Paeds · adolescent-and-young-adult-medicine
Adolescent health care for young people in out-of-home care
Also known as Health care for young people in foster care · Looked-after children and adolescents · Care-experienced youth · Children in out-of-home care · Foster care health · Kinship and residential care health
A fellowship approach to health care for adolescents living in out-of-home (foster, kinship, residential) care: classification of placement and legal status; the heavy cumulative mental-health, developmental, reproductive, dental, growth and immunisation burden and its toxic-stress mechanism; a trauma-informed initial and comprehensive health assessment on entry to care; consent-authority and conditional confidentiality when the state holds parental responsibility; management of pregnancy, sexual-health, mental-health and substance-use needs; transition to adult care and support for aging out — across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old moves into her third foster placement in a year and lands in your clinic for an "entry health check." She will not meet your eye, her immunisation record is missing, and she asks whether what she tells you will "go to the caseworker." This is the everyday work of caring for adolescents in out-of-home care, and the clinical skill it tests is delivering consistent, trauma-aware, confidential medicine to a young person whose life has been disrupted. [1] [6]
Out-of-home care is the arrangement made when a child or young person cannot safely live with their family of origin and is placed, usually under child-protection authority, in the care of relatives, an approved foster family, or a residential setting. It is temporary for some, long-term for others, and it ends — for many — when the young person "ages out" into adulthood. [1] [2]
What makes this population clinically distinct is not the placement itself but the accumulated adversity that brought them there and that often continues as placements move. Mental-health disorders, developmental and educational difficulty, early pregnancy, untreated dental disease, growth faltering and incomplete immunisation are all far more common than in community peers. Recognising that burden — and treating the person rather than the paperwork — is the core task. [3] [4] [2]
The clinician's role is to be the stable, trusted medical home that the chaos of placement moves cannot easily break. You assess on entry, you screen at every contact, you coordinate the team around the young person, and you plan the handover to adult care so that aging out does not mean dropping out of health. [1] [5]
Classification
Begin with the young person in front of you, then classify where they are living and what legal authority governs their care, because the second determines who can consent to your treatment. [1]
Kinship care
Relative or family friend
- Preserves family, culture and identity
- Often less disruption and better stability
- Carers may themselves need support and resources
- Still requires the full health-needs lens
Family-based foster
Approved non-relative household
- The most common placement type
- Approved and supervised carers
- Stability varies with carer support and matching
- Higher need with each placement change
Residential / group
Staffed unit
- Older youth and those with complex needs
- Higher rates of mental-health and behavioural difficulty
- Greater exposure to risk and placement turnover
- Needs intensive multidisciplinary input
Therapeutic / treatment
Specialised
- For high medical or behavioural acuity
- Embeds clinical and trauma-informed care
- Often a step-up or step-down from residential
- Plan for step-down to family-based care where possible
The legal or care status runs orthogonally to the placement and matters most at the bedside because it fixes who holds parental responsibility. A placement may be voluntary (the family agrees to temporary care and parents usually retain parental responsibility), statutory or court-ordered (a child-protection authority holds placement decisions), interim or emergency (short-term pending assessment or court), or long-term until majority (permanency not to the family, with aging out typically at 18 to 21). Before you treat, you must know which of these applies, because it tells you whether a parent, a guardian, the state, or — for a capable young person — the adolescent themselves can consent. [1] [6]
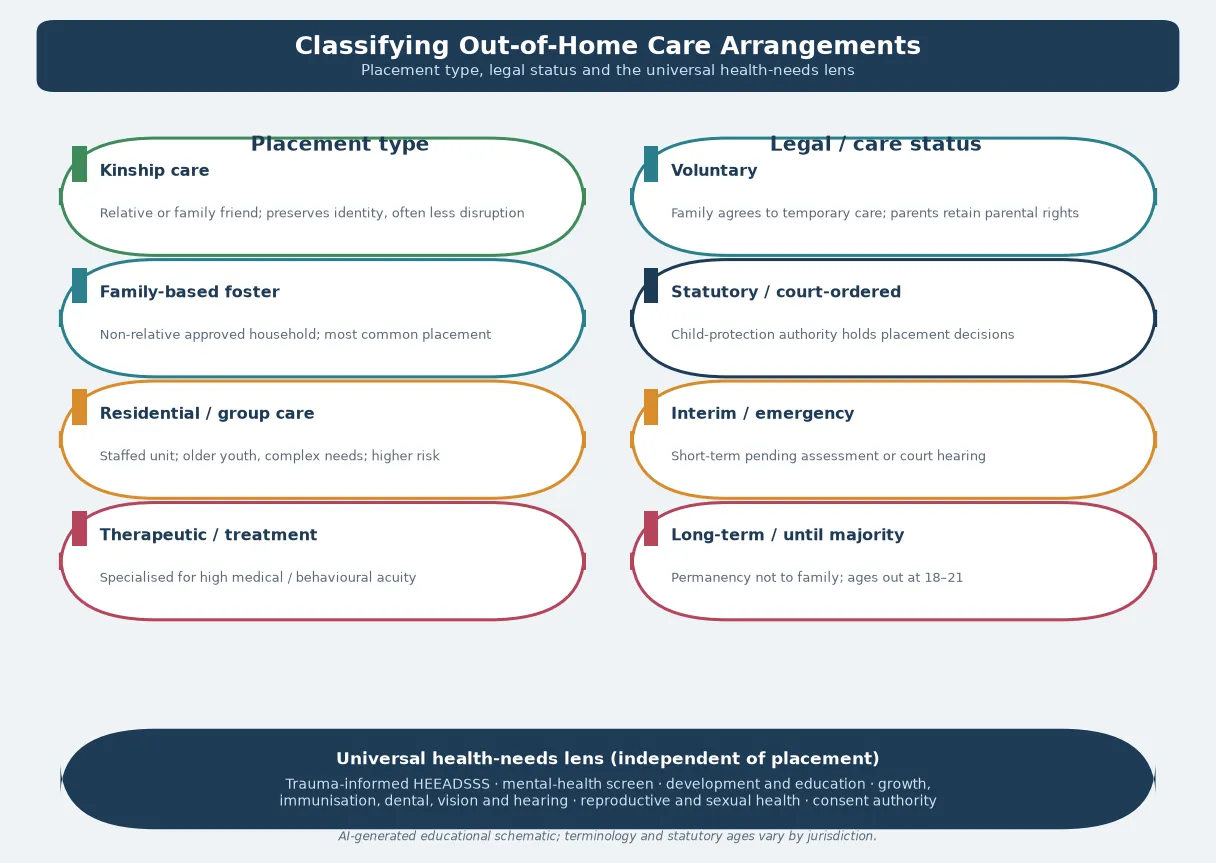
Whatever the placement, the health-needs lens is universal. Every care-experienced young person deserves a trauma-informed psychosocial assessment, a mental-health and developmental screen, attention to growth, immunisation, dental and sensory health, proactive reproductive and sexual-health care, and a clear statement of who can consent. The placement changes the intensity and the risks; it does not change the bundle. [1] [6]
Epidemiology & Risk Factors
The numbers are stark and they repeat across countries and systems. Children and adolescents entering out-of-home care are far sicker, in the psychosocial sense, than their community peers, and they stay sicker if the health system does not actively catch them. [2] [3]
Mental-health disorder is the dominant burden. A systematic review of children in foster care found rates of mental-health disorder several times higher than in community samples — anxiety, depression, post-traumatic stress, externalising behaviour and attachment difficulty all cluster here. [3]
Reproductive and sexual-health risk is conspicuously elevated in adolescent girls in the child-welfare system, with higher rates of early pregnancy and sexually transmitted infection than peers. Font and colleagues showed measurable differences in sexual and reproductive health outcomes for adolescent girls following child-protection intervention, and King and Van Wert mapped the predictors of early childbirth among female adolescents in foster care. [9] [8]
Physical and preventive health gaps are common on entry. Growth may be faltering, immunisation is frequently incomplete, dental need is high and often unmet, and undetected vision, hearing and developmental problems surface only when someone looks for them. [2] [13] [11]
Risk accumulates with placement instability, older age at entry, residential rather than family-based placement, and the cumulative load of adverse childhood experiences. Rebbe and colleagues showed that adverse childhood experiences predicted worse young-adult health outcomes among youth aging out of foster care — the dose matters, and each move adds to the dose. [4]
The endpoint for many is aging out: the transition to adulthood from a care setting, often around 18 to 21, when formal support falls away. Outcomes for care-leavers — in mental health, education, employment, housing and even early mortality — lag behind peers, which is why transition planning is a clinical and advocacy task, not an administrative one. [4] [10] [5]
Pathophysiology
The mechanism behind the burden is not mysterious. It is the accumulation of adversity, operating through a stress system that was built for acute threat, not for chronic, inescapable danger during development. [7] [4]
Adverse childhood experiences — maltreatment, neglect, household dysfunction, parental substance use or mental illness, and the loss and disruption of placement itself — pile up in this population. The relationship is dose-responsive: the more adversity, the worse the mental-health, developmental and later physical-health outcomes. [4] [7]
When adversity is severe and sustained it becomes toxic stress: the stress response stays activated, the systems that regulate arousal, emotion, immunity and metabolism are dysregulated, and the developing brain is shaped by chronic threat rather than by safety. This is the biological substrate of the clinical pattern you see — hypervigilance, emotional dysregulation, learning difficulty, and the long shadow of chronic disease and early mortality. [7] [15]
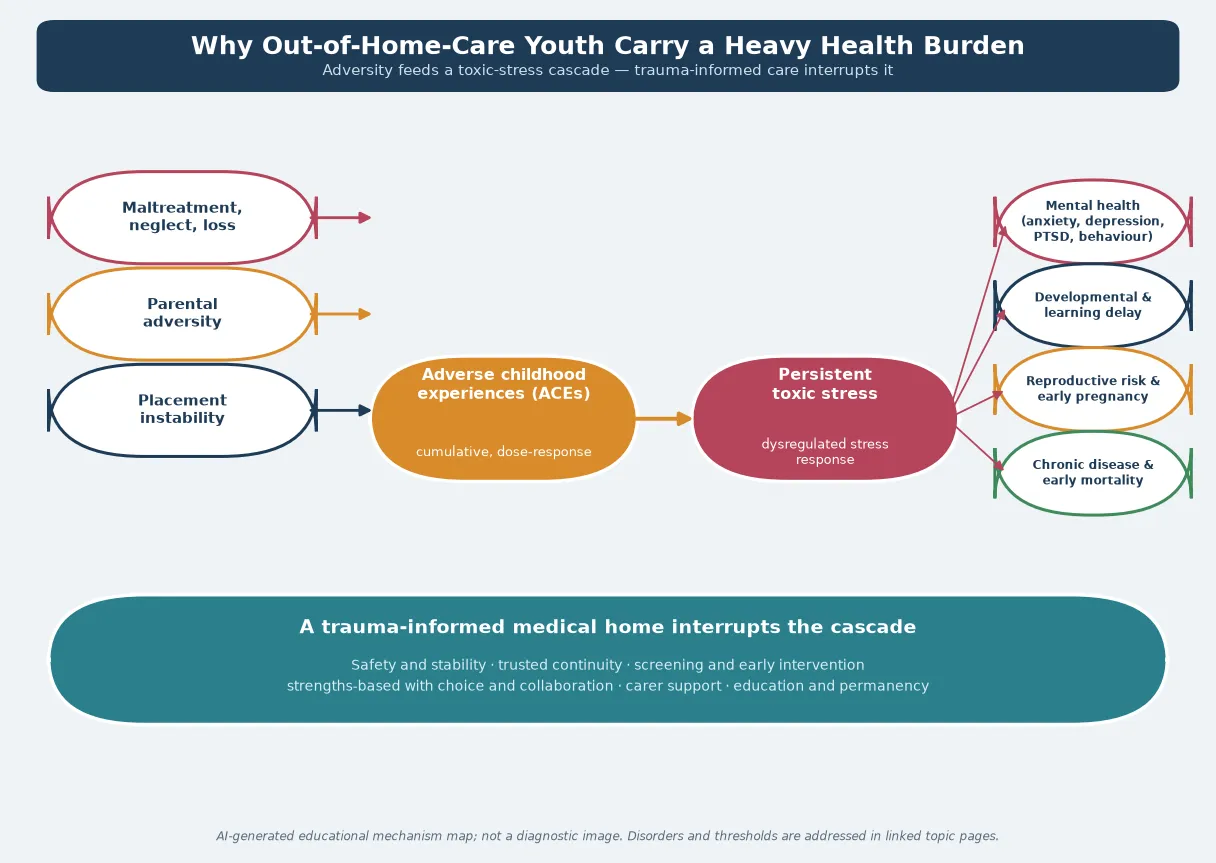
Two downstream consequences deserve attention. First, disrupted attachment and repeated loss change how a young person experiences the clinical encounter itself — authority, examination and information-giving can feel threatening, and distrust is an adaptation, not a character flaw. Second, placement instability independently worsens outcomes beyond the original maltreatment, because each move breaks therapeutic relationships, fragments records and interrupts treatment. [6] [15]
The clinical implication is hopeful: because the mechanism is reversible in part by safety, stability and trusted relationship, your trauma-informed continuity is itself a treatment. You are not only screening and referring; you are delivering the antidote to chaos. [6] [7]
Clinical Presentation
An adolescent in care rarely presents with "out-of-home care" written on the ticket. The presentation is the consequence — and your job is to recognise it and connect it back to the context. [2] [6]
The newly entered young person may arrive for a routine entry assessment carrying acute, unrecognised need: an injury that was never assessed, an infection never treated, a mood that has been low for months, or a disclosure held back because no one had earned the trust to hear it. [2] [12]
Mental-health disorder surfaces as behaviour as often as as symptom: school refusal, running away, aggression, withdrawal, self-harm, substance use, somatic complaints, or a flatness that reads as "difficult" rather than depressed. Trauma symptoms — hypervigilance, dissociation, sleep disturbance, flashbacks — may be invisible unless you ask. [3] [15]
Reproductive and sexual-health need may present as a contraception request, a suspected pregnancy, a sexually transmitted infection, or — more quietly — as coercive control or exploitation that the young person does not name as abuse. Because pregnancy rates are elevated in this group, a missed opportunity here has real downstream cost. [8] [9]
Placement instability presents clinically as missed appointments, repeat acute presentations, lost prescriptions, and treatment plans that never had time to work. Each acute visit from a young person with multiple placements should prompt you to ask what continuity has been lost. [6] [1]
The trauma history may surface indirectly. A young person who flinches at examination, who over-complies to avoid conflict, who cannot tolerate waiting, or who distrusts every promise is showing you the adversity, not a behaviour problem. Reading these signs correctly protects the relationship and the assessment. [15] [6]
Differential Diagnosis
In this topic the differential is less "which disease" and more "what is driving what I see, and what am I missing." [6] [7]
| What you see | The real question | Do not miss |
|---|---|---|
| Aggression, dysregulation | Trauma-driven dysregulation vs primary mental-health disorder | Untreated PTSD, mood disorder, or ongoing abuse |
| Distrust, withdrawal | Attachment and loss vs primary attachment or conduct disorder | Ongoing exploitation or family contact that is unsafe |
| Developmental delay | Early-adversity effect vs specific neurodevelopmental disorder | Fetal alcohol spectrum disorder, intellectual disability, hearing loss |
| Somatic complaint | Physical illness vs trauma or mental-health manifestation | Real physical disease missed by diagnostic overshadowing |
| Risk-taking | Normal adolescent exploration vs amplified risk from maltreatment | Coercion, exploitation, substance dependence |
| Non-adherence | Placement moves and lost prescriptions vs wilful refusal | A treatment plan that no placement could sustain |
Separate trauma-driven behaviour from primary mental-health disorder carefully. The two overlap and coexist, but labelling all dysregulation as a disorder risks over-medicalising a normal response to abnormal circumstances — while missing a genuine depression or PTSD is equally harmful. Screen, then formulate, then treat the formulation. [3] [7]
Avoid diagnostic overshadowing: the assumption that because a young person is in care and traumatised, every symptom is "behavioural." A headache is still a headache, abdominal pain still has a differential, and a limping adolescent still needs the joint examined. The context raises the prior; it does not abolish the differential. [6] [2]
Clinical & Bedside Assessment
1. Open with safety and trust
Greet the young person first, not the carer or caseworker. Explain who you are, what the visit is for, and that you will work at their pace. Trauma-informed care begins with the first sentence: safety, trustworthiness, choice, collaboration and strengths. [15] [6]
2. Clarify consent authority before you act
Establish and document who holds parental responsibility — parent, guardian, the state, or the young person as a mature minor — because this governs consent for every assessment and treatment you propose. If authority is unclear and the decision is not urgent, clarify it before acting. In a true emergency, treat first under best interests and reconcile consent afterwards. [1] [6]
3. State conditional confidentiality honestly
Say the frame aloud: what you discuss privately stays private unless you are worried the young person is not safe, someone else is being hurt, or the law requires you to act. Be explicit about what a caseworker or carer will and will not be told, because silence here breeds the breach that destroys trust later. [1] [15]
4. Adapt the HEEADSSS frame
Run a developmentally-tuned psychosocial assessment — Home, Education and employment, Eating, Activities, Drugs, Sexuality, Suicide and mood, Safety — adapted for the care context. Ask specifically about placement safety, contact with family, school stability, exploitation, and experiences of loss. Use trained interpreters, never carers or family members, for sensitive content. [1] [6]
5. Screen for mental-health and trauma
Use validated tools appropriate to age and setting for depression, anxiety, post-traumatic stress and suicidality, and screen for trauma symptoms. A positive screen triggers a formulation and a referral, not a label. Always assess immediate safety if any suicidal ideation is present. [3] [15]
6. Reconstruct the history and examine trauma-informed
Piece together developmental, educational, medical and placement history from whatever records, carers and the young person can provide — expect gaps. Examine sensitively, explaining what you are doing and why, offering choice about sequence and chaperone, and stopping to debrief if distress appears. [6] [2]
7. Screen reproductive and developmental need
Offer proactive reproductive and sexual-health screening where indicated, and arrange developmental or psychoeducational assessment when there is educational or developmental concern. Reassess at every contact, because need emerges over time as trust builds. [9] [8] [1]
8. Document to protect and inform
Record findings, consent authority, confidentiality reasoning and the plan in a way that informs the lawful care team and protects the young person's sensitive content. Documentation is part of the medicine here, not paperwork. [1] [6]
Investigations
There are no laboratory tests for "being in care," but there is a defined screening bundle that turns the burden into an actionable plan. The American Academy of Pediatrics sets the timing: an acute/entry screen within 72 hours and a comprehensive health assessment within 30 days. [1] [12]
The initial screening (on entry) looks for the acute problems that need immediate action: abuse or injury, infection, mental-health and safety risk, current medication, and acute illness. It is a triage, not a full assessment, and it decides who needs the urgent pathway now. [12] [6]
The comprehensive assessment (within 30 days) is the bundle that defines good care: growth and pubertal assessment, vision and hearing, dental review, developmental and educational screen, mental-health and trauma screen, reproductive and sexual-health assessment, immunisation reconstruction, and targeted laboratory testing. Szilagyi and Schulte address the specific laboratory issues for children and adolescents entering foster care. [1] [12]
Mental-health and trauma screening instruments appropriate to age and setting sit around the formulation — they do not replace clinical interview, but they make the burden measurable and the response auditable. Choose validated tools used in your service. [3] [14]
Immunisation reconstruction is a recurring task. Walton and Bedford's review of looked-after children found immunisation coverage often incomplete, so verify records actively and plan catch-up against the national schedule. Growth is interpreted against the history of deprivation and catch-up need, not as a single point. [11] [1]
Reproductive-health screening — chlamydia, gonorrhoea, HIV, syphilis and pregnancy where indicated — is offered proactively to sexually active adolescent girls in care, because the elevated pregnancy and infection rates make opportunistic screening cost-effective and protective. [9] [8]
Management — Resuscitation
A routine entry visit can become an emergency in one disclosure, and the skill is to recognise the pivot and act without abandoning the relationship. [6] [1]
- Stabilise physiology first if there is medical emergency: ABCDE, glucose, treat overdose or intoxication complications, manage injuries, treat sepsis or serious infection. [6]
- Secure immediate safety for a mental-health or safeguarding crisis: do not leave the young person alone, remove means if safe, and activate crisis, safeguarding or ED pathways the same day. [3] [1]
- Break confidentiality ethically when a threshold is crossed: tell the young person what you must share and why, share the minimum necessary with the people who need it, involve carer, caseworker and safeguarding services as required, and document decisions and the safety plan. [1] [15]
- Treat under best interests when consent cannot be obtained in the usual way, then return to consent and information-sharing as soon as the young person can engage. [1] [6]
In an emergency where consent authority is unclear, provide life-saving treatment under the emergency or best-interests doctrine and reconcile authority afterwards — but never use uncertainty as a reason to delay time-critical care. [1] [6]
Management — Definitive & Stepwise
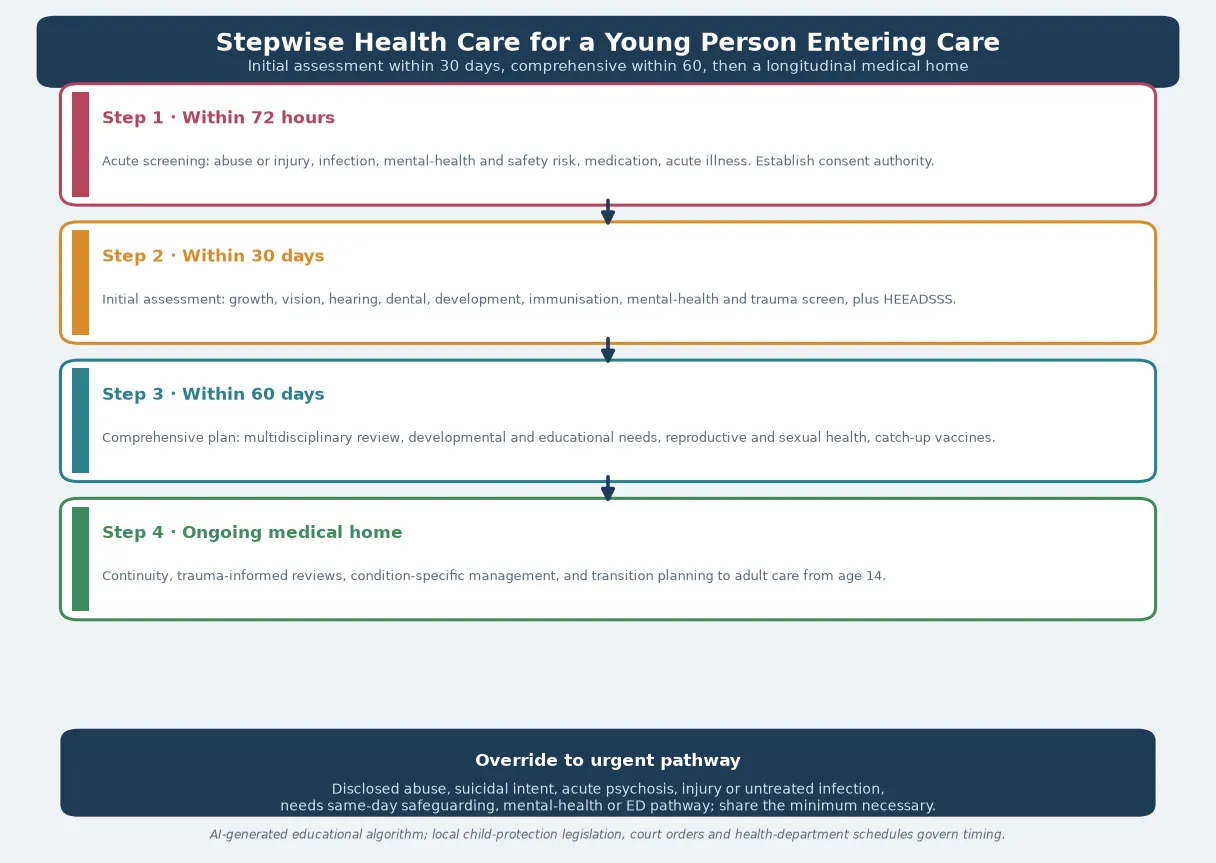
The entry-to-care pathway
- Within 72 hours — acute screening. Abuse or injury, infection, mental-health and safety risk, medication, acute illness. Establish consent authority. [12] [6]
- Within 30 days — initial health assessment. Growth, vision, hearing, dental, development, immunisation, mental-health and trauma screen, plus an adolescent HEEADSSS. [1]
- Within 30 days — comprehensive plan. Multidisciplinary review, developmental and educational needs, reproductive and sexual health, catch-up immunisation, and a written, shared care plan. [1] [12]
- Ongoing medical home. Continuity with predictable clinicians, trauma-informed reviews, condition-specific management, and transition planning to adult care from age 14. [6] [5]
The ongoing medical home
Trauma-informed continuity is the treatment. Offer predictable clinicians, strengths-based reviews, and a single coordinated plan that survives placement moves. Coordinate the multidisciplinary team — paediatrician, mental-health clinician, dental, education, social work and carer — around the young person, and make sure each knows the plan. [6] [1]
Reproductive, mental-health and substance-use care
For pregnancy and contraception, follow local adolescent sexual-health and contraception protocols, assess capacity and consent for the young person, screen for coercion and exploitation, and layer in safeguarding where indicated. For mental-health and substance-use need, use evidence-based psychological therapy first, reserve psychotropic medication for defined indications under specialist oversight, and avoid the over-medication of behaviour that the evidence warns against. Trubey and colleagues' meta-analysis supports the effectiveness of structured mental-health interventions for care-experienced young people. [9] [14] [3]
Catch-up and rehabilitation
Reconstruct and catch up immunisation, support growth and nutrition rehabilitation, and arrange dental care — the unmet dental burden in this population is well documented. Each is a concrete, achievable intervention that materially improves quality of life. [11] [13] [1]
Transition and care-leaving
Plan transition to adult care from age 14, building a written health summary and a continuity plan so that aging out does not mean losing health care. Taylor and colleagues' systematic review and meta-analysis identifies the policies and interventions that improve health, psychosocial and economic outcomes for young people leaving out-of-home care — extended support, preparation, and stable relationships consistently help. [10] [5]
Specific Subtypes & Scenarios
Kinship versus residential care. Kinship placements tend to preserve identity, culture and stability, while residential and group care carries higher rates of mental-health and behavioural difficulty and greater exposure to risk. Match your intensity to the placement, but apply the full health-needs lens in both. [1] [6]
The multiply-placed, distrustful adolescent. When a young person has moved many times, expect distrust to be the presenting feature. Invest deliberately in relationship-building, accept that disclosure will come slowly, and never penalise missed appointments — each represents a placement failure, not a patient failure. [6] [15]
Pregnant adolescent in care. Layer reproductive care onto safeguarding assessment: confirm capacity and consent, screen for coercion and exploitation, arrange antenatal care, and plan parenting support, because a pregnant adolescent in care is both a patient and, after birth, a prospective parent with their own support needs. [9] [8]
Adolescent with a neurodevelopmental disorder. Fetal alcohol spectrum disorder, intellectual disability and autism are over-represented and under-recognised in care. Arrange formal developmental or psychoeducational assessment when there is educational concern, and adapt communication and capacity assessment to ability. [6] [2]
Indigenous and minority adolescents. Cultural safety is non-negotiable. Indigenous children are over-represented in care across ANZ and Canada; respect family and community decision-making, use local culturally safe services, and recognise racism as a health exposure. [1] [6]
Unaccompanied and refugee minors. Use trained interpreters, never carers, take a trauma-informed catch-up history, and address missed preventive care, immunisation and the psychological legacy of displacement. [1]
The aging-out young person. Begin transition planning early, build a health summary, connect the young person to adult primary and mental-health services, and advocate for housing, education and continuity — because the drop-off at aging out is where harm concentrates. [10] [5] [4]
Youth justice overlap. Young people in care are over-represented in youth justice. Clarify consent and information-sharing between the care and justice systems, and maintain the same trauma-informed, confidential, continuity-based approach. [6] [1]
Complications & Pitfalls
- Failing to clarify consent authority before treating, then discovering the state — not the carer — holds parental responsibility. [1] [6]
- Allowing fragmented records and care discontinuity to repeat investigations and lose diagnoses; rebuild the record actively. [2] [11]
- Letting placement instability silently dismantle a treatment plan; build portability and redundancy into every plan. [6]
- Over-diagnosing trauma-driven behaviour as a primary disorder, or over-medicating it — the evidence cautions against reflexive psychotropic use. [3] [14]
- Diagnostic overshadowing that misses real physical illness behind the "behavioural" label. [6]
- Handling a safeguarding disclosure clumsily, retraumatising the young person or breaching trust through an avoidable leak. [15] [1]
- Using carers or family members as interpreters or sole historians for sensitive content; always use trained interpreters. [1]
- Failing to plan transition, so aging out becomes dropping out of care. [10] [5]
Prognosis & Disposition
Prognosis here means the trajectory of safety, mental-health recovery, educational engagement and stable relationship, not a disease stage — and it is more modifiable than it looks. [6] [1]
Routine disposition: a stable placement, a completed assessment bundle, a shared care plan, and a safe young person with routine follow-up in the medical home. [1]
Early-review disposition: a new disclosure, a placement move, an incomplete assessment, or a young person still building trust — bring them back in days to weeks, not months. [6]
Urgent disposition: active suicide risk, disclosed abuse or exploitation, acute psychosis, medical instability, or a serious unmet physical need — use ED, crisis or safeguarding pathways the same day. [3] [1]
Safety-net explicitly: who to call tonight, when to come back sooner, and how confidentiality will work with carer and caseworker after any override. Close the loop after mental-health, safeguarding, education or placement involvement. [1] [6]
Over time, early, trauma-informed, continuous medical-home care improves trajectory compared with fragmented acute-only contact — and the long-term outcomes for care-leavers in mental health, education, employment and housing are the measure of whether the system, not just the visit, worked. [4] [10]
Special Populations
Indigenous adolescents (Aboriginal, Torres Strait Islander, Māori, First Nations). Over-represented in care; cultural safety, respect for family and community decision-making, and locally appropriate services are essential. Racism is a health exposure. [1] [6]
Migrant, refugee and asylum-seeking youth. Use trained interpreters, take a trauma-informed catch-up history, and address missed preventive care and the psychological legacy of displacement. [1]
Adolescents with disability or neurodiversity. Adapt communication and capacity assessment to ability, use supported decision-making, and avoid the diagnostic overshadowing that wrongly assumes incapacity or attributes symptoms to disability. [6] [2]
Gender- and sexually-diverse youth. Over-represented and vulnerable in care; confidentiality, chosen name and pronouns, and tailored, affirmative care are central, with attention to family rejection, bullying and minority stress. [1]
Pregnant and parenting adolescents. Layered capacity and safeguarding apply — they may be deciding for themselves and, after birth, for their own child. [9] [8]
Youth-justice-involved young people. Clarify consent and information-sharing between systems, and maintain the same trauma-informed, continuity-based approach. [6]
Rural and remote adolescents. Fragmented service access and small-community dual relationships threaten confidentiality and continuity; create deliberate pathways including telehealth with private space. [1]
Evidence, Guidelines & Regional Differences
The AAP standard. The American Academy of Pediatrics Council on Foster Care, Adoption, and Kinship Care clinical report — Szilagyi and colleagues, 2015 — sets the current practice standard: a medical home, screening on entry, entry screening within 72 hours, comprehensive assessment within 30 days, and coordinated, trauma-informed ongoing care. This is the framework an examiner expects you to know. [1] [2]
The mental-health burden. Engler's 2022 systematic review quantifies the several-fold elevation in mental-health disorder among children in foster care. Trubey's 2024 meta-analysis shows that structured mental-health and wellbeing interventions can be effective — so evidence-based therapy is the first line, with psychotropic medication reserved for defined indications. [3] [14]
Reproductive health. Font's 2022 JAMA Pediatrics study and King and Van Wert's 2017 work establish the elevated reproductive and pregnancy risk for adolescent girls in the child-welfare system, justifying proactive screening and contraception access. [9] [8]
Aging out and care-leaving. Rebbe's work links adverse childhood experiences to young-adult health outcomes among youth aging out, and Taylor's 2024 systematic review and meta-analysis identifies the policies and interventions — extended support, preparation, stable relationships — that improve outcomes for young people leaving out-of-home care. [4] [10] [5]
Preventive gaps. Walton and Bedford document incomplete immunisation coverage in looked-after children, and Sarvas documents high unmet dental need — concrete, fixable targets. [11] [13]
Trubey et al, 2024 — mental-health interventions for care-experienced young people
Systematic review and meta-analysis
Population: Children and young people in foster, kinship and residential care
Key finding
Structured mental-health and wellbeing interventions show measurable effectiveness in this population, supporting evidence-based psychological therapy as first-line treatment.
Practice change
Reserve psychotropic medication for defined indications under specialist oversight; offer evidence-based psychological intervention as the foundation of the mental-health plan.
ANZ: each state and territory governs child-protection legislation, care-leaving ages and mandatory-reporting duties; Aboriginal community-controlled services and cultural-safety requirements apply. RCH Melbourne provides clinical guidance for children in care. UK: NICE guidance on looked-after children and young people (NG205) frames assessment and ongoing care; local-authority corporate parenting and the role of the designated doctor apply. US: the AAP foster-care clinical report sets the standard; Medicaid and the Chafee Foster Care Independence Act frame coverage and transition support, and care-leaving typically occurs around 18 to 21 with state variation. Canada: provincial child-welfare legislation governs; Indigenous child and family services and Jordan's Principle apply for First Nations, Inuit and Métis children.
State the principle and check local law. Do not invent a universal care-leaving age or a universal consent rule — they do not exist, and the child-protection authority and local statute govern the operative detail. [1] [6]
Exam Pearls
- Open every answer with trauma-informed principles — safety, trust, choice, collaboration, strengths — then the timing standard: initial within 72 hours (entry screen), comprehensive within 30. [1] [6]
- Always clarify and document consent authority (parental responsibility) before treating an adolescent in care. [1]
- Name the high-prevalence needs: mental health, development and education, reproductive and sexual health, dental, growth, immunisation. [3] [9] [13]
- Hold conditional confidentiality honestly — be explicit about what carer and caseworker will and will not be told. [1] [15]
- Early pregnancy and STI rates are markedly higher — screen proactively and offer contraception access. [9] [8]
- Mental-health disorder prevalence is several-fold higher than community peers — screen at every contact. [3]
- Plan transition to adult care from age 14 and a written health summary before the young person leaves care. [10] [5]
- Avoid over-medication of behaviour; evidence-based psychological therapy is first line. [14]
CARES for a care-experienced adolescent encounter
References
- [1]Szilagyi MA, Rosen DS, Rubin D, Zlotnik S, Council on Foster Care, Adoption, and Kinship Care, Committee on Adolescence, Council on Early Childhood Health Care Issues for Children and Adolescents in Foster Care and Kinship Care. Pediatrics, 2015.PMID 26416934
- [2]Simms MD, Dubowitz H, Szilagyi MA Health care needs of children in the foster care system. Pediatrics, 2000.PMID 11044143
- [3]Engler AD, Sarpong KO, Van Horne BS, Greeley CS, Keefe RJ A Systematic Review of Mental Health Disorders of Children in Foster Care. Trauma, Violence & Abuse, 2022.PMID 32686611
- [4]Rebbe R, Nurius PS, Courtney ME, Ahrens KR Adverse Childhood Experiences and Young Adult Health Outcomes Among Youth Aging Out of Foster Care. Academic Pediatrics, 2018.PMID 29709622
- [5]Lopez P, Allen PJ Addressing the health needs of adolescents transitioning out of foster care. Pediatric Nursing, 2007.PMID 17907736
- [6]Schilling S, Fortin K, Forkey H Medical Management and Trauma-Informed Care for Children in Foster Care. Current Problems in Pediatric and Adolescent Health Care, 2015.PMID 26381646
- [7]Forkey H, Szilagyi M Foster care and healing from complex childhood trauma. Pediatric Clinics of North America, 2014.PMID 25242716
- [8]King B, Van Wert M Predictors of Early Childbirth Among Female Adolescents in Foster Care. Journal of Adolescent Health, 2017.PMID 28438523
- [9]Font SA, Caniglia M, Kennedy R, Noll JG Child Protection Intervention and the Sexual and Reproductive Health of Female Adolescents Ages 13 to 17 Years. JAMA Pediatrics, 2022.PMID 35188543
- [10]Taylor D, Albers B, Mann G, Lewis J, Taylor R, Mendes P, Macdonald G, Shlonsky A Systematic Review and Meta-Analysis of Policies and Interventions that Improve Health, Psychosocial, and Economic Outcomes for Young People Leaving the Out-of-Home Care System. Trauma, Violence & Abuse, 2024.PMID 38828776
- [11]Walton S, Bedford H Immunization of looked-after children and young people: a review of the literature. Child: Care, Health and Development, 2017.PMID 28317146
- [12]Szilagyi M, Schulte E Issues Related to Laboratory Screening for Children and Adolescents Entering Foster Care. Pediatrics, 2017.PMID 29141917
- [13]Sarvas EW, Eckerle JK, Gustafson KL, Freese RL, Shlafer RJ Oral health needs among youth with a history of foster care: A population-based study. Journal of the American Dental Association, 2021.PMID 34090662
- [14]Trubey R, Evans R, McDonald S, Noyes J, Robling M, Willis S, Boffey M, Wooders C, Vinnicombe S, Melendez-Torres GJ Effectiveness of Mental Health and Wellbeing Interventions for Children and Young People in Foster, Kinship, and Residential Care: Systematic Review and Meta-Analysis. Trauma, Violence & Abuse, 2024.PMID 38362816
- [15]Fratto CM Trauma-Informed Care for Youth in Foster Care. Archives of Psychiatric Nursing, 2016.PMID 27256954