Paeds · acute-care-resuscitation-and-toxicology
Submersion injury and hypothermia
Also known as Drowning · Non-fatal drowning · Submersion injury · Cold water immersion · Accidental hypothermia · Hypothermic submersion cardiac arrest
Fellowship guide to submersion injury (drowning) and hypothermia in children: the van Beeck definition, the Szpilman severity stratification, the asphyxial and cold-water pathways, the rescue-breath-first and rewarming ladders, hypothermic cardiac arrest ('warm and dead'), prognostic factors, and drowning prevention.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old is carried into the emergency department blue and limp, pulled from a backyard pool minutes before, and a teenager arrives cold and unconscious after falling through winter ice into a lake. These are the two faces of submersion injury, and the decisions in the first minutes decide whether the child survives intact, survives disabled, or dies. Submersion injury is the umbrella term for the harm that follows being under or in water; drowning is now defined, since the 2002 World Congress on Drowning and the van Beeck consensus, as the process of experiencing respiratory impairment from submersion or immersion in liquid, with outcomes classified as death, morbidity, or no morbidity. [1]
The definition was written deliberately to kill off a vocabulary that muddles care and prognosis. The terms near-drowning, secondary drowning, wet and dry drowning, and active versus passive drowning are obsolete and must not be used, because they describe neither mechanism nor severity and they obscure outcome reporting. A child either drowned and died, drowned with morbidity, or drowned without morbidity — there is no "near" about it. The standardised Utstein template then asks every rescuer to record the time intervals — submersion time, time to first rescue breath, scene time, and return of spontaneous circulation — because submersion duration is the single strongest predictor of survival. [2]
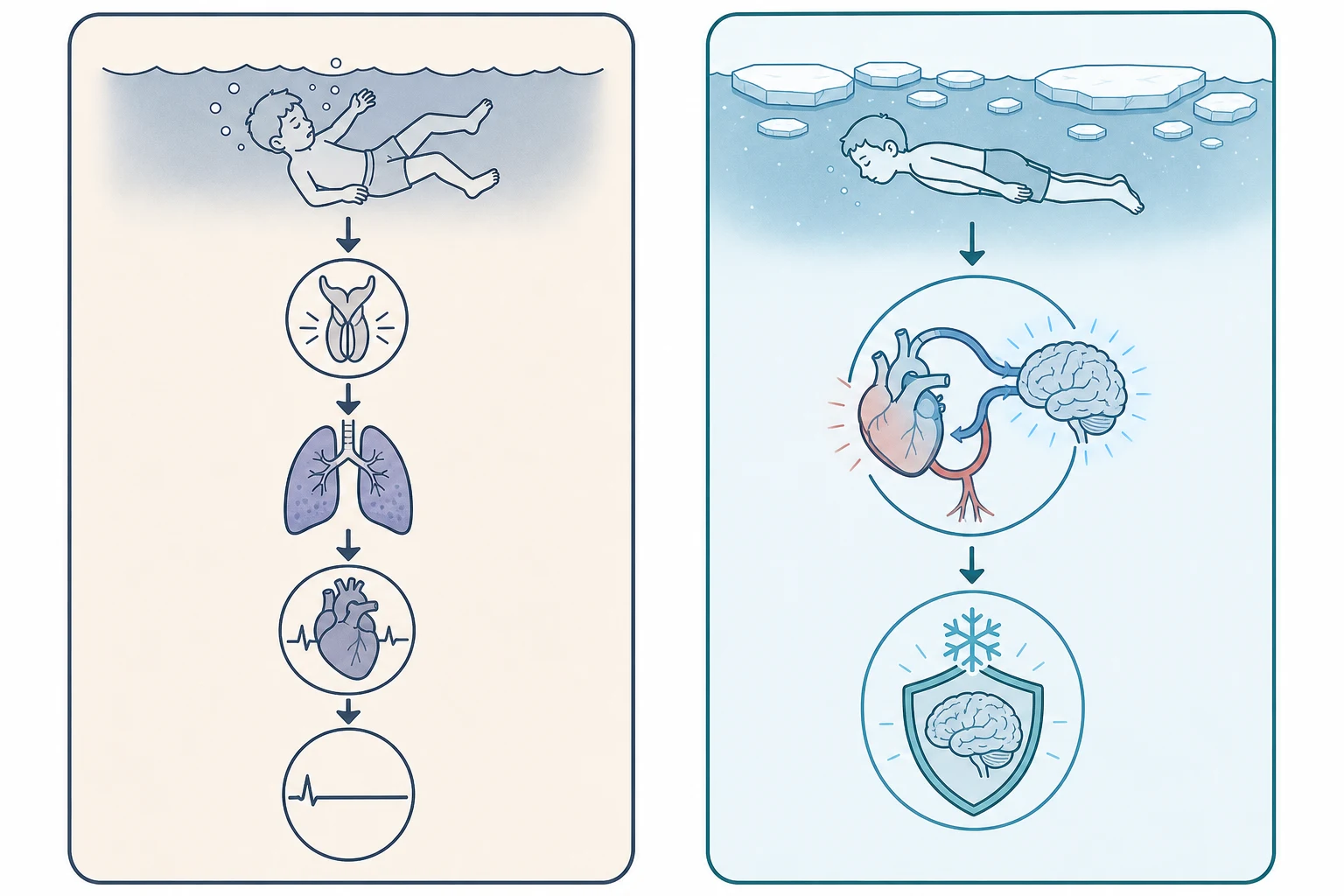
Two mechanisms run in parallel in the submerged child. The first is asphyxia: liquid in the airway triggers laryngospasm or floods the alveoli, gas exchange stops, oxygen falls, and the heart slows and arrests from hypoxia. The second is temperature: cold water cools the body, and in the right circumstances that cooling protects the brain by lowering its metabolic demand. These two mechanisms explain why a child pulled cold and pulseless from ice water can sometimes recover intact after an hour, and why a warm-water drowning of the same duration is usually fatal. Drowning and hypothermia must therefore be assessed and managed together, not separately. [1] [6]
Classification
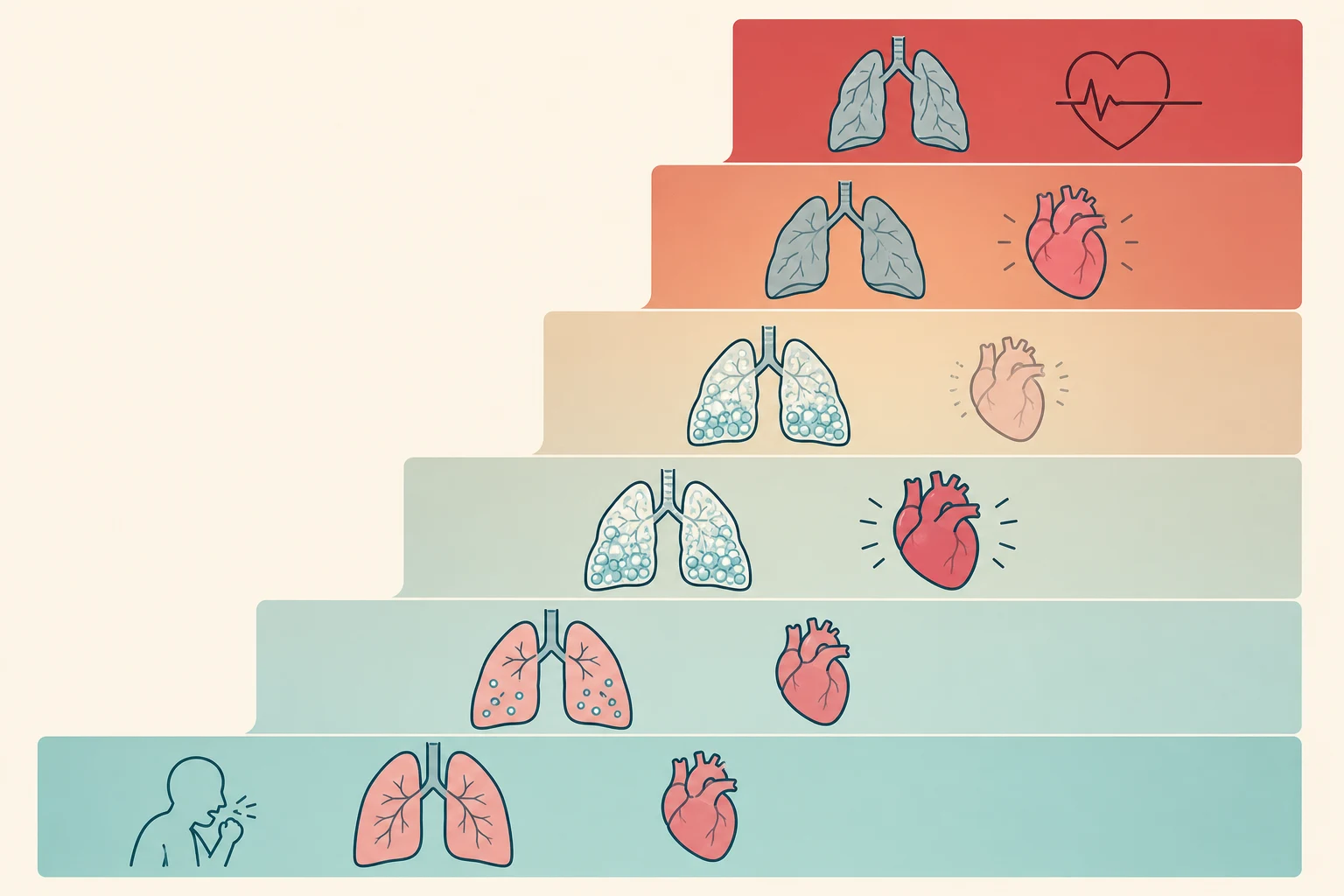
A drowned child is classified along two axes — the severity of the lung injury and the depth of the hypothermia — because each axis changes both the resuscitation and the prognosis. The lung-injury axis is captured by the Szpilman drowning classification, built from the analysis of 1,831 cases on Brazilian beaches, which stratifies presentation into six grades of rising mortality. Grade one is cough with normal auscultation; grade two adds scattered crackles; grade three is pulmonary oedema without hypotension; grade four is pulmonary oedema with hypotension; grade five is isolated respiratory arrest with a pulse; and grade six is cardiopulmonary arrest. Mortality rises stepwise through these grades — from near zero in grades one and two to roughly three per cent in grade three, fourteen per cent in grade four, a third in grade five, and around three-quarters in grade six. [3]
A modern reappraisal confirmed that this stratification still tracks prognosis for severe cases and that the grade assigned at the scene is one of the few reliable early signals of who will recover. The reappraisal also sharpened the clinical point that the grade can climb in the first hours: a child who looks well at grade one or two can develop pulmonary oedema and hypoxaemia over four to six hours, so observation is mandatory even after an apparently trivial event. [4]
The hypothermia axis is classified by the Swiss (Bernese) staging, which uses the core temperature and the clinical state rather than a thermometer alone, so that a rescuer can stage a child in the field. Stage one is mild hypothermia at thirty-five to thirty-two degrees, with a clear conscious level and shivering. Stage two is moderate, thirty-two to twenty-eight degrees, with impaired or altered consciousness. Stage three is severe, twenty-eight to twenty-four degrees, with unconsciousness but vital signs still present. Stage four is profound, below twenty-four degrees, with no detectable vital signs and a high risk of cardiac arrest. A child can sit anywhere on this axis independent of the lung grade, and the staging decides the rewarming strategy. [6]
Hypothermia severity by Swiss stage
- Core 35 to 32 degrees Celsius
- Clear consciousness, shivering
- Passive rewarming
- Low arrhythmia risk
- Core 32 to 28 degrees
- Impaired or altered consciousness
- Active external rewarming
- Arrhythmia risk rising
- Core 28 to 24 degrees
- Unconscious, vital signs present
- Active internal rewarming
- High arrhythmia risk, move gently
- Core below 24 degrees
- No vital signs, cardiac arrest risk
- Extracorporeal rewarming
- Nobody dead until warm and dead
Epidemiology & Risk Factors
Drowning is a global child-health emergency and one of the commonest causes of unintentional injury death in the young. The World Health Organization estimates that around a quarter of a million people die by drowning each year, and drowning ranks among the leading causes of unintentional injury death worldwide, with the burden falling hardest on children and on low- and middle-income countries where most deaths occur. In high-income settings the under-fives carry the highest rate, typically around home pools, baths, and garden water features; older children and adolescents add open-water and boating deaths, and males drown at several times the rate of females. [11]
The risk factors cluster by age and environment. Infants and toddlers drown in buckets, baths, and unfenced pools in the seconds a caregiver looks away; school-age children drown in rivers, lakes, and at the beach, often after underestimating depth or current; and adolescents add alcohol, risk-taking, and boating without life jackets. Children with epilepsy, with autism spectrum disorder, and with complex chronic conditions are over-represented, and in many regions Aboriginal, Torres Strait Islander, Maori, and Pacific children, and children in remote communities, carry a disproportionate burden tied to water access and reduced supervised swimming. [11]
Outcomes are dominated by two modifiable scene factors that an examiner will probe. The first is the submersion time, which is the single strongest predictor of survival — submersion under five minutes favours a good outcome and submersion beyond ten minutes is usually grim, with the dramatic exception of cold-water immersion. The second is bystander resuscitation, because drowning is an asphyxial arrest and the child who receives rescue breaths early reaches hospital with a better chance. Together these explain why resuscitation should be started and continued at the scene and the child transported, rather than declared dead in the field. [10] [12]
Pathophysiology
To resuscitate a drowned child well you must hold the asphyxial cascade and the protective cold mechanism together. The dominant event is asphyxia: when the face is submerged, breath-holding is followed by panic, swallowing, and then either laryngospasm or aspiration of liquid. Gas exchange stops, the alveolar-capillary membrane is injured, surfactant is washed out and disrupted, and a non-cardiogenic pulmonary oedema develops — the frothy, pink fluid that characterises the severe drowning lung. Arterial oxygen falls, the hypoxic myocardium bradycardes, and the child progresses through Szpilman grades until, at grade six, the heart arrests in asystole or pulseless electrical activity from hypoxia. [1] [2]
The volume of liquid aspirated is small and is not the point — the lungs do not "fill with water" in the popular sense, and only a few millilitres per kilogram are enough to wreck gas exchange. This is why attempted drainage manoeuvres, hanging the child head-down, or abdominal thrusts to "empty the water" are useless and dangerous — they delay rescue breaths, provoke vomiting and aspiration, and are not recommended. The treatment of the drowning lung is oxygen, positive pressure, and time, and the resuscitation starts with ventilation, not drainage. [5]
The second mechanism, cold-water protection, is what makes submersion injury so unpredictable and so important to understand. Sudden immersion in cold water triggers the diving response — bradycardia, peripheral vasoconstriction, and a shunting of oxygenated blood to the heart and brain — while rapid cooling of the brain lowers its metabolic oxygen demand. In the right child, in truly cold water, these two effects extend the window of cerebral tolerability to hypoxia well beyond the four to six minutes of a warm-water drowning, which is the physiological basis for attempting prolonged resuscitation in cold-water submersion. The protective effect is not guaranteed: it depends on the speed and depth of cooling and on the child, and warm water confers none of it. [6] [9]
Hypothermia, once established, becomes a separate threat through its effect on the heart. As core temperature falls, conduction slows, the PR and QT intervals lengthen, and the risk of ventricular arrhythmia rises sharply below thirty degrees. The cold myocardium is electrically irritable, which is why rough handling, jarring transport, or sudden movement can precipitate ventricular fibrillation — the practical rule that a cold child is moved gently and never roughly. Below twenty-eight degrees the risk is high, and below twenty-four degrees the child may be in or close to cardiac arrest. [6] [7]
Clinical Presentation
The presentation spans the whole spectrum, from the child who coughs once and looks well to the child carried in cold, blue, and pulseless. At the scene the immediate question is the same as for any arrest: is the child unresponsive and not breathing normally? If so, begin the drowning sequence with airway opening and five rescue breaths. The child who is breathing but coughing, with crackles or frothy sputum, has a Szpilman grade two or three injury and needs oxygen and observation, because the grade can climb over hours. The child who is apnoeic with a pulse is in grade five and needs immediate bag-mask ventilation, and the child with no pulse is in grade six and needs the full arrest algorithm. [3] [5]
The history at the scene must capture the factors that drive prognosis and that the Utstein template demands: the submersion time, the water temperature and type (pool, bathtub, sea, ice), the time to first rescue breath and to bystander cardiopulmonary resuscitation, any mechanism of injury such as a dive or a fall, and any comorbidity such as epilepsy, a seizure, or a cardiac event that preceded the submersion. A history of a seizure in the water, a long QT syndrome unmasked by cold water, or a primary arrhythmia can flip the assumed mechanism from asphyxia to cardiac, and a dive or a fall raises the cervical spine. [2]
A frequent and dangerous pitfall is the child who looks well in the first hour and is sent home. Drowning lung injury can evolve over four to six hours into pulmonary oedema and hypoxaemia, so any child with a significant submersion — any symptoms, any abnormality on examination, or any desaturation — must be observed, and the well child who is asymptomatic with normal saturations and examination for a sustained period is the only one suitable for discharge with clear safety-net advice. [3] [4]
Differential Diagnosis
During the resuscitation the differential condenses to the causes that sit behind the drowning and that change management. The first is cervical spine injury, suggested by a dive, a slip, a fall, a boating collision, or signs of trauma, which mandates a jaw thrust and inline immobilisation while the airway is opened — though routine spinal immobilisation is not needed for a simple swimming-pool drowning without a mechanism of injury. The second is a primary cardiac event, because a sudden arrhythmia in the water — a channelopathy such as long QT, or a commotio cordis — can present as drowning, and cold-water immersion is a classic trigger for long-QT-related arrhythmia. [5]
Reversible considerations in the submerged child
- Laryngospasm and aspiration
- Pulmonary oedema from the drowning lung
- Hypoxaemia out of proportion to examination
- Tension pneumothorax if ventilated
- Cervical spine injury from a dive or fall
- Primary arrhythmia — long QT, commotio cordis
- Hypoglycaemia in the cold or exhausted child
- Hypothermia raising the arrhythmia threshold
The third is hypoglycaemia, common in the cold, exhausted, or convulsing child and easy to miss, which a bedside glucose corrects. The fourth is hypothermia itself, which both causes arrhythmia and resists defibrillation and drug action, and which must be staged and treated alongside the drowning. The fifth, and the one that must not be missed in a young child, is non-accidental injury: a submersion that is unwitnessed, where the history is inconsistent or changing, where there is a delay in seeking help, or where there are other injuries, raises safeguarding concerns and demands the same structured assessment as any suspected maltreatment. [5]
Clinical & Bedside Assessment
The assessment runs inside the rescue-breath-first sequence, not beside it. The first ten seconds confirm the arrest: is the child unresponsive and not breathing normally? Open the airway with a head tilt and chin lift, or a jaw thrust if a dive or fall raises the cervical spine, and look, listen, and feel for no more than ten seconds. If the child is not breathing normally, give five rescue breaths — each about one second, with enough volume to produce gentle chest rise — before checking for a pulse and starting compressions. This ventilation-first order is the defining difference from the adult cardiac arrest and exists because the child's arrest is asphyxial. [5]
The pulse check follows the rescue breaths, not precedes them, and takes no longer than ten seconds. Feel the brachial pulse in an infant and the carotid in a child; if there is no pulse, or a heart rate under sixty beats per minute with poor perfusion after the rescue breaths, begin chest compressions at fifteen to two. Remove the wet clothing, dry the child, insulate with blankets, and protect from further heat loss, because ongoing cooling deepens hypothermia and provokes arrhythmia. Measure a low-reading core temperature — a standard thermometer stops at 34 degrees and will miss profound hypothermia, so a low-reading rectal, oesophageal, or bladder probe is essential. [5] [6]
The drowning resuscitation sequence — rescue breaths first
After return of spontaneous circulation, assess the lung injury and the neurological state together. Auscultate for crackles and wheeze, look for frothy secretions, apply oxygen and escalate to high-flow nasal cannula, continuous positive airway pressure, or intubation for the failing lung, and re-examine over hours for the delayed oedema. Assess the conscious level with the Glasgow or AVPU scale, recheck the glucose, and examine for signs of trauma, seizure, or the stigmata of non-accidental injury, each of which redirects the workup. [3] [10]
Investigations
Investigations serve two questions: how badly is the lung injured, and how cold and how deranged is the metabolism. The single most useful bedside monitor is the oxygen saturation, repeated over hours because a child who is normal at presentation can desaturate as the drowning lung evolves. A chest radiograph confirms pulmonary oedema, aspiration, or a pneumothorax in the ventilated child, and arterial or capillary blood gases quantify the hypoxaemia, the acidosis, and the carbon dioxide, guiding ventilation and the correction of acidosis. [3] [5]
The cold child needs a blood gas and electrolytes at the first access, because hypothermia and hypoxia drive a metabolic acidosis, because cold suppresses renal and hepatic function, and because hypoglycaemia is common and correctable. Blood glucose must be checked at the bedside in every submerged child and treated if low. A coagulation profile and a full blood count round out the search for complications, and a twelve-lead electrocardiogram, once the child is stable, looks for the long QT, the Brugada pattern, or another channelopathy that points to a primary arrhythmic cause and demands cardiology follow-up. [6] [7]
In the hypothermic arrest, the core temperature directs the resuscitation. Below thirty degrees, the standard rules for defibrillation and drugs change — this is examined heavily and is detailed in the management section. A potassium that is very high in a profoundly hypothermic patient is a marker of severe cell death and, with the HOPE score, helps separate the child who may survive from the one who will not, but a high potassium alone does not withhold resuscitation unless the child is clearly frozen solid or has a lethal injury. [7] [8]
Management — Resuscitation
The first act is the rescue-breath-first resuscitation, begun at the scene and continued without interruption. Open the airway with a jaw thrust if cervical injury is possible, give five rescue breaths, check the pulse for under ten seconds, and begin chest compressions at fifteen to two if there is no pulse or a heart rate under sixty with poor perfusion. Do not attempt to drain water from the lungs, do not use abdominal thrusts, and do not delay ventilations for any manoeuvre that does not deliver oxygen, because the cause of death in drowning is hypoxia and the treatment is ventilation. [5]
Rescue breaths and chest compressions (drowning)
Dose
Five rescue breaths first, each about one second with gentle chest rise; then if no pulse or heart rate under 60 with poor perfusion, compressions at 15 to 2 at 100 to 120 per minute and one third of chest depth
Oxygen is the specific therapy for the drowning lung, titrated from the lowest effective flow up the respiratory support ladder to high-flow nasal cannula, continuous positive airway pressure, non-invasive ventilation, or intubation and lung-protective mechanical ventilation for the child with pulmonary oedema, rising work of breathing, or failing gas exchange. End-tidal carbon dioxide confirms the airway and tracks both compression quality and recovery, and early application of non-invasive ventilation reduces the need for intubation in children with pulmonary oedema after drowning. [3]
The cold child is warmed and insulated from the first contact, because ongoing heat loss deepens hypothermia and provokes arrhythmia. Remove wet clothing, dry the skin, wrap in warm dry blankets including the head, and handle gently, avoiding any jarring movement that could precipitate ventricular fibrillation in the cold myocardium. Establish intravenous or intraosseous access, give warmed fluids for hypovolaemia, check the glucose and treat hypoglycaemia, and measure a low-reading core temperature to set the rewarming strategy. [6]
The first ten minutes for the submerged child
Open the airway (jaw thrust if a dive or fall); give FIVE rescue breaths
Check the pulse under 10 seconds; begin compressions at 15 to 2 if no pulse or HR under 60
Attach oxygen and the monitor; apply bag-mask ventilation and escalate as needed
Remove wet clothes, DRY, INSULATE, handle gently; measure a low-reading core temperature
Establish IV or IO access; give warmed crystalloid; check and treat the glucose
Stage hypothermia (Swiss I to IV) and start the matching rewarming strategy
Management — Definitive & Stepwise
The definitive management branches on the hypothermia stage, because the stage sets the rewarming ladder and, in arrest, the rules for shock and drugs. For mild hypothermia, Swiss stage one, passive rewarming suffices: the child is conscious and shivering, so remove wet clothes, insulate with blankets in a warm environment, and allow endogenous heat production to do the work, checking that the core rises steadily. For moderate, stage two, add active external rewarming with forced warm air at thirty-eight to forty-two degrees over the trunk, and warmed blankets; this is effective while the child still has a perfusing rhythm. [6]
Active external rewarming (forced warm air)
Dose
Forced warm air blanket at 38 to 42 degrees Celsius applied to the trunk
For severe, stage three, active internal rewarming is added: warmed humidified oxygen at forty-two to forty-six degrees, warmed intravenous crystalloid at around forty degrees, and consideration of body cavity lavage, while monitoring for rewarming shock and afterdrop. For profound, stage four — the cold, pulseless child — the treatment is extracorporeal rewarming, because extracorporeal membrane oxygenation or cardiopulmonary bypass rewarms fastest, supports the circulation, and carries the best survival in hypothermic cardiac arrest, with individual-patient meta-analysis showing meaningful survival where conventional resuscitation has failed. [6] [8]
Warmed intravenous crystalloid (hypothermia)
Dose
0.9 per cent saline warmed to approximately 40 degrees Celsius, 10 to 20 mL per kilogram boluses titrated to perfusion

The hypothermic cardiac arrest has its own rules, and these are high-yield for any exam. Continue high-quality cardiopulmonary resuscitation without interruption, because prolonged resuscitation can succeed and the maxim holds that nobody is dead until they are warm and dead. If the rhythm is ventricular fibrillation and the core is below thirty degrees, deliver a single shock at the standard energy and, if it fails, withhold further shocks and resuscitation drugs until the core rises above thirty degrees, because the cold myocardium is refractory to both. Once above thirty degrees, resume standard shocks and drugs, but lengthen the interval between adrenaline doses because drug clearance is slowed. Escalate to extracorporeal rewarming as early as the system allows, and continue resuscitation until the core reaches at least thirty-two degrees before terminating efforts. [5] [7]
After return of spontaneous circulation, hold a neuroprotective bundle: maintain normothermia and avoid fever, target normoxia (saturations 94 to 99 per cent) and normocapnia guided by capnography, check and control the glucose, and surveil for seizures. Admit to the paediatric intensive care unit, support the lung with lung-protective ventilation, and refer early to a retrieval and an extracorporeal service if the child is cold or if a tertiary centre is needed, because the window for extracorporeal rewarming is narrow and transport must be planned from the first contact. [9] [10]
Specific Subtypes & Scenarios
Cold-water submersion is the scenario that most rewards an understanding of physiology. The same child who would not survive ten minutes of warm-water drowning may recover intact after an hour under ice, because the diving response and rapid cerebral cooling protected the brain, which is why resuscitation is attempted and continued for prolonged cold-water submersion even when the outlook seems hopeless. Case series and reports of children surviving prolonged hypothermic submersion cardiac arrest with good neurological outcome after extracorporeal rewarming underpin the principle that the duration alone does not futility make, provided the water was cold. [9]
The bathtub drowning in an infant carries a different question. The mechanism is usually asphyxia in warm water with a short window, but the setting — an infant alone in a bath, or with an inconsistent history — raises non-accidental injury and the welfare of siblings, and demands a thorough safeguarding assessment alongside the resuscitation. A primary arrhythmia such as long QT, unmasked by the autonomic stress of immersion, can present as a bathtub drowning and is sought on the electrocardiogram once the child is stable. [5]
In Australia and New Zealand, follow the ANZCOR Guideline 9.3.2 on drowning and Guideline 9.3.3 on hypothermia: the rescue-breath-first sequence with five breaths, oxygen and respiratory support titrated to the lung injury, gentle handling and staged rewarming, and the principle that resuscitation is begun and continued at the scene and the child transported. The Royal Children's Hospital Melbourne clinical practice guidelines on drowning and hypothermia are the regional bedside reference, and retrieval to a centre with extracorporeal capability is arranged early for the cold, arrested child.
[5][6]Complications & Pitfalls
The commonest preventable failure in drowning is delaying ventilation. A team that wastes precious minutes trying to drain water, perform abdominal thrusts, or wait for equipment before giving rescue breaths has misread the mechanism — the child is dying of hypoxia, and the only treatment is oxygen delivered to the lung. Attempted drainage, head-down positioning, and the Heimlich manoeuvre are explicitly not recommended, cause vomiting and aspiration, and have no role in modern drowning resuscitation. [5]
In hypothermia, the dangerous errors cluster around handling and the defibrillation rules. Rough handling, jarring transport, or sudden movement can precipitate ventricular fibrillation in the cold myocardium, which is why the child is moved gently and never roughly. Repeated shocks and escalating drug doses below thirty degrees are ineffective and divert effort from rewarming — the correct move is one shock, then rewarm. Afterdrop — a further fall in core temperature after rewarming begins — and rewarming shock from vasodilation must be anticipated with warmed fluids and continued monitoring. [6] [7]
The final pitfall is discharging the well child too early. Because the drowning lung can evolve over four to six hours, any child with a significant submersion who has symptoms, abnormal examination, or any desaturation is observed, and only the asymptomatic child with normal saturations and a normal examination over a sustained period is discharged with a clear safety net and drowning-prevention advice. [3] [4]
Prognosis & Disposition
Outcome after submersion injury is driven by the scene factors, the water temperature, and the quality and duration of the resuscitation. The single strongest predictor is the submersion time: submersion under five minutes, a reactive pupil or a higher Glasgow Coma Scale score, a first documented rhythm with a pulse, and early bystander rescue breaths all favour a good outcome, while submersion beyond ten minutes in warm water, an asystolic arrest, fixed pupils, and a severe acidosis predict a poor outcome — with the cold-water exception that can overturn all of these. [10] [12]
Hypothermic cardiac arrest and extracorporeal life support (Saczkowski 2018)
Population: Patients in accidental hypothermic cardiac arrest requiring extracorporeal life support, individual-patient-data meta-analysis
Key finding
Survival to discharge was meaningful, and a higher potassium, a lower Glasgow Coma Scale score, and asystole predicted non-survival; the HOPE score stratified risk
Practice change
Extracorporeal rewarming is the treatment of profound hypothermic arrest and can be life-saving; the HOPE score helps identify who is likely to survive
The neurological outcome is shaped by what happens after return of spontaneous circulation. There is no role for routine therapeutic hypothermia in the comatose child after a non-hypothermic drowning cardiac arrest, because the paediatric THAPCA trials showed hypothermia was not superior to normothermia; the standard is to maintain normothermia and avoid fever, target normoxia and normocapnia, control the glucose, and surveil for seizures. For the child who arrived profoundly hypothermic, the rewarming itself is the treatment, and overcorrection into hyperthermia is avoided. [7] [9]
Disposition after return of spontaneous circulation is to a paediatric intensive care unit with lung-protective ventilation, haemodynamic support, seizure surveillance, and early liaison with cardiology if a channelopathy is found and with retrieval and extracorporeal services if the child is cold. The child who arrests out of hospital or in a smaller centre is retrieved by a paediatric retrieval team with the airway secured and the haemodynamics supported in transit. The family is told honestly and early, the prognostic uncertainty of the first days is named, and the possibility of neurological recovery — or of catastrophic brain injury and death — is held with them, alongside the discussion of organ donation should the outcome prove fatal. [10]
Special Populations
Children with epilepsy and with autism spectrum disorder drown at higher rates, and their families need anticipatory guidance — supervised showering and bathing, a shower rather than a bath where possible, and constant supervision around all water. A first or unexplained drowning in a child with epilepsy or a family history of sudden death prompts an electrocardiogram for a channelopathy, because long QT syndrome and other inherited arrhythmias present as drowning and demand cardiology follow-up and family screening. [11]
Aboriginal, Torres Strait Islander, Maori, Pacific, and remote-community children carry a disproportionate drowning burden tied to water access, lower supervised-swimming rates, and environmental hazards, and these children are reached by community-led water-safety and learn-to-swim programmes rather than by emergency care alone. The pregnant adolescent who drowns or becomes hypothermic adds the physiology of pregnancy and the need to manage both mother and fetus, and the child with a complex chronic condition or a tracheostomy drowns by a wider range of mechanisms and needs an individualised water-safety plan. [11]
In rural and remote settings the irreducible core is bystander rescue breaths, early contact with a retrieval service, gentle handling, and insulation and rewarming begun at the scene, because the tertiary centre and the extracorporeal service may be hours away. Telehealth-supported resuscitation and dispatcher coaching extend the reach of the algorithm, and a generalist who can run the rescue-breath-first sequence and stage hypothermia until retrieval arrives is the pivot of the whole system. [10]
Evidence, Guidelines & Regional Differences
The current global standard rests on the van Beeck definition, the Utstein reporting template, the Szpilman severity classification and its reappraisal, the European Resuscitation Council 2021 cardiac arrest in special circumstances guideline for drowning and hypothermia, and the Brown and Darocha reviews of accidental hypothermia. These agree on the fundamentals: the rescue-breath-first sequence, the staged rewarming ladder, the single-shock and withhold-drugs rule below thirty degrees, and the principle that a cold, pulseless child is resuscitated until warm. The American Heart Association special-circumstance guidance aligns, and in Australia and New Zealand the ANZCOR guidelines 9.3.2 and 9.3.3 are the regional authority. [1] [5] [6]
The first hours of a submerged child
Where the evidence is still maturing, answer with the current guideline and name the source. The role of extracorporeal rewarming is expanding as access grows, and the HOPE score and its variants are refining the selection of who will benefit. Routine therapeutic hypothermia after paediatric cardiac arrest, including after drowning, is not supported by the THAPCA trials; the defensible answer is normothermia and avoidance of fever, with rewarming reserved for the genuinely hypothermic child. [7] [8]
Exam Pearls
- Drowning is "respiratory impairment from submersion or immersion in liquid"; drop the terms near-drowning, secondary, dry and wet drowning. [1]
- Resuscitate drowning with five rescue breaths before the pulse check, because the mechanism is asphyxia — ventilation is the treatment. [5]
- Never attempt to drain water, hang the child head-down, or use abdominal thrusts; these delay ventilation and cause vomiting. [5]
- The Szpilman grades one to six stratify severity and mortality, from near zero in grades one to two to around three-quarters in grade six. [3]
- Submersion time is the strongest predictor of outcome; under five minutes favours survival, over ten minutes is usually grim, with the cold-water exception. [10]
- Stage hypothermia by Swiss stages: stage one 35 to 32 degrees (conscious, shivering), stage two 32 to 28, stage three 28 to 24, stage four below 24. [6]
- Rewarm passively for stage one, add forced warm air at 38 to 42 degrees for stage two, active internal warmed oxygen and fluids for stage three, and extracorporeal for stage four. [6]
- In hypothermic arrest, continue CPR, give one shock for VF below 30 degrees, then withhold shocks and adrenaline until above 30 degrees; continue until the core is at least 32 degrees. [5]
- Nobody is dead until warm and dead — resuscitate and transport cold, pulseless children, especially after cold-water submersion. [9]
- Extracorporeal rewarming is the treatment of profound hypothermic cardiac arrest and can be life-saving. [8]
- Observe any symptomatic child for four to six hours, because the drowning lung can evolve late into pulmonary oedema. [4]
- Prevention — four-sided isolation pool fencing, supervision, life jackets, swim lessons from around one year, and CPR training — is the public-health core. [11]
References
- [1]van Beeck EF A new definition of drowning: towards documentation and prevention of a global public health problem. Bull World Health Organ, 2005.PMID 16302042
- [2]Idris AH Recommended guidelines for uniform reporting of data from drowning: the "Utstein style". Circulation, 2003.PMID 14623794
- [3]Szpilman D Near-drowning and drowning classification: a proposal to stratify mortality based on the analysis of 1,831 cases. Chest, 1997.PMID 9315798
- [4]Markarian T Drowning Classification: A Reappraisal of Clinical Presentation and Prognosis for Severe Cases. Chest, 2020.PMID 32067943
- [5]Lott C European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation, 2021.PMID 33773826
- [6]Brown DJ Accidental hypothermia. N Engl J Med, 2012.PMID 23150960
- [7]Darocha T Accidental hypothermia. Nat Rev Dis Primers, 2026.PMID 42393082
- [8]Saczkowski RS Prediction and risk stratification of survival in accidental hypothermia requiring extracorporeal life support: An individual patient data meta-analysis. Resuscitation, 2018.PMID 29580960
- [9]Anadolli V Management of hypothermic submersion associated cardiac arrest in a 5-year-old child: A case report. Resusc Plus, 2021.PMID 34485955
- [10]Shenoi RP Prehospital and Resuscitation Factors Associated With Favorable Pediatric Drowning Outcomes. Pediatr Emerg Care, 2025.PMID 40129133
- [11]Denny SA Prevention of Drowning. Pediatrics, 2021.PMID 34253571
- [12]Koon W Studying outcome predictors of drowning at the scene: Why do we have so few answers? Am J Emerg Med, 2021.PMID 33069542