Paeds · adolescent-and-young-adult-medicine
Adolescent pregnancy and parenting
Also known as Teenage pregnancy · Adolescent parent · Young parent care · Pregnancy in adolescence · Rapid repeat pregnancy · Teen mother and teen father · Adolescent reproductive health in pregnancy
A fellowship approach to adolescent pregnancy and parenting: non-judgemental confirmation and dating, safeguarding-aware options counselling, coordinated antenatal care, adolescent-specific obstetric and psychosocial risk recognition, mental health, nutrition, breastfeeding and education support, postpartum contraception to prevent rapid repeat pregnancy, and longitudinal parenting support across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 16-year-old presents with six weeks of amenorrhoea and nausea. She has not told her mother. The temptation is to treat this as a discrete "problem to solve" — confirm, refer, discharge. But adolescent pregnancy is a developmental crossroads: the young person is still completing their own growth, education and identity formation while becoming a parent, and the choices made in the next few months shape two trajectories for decades. The clinician who sees only a positive test misses the patient. [2] [10]
Adolescent pregnancy is pregnancy in a young person, conventionally 10–19 years, though many services extend the frame into the early twenties (young parent). It is not a single entity. A planned, wanted pregnancy in a supported 18-year-old is a different clinical and ethical task from a concealed pregnancy in a 13-year-old with an older partner. The clinician's job is to classify which adolescent pregnancy is in front of them — by intent, gestation, risk and context — and tailor care accordingly, while holding the same non-judgemental, safeguarding-aware stance throughout. [2] [1]
The evidence is unambiguous on two points. First, biological immaturity and psychosocial stress raise the obstetric and mental-health risks of pregnancy in adolescents, particularly in the youngest and least-supported. Second, outcomes improve dramatically with early, supportive, coordinated care — and the single most powerful preventer of repeat adversity is effective postpartum contraception. The framing matters: adolescent parents who are supported can parent well, and a deficit-only stance causes harm. [3] [12] [4]
Core arc of adolescent pregnancy and parenting care
Confirm & date
Urine β-hCG, serum β-hCG if unclear, dating ultrasound; exclude ectopic.
Engage alone
Time alone, confidentiality with lawful limits, non-judgemental stance, capacity and who-to-involve.
Options & safeguarding
Parenting, adoption, termination where legal — non-directive; safeguarding review for coercion/age gap.
Antenatal MDT
Midwifery + obstetrics + paeds + social work + mental health; screening, nutrition, education.
Birth, postpartum & prevent repeat
Breastfeeding, mood, attachment; contraception planned before discharge.
Classification
Start with the person in front of you, then classify on four axes that change the care plan: pregnancy intent, gestation at presentation, risk profile, and parenting context. [2]
Pregnancy intent
A pregnancy may be intended and wanted — some young people actively choose parenthood, and the clinician's role is to support, not to pathologise. It may be unintended but now wanted, where the task is antenatal and parenting support. It may be unintended and ambivalent, where time-pressured, non-directive options counselling is the urgent skill. Or it may be unintended and unwanted, where termination counselling (where legally available) and safeguarding review come to the fore. Intent is not static — adolescents reassess as gestation advances and as supports become clear. [2] [11]
Gestation at presentation
Gestation at first contact is itself a risk marker. Early presenters (before 20 weeks) allow full dating, screening and an open options window. Mid-pregnancy presenters (20–34 weeks) can still complete most screening but need a catch-up antenatal plan. Late or unbooked presenters (≥35 weeks with little or no care) are a high-risk subtype: missed antenatal opportunity, higher complication rates, and a staged, rapid MDT assessment. Occasionally the pregnancy is revealed only postpartum, when both parent and infant need assessment and the mental-health, feeding and safeguarding work begins at once. [2] [12]
Risk profile and parenting context
Risk layers into obstetric (pre-eclampsia, preterm birth, anaemia, STI, low birthweight), psychosocial (housing, school, finance, intimate partner violence), mental health (antenatal/postnatal depression, substance use, self-harm), and safeguarding (coercion, age or power asymmetry, trafficking, abuse). The parenting context — co-parenting, solo/unsupported, grandparent-supported, or care-experienced (out-of-home care or youth justice) — further shapes the support intensity required. [3] [10]
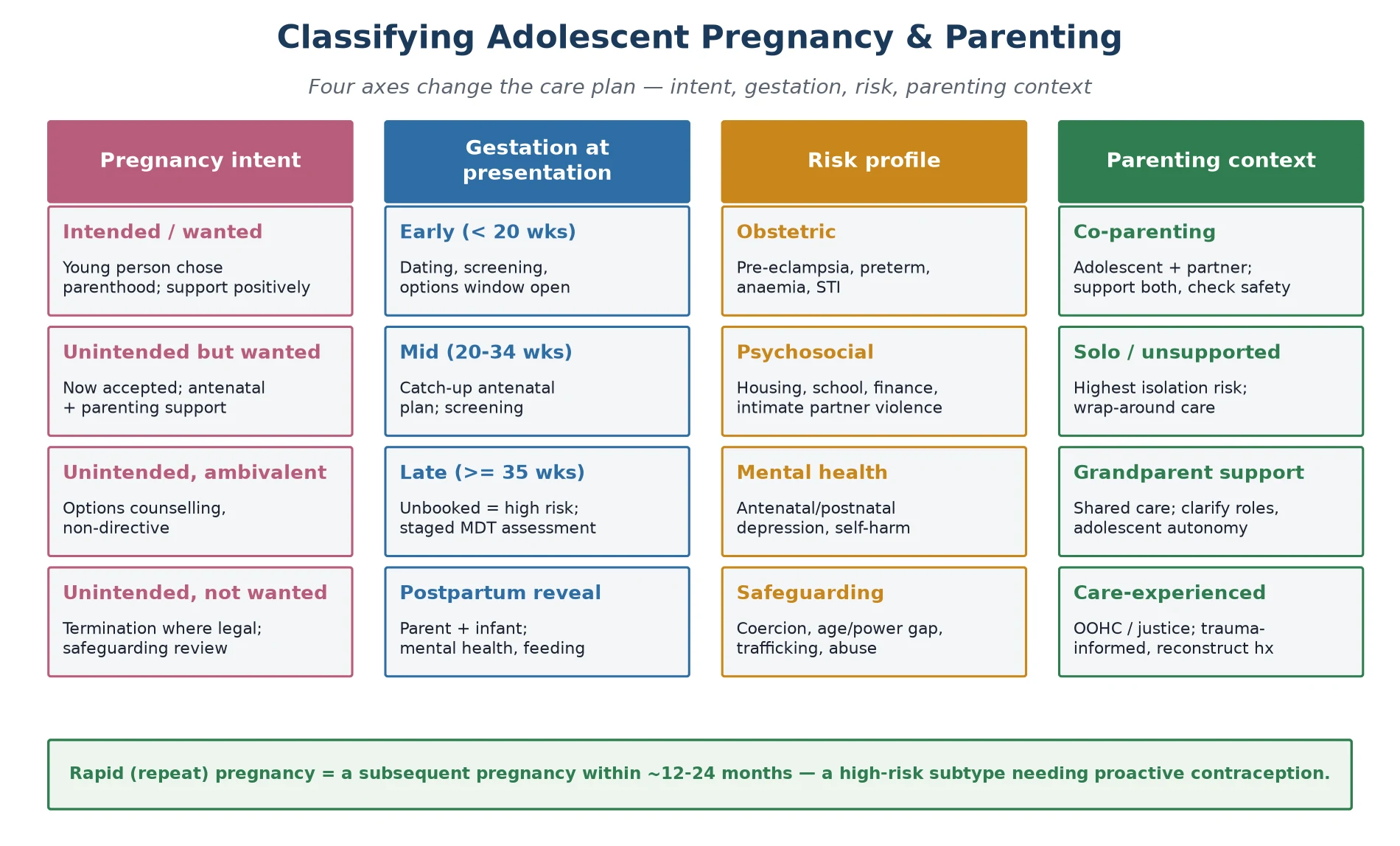
Read the figure like this: if you have not actively classified intent, you cannot counsel; if you have not checked gestation, you may miss the options window; if you have not screened for safeguarding, you may be providing care inside a coercive relationship. [2] [10]
Planned, wanted
Supported young parent
- 18–19y, stable relationship
- Affirm and support positively
- Antenatal + parenting focus
- Contraception still planned postpartum
Unintended, ambivalent
Time-pressured counselling
- Non-directive options
- Safeguarding review
- Avoid pushing any single path
- Close follow-up of decision
Coercion suspected
Safeguarding first
- Older partner, age/power gap
- Reproductive coercion screen
- Mandatory reporting per local law
- Support, do not punish
Late / unbooked
High-risk obstetric
- Missed antenatal care
- Rapid MDT assessment
- Higher complication rate
- Exclude concealed abuse
Epidemiology & Risk Factors
Adolescent pregnancy rates have fallen substantially in most high-income settings over recent decades, driven by better sex education, contraception access (especially long-acting reversible methods) and, in some regions, changing aspirations. But rates vary enormously between and within countries, and the burden falls hardest on the most disadvantaged young people. Cross-country comparisons make clear that adolescent birth rates are a marker of social policy and equity as much as of individual behaviour. [1] [10]
The risk is not evenly distributed. Poverty, school disengagement, out-of-home care, rural and remote location, Indigenous status, migrant and refugee background, intimate partner violence and a personal or family history of teenage pregnancy all raise risk. Younger adolescents (under 15) carry the greatest biological and safeguarding concern, while 18–19-year-olds approach adult risk profiles. A key subtype is rapid repeat pregnancy — a subsequent pregnancy within roughly 12–24 months — which compounds educational, economic and obstetric disadvantage and is strongly predicted by absent or delayed postpartum contraception. [6] [7] [3]
Partner factors matter and are often under-explored. An older partner, a coercive relationship, or reproductive coercion (interfering with contraception or pressuring pregnancy) not only raises pregnancy risk but triggers safeguarding obligations. The clinician who documents "single partner, age appropriate" without actually asking has not assessed risk. [10] [11]
Pathophysiology
You do not need a full reproductive endocrinology lecture to counsel well. You do need a usable model of why adolescents carry extra risk, because the model drives the screening and support you offer. [3]
Biological immaturity is real. A still-growing adolescent competes for nutrients with a fetus; in the youngest, pelvic and reproductive structures may be incompletely developed. These biological facts underpin the excess of anaemia, pre-eclampsia, preterm labour and low birthweight seen in adolescents — an excess that narrows but does not vanish when antenatal care is excellent and social confounders are controlled. [3] [12]
Psychosocial stress is not background noise; it is a physiological driver. Stigma, isolation, financial precarity, housing instability and intimate partner violence raise cortisol, worsen sleep, impair nutrition and reduce clinic attendance. The adolescent who "does not engage" is often an adolescent under such stress that engagement is nearly impossible without active outreach. [2] [10]
Interrupted development is the strand examiners reward you for naming. Pregnancy and early parenthood collide with the developmental tasks of adolescence itself — identity formation, education, peer relationships and the brain maturation that underpins executive function and long-term planning. When these tasks are disrupted, the pathway to adult independence is derailed, and that derailment is partly how adolescent parentage propagates disadvantage across generations. The protective modifiers are the same things the management section operationalises: supportive antenatal care, mental-health screening, breastfeeding support, education continuity, and contraception before discharge. [2] [8]
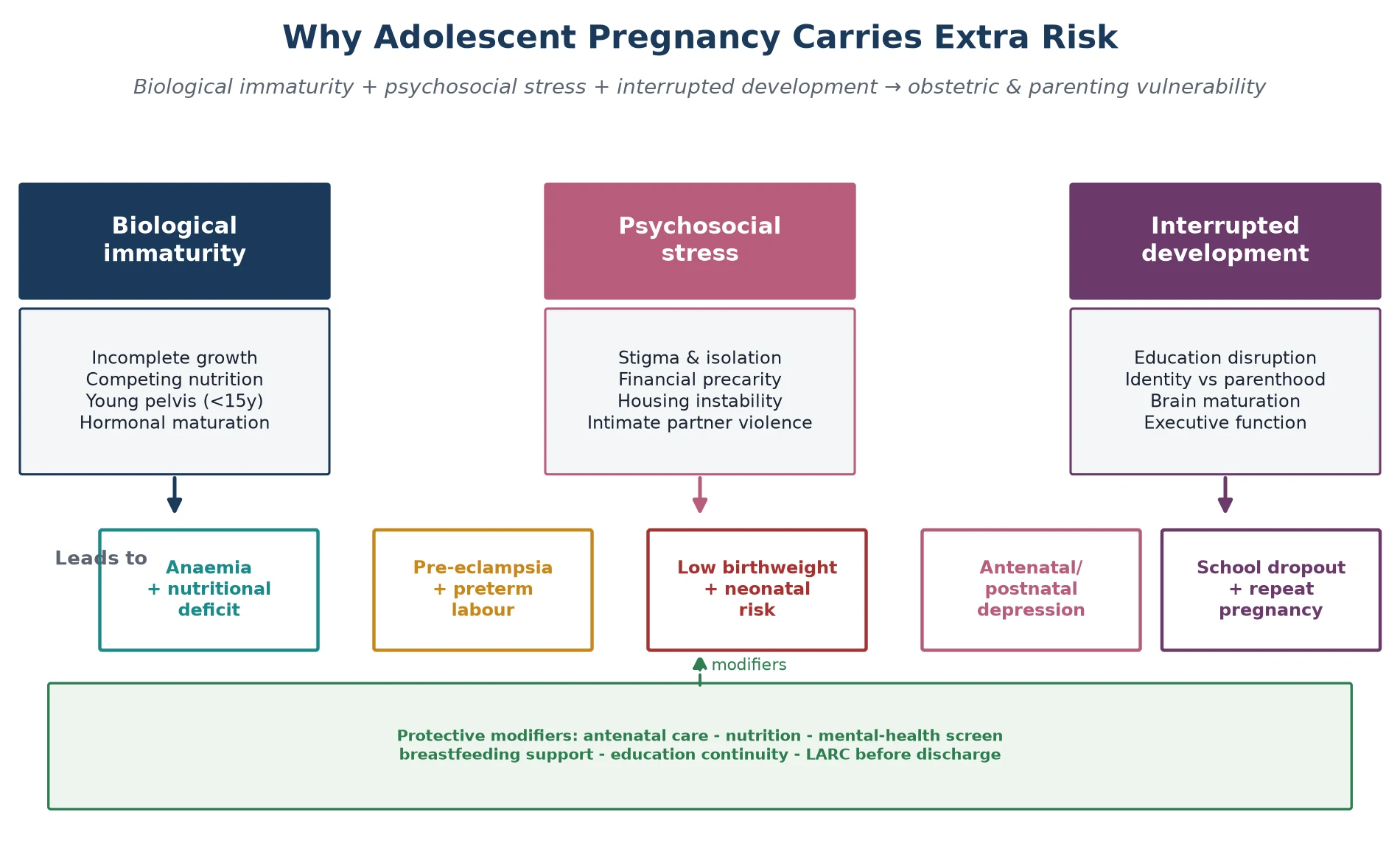
Read the figure like this: the arrows run both ways. Good antenatal care does not erase biological immaturity, but it shifts every outcome to the right. The clinician's job is to maximise the modifiers. [3] [12]
Clinical Presentation
A pregnant adolescent rarely walks in announcing the diagnosis. More often she presents with missed periods, nausea, fatigue or weight change, or she surfaces in a "routine" adolescent visit where the pregnancy is undisclosed. A high index of suspicion and a confidential, non-judgemental opening are what surface the truth. [2] [10]
Atypical and emergency presentations are the traps. Abdominal pain with vaginal bleeding may be ectopic — a time-critical diagnosis not to be attributed to "normal pregnancy cramps." Heavy bleeding may signal miscarriage. An adolescent may first present through a mental-health crisis, substance intoxication, or an injury that masks the pregnancy entirely. The clinician who forgets to consider pregnancy in a symptomatic adolescent misses a common, consequential diagnosis. [2]
The distressed pregnant adolescent presents with stigma, concealment and fear of family disclosure; conflict with education; or coercive relationship dynamics that she may not name as abuse. A late or unbooked presentation is itself a red flag for concealed abuse, neglect or barriers to access. Postpartum, the adolescent parent may present with isolation, low mood, breastfeeding struggle or attachment difficulty — or, deceptively, as a "well-child" visit where the parent is the unwell one. Intimate partner violence or reproductive coercion frequently sits alongside pregnancy and must be actively sought. [10] [9]
[9] [10]Differential Diagnosis
In this topic the differential is "what else could this be, and what must I not miss alongside the pregnancy." [2]
| Presentation | Consider alongside | Do not miss |
|---|---|---|
| Positive pregnancy test | False positive, chemical pregnancy, recent miscarriage, molar pregnancy | Ectopic (pain/bleeding) |
| Nausea and vomiting | Hyperemesis, gastroenteritis, urinary tract infection | Ectopic; dehydration and electrolyte disturbance |
| Abdominal pain in pregnancy | Round-ligament pain, urinary tract infection, constipation | Ectopic, miscarriage, pre-eclampsia, appendicitis |
| Fatigue and low mood | Normal pregnancy fatigue, anaemia, thyroid disease | Major depression, iron-deficiency anaemia |
| Postpartum low mood | Normal adjustment, sleep deprivation | Postnatal depression, postpartum psychosis (emergency) |
| Breastfeeding difficulty | Poor latch, low supply, engorgement | Mastitis, abscess, maternal ambivalence/depression |
| Parenting struggle | Developmental, expected learning curve | Neglect, safeguarding concern |
Two traps recur. The first is attributing all symptoms to "normal pregnancy" and missing coincident anaemia, thyroid disease, STI or mental illness — pregnancy does not confer immunity from anything else. The second is attributing parenting difficulty to youth alone and missing a treatable postnatal depression or, in the worst case, a safeguarding concern about the infant. When in doubt, investigate and ask; do not reassure on assumption. [9] [12]
Clinical & Bedside Assessment
1. Open and set the frame
Greet the young person first. Establish time alone before the sensitive history. State conditional confidentiality with its lawful limits, and explicitly assess capacity and who should be involved. A non-judgemental stance is not optional courtesy — it is what makes accurate information possible. [10]
2. Focused history
Take a menstrual, sexual and obstetric history; confirm LMP and contraceptive use. Tailor a HEEADSSS-style psychosocial assessment to the pregnant context: home and who is safe there, education and whether she plans to return, eating and nutrition, activities and supports, drugs including alcohol and vaping, sexuality and partner safety, and mood and self-harm. Screen actively for intimate partner violence and reproductive coercion. [2] [10]
3. Confirm gestation and exclude emergency
Establish gestational age from LMP and confirm with a dating ultrasound. If there is pain, bleeding, haemodynamic compromise or a non-typical trajectory, exclude ectopic pregnancy and miscarriage — do not file these as "normal." Blood pressure, urinalysis and a focused abdominal exam belong in the first contact. [2]
4. Obstetric and adolescent-specific risk screen
Assess for the risks adolescents carry disproportionately: anaemia, hypertensive disease, preterm labour risk, STIs, nutritional deficit and mental ill-health. Examine respectfully, with consent and chaperone for any sensitive exam. [3] [12]
5. Social and safeguarding assessment
Map housing, finances, education status, partner and family support, and safety. Where there is a child below the local age of consent, a coercive older partner, trafficking indicators, or ongoing abuse, escalate safeguarding per local statute — while explaining to the young person what you must share and why. [10] [2]
6. Postpartum and parenting assessment
After birth, assess breastfeeding, parent–infant interaction, postpartum anaemia and mood. Use a validated depression screen where available. Crucially, assess contraceptive needs and plans before discharge — this is the single highest-yield postpartum assessment for preventing rapid repeat pregnancy. [6] [8] [9]
[2] [9] [10]Investigations
Investigations serve three goals: confirm and date the pregnancy, complete antenatal screening, and detect the risks adolescents carry disproportionately. [2] [12]
Confirm and date: a urine β-hCG confirms pregnancy; serum β-hCG helps where the urine test is equivocal or ectopic is suspected (serial titres matter more than a single value). A pelvic ultrasound confirms a viable intrauterine pregnancy and establishes gestational age. In a symptomatic early pregnancy, ultrasound plus serial β-hCG is the ectopic-exclusion pathway. [2]
Routine antenatal panel (per local guidance): blood group and antibodies, full blood count, ferritin, blood pressure, urinalysis and culture, syphilis, HIV, hepatitis B, and rubella/varicella status where relevant. STI screening — chlamydia and gonorrhoea, with syphilis and HIV — is indicated in all sexually active adolescents and is often repeated in pregnancy given higher acquisition risk. Anaemia screening is especially important in adolescents, who start pregnancy with lower iron stores. [3] [12]
Selective investigations: where obstetric or nutritional risk is high, growth ultrasound and targeted nutritional markers guide care. Mental-health screening instruments (e.g. Edinburgh Postnatal Depression Scale principles adapted antenatally and postnatally) are part of the investigation set, not optional extras. Genetic and aneuploidy screening is offered per local guidance, with counselling adapted to the adolescent's developmental level. [9]
Low-value patterns: routine endocrine or extensive panels without indication, repeated STI panels without exposure or symptom change, and using a screen score as a diagnosis. Pregnancy does not justify investigation theatre; it justifies targeted, guideline-led testing. [12]
Management — Resuscitation
Most adolescent pregnancy care is planned and supportive, but a "routine" visit can tip into an emergency in one disclosure. [2]
- Suspected ectopic or miscarriage with compromise: ABCDE, IV access, cross-match, urgent obstetric/gynaecology referral and theatre pathway. Do not delay for paperwork. [2]
- Severe pre-eclampsia, eclampsia or HELLP: blood pressure control, magnesium sulfate per local protocol for seizure prophylaxis (dose and monitoring per institutional guideline), and urgent obstetric transfer. [2]
- Sepsis or septic miscarriage: sepsis bundle, cultures, broad-spectrum antibiotics per local guidance, and source control with obstetrics. [2]
- Acute mental-health crisis: do not leave a suicidal adolescent or a postpartum psychosis patient alone; escalate to crisis/ED, remove means, and arrange urgent psychiatric assessment. Postpartum psychosis is a psychiatric emergency. [9]
- Safeguarding disclosure: intimate partner violence, reproductive coercion, sexual assault, trafficking, or a child below the local age of consent with an older partner — follow local mandatory-reporting and child-protection pathways, share the minimum necessary, and support the young person through the process. [10]
Document decisions, who was informed, and the safety plan. Where confidentiality is overridden for safety, tell the young person what you must do and why, and preserve dignity throughout. [10]
Management — Definitive & Stepwise
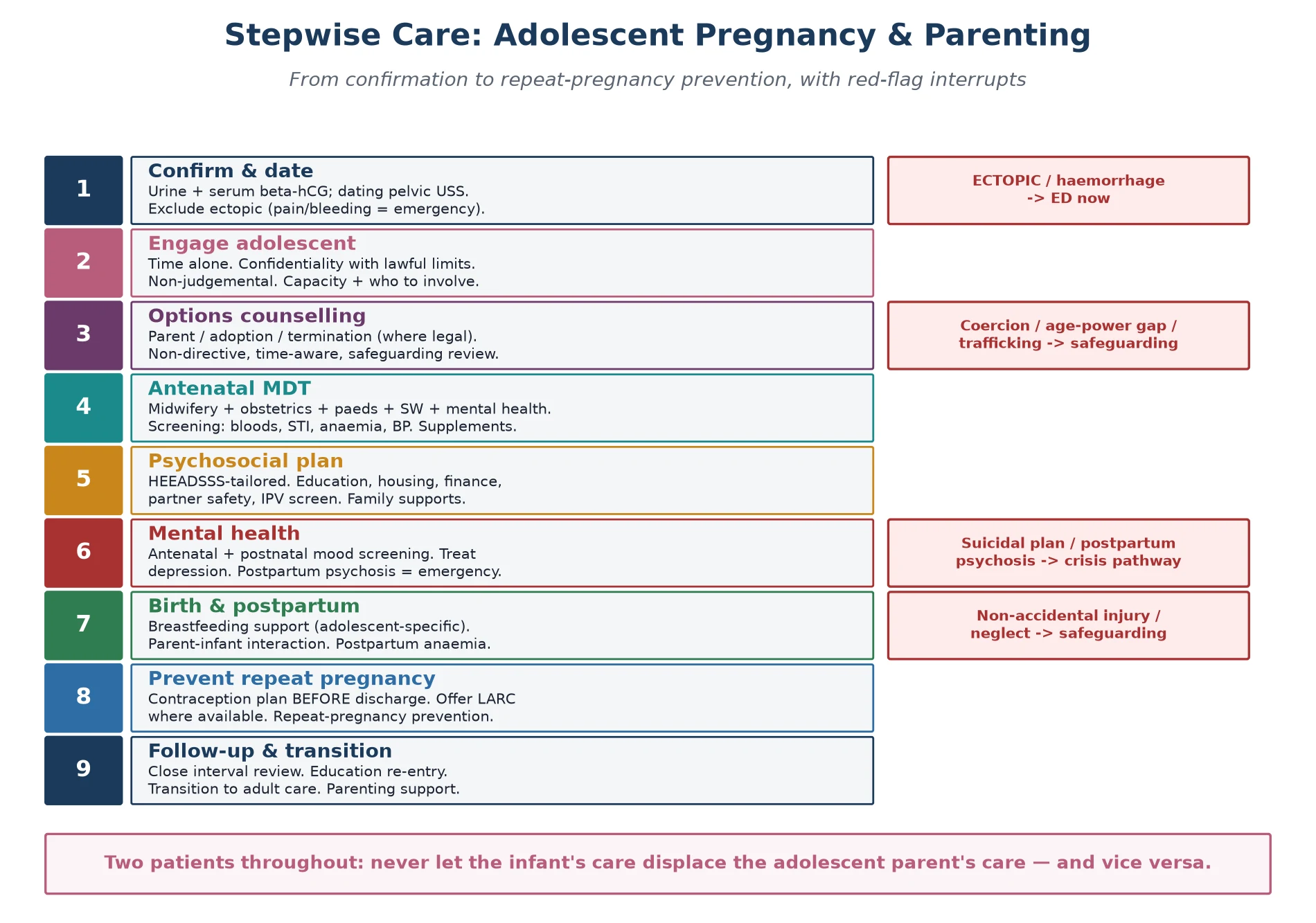
Read the figure like this: contraception sits before discharge, not after. The rapid-repeat-pregnancy prevention loop is part of the algorithm, not an afterthought. [4] [6]
Stepwise pathway
- Confirm and date. Urine ± serum β-hCG and dating ultrasound; exclude ectopic. [2]
- Engage the adolescent alone. Confidentiality with lawful limits; non-judgemental stance; assess capacity and who to involve. [10]
- Options counselling. Present continuing with parenting, continuing with adoption, and termination (where legally available) in a balanced, non-directive way, within the relevant time window, and complete a safeguarding review. Do not steer. [2] [11]
- Coordinate antenatal care. A multidisciplinary team — midwifery, obstetrics, paediatrics, social work, mental health, and education liaison — delivers better outcomes than fragmented care. Arrange routine antenatal visits, screening and supplementation (folic acid, iron, iodine per local antenatal guidance). [12] [3]
- Nutrition and supplementation. Folic acid from before conception through the first trimester (higher dose in specified high-risk groups), and iron and iodine per national antenatal guidance — quote local protocol for exact doses rather than a universal number. [12]
- Mental health. Screen antenatally and postnatally for depression; treat actively; ensure crisis pathways are known. [9]
- Education, housing and finance. Plan school re-entry, link to financial and housing supports, and engage the partner and family where safe and appropriate. [10]
- Birth and postpartum. Support breastfeeding initiation (adolescent-specific interventions help), observe parent–infant interaction, manage postpartum anaemia, and build the well-child plan. [8]
- Prevent rapid repeat pregnancy. Agree a contraception plan before discharge, offering the most effective acceptable method — long-acting reversible contraception where available and chosen. [4] [5] [6]
- Follow-up and transition. Close interval review; track education re-entry; and, for adolescents with chronic disease, plan transition to adult services while sustaining parenting support. [10]
Contraception to prevent repeat pregnancy
Long-acting reversible contraception — the intrauterine device and the implant — is the most effective reversible method and the single most evidence-based lever for reducing adolescent and rapid repeat pregnancy. It does not suit everyone and must be offered, never imposed; the autonomy and consent of the young person are paramount. Where a young person declines LARC, support her chosen method and plan a clear follow-up. Post-placental IUD insertion (where available) is a high-yield strategy because the postpartum visit is so often missed. [4] [5] [11]
Follow-up intensity
- Low-risk, well-supported: routine antenatal schedule with clear safety-netting.
- New mental-health, housing or safeguarding concerns: early multidisciplinary review (days to weeks). [9]
- Obstetric or safeguarding emergency: same-day escalation as above. [2]
Specific Subtypes & Scenarios
Very young adolescent (< 15). Highest biological and safeguarding concern. Treat as presumed safeguarding-positive until assessed: clarify the partner, the consent context, and any coercion. Specialist adolescent and child-protection input is usually indicated. [2] [10]
Late or unbooked presentation. A staged rapid MDT assessment: establish gestation, run catch-up screening, and actively exclude concealed abuse or neglect. Higher complication rates justify a lower threshold for obstetric involvement. [2] [12]
Out-of-home care, youth justice, or unstable housing. Assume trauma exposure, fragmented records and incomplete immunisations. Clarify legal consent, reconstruct the history actively, and build wrap-around supports. [10]
Indigenous, migrant or refugee adolescent. Cultural safety and community partnership are part of the medicine. Use a professional interpreter (never a family member for sensitive content); apply trauma-informed pacing; and respect the role of family, community and Elders where appropriate. Female genital cutting may be relevant for some migrant patients and should be asked about sensitively. [10]
Pre-existing chronic illness, mental illness, substance use or disability. Integrate disease-specific obstetric and paediatric goals with whole-person adolescent care. Avoid diagnostic overshadowing — pregnancy does not make a chronic disease disappear, and a disability does not make parenting impossible. [2]
Planned, wanted pregnancy. Affirm the choice, provide excellent antenatal and parenting support, and still plan contraception postpartum — even wanted first pregnancies can be followed by an unwanted rapid repeat. [11]
Adolescent father or co-parent. Paternal involvement improves outcomes for mother and child when the relationship is safe; engage the young father supportively and assess for his own health, education and mental-health needs. Fathers are under-researched and under-served. [10]
Rapid repeat pregnancy. Prevent it (contraception before discharge), and when it occurs, address the drivers — not just the biology. Each repeat pregnancy compounds disadvantage. [6] [7]
The infant of an adolescent parent. Fold parenting support, developmental surveillance and the parent's health into well-child care; a delay in the infant is sometimes the first sign of a struggling parent. [8] [9]
Gender-diverse adolescent who is pregnant. Use correct name and pronouns, acknowledge the specific psychosocial complexity, and tailor care to anatomy and identity without making the patient a curiosity. [10]
Complications & Pitfalls
- Judgemental clinician stance that suppresses disclosure and drives disengagement. [10]
- Excluding parents without the adolescent's consent, or, conversely, breaching confidentiality unnecessarily. [10]
- Missing safeguarding — an older partner, coercion, trafficking, or a child below the local age of consent. [2]
- Assuming capacity without actually assessing it; capacity is decision-specific and must be checked. [10]
- Attributing abdominal pain to "normal pregnancy" and missing ectopic, miscarriage or pre-eclampsia. [2]
- Filing a positive depression screen without a same-visit suicide assessment. [9]
- Discharging postpartum without a contraception plan — the classic driver of rapid repeat pregnancy. [6] [4]
- Attributing postpartum low mood to "tiredness" and missing postnatal depression or, rarely, postpartum psychosis. [9]
- Fragmented care — paediatrics, obstetrics, mental health and education not communicating. [10]
- The two-patients trap: focusing only on the baby and losing the parent, or vice versa. [8]
Prognosis & Disposition
Prognosis here means the long-term trajectory of the young parent and the child, not a disease stage — and it is striking how modifiable it is. [10]
Better outcomes are predicted by continued education, stable housing, strong social and family support, a planned and chosen contraceptive method, treated mental ill-health, and positive family or community involvement. Where these are present, adolescent parents can and do parent well, and the intergenerational disadvantage often assumed is not inevitable. Where they are absent — isolation, school dropout, untreated depression, repeat pregnancy, ongoing violence — outcomes worsen for both parent and child. [3] [8] [9]
The disposition plan spans antenatal, postpartum and early-parenting phases and names who owns each: the obstetric team for pregnancy complications, the paediatrician for the infant and the parent's adolescent-health needs, mental health for mood, social work for housing and finance, and education liaison for re-entry. After delivery, the paediatrician has a continuing role: supporting the adolescent parent's health, the child's development, and the parent's transition toward adult services where chronic disease exists. The prognosis for rapid repeat pregnancy risk is reduced by the single act of contraception before discharge. [4] [6] [10]
Special Populations
Indigenous adolescent parents. Cultural safety, community connection, racism recognised as a health exposure, and local service partnerships matter as much as any guideline. Centre the young person's community and avoid deficit framing. [10]
Migrant and refugee adolescent parents. Professional interpreter is mandatory for sensitive content; family members are not equivalent. Apply trauma-informed care, clarify legal status where relevant, and ask sensitively about practices such as female genital cutting. [10]
Out-of-home care and youth justice. Assume incomplete records, trauma and fragmented care. Clarify legal consent carefully and reconstruct the history actively. [10]
Gender and sexual diversity. Use correct name and pronouns, tailor sexual and reproductive health to anatomy and identity, and watch for family rejection and minority stress alongside pregnancy. [10]
Intellectual disability or neurodiversity. Easy-read materials, longer appointments, capacity assessment tailored to the decision, and carer involvement that does not erase the young person's autonomy. [10]
Housing or food insecurity. Ask before blaming "non-adherence"; instability derails every plan you write. [10]
Intimate partner violence or reproductive coercion. A trained pathway, not a one-off question — and a safeguarding response when thresholds are met. [10]
Evidence, Guidelines & Regional Differences
Epidemiology: Sedgh and colleagues' cross-country analysis of adolescent pregnancy, birth and abortion rates documents substantial declines in most high-income settings alongside persistent inequities — useful for framing "why" in a viva. [1]
Outcomes: the WHO multicountry study (Ganchimeg and colleagues) is the key source for the elevated obstetric and perinatal risks in adolescents; it should be quoted for the direction of effect (anaemia, pre-eclampsia, preterm birth, low birthweight, STI) and for the social confounders that modulate it, not for memorised relative risks. Scholl and Hediger's earlier meta-analysis of prenatal care and maternal health in adolescent pregnancy underpins the nutrition and anaemia framing. [3] [12]
Contraception and prevention: Curtis and Peipert's review of long-acting reversible contraception, and Rosenthal and McQuillan's Canadian adolescent contraception guidance, anchor the LARC-first prevention argument; Borovac-Pinheiro and Surita frame the before-and-after-pregnancy contraceptive challenge. The autonomy and consent of the young person are a recurring theme — LARC must be offered, never imposed. [4] [5] [11]
Rapid repeat pregnancy: Rigsby and Macones' review of risk factors, and Ramage and colleagues' Canadian trend data, define the subtype and its predictors. [6] [7]
Breastfeeding: Sipsma and colleagues' systematic review of breastfeeding interventions for adolescent mothers in high-income countries shows that adolescent-specific support improves initiation and duration — a directly actionable finding. [8]
Mental health: Dinwiddie and Schillerstrom's review of postpartum depression in adolescent mothers confirms the elevated risk and the need for active screening. [9]
Comprehensive clinical framing: Leftwich and Alves' Pediatric Clinics review and Mann and Bateson's Australian general-practice overview provide accessible whole-pathway summaries suitable for exam preparation. [2] [10]
ANZ: youth-friendly care principles (RCH Melbourne and similar), local consent and mandatory-reporting statutes, and Medicare/pathway variation; termination access differs by state and territory. UK: NICE guidance on pregnancy with complex social factors; Gillick/Fraser capacity concepts in reproductive care for under-16s — apply with current local legal teaching; safeguarding via local children's services. US: AAP adolescent pregnancy policy, Bright Futures adolescent care, USPSTF screening statements, and state-level variation in adolescent consent and abortion access. Canada: Canadian Paediatric Society guidance, provincial consent variation, and Rosenthal/McQuillan adolescent contraception framing.
Exam Pearls
- Open every answer with non-judgement + time alone + confidentiality with lawful limits. [10]
- Confirm and date the pregnancy; exclude ectopic as your first clinical act when symptomatic. [2]
- Name the adolescent-specific obstetric risks: anaemia, pre-eclampsia, preterm birth, low birthweight, STI. [3]
- Contraception before discharge is the single highest-yield postpartum act. [4] [6]
- Screen antenatally and postnatally for depression; postpartum psychosis is an emergency. [9]
- Breastfeeding initiation and duration are lower in adolescents; adolescent-specific support works. [8]
- Mandatory safeguarding if coercion, a child below the local age of consent, trafficking, or an age/power asymmetry. [10]
- Two patients: never let the infant's care displace the parent's, or vice versa. [8]
- Support return to education and housing — these drive long-term outcome as much as the medical care. [10]
- Do not invent jurisdiction-specific consent ages or abortion law; name the principle and local statute. [10]
PREGNANT care anchors
References
- [1]Sedgh G; Finer LB Adolescent pregnancy, birth, and abortion rates across countries: levels and recent trends. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2015.PMID 25620306
- [2]Leftwich HK; Alves MV Adolescent Pregnancy. Pediatric clinics of North America, 2017.PMID 28292453
- [3]Ganchimeg T; Ota E Pregnancy and childbirth outcomes among adolescent mothers: a World Health Organization multicountry study. BJOG : an international journal of obstetrics and gynaecology, 2014.PMID 24641534
- [4]Curtis KM; Peipert JF Long-Acting Reversible Contraception. The New England journal of medicine, 2017.PMID 28146650
- [5]Rosenthal MA; McQuillan SK Adolescent contraception. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne, 2021.PMID 34373270
- [6]Rigsby DC; Macones GA Risk factors for rapid repeat pregnancy among adolescent mothers: a review of the literature. Journal of pediatric and adolescent gynecology, 1998.PMID 9704301
- [7]Ramage K; Tough S Trends in Adolescent Rapid Repeat Pregnancy in Canada. Journal of obstetrics and gynaecology Canada : JOGC = Journal d'obstetrique et gynecologie du Canada : JOGC, 2021.PMID 33309019
- [8]Sipsma HL; Jones KL Breastfeeding among adolescent mothers: a systematic review of interventions from high-income countries. Journal of human lactation : official journal of International Lactation Consultant Association, 2015.PMID 25480018
- [9]Dinwiddie KJ; Schillerstrom TL Postpartum depression in adolescent mothers. Journal of psychosomatic obstetrics and gynaecology, 2018.PMID 28574297
- [10]Mann L; Bateson D Teenage pregnancy. Australian journal of general practice, 2020.PMID 32464731
- [11]Borovac-Pinheiro A; Surita FG Adolescent Contraception Before and After Pregnancy-Choices and Challenges for the Future. Revista brasileira de ginecologia e obstetricia : revista da Federacao Brasileira de Sociedades de Ginecologia e Obstetricia, 2016.PMID 27832675
- [12]Scholl TO; Hediger ML Prenatal care and maternal health during adolescent pregnancy: a review and meta-analysis. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 1994.PMID 7811676