Paeds · acute-care-resuscitation-and-toxicology
Septic shock resuscitation and vasoactive support
Also known as Paediatric septic shock resuscitation · Fluid-refractory septic shock · Vasoactive support in paediatric sepsis · Catecholamine-resistant septic shock · First-hour sepsis bundle
A fellowship approach to resuscitating paediatric septic shock: recognise the failing circulation early, restore perfusion with reassessed crystalloid aliquots, give broad-spectrum antibiotics within the first hour, and escalate to adrenaline for cold shock or noradrenaline for warm shock as the first-line vasoactive agent when shock is fluid refractory. Treat every step as a reassessment loop, watch for fluid accumulation, and call for critical-care help before local support is exceeded.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Septic shock is the life-threatening circulatory failure that follows a dysregulated host response to infection. The problem is not the infection itself but the body's reaction to it: inflammation deranges blood vessel tone, leaks fluid out of the circulation, and weakens the heart, so that blood is no longer delivered to tissues in the amount they need. The child looks cold, mottled and poorly perfused long before the blood pressure falls, because children hold their pressure up by raising heart rate and squeezing down their blood vessels. Waiting for hypotension to diagnose shock is the classic, dangerous error. [1] [5]
The modern international definition is the Phoenix criteria, agreed in 2024. A child has paediatric sepsis when the Phoenix sepsis score totals 2 or more points across its organ-dysfunction domains, and paediatric septic shock when that sepsis includes at least one point of cardiovascular dysfunction. The cardiovascular component captures the children who need vasoactive medication, have a raised lactate despite fluid, or have a mean arterial pressure below the threshold for their age. This replaced the older Sepsis-2 framework because the old definition relied heavily on systemic inflammatory response criteria that are neither sensitive nor specific. [3] [11]
Resuscitation of septic shock is a race to restore oxygen delivery before cells are starved, run in parallel with finding and killing the organism. The first hour is decisive: airway and breathing are supported, circulation is restored with fluid and then vasoactive drugs, glucose and electrolytes are corrected, and source control with antibiotics and drainage is begun. The Surviving Sepsis Campaign 2026 children's guideline sets the structure, but every step is a reassessment loop rather than a fixed prescription, because the same fluid that rescues one child can drown another. [1] [2]
Classification
The single most useful bedside classification is the haemodynamic phenotype, because it tells you which vasoactive agent to choose. Look at the skin temperature, the pulse character and the pulse pressure. [5] [10]
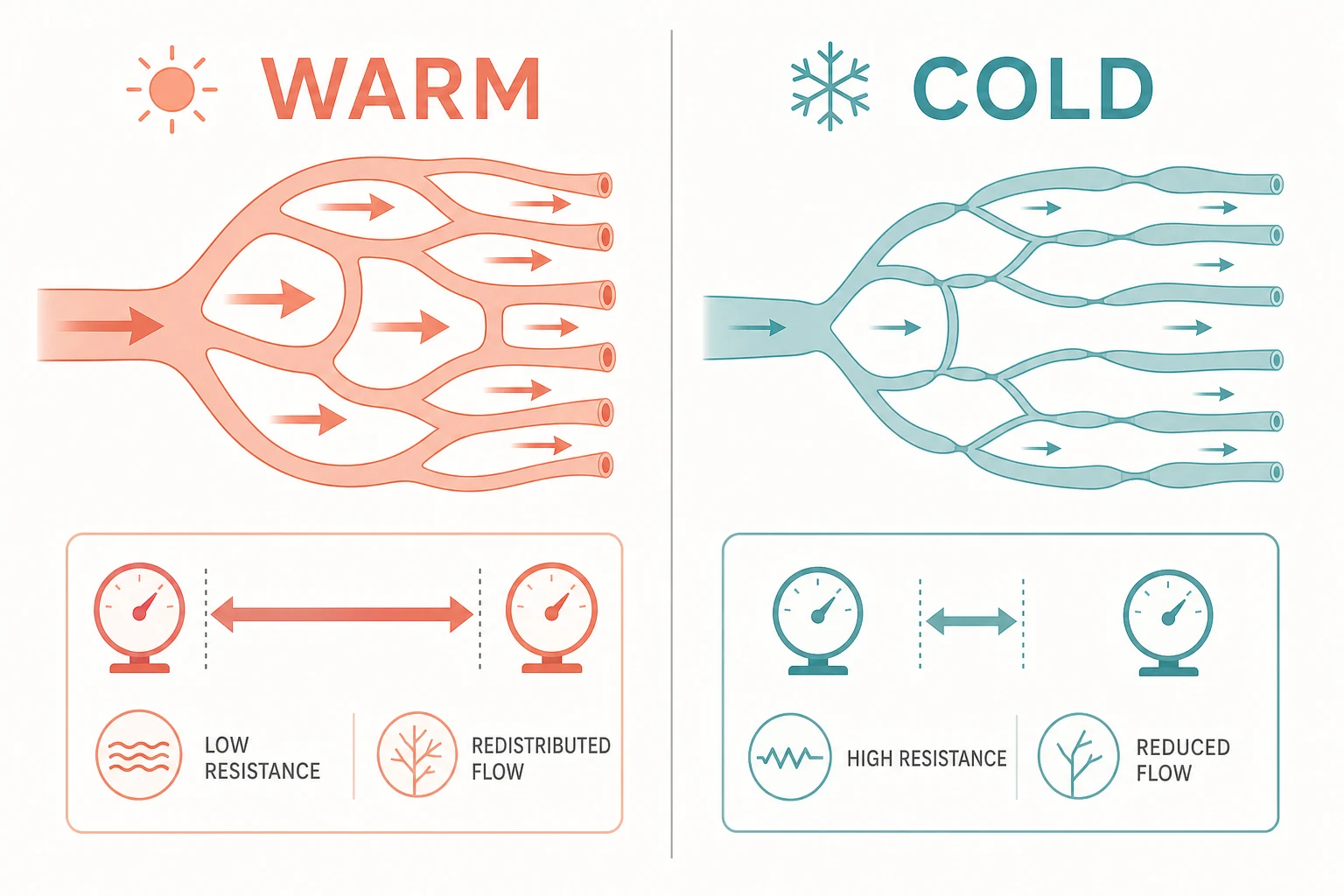
Cold shock
Most common in children
- Vasoconstricted: cold, mottled, prolonged capillary refill
- Weak, thready peripheral pulses with narrow pulse pressure
- Low cardiac output with high systemic vascular resistance
- First-line vasoactive: adrenaline (epinephrine)
Warm shock
Less common, older children
- Vasodilated: warm, flushed, flash capillary refill
- Bounding pulses with wide pulse pressure
- High or normal cardiac output with low systemic vascular resistance
- First-line vasoactive: noradrenaline (norepinephrine)
Mixed or evolving
Reassess repeatedly
- Phenotype can shift as resuscitation proceeds
- Capillary leak and myocardial depression coexist
- Re-examine skin, pulses and perfusion after every bolus
- Adjust the vasoactive agent to the phenotype in front of you
Classification by response to fluid drives the timeline of escalation. Fluid-responsive shock improves with boluses and may need no vasoactive agent. Fluid-refractory shock persists after two or three reassessed boluses and demands a vasoactive infusion. Catecholamine-resistant shock fails to correct on adequate vasoactive doses and prompts stress-dose hydrocortisone and a search for reversible causes such as tamponade, pneumothorax, ongoing blood loss or an undrained source. Each step is a decision point, not a label you carry to discharge. [1] [2]
Epidemiology & Risk Factors
Septic shock remains a leading cause of paediatric critical illness and death worldwide. Mortality in well-resourced paediatric intensive care settings is now in the single digits, but it climbs steeply where recognition is late, where fluid and vasoactive rescue are delayed, and where the child is very young or has limiting comorbidity. The risk context changes the tempo of your assessment and the threshold for early escalation, not the structure of resuscitation. [5] [11]
The children at highest risk are the ones with the least physiological reserve and the most attenuated inflammatory responses. A young infant may show only poor feeding, floppiness or a change in behaviour rather than fever. An immunocompromised child or one on chemotherapy can be neutropenic and afebrile yet still have overwhelming sepsis. A technology-dependent child with a central line lives with a permanent portal for bloodstream infection. Recognising these contexts lowers the threshold to act. [1] [5]
Host factors
- Young infant or neonate with limited reserve
- Severe malnutrition or chronic complex disease
- Immunocompromise, chemotherapy or transplant
- Indwelling central venous catheter or implanted device
Presentation factors
- Delayed or repeated presentation
- Caregiver reports the child is different from usual
- Reduced interaction, mottling, poor urine output
- Underlying source: pneumonia, meningitis, gut, urinary, line
System factors
- Rural or remote location with transport delay
- Limited monitoring, airway or vasoactive rescue
- After-hours or single-handed cover
- Communication, language or socio-economic barriers
Pathophysiology
Septic shock is the end result of a response that was meant to localise infection but instead becomes generalised and self-destructive. Three mechanisms run together, and which one dominates in a given child decides the phenotype and therefore the drug. [5] [10]
The first is vasodilation. Inflammatory mediators relax vascular smooth muscle, so systemic vascular resistance falls and blood is maldistributed through open, poorly perfused beds. This is the warm-shock picture: the heart pumps well into a floppy circuit, the skin is flushed and the pulse pressure is wide. The second is capillary leak. The endothelial barrier fails and fluid, albumin and electrolytes pour into the tissues, shrinking the circulating volume even though the child may look oedematous. The third is myocardial dysfunction. Circulating myocardial depressant substances blunt contractility, so cardiac output falls. These last two produce the cold-shock picture: a weakly contracting heart pushing a reduced volume through tight vessels into cold, mottled limbs. [5] [10]
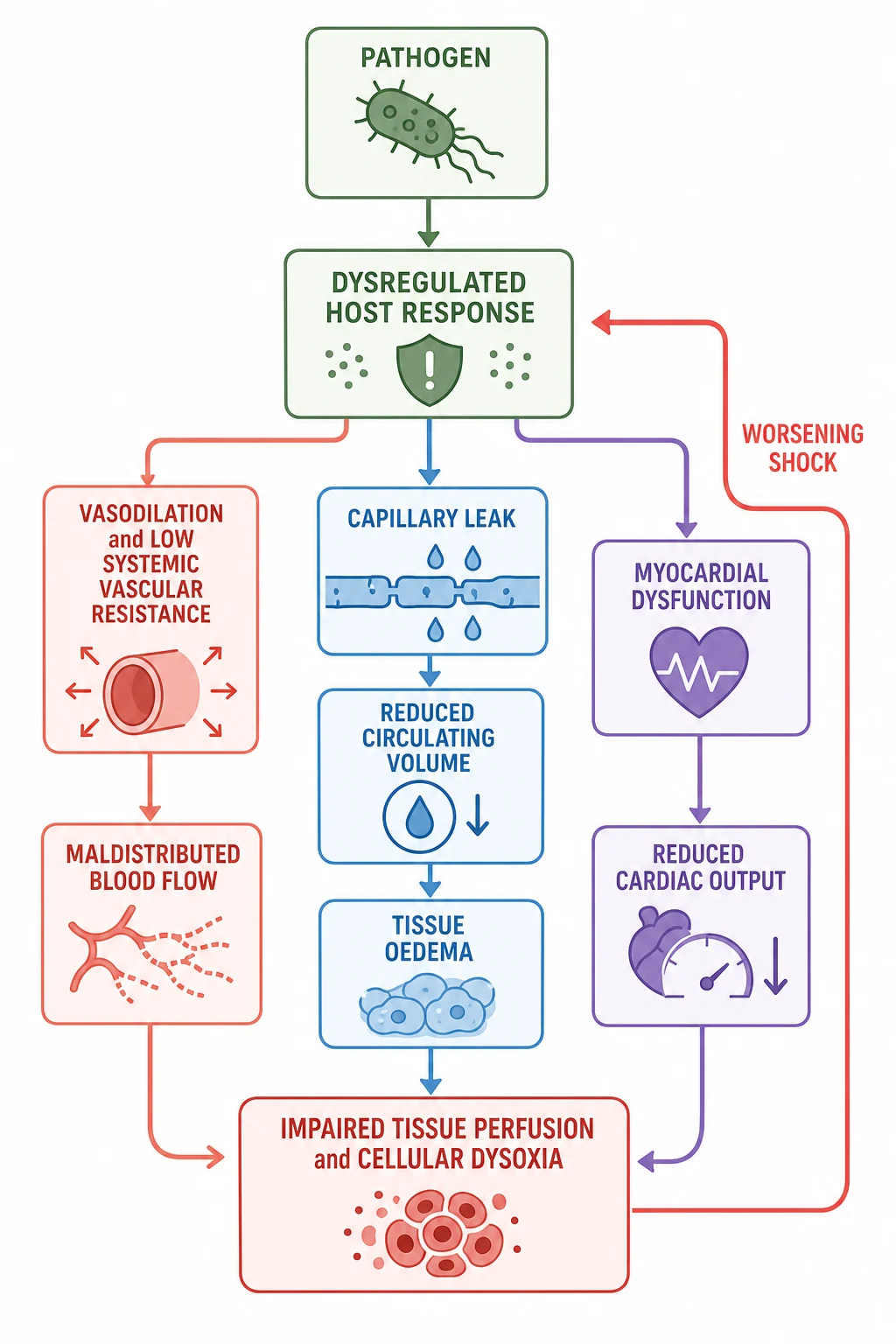
Why does this matter clinically? Because oxygen delivery depends on cardiac output and arterial oxygen content, and cardiac output depends on stroke volume and heart rate. In septic shock all three levers can fail at once: contractility falls, preload falls as volume leaks out, and the heart, already running fast to compensate, cannot speed up indefinitely. The tissue runs out of oxygen, switches to anaerobic metabolism, and generates lactate. A rising or stubbornly high lactate is therefore a marker of ongoing cellular distress, not simply a number to chase down. [1] [10]
The compensation that hides early shock is also the reason collapse is sudden. Children raise heart rate and vascular tone to defend blood pressure and cerebral perfusion, which buys time but spends reserve. The moment reserve runs out the fall is steep, and the child who looked merely unwell minutes ago can arrest. This is why resuscitation is measured in minutes, and why a child with poor perfusion but a normal blood pressure is already an emergency. [1] [5]
Clinical Presentation
Begin with the first impression from the doorway, then move to a hands-on assessment that judges the whole circulation. Describe what you see objectively: "This child is pale, mottled, tachycardic with weak pulses and barely responds to voice" tells the team far more than "this child looks septic." [1] [5]
The classic presentation is the child with fever or a localising source who develops the signs of a failing circulation. Tachycardia is the earliest and most sensitive sign, followed by cool mottled skin, a prolonged capillary refill and weak peripheral pulses. The child is tachypnoeic from acidosis and from any concurrent respiratory source. Urine output falls because the kidneys are underperfused. Conscious level drops as cerebral perfusion worsens. Blood pressure is preserved until relatively late, so a normal reading never excludes shock. [5] [10]
[5]Atypical presentations are the trap the examiner sets deliberately. The young infant may be afebrile and hypothermic with only poor feeding and floppiness. The immunocompromised child may have blunted inflammatory signs and no fever. The child with diabetic ketoacidosis can be in shock from dehydration complicated by sepsis. The technology-dependent child with a line may present with the symptoms of line sepsis alone. Each of these still needs the same resuscitation structure, applied with a lower threshold to act. [1] [5]
Differential Diagnosis
Septic shock is one cause of paediatric shock, and the resuscitation of the circulation does not wait for certainty about which type it is. But the cause changes the definitive treatment, so build the differential in a fixed order: what can kill now, what is most likely, what is reversible, and what is most harmful to miss. [5]
Distributive
- Septic shock: infection, warm or cold phenotype
- Anaphylaxis: exposure, rapid onset, skin plus respiratory or circulatory features
- Neurogenic: spinal cord injury with warm vasodilated shock
- Give the cause-specific treatment once shock is identified
Hypovolaemic
- Haemorrhage from trauma, gut or surgical cause
- Severe dehydration from gastroenteritis or DKA
- Capillary leak from sepsis itself contributes here
- Ongoing loss must be controlled alongside resuscitation
Cardiogenic
- Myocarditis, cardiomyopathy, dysrhythmia
- Duct-dependent congenital heart disease in the infant
- Septic myocardial depression blurs into this category
- Echocardiography clarifies when shock is fluid refractory
Obstructive
- Tension pneumothorax: asymmetric air entry, tracheal deviation
- Cardiac tamponade: muffled sounds, pulsus paradoxus
- Massive pulmonary embolism
- Each has a single corrective action; look for them actively
The practical point is that the first fluid bolus is given on the recognition of shock, before the type is certain. As the response unfolds, the differential narrows. A child whose shock does not improve with fluid needs the mechanical causes sought, an echocardiogram to define cardiac function, and a vasoactive agent matched to the phenotype. Keeping anaphylaxis, a duct-dependent lesion and a mechanical obstruction open early prevents the lethal error of treating only the sepsis pathway. [1] [5]
Clinical & Bedside Assessment
Assess the circulation as an integrated whole, then re-assess it after every intervention. The hands-on examination at the bedside is where shock is recognised and where the response to treatment is judged. [5] [10]
Start with the pulses: rate, rhythm and quality at central and peripheral sites. A thready peripheral pulse with a weak central pulse signals low stroke volume. Feel the skin: cold, mottled, clammy skin with a prolonged capillary refill indicates poor perfusion, while warm flushed skin with a brisk refill suggests a vasodilated phenotype. Measure capillary refill with the technique stated (sternum or fingertip, firm pressure for a stated time, ambient temperature), because the sign is technique-dependent. Take the blood pressure and interpret it alongside everything else, never alone. Note the mental state and the urine output, both of which reflect cerebral and renal perfusion. [5]
While resuscitation proceeds, take a focused history in parallel. Ask about the onset and pace of illness, fever and source, intake and urine output, underlying conditions and devices, medications and allergies, immunisation status, and any known exposures or recent travel. For a young infant clarify the perinatal history. Use a professional interpreter whenever needed. This history shapes the antibiotic choice and the source control plan, but it never delays the first bolus. [1]
The reassessment after each intervention is the examination that matters most. After a fluid bolus, ask whether the pulses are stronger, the skin warmer, the capillary refill shorter, the interaction better and the urine output rising. State the change you expected before giving the bolus, and compare it with what actually happened. A child who improves transiently then slides back is not fluid responsive; one who worsens or develops crackles and hepatomegaly is being overloaded. [1] [9]
Investigations
Stabilise first, then order each test for a named question. In septic shock the immediate tests quantify the failing physiology, identify the organism, and define the cause and complications. [1] [3]
Immediate and bedside
- Point-of-care blood gas and lactate to quantify perfusion and metabolic state
- Bedside glucose: hypoglycaemia is common and dangerous in the septic child
- Credible oxygen saturation and, in serious illness, capnography
- Blood culture before antibiotics when it does not delay treatment
Core laboratory
- Full blood count, electrolytes, renal and hepatic function, coagulation
- C-reactive protein and procalcitonin as adjuncts, never sole decision tools
- Group and hold or crossmatch if haemorrhage or transfusion is possible
- Calculate the Phoenix score to confirm severity and track organ dysfunction
Targeted imaging
- Chest imaging when a pulmonary source changes management
- Echocardiography for fluid-refractory shock to define cardiac function and filling
- Point-of-care ultrasound within operator competence for effusion or volume
- Never move an unstable child to imaging without monitoring, escort and rescue plan
Interpret the urgent tests as physiology and trend, not as binary reassurance. A high lactate reflects ongoing anaerobic metabolism and should fall with effective resuscitation; a normal lactate never excludes shock. A blood gas shows the acid-base cost of poor perfusion and confirms whether ventilation is adequate. The Phoenix score, built from cardiovascular, respiratory, neurological and coagulation variables, both defines septic shock at the bedside and tracks whether the organs are recovering as you treat. [3] [11]
[1]Management — Resuscitation
Resuscitation of paediatric septic shock follows the first-hour bundle: recognise and call for help, secure airway and breathing, restore the circulation with reassessed fluid, give antibiotics and source control, correct glucose and electrolytes, and escalate to vasoactive support when shock is fluid refractory. Every element runs in parallel, and every action is followed by reassessment. [1] [2]
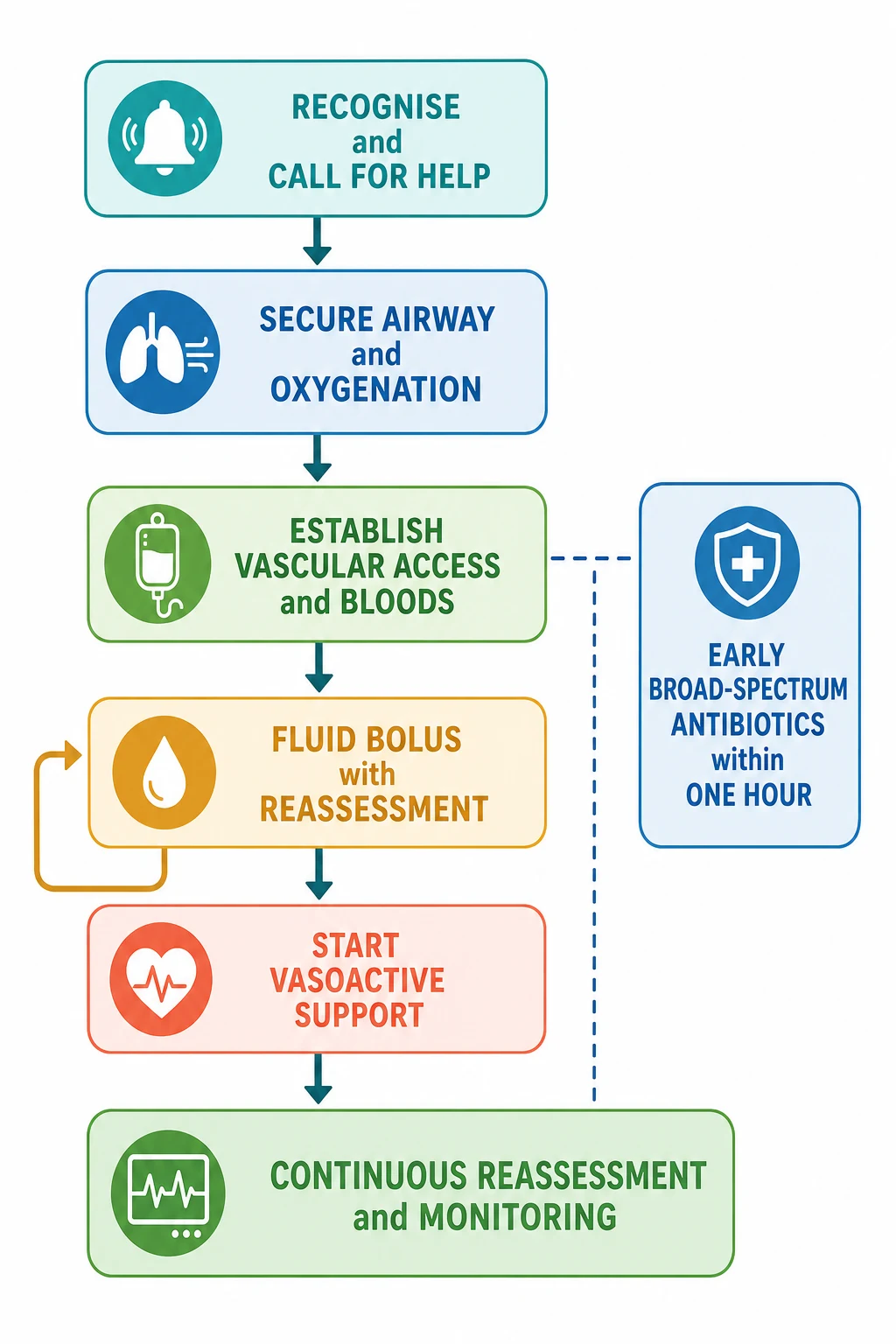
The first hour in septic shock
Recognise and call for help
Declare the concern, call the senior paediatric and resuscitation teams, name a leader, allocate roles, and bring age- and weight-appropriate equipment and monitoring.
Secure airway and breathing
Give high-flow oxygen in failure and support ventilation if it is ineffective; protect the threatened airway and prepare for definitive airway control in the deteriorating child.
Establish access and take bloods
Gain intravenous access promptly; use intraosseous access early if peripheral access is delayed. Send point-of-care gas, lactate, glucose, cultures and core bloods.
Restore the circulation with reassessed fluid
Give reassessed weight-based crystalloid aliquots, state the expected response before each, reassess after each, and stop for overload or no benefit. The first-hour total is a ceiling, not a target.
Give antibiotics and source control
Administer broad-spectrum antibiotics within the first hour at weight-appropriate doses, and arrange source control such as drainage or line removal.
Start vasoactive support if fluid refractory
If shock persists after two or three reassessed boluses, start adrenaline for cold shock or noradrenaline for warm shock, and arrange central access and intensive care.
Reassess from the top
After every action, return to airway, breathing, circulation and consciousness, judge the trend, and revise the plan.
Airway and breathing
Give high-flow oxygen to any child in respiratory, circulatory or neurological failure and titrate to a saturation of 94 to 98% in the previously well child. Support ventilation with bag and mask if breathing is ineffective, and prepare for a definitive airway in the child who is tiring, comatose or haemodynamically unstable. Respiratory failure from acidosis, a pulmonary source or fatigue can coexist with septic shock and will worsen it if untreated. [1]
Circulation: fluid as a ceiling, not a target
Restore the circulation with crystalloid aliquots of 10 to 20 mL per kilogram. Before each bolus, state the improvement you expect: stronger pulses, warmer skin, shorter capillary refill, better interaction and rising urine output. After each bolus, reassess and decide between sustained improvement, transient improvement, no response and harm. The first-hour fluid total is a ceiling, never a target to be reached for its own sake. [1] [9]
The Surviving Sepsis Campaign 2026 children's guideline supports up-front fluid boluses in septic shock with careful reassessment and explicit attention to fluid balance. It cautions against fluid accumulation injury, the harm that comes from driving fluid into a leaking circulation that cannot hold it. Watch for crackles, hepatomegaly, a rising oxygen requirement and a positive balance that outpaces improvement. [1] [9]
FEAST
New England Journal of Medicine
Randomised fluid-bolus trial in African children with severe febrile illness
Key finding
Saline or albumin bolus increased 48-hour mortality compared with no bolus in that population.
Practice change
Fluid strategy must stay specific to the population, shock type and available rescue; do not transplant a bolus protocol uncritically. In a well-resourced setting a child in septic shock still receives reassessed aliquots, but the response is watched and the ceiling respected.
The lesson of FEAST is not that fluid is forbidden, but that a fluid algorithm cannot be transplanted across populations, shock types and rescue resources. Apply the strategy to the child in front of you, reassess rigorously, and escalate to vasoactive support and retrieval rather than forcing a fixed volume. [4]
Antibiotics and source control
Give broad-spectrum antibiotics within the first hour of recognising septic shock, at weight-appropriate doses and by the intravenous or intraosseous route. The choice is guided by the likely source, local resistance patterns, allergy history and any focal findings: a community-acquired regimen, a neutropenic regimen, a meningitic regimen or a line-infection regimen. Source control — draining a collection, removing an infected line, relieving an obstruction — proceeds in parallel once the circulation is supported. [1] [2]
Glucose and electrolytes
Check bedside glucose in every septic child and correct a dangerous low immediately through the local pathway, because hypoglycaemia is common in the septic infant and worsens neurological outcome. Correct calcium, sodium and potassium disturbances as they are found, and avoid hyperglycaemia from unnecessarily concentrated dextrose. [1]
When ABCDE becomes advanced life support
If the child becomes unresponsive with absent or agonal breathing and no central pulse, move straight into the paediatric arrest algorithm rather than completing the survey. The arrest-dose anchors from the resuscitation sources are intravenous or intraosseous adrenaline at 10 micrograms per kilogram (0.1 mL per kilogram of 1 in 10,000 adrenaline) every three to five minutes, and defibrillation at 4 joules per kilogram for a shockable rhythm. The full algorithm lives in the paediatric basic and advanced life support topic. [1]
[1]Management — Definitive & Stepwise
Once the first-hour bundle is running, definitive management moves to vasoactive support, ongoing monitoring and the resolution of organ dysfunction. This is the phase where shock becomes fluid refractory, catecholamine resistant, or resolves, and the decisions are made hour by hour with the trend, not the snapshot. [1] [10]
Vasoactive support: choose by phenotype
Start a vasoactive agent when shock persists after two or three reassessed fluid boluses, or earlier if the child is clearly fluid refractory or overload is developing. The first-line agent is chosen by the haemodynamic phenotype. [1] [6]
| Phenotype | First-line agent | Typical infusion range | What it does |
|---|---|---|---|
| Cold shock (most children) | Adrenaline (epinephrine) | 0.05 to 1.0 microgram per kilogram per minute, titrated | Raises contractility and cardiac output; alpha effect restores vascular tone at higher doses |
| Warm shock | Noradrenaline (norepinephrine) | 0.05 to 1.0 microgram per kilogram per minute, titrated | Predominant alpha effect restores systemic vascular resistance and blood pressure |
| Adjunct or second line | Dopamine | 5 to 20 microgram per kilogram per minute | No longer preferred first line: higher dysrhythmia burden and no survival advantage over adrenaline or noradrenaline |
| Catecholamine resistant | Add vasopressin or stress-dose hydrocortisone | Per local intensive-care protocol | Adjuncts for shock unresponsive to adequate first-line vasoactive doses |
Adrenaline is the first-line agent for cold shock because it restores inotropy and, at higher doses, vascular tone. Noradrenaline is the first-line agent for warm shock because its predominant alpha effect tightens the vasodilated circuit. Doses are started low, at around 0.05 to 0.1 microgram per kilogram per minute, and titrated to the perfusion endpoints: stronger pulses, warmer and better perfused skin, a shorter capillary refill, a mean arterial pressure appropriate for age, a falling lactate, and a urine output above 1 mL per kilogram per hour. [1] [10]
Dopamine is no longer the preferred first-line agent. The Surviving Sepsis Campaign children's guidelines recommend adrenaline or noradrenaline over dopamine, and a meta-analysis of randomised studies found no survival advantage for dopamine over adrenaline in paediatric and neonatal septic shock, with dopamine carrying a higher burden of dysrhythmia. Dopamine remains an option where adrenaline or noradrenaline is unavailable, but it is no longer the default. [1] [6]
Catecholamine-resistant shock
Shock that fails to correct despite adequate fluid and appropriately titrated vasoactive support is catecholamine resistant. The first move is to reconsider reversible causes: a missed tension pneumothorax or tamponade, ongoing haemorrhage, an undrained source, an electrolyte or metabolic derangement, or hypoadrenalism. Stress-dose hydrocortisone is suggested by the Surviving Sepsis Campaign for shock that is not responsive to adequate fluid and vasoactive therapy, particularly in children with known or suspected adrenal insufficiency. Vasopressin may be added as an adjunct in refractory vasodilatory shock, guided by intensive care. [1] [2]
Goals and monitoring
Set explicit resuscitation endpoints and watch the trend toward them. The targets are normal perfusion (warm, well-perfused skin with a capillary refill under 2 seconds), a mean arterial pressure normal for age, a falling lactate, a urine output above 1 mL per kilogram per hour, and a normal mental state. Advanced monitoring in intensive care may add central venous oxygen saturation and cardiac output assessment, but the bedside clinical signs remain the core of the reassessment. A child whose lactate is falling and whose perfusion is improving is heading the right way, even if the numbers are not yet normal. [1] [10]
Adrenaline (epinephrine) infusion — cold shock
Specific Subtypes & Scenarios
The resuscitation structure stays the same, but age, comorbidity, source and setting change what you watch for, which antibiotic you choose, and how early you escalate. [1]
Neonate and young infant
- May be afebrile or hypothermic with only poor feeding and floppiness
- Consider late-onset neonatal sepsis, metabolic disease and duct-dependent cardiac lesions
- Check bedside glucose early and correct a dangerous low immediately
- Use neonatal antibiotic and vasoactive dosing; seek senior and neonatal review early
Immunocompromised child
- May be neutropenic and afebrile with blunted signs
- Use a neutropenic sepsis antibiotic regimen covering gram-negative organisms
- Central line is often the source: consider removal in refractory line sepsis
- Escalate on physiology and risk context, not on fever alone
Severe malnutrition
- Reserve is limited and fluid tolerance reduced
- Reassess even more rigorously after each bolus
- Refeeding and electrolyte risks accompany resuscitation
- Dopamine, epinephrine and transfusion have been studied in this group; follow local protocol
Technology-dependent child
- Assess the child and the device in parallel
- Ask the caregiver what normal device function looks and sounds like
- Central line or implanted device is a likely source
- Use the personal emergency plan and the specialty pathway
Rural or remote setting
- Call retrieval in parallel with resuscitation, before local support is exceeded
- State equipment, staff, weather, distance and transport limits
- Begin fluid and antibiotics; arrange the safest escort and destination
- Agree a contingency for deterioration or transport delay
In severe malnutrition the principles hold but the margins narrow. These children have little cardiovascular reserve, and aggressive fluid can cause harm; boluses are smaller, reassessment is more frequent, and transfusion may be part of restoring oxygen-carrying capacity. A randomised study in children with severe malnutrition and fluid-refractory shock evaluated dopamine and epinephrine alongside transfusion, and its lesson is that resuscitation in this group must follow a tested, population-specific protocol rather than a transplanted generic one. [7]
Complications & Pitfalls
Most preventable harm in paediatric septic shock comes from one of three errors: waiting for hypotension, driving fluid as a target, or delaying the vasoactive agent. Each is a failure of reassessment rather than a failure of knowledge. [1] [9]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Waiting for hypotension to diagnose shock | Compensated shock is missed and decompensation follows | Diagnose from the whole circulation; treat poor perfusion now |
| Treating the fluid ceiling as a target | Fluid accumulation injury and worsening oxygenation | State the expected response; reassess after each bolus; stop for overload or no benefit |
| Delaying the vasoactive agent | Prolonged untreated shock and organ failure | Start adrenaline or noradrenaline after two or three refractory boluses; do not wait for collapse |
| Defaulting to dopamine | Higher dysrhythmia burden, no survival advantage | Use adrenaline for cold shock and noradrenaline for warm shock as first line |
| Delaying antibiotics beyond the first hour | Organism load and mortality rise | Give broad-spectrum antibiotics within the first hour; culture does not delay treatment |
| Forgetting glucose and electrolytes | Hypoglycaemia and dysrhythmia complicate the picture | Check and correct bedside glucose and electrolytes early |
| Missing a mechanical or cardiac cause | Reversible obstruction or myocarditis is left untreated | Seek tamponade, pneumothorax and cardiac dysfunction in fluid-refractory shock |
| Late escalation and retrieval | Support is unavailable when collapse happens | Call senior, PICU or retrieval before local support is exceeded |
After resuscitation, watch actively for harm from the treatment itself: fluid overload with pulmonary oedema, vasoactive extravasation causing tissue ischaemia, line-related infection or thrombosis, acute kidney injury, and critical-illness neuropathy or myopathy in the prolonged case. The child who survives the first hour still needs meticulous ongoing care, and a new sign can mark a complication as readily as a relapse. [1] [9]
[1] [6]Prognosis & Disposition
Disposition follows the trend and the response to treatment, not a single reassuring number. Consider the child's age and reserve, the severity and reversibility of organ dysfunction, the harm from treatment, the local resources, the transport risk, and whether the family can carry the plan forward. [1] [11]
Intensive care or retrieval
- Fluid-refractory, catecholamine-resistant or evolving shock
- Need for vasoactive support, mechanical ventilation or advanced monitoring
- Multi-organ dysfunction or a rising lactate despite treatment
- Transport risk that needs early specialist planning
High-dependency
- Physiology currently supported but trend, age or diagnosis needs close reassessment
- Monitoring and staffing can detect and respond to deterioration
- Vasoactive support being weaned with stable perfusion
- A named escalation pathway exists
Ward, then discharge
- Sustained normal perfusion off vasoactive support
- Falling lactate, rising urine output, normal mental state
- Source identified and controlled; antibiotics transitioned to oral where appropriate
- Family understands warning signs, access route and follow-up
Mortality in well-resourced settings is now comparatively low for previously well children who receive early, protocolised resuscitation, but it remains high in the very young, the malnourished, the immunocompromised and those with complex chronic disease. Survivors can develop new or progressive chronic conditions after a sepsis admission requiring critical care, so follow-up should screen for new morbidity as well as for recurrence. Give the family a clear safety net: what change to watch for, how urgently to act, and exactly where to return. [1] [11]
Special Populations
Adapt how you assess, dose and escalate, but never lower the standard for recognising shock. The principles of resuscitation apply across ages and abilities; the differences are in reserve, communication, drug handling and the social context. [1]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Neonate | Neonatal antibiotic and vasoactive dosing; check glucose and duct-dependent lesions; use neonatal life support at birth | State the local neonatal-to-paediatric boundary rather than inventing an age cut-off |
| Immunocompromised | Neutropenic regimen; central line likely source; afebrile does not exclude sepsis | Escalate on physiology and risk context |
| Severe malnutrition | Smaller reassessed boluses; transfusion may be needed; refeeding and electrolyte care | Follow a tested population-specific protocol |
| Disability or neurodiversity | Compare with the caregiver's baseline; use adapted communication and observation | A changed baseline is the key sign, not a single number |
| Indigenous, migrant or refugee | Use professional interpreters; respect cultural and family structures; address access barriers | Apply local consent and mandatory-reporting rules |
| Technology-dependent | Assess child and device; use the personal emergency plan; bring caregiver expertise in | The device may be both the source and the rescue |
Safeguarding runs in parallel with medical care, and immediate stabilisation comes first. Septic shock can arise from neglect, an untreated source, induced or fabricated illness, or an unsafe home environment. Ask only necessary open, non-leading questions, document objective findings and spontaneous words, and use the local safeguarding pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [1]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The structure of the first-hour bundle — early recognition, oxygen, access, reassessed fluid, antibiotics within the hour, and vasoactive support for fluid-refractory shock — is strongly endorsed by the Surviving Sepsis Campaign 2026 children's guideline and is consensus across the major resuscitation sources. What remains population- and resource-specific is the fluid strategy: how much, how fast, and when to stop. [1] [2]
Phoenix sepsis criteria
JAMA
International retrospective cohort development and validation study of a new paediatric sepsis definition
Key finding
The Phoenix score, based on cardiovascular, respiratory, neurological and coagulation dysfunction, defined paediatric sepsis (score 2 or more) and septic shock (sepsis with cardiovascular dysfunction) more robustly than the prior Sepsis-2 framework.
Practice change
Phoenix is the current international definition of paediatric sepsis and septic shock, replacing SIRS-based definitions.
The Phoenix criteria were developed to fix the central weakness of the older definitions: their dependence on systemic inflammatory response variables that are common and non-specific. A child has sepsis at a Phoenix score of 2 or more, and septic shock when that sepsis includes cardiovascular dysfunction. This definition is validated for prognostic performance and is now the international standard. The older pSOFA score remains a validated organ-dysfunction tool and is still used in research and at some centres, but Phoenix is the current consensus definition. [3] [8]
On vasoactive agents, the evidence favours adrenaline and noradrenaline over dopamine. A meta-analysis of randomised studies found no survival advantage for dopamine over adrenaline in paediatric and neonatal septic shock, and dopamine carried a higher dysrhythmia burden. The Surviving Sepsis Campaign therefore recommends adrenaline for cold shock and noradrenaline for warm shock as first-line agents, with dopamine demoted. [1] [6]
On fluid strategy, the debate between liberal and restrictive approaches remains active. A systematic review of restrictive versus liberal fluid strategies found that the evidence does not support an unqualified push to large fixed volumes, and supports the reassessed-aliquot approach with attention to fluid balance that the guidelines now advocate. The FEAST trial remains the cautionary anchor that no fluid algorithm can be transplanted uncritically across populations and resources. [4] [9]
Jurisdictional implementation
Australia and Aotearoa New Zealand: ANZCOR Guideline 12.2 is the 2026 regional paediatric advanced life support source. The Royal Children's Hospital Melbourne sepsis guideline supports local implementation of recognition and emergency management. Retrieval systems, antibiotic formularies, vasoactive availability and mandatory reporting remain state-, territory- or service-specific. In Aotearoa New Zealand, verify the active local sepsis, retrieval and safeguarding pathways rather than borrowing an Australian threshold.
Exam Pearls
Recognition
- Diagnose shock from the whole circulation, never the blood pressure
- Phoenix sepsis threshold is 2 or more points; septic shock adds cardiovascular dysfunction
- Tachycardia, cold mottled skin, prolonged capillary refill and weak pulses are the core signs
- A normal pressure never excludes shock
First hour
- Recognise and call for help; secure airway and oxygen
- Establish IV or IO access; send gas, lactate, glucose, cultures
- Reassessed fluid aliquots; the first-hour total is a ceiling, not a target
- Broad-spectrum antibiotics within the first hour
Vasoactive support
- Start after two or three refractory boluses or earlier if overloaded
- Adrenaline for cold shock; noradrenaline for warm shock
- Dopamine no longer first line
- Titrate to perfusion, MAP for age, lactate, urine output
Escalation
- Call senior, PICU or retrieval before local support is exceeded
- Catecholamine resistant: add hydrocortisone and seek reversible causes
- Arrest: adrenaline 10 micrograms per kg IV/IO, defibrillate at 4 J per kg
- Continuous reassessment from the top
Pitfalls
- No hypotension-waiting
- No fluid ceiling as target
- No delayed vasoactive
- No dopamine default
- No culture delaying antibiotics
“Recognise shock from the whole circulation → oxygenate and access → reassessed fluid aliquots → antibiotics within the hour → adrenaline for cold shock or noradrenaline for warm shock if fluid refractory → reassess and escalate before local support is exceeded.”
Viva: why adrenaline for cold shock and noradrenaline for warm shock?
Cold shock is a low-output, high-resistance state: the heart is failing and the vessels are tight. Adrenaline restores inotropy and therefore cardiac output, and adds an alpha effect at higher doses. Warm shock is a high-output, low-resistance state: the circuit is vasodilated. Noradrenaline's predominant alpha effect restores systemic vascular resistance and blood pressure. Choosing the drug for the phenotype corrects the dominant fault rather than worsening it.
Viva: what does FEAST actually teach?
FEAST found that saline or albumin bolus increased early mortality compared with no bolus in African children with severe febrile illness. Its correct lesson is not that fluid is forbidden, but that a fluid algorithm cannot be transplanted across populations, shock types and rescue resources. In a well-resourced setting, a child in septic shock still receives reassessed crystalloid aliquots, but the response is watched and the ceiling respected, and vasoactive support and retrieval are started early.
Structured oral: fluid-refractory shock in a rural hospital
State the diagnosis of fluid-refractory shock after two or three reassessed boluses. Begin adrenaline for the cold phenotype (or noradrenaline for warm shock) at 0.05 to 0.1 microgram per kilogram per minute and titrate to perfusion endpoints. Call retrieval in parallel, arrange central access and the safest escort, and agree the destination, the expected deterioration and the plan if transfer is delayed. Do not keep driving fluid toward a target while the child accumulates it.
References
- [1]Weiss, Scott L Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026 Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2026.PMID 41869844
- [2]Weiss, Scott L Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2020.PMID 32032273
- [3]Sanchez-Pinto, L Nelson Development and Validation of the Phoenix Criteria for Pediatric Sepsis and Septic Shock JAMA, 2024.PMID 38245897
- [4]Maitland, Kathryn Mortality after fluid bolus in African children with severe infection The New England journal of medicine, 2011.PMID 21615299
- [5]Bjorklund, Ashley Pediatric Shock Review Pediatrics in review, 2023.PMID 37777656
- [6]Wen, L The efficacy of dopamine versus epinephrine for pediatric or neonatal septic shock: a meta-analysis of randomized controlled studies Italian journal of pediatrics, 2020.PMID 31937353
- [7]Sarmin, Mohammed Efficacy of dopamine, epinephrine and blood transfusion for treatment of fluid refractory shock in children with severe acute malnutrition or severe undernutrition BMJ open, 2023.PMID 37045565
- [8]Balamuth, Frances Validation of the Pediatric Sequential Organ Failure Assessment Score and Evaluation of Third International Consensus Definitions for Sepsis and Septic Shock in Children JAMA pediatrics, 2022.PMID 35575803
- [9]Ali, Ahmed O Restrictive Versus Liberal Fluid Strategy for Initial Resuscitation in Sepsis and Septic Shock: A Systematic Review and Meta Analysis Journal of clinical medicine research, 2026.PMID 41953594
- [10]Lee, Eugene P Hemodynamic monitoring and management of pediatric septic shock Biomedical journal, 2022.PMID 34653683
- [11]Schlapbach, Luregn J Scoring Systems for Organ Dysfunction and Multiple Organ Dysfunction: The PODIUM Consensus Conference Pediatrics, 2022.PMID 34970683