Paeds · acute-care-resuscitation-and-toxicology
Shock in children: physiology and classification
Also known as Paediatric shock · Childhood circulatory failure · Compensated and decompensated shock in children · Classification of shock in children · Paediatric shock physiology
A fellowship approach to the physiology and classification of shock in children. Shock is inadequate delivery or use of oxygen and substrate at the mitochondrion, not a blood pressure number. Children compensate with tachycardia and vasoconstriction and maintain blood pressure until late, so recognise compensated shock from the whole child, watch the trend, and never wait for hypotension. Classify by haemodynamic phenotype as hypovolaemic, distributive, cardiogenic or obstructive, and grade severity as compensated, decompensated or irreversibly failing.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Shock is not low blood pressure. It is the state in which the delivery of oxygen and metabolic substrate to the tissues, or the cell's ability to use them, falls below demand, so cells shift to anaerobic metabolism and ATP production fails. Blood pressure is only one of several perfusion signs, and in children it is the last to fall. If you wait for hypotension to recognise shock you have already missed the child. [1] [9]
The clinical task is to spot the failing circulation from the whole child before blood pressure collapses, and to act on the trend. A child who is tachycardic with cool peripheries, prolonged capillary refill and altered interaction is in shock even when the blood pressure reads normal. A child whose perfusion improves after one action but then drifts back is still in shock and needs the next decision, not a pause. Shock is dynamic, and its management is reassessment. [1] [6]
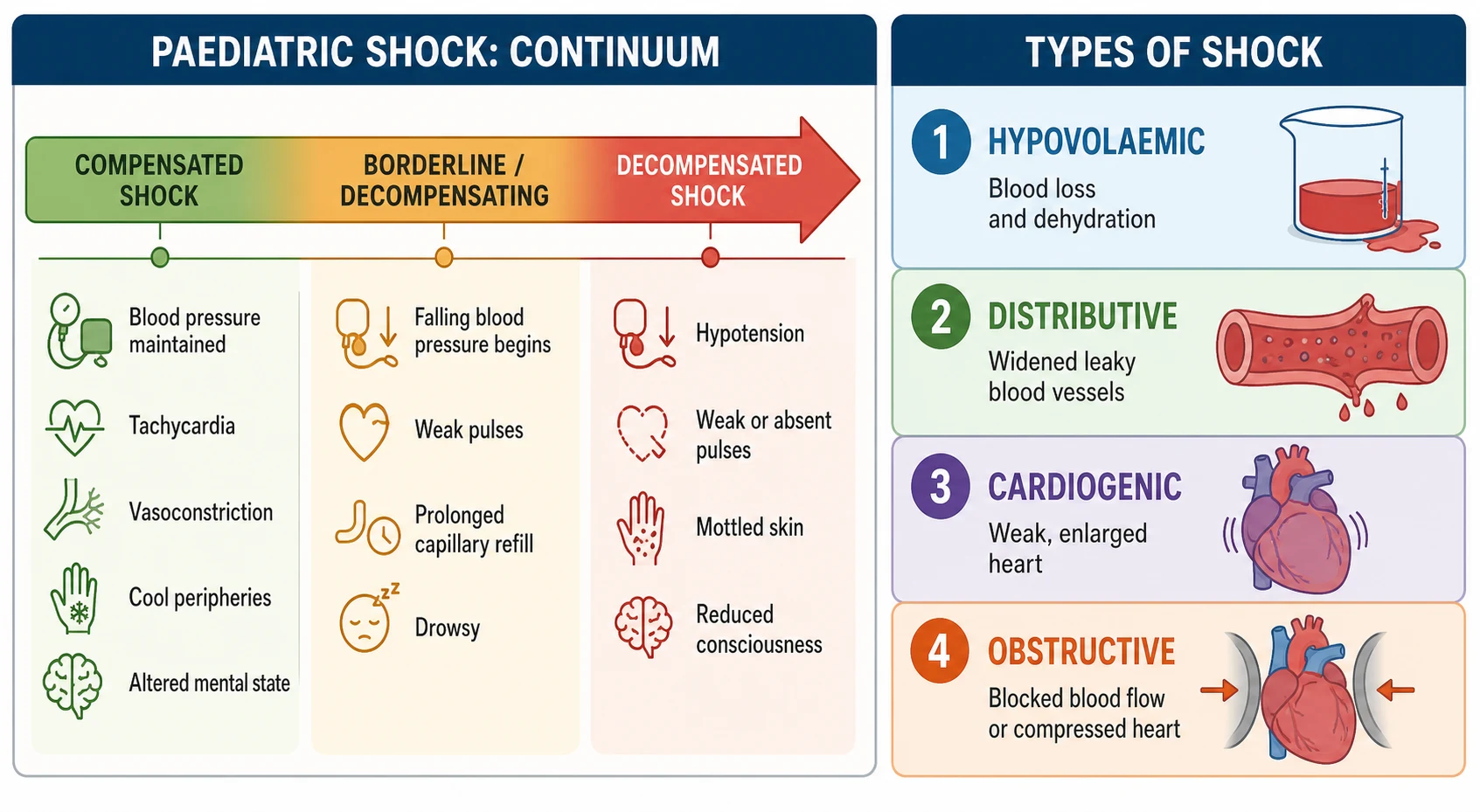
[1] [9]Shock grades through a recognisable trajectory as reserve is spent. Compensated shock keeps blood pressure in the normal range for age through tachycardia and vasoconstriction, even though perfusion is already failing at the tissue. Decompensated shock adds hypotension for age with falling consciousness and weak or absent pulses. Irreversible shock is the late phase in which organ failure and cell death can no longer be reversed even by restoring perfusion; the practical point is to act long before the child reaches it. Each grade changes the tempo and the first action. [1] [6]
This topic is the physiology and classification hub. It tells you what shock is, how to grade it, and how to name the type. The complete fluid, vasoactive and sepsis algorithms live in the dedicated septic shock resuscitation and paediatric life support pages; this hub gives the principles, the phenotypes and the thresholds that connect them. [5] [9]
Classification
Two classifications run together at the bedside. The first grades severity along the compensation-to-collapse continuum and tells you how urgently to act. The second names the haemodynamic phenotype and tells you what treatment will reverse the failure. Holding both at once is what separates a stable answer from a dangerous one. [1]
Severity: the compensation continuum
| Grade | Blood pressure | Hallmark signs | Clinical point |
|---|---|---|---|
| Compensated | Normal for age | Tachycardia, cool peripheries, prolonged capillary refill, weak peripheral pulses, reduced urine output, mild anxiety or irritability | Recognise from the whole child; blood pressure is still normal so do not wait for it to fall |
| Decompensated | Low for age | Weak or absent central pulses, cold mottled or pale skin, prolonged capillary refill, oliguria, drowsiness or confusion | Hypotension is late and dangerous; act on the trend before this point and escalate immediately here |
| Irreversible | Very low or unrecordable | Bradycardia, agonal breathing, multi-organ failure, no response to resuscitation | Cell death and organ failure can no longer be reversed; the goal is never to reach this phase |
Phenotype: what is failing in the circulation
| Type | Mechanism | Typical paediatric causes | Bedside clue |
|---|---|---|---|
| Hypovolaemic | Loss of circulating volume reduces preload and cardiac output | Haemorrhage, dehydration from gastroenteritis or DKA, burns, third-space losses, diabetic osmotic diuresis | Cold peripheries, narrow pulse pressure, clear volume-loss history |
| Distributive | Vasodilation and capillary leak maldistribute a normal or high volume | Sepsis, anaphylaxis, spinal or neurogenic shock, drug or toxin vasodilation | Warm peripheries early, wide pulse pressure, flash capillary refill, then cold as it worsens |
| Cardiogenic | Pump failure reduces cardiac output directly | Myocarditis, cardiomyopathy, congenital heart disease, dysrhythmia, post-arrest stunning, septic cardiomyopathy | Cold peripheries, hepatomegaly, gallop, raised jugular venous pressure, abnormal chest radiograph and echo |
| Obstructive | Mechanical obstruction limits cardiac output despite a normal pump | Tension pneumothorax, cardiac tamponade, massive pulmonary embolism, duct-dependent congenital obstructive lesions | Sudden collapse, asymmetric breath sounds, muffled heart sounds, differential cyanosis or femoral pulse deficit |
The phenotypes are not mutually exclusive. Septic shock classically combines distributive vasodilation and capillary leak with myocardial depression and often relative hypovolaemia, which is why a single sign such as warm skin never confirms one type and why treatment must be guided by reassessment. Anaphylactic shock is distributive but can carry a cardiogenic component late. Read the phenotype as the leading mechanism, keep the others open, and revise after every action. [1] [5]
Cold shock
- Cool mottled peripheries, weak thready pulses, narrow pulse pressure, prolonged capillary refill
- Low cardiac output with high systemic vascular resistance
- Typical of hypovolaemic, cardiogenic and late distributive shock
- Leads toward fluid then inotrope support
Warm shock
- Warm dry peripheries, bounding pulses, wide pulse pressure, flash capillary refill
- High or normal cardiac output with low systemic vascular resistance
- Typical of early distributive shock from sepsis or anaphylaxis
- Leads toward fluid then vasoconstrictor support
Epidemiology & Risk Factors
Shock is common in acutely ill children and it kills when recognition is late. Sepsis remains the leading pathway to paediatric shock worldwide, and the highest risk sits with the youngest infants, children with chronic or technology-dependent conditions, and families whose access to timely care is limited. Risk context changes the threshold to look for shock, not the definition of it. [5] [10]
The Improving Pediatric Sepsis Outcomes collaborative showed that bundled recognition and treatment across many hospitals reduced sepsis mortality, which is the clearest population-level argument that earlier recognition of shock changes outcome. The same evidence underlines that shock is missed, not rare: mortality fell because teams got faster, not because the disease became milder. [10]
Child and disease factors
- Young infant, especially under three months, with limited physiological reserve
- Chronic, multisystem or technology-dependent disease with a shifted baseline
- Immunocompromise or an attenuated inflammatory response
- Congenital heart disease, cardiomyopathy or pulmonary hypertension
- Recent surgery, trauma, burns or major fluid loss
Presentation factors
- Caregiver concern that the child is different from usual
- Poor intake, reduced urine output, altered behaviour or tone
- Fever with rigors, rash, pallor or mottling
- Known ingestion, anaphylaxis trigger, or traumatic mechanism
- Recurrent presentation or recent discharge
Health-system factors
- Rural distance, weather and delayed transport
- Limited monitoring, vasoactive agents or critical-care rescue on site
- Communication or language barriers
- After-hours or single-handed cover
- Incomplete observation sets and weak escalation systems
Young infants deserve special caution. A neonate has a relatively fixed stroke volume and relies almost entirely on heart rate to maintain cardiac output, so bradycardia is an ominous sign rather than recovery. Duct-dependent cardiac obstruction can present as shock in the first weeks of life as the ductus closes. Treat non-specific feeding or behaviour change in a young infant as high risk, check the bedside glucose, and seek senior review early. [2] [9]
Pathophysiology
Understanding why children compensate then collapse turns shock from a memorised list into a bedside skill. Oxygen delivery to the tissues depends on arterial oxygen content, cardiac output, the distribution of flow across the vascular bed, and the cell's ability to use oxygen. Shock begins when one or more of these fails, and the body mounts a stereotyped compensation that buys time at the cost of reserve. [1] [9]
Cardiac output is the product of heart rate and stroke volume. In infants and young children stroke volume is relatively fixed because the ventricle is less compliant, so the heart raises output mainly by increasing heart rate. Tachycardia is therefore the first and most important compensatory response to a falling stroke volume. Vasoconstriction then redirects the reduced output toward the brain and heart and away from the skin, muscle and splanchnic bed, which is why cool mottled skin and weak peripheral pulses appear while blood pressure is still preserved. [1] [2]
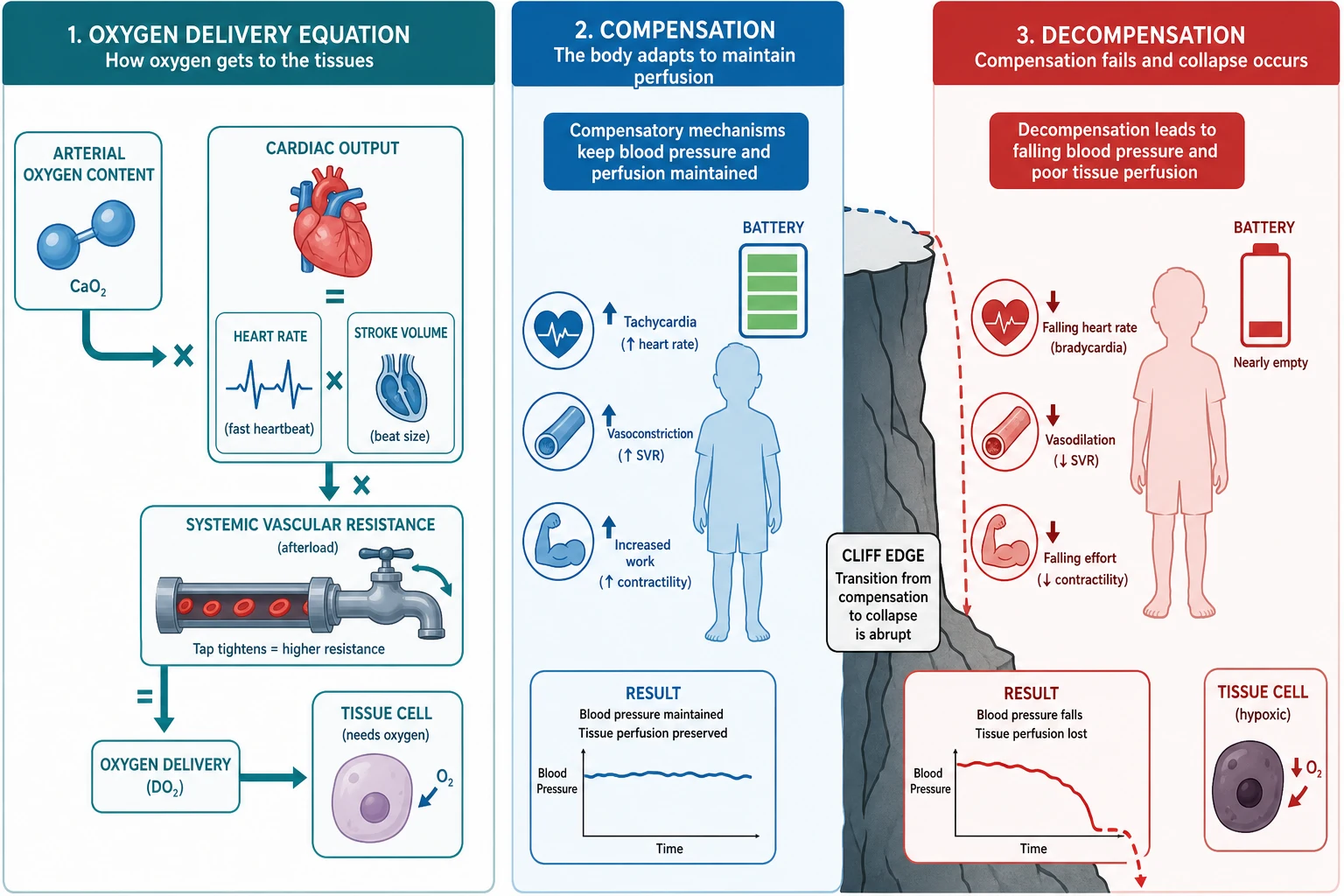
This is why blood pressure is maintained until late. Mean arterial pressure is held by raising systemic vascular resistance as cardiac output falls, so a normal blood pressure coexists with severe underperfusion. Hypotension appears only when compensation finally breaks, which is the haemodynamic cliff edge. Waiting for the number to drop is waiting for the child to be nearly dead. The same logic explains why a falling or abnormally low heart rate in a deteriorating child is a sign of decompensation, not reassurance: the compensatory tachycardia has failed. [1] [6]
Each phenotype fails the system at a different point. Hypovolaemic shock reduces preload and therefore stroke volume, so compensation is tachycardia and vasoconstriction against a smaller circulating volume. Distributive shock starts with vasodilation and capillary leak that lower effective circulating volume and venous return; early warm skin and a wide pulse pressure give way to cold shock as reserve is spent. Cardiogenic shock fails the pump directly, raising venous pressure and producing hepatomegaly and pulmonary congestion alongside poor perfusion. Obstructive shock limits filling or ejection mechanically, so the pump and the volume may both be normal but output still collapses. [1] [9]
At the cell, inadequate oxygen delivery forces a shift from aerobic to anaerobic metabolism. Lactate accumulates, hydrogen ions accumulate, and the sodium-potassium pump fails as ATP runs out, leading to cellular oedema and eventually cell death. This cellular failure is the substrate for multi-organ dysfunction and explains why a raised lactate or a worsening metabolic acidosis is a marker of severity and a target for resuscitation, not a number to chase in isolation. Restoring perfusion reverses anaerobic metabolism if the cell is still viable, which is the entire rationale for early, graded resuscitation. [1] [8]
Clinical Presentation
Recognise shock by integrating perfusion signs, not by reading a blood pressure. Begin at the doorway with the paediatric assessment triangle: appearance, work of breathing and circulation to skin. A child who is poorly interactive, floppy, pale or mottled, with fast laboured breathing or a weak cry, is in trouble before you touch them. State the concern, call for help, and move into the hands-on circulation assessment. [6]
The circulation assessment gathers pulse rate and quality, skin colour and temperature, capillary refill measured with the technique stated, blood pressure, mental state and urine output. Tachycardia out of keeping with fever, distress or pain is the single most important early sign. Cool peripheries with weak peripheral pulses and a narrow pulse pressure indicate a cold, low-output state. Warm peripheries with bounding pulses and a wide pulse pressure indicate a warm, vasodilated state. Either can be shock. [2] [3]
SHOCKED
Compensated shock
The compensated child looks unwell but holds their blood pressure. Heart rate is high for age and condition, peripheral pulses are weak while central pulses remain felt, the skin is cool and pale or mottled, capillary refill is prolonged beyond two to three seconds, and the child is irritable or anxious rather than alert and settled. Urine output falls. Blood pressure is normal for age, and this is exactly why compensated shock is missed: the reassuring number hides the failing perfusion. The trend toward these signs is the signal. [1] [9]
Decompensated shock
The decompensated child has crossed the cliff. Central pulses become weak or absent, the skin is cold, grey and markedly mottled, capillary refill is markedly prolonged, consciousness falls toward drowsiness or unresponsiveness, and blood pressure is now low for age. Bradycardia, sighing or irregular breathing and loss of consciousness herald imminent arrest. This is a pre-terminal state: move immediately toward the resuscitation and arrest pathways and call critical care in parallel. [6] [9]
| Life stage | Heart rate concern | Blood pressure concern |
|---|---|---|
| Neonate | Sustained above 160 or below 100 is abnormal | Systolic below 60 mmHg is hypotensive |
| Infant (1 to 12 months) | Sustained above 160 is abnormal | Systolic below 70 mmHg is hypotensive |
| Child (1 to 10 years) | Sustained above 140 with perfusion failure is abnormal | Systolic below 70 plus twice the age in years is hypotensive |
| Older child and adolescent | Sustained above 120 with perfusion failure is abnormal | Systolic below 90 mmHg is hypotensive |
The numbers above are widely taught thresholds to frame concern; they are not diagnostic cut-offs and they vary by source and condition. Fever, pain, fear and crying raise heart rate, so interpret any value in context and reassess after the child is settled. The principle that holds across every age is to integrate multiple signs and the direction of change, and never to exclude shock from a normal blood pressure. [2] [3]
Differential Diagnosis
The first differential question in shock is not "what is the disease" but "which part of the circulation is failing". Naming the failing component directs the first treatment, then the named disease takes over. Keep the phenotypes open in parallel because mixed shock is common, and revise the leading mechanism after every reassessment. [1] [9]
Hypovolaemic causes
- Haemorrhage from trauma, surgery or gastrointestinal bleeding
- Dehydration from gastroenteritis, poor intake or DKA osmotic diuresis
- Burns with large fluid and protein loss
- Third-space losses in pancreatitis, peritonitis or bowel obstruction
Distributive causes
- Sepsis and septic shock, the commonest pathway
- Anaphylaxis with food, drug, sting or latex trigger
- Spinal or neurogenic shock after high spinal cord injury
- Drug or toxin-mediated vasodilation, including poisoning and anaesthesia
Cardiogenic causes
- Myocarditis and cardiomyopathy
- Congenital heart disease, especially duct-dependent lesions and obstructive left-heart lesions
- Dysrhythmia: supraventricular tachycardia, complete heart block, ventricular arrhythmia
- Post-arrest myocardial stunning and septic cardiomyopathy
Obstructive causes
- Tension pneumothorax, especially in the ventilated child
- Cardiac tamponade after surgery, trauma or central line insertion
- Massive pulmonary embolism, rare but possible in adolescents and central-line carriers
- Duct-dependent obstructive congenital heart disease presenting as the duct closes
A few mimics must be separated from shock because their management differs. Syncope and vasovagal collapse produce brief hypotension with rapid spontaneous recovery and warm peripheries. Breath-holding produces a short loss of consciousness with a clear trigger. A simple febrile illness with tachycardia from fever alone has normal perfusion once the child is settled and rehydrated. These resolve or improve quickly; shock does not. When the picture does not fit a mimic, or does not improve, treat for shock and keep looking. [1]
Clinical & Bedside Assessment
Assess the whole circulation in one integrated pass. State each sign you find and integrate it rather than waiting for a single number to decide. Document the heart rate and pulse quality centrally and peripherally, the skin colour and temperature, the capillary refill with site and compression time stated, the blood pressure, the mental state and the urine output, then weigh them together against the child's baseline and age. [2] [3]
Measure capillary refill with a consistent technique. Compress the sternum or a fingertip pulp with firm pressure for five seconds, release, and time the return of colour. A refill beyond two to three seconds on the sternum is prolonged, but the test is heavily influenced by ambient temperature, the operator, the site and the child's distress, so it has only modest diagnostic value on its own. Treat it as one input that must agree with the rest of the circulation picture. [3]
[3]Blood pressure deserves its own warning. Because children hold mean arterial pressure through vasoconstriction, a normal reading is fully compatible with severe compensated shock. Hypotension for age is a late, pre-terminal sign. Use the blood pressure to confirm severity and trend, never to exclude shock. A widened pulse pressure with warm skin and bounding pulses points to distributive shock; a narrowed pulse pressure with cool skin and weak pulses points to hypovolaemic or cardiogenic shock. [1] [9]
Take a focused history in parallel with resuscitation. Ask what changed from the child's usual self, then probe for fluid loss, intake, fever, rash, collapse, seizure, trauma, ingestion, allergy and known cardiac or chronic disease. Obtain the baseline observations and the personal emergency plan if the child has complex needs. Use a professional interpreter whenever language is a barrier, and ask adolescents privately about substances and self-harm when it is safe to do so. [6]
Investigations
Stabilise first, then order a test only when it answers a named question. Bedside tests that change the immediate management of shock are few and fast: a point-of-care blood gas and lactate to quantify perfusion and acid-base state, a bedside glucose because hypoglycaemia complicates shocked children, a credible oxygen saturation, and an ECG whenever a cardiogenic or dysrhythmic cause is possible. [1] [8]
Immediate and bedside
- Point-of-care blood gas and lactate to quantify hypoperfusion and metabolic acidosis
- Bedside glucose whenever shock, altered consciousness or poor intake is present
- Credible oxygen saturation and ECG for any circulatory concern
- Blood pressure and capillary refill serially to track the trend
Conditional on a question
- Blood count, electrolytes, renal and hepatic function and coagulation for a defined branch
- Blood, urine and other cultures before antimicrobials when this does not delay time-critical treatment
- Ammonia and metabolic and endocrine samples when a metabolic cause is plausible
- Minimum necessary volume, with good pain relief
Targeted imaging
- Chest radiograph for cardiogenic or obstructive clues and to guide ventilation
- Echocardiography to assess pump function and obstruction, within operator competence
- Point-of-care ultrasound for tamponade or pneumothorax within competence
- Never move an unstable child to imaging without monitoring, escort and a rescue plan
Interpret the results as physiology and trend, not as binary reassurance. A raised lactate reflects anaerobic metabolism from poor perfusion and should fall with effective resuscitation; a normal lactate does not exclude shock. A metabolic acidosis with a high lactate and base deficit tracks severity. Lactate can also rise from seizures, shivering, liver dysfunction or epinephrine, so read it alongside the child. The Phoenix-8 sepsis criteria use organ dysfunction to define septic shock, and a structured organ-dysfunction assessment belongs in the shocked child, but no single score replaces the clinical circulation assessment. [8]
Management — Resuscitation
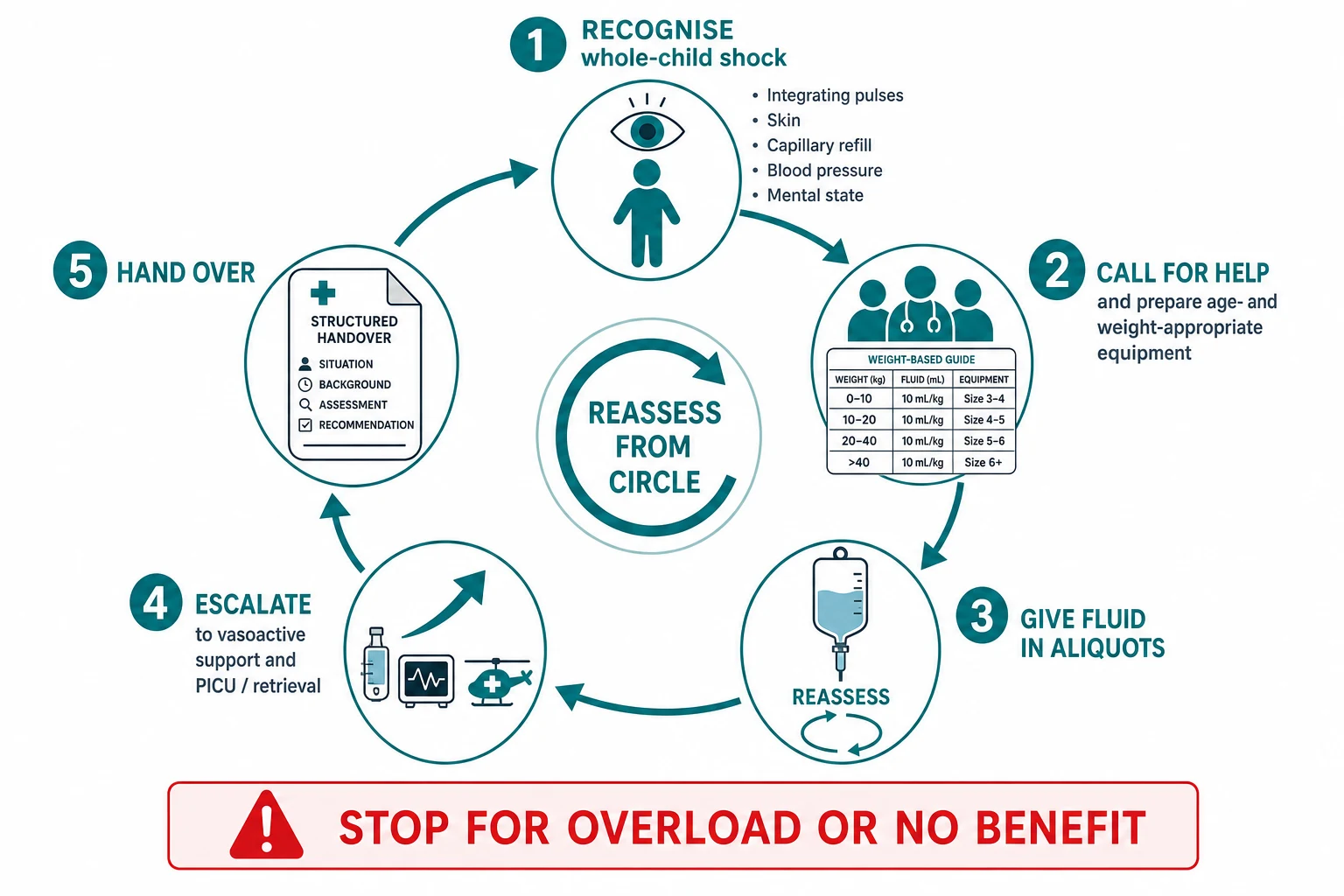
Resuscitation of the shocked child follows the same recognise, treat-as-found, reassess discipline as any acute presentation, focused on the circulation. Declare concern, call for help, name a leader, allocate roles, and bring age- and weight-appropriate equipment and monitoring. Give oxygen in failure, support ineffective breathing, control obvious fluid loss, gain access, and treat the circulation while the named-disease pathway is activated. Reassess from the start after every action. [6] [9]
The first ten minutes of paediatric shock
Recognise and call for help
State that the child is in shock from the whole circulation picture, call the senior and resuscitation or critical-care team, name a leader and allocate roles.
Support oxygenation and breathing
Give high-flow oxygen in failure; support ineffective breathing with bag-mask ventilation so the failing circulation is not also hypoxic.
Control loss and gain access
Apply direct pressure to external bleeding, establish intravenous or intraosseous access without repeated failed attempts, and send the immediate bedside tests.
Give fluid in aliquots with reassessment
For shock where fluid responsive, give a crystalloid aliquot, state the response you expect, reassess, and repeat only if still in shock and not overloaded.
Escalate to vasoactive support and critical care
If shock persists after aliquots or is clearly not fluid-responsive, start vasoactive support early and call PICU or retrieval in parallel, before local options are exhausted.
Reassess and hand over
After every action return to the whole circulation assessment, record benefit or harm, revise the phenotype, and give a structured handover with the trend and contingency.
Fluid: a ceiling, not a target
First decide whether the shock is likely to be fluid-responsive, which is usually true early in hypovolaemic and distributive shock. Give an isotonic crystalloid aliquot, state the response you expect before it goes in, and reassess the whole circulation immediately afterwards. The Surviving Sepsis Campaign 2026 children's guideline supports up-front fluid boluses in septic shock with careful reassessment and explicit attention to fluid balance, and the American College of Critical Care Medicine parameters frame the first-hour total as a ceiling rather than a goal. Stop the moment the child is no longer fluid-responsive or shows overload. [5] [9]
The FEAST trial is the cautionary anchor. In African children with severe febrile illness, saline or albumin bolus increased early mortality compared with no bolus. Its correct lesson is not that every bolus is harmful everywhere, but that a fluid algorithm cannot be transplanted across populations, shock types and rescue resources. Apply fluid strategy to the child in front of you, reassess rigorously after each aliquot, and escalate to vasoactive support and critical care rather than driving toward a fixed volume. [4]
Fluid bolus in paediatric shock (principle)
Vasoactive support and the decompensated child
If shock persists after the first fluid aliquots, or if the phenotype is cardiogenic or clearly not fluid-responsive from the outset, start vasoactive support early rather than pushing more fluid. The first agent follows the phenotype: a cold, low-output state leans toward an inotrope such as adrenaline, while a warm, vasodilated state leans toward a vasoconstrictor such as noradrenaline. The exact drug, dose and titration belong to the dedicated septic shock and critical-care pages and to local protocols; the principle here is to escalate to vasoactive support before the child arrests and to call critical care in parallel. [5] [9]
When shock becomes arrest
Bradycardia with poor perfusion, agonal or absent breathing and loss of consciousness mean the child is about to arrest or has arrested. Move directly into the paediatric arrest algorithm: high-quality chest compressions, ventilation with oxygen, attach a defibrillator, and establish intraosseous access. The arrest-dose anchors from the AHA 2020 and ILCOR 2020 paediatric life support sources are intravenous or intraosseous adrenaline at 10 micrograms per kilogram every three to five minutes, and defibrillation at 4 joules per kilogram for a shockable rhythm. Do not finish a survey of an arrested child. [6] [7]
[4] [9]Management — Definitive & Stepwise
After the immediate circulation is supported, move into the pathway for the named cause without stopping reassessment. The complete sepsis, anaphylaxis, cardiac, dysrhythmia, trauma and metabolic algorithms live in their dedicated pages; this hub states the principles that connect them. Treat the most reversible dangerous cause first while keeping the others open, and revise the leading phenotype after every reassessment. [1] [5]
From resuscitation to the right ongoing plan
Name the expected response
Before each action, state the change you expect in pulse quality, skin temperature, capillary refill, consciousness and urine output.
Measure what happened
Repeat the whole circulation assessment. Distinguish sustained improvement, brief improvement, no response and harm such as overload.
Choose the cause-specific pathway
Move to sepsis, anaphylaxis, cardiac, dysrhythmia, trauma, metabolic or obstructive care as the phenotype and the history clarify.
Agree monitoring and contingency
Specify the location, staff, observation intensity, response owner, next sign of failure and the action if transfer is delayed.
Hand over and dispose
Transfer baseline, trend, timed actions, response, unresolved risks, pending tests, family and safeguarding information, and the next action.
Improvement must be coherent across several findings. Better blood pressure alone does not prove restored perfusion. A warmer, better-perfused child who becomes more interactive and passes urine is improving; a child whose blood pressure rises but who remains mottled, oliguric and drowsy is not. A corrected glucose needs a documented recheck and a plan for the cause. Reassess after each action and after any meaningful change rather than waiting for a fixed interval. [3] [8]
Early critical-care and retrieval consultation
Call PICU or retrieval when the child may need support your service cannot reliably provide, not after every local option has failed. Discuss the likely support, the present monitoring and access, the equipment and staff limits, the transport time and weather, the safest destination, the escort, the expected deterioration and the plan if transfer is delayed. Exact thresholds, escort arrangements, transport mode and the accepting service remain local or regional. [6]
| Domain | Content that must cross the boundary |
|---|---|
| Identity and baseline | Age, measured or working weight, development, usual observations, devices and personal emergency plan |
| Physiology and trend | Current circulation findings, the shock grade and phenotype, and the direction of change |
| Actions and response | Each fluid aliquot and vasoactive agent, with time, dose, expected result and actual response |
| Reasoning | Prioritised phenotype-based differential, key tests, pending results and unresolved risks |
| Local limits | Access, equipment, staff, vasoactive and airway limits, transport constraints and requested destination |
| Child and family | Caregiver concern, communication needs, professional interpreter and family understanding |
| Contingency | Next failure marker, action if deterioration occurs and named ownership until transfer is complete |
Specific Subtypes & Scenarios
The classification stays the same, but the leading phenotype, the cause and the setting change what you expect and how early you escalate. In each scenario: diagnose shock from the whole child, name the phenotype, activate the correct pathway, and state what is specific to that context. [1]
Septic shock
- Commonest paediatric shock pathway; mixed distributive, cardiogenic and hypovolaemic
- Warm early, cold late; recognise from the trend before hypotension
- Fluid aliquots with reassessment, early vasoactive support, source control and antimicrobials
- Keep cardiogenic and obstructive causes open in parallel
Hypovolaemic shock
- Haemorrhage, dehydration, burns and third-space loss reduce preload
- Cold peripheries, narrow pulse pressure, clear volume-loss history
- Control the loss, give fluid aliquots, transfuse for haemorrhagic shock
- Reassess for ongoing concealed loss
Cardiogenic shock
- Myocarditis, cardiomyopathy, dysrhythmia and duct-dependent obstruction
- Cold peripheries, hepatomegaly, gallop, raised venous pressure
- Caution with fluid; early inotrope and cardiology input
- Treat dysrhythmia and duct-dependent lesions specifically
Obstructive shock
- Tension pneumothorax, tamponade, massive embolism, duct-dependent obstruction
- Sudden collapse, asymmetric breath sounds, muffled heart sounds
- Immediate needle or finger thoracostomy for tension; pericardiocentesis for tamponade
- A prostaglandin infusion for duct-dependent obstruction in the neonate
Anaphylactic shock
- Distributive shock with airway or breathing threat and a rapid trigger
- Intramuscular adrenaline is first-line, then fluid for shock
- Repeat adrenaline and escalate to infusion as the pathway allows
- Keep asthma, sepsis and vasovagal causes open
Neonate and young infant
- Duct-dependent cardiac obstruction presents as shock as the duct closes
- Fixed stroke volume: bradycardia is decompensation, not recovery
- Check bedside glucose early and start a prostaglandin infusion if duct-dependent
- State the local newborn to paediatric life support boundary
Trauma
- Hypovolaemic shock from haemorrhage is the default; preserve cervical spine and temperature
- Do not wait for hypotension; treat from the trend
- Obstructive causes: tension pneumothorax and tamponade
- Consider non-accidental injury when the history requires it
Rural or remote setting
- Call retrieval before the child needs support unavailable locally
- State equipment, staff, vasoactive and airway limits, distance and weather
- Agree a delayed-transfer contingency driven by acuity
- Package monitoring, access and escort for transport
Complications & Pitfalls
Most harm in paediatric shock begins with one of two errors: recognising it too late because a single sign was reassuring, or treating it too hard because a fluid volume became a target. The defences are the same habits that protect every resuscitation: integrate the whole child, follow the trend, state the expected response before each action, and reassess afterwards. [1] [4]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Waiting for hypotension to diagnose shock | Compensated shock is missed until near-arrest | Diagnose from the whole circulation and the trend; treat before blood pressure falls |
| Treating the first-hour fluid total as a target | Fluid overload, pulmonary oedema and harm | Give fluid in aliquots with reassessment; stop for overload or no benefit |
| Naming the shock type from a single sign | Warm skin or a wide pulse pressure is misread as well | Hold the phenotypes in parallel; sepsis is commonly mixed; revise after each action |
| Anchoring on the referral diagnosis | The true phenotype is missed while the label is chased | Reassess the circulation and revise the leading mechanism after every action |
| Using adult blood pressure or heart-rate thresholds | Age-appropriate concern is missed, especially in infants | Apply age-specific thresholds and interpret in context |
| Repeated failed vascular access attempts | Resuscitation is delayed while access is sought | Move to intraosseous access early rather than persisting with peripheral attempts |
| Delaying vasoactive support for more fluid | Cardiogenic or non-responsive shock is drowned | Escalate to vasoactive support when the child is no longer fluid-responsive |
| Late retrieval call | The child arrests before critical care arrives | Call retrieval before local options are exhausted |
After stabilisation, look actively for harm from treatment. Fluid overload shows as a rising respiratory rate, basal crackles, hepatomegaly and gallop, and it demands stopping fluid and starting respiratory or vasoactive support. Intraosseous and vascular-access sites need monitoring for dislodgement, extravasation and infection. Repeated sampling and cold exposure add their own harm. The fact that the child did not arrest does not prove that an intervention was harmless. [4] [9]
[1] [9]Prognosis & Disposition
Outcome in paediatric shock depends on the age and reserve of the child, the duration and severity of organ dysfunction before treatment, the reversibility of the cause, the harm from treatment, and the quality and speed of the local and retrieval response. Early recognition and bundled treatment reduce mortality, and survivors can carry new or progressive conditions after critical sepsis, so disposition must look beyond survival. [10] [11]
Critical care or retrieval
- Unresolved or worsening shock despite aliquots
- Need for vasoactive support, ventilation or monitoring unavailable locally
- Cardiogenic, obstructive or mixed shock needing subspecialty input
- Transport risk that needs early specialist planning
Ward or high-dependency
- Shock reversed but trend, age or diagnosis needs close reassessment
- Monitoring and staffing can detect and respond to recurrence
- Pending tests or treatment response still change disposition
- A named escalation pathway exists
Discharge only when defensible
- Sustained stability after appropriate reassessment
- No unresolved high-harm diagnostic concern
- Caregiver concern addressed and understanding confirmed
- Specific warning changes, access route, follow-up and pending-result ownership agreed
Children who survive septic shock can develop new and progressive medical conditions in the months that follow, so recovery includes a plan for follow-up of physical, developmental and psychological needs. A useful safety net states what change to watch for, how urgently to act, and exactly where or how to get help, and it names who owns pending results and when review occurs. After a critical event, explain what happened and what remains uncertain, invite questions, and consider debriefing for the child, family and team. [11]
Special Populations
Adapt how you observe, examine and communicate, but never lower the standard for recognising shock. Evidence for recognition tools is sparse in several populations, so present these adaptations as safer practice, not as proven improvements in diagnostic accuracy. [1]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Neonate or young infant | Treat non-specific change as high risk; check glucose early; consider duct-dependent obstruction and a prostaglandin infusion | State the local newborn to paediatric life support boundary |
| Complex or technology-dependent child | Establish personal baseline, device function and emergency plan; assess child and device in parallel | A chronically abnormal observation is not automatically safe; compare with the personal baseline |
| Severe neurodisability | Establish usual interaction, tone and pain expression; treat caregiver-described change as evidence | Adaptation improves communication, not proven diagnostic sensitivity |
| Immunocompromised child | Absence of fever does not exclude shock; sample and escalate on context | Do not delay time-critical treatment for complete sampling in an unstable child |
| Adolescent | Create private time; ask about substances, self-harm and pregnancy; explain confidentiality limits | Confidentiality has safety limits; safeguarding duties still apply |
| Indigenous, migrant or remote family | Use cultural safety and a professional interpreter; address access and transport barriers | Retrieval and safeguarding routes remain jurisdiction-specific |
Safeguarding runs in parallel with medical care, but immediate stabilisation and safety come first. Ask only necessary open, non-leading questions. Explain confidentiality and information sharing, document objective findings and spontaneous words, preserve evidence when safe, and use the local safeguarding pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [6]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The cellular definition of shock and the compensation-to-collapse trajectory are consensus physiology, supported across the AHA 2020 Paediatric Life Support guideline, the ILCOR 2020 consensus, the American College of Critical Care Medicine 2017 parameters and the Surviving Sepsis Campaign 2026 children's guideline. The structure is not in dispute; the specific fluid volumes, vasoactive agents, thresholds and oxygen targets attached to each step are source-, age- and population-specific. [5] [6]
FEAST
New England Journal of Medicine
Randomised fluid-bolus trial in African children with severe febrile illness
Key finding
Saline or albumin bolus increased 48-hour mortality compared with no bolus in that population.
Practice change
Fluid strategy must stay specific to the population, shock type and available rescue; do not transplant protocols uncritically.
The Phoenix-8 international consensus criteria reframed paediatric sepsis and septic shock around organ dysfunction rather than the old systemic inflammatory response criteria, and they perform better across populations. They define septic shock as sepsis with cardiovascular dysfunction, but they do not replace the bedside recognition of compensated shock, which remains a clinical, whole-child judgement. [8]
The Surviving Sepsis Campaign 2026 children's guideline supports early recognition and first-hour fluid resuscitation with vasoactive support for septic shock, with explicit attention to fluid balance. The Improving Pediatric Sepsis Outcomes collaborative showed that bundled care reduced sepsis mortality across many hospitals, which is strong population-level evidence that faster recognition and treatment of shock change outcome. The exact crystalloid choice, aliquot size and first vasoactive agent are read alongside local resources and the child's shock phenotype. [5] [10]
Capillary refill has modest diagnostic value and is highly technique-dependent, blood pressure is a late marker, and there is no universal vital-sign range, fluid volume or vasoactive dose that fits every child. Attach each rule to its population, purpose, conditions and jurisdiction. [2] [3]
Jurisdictional implementation
Australia and Aotearoa New Zealand: ANZCOR Guideline 12.2 is the 2026 regional paediatric advanced life support source. The Royal Children's Hospital Melbourne shock overview and the acceptable ranges for physiological variables support local implementation. Retrieval systems, observation charts, vasoactive availability, mandatory reporting and consent remain state-, territory- or service-specific. In Aotearoa New Zealand, verify the active local deterioration, retrieval and safeguarding system rather than borrowing an Australian threshold.
Exam Pearls
Definition
- Shock is failed oxygen and substrate delivery or use at the cell, not a blood pressure number
- Compensated shock keeps blood pressure normal; decompensated shock adds hypotension
- Irreversible shock is the late phase to be avoided, not reached
Classification
- Grade severity: compensated, decompensated, irreversible
- Name phenotype: hypovolaemic, distributive, cardiogenic, obstructive
- Cold shock vs warm shock points to inotrope vs vasoconstrictor
- Mixed shock is common in sepsis; revise after each reassessment
Recognition
- Tachycardia out of keeping with fever or distress is the key early sign
- Integrate pulses, skin, capillary refill, blood pressure, mental state, urine output, trend
- Do not wait for hypotension; it is late and dangerous
- Bradycardia in a deteriorating child is decompensation, not recovery
Resuscitation principles
- Recognise, call for help, oxygen and ventilation, control loss, access
- Fluid 10 to 20 mL per kilogram aliquots with reassessment; a ceiling not a target
- Escalate to vasoactive support when no longer fluid-responsive
- Arrest: adrenaline 10 micrograms per kilogram IV or IO, defibrillation 4 J per kilogram
Pitfalls
- No hypotension-waiting for shock
- No fluid volume as a target
- No single-sign typing
- No adult thresholds or late retrieval
“Shock is failed cellular oxygen delivery, recognised from the whole child and the trend, never from blood pressure. Classify severity and phenotype, give fluid in aliquots with reassessment, escalate to vasoactive support and critical care early, and never wait for hypotension.”
Viva: why does a child maintain blood pressure until late?
Because cardiac output is heart-rate dependent in young children, and mean arterial pressure is held by raising systemic vascular resistance as output falls. Tachycardia and vasoconstriction preserve blood pressure and cerebral perfusion while perfusion to skin, gut and muscle quietly fails. Hypotension appears only when compensation finally breaks, which is the haemodynamic cliff edge. Waiting for the blood pressure to drop is waiting for the child to be nearly dead.
Viva: compensated versus decompensated shock
Compensated shock keeps blood pressure normal for age through tachycardia and vasoconstriction, with cool peripheries, weak peripheral pulses, prolonged capillary refill, reduced urine output and irritability. Decompensated shock adds hypotension for age with weak or absent central pulses, cold mottled skin, falling consciousness and oliguria. The boundary is clinical and dynamic: a child can cross it in minutes, so recognise and act in the compensated phase.
Structured oral: warm versus cold shock and the first vasoactive agent
Warm shock is high or normal output with low systemic vascular resistance: warm dry peripheries, bounding pulses, a wide pulse pressure and flash capillary refill, typical of early distributive shock. It leans toward a vasoconstrictor such as noradrenaline once fluid-responsive shock is exhausted. Cold shock is low output with high resistance: cool mottled peripheries, weak thready pulses, a narrow pulse pressure and prolonged refill, typical of hypovolaemic, cardiogenic and late distributive shock. It leans toward an inotrope such as adrenaline. The first agent follows the phenotype, and the exact dose belongs to local protocol and the dedicated critical-care pages.
References
- [1]Bjorklund, Ashley Pediatric Shock Review Pediatrics in review, 2023.PMID 37777656
- [2]Fleming, Susannah Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies Lancet (London, England), 2011.PMID 21411136
- [3]Fleming, Susannah The Diagnostic Value of Capillary Refill Time for Detecting Serious Illness in Children: A Systematic Review and Meta-Analysis PloS one, 2015.PMID 26375953
- [4]Maitland, Kathryn Mortality after fluid bolus in African children with severe infection The New England journal of medicine, 2011.PMID 21615299
- [5]Weiss, Scott L Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026 Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2026.PMID 41869844
- [6]Topjian, Alexa A Part 4: Pediatric Basic and Advanced Life Support 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Pediatrics, 2021.PMID 33087552
- [7]Maconochie, Ian K Pediatric Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations Circulation, 2020.PMID 33084393
- [8]Schlapbach, Luregn J International Consensus Criteria for Pediatric Sepsis and Septic Shock JAMA, 2024.PMID 38245889
- [9]Davis, Allan de Caen The American College of Critical Care Medicine Clinical Practice Parameters for Hemodynamic Support of Pediatric and Neonatal Septic Shock: Executive Summary Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2017.PMID 28723883
- [10]Paul, Fran Balamuth Bundled Care to Reduce Sepsis Mortality: The Improving Pediatric Sepsis Outcomes (IPSO) Collaborative Pediatrics, 2023.PMID 37435672
- [11]Carlton, Emily F New and Progressive Medical Conditions After Pediatric Sepsis Hospitalization Requiring Critical Care JAMA pediatrics, 2022.PMID 36215045