Paeds · adolescent-and-young-adult-medicine
Adolescent chronic pain and functional symptoms
Also known as Chronic primary pain in adolescence · Juvenile fibromyalgia · Complex regional pain syndrome in adolescence · Amplified musculoskeletal pain · Functional symptoms in adolescents · Central sensitisation syndrome · Paediatric chronic widespread pain
A fellowship approach to adolescent chronic pain and functional symptoms: a biopsychosocial, function-first model. Validate the symptom as real, screen for red flags once, avoid over-investigation and opioid escalation, and coordinate an interdisciplinary plan (physiotherapy, psychology, sleep, school reintegration) across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old has had daily widespread body pain, broken sleep and missed school for four months. She has seen three specialists and had two normal MRI scans. She arrives in your clinic with a folder of results and a family convinced something is being missed. The temptation is either to order one more test, or to tell her the pain is "just stress." Both are harmful. The clinician who understands chronic pain does neither: they recognise a real nervous-system problem, stop the cascade, and start a recovery plan. [10] [1]
Chronic pain in children and adolescents is conventionally defined as pain lasting longer than three months. It is common, not rare, and it is one of the most disabling conditions an adolescent can carry. The modern reframing matters: in ICD-11, chronic pain is split into chronic primary pain — where the pain is itself the disease — and chronic secondary pain, where pain accompanies another condition. For the adolescent in front of you, the primary-pain framing is liberating, because it says the pain is real and treatable without needing to find a damaged organ. [12] [1]
Functional symptoms sit on the same spectrum. These are genuine, distressing bodily experiences — weakness, sensory change, fatigue, non-epileptic events, abdominal or chest symptoms — that arise from altered nervous-system processing rather than from damaged tissue. The term "functional" has replaced older, stigmatising words like "somatisation" for good reason: it does not imply the symptom is invented, and it protects the therapeutic relationship. The examiner expects you to use "functional" and to mean it. [10] [3]
Two facts anchor everything that follows. First, chronic pain and functional symptoms cluster and overlap in the same adolescent, and they share a common biology and a common management approach — so a rigid single-diagnosis hunt is the wrong frame. Second, outcomes are far more modifiable than families fear, and the lever that matters most is restoration of function: getting the adolescent back to school, sleep, movement and friends. [1] [7]
Core arc of function-first care
Validate
Name the pain as real; never dismiss as 'just stress'.
Screen once
Red flags and suicidality, targeted tests to exclude organic disease — then stop the cascade.
Reframe
Explain central sensitisation / functional processing in validating language.
Co-build plan
Function goals (school, sleep, movement); physio + psychology + school liaison.
Restore & sustain
Graded return to function; relapse (flare) plan; transition to adult care.
Classification
Classify the presentation on two axes that change the plan: which symptom dominates and what mechanism is driving it. The shared core — genuine distress, nervous-system sensitisation, comorbid mood, school absence — runs underneath all of them, which is why management converges regardless of the label. [10] [12]
On the pain-predominant side, the commonest phenotypes are juvenile fibromyalgia (widespread pain with fatigue, sleep disturbance and tenderness), complex regional pain syndrome (a limb with severe pain, allodynia, colour and temperature change, often after a minor injury), chronic primary pain of widespread or regional distribution, and the recurrent primary pain syndromes such as chronic headache and chronic abdominal pain. Amplified musculoskeletal pain syndrome is a related umbrella term used in North American paediatric rheumatology. [9] [6]
On the functional-symptom side, adolescents present with functional neurological symptoms (non-epileptic events, functional weakness or sensory change), chronic fatigue syndrome (post-exertional fatigue and unrefreshing sleep), functional abdominal pain and irritable-bowel-type symptoms, and persistent dizziness or non-cardiac chest pain. These overlap heavily with chronic pain, and a single adolescent often shifts between sites over time. [10] [3]
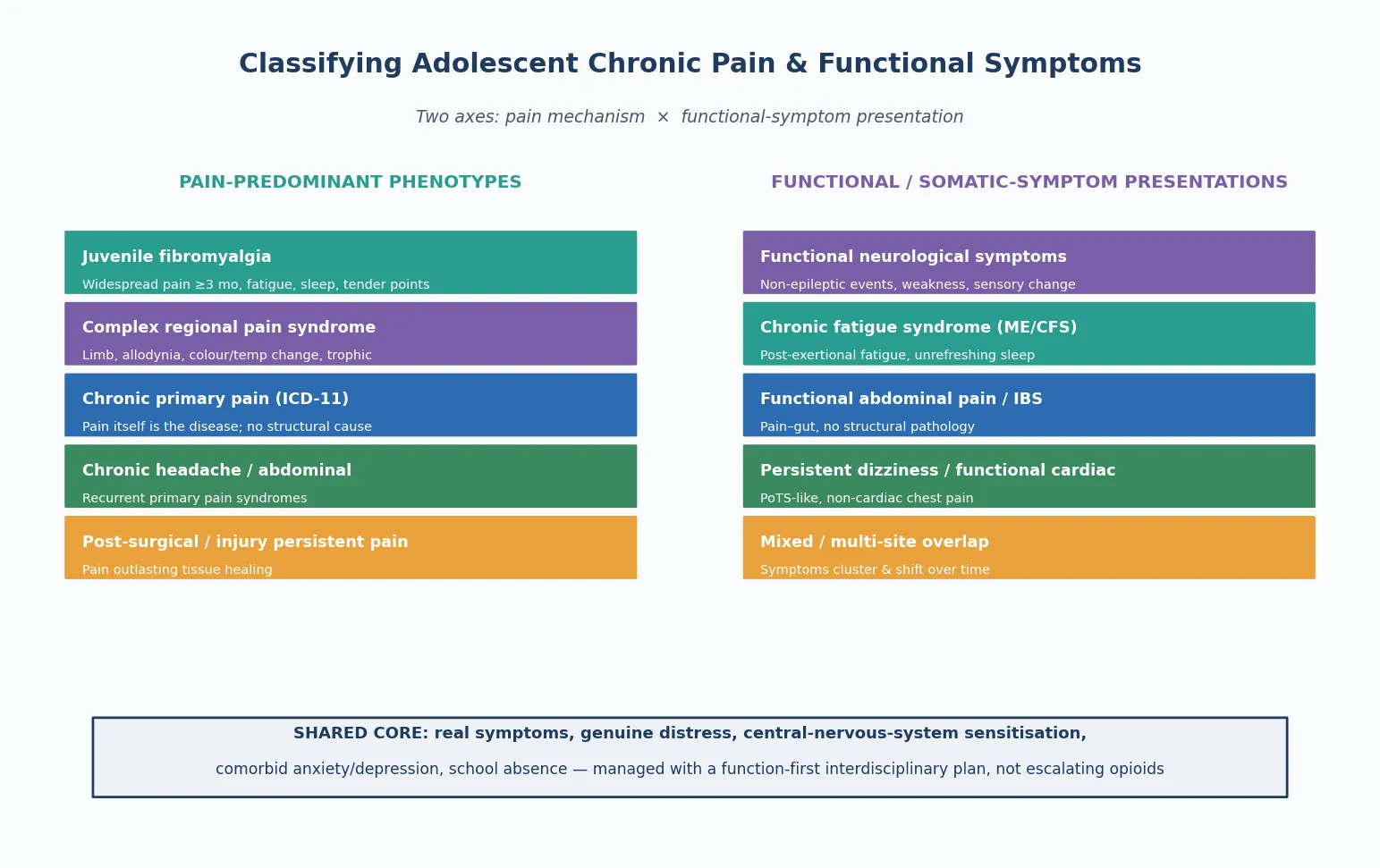
Read the figure like this: do not try to force the adolescent into one box. Many sit across both columns, and the management plan is built from the shared core below, not from the column heading. [10]
Juvenile fibromyalgia
Widespread pain phenotype
- Pain widespread, ≥3 months, with fatigue
- Sleep disturbance and cognitive 'fibro-fog'
- CBT has RCT evidence (Kashikar-Zuck 2012)
- Exercise and sleep are first-line
Complex regional pain syndrome
Limb-specific phenotype
- Limb pain, allodynia, colour/temp change
- Often follows minor injury
- Early mobilisation is key
- Intensive rehab if refractory
Functional neurological symptoms
Nervous-system phenotype
- Non-epileptic events, weakness, sensory
- Incongruent exam signs
- Neurology confirms; physio + psychology
- Validate reality, never dismiss
Severe school-absent subtype
High-disability phenotype
- School absence is the main disability
- Family conflict common
- Graded return-to-school is central
- Multidisciplinary intensity needed
Epidemiology & Risk Factors
Chronic pain in children and adolescents is common. King and colleagues' systematic review found substantial prevalence across pain sites, with headache, abdominal and musculoskeletal pain most frequent, and a meaningful proportion of affected young people reporting recurrent or persistent pain that interferes with daily life. This is a high-volume presentation in general paediatrics, not a rare referral problem. [1]
Risk is not evenly distributed. Older adolescence, female sex, pre-existing anxiety or depression, sleep disturbance, a family history of chronic pain, and exposure to early adversity or trauma all raise the likelihood of persistent pain and functional symptoms. Huguet and Miró's epidemiological study mapped the severity of chronic paediatric pain, showing that a sizeable minority experience high-intensity, disabling pain — the very adolescents who then accumulate school absence and disability. [2] [1]
The social cost is large and measurable. School impairment is one of the clearest markers of chronic pain in adolescence, and Logan and colleagues showed that adolescents with chronic pain have substantial school absences and academic disruption, which in turn worsen mood, isolation and pain itself. This is why school reintegration is treated as a clinical outcome, not an administrative afterthought, throughout this topic. [7] [8]
Pathophysiology
You do not need a neuroscience doctorate to counsel well, but you do need a usable model of why pain persists, because the model drives the whole plan. [3]
Central sensitisation is the keystone concept. It describes a state in which the nervous system becomes more responsive to normal input — ordinary touch, movement and temperature begin to generate pain, and pain from a small stimulus is amplified. Woolf framed central sensitisation as a shift in how the system processes signals, with direct implications for diagnosis and treatment: the problem is not ongoing tissue damage but altered processing, which is why more imaging and more opioids do not fix it, but graded activity, sleep and psychology can. [3]
The fear-avoidance loop is the psychological mirror of sensitisation. An adolescent in pain becomes frightened of movement (catastrophising — "moving will damage me"), avoids activity, becomes deconditioned, sleeps worse, and so experiences more pain — which confirms the fear and deepens the loop. The loop is self-sustaining, and it is also the loop the clinician breaks: graded exposure teaches the brain that movement is safe, and the cycle reverses. [10] [3]
Three modifiers run through both biology and psychology. Sleep disruption lowers pain thresholds and creates a pain-sleep cycle. Stress, arousal and early adversity sensitise pain and stress systems, partly through cortisol and arousal pathways. And deconditioning — the loss of fitness, strength and confidence that comes with avoidance — means a weaker body feels more pain, not less. Functional symptoms share the same substrate: they are disorders of nervous-system processing, not of damaged organs, which is why the explanation and the treatment overlap. [10] [3]
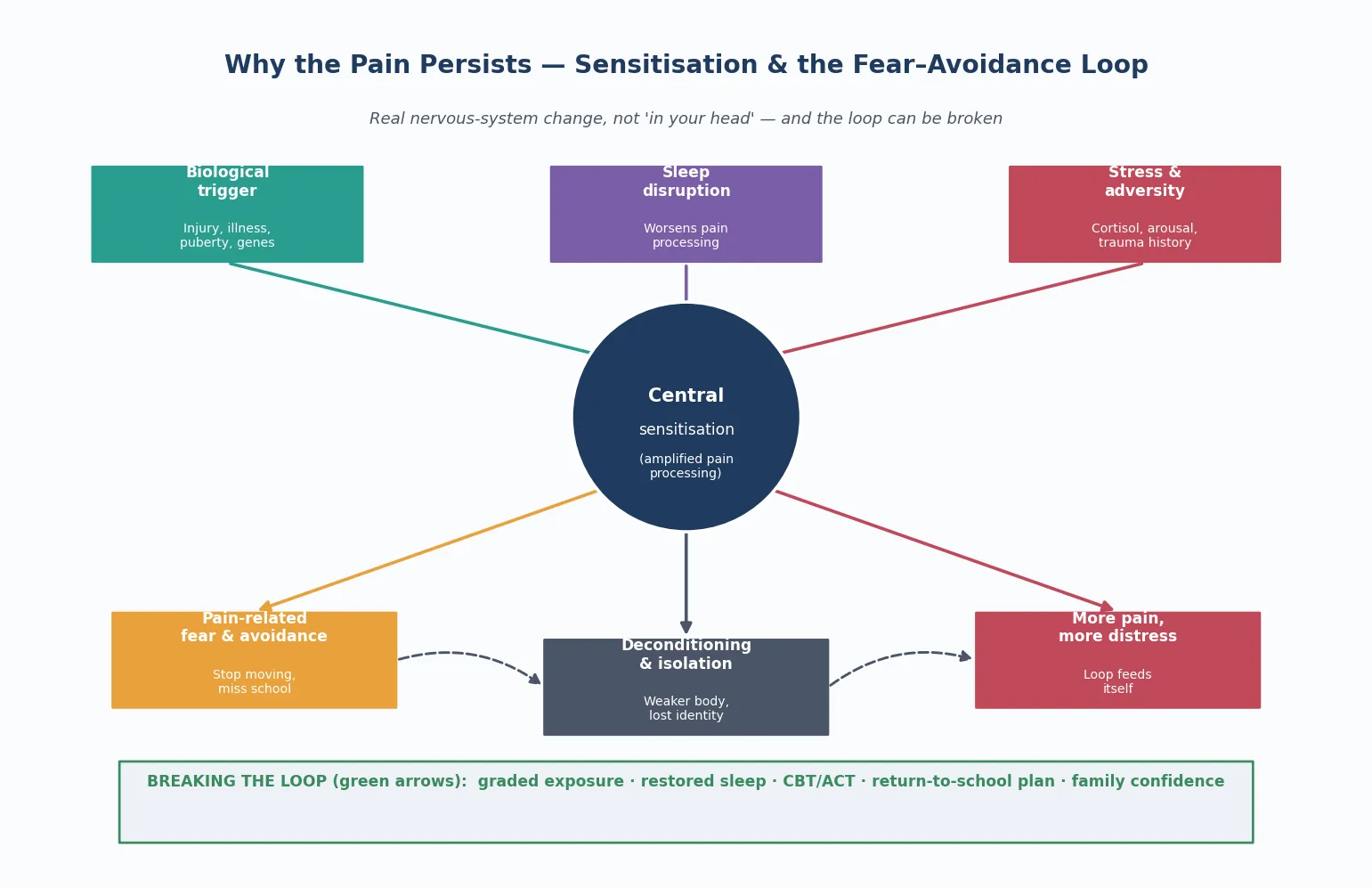
Read the figure like this: the arrows run both ways — sensitisation worsens fear and fear worsens sensitisation — which is exactly why a single-modality fix fails. The clinician's job is to interrupt the loop at several points at once. [10]
Clinical Presentation
An adolescent with chronic pain rarely arrives labelled and tidy. More often they present with widespread aching and fatigue (juvenile fibromyalgia), a severely painful, changed-colour limb that resists use (complex regional pain syndrome), or a parade of shifting symptoms — dizziness, abdominal pain, fatigue, non-epileptic events — that have defeated repeated normal investigations. A high index of suspicion for the functional and primary-pain frame is what surfaces the right plan. [9] [6]
The presentation is rarely just about the pain. The adolescent in distress shows school refusal or prolonged absence, withdrawal from friends, broken sleep, low mood, family conflict and a shrinking sense of identity — they describe themselves as "a sick person" rather than a teenager who happens to have pain. The pain and the disability are entangled, and you assess both. [7] [8]
Atypical and red-flag presentations are the trap. Weight loss, failure to grow, fever or night sweats suggest organic or malignant disease. A new or progressive neurological deficit points to spinal cord or central pathology. Pain that wakes the adolescent from sleep, or is consistently unchanged by position, demands reassessment rather than reassurance. And because chronic pain and self-harm cluster, any presentation through a mental-health crisis — self-harm, suicidal ideation, acute deterioration — must trigger a same-visit suicide assessment. [10] [9]
[7] [10]Differential Diagnosis
In this topic the differential is "what else could this be, and what must I rule out once — then stop." [10]
| Presentation | Consider alongside | Do not miss |
|---|---|---|
| Widespread pain, fatigue | Juvenile fibromyalgia, deconditioning, vitamin D deficiency | Inflammatory rheumatological disease (JIA, lupus), hypothyroidism |
| Painful changed limb | Complex regional pain syndrome | Infection (osteomyelitis, septic arthritis), fracture, tumour |
| Functional weakness / events | Functional neurological symptoms | Multiple sclerosis, spinal cord lesion, myasthenia |
| Persistent fatigue | Chronic fatigue syndrome, sleep disorder | Anaemia, thyroid disease, coeliac disease, sleep apnoea |
| Chronic headache | Migraine, tension-type, medication-overuse | Raised intracranial pressure, space-occupying lesion |
| Chronic abdominal pain | Functional abdominal pain, IBS | Inflammatory bowel disease, surgical cause |
Two traps recur. The first is over-investigating and medicalising — each extra normal MRI or autoimmune panel can reinforce a disease model, cause nocebo harm, and delay recovery. The second, opposite trap is dismissing genuine organic disease by attributing everything to "functional," which is how adolescents with evolving inflammatory or neurological illness get missed. The discipline is to screen for red flags once, with targeted tests, and then commit to the functional or primary-pain frame. [10] [3]
Clinical & Bedside Assessment
1. Open and validate
Greet the adolescent first, secure time alone, and state conditional confidentiality with its lawful limits. Then do the single most therapeutic thing you can do early: validate the pain as real. A sentence like "I believe your pain is real, and it is not your fault" sets the foundation for everything that follows. A non-judgemental, unhurried stance is what makes accurate assessment possible. [10]
2. Focused pain and symptom history
Take the pain history (site, onset, course, character, triggers, previous investigations and treatments, and functional impact), and map how the symptoms have shifted over time. Listen for the language of catastrophising ("moving will damage me") and for the cascade of normal results that has eroded trust. Establish what the adolescent and family currently believe is wrong, because the explanatory model drives adherence. [10] [9]
3. Biopsychosocial and HEEADSSS assessment
Run a HEEADSSS-tailored assessment emphasising mood, sleep, school attendance, peers, family function and adversity. Screen actively for anxiety and depression, and — because chronic pain and self-harm cluster — assess suicidality at every meaningful contact. Ask about sleep onset, night wakening and whether sleep is refreshing. Ask about family pain modelling, parental distress, and any reinforcement of the sick role, without blaming the family. [10] [1]
4. Focused examination
Examine generally, then the affected region. Look for allodynia (pain on light touch) and hyperalgesia in suspected sensitisation, and for the colour, temperature, trophic and mobility changes of complex regional pain syndrome. In functional neurological symptoms, look for incongruence — findings that do not map to a single anatomical pathway — which supports (but never alone proves) a functional origin. Complete a neurological screen. Examine respectfully and with consent. [9] [10]
5. Functional and goal assessment
Quantify functional disability directly: current school attendance, activity level, sleep, and participation. Frame goals around function, not pain scores — what does the adolescent want to get back to? Patient-reported outcome principles (function, mood, sleep, school) matter more than a pain number. [7] [8]
[9] [10]Investigations
Investigations in chronic pain and functional symptoms serve one purpose: to exclude organic disease once, then stop. A focused, rationale-led set is a clinical act of care; an open-ended cascade is a cause of harm. [10]
Targeted exclusion. A focused panel — full blood count, inflammatory markers (CRP, ESR), a basic biochemical and endocrine screen (including thyroid), and coeliac serology where indicated — excludes common organic mimics. Imaging is reserved for genuine red flags or focal neurological findings; routine extensive imaging of a chronic primary-pain presentation is low-value and reinforces a disease model. [9] [10]
Functional and symptom-specific assessment. Screening instruments for functional disability, mood and catastrophising are part of the investigation set, not optional extras. Sleep assessment is usually clinical; polysomnography is reserved for suspected sleep-disordered breathing or periodic limb movement. For functional neurological symptoms, the diagnosis is established clinically after neurology assessment excludes mimics — not by adding more scans. [10] [3]
Communicating normal results. This is a clinical skill the examiner rewards. Reframe a normal test as "the tests are reassuring because they show your body is healthy — not because nothing is wrong," rather than "the tests were normal, so there's nothing to find." The first sentence validates and opens a recovery plan; the second closes the relationship. [10]
Low-value patterns. Routine extensive autoimmune panels, repeated MRI of the same region without new red flags, and escalating analgesic trials without a function plan are all markers of a stalled, iatrogenic trajectory. [10]
Management — Resuscitation
Most adolescent chronic pain care is planned and rehabilitative, but a "routine" visit can tip into crisis in one disclosure. [10]
- Acute suicidality or self-harm: never leave the adolescent alone; perform a same-visit suicide and safety assessment (ideation, plan, intent, means, prior attempts, protective factors), remove means, and arrange urgent mental-health or crisis pathway care. Chronic pain and self-harm cluster, so this is a common emergency in this population. [10]
- Acute organic deterioration or a new red flag: re-enter the diagnostic pathway — targeted bloods and imaging for the specific concern (suspected infection, malignancy, spinal cord compression). A functional label is never a reason to stop thinking. [9]
- Severe dehydration or physiological compromise (e.g. an adolescent with profound fatigue or a flurry of non-epileptic events who has stopped eating and drinking): inpatient stabilisation, fluid and electrolyte correction, and a rapid multidisciplinary plan. [10]
- Acute pain flare: non-pharmacological measures first (environmental modulation, positioning, relaxation, calm presence), simple analgesia within local guidance, and avoidance of an opioid default. A flare plan agreed in advance with the family prevents the emergency-department opioid spiral. [10]
- Disclosure of abuse or family violence: follow local safeguarding pathways, share the minimum necessary, and support the adolescent through the process while sustaining the therapeutic relationship. [10]
Document decisions, the safety plan, and who was informed. Where confidentiality is overridden for safety, tell the adolescent what you must do and why. [10]
Management — Definitive & Stepwise
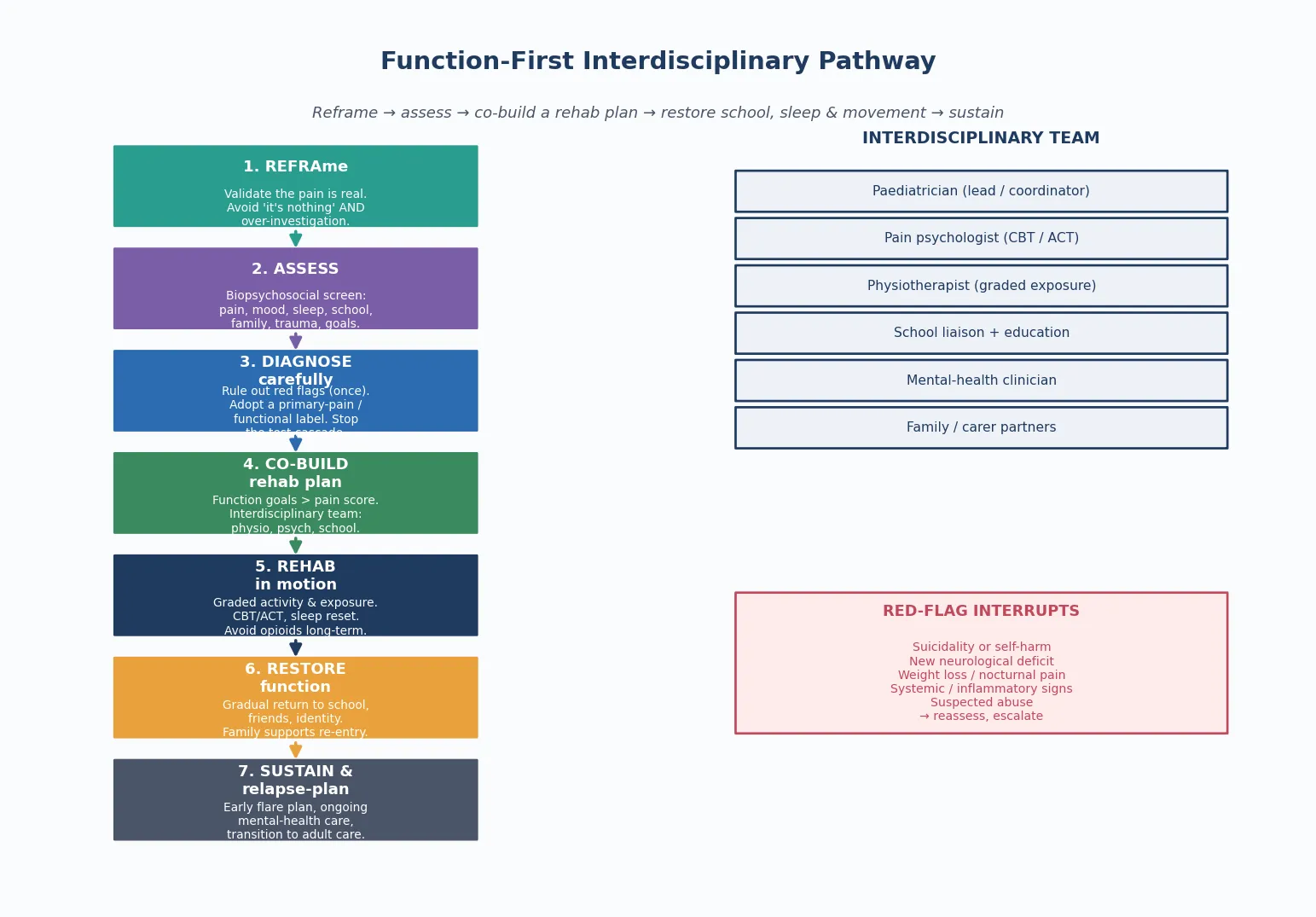
Read the figure like this: school reintegration and restored movement sit at the centre of the algorithm, not at the end. The interdisciplinary team is not optional ornamentation — it is the active ingredient. [7] [10]
Stepwise pathway
- Reframe the symptom. Validate the pain as real, then introduce central sensitisation or the functional-processing model in plain language. The explanation is itself a treatment. [3] [10]
- Assess biopsychosocially. Pain, mood, sleep, school, family, adversity and goals — measured by function. [10]
- Diagnose carefully. Screen for red flags once with targeted tests; commit to a primary-pain or functional label; stop the cascade. [9] [10]
- Co-build a function-first plan with the adolescent. Set shared functional goals (school, sleep, movement, friends) — explicitly not a pain-elimination goal. [7]
- Physiotherapy — movement is the medicine. Graded activity, graded exposure and desensitisation reverse deconditioning and retrain the nervous system. The goal is confident movement, not pain-free stillness. [10]
- Psychology — CBT and ACT. Psychological therapies reduce pain and disability in children and adolescents with chronic pain, with the strongest evidence for cognitive behavioural and acceptance-and-commitment approaches. Remotely delivered therapy extends reach. [4] [5]
- Sleep and mood. Treat sleep disruption directly (sleep hygiene, CBT for insomnia principles) and treat comorbid anxiety and depression actively — they are modifiable drivers of pain. [10]
- School reintegration. Build a graded, school-led return-to-school plan with education liaison; reducing the sick role is a core treatment. [7] [8]
- Medicines — judicious and adjunctive. Simple analgesia may help; some adjuvants have limited roles per local specialist guidance. Opioids generally have no place in chronic primary adolescent pain — the risk of dependence and adverse effects outweighs any long-term benefit. [10]
- Sustain and relapse-plan. Agree a written flare plan, maintain mental-health care, and plan transition to adult services. [10]
Intensive interdisciplinary rehabilitation
For adolescents with severe disability, prolonged school absence or refractory pain, intensive interdisciplinary pain rehabilitation — day-program or inpatient — is the evidence-based escalation. These programs deliver concentrated physiotherapy, psychology, school reintegration and medical coordination, and they work because they interrupt the fear-avoidance loop on every front at once. Simons and Basch set out the state of the art: biobehavioural, function-first, team-delivered care outperforms escalating solo biomedical management. [10]
Juvenile fibromyalgia specifics
Kashikar-Zuck and colleagues' multisite, single-blind RCT showed cognitive behavioural therapy improves function and reduces disability in juvenile fibromyalgia, complementing exercise and sleep interventions. The implication for the general paediatrician is direct: refer early to psychology and physiotherapy rather than escalating analgesia. [6]
Follow-up intensity
- Low disability, engaged adolescent and family: coordinated outpatient review with clear safety-netting. [10]
- Significant school absence, comorbid mood, or family conflict: early multidisciplinary review and a structured school plan. [7]
- Severe disability or crisis (suicidality, physiological compromise): same-day or inpatient escalation. [10]
Specific Subtypes & Scenarios
Juvenile fibromyalgia. Widespread pain with fatigue, sleep disturbance and tenderness. Management is exercise, CBT, sleep work and coordination; Kashikar-Zuck's RCT anchors the CBT evidence, and early interdisciplinary referral outperforms analgesic escalation. [6]
Complex regional pain syndrome. A limb with severe pain, allodynia, colour and temperature change, often after minor injury. Early mobilisation and graded exposure are central; intensive rehabilitation is effective for refractory cases. Sherry and colleagues describe the spectrum of amplified musculoskeletal pain of which CRPS is part. [9]
Functional neurological symptoms. Non-epileptic events, functional weakness or sensory change. Neurology confirms the diagnosis and excludes mimics; physiotherapy (often a specific functional-movement approach) and psychology are the treatment, built on validation that the symptoms are real. [10] [3]
Severe school-absent subtype. The adolescent whose main disability is school absence. A graded, school-led return-to-school plan, with education liaison and family work, is the central intervention; Logan and colleagues show school impairment tracks severity and recovery. [7] [8]
Chronic pain with comorbid anxiety or depression. Treat both — mood is a modifiable driver of pain, and untreated depression predicts poor outcomes and raises self-harm risk. Mental-health care is part of the pain plan, not a separate referral to defer. [10]
Neurodivergent adolescent (autism, ADHD). Adapt assessment and explanation to communication style and sensory profile; pain presentation and the fear-avoidance loop may look different, and pacing matters. [10]
Trauma, out-of-home care, or housing insecurity. Assume trauma exposure and fragmented records; adopt trauma-informed pacing, clarify consent, and rebuild trust before expecting adherence to a rehab plan. A "non-adherent" adolescent is often an adolescent whose plan was built without accounting for instability. [10]
The family seeking a biomedical diagnosis. Some families arrive convinced a hidden disease is being missed and reject a functional model. The skill is to validate their observation that the suffering is real, complete the targeted exclusion honestly, and then bring them into the sensitisation explanation gradually — never by arguing. [10] [9]
Overlapping chronic pain and chronic physical illness. An adolescent with inflammatory bowel disease or coeliac disease can have both genuine disease-related pain and a superimposed sensitisation component. The clinician separates the two and treats the functional layer without ignoring the disease. [10]
Complications & Pitfalls
- Over-investigation and medicalisation — each unnecessary test can reinforce a disease model and cause nocebo harm. [10]
- Dismissing symptoms as "just stress" or "all in your head" — destroys trust and misses comorbidity. [3]
- Prescribing opioids for chronic primary pain — risks dependence and adverse effects without long-term benefit. [10]
- Prolonged school absence going unaddressed — worsens pain, mood, isolation and prognosis. [7] [8]
- Missing comorbid depression or suicidality behind a pain explanation. [10]
- Family conflict, parental distress or inadvertent sick-role reinforcement perpetuating disability. [8]
- Fragmented care — multiple specialists giving contradictory messages, each adding another test. [10]
- Stigmatising language ("somatisation," "it's all in your head") — a direct harm to the therapeutic relationship. [10]
- Missing a genuine organic disease by attributing everything to "functional." [9]
Prognosis & Disposition
Prognosis here means the functional trajectory of the adolescent, and it is striking how modifiable it is — a fact families often do not believe at first contact. [10]
Better outcomes are predicted by restoration of function (school, sleep, movement, friends), treated anxiety and depression, engaged family and an interdisciplinary plan. Where these are present, adolescents recover meaningfully — not always to zero pain, but to a life no longer organised around pain. Where they are absent — ongoing school absence, untreated mood, family conflict, opioid use, repeated ineffective interventions — outcomes worsen and the pain is more likely to persist into adulthood. [7] [1]
The disposition plan spans assessment, rehabilitation and maintenance phases and names who owns each: the paediatrician as coordinator, physiotherapy for movement, psychology for fear and mood, mental health for comorbid illness, and school liaison for reintegration. Specialist interdisciplinary pain services and intensive rehabilitation are indicated for severe disability or refractory presentations. The transition to adult services is planned early, sustaining the recovery plan rather than restarting the diagnostic cascade. [10]
Special Populations
Neurodivergent adolescents (autism, ADHD, intellectual disability). Adapt assessment and explanation to communication and sensory profile; sensory differences alter pain experience, and pacing the rehabilitation plan matters. Avoid diagnostic overshadowing — neurodivergence does not explain away pain. [10]
Indigenous adolescents. Cultural safety, recognition of racism as a health exposure, and holistic framing matter as much as the guideline. Centre the young person's community and avoid deficit-only narratives; integrate cultural and family supports into the plan. [10]
Migrant and refugee adolescents. A professional interpreter is required for sensitive content; family members are not equivalent. Apply trauma-informed care, explore the family's explanatory model of the symptoms, and respect cultural framings of pain. [10]
Out-of-home care and youth justice. Assume trauma exposure, fragmented records and interrupted schooling. Clarify legal consent carefully and rebuild the history actively. [10]
Gender-diverse adolescents. Use correct name and pronouns, recognise minority stress as a contributor to arousal and pain, and tailor assessment without making the patient a curiosity. Chronic pain is over-represented in gender-diverse young people. [10]
Chronic physical illness or disability. Separate disease-related pain from superimposed sensitisation and treat both; a disability does not make functional pain untreatable. [10]
Housing or food insecurity. Ask before labelling a plan "non-adherent"; instability derails every rehabilitation plan you write. Gauntlett-Gilbert and colleagues noted altered body mass in adolescents with chronic pain, a reminder that nutrition and material circumstance shape recovery. [11]
Evidence, Guidelines & Regional Differences
Epidemiology. King and colleagues' systematic review remains the reference for the prevalence of chronic pain in children and adolescents, and Huguet and Miró's study maps its severity distribution — together they establish that chronic pain is common and that a meaningful minority suffer high-intensity, disabling pain. [1] [2]
Mechanism. Woolf's central sensitisation paper reframes chronic pain as altered nervous-system processing and lays the conceptual basis for diagnosis and treatment. It should be quoted for the mechanism, not for a memorised sensitivity threshold. [3]
Psychological therapies. Fisher and colleagues' Cochrane reviews — 2018 for in-person psychological therapies and 2014 for remotely delivered therapies — show that psychological treatments reduce pain and disability in children and adolescents with chronic pain. They are the evidence base for the psychology component of the interdisciplinary plan. [4] [5]
Juvenile fibromyalgia. Kashikar-Zuck and colleagues' multisite RCT supports cognitive behavioural therapy for juvenile fibromyalgia, anchoring the CBT-plus-exercise approach. [6]
School functioning. Logan and colleagues (2008; 2012) link chronic pain to school impairment and show the centrality of family and school factors — the evidence base for treating school reintegration as a clinical outcome. [7] [8]
Phenotype spectrum. Sherry and colleagues describe the spectrum of paediatric amplified musculoskeletal pain syndrome, situating CRPS within a broader amplified-pain frame. [9]
Biobehavioural state of the art. Simons and Basch set out the modern interdisciplinary, function-first approach that underpins this whole topic. [10]
Classification. Barke and colleagues report the WHO field testing of the ICD-11 chronic pain classification, which establishes the primary/secondary pain distinction that liberates the consultation from an endless disease hunt. [12]
ANZ: RCH Melbourne clinical guidance and state-based paediatric pain services deliver interdisciplinary and intensive rehabilitation; school-health integration varies by state. UK: NICE guidance on chronic primary and secondary pain in over-16s (with paediatric principles applied below that threshold) explicitly cautions against opioids and favours psychological therapies, exercise and sleep work. US: AAP guidance and the shift away from opioids for chronic non-cancer pain in young people; access to intensive interdisciplinary programs is uneven. Canada: Canadian Paediatric Society guidance and provincial paediatric chronic pain networks; rural-remote access is a recognised equity gap.
Exam Pearls
- Open every answer by validating the pain as real and screening once for red flags — never dismiss as "just stress." [10]
- Frame chronic primary pain as "pain as a disease," not a symptom (ICD-11; central sensitisation). [12] [3]
- The goal is function (school, sleep, movement, friends), not pain elimination. [7]
- Avoid over-investigation and opioid escalation — the harm of cascading tests and opioids is iatrogenic. [10]
- The interdisciplinary team — physio, psychology, school liaison, paediatrician — outperforms solo biomedical care. [10]
- School reintegration is central; prolonged absence worsens pain, mood and prognosis. [7] [8]
- Screen for and treat comorbid anxiety and depression; never let pain explanations overshadow suicidality. [10]
- CBT has RCT evidence in juvenile fibromyalgia (Kashikar-Zuck 2012) and broader chronic paediatric pain (Fisher 2018). [6] [4]
- Always assess suicidality when an adolescent with chronic pain is distressed — pain and self-harm cluster. [10]
- Never use stigmatising language; explain sensitisation in validating, understandable terms. [3] [10]
PAIN-FREE care anchors
References
- [1]King S; Chambers CT; Huguet A The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Pain, 2011.PMID 22078064
- [2]Huguet A; Miro J The severity of chronic pediatric pain: an epidemiological study. The journal of pain : official journal of the American Pain Society, 2008.PMID 18088558
- [3]Woolf CJ Central sensitization: implications for the diagnosis and treatment of pain. Pain, 2011.PMID 20961685
- [4]Fisher E; Law E; Dudeney J Psychological therapies for the management of chronic and recurrent pain in children and adolescents. Cochrane database of systematic reviews, 2018.PMID 30270423
- [5]Fisher E; Law E; Palermo TM Psychological therapies (remotely delivered) for the management of chronic and recurrent pain in children and adolescents. Cochrane database of systematic reviews, 2014.PMID 25221436
- [6]Kashikar-Zuck S; Ting TV; Arnold LM Cognitive behavioral therapy for the treatment of juvenile fibromyalgia: a multisite, single-blind, randomized, controlled clinical trial. Arthritis and rheumatism, 2012.PMID 22108765
- [7]Logan DE; Simons LE; Stein MJ School impairment in adolescents with chronic pain. The journal of pain : official journal of the American Pain Society, 2008.PMID 18255341
- [8]Logan DE; Simons LE; Carpino EA Too sick for school? Parent influences on school functioning among children with chronic pain. Pain, 2012.PMID 22169177
- [9]Sherry DD; Sonagra M; Gmuca S The spectrum of pediatric amplified musculoskeletal pain syndrome. Pediatric rheumatology online journal, 2020.PMID 33046102
- [10]Simons LE; Basch MC State of the art in biobehavioral approaches to the management of chronic pain in childhood. Pain management, 2016.PMID 26678858
- [11]Gauntlett-Gilbert J; Bhat C; Clinch J Body mass in adolescents with chronic pain: observational study. Archives of disease in childhood, 2020.PMID 31780522
- [12]Barke A; Korwisi B; Jakob R Classification of chronic pain for the International Classification of Diseases (ICD-11): results of the 2017 international World Health Organization field testing. Pain, 2022.PMID 33863861