Paeds · adolescent-and-young-adult-medicine
Adolescent health in rural and remote settings
Also known as Rural and remote adolescent health · Frontier youth health · Adolescent health equity in remote communities · Rural youth access to care · Telehealth for rural adolescents · School-based health for rural young people
A fellowship approach to the equity gap in adolescent health in rural and remote settings: why the gap exists, how it presents clinically, and the tiered service model — youth-friendly primary care, telehealth, outreach, school-based health and retrieval — that closes it across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old in a town of 800 people tells the school nurse she has been "feeling nothing" for months and has thought about not being here. The nearest child psychiatrist is six hours away. The family knows the GP socially. There is no bus to the regional centre, and the mobile signal drops out at the edge of town. This is the real patient behind the phrase "rural and remote adolescent health" — a young person whose needs are identical to a city adolescent's but whose path to care is longer, less private, and far more likely to end in nothing being done. [1] [4]
Rural and remote adolescent health is the study and practice of delivering developmentally appropriate adolescent care across a geography where distance, workforce scarcity, social visibility and digital exclusion conspire to widen the gap between need and service. It is not a separate speciality of adolescence; it is adolescence viewed through the lens of access equity. The same HEEADSSS domains, the same validated screens, the same confidentiality principles apply — but they must be re-engineered for a setting where the nearest specialist may be hundreds of kilometres away and the only clinician may be the patient's neighbour. [1] [6]
The clinical heart of the topic is recognising that distance is a determinant of health, not merely an inconvenience. Rural and remote young people present later, sicker, and more often in crisis; the conditions most sensitive to access — mental health, sexual and reproductive health, substance use — are precisely those an adolescent will not raise unless confidentiality is ironclad, and confidentiality is hardest to guarantee where everyone is connected. Closing the gap therefore means redesigning the delivery model, not just educating individual clinicians. [4] [5]
Classification
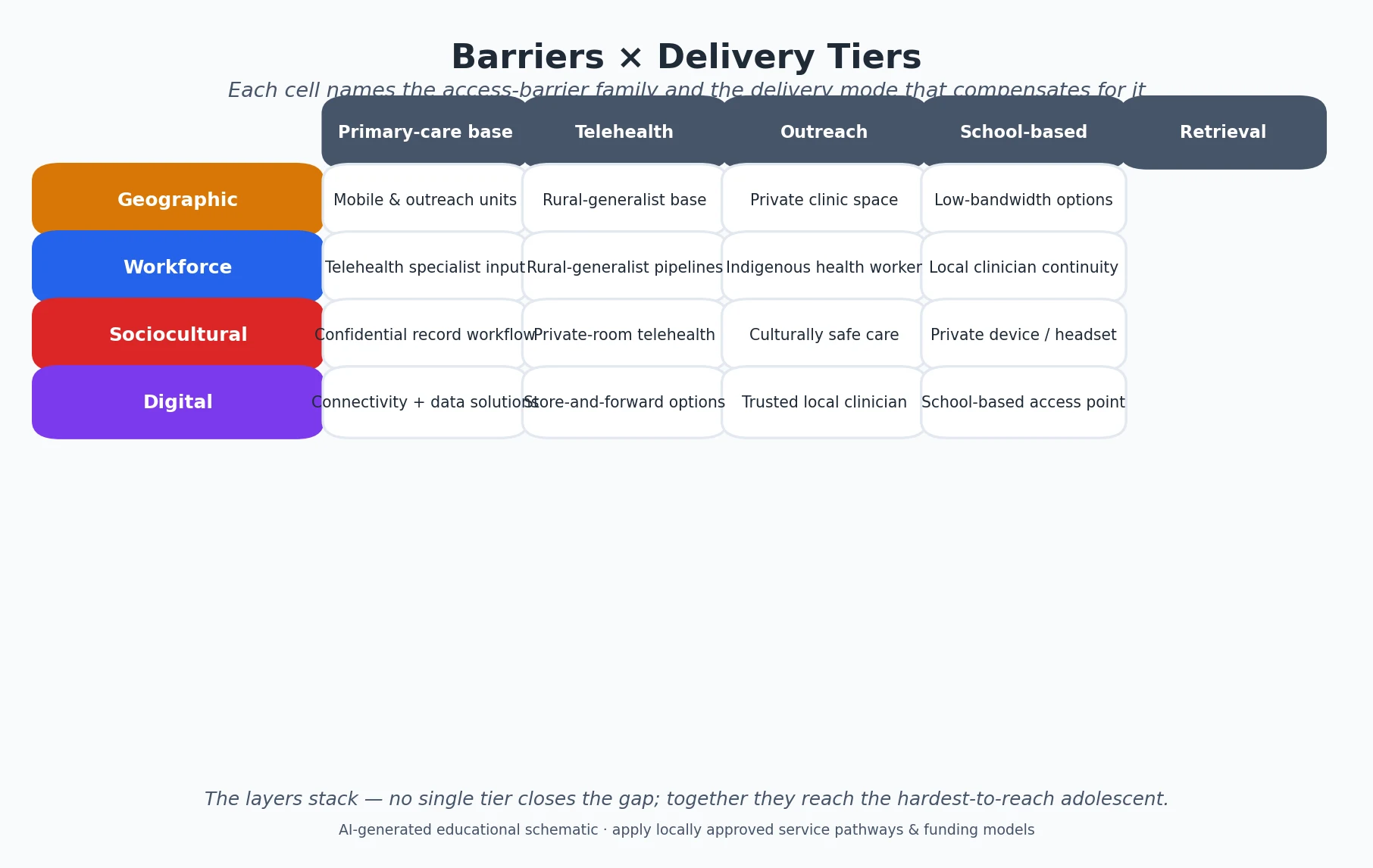
Classify the problem along three axes that each point to a different lever: how remote, what blocks access, and how the service is delivered. Naming the remoteness tier tells you how far care must travel; naming the barrier tells you what to dismantle; naming the delivery mode tells you which tool to deploy. [4] [15]
Remoteness tiers
Countries classify remoteness differently but with the same intent — to tie funding, workforce incentives and retrieval planning to how far a community sits from a service centre. Australia's Modified Monash Model (MMM) grades postcodes from MM1 (metropolitan) to MM7 (very remote); the US uses Rural-Urban Commuting Area (RUCA) codes and a separate "frontier" concept for the most sparsely settled counties; Canada and the UK use population-density and travel-time indices. The tier matters because the higher it is, the more the service model must compensate for distance with outreach, telehealth and retrieval. [4] [15]
Barriers to access
The barriers fall into four families that overlap in real towns. Geographic barriers are distance, travel time, road conditions and the cost of fuel or flights. Workforce barriers are the shortage and rapid turnover of clinicians willing and trained to work remotely. Sociocultural barriers are the erosion of confidentiality in small communities, stigma, language, and — for Indigenous and migrant young people — services that do not feel safe or culturally competent. Digital barriers are the poor connectivity that makes telehealth impossible exactly where it is most needed. [4] [14]
Delivery models
Rural adolescent care is delivered through a tiered model that stacks five components so no young person falls through the gap: a youth-friendly primary-care base (the GP, rural generalist or remote-area nurse who knows adolescent health), telehealth for subspecialty and mental-health input, outreach visiting services that travel to the community, school-based or mobile health that finds adolescents where they congregate, and a retrieval and referral backbone for acute and complex need. [6] [12]
Epidemiology & Risk Factors
Rural and remote adolescents are not uniformly sicker than their urban peers — they are sicker in a specific, repeatable pattern, concentrated in the conditions that depend on timely, confidential, specialist-supported care. [1] [9]
Mental health and suicide show the steepest and most consequential gradient. Population-based data show rural adolescents carry a higher burden of non-fatal suicidal ideation and suicide attempt than urban adolescents, and access to treatment is the limiting step — the crisis presents, but the service often does not. The pattern worsened through the COVID-19 pandemic, when rural adolescents reported more symptoms and self-harm alongside reduced access. [2] [3]
Sexual and reproductive health follows the same logic. Rural and remote young women have higher rates of adolescent birth and lower access to contraception, long-acting reversible contraception and termination services, so a preventable outcome becomes a common one. Substance use, especially smoking and increasingly vaping, is more prevalent in rural adolescents, and treatment services are scarcer. [8] [9] [10]
Injury is the leading cause of adolescent death everywhere, but the rural penalty is real: motor-vehicle crash fatality and hospitalisation rates are higher among rural children and youth, driven by speed, distance, lower restraint use, poorer roads and longer time to definitive care. [11]
The risk factors amplify one another. Poverty, lower health literacy, food insecurity, limited public transport, social isolation and intergenerational disadvantage concentrate in remote communities, and in ANZ they compound for Indigenous young people, who are overrepresented in remote populations and carry a disproportionate burden of the access gap. [1] [4]
Pathophysiology
There is no single molecular mechanism here — the "pathophysiology" is the mechanism of the access gap, the chain of causes that turns equal need into unequal outcome. Understanding the chain lets you intervene at the right link instead of blaming the young person for not seeking help. [1] [14]
The chain begins with workforce maldistribution. Specialists, adolescent physicians, child psychiatrists, psychologists and trained primary-care clinicians cluster in cities; remote communities rely on a thin layer of rural generalists, remote-area nurses and short-term locums who may rotate before trust is built. A national view of rural workforce shows persistent shortages in the very disciplines adolescence demands. [15] [16]
The second link is distance decay — the empiric observation that the further a patient lives from a service, the less likely they are to use it. For an adolescent dependent on a parent for transport, an hour-and-a-half drive and a day off school are often enough to suppress a confidential consultation entirely, so the consultation simply never happens. [4] [14]
The third link is the confidentiality paradox of small communities. Adolescence is the developmental stage at which a young person begins to seek care independently and to need privacy for sensitive disclosures — mental health, sexuality, sexual activity, substance use, abuse. In a town of a few hundred families, the receptionist, the nurse, the pharmacist and the clinician may all be known to the household. The fear that a disclosure will travel suppresses the very help-seeking the developmental stage demands, and the most sensitive conditions are the first to go unspoken. [1] [10]
The fourth link is the digital divide. Telehealth is the obvious answer to distance, but the connectivity that telehealth requires is weakest where distance is greatest, so the intervention can bypass the population it was designed to serve. Where a young person must take a video call from a shared household device on a throttled connection, privacy and access collapse together. [5] [7]
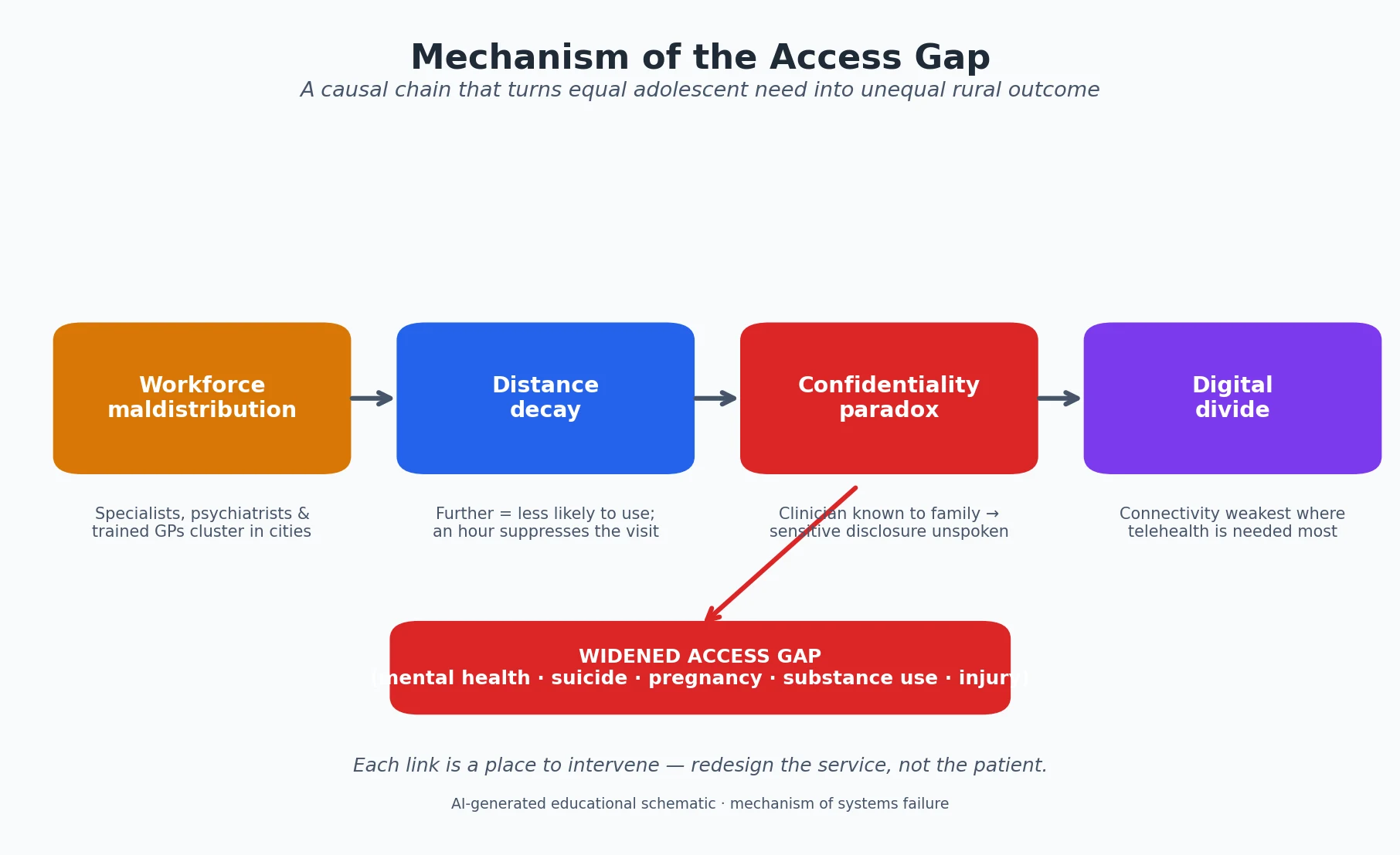
The chain resolves into one principle: the rural gap is a systems failure, not a patient failure. The young person who "didn't seek help" usually faced a path to care that was too long, too public, too slow or too disconnected — and redesigning that path is the treatment. [4] [14]
Clinical Presentation
Rural adolescents present with the same conditions as urban adolescents, but the tempo and the route of presentation differ, and examiners test these differences deliberately. Expect delayed presentation, more advanced disease at first contact, and presentations through non-clinical doors. [1] [11]
Delayed and advanced presentation is the hallmark. A depressive illness that an urban adolescent might bring to a GP at six weeks may present in a rural adolescent at six months, or only when it has become a self-harm presentation to an emergency department that is itself understaffed. A pregnant adolescent may present late to antenatal care because the local service does not feel confidential or because transport to the regional clinic was never available. [9] [3]
Mental-health crisis presentation dominates the acute end. Rural and remote adolescents more often present in suicide attempt, severe self-harm or acute behavioural disturbance, frequently to an ED without on-site mental-health staff, where the clinician must hold the young person safely while retrieval is arranged over hours. [2] [4]
Non-traditional entry points are common and important. The first contact may be a school nurse, a remote-area nurse, a youth worker, a pharmacist, a sports coach or a telehealth triage line rather than a doctor. Each of these gatekeepers needs to be equipped to recognise adolescent risk and to know the local pathway, because they are often the only accessible clinician. [12] [6]
Chronic-disease destabilisation appears in the adolescent with type 1 diabetes, complex asthma, chronic kidney disease or epilepsy whose condition worsens because specialist outreach lapsed, supplies ran out, or transition to adult care was never organised. The presentation is a preventable complication of interrupted care. [13]
Differential Diagnosis
The "differential" in this topic is twofold: the differential of the access gap itself (why did this young person not get care?), and the differential of anonymity-sensitive conditions that are systematically under-detected in small communities. [4] [14]
The first question to hold in mind is what is keeping the young person from care. Is it distance and transport, a workforce gap, a confidentiality fear, a cultural or language mismatch, cost, digital exclusion, or simply that no one asked? Naming the barrier is diagnostic, because it points to the structural fix and stops the team from concluding the young person was "non-compliant." [14] [4]
The conditions most likely to be missed are those an adolescent will not disclose without a guarantee of privacy. These are the same everywhere, but the rural penalty sharpens them. [1] [10]
Mental health
Depression, anxiety, suicidality
- Steepest rural-urban gradient
- Suppressed by confidentiality fear
- Specialist workforce thinnest here
- Often presents late, in crisis
Sexual & reproductive
STI, pregnancy, contraception
- Contraception and termination distant
- Higher teen-birth rate
- Pharmacy and GP known to family
- School-based access helps
Substance use
Smoking, vaping, alcohol
- Higher rural prevalence
- Treatment services scarce
- Stigma in small community
- Harm-reduction harder to deliver
Chronic disease
Diabetes, asthma, epilepsy
- Destabilises when outreach lapses
- Transition to adult care unmet
- Supplies and review distant
- Telehealth can stabilise
Hold a second differential for the crisis that exceeds local capacity. In a remote setting you must distinguish early what can be managed locally from what needs retrieval — sepsis, anaphylaxis, diabetic ketoacidosis, overdose, non-accidental injury and acute suicidality with a plan all cross the threshold where the right answer is to activate retrieval immediately rather than to wait and see. [4] [11]
Clinical & Bedside Assessment
The assessment tool is HEEADSSS, but the way it is run in a rural setting must be rebuilt around privacy, opportunism and the limitations of a thin workforce. A checklist completed in a shared consulting room with the parent present is worse than useless — it manufactures reassurance while finding nothing. [1] [6]
Secure privacy first. In a rural setting this is an engineering problem. Find a space where the conversation cannot be overheard; arrange telehealth from a private room with a headset, not a shared device; use interpreter and chaperone policies that do not compromise confidentiality; and build local protocols so that sensitive information is not routed through a community member at the front desk. If true privacy is impossible on the day, name that openly with the young person and arrange a confidential alternative rather than proceed and breach trust. [5] [7]
Run a rural-optimised HEEADSSS. The domains are unchanged — Home, Education/Employment, Eating, Activities, Drugs, Sexuality, Suicide and mood, Safety — but rural weighting shifts. Probe transport, isolation and connection to country and community under Home; probe school engagement and attendance under Education, since school disengagement predicts dropout and risk; ask about online exposure and digital access under Activities; and under Safety ask explicitly about access to firearms and other lethal means, which are more prevalent in rural households and directly raise suicide lethality. [1] [4]
Assess opportunistically at every contact. Because encounters are rare, every contact must count. A sports medical, an immunisation visit, an asthma review, an ED presentation for an unrelated injury, a telehealth follow-up — each is a chance to complete a focused HEEADSSS and to add a validated screen (CRAFFT or a frequency-based tool for substances; a mood and suicide instrument such as ASQ for low mood) when a lead appears. Build the screen into the template so it happens by default, not by memory. [6] [12]
Assess capacity for local management versus retrieval. At the bedside, gauge severity against what the local service can hold. A positive suicide screen with a plan, an overdose needing observation beyond local capability, a medically unstable adolescent, or safeguarding concern that cannot be protected locally all trigger the retrieval pathway there and then. [2] [4]
Investigations
Investigations in the rural setting are governed by one question: what can be done here, now, reliably, and what must travel? The strategy is point-of-care testing where it changes management, and a clear plan for everything that requires a laboratory, imaging or specialist interpretation at a distance. [6] [13]
Point-of-care and locally feasible tests include point-of-care HbA1c and ketones for a young person with diabetes, urine pregnancy testing and STI nucleic-acid amplification from self-collected samples where available, point-of-care testing for infectious presentations, and spirometry in a school-based or outreach asthma clinic. The advantage is immediacy — a result that changes management on the day the adolescent is actually present, who may not return for weeks. [13] [10]
Tests that travel are handled through a specimen logistics chain and a telehealth result-review plan. Bloods, microbiology and pathology specimens must reach the laboratory in time, and the result must reach a clinician who knows the young person and can act on it — a result filed in a distant system that no one actioned is a failure of the model, not a success of the test. [6]
Telehealth-enabled assessment extends what the local clinician can do. A remote adolescent physician or psychiatrist can direct a focused examination, interpret a screen, supervise a mental-health assessment, and decide with the local team whether management can stay local or whether retrieval is warranted. The evidence on rural and remote youth preference is that telehealth is accepted and often preferred for mental-health access, provided privacy and connectivity are solved. [5] [7]
Management — Resuscitation
The resuscitation phase in a rural setting is dominated by time and distance: the life-threatening problem must be identified and held while retrieval is mobilised, because definitive care is hours away rather than minutes. The bundle is recognition, stabilisation, safety, and early retrieval activation. [4] [11]
Recognise and stabilise using the same ABCDE approach as anywhere, but with an honest reading of local limits. A deteriorating adolescent in a one-doctor town needs early help: call the retrieval service and the regional paediatric or intensive-care team at the point of concern, not after exhausting local options. Resuscitation in remoteness is a team sport played over a radio link. [4]
Hold the suicidal or self-harming adolescent safely. After a positive suicide screen with plan or intent, or after an attempt, do not leave the young person alone, remove access to means — including firearms, which are more accessible in rural households — and activate the local mental-health crisis or retrieval pathway. A promise of safety is not a disposition; a structured same-visit risk assessment and a supervised handover are. [2] [4]
Activate retrieval early. In remote Australia and analogous settings, aeromedical retrieval services such as the Royal Flying Doctor Service exist precisely to compress distance for the acutely unwell. The principle is to call early: retrieval teams can advise, stabilise by phone, and time the aircraft to the patient rather than the patient to the aircraft. Early activation is not over-calling; it is the rural standard of care. [4]
Rural adolescent resuscitation and retrieval sequence
Recognise
ABCDE; identify the time-critical problem and read local limits honestly.
Stabilise
Hold airway, breathing, circulation; for self-harm, do not leave alone and remove means.
Call early
Contact retrieval and regional paediatric/ICU/mental-health teams at the point of concern.
Prepare for transfer
Gather records, medications, safeguarding context; brief the receiving team.
Handover
Structured handover; confirm receiving plan and who follows up after discharge.
Close the loop
Arrange local follow-up, results review, and reconnection to the young person's community.
Management — Definitive & Stepwise
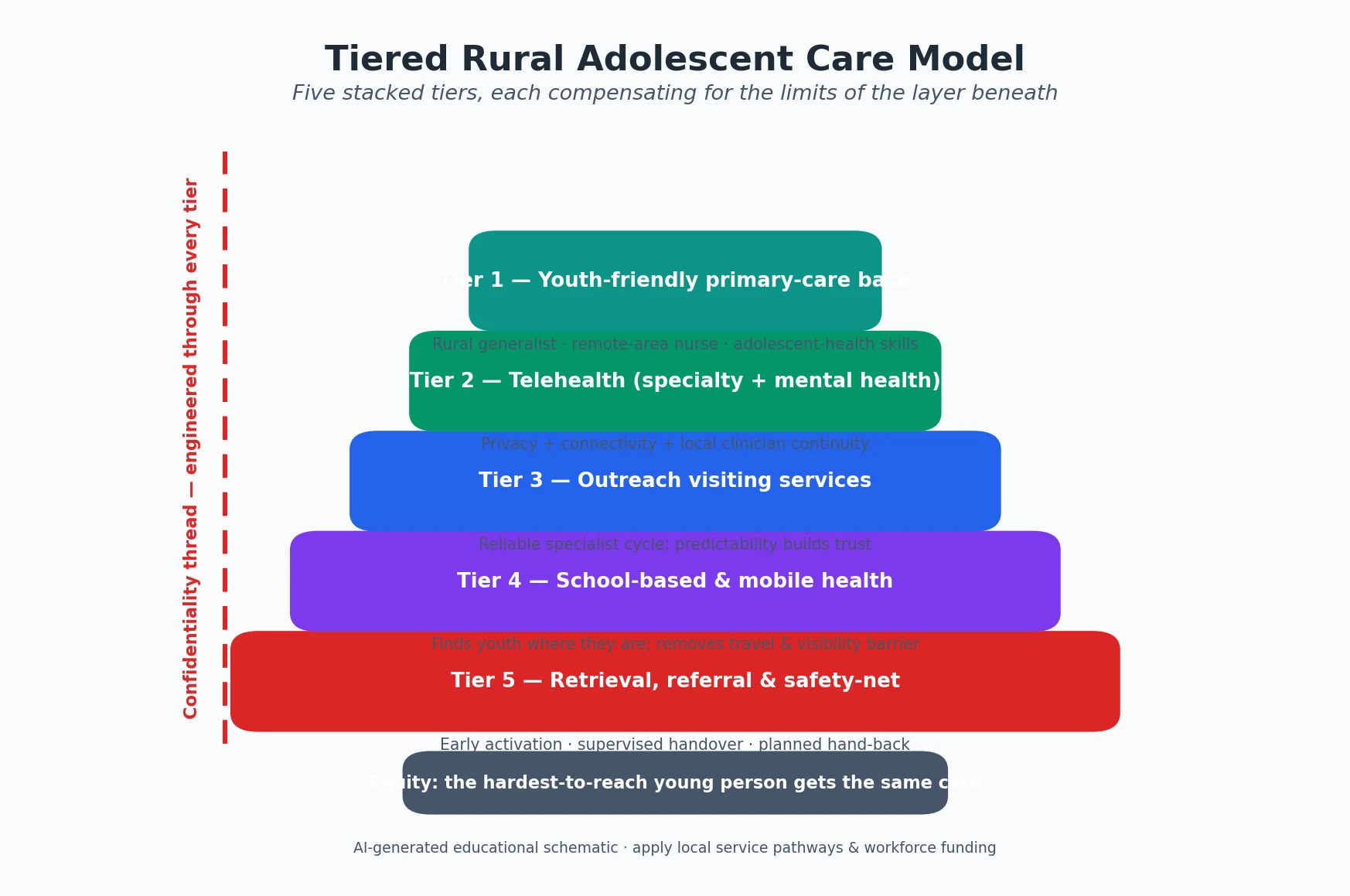
Definitive management is the tiered service model built deliberately so that prevention, early intervention and specialist care all reach the rural adolescent. The layers stack: each compensates for the limits of the one below it, and the measure of the system is the hardest-to-reach young person. [6] [12]
Tier 1 — Youth-friendly primary care
Every rural adolescent needs a home base of primary care that is trained in adolescent health, offers confidential consultation as a default, and can complete a HEEADSSS and add validated screens. Rural generalists, remote-area nurses and GPs with adolescent-health skills are the foundation; without them, every higher tier arrives into a vacuum. Workforce pipelines such as rural-generalist training exist precisely to grow this base. [16] [1]
Tier 2 — Telehealth
Telehealth brings adolescent medicine, child psychiatry, psychology, sexual health and subspecialty expertise to the community without moving the young person. The evidence shows rural and remote youth accept and often prefer telehealth for mental-health access, and primary-care telehealth strategies expand the range of adolescent issues a rural clinician can manage. The prerequisites are privacy, connectivity, and a local clinician who remains the continuous face of care — telehealth is an input to the team, not a replacement for it. [5] [6] [7]
Tier 3 — Outreach and visiting services
Outreach places the specialist physically in the community on a planned cycle — adolescent medicine clinics, child psychiatry, endocrinology for diabetes, nephrology for chronic kidney disease. The discipline of outreach is reliability: a predictable visiting pattern lets the local team plan and lets the young person trust that the specialist will return. Intermittent, uncoordinated visiting destroys continuity. [13] [6]
Tier 4 — School-based and mobile health
School-based health centres find adolescents where they already congregate and remove the largest single barrier — the need to travel and to be seen seeking care. In rural areas, school-based centres improve attendance and chronic-disease management such as asthma, and they are a preferred route to contraception and confidential care for young people. Mobile health units extend the same logic to communities without a fixed school clinic. [12] [13] [10]
Tier 5 — Retrieval, referral and safety-net
The final tier is the retrieval and referral backbone: aeromedical and road retrieval for acute need, clear referral pathways to regional centres, and a safety-net of follow-up that reconnects the young person to their community after an episode of distant care. Transition to adult services — often delayed or absent for rural adolescents with chronic disease — belongs here and must be planned, not assumed. [4] [13]
Specific Subtypes & Scenarios
Each major rural adolescent scenario has its own access problem and its own service response. Examiners expect the candidate to move from the general model to the specific case. [1] [4]
Rural adolescent mental health and suicide
This is the scenario with the steepest gradient and the highest stakes. Rural adolescents carry more suicidal ideation and attempt, present more often in crisis, and meet the thinnest specialist workforce. The response is a stepped-care model: HEEADSSS and a validated suicide screen at the primary-care base; telehealth psychology and child psychiatry for moderate need; outreach psychiatric clinics for severe or complex presentations; a clear crisis-and-retrieval pathway for acute risk; and lethal-means counselling that addresses rural firearm access directly. [1] [2] [3]
Rural sexual and reproductive health
The access gap produces higher adolescent birth rates and lower contraception uptake. The response is confidential contraception provision (including long-acting reversible contraception) through primary care and school-based centres, STI testing to disclosed sites, pregnancy options counselling with a clear pathway to termination services where lawful and available, and telehealth sexual-health input. The barrier to dismantle is the confidentiality fear that keeps young people from asking. [9] [10]
Rural substance use
Smoking and vaping are more prevalent in rural adolescents and treatment is scarcer. Apply the harm-minimisation stance: screen with a validated tool, give brief motivational intervention, offer harm-reduction and cut-down support, and link to telehealth or outreach substance-use treatment. Non-judgemental, low-threshold access matters more in a small community, where stigma is a stronger suppressor. [8]
Rural chronic disease and transition
The adolescent with type 1 diabetes, complex asthma, chronic kidney disease or epilepsy is destabilised when outreach lapses or transition is never organised. School-based centres improve rural asthma management; telehealth stabilises diabetes review; and a planned transition to adult care prevents the gap-year in which a rural young person is lost to follow-up. [13] [6]
Indigenous, remote and culturally diverse young people
In ANZ, Indigenous young people are overrepresented in remote populations and carry a disproportionate share of the access gap, compounded by intergenerational trauma and services that historically did not feel safe. The response is culturally safe, community-led care, Indigenous health workers in the team, and respect for connection to country. For migrant, refugee and asylum-seeking rural adolescents, language, interpreter access and cultural competence are part of the service, not optional extras. [1] [4]
Complications & Pitfalls
The complications of rural adolescent care are mostly system complications — the predictable failures of a model run thin. Naming them lets you build the guard-rails that prevent them. [4] [14]
Confidentiality breach in a small community is the single most damaging pitfall. A sensitive disclosure that travels — through a receptionist, a shared record, a portal, or a clinician who is the family friend — destroys trust not only for that young person but for every adolescent who hears about it. Guard-rails include confidential adolescent records, sensitive-note workflows, private telehealth spaces, and a standing rule to verify who may receive information before it is shared. [1] [10]
The "abstinence-only" or "wait-and-see" default fails rural adolescents hardest. Demanding that a young person stop a behaviour before any support is offered, or deferring care because the specialist is distant, removes the only low-threshold contact the young person may have. Harm-minimisation and opportunistic intervention are rural imperatives, not urban luxuries. [4]
Telehealth inequity is a pitfall disguised as a solution. If telehealth is delivered over a connection that drops out, from a shared device, or without a private space, it widens the gap rather than closing it. Build telehealth with connectivity, privacy and a local clinician, or it will fail the adolescents who need it most. [5] [7]
Failure to retrieve, and failure to return. Under-calling retrieval delays definitive care; over-calling without follow-up strands a young person in a distant system. Both are corrected by early, structured retrieval activation and by a planned hand-back to the local team and community after the episode. [4] [11]
Workforce burnout and turnover breaks continuity. The sole rural clinician who holds every adolescent in the district is vulnerable, and rotation of locums erodes the trust that confidential adolescent care requires. Sustainable rosters, peer support, and rural-generalist pipelines that retain clinicians are clinical interventions, not merely workforce policy. [15] [16]
Prognosis & Disposition
Prognosis in rural adolescent health is determined less by the disease than by whether the service model reaches the young person in time and in confidence. The same depressive illness has a different outcome when a confidential telehealth psychology session is a week away versus when the nearest help is six hours and a broken trust away. [1] [5]
Disposition follows the tiered model. The majority of rural adolescent presentations are managed at the primary-care base with telehealth support; a minority require outreach specialist input; a smaller minority require retrieval and referral. The disposition decision turns on severity, local capability, and the reliability of follow-up — and follow-up must always be explicit, because in a remote setting "the family will follow up" is a hope, not a plan. [6] [4]
Transition to adult care is a disposition problem that is routinely failed for rural adolescents with chronic disease. A planned, telehealth-supported transition with a named adult provider and a hand-back to the local team prevents the lost-to-follow-up year that drives long-term complications. [13]
The safety-net is the final determinant of prognosis: a young person who knows how to re-access care, who has a crisis plan, and who is held by a local clinician between visits does better than one discharged to a void. Building that safety-net is the disposition, not an afterthought to it. [2] [12]
Special Populations
Several rural adolescent populations carry compounded risk and need a deliberately adapted service. [4] [1]
Indigenous young people in remote ANZ carry the heaviest compounded burden — of access gap, of intergenerational trauma, and of historical services that did not feel safe. Culturally safe, community-led care with Indigenous health workers in the team is the standard, and connection to country and community are protective factors to build on, not barriers to manage around. [1]
Migrant, refugee and asylum-seeking adolescents in rural areas face language barriers, interpreter access problems, and services that may not be culturally competent. Interpreter-mediated consultation, trauma-informed care, and attention to the legal and financial barriers to care are part of the service model. [4]
Young people in out-of-home care and youth justice are overrepresented in rural and remote systems and carry high rates of trauma, mental-illness and risk behaviour. Their care must be coordinated, trauma-informed, and continuous across placements — exactly the continuity that distance and turnover threaten. [4]
LGBTQI+ young people in small communities face a sharper confidentiality paradox: the disclosure that matters most to them is the one hardest to keep private. Confidential, affirming care, delivered in person or by telehealth with a clinician trained in gender and sexual diversity, is essential. [10]
Adolescents with disability and neurodiversity in rural settings face combined barriers of access, communication and specialist scarcity. Longer appointment times, telehealth specialist input, and coordination with education and therapy services are the adaptations that make care equitable. [6]
Evidence, Guidelines & Regional Differences
The evidence base for rural adolescent health is strengthening fastest in telehealth and school-based care, while the core disparities are long-standing and reproducible across countries. Regional differences are mostly in how services are funded and classified, not in the underlying gap. [4] [6]
Telehealth evidence now shows that rural and remote youth accept and often prefer telehealth for mental-health access, and that primary-care telehealth strategies expand the adolescent agenda a rural clinician can safely manage. The open question is equity: telehealth helps most where connectivity and privacy are solved, and bypasses those without them. [5] [6] [7]
School-based health evidence is among the strongest in the field: rural school-based centres improve school attendance and chronic-disease outcomes such as asthma, and they are a preferred route to confidential contraception for rural young people. The mechanism is removal of the travel and visibility barrier. [12] [13] [10]
ANZ
MMM tiers, rural generalist
- Modified Monash Model grades MM1–MM7
- Rural-generalist and ACRRM/RACGP pathways
- Royal Flying Doctor Service retrieval
- Indigenous community-led care emphasis
United States
RUCA and frontier
- RUCA codes plus 'frontier' counties
- HRSA workforce and shortage designations
- School-based health centre expansion
- Medicaid and insurance-driven access
UK & Europe
Rural and island
- Remote Scottish island sexual-health access
- Distance and ferry/air dependency
- NHS telehealth and outreach
- Smaller absolute numbers, same equity logic
Canada & global
Frontier and LMIC
- RCPSC rural and remote competencies
- Indigenous and northern-community care
- LMIC rural adolescent access barriers
- Stigma, cost and workforce scarcity
Regional classification differences do not change the clinical logic. Whether a community is MM7, a frontier county, or a remote island, the response is the same tiered model adapted to local funding, workforce and geography. The controversy in the field is not whether the gap is real — it is reproducibly documented — but how to fund the workforce and connectivity that close it, and how to ensure telehealth reaches those without reliable connections. [14] [15]
Exam Pearls
A fellowship candidate should leave no corner of this topic unattended. The high-yield facts below are the ones examiners reach for in written, long-case, communication and structured-oral formats. [1] [4]
REMOTE — the rural adolescent care principles
Frequently tested facts, correctly stated: [1] [2]
- Rural and remote adolescents carry a higher burden of suicidal ideation and attempt than urban peers, and access to treatment is the limiting step — not recognition alone. [2]
- Rural-urban disparities in adolescent birth rates widened over two decades in the US; contraception and termination access drive the gap. [9]
- Rural disparities in adolescent smoking are persistent; vaping follows the same pattern. [8]
- Motor-vehicle crash fatality and hospitalisation rates are higher among rural children and youth. [11]
- Rural and remote youth often prefer telehealth for mental-health access, provided privacy and connectivity are solved. [5]
- Rural school-based health centres improve attendance and chronic-disease management such as asthma. [12] [13]
- Rural-generalist training pathways are a workforce intervention that directly grows the primary-care base. [16]
- Early retrieval activation compresses distance for the acutely unwell; waiting to exhaust local options delays definitive care. [4]
References
- [1]Boyd CP, Aisbett DL, Francis K et al Issues in rural adolescent mental health in Australia Rural and remote health, 2006.PMID 16506881
- [2]Goldman-Mellor S, Allen K, Kaplan MS Rural/Urban Disparities in Adolescent Nonfatal Suicidal Ideation and Suicide Attempt: A Population-Based Study Suicide & life-threatening behavior, 2018.PMID 28940747
- [3]Brausch AM, Whitfield M, Clapham RB Comparisons of mental health symptoms, treatment access, and self-harm behaviors in rural adolescents before and during the COVID-19 pandemic European child & adolescent psychiatry, 2023.PMID 35817947
- [4]Brooks D, Jani S Rural and Frontier Communities Child and adolescent psychiatric clinics of North America, 2024.PMID 39277322
- [5]Mseke EP, Jessup B, Barnett T A systematic review of the preferences of rural and remote youth for mental health service access: Telehealth versus face-to-face consultation The Australian journal of rural health, 2023.PMID 36606417
- [6]Chiccarelli E, North S, Pasternak RH Innovative Strategies for Addressing Adolescent Health in Primary Care Through Telehealth Pediatric clinics of North America, 2024.PMID 39003011
- [7]Svistova J, Harris C, Fogarty B et al Use of Telehealth Amid the COVID-19 Pandemic: Experiences of Mental Health Providers Serving Rural Youth and Elderly in Pennsylvania Administration and policy in mental health, 2022.PMID 34846613
- [8]Kim S, Selya A Rural disparities in adolescent smoking prevalence The Journal of rural health : official journal of the American Rural Health Association and the National Rural Health Care Association, 2022.PMID 34339070
- [9]Sutton A, Lichter DT, Sassler S Rural-Urban Disparities in Pregnancy Intentions, Births, and Abortions Among US Adolescent and Young Women, 1995-2017 American journal of public health, 2019.PMID 31622143
- [10]Westbrook M, Martinez L, Mechergui S et al Contraceptive Access Through School-Based Health Centers: Perceptions of Rural and Suburban Young People Health promotion practice, 2022.PMID 34338038
- [11]Kmet L, Macarthur C Urban-rural differences in motor vehicle crash fatality and hospitalization rates among children and youth Accident; analysis and prevention, 2006.PMID 16139232
- [12]Kjolhede C, Brunner WM, Sipple JW School-Based Health Centers and School Attendance in Rural Areas JAMA network open, 2025.PMID 40358944
- [13]Brunner WM, Han Z, Tennyson S et al Impact of Rural School-Based Health Centers on Asthma Management The Journal of pediatrics, 2025.PMID 39491783
- [14]Mengesha AK, Ayele HS, Beyna AT et al Exploring barriers to mental health care access among rural adolescents in Gondar Zuria, Ethiopia: a qualitative study BMC public health, 2025.PMID 41469875
- [15]MacDowell M, Glasser M, Fitts M et al A national view of rural health workforce issues in the USA Rural and remote health, 2010.PMID 20658893
- [16]Woolley T, Larkins S, Sen Gupta S Career choices of the first seven cohorts of JCU MBBS graduates: producing generalists for regional, rural and remote northern Australia Rural and remote health, 2019.PMID 30943751