Paeds · adolescent-and-young-adult-medicine
Adolescent sexual health and contraception
Also known as Adolescent contraception · Youth sexual and reproductive health · LARC for adolescents · Confidential contraceptive counselling · Dual protection in youth · Teen pregnancy prevention
A fellowship approach to adolescent sexual health and contraception: confidential, youth-centred sexual history (the 5 Ps), LARC-first counselling using Medical Eligibility Criteria principles, dual protection against pregnancy and STIs, quick-starting, emergency contraception, HPV vaccination, red-flag safety action, and follow-up across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 16-year-old asks for "the pill." You write the script, never ask about partners, pressure or periods, and miss a coercive relationship and an unsafe home. Six weeks later the same young person is pregnant. The failure was not the molecule. It was a sexual health visit without youth-centred process. [6] [16]
Adolescent sexual health is the lifelong wellbeing of young people in relation to sexuality — physical, emotional and social — not merely the absence of disease or unplanned pregnancy. Contraception is one tool within that frame. The clinician's job is confidential counselling, accurate information, method provision, STI prevention and timely safety action, delivered with respect for the young person's emerging autonomy. [6]
Long-acting reversible contraception (LARC) — the intrauterine device (IUD) and the subdermal implant — is the effectiveness backbone for this age group. In the Contraceptive CHOICE Project, LARC methods had far lower failure than pills, patches or rings precisely because they remove the user from the equation. [1] [4]
Core sequence of a contraceptive consult
Private frame
Time alone and conditional confidentiality stated before any history.
5 Ps history
Partners, Practices, Protection, Past STI, Pregnancy intention — plus coercion.
Screen and rule out
Pregnancy test, STI risk, contraindications using Medical Eligibility Criteria principles.
Method counselling
Full options, LARC-first, side-effects and reversibility — the young person chooses.
Dual protection + plan
Condoms for STI, HPV vaccine, emergency contraception plan, close follow-up.
Classification
Classify by method tier (effectiveness), by visit intent, and by confidentiality frame. [6]
Method effectiveness tiers
Tiering by typical-use failure is the most useful clinical classification because it maps directly to adolescent outcomes. [1]
| Tier | Methods | Typical-use failure | Why it matters in youth |
|---|---|---|---|
| 1 · LARC | Copper IUD, hormonal IUD, subdermal implant | Less than 1% | Set-and-forget; highest continuation |
| 2 · Hormonal, user-dependent | Combined pill, patch, ring; progestin-only pill; injectable (DMPA) | Roughly 4–7% | Daily or cyclical adherence needed |
| 3 · Barrier and behavioural | Male/female condom, withdrawal, fertility-awareness | Roughly 13–21% | Highest typical-use failure; condom protects STI |
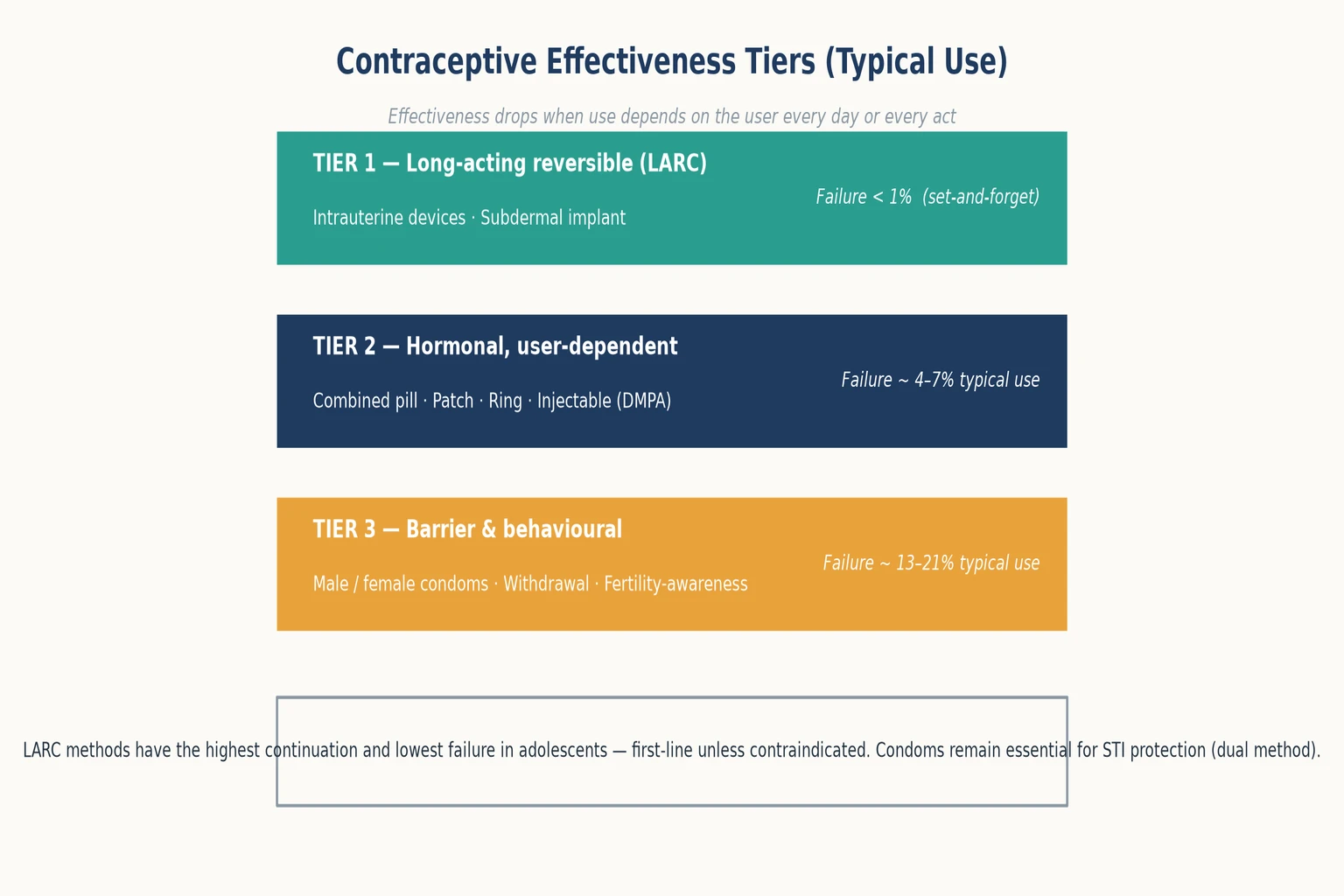
Read the figure like this: the cliff between Tier 1 and Tier 3 is the user-dependency gap. Your counselling should not pretend all methods are equal for a young person. [1]
LARC (Tier 1)
First-line
- Implant and IUD
- Lowest failure in teens
- Highest continuation
- Reversible, fertility returns quickly
Hormonal user-dependent (Tier 2)
Effective if adhered
- Pill, patch, ring, DMPA
- Needs daily/cyclical use
- Quick-start possible
- DMPA bone-density caveat
Barrier (Tier 3)
STI protection
- Condoms are the STI method
- Higher pregnancy failure
- Use as dual method
- Withdrawal is not contraception
Visit and confidentiality classification
A confidential contraceptive visit is one in which the young person can access counselling, testing and a method without a parent present, where local law supports it and the young person has the capacity to understand. Conditional confidentiality means what is said stays private unless there is a serious risk of harm, abuse or exploitation, or the law requires action. [6] [16]
Epidemiology & Risk Factors
Unintended pregnancy and sexually transmitted infections are concentrated in the second decade of life. The structural reasons are biological (cervical ectopy and adolescent fertility), behavioural (inconsistent method use), and social (barriers to confidential care). [10] [11]
The single most important modifiable risk factor for adolescent contraceptive failure is use of a user-dependent method when a LARC would have suited. When CHOICE removed cost and access barriers and counselled LARC-first, the great majority of adolescents chose a LARC method. [2] [4]
Risk amplifiers cluster together: poverty, rural isolation and transport barriers; cost and insurance that expose sensitive content to parents; lack of confidential adolescent services; coercive or much-older partners; out-of-home care and youth justice with fragmented records; cognitive or communication disability that limits self-advocacy; and clinician myths that adolescents "cannot" use IUDs. [6] [5] [16]
Chlamydia and gonorrhhea burden is highest in sexually active young women under 25, which is why universal screening in that group is recommended where guidelines apply. [10] [11]
Pathophysiology
A workable mechanism model explains why adolescents fail user-dependent methods even when they understand the risk. [6]
Brain development pairs high reward sensitivity with still-maturing planning and impulse control. Memory for daily pills and motivation for each-act protection compete with sleep, school and peer context. Counselling that ignores the biology of planning will under-deliver. [6]
Fertility arrives before readiness to manage it. Ovulation and cervical ectopy make adolescents both highly fertile and more susceptible to ascending STI. The method must therefore be forgiving of imperfect use — which is the LARC argument. [1]
Access and confidentiality barriers are themselves mechanisms of harm. When a young person expects a parent, a portal message or a bill to reveal the visit, they delay or avoid care, request less effective methods, or skip STI testing. [16]
The user-dependency gap is the measurable distance between perfect-use and typical-use effectiveness. Pills, patches and condoms look excellent in perfect use and fail often in real life. LARC collapses that gap to near zero because there is nothing for the user to remember. [1] [3]
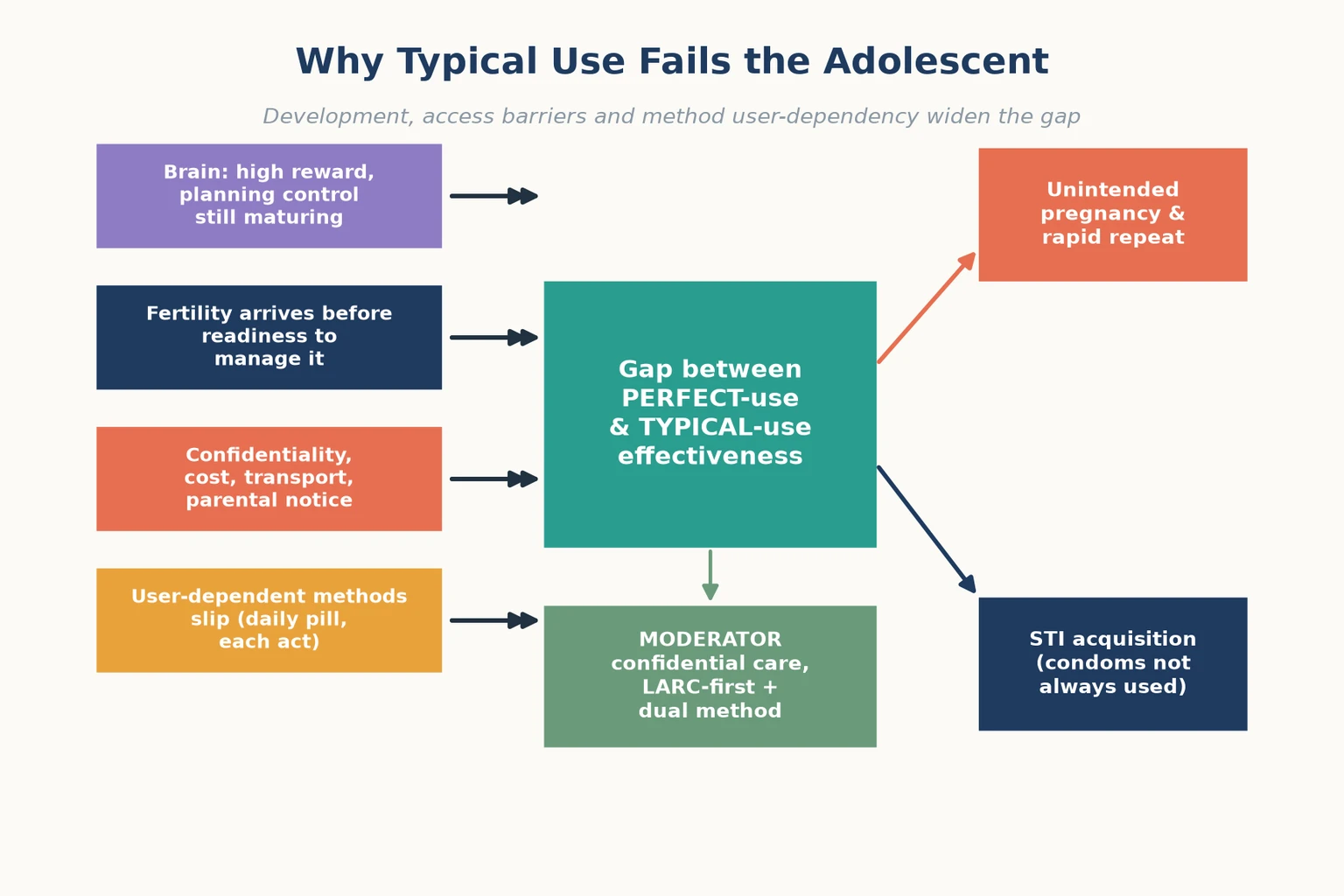
Read the figure like this: the green moderator is where your clinical effort lands. You cannot accelerate brain maturation, but you can remove the user-dependency gap with a LARC and protect confidentiality. [1]
Clinical Presentation
A young person may present with a direct request ("I want contraception"), an indirect request ("my periods are irregular"), or an unrelated complaint where sexual health need is hidden. The skilled clinician looks for all three. [6]
Organised contraceptive visit: private time secured, conditional confidentiality stated, 5 Ps history taken, pregnancy ruled out, contraindications checked, method chosen, dual protection agreed, follow-up planned. [6] [7]
High-risk patterns that hide inside ordinary visits: a parent who will not leave the room; a much-older or controlling partner; requests for emergency contraception after a single event ( signalling no regular method ); irregular bleeding in a young person on no method; dysuria, discharge or pelvic pain in a sexually active teen; and a young person who is sexually active but has never been offered screening. [10] [8] [6]
Differential Diagnosis
In sexual health the "differential" is less about naming one disease and more about naming which driver is active and which needs to be addressed first. [6]
| What it looks like | Safer framing question | Do not miss |
|---|---|---|
| Irregular bleeding on no method | Pregnancy, STI, or underlying cycle disorder? | Ectopic pregnancy, cervicitis |
| Request for emergency contraception | Why no regular method? Barrier to access or coercion? | Coercive partner, sexual assault |
| Pelvic/lower abdominal pain | Cervicitis, PID, pregnancy, torsion? | Ectopic, PID, abuse |
| Heavy or painful periods | Is this contraception seeking disguised as a menstrual complaint? | Bleeding disorder, dysmenorrhoea |
| "I'm not sexually active" | Ask again in private — disclosure needs trust and time | Hidden risk from earlier assumption |
Separate a contraception problem (method choice, side-effects, adherence) from an infection problem (screening, symptoms, partner notification) from a safety problem (coercion, assault, capacity). They coexist and each needs its own plan. [6]
Clinical & Bedside Assessment
1. Open in private and set the confidentiality frame
Greet the young person first. Explain that some time will be spent alone. State conditional confidentiality aloud: what you discuss privately stays private unless there is a serious risk of harm to them or others, abuse or exploitation, or a legal duty to act. Check their understanding. [6] [16]
2. Take the 5 Ps sexual history
Work through the 5 Ps with open then focused questions. Partners — who, gender(s), number, and whether the relationship feels safe and equal. Practices — vaginal, oral, anal — so you test the right sites. Protection — from both STI and pregnancy, and whether protection was the young person's choice. Past STI history — previous infections, treatments, partner notification. Pregnancy intention — desire, last menstrual period, and any chance of pregnancy now. Then ask directly about coercion, which is not optional. [6] [10]
3. Tailor the method conversation to the person
Present methods by effectiveness tier, leading with LARC, and describe side-effects, bleeding changes and reversibility honestly. Use Medical Eligibility Criteria principles to match method to medical conditions rather than excluding whole categories by habit. The young person chooses; you support. [6] [7]
4. Examine only what the history demands
A method visit rarely needs a pelvic exam. Offer chaperones for any sensitive examination, and match genital examination to a clear indication (symptoms, STI testing) rather than routine. [6]
5. Screen and test by risk and anatomy
Offer chlamydia and gonorrhoea testing to sexually active young women under 25 and to any young person by risk, testing the sites that match the practices disclosed. Confirm HPV vaccination status. Offer a pregnancy test if any chance of pregnancy exists, including before starting a method. [10] [11]
6. Document with discretion
Record enough for safety and continuity while protecting sensitive detail according to local medical-record, portal and billing rules. A leaked portal message or itemised bill is a modern confidentiality failure that can stop a young person returning. [16]
Investigations
Most contraceptive visits need few routine laboratory tests. Investigation is selective and history-led. [6] [7]
Often indicated: a urine pregnancy test before starting any hormonal method or IUD if pregnancy cannot be reasonably excluded; chlamydia and gonorrhoea NAAT from the sites that match disclosed practices; HIV and syphilis testing by risk; and a baseline blood pressure with review of personal and family history for oestrogen contraindications. [10] [6]
Not routinely required before LARC: a cervical screening test, a pelvic exam, or extensive laboratory panels in an asymptomatic young person — Medical Eligibility Criteria principles support LARC provision without these barriers. [7] [5]
Low-value patterns: withholding an IUD or implant for an unmet STI screen when treatment can proceed in parallel; repeating STI panels without indication; or demanding a pap test before contraception in a young person below screening age. [7]
Management — Resuscitation
A contraceptive consult can become a safeguarding or medical emergency in one disclosure. Recognise the pivot and act before returning to method counselling. [6]
- Stabilise physiology if a medical emergency exists: possible ectopic pregnancy, severe pelvic infection, suspected thromboembolism, or haemodynamic instability. [10]
- Secure immediate safety after a coercion or assault disclosure: do not let the young person leave with a dangerous partner, involve local sexual-assault and safeguarding pathways, and preserve forensic options where relevant. [6]
- Address pregnancy now if the test is positive: offer non-directive options counselling and exclude ectopic before any method is started. [8]
- Honour confidentiality limits: tell the young person what you must share and why, share the minimum necessary, and document decisions and who was informed. [6] [16]
Management — Definitive & Stepwise
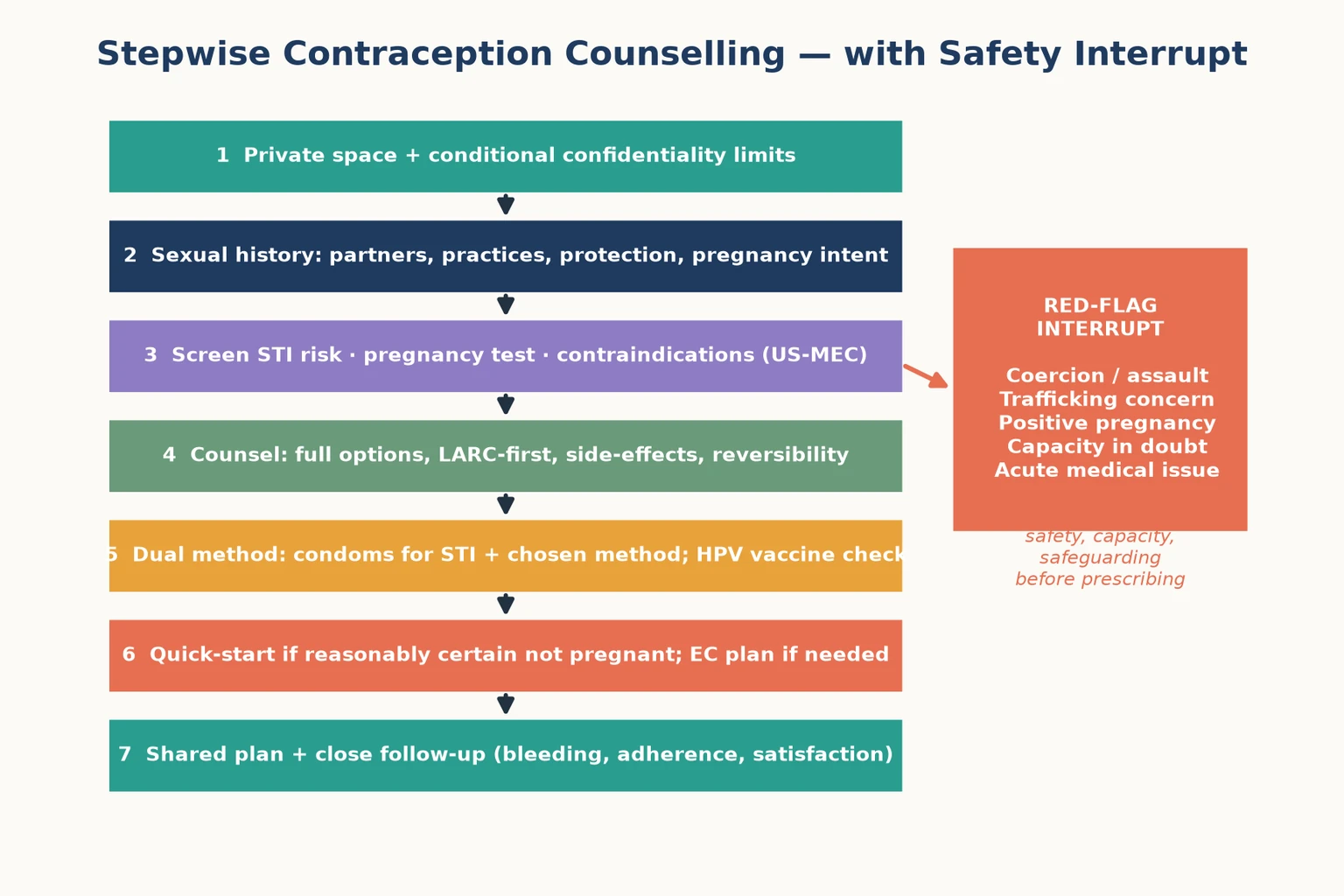
Read the figure like this: the red box is a branch, not decoration. A positive pregnancy test or an assault disclosure exits the routine method pathway. [6]
Stepwise routine pathway
- Private frame and conditional confidentiality before any history. [6]
- 5 Ps sexual history, including a direct question about coercion. [6]
- Screen and rule out pregnancy and contraindications using Medical Eligibility Criteria principles. [7]
- Counsel all methods, LARC-first, with honest side-effects and reversibility information; the young person chooses. [1] [6]
- Dual method: the chosen method plus condoms for STI protection, because no hormonal or intrauterine method prevents infection. [14] [15]
- Quick-start the method if you are reasonably certain the young person is not pregnant, and provide an emergency contraception plan for method failures or unprotected sex. [8] [9]
- Shared plan and close follow-up for bleeding, side-effects, satisfaction and method continuation. [3] [5]
Emergency contraception — principle only
Dose
Refer to current local protocol and product information for the regimen in your jurisdiction
Continuation is the outcome
Continuation rates are higher with LARC than with user-dependent methods in adolescents and young women, which is why method choice should privilege methods the young person can sustain. Early follow-up for bleeding or side-effects prevents abandonment. [3] [5]
Specific Subtypes & Scenarios
Early adolescent, parent in the room. Build private time and use short, concrete questions. Address the parent's agenda (safety, periods, vaccines) in parallel while securing confidential one-to-one time. [6]
Emergency contraception presentation. A request for emergency contraception is an opportunity to start a regular method. Offer quick-start of an ongoing method alongside emergency contraception, screen for STI if relevant, and ask about coercion. [8] [9]
ED or inpatient opportunity. A young person admitted for any reason may never have had a confidential sexual health visit. A focused history, STI screen and method discussion can change long-term outcomes. [10] [6]
Post-abortion or post-pregnancy. Fertility returns immediately; offer LARC before discharge, as rapid repeat pregnancy is a major risk. [4]
Gender-diverse and sexual-minority youth. Tailor anatomy-based language and STI testing to practices, affirm identity, and watch for minority stress and family rejection. A testosterone-taking youth with a uterus still needs contraceptive and pregnancy-prevention counselling. [6]
Disability and neurodiversity. Use accessible language, longer appointments, capacity assessment and chaperones. Private time may still be possible with support; never assume a young person with a disability is not sexually active. [6]
The pregnant adolescent. Provide non-directive options counselling, exclude ectopic, and arrange the chosen pathway with continuity. Contraception planning belongs in the same visit. [8]
Complications & Pitfalls
- Treating "the pill" as a transaction and skipping the 5 Ps. [6]
- Assuming adolescents cannot or should not use IUDs — an outdated myth that Medical Eligibility Criteria principles do not support. [7] [5]
- Prescribing a user-dependent method by default when a LARC would better match the young person's life. [1]
- Offering contraception without dual protection, leaving the STI risk unaddressed. [14] [15]
- Delaying emergency contraception out of gatekeeping rather than effectiveness logic — earlier is more effective. [9]
- Forgetting DMPA and bone mineral density: use is acceptable, but counsel and review, particularly with long duration in adolescence. [13]
- Leaking sensitive content through portals, itemised bills or parent-addressed letters. [16]
- Missing pregnancy before starting a method, or ectopic in a symptomatic young person. [8]
Prognosis & Disposition
Prognosis in this topic means continuation, avoidance of unintended pregnancy and STI, and sustained engagement with care, not a single disease course. [4]
Routine disposition: method started or continued, dual protection agreed, screening complete, follow-up booked. Early review disposition: new side-effects, bleeding concern, method dissatisfaction, a positive STI result needing treatment and partner notification, or an emergency contraception event needing a regular method. Urgent disposition: positive pregnancy needing options, ectopic, pelvic infection, coercion or assault — escalate to safeguarding, sexual-assault services or emergency care. [6] [10] [8]
Close the loop after referral to sexual health, psychology or social work, and name the next concrete contact so a young person is not lost between services. [16]
Special Populations
Indigenous adolescents. Deliver culturally safe care, address racism as a health exposure, connect to community-controlled services, and respect that sexual health sits within kinship and cultural context. [6]
Migrant and refugee youth. Use professional interpreters (never family members) for confidential content; offer catch-up HPV vaccination; and apply trauma-informed pacing. [6]
Out-of-home care and youth justice. Assume fragmented records, higher STI and pregnancy risk, and consent complexity. Reconstruct history actively and clarify legal consent for the placement context. [6]
Gender and sexual diversity. Affirm identity, tailor contraception and STI testing to anatomy and practices, and screen for bullying and family rejection. [6]
Disability and neurodiversity. Use accessible materials, assess capacity properly, and offer the full method range — do not let diagnostic overshadowing deny contraceptive choice. [6]
Socioeconomic disadvantage and rural youth. Address cost, transport and digital access before labelling a method "non-adherent"; telehealth can help if a confidential private audio space is created. [16]
Evidence, Guidelines & Regional Differences
LARC effectiveness and adolescent acceptance. Winner and colleagues showed LARC methods had substantially lower failure than short-acting methods, driven by the user-dependency gap. The CHOICE Project demonstrated that when cost and counselling barriers were removed, most adolescents chose and accepted LARC, and the programme reduced unintended pregnancy and abortion at population scale. [1] [2] [4]
Continuation evidence. A systematic review of intrauterine contraception continuation in adolescents and young women supports IUD use in this group with good continuation, countering clinician myths. Early discontinuation of LARC within six months is associated with identifiable, addressable factors such as bleeding and dissatisfaction, which close follow-up can intercept. [5] [3]
Method eligibility and counselling standards. The CDC U.S. Medical Eligibility Criteria for Contraceptive Use, 2016 (and updates) classify method safety by medical condition into categories, supporting LARC and most methods for adolescents. ACOG Committee Opinion 710 frames counselling adolescents about contraception as a confidential, full-options, LARC-inclusive conversation. [7] [6]
STI screening. The USPSTF recommends screening sexually active women 24 years and younger for chlamydia and gonorrhoea, supported by an updated evidence report and systematic review. Screening of men and older adults is by risk. [10] [11]
Dual protection and dual method. Dual-method research in adolescents and young adults shows that adding condoms to a pregnancy-prevention method is the practical route to reducing both pregnancy and STI, while highlighting the negotiation challenges young people face. [14] [15]
Emergency contraception. Reviews of emergency contraception for adolescents and of its current state confirm that earlier administration is more effective, that ulipristal acetate extends the window relative to levonorgestrel, and that a copper IUD is the most effective option. [8] [9]
HPV vaccination. A Swedish population study found HPV vaccination substantially reduced the risk of invasive cervical cancer, reinforcing vaccination as part of adolescent sexual health. [12]
DMPA and bone. DMPA use is associated with lower bone mineral density in adolescent women; gains largely recover after discontinuation, but counselling and periodic review are appropriate for prolonged use. [13]
Confidentiality and access. Research on minors' experiences accessing confidential contraception shows that perceived and actual barriers — parental notification, cost and logistics — shape whether a young person obtains effective care at all. [16]
ANZ: youth-friendly services, confidential contraceptive provision supported by local consent statutes (e.g. "mature minor"/Gillick-equivalent principles), school-based immunisation for HPV, and RCH-linked adolescent pathways. UK: FSRH and NICE contraceptive guidance; Gillick/Fraser competence underpins a competent young person's capacity to consent to contraception confidentially. US: CDC U.S. Medical Eligibility Criteria, ACOG Committee Opinion 710, USPSTF STI screening; open-notes and insurance confidentiality create distinct portal and billing challenges. Canada: Canadian contraception guidance and CPS-aligned resources; provincial consent ages vary, so state the principle and check local law.
Exam Pearls
- Open every answer with private space + conditional confidentiality limits before any sexual history. [6] [16]
- Name the 5 Ps: Partners, Practices, Protection, Past STI, Pregnancy intention — and add coercion. [6]
- LARC is first-line for adolescents because typical-use failure is lowest and continuation is highest. [1] [2]
- IUDs are not contraindicated by age or nulliparity — Medical Eligibility Criteria principles, not myths, guide choice. [7] [5]
- Dual method: condoms for STI plus the chosen method for pregnancy. [14] [15]
- Emergency contraception: earlier is better; ulipristal extends the window; copper IUD is most effective. [8] [9]
- Sexually active young women under 25 get chlamydia and gonorrhoea screening. [10]
- Confirm HPV vaccination status at every adolescent visit. [12]
- DMPA and bone mineral density: counsel and review, do not ban outright. [13]
- A portal, bill or parent letter can leak confidentiality and stop a young person returning. [16]
CONTRACEPT framework
References
- [1]Winner B, Peipert JF, Zhao Q, Buckel C, Madden T, Allsworth JE, Secura GM Effectiveness of long-acting reversible contraception. N Engl J Med, 2012.PMID 22621627
- [2]Mestad R, Secura G, Allsworth JE, Madden T, Zhao Q, Peipert JF Acceptance of long-acting reversible contraceptive methods by adolescent participants in the Contraceptive CHOICE Project. Contraception, 2011.PMID 22018123
- [3]Grunloh DS, Casner T, Secura GM, Peipert JF, Madden T Characteristics associated with discontinuation of long-acting reversible contraception within the first 6 months of use. Obstet Gynecol, 2013.PMID 24201685
- [4]Birgisson NE, Zhao Q, Secura GM, Madden T, Peipert JF Preventing Unintended Pregnancy: The Contraceptive CHOICE Project in Review. J Womens Health (Larchmt), 2015.PMID 25825986
- [5]Usinger KM, Gola SB, Weis M, Smaldone A Intrauterine Contraception Continuation in Adolescents and Young Women: A Systematic Review. J Pediatr Adolesc Gynecol, 2016.PMID 27386754
- [6]American College of Obstetricians and Gynecologists Committee Opinion No. 710: Counseling Adolescents About Contraception. Obstet Gynecol, 2017.PMID 28742675
- [7]Tepper NK, Krashin JW, Curtis KM, Cox S, Whiteman MK Update to CDC's U.S. Medical Eligibility Criteria for Contraceptive Use, 2016: Revised Recommendations for the Use of Hormonal Contraception Among Women at High Risk for HIV Infection. MMWR Morb Mortal Wkly Rep, 2017.PMID 28934178
- [8]Rome ES, Issac V Sometimes You Do Get a Second Chance: Emergency Contraception for Adolescents. Pediatr Clin North Am, 2017.PMID 28292452
- [9]Haeger KO, Lamme J, Cleland K State of emergency contraception in the U.S., 2018. Contracept Reprod Med, 2018.PMID 30202545
- [10]US Preventive Services Task Force Screening for Chlamydia and Gonorrhea: US Preventive Services Task Force Recommendation Statement. JAMA, 2021.PMID 34519796
- [11]Cantor A, Dana T, Griffin JC, Nelson HD, Weeks C, Winthrop KL, Chou R Screening for Chlamydial and Gonococcal Infections: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA, 2021.PMID 34519797
- [12]Lei J, Ploner A, Elfström KM, Wang J, Roth A, Fang F, Sundström K, Dillner J, Sparén P HPV Vaccination and the Risk of Invasive Cervical Cancer. N Engl J Med, 2020.PMID 32997908
- [13]Busen NH Bone mineral density in adolescent women using depot medroxyprogesterone acetate. J Am Acad Nurse Pract, 2004.PMID 15055422
- [14]Hood JE, Hogben M, Chartier M, Bolan G, Bauer H Dual contraceptive use among adolescents and young adults: correlates and implications for condom use and sexually transmitted infection outcomes. J Fam Plann Reprod Health Care, 2014.PMID 24293508
- [15]Carter MW, Hock-Long L, Kraft JM, Henry-Moss D, Hatfield-Timajchy K, Singer M Strategies for managing the dual risk of sexually transmitted infections and unintended pregnancy among Puerto Rican and African American young adults. Am J Public Health, 2012.PMID 22390507
- [16]Whitfield B, Vizcarra E, Dane'el A, Palomares L, D'Amore G, Maslowsky J, White K Minors' Experiences Accessing Confidential Contraception in Texas. J Adolesc Health, 2023.PMID 36604208