, traffic | Sea-level pressure; no altitude gas expansion |
| Rotary-wing (helicopter) | Medium distance, time-critical transfer, scene or hospital to centre | Weather, vibration, noise, small cabin, limited range, cost | Cabin altitude can reach 5000 to 8000 ft; gas expands by up to about a third |
| Fixed-wing aircraft | Long distance, inter-regional, international, island retrievals | Ground transfer legs at both ends, slower to launch, airport access | Pressurised cabin (typically 6000 to 8000 ft) reduces but does not remove gas expansion |
| Specialist retrieval team (any mode) | Any critically ill child needing intensive-care level escort | Launch time to assemble team and kit | The team carries the monitoring, drugs and skills; it is the key safety factor, not the vehicle |
The fourth and most important classifier is physiological stability at the moment of departure. The child who leaves with an uncontrolled airway, an unresolved metabolic acidosis, an undrained pneumothorax, untreated shock, or a falling consciousness level is classified as unsafe to transport. The fix is never to move faster; it is to complete resuscitation first, or to bring the definitive intervention to the child. [2] [1]
Epidemiology & Risk Factors
Critically ill children are moved between hospitals every day, and the volume rises with geographic dispersal, the concentration of paediatric intensive care in tertiary centres, and the reliance on regional services for specialist surgery, cardiac care, neurosurgery and extracorporeal support. In large systems, tens of thousands of neonatal and paediatric interfacility transports occur each year, and the number grows as care centralises. [3] [4]
Adverse events during transport are common when the move is treated as logistics rather than critical care. Studies of intrahospital and interhospital transport of critically ill children report equipment failures, oxygen desaturation, hypotension, hypothermia, line and tube displacement, and unplanned interventions in a substantial proportion of unescorted or under-prepared transfers. The signal is consistent: the uncontrolled move is the hazard, and pre-transport stabilisation plus a specialist team reduce the rate sharply. [2] [3]
Several child and journey factors raise the risk. Young age and small size, neonatal transition, an uncuffed or poorly secured airway, shock on vasoactive drugs, raised intracranial pressure, a tension-prone chest, and metabolic instability all make the cabin a more dangerous place. Long distance, night transport, bad weather, vibration and altitude add environmental risk. Communication gaps at referral and handover compound all of these. [2] [6]
Outcomes are better when a specialist paediatric retrieval team performs the transfer. Specialist retrieval is associated with lower rates of transport-related morbidity and with improved survival and length-of-stay outcomes for the sickest children, compared with transfer by non-specialist teams. The benefit is largest for the time-critical and physiology-unstable child, where every avoidable deterioration matters. [3] [1]
Pathophysiology
The reason transport is dangerous is that it adds a hostile environment to critical illness. Three physical effects drive most of the physiology: altitude and pressure change, vibration and acceleration, and thermal stress. Each of them takes a system that is already failing and makes it harder to monitor and harder to fix. [4] [8]
Altitude changes gas volume by Boyle's law. As the aircraft climbs, ambient pressure falls and any trapped gas expands. At a typical pressurised cabin altitude of around 6000 to 8000 feet, an enclosed gas volume expands by roughly a quarter to a third. An undrained pneumothorax can become a tension pneumothorax in flight; air in the bowel can worsen distension and splint the diaphragm; a gas embolism can expand; and the cuff of a cuffed endotracheal tube can overinflate and press on the tracheal mucosa. [4] [7]
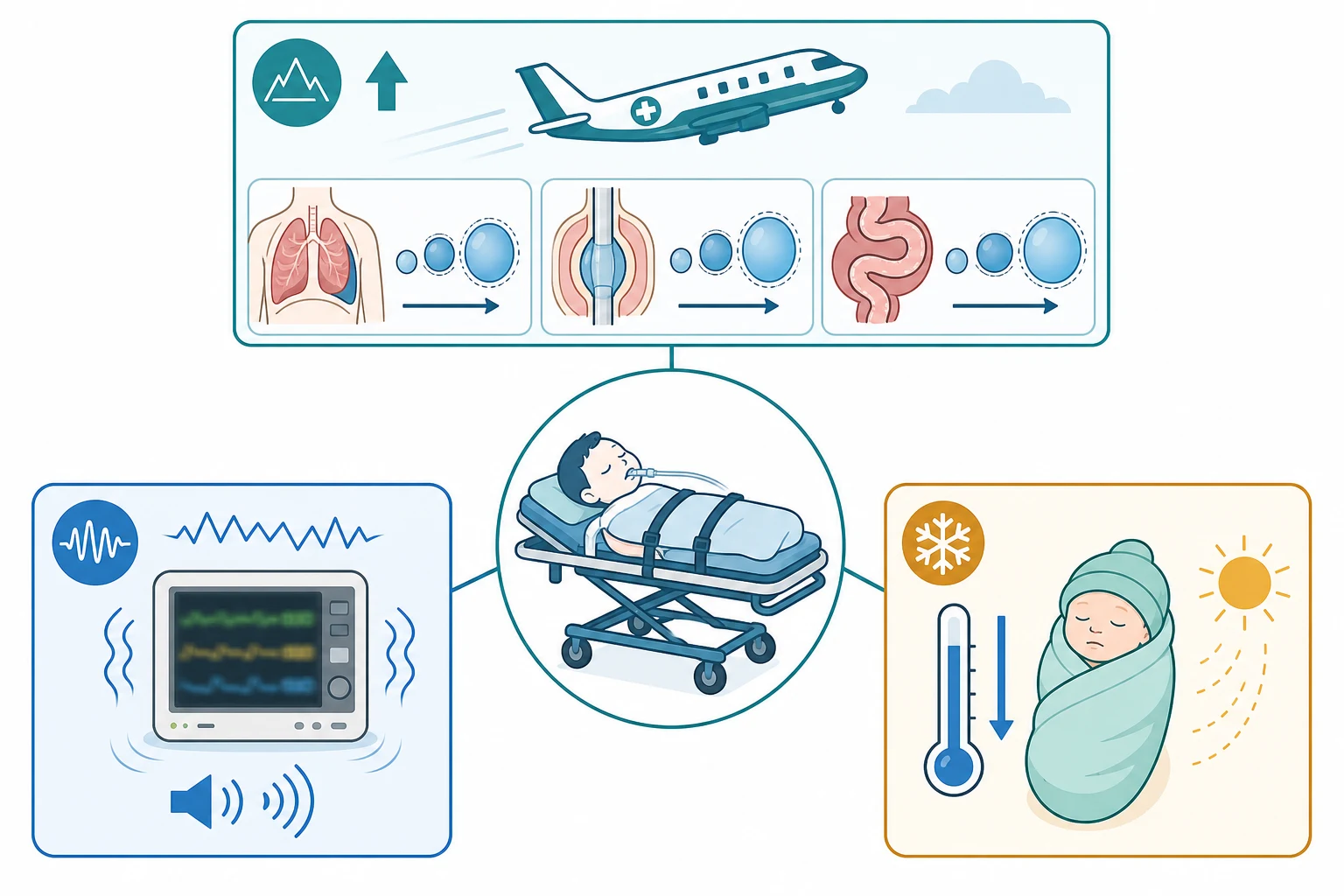
Vibration, noise, poor lighting and acceleration degrade monitoring and clinical assessment. Waveforms jitter, alarms are hard to hear over engine noise, the screen is hard to read in cabin light, and clinical signs are harder to elicit in a moving vehicle. The practical effect is that you must trust monitored data and secure the child before departure, because reassessment in flight is far less reliable than at the bedside. [2] [4]
Thermal stress disproportionately harms the small child. The high surface-area-to-mass ratio of an infant, combined with a cold cabin and an exposed body for procedures, drives hypothermia quickly. Hypothermia worsens acidosis, coagulopathy and oxygen consumption, and in the neonate it is linked to worse outcomes. Active warming before and during transport, a warm cabin, and a covered child are not comfort measures; they are resuscitation. [8] [2]
The fifth mechanism is deterioration of the underlying illness during the unmonitored window. Shock that was compensated decompensates; a partially treated airway obstructs; a metabolic or acid-base problem worsens out of sight. The child who was "stable enough to move" is not the child who stays stable without active management, which is why continuous monitoring and a defined contingency are mandatory. [2] [3]
Clinical Presentation
Begin from the referral. A structured call gives you the identity, age and a working weight, the working diagnosis, the current physiology, what has been done and the response, the local limits, and what the child needs next. The pattern of the call tells you the tempo: a time-critical neurosurgical or cardiac problem, an unstable septic or traumatic child, or a stable child needing a higher level of care. Name that tempo before you plan the move. [6] [1]
At the bedside, describe the child objectively before you classify the move. Note the appearance and interaction, the work of breathing, the colour and perfusion, the neurological state, the monitoring, and every tube, line and device in place. A child who is pale, tachypnoeic, cool, and only partially responsive is not yet stable enough to move, whatever the urgency of the destination. State that plainly and act on it. [4] [2]
What each system must show before departure
At the airway, confirm that the airway is secure and protected. An intubated child needs a correctly placed and firmly secured tube, a checked cuff pressure if cuffed, and a verified position. A non-intubated child with a threatened airway needs definitive airway control before transport, because the cabin is the worst place to perform a difficult intubation. [1] [4]
At breathing, confirm effective and controllable ventilation. The ventilator or bag circuit must deliver the set pressures and tidal volume, the oxygen supply must be sufficient for the whole journey with reserve, and any pneumothorax must be drained before flight. Capnography travels with the child. [10] [4]
At circulation, confirm that shock is treated and perfusion is sustained. Reliable vascular access is secured and immobilised, vasoactive infusions are running on dedicated lines, fluid and blood are available, and the heart rate, blood pressure and perfusion trend are acceptable. A child still needing escalating fluid or inotropes to maintain perfusion is not yet stable for a routine move. [5] [4]
At disability, confirm the neurological state is controlled. A falling conscious level, uncontrolled seizures, or a pupil change en route is a disaster in a moving vehicle. Treat seizures, check glucose, and secure the airway before departure if the Glasgow Coma Scale is falling or the child cannot protect it. [2] [4]
At exposure and environment, confirm the child is warm, every line and drain is secured, the bladder and stomach are decompressed as indicated, and the monitoring is attached and reading reliably. A final pre-departure checklist confirms each of these before the trolley moves. [8] [2]
Differential Diagnosis
The retrieval differential is framed differently from a disease differential. The question is not "what is the diagnosis" but "what will go wrong on the journey, and what can I do now to prevent it." Build that list in a fixed order: what can deteriorate now, what the environment will worsen, what has been done incompletely, and what is hardest to fix in the cabin. [2] [4]
The immediately reversible en-route threats are airway obstruction or tube displacement, a blocked or malpositioned endotracheal tube, ventilator or oxygen failure, pneumothorax under altitude, hypoxia, hypotension, hypothermia, hypoglycaemia, seizure, and loss of vascular access. Each has a pre-emptive fix: secure the airway and tube, check gas supply, drain the chest, oxygenate, support the circulation, warm the child, check glucose, treat seizures, and establish reliable access before the move. [4] [2]
The environment-amplified threats are altitude gas expansion in a pneumothorax, cuff or bowel; vibration degrading monitoring; cold driving hypothermia; and noise masking alarms. Anticipate them by draining gas collections, measuring and adjusting cuff pressure, securing and trusting monitored data, and warming actively. [4] [7]
Keep the communication threats open alongside the clinical ones. An ambiguous referral, a mismatched expectation between referring and receiving teams, or an unstructured handover each creates harm that is invisible until the child arrives. A standardised handover format closes that gap. [6] [1]
Clinical & Bedside Assessment
Run the pre-transport assessment as a structured pass that ends in a decision: is this child safe to move now, and if not, what must be done first. State each finding, declare the action, and record the result on a pre-transport checklist. The checklist is not bureaucracy; it is the instrument that converts intention into a safe departure. [1] [8]
Confirm the airway and breathing at the bedside. Verify endotracheal tube position and security, ventilator settings and alarms, oxygen reserve for the journey plus a margin, capnography, and a clear chest with any pneumothorax drained. Estimate the oxygen consumed for the expected journey time and carry at least that again as reserve. [10] [4]
Confirm the circulation. Check the number and security of access sites, the running infusions and their dedicated lines, the available fluid and blood, the blood pressure and perfusion trend, and the response to resuscitation so far. Two reliable points of access, with at least one that can take rapid fluid, is the practical floor for a sick child. [5] [4]
Confirm disability and metabolic state. Record the Glasgow Coma Scale or AVPU, pupil size and reactivity, seizure control, a recent glucose, the temperature, and the acid-base and electrolyte picture. A worsening trend in any of these is a reason to delay departure and intervene first. [2] [4]
Confirm the environment and packaging. Check that every tube, line, drain and device is secured and labelled, the stomach and bladder are decompressed where indicated, the child is warm and covered, the monitors are attached and visible, and the escort team has the drugs, equipment and contingency it needs. A child who is fully packaged is a child who is ready to move. [8] [2]
[1] [4]Investigations
Name the question before you order any test, because a test that will not change the immediate plan only delays departure. The pre-transport investigations are those that confirm stability or expose a hidden reason not to move. They are few, and they are bedside-first. [4] [1]
Bedside investigations confirm the airway, breathing, circulation and metabolic state. Continuous pulse oximetry and capnography, a credible blood pressure, an ECG when indicated, and a point-of-care glucose are mandatory before the move. A reliable temperature is monitored throughout, most of all in the neonate and infant. [2] [4]
Blood tests drawn at the last access answer the stability question. A venous gas with lactate and base deficit, a full blood count, electrolytes, glucose, coagulation, and a blood group and crossmatch show whether shock, acidosis, anaemia or coagulopathy remain. A worsening base deficit or failing lactate clearance is a reason to keep resuscitating rather than departing. [4] [5]
Imaging is reserved for what changes the move. A chest radiograph confirms tube and line positions and excludes a pneumothorax before flight. A cranial study is obtained at the referring hospital if it changes the plan, rather than transporting an unstable child for a scan elsewhere. Imaging for the complete diagnosis is the receiving centre's job once the child is safe. [7] [4]
The retrieval team carries the transport-specific checks: oxygen cylinder duration against expected journey time, ventilator battery and power, monitor battery, infusion pump batteries, and the contents and labeling of the drug box. Equipment failure is a leading adverse event, and most of it is prevented by a pre-departure equipment check. [2] [11]
Management — Resuscitation
Run retrieval resuscitation as stay and stabilise, then move. The child is resuscitated to the same standard that will apply in the receiving intensive care unit, at the referring hospital, before the trolley moves. Speed of departure is never a substitute for completeness of resuscitation, and a child who departs unstable arrives worse. [1] [4]
Secure the airway before departure if it is threatened or unprotected. Use the principles of paediatric rapid sequence intubation, confirm tube position with capnography, fix the tube firmly, and check cuff pressure if the tube is cuffed, because cuff gas will expand at altitude. A non-intubated child with respiratory failure, shock, or a falling conscious level should be intubated and ventilated before transport. [1] [10]
Control breathing and ventilation. Set the ventilator to deliver effective tidal volume and oxygenation, confirm the oxygen supply covers the journey with reserve, drain any pneumothorax before flight, and decompress the stomach to protect ventilation. Continuous capnography is the single most useful monitored value in a moving, noisy cabin. [10] [4]
Restore and support the circulation. Give weight-based fluid aliquots with early blood where indicated, start vasoactive drugs on dedicated lines, secure reliable access, and crossmatch if transfusion is likely. Treat shock to a sustained perfusion trend, not to a single blood pressure, because a compensated child can decompensate out of sight in transit. [5] [4]
Protect the brain and control disability. Treat seizures, correct hypoglycaemia, avoid hypoxia and hypotension in any child with a brain insult, and secure the airway if the conscious level is falling. The journey must not add a secondary brain injury to the primary one. [2] [4]
Warm the child actively. Pre-warm the cabin or ambulance, cover and wrap the child, use forced-air or exothermic warming as appropriate, and monitor temperature continuously, most of all in the neonate. Keeping a small child normothermic is a resuscitation act, not a comfort measure. [8] [2]
Pre-transport stabilisation: the non-negotiable set

Management — Definitive & Stepwise
Once the child is stable, move deliberately through a stepwise plan that hands the child from the referring team to the retrieval team to the receiving team without a gap. Each handover uses the same structured format, and each step has a named owner. The plan covers the destination, the route, the mode, the escort, the monitoring, the drugs, the contingency, and the communication with the family. [1] [6]
Agree the destination and the receiving team early. Confirm the bed, the accepting consultant, and what the receiving unit will do first. A retrieval without a confirmed receiving bed is a retrieval that strands a sick child, so close that loop before departure and re-confirm on route if the journey is long. [4] [3]
Choose the mode and the escort for the child and the weather. A specialist retrieval team escorts any child needing intensive-care-level support; the mode is road, rotary-wing or fixed-wing by distance, urgency, weather and the physiological cost of altitude and vibration. Match the escort's skills to the child's needs, and never send a child with a team that cannot manage its foreseeable deterioration. [1] [7]
Run a structured handover at referral, at the bedside on arrival of the retrieval team, and at the receiving door. Use a standardised format such as ISBAR or ISOBAR that transfers identity and a working weight, the diagnosis and current physiology, the actions and the response, the local limits, the family and safeguarding context, and the next contingency with a named owner. Communication failure is a leading contributor to transport harm, and structure is the antidote. [6] [1]
Rehearse the contingency for deterioration. Decide in advance who will do what if the child obstructs, desaturates, hypotenses, seizes, or loses a line in transit, and where the journey can be interrupted if needed. A rehearsed plan turns an in-flight emergency into a managed event rather than a crisis. [2] [4]
Prepare the family. Explain the move, the destination, the mode and the contingency in plain language, arrange parental presence or communication according to the system's policy and the clinical situation, and document consent for transport and for any procedure that may be needed. Families who understand the plan are partners in it. [9] [8]
Viva: stay and stabilise versus scoop and run for a deteriorating child
The evidence favours stay and stabilise for the critically ill child. Complete the airway, breathing and circulation work at the referring hospital before departure, because the cabin is the worst place to intubate, decompress or resuscitate. Scoop and run is reserved for the rare situation where the definitive, life-saving intervention, such as emergency neurosurgery or extracorporeal support, cannot be brought to the child and the time cost of full stabilisation exceeds the benefit. The default is to bring intensive care to the child and then move the child through it.
Specific Subtypes & Scenarios
The time-critical retrieval, such as an expanding intracranial lesion needing neurosurgery or a duct-dependent cardiac lesion in collapse, changes the balance toward speed, but never at the cost of an unsecured airway or untreated tension physiology. Resuscitate and stabilise in parallel with activating the fastest mode, and hand over a child who will survive the journey to reach the definitive intervention. [5] [7]
The trauma retrieval follows the trauma primary survey at the referring hospital. Control catastrophic haemorrhage, protect the airway and cervical spine, decompress the chest, restore the circulation with early blood, and package the child before helicopter or road transfer to the paediatric trauma centre. Call retrieval in parallel with resuscitation, before local resources are exceeded. [7] [4]
The cardiac retrieval carries a duct-dependent or failing circulation. Match prostaglandin, vasoactive and ventilatory support to the lesion, anticipate the haemodynamic effect of altitude and vibration, and escort the child with a team that can manage the specific physiology, including escalation to extracorporeal support if that is the plan. [5] [4]
The neonatal retrieval is dominated by temperature and airway. Keep the neonate normothermic from the first minute, secure the airway and ventilation, manage the duct and glucose, and package with warming for the move. Neonatal hypothermia on arrival is a marker of a failed retrieval and is linked to worse outcomes, so warming is a core intervention, not an add-on. [8] [2]
The septic shock retrieval demands completed initial resuscitation before departure. Give fluid aliquots and start vasoactive drugs, secure the airway and ventilation, achieve a sustained perfusion trend, and transport with ongoing support and a plan for further escalation. A child still climbing the resuscitation curve is not yet stable to move. [4] [3]
The child on non-invasive support can sometimes be transported without intubation when a specialist team, continuous monitoring, and a low threshold to intubate are in place. The decision is individual and carries a real risk of deterioration, so the team must be able to intubate and ventilate at any point en route. [10] [2]
The long-distance or international retrieval adds fixed-wing logistics, ground-transfer legs at each end, customs and documentation, crew fatigue, and a longer exposure to the hostile environment. It demands a pressurised cabin, meticulous oxygen and power reserves, a larger team, and a contingency for deterioration far from help. [4] [8]
The rural or remote retrieval is defined by distance and by limited local resources. The decision to call retrieval is made early, in parallel with resuscitation, and the referring team holds the child with telehealth support until the team arrives. Distance makes pre-transport stabilisation even more important, because help is further away. [12] [4]
Complications & Pitfalls
Most preventable transport harm comes from moving a child who was not fully stabilised, or from doing so without the right team and kit. The classic errors are departing with an unsecured airway, an undrained pneumothorax, untreated shock, a falling conscious level, or hypothermia. Each is preventable by completing resuscitation first and by using a pre-transport checklist. [2] [1]
Equipment and monitoring failures are a leading class of adverse event. Empty oxygen cylinders, flat monitor or pump batteries, dislodged lines and tubes, and alarms lost in engine noise all cause deterioration that is hard to reverse in the cabin. A pre-departure equipment check and a policy of securing every line and tube prevent most of them. [2] [11]
Altitude and thermal errors are predictable and serious. An undrained pneumothorax that tensions in flight, an endotracheal tube cuff that overinjures the trachea, bowel gas that splints the diaphragm, and a neonate who arrives cold are all failures to manage the physics of transport. Drain the chest, check cuff pressure, decompress the bowel, and warm the child before and during the move. [4] [8]
Communication errors lose the trend and the contingency. An unstructured referral, a handover that drops the working weight or the safeguarding context, or an assumption that the receiving team knows the plan all create harm at the boundary between teams. A standardised handover format is the reliable fix. [6] [1]
Escalation errors cost time. Waiting until local resources are exhausted before calling retrieval, sending a child with an under-skilled escort, or choosing the wrong mode for the weather or the distance all delay definitive care. Call retrieval in parallel with resuscitation, and match the team and the mode to the child. [3] [4]
Diagnostic overshadowing and anchoring are quieter harms. A child labelled "stable for transfer" who is quietly decompensating, or a deterioration attributed to the journey rather than to an evolving problem, is missed because the label closed the reassessment loop. Keep reassessing the failing system, not the label. [2] [4]
Prognosis & Disposition
Outcome after retrieval is determined by the severity and duration of the physiological insult, the completeness of pre-transport stabilisation, the quality of the escort, the timeliness of definitive care, and the avoidance of secondary injury during the move. The modifiable elements are the ones the candidate controls: stabilise fully, move with the right team and monitoring, and hand over without a gap. [3] [4]
Specialist paediatric retrieval is associated with better outcomes for the sickest children than transfer by non-specialist teams, including lower transport-related morbidity and, in several studies, improved survival and shorter length of stay. The benefit is clearest for the time-critical and physiology-unstable child, where avoidable deterioration changes the outcome. [3] [1]
Disposition is a decision about monitoring intensity and capability, not about geography. The child goes to the paediatric intensive care unit, the cardiac or neurosurgical centre, the neonatal intensive care unit, or the high-dependency or ward bed that matches the predicted trajectory. A defensible disposition is one where the receiving area can manage the foreseeable deterioration without delay. [4] [8]
A usable safety net closes the retrieval loop. It states what to watch for, how urgently to act, and exactly where to get help, and it is owned by a named clinician at the receiving end. After the move, feed the case back into the system for review, because retrieval is a system that learns from every journey. [1] [6]
Special Populations
Adapt the packaging and the escort, never the standard of care. The neonate and small infant is dominated by temperature and airway: warm from the first minute, secure the airway, and package with active warming for the whole journey. Neonatal hypothermia on arrival is a marker of a failed retrieval. [8] [2]
The technology-dependent child is assessed against their personal baseline and device. Confirm the tracheostomy, ventilator, shunt or feeding device is functioning and secured, carry the child's emergency plan, and escort with a team that understands the technology. [4] [11]
The child with complex cardiac disease needs a team that understands the lesion and its response to altitude, vibration and ventilation. Match prostaglandin, vasoactive and ventilatory support to the physiology, and plan for escalation up to extracorporeal support where that is the agreed pathway. [5] [4]
The child with severe neurodisability is assessed against their usual interaction, tone and pain expression, and the caregiver's knowledge is treated as clinical data. Communicate with the family in their usual method, and do not let diagnostic overshadowing mask a genuine deterioration. [2] [4]
The adolescent is offered a private history where appropriate, with attention to confidentiality limits, consent, and substance or self-harm risk. The escort plans for psychological as well as physiological safety on the journey. [9] [4]
Indigenous, migrant, refugee and remote families face access, language and cultural barriers that change the retrieval before and after the move. Use a professional interpreter, apply cultural safety, and coordinate the return or repatriation so that distance and disadvantage do not extend the harm. [12] [8]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The principle of stay-and-stabilise, the use of a specialist retrieval team, the pre-transport checklist, the structured handover, and the management of altitude and thermal hazards are supported by consensus, systematic review and cohort evidence. National and international consensus conferences agree on the core requirements for safe paediatric and neonatal interfacility transport. [1] [8]
The strongest signal is that transport adds adverse events and that pre-transport stabilisation and a specialist team reduce them. Systematic reviews of intrahospital and interfacility transport report substantial rates of equipment failure, physiological deterioration and line and tube displacement, and the consistent finding is that the uncontrolled move is the hazard. [2] [3]
Where the evidence is weaker, say so. The exact optimal mode of transport for a given distance, the balance of speed against stabilisation in specific time-critical subgroups, the effect of telemedicine on rural retrieval, and the best escort composition for the child on non-invasive support are all still being defined by cohort and simulation studies. Quote the source and direct the reader to it rather than inventing precision. [12] [10]
Jurisdictional implementation
Australia and Aotearoa New Zealand: paediatric and neonatal retrieval is delivered by dedicated specialist services coordinated through state and territory systems. In New South Wales the Newborn and paediatric Emergency Transport Service (NETS) provides round-the-clock paediatric and neonatal retrieval; Victoria uses the Paediatric, Infant and Perinatal Emergency Retrieval (PIPER) service; Queensland and Western Australia combine road, rotary-wing and fixed-wing retrievals across vast distances, often with the Royal Flying Doctor Service. The Royal Children's Hospital Melbourne transfer and retrieval guideline supports local practice. Distance makes pre-transport stabilisation and telehealth support especially important.
[1]Exam Pearls
Principle
- Bring intensive care to the child, then move the child through it
- Stay and stabilise, then transport
- Stabilise in full, never move an unstable child faster
Pre-transport checklist
- Airway secure and verified, cuff pressure checked
- Ventilation effective with oxygen reserve
- Pneumothorax drained; shock treated; access reliable
- Glucose checked, seizures controlled, child warm
- Lines and tubes secured; monitoring continuous
Physics of transport
- Gas expands at altitude by Boyle's law
- Cabin altitude around 6000 to 8000 ft expands gas by up to about a third
- Drain pneumothorax, check cuff, decompress bowel before flight
- Vibration and noise degrade monitoring; cold drives hypothermia
Mode and team
- Road, rotary-wing, fixed-wing by distance, urgency and weather
- Specialist retrieval team is the key safety factor
- Match the escort's skills to the child's foreseeable deterioration
Communication
- Structured referral and ISBAR or ISOBAR handover
- Confirm receiving bed and accepting consultant before departure
- Rehearse the contingency for deterioration en route
Pitfalls
- Scoop and run on an unstable child
- Undrained pneumothorax in flight
- Unmeasured cuff pressure at altitude
- Cold neonate; flat batteries and empty oxygen
- Unstructured handover; calling retrieval too late
“Call retrieval in parallel with resuscitation → bring intensive care to the child → complete the airway, breathing and circulation work before departure → drain the chest, check the cuff, warm the child, secure every line → choose the right mode and escort → move with continuous monitoring and a rehearsed contingency → hand over in a structured way and close the loop.”
Viva: the undrained pneumothorax and the flight
Gas expands by Boyle's law as ambient pressure falls with altitude, so an undrained pneumothorax can become a tension pneumothorax in the cabin. At a pressurised cabin altitude of around 6000 to 8000 feet a trapped gas volume expands by up to about a third. I drain any pneumothorax before flight, decompress the stomach and bowel where indicated, and check and adjust the endotracheal tube cuff pressure because cuff gas also expands and can injure the tracheal mucosa. I carry a plan to decompress the chest in flight if needed.
Structured oral: rural retrieval of a deteriorating child
I call the retrieval service in parallel with resuscitation, before local resources are exceeded, and I agree the destination, the mode and the escort. I stabilise in full at the referring hospital: secure the airway, ventilate with oxygen reserve, drain the chest, treat shock, check glucose and seizures, and warm the child. I package the child, run a pre-transport checklist, rehearse the contingency, and keep telehealth support open until the team arrives. I hand over in a structured way and close the loop with the receiving team.
References
- [1]Stroud, Matthew H Pediatric and neonatal interfacility transport: results from a national consensus conference Pediatrics, 2013.PMID 23821698
- [2]Haydar, Sarah Adverse Events During Intrahospital Transport of Critically Ill Children: A Systematic Review Anesthesia and analgesia, 2020.PMID 32925334
- [3]Shinozaki, Renata M Pediatric interfacility transport effects on mortality and length of stay World journal of pediatrics, 2021.PMID 34319538
- [4]Wilcox, Sarah R Interfacility Transport of Critically Ill Patients Critical care medicine, 2022.PMID 36106970
- [5]Ramnarayan, Parviz Inter-hospital transport of the child with critical cardiac disease Cardiology in the young, 2017.PMID 29198261
- [6]Thirnbeck, Catherine K Interfacility Referral Communication for PICU Transfer Pediatric critical care medicine, 2024.PMID 38483193
- [7]Patterson, Katherine N Interfacility helicopter transport to a tertiary pediatric trauma center Journal of pediatric surgery, 2022.PMID 35672168
- [8]Noje, Carolin Consensus on Neonatal and Pediatric Interfacility Transport Air medical journal, 2026.PMID 42331499
- [9]Ali, Amina Pediatric Transport Safety Collaborative: Adverse Events With Parental Presence During Pediatric Critical Care Transport Pediatric emergency care, 2022.PMID 34693934
- [10]Hutton, Heather Noninvasive Respiratory Support during Pediatric Critical Care Transport: A Retrospective Cohort Study Journal of pediatric intensive care, 2024.PMID 39629146
- [11]Campbell, Angela An Integrative Review Regarding Knowledge and Self-Competency of Pediatric and Neonatal Critical Care Transport Nurses Air medical journal, 2022.PMID 36153147
- [12]Gleich, Scott J Low Utilization of Synchronous Telemedicine in Pediatric Critical Care Interfacility Transport: Barriers and Lessons Air medical journal, 2022.PMID 35750446