Paeds · adolescent-and-young-adult-medicine
Adolescent substance-use screening, brief intervention and harm reduction
Also known as Adolescent SBIRT · Youth substance-use screening · CRAFFT and S2BI screening · Brief intervention for adolescent substance use · Adolescent harm reduction · Motivational interviewing for youth substance use
A fellowship approach to adolescent substance-use screening, brief intervention and harm reduction: universal frequency-based screening (S2BI/CRAFFT), motivational-interviewing brief intervention, a domain-specific harm-reduction bundle (naloxone, needle–syringe linkage, vaping cut-down), and the fentanyl-era safety response across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A registrar sees a 15-year-old who vapes "just socially." The screen is skipped, mood is "fine," and the visit closes in eight minutes. Three months later the same teenager is in resus after a fentanyl overdose from a counterfeit pill they never knew was an opioid. The missed work was not a rare diagnosis. It was a screen nobody ran, and a plan that demanded abstinence the young person could not yet give. [1] [8]
Substance-use screening, brief intervention and harm reduction is the clinical workflow that closes that gap. SBIRT (Screening, Brief Intervention, and Referral to Treatment) is the AAP-endorsed structure: screen every adolescent universally, deliver a brief intervention when risk is present, and refer indicated cases to treatment. Harm reduction is the pragmatic stance that lowers the adverse consequences of use even when the use continues, keeping young people alive and engaged enough to take the next step. [1] [7]
The skill is the marriage of the two. Screen thoroughly with validated tools. Meet the young person at their readiness with a brief intervention that evokes rather than imposes change. Then lower the consequences today — naloxone, needle–syringe access, a vaping cut-down, means restriction — while keeping the door open for bigger change later. The goal is any positive change, not perfection. [1] [10]
The SBIRT + harm-reduction sequence
Engage
Greet the young person first, secure time alone, state conditional confidentiality with its limits, adopt a non-judgemental stance.
Screen
Universal frequency-based S2BI for every adolescent; CRAFFT as the deeper/back-up screen; pair with mood/suicide and sexual-health inquiry.
Assess if positive
Structured detail on pattern, frequency, function, harm, dependence, co-occurring mood or trauma, and fentanyl exposure risk.
Brief intervention
Motivational interviewing — evoke own reasons for change; give personalised feedback; explore readiness.
Harm-reduction bundle
Domain-specific: naloxone, needle–syringe linkage, vaping cut-down/varenicline, cannabis frequency reduction, BBV testing, means restriction.
Referral + follow-up
Refer indicated cases to treatment; safety plan; low-threshold re-access; timed review; build transition.
Classification
Classify substance-use risk by substance class, screening intensity, and risk tier. The substance tells you what to ask; the intensity tells you how deep to go; the tier tells you how to respond. [1] [3]
Substance classes in adolescence
The substances that matter most in adolescent practice are alcohol, cannabis, nicotine/vaping products, prescription and illicit opioids, and stimulants (including counterfeit pills). Each has a distinct harm profile, a distinct escalation pattern, and a distinct harm-reduction option. A visit that asks only about "drugs" has not screened. [1] [10]
Screening intensity: universal → selective → indicated
Universal screening means asking every adolescent about substance-use frequency with a validated tool — this is the S2BI model, tiered by past-year use frequency. Selective screening adds a deeper instrument (CRAFFT) when a positive lead or risk amplifier appears. Indicated assessment is the formal, structured evaluation after a positive screen — pattern, dependence features, co-occurring disorders, fentanyl exposure. You move right only when the history pushes you there. [1] [3] [4]
Risk tiers and readiness
Risk is not binary. Stratify into low (no use or rare use, function preserved), moderate (regular use present, function preserved, no dependence), and high (impairment, danger, dependence, overdose history, or instability). Pair the tier with the young person's stage of change, because the right intervention for a precontemplative vaper is not the right one for someone asking to quit. [5] [10]
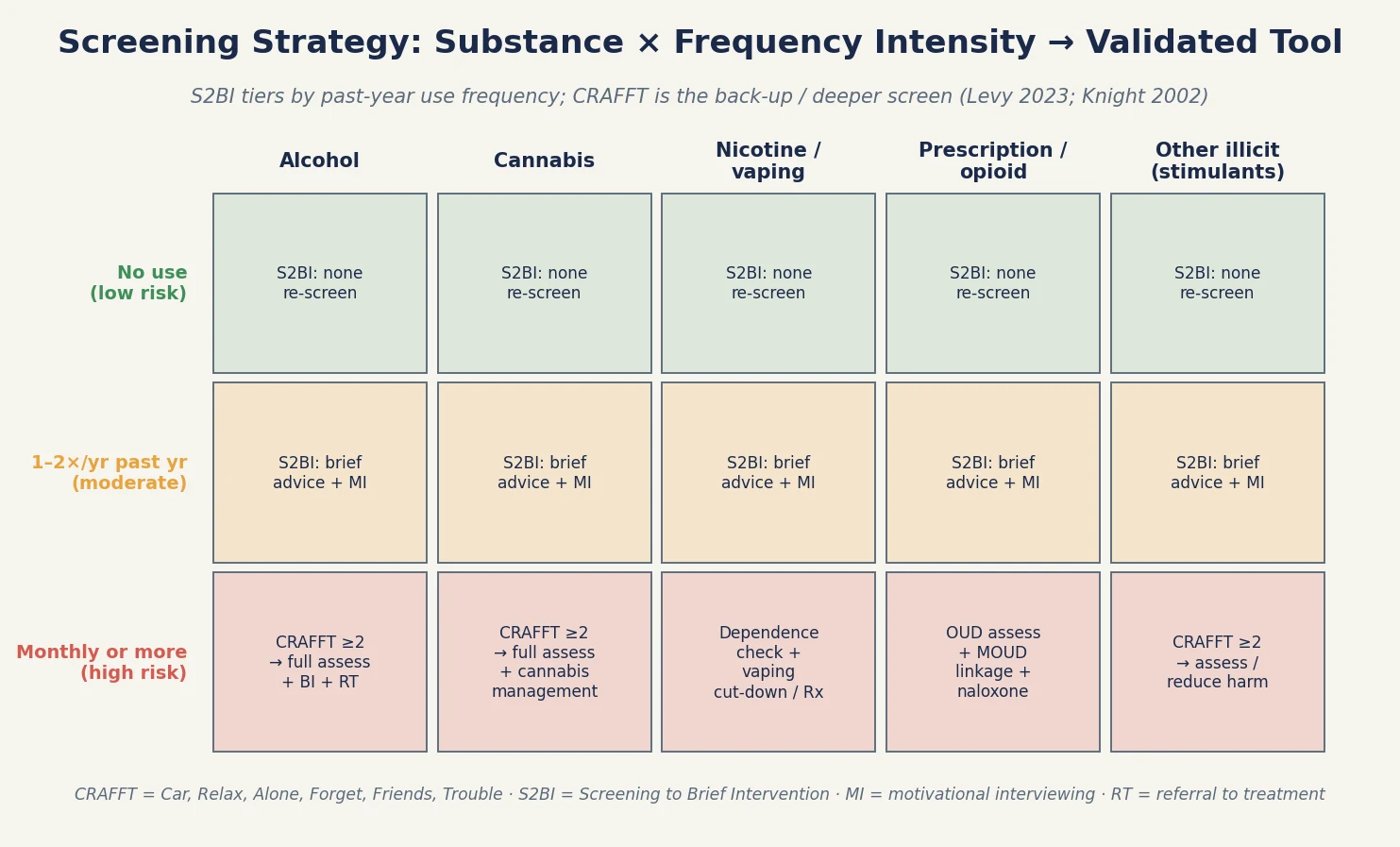
Read the figure like this: if every adolescent gets a universal S2BI but nobody ever moves into the selective or indicated column when a positive lead appears, screening is theatre. Positive leads must trigger the next instrument and same-visit clinical action. [1]
S2BI
Frequency screen
- Past-year frequency for each substance
- Tiers into no-use / brief-advice / full-assess
- Fast, free, universal at every visit
- Validated for alcohol, cannabis, vaping
CRAFFT
Deeper screen
- Car, Relax, Alone, Forget, Friends, Trouble
- Detects use-related risk and problems
- Validated in adolescent clinic populations
- Use when S2BI positive or as standalone
Urine drug screen
Limited role
- Not for routine screening
- Consent-governed, never punitive
- False positives/negatives common
- Risk erodes trust if used coercively
Epidemiology & Risk Factors
Substance use is a leading driver of adolescent morbidity and mortality across high-income settings. Alcohol contributes to injury and trauma; cannabis to psychiatric and educational harm, especially with early and heavy use; nicotine vaping to dependence and lung injury; and the fentanyl era has made opioid overdose a leading cause of adolescent death in North America. [10] [15]
Risk is not evenly distributed. Poverty, housing instability, family rejection, out-of-home care, youth-justice involvement, and refugee or migrant status all amplify exposure and reduce access to confidential care. LGBTQ+ minority stress and neurodiversity add further risk that is often missed through diagnostic overshadowing. Early initiation (before 14–15 years) and a family history of substance-use disorder raise the probability of progression to a use disorder. [7] [11]
The fentanyl era has changed the overdose picture fundamentally. A young person who believes they are taking a pill, powder, or even a non-opioid substance may be exposed to a potent opioid they never chose. Counterfeit pills, cross-contamination of stimulants, and variable potency make naloxone availability and overdose education a routine harm-reduction conversation, not a fringe one reserved for known opioid users. [8] [7]
Vaping is now the most common form of adolescent nicotine exposure in many countries. Most vaping begins without intent to use nicotine (mislabeled products), dependence develops quickly, and e-cigarette or vaping product use–associated lung injury (EVALI) demonstrated that the devices carry acute pulmonary harm beyond dependence alone. [15] [12]
Pathophysiology
You do not need a neuroscience lecture to counsel well. You do need a usable model of why adolescents take substance risks, because it explains why harm reduction works and why abstinence-only messaging often fails. [10]
The dual-systems model describes two developmental curves. The reward and socio-emotional system, anchored in limbic circuitry, matures early and peaks through mid-adolescence. The cognitive-control system, anchored in the prefrontal cortex, matures later, continuing into the mid-twenties. The gap between them is the window of heightened risk-taking, especially under peer presence and emotional arousal. [10]
This matters clinically. Under affective and social load, an adolescent may genuinely intend not to use, and still use. Counselling that treats a broken promise as a moral failure ignores the biology and disengages the young person. Counselling that reduces access to means, delays initiation, builds skills, and lowers consequences works with the biology rather than against it. [10] [7]
Harm reduction fits the neuroscience precisely. Where a young person is not ready to stop, lowering the consequences — naloxone for overdose, needle–syringe access for injecting use, a cut-down plan for vaping, restricted access to lethal means during intoxication — keeps them alive and in contact long enough for the control system to mature and for bigger change to become possible. [7] [8]
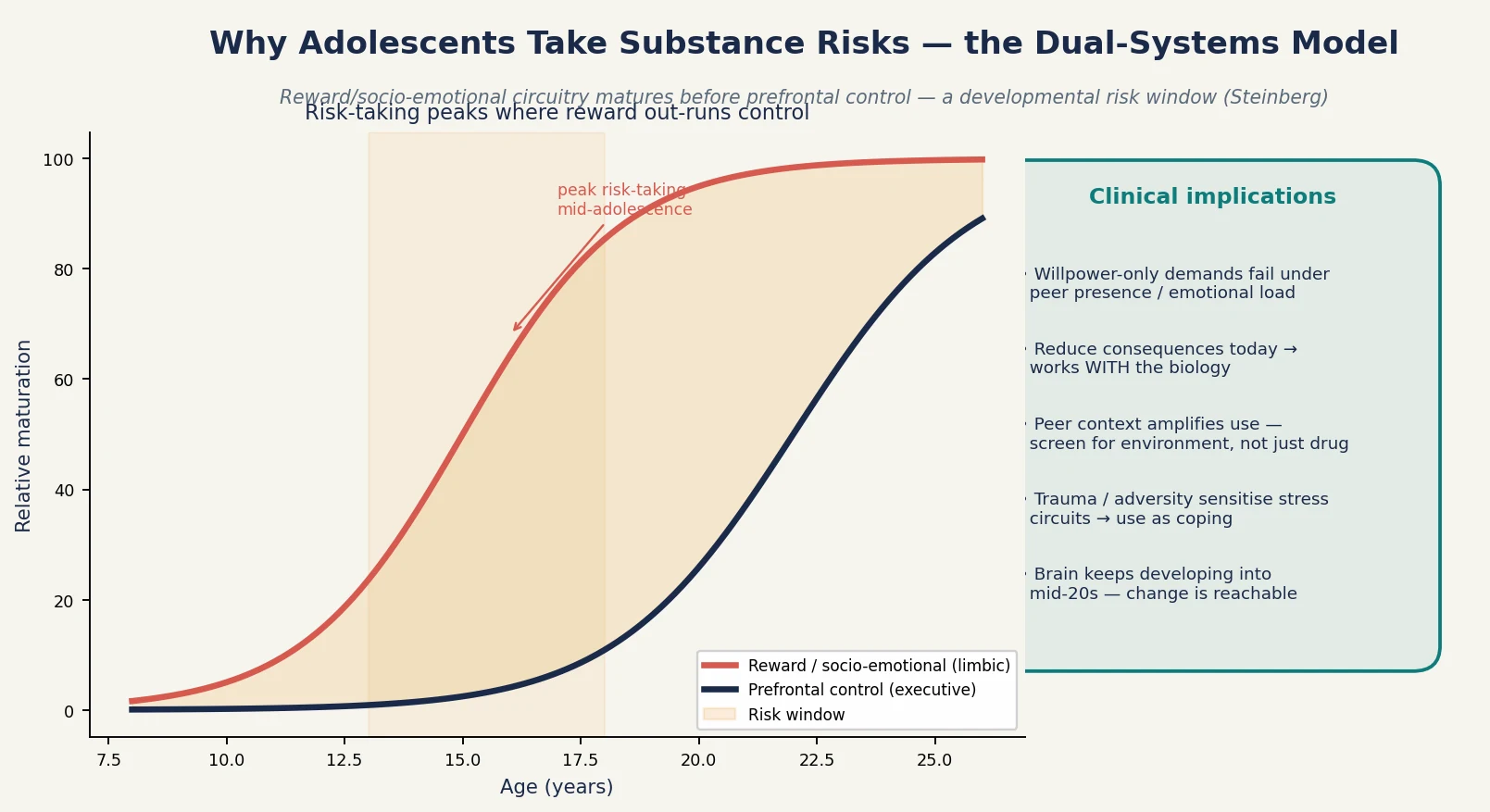
Read the figure like this: the shaded gap between the two curves is not a character flaw. It is a developmental fact. Your job is to narrow the harm inside that gap, not to lecture it shut. [10]
Clinical Presentation
Substance-use risk presents across a spectrum, from openly disclosed to completely hidden. The most dangerous presentations are often the quiet ones, because nobody asked and nobody screened. [1]
Low-risk presentation: the young person engages, private time is secured, the S2BI returns "no use" or rare past-year use, function is intact, and the only finding is normative exploration. The task is brief reinforcement, psychoeducation, and a safety net. [1] [14]
High-risk patterns hiding inside ordinary visits: the parent who answers every question; recurrent somatic complaints with school decline; sleep reversal dismissed as attitude; weight loss or food-rule changes; "social" vaping that is daily; a confidential request for STI testing; an older teen who acquired counterfeit pills from a peer. Each is a door into a substance-use domain that needs assessment, not closure. [11] [2]
Acute risk presentations arrive in ED or crisis: overdose or suspected fentanyl exposure with reduced consciousness, self-harm with substance involvement, intoxication with injury or danger, or a positive suicide screen disclosed during a substance-use history. These exit the routine pathway immediately and enter resuscitation and safety care. [8] [7]
Differential Diagnosis
In substance-use assessment the differential is less "which disease" and more "what is driving the use, is there a co-occurring disorder, and is it dangerous." [10]
| What it looks like | Safer framing question | Do not miss |
|---|---|---|
| "Recreational" vaping | Frequency, dependence, nicotine withdrawal | Escalation to other substances; co-occurring mood disorder; EVALI |
| Cannabis "just on weekends" | Frequency, potency, age of initiation | Cannabis-use disorder; emerging psychosis; motivational/amotivational decline |
| Binge drinking | Frequency, context, impaired driving | Fentanyl exposure in counterfeit pills or contaminated supply |
| Prescription-pill sharing | Source, opioid content, route, dependence | Opioid-use disorder; overdose risk; transition to injecting |
| Sedation / reduced consciousness | Opioid exposure, fentanyl, co-ingestants | Overdose requiring naloxone reversal and airway support |
The core discriminator is function and danger: does the use sit alongside intact home, school, and peer function, or is it accompanied by impairment, dependence features, overdose history, or instability? Normative experimentation does not need treatment. Impairment, dependence, and danger do. [10] [13]
CRAFFT — the six deeper-screen items
Clinical & Bedside Assessment
Substance-use assessment is history- and screen-led, not laboratory-led. The encounter's quality hinges on the opening thirty seconds: greet the young person first, set a joint agenda, secure time alone, and state conditional confidentiality with its limits before any substance question. [1] [11]
The opening frame
State the frame explicitly: "I ask all my teenage patients about substances, and what you tell me stays between us unless I'm worried you're in serious danger." This is conditional confidentiality — confidential unless serious harm to self or others, abuse or exploitation, or a legal mandate overrides it. Name the limits up front so a later override is not a betrayal. [1]
Running the screen
Administer a validated screen to every adolescent. S2BI asks past-year frequency of use (never, 1–2 times, monthly or more) for each substance class and tiers the response. CRAFFT is the deeper screen used when S2BI is positive or as a standalone — its six items detect use-related risk and problems. Follow every positive lead with focused questions on pattern, context, function, dependence features, and harm. [2] [3] [4]
Pairing the substance screen
Substance use rarely travels alone. Pair the substance screen with a mood/suicide screen and a sexual-health history, because intoxication, low mood, and sexual risk cluster. Ask about coercion and exploitation separately from "risk-taking behaviour" — they are not the same and the framing changes everything. [7] [11]
Structured assessment after a positive screen
A positive screen triggers a structured same-visit assessment: substance(s), frequency, route, age of initiation, dependence features (tolerance, withdrawal, loss of control, continued use despite harm), co-occurring mood or trauma, fentanyl-exposure risk, overdose history, and access to means. Build a risk formulation that names drivers, protective factors, and a risk tier. [1] [10]
Investigations
Risk assessment is primarily history- and screen-led. Laboratory testing is selective, consent-governed, and never a substitute for the interview. [1]
When investigations help
Pregnancy testing and STI testing to disclosed sites are indicated when sexual risk is present. Blood-borne-virus testing (hepatitis B and C, HIV) and hepatitis B vaccination status review are indicated for injecting use or mucosal exposure. A glucose level and paracetamol/salicylate levels may guide overdose management. [7] [9]
The limited, consent-governed role of urine drug screening
Urine drug screening has a narrow, consent-governed role — it is not a screening tool for asymptomatic adolescents. It detects a limited and time-limited set of substances, produces false positives and false negatives, and used punitively it erodes trust and suppresses future disclosure. Use it only when the result will change acute management, with informed consent, and document the reasoning. [1] [11]
Validated instruments function as triggers, not diagnoses
Validated screens (S2BI, CRAFFT) are triggers for clinical thinking, not diagnoses. A positive screen is a prompt to assess, not a label. Distinguish screening (population-level, brief) from assessment (individual, structured) from diagnosis (criteria-based, by a clinician). [2] [3]
S2BI performance (Levy 2023 — JAMA Network Open)
Population: Adolescents in primary care, assessed against DSM-5 substance use disorders
Key finding
Frequency-based S2BI screening identifies most adolescents with substance use disorders while keeping false positives low; the no-use tier reliably excludes disorder.
Practice change
Universal frequency screening is feasible and valid in routine adolescent primary care; positive tiers warrant a brief intervention or deeper assessment.
Management — Resuscitation
Acute-safety findings exit the SBIRT pathway immediately and enter resuscitation and safety care. The principles are airway, breathing, circulation, glucose, and specific reversal. [8] [7]
Opioid toxicity and the fentanyl era
Suspected opioid overdose presents with reduced consciousness, miosis, and respiratory depression. Reversal is with naloxone — a μ-opioid receptor antagonist. In the fentanyl era, be prepared for rapid re-sedation because fentanyl's duration exceeds naloxone's; titrate to adequate breathing (not full alertness), provide airway and ventilatory support, and observe for an extended period. Naloxone is both a resuscitation drug in overdose and a take-home harm-reduction tool for the future. [8]
Acute suicide risk disclosed during a substance-use visit
If a substance-use history surfaces suicidal plan, intent, recent attempt, or access to lethal means, move immediately to a same-visit structured suicide risk assessment. Remove access to means, do not leave the young person alone, and activate the crisis or mental-health pathway. Do not rely on a promise of safety or on delayed psychology alone. [7] [10]
Intoxication with medical instability
Manage alcohol or polysubstance intoxication with airway protection, glucose if hypoglycaemic, fluid resuscitation if indicated, and a low threshold for observation. Search for co-ingestants, head injury, and occult trauma. Coercion, assault, or exploitation disclosed during intoxication must trigger local safeguarding and mandatory-reporting duties. [7] [11]
Management — Definitive & Stepwise
The definitive pathway is the SBIRT sequence with harm reduction woven through every step. It is iterative — repeat at every visit, because engagement and screen status change over time. [1] [14]
Brief intervention with motivational interviewing
The evidence-based brief intervention is motivational interviewing: open questions, affirmation, reflective listening, and summaries (OARS). The aim is to evoke the young person's own reasons for change rather than impose yours. Meta-analyses confirm motivational interviewing works for adolescent substance use and generalises across health behaviours. It is a method, not a medication. [5] [6]
Domain-specific harm-reduction bundles
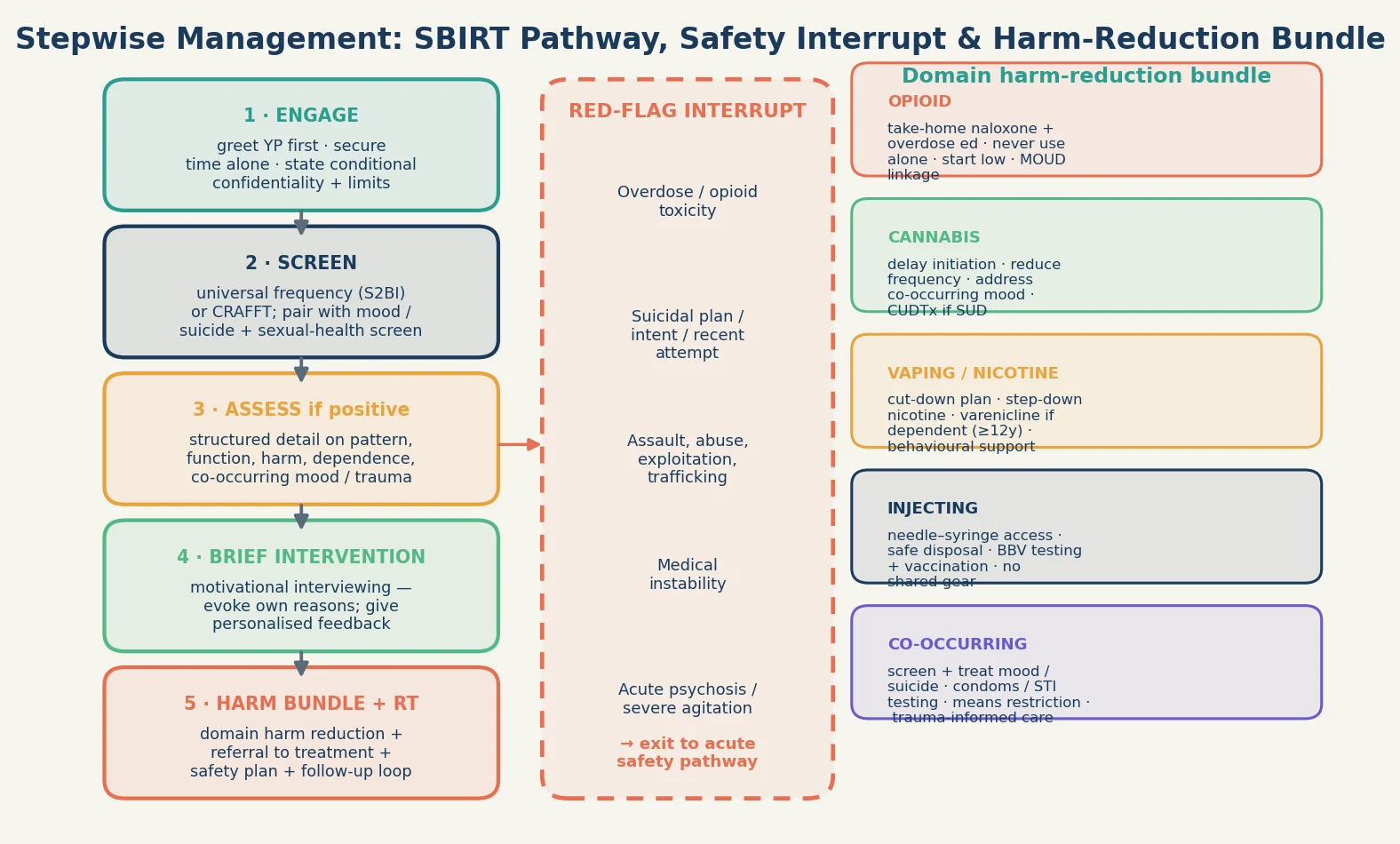
Opioid harm reduction (fentanyl era): take-home naloxone plus overdose education for the young person and, with consent, family or peers; safer-use messaging (avoid mixing, start low, never use alone, don't use alone); opioid-use-disorder assessment and linkage to medications for opioid-use disorder (MOUD); needle–syringe access and safe-disposal advice if injecting; and blood-borne-virus testing with vaccination. [7] [8]
Cannabis harm reduction: delay initiation, reduce frequency, lower potency, address co-occurring mood, and link to cannabis-use-disorder treatment (evidence-based psychotherapy — motivational interviewing, cognitive-behavioural therapy, and family-based therapy) when criteria are met. There are no FDA-approved medications for adolescent cannabis-use disorder; treatment is primarily behavioural. [13] [10]
Vaping/nicotine harm reduction: a cut-down plan, step-down nicotine, behavioural support, and varenicline for adolescents with established dependence — a randomised trial demonstrated varenicline's efficacy for youth nicotine vaping cessation above placebo, which has shifted the pharmacotherapy options. Follow locally approved prescribing guidance and age thresholds. [12] [15]
Injecting harm reduction: needle–syringe access and safe disposal, blood-borne-virus testing plus hepatitis B vaccination, no shared equipment, and never use alone. Needle–syringe provision and opioid-substitution therapy reduce blood-borne-virus transmission and overdose — describe the evidence rather than fabricating product-specific doses. [9] [7]
Referral to treatment and follow-up
Refer indicated cases — moderate-to-severe use disorder, dependence, co-occurring mental disorder, overdose history — to youth-appropriate substance-use treatment. Close the follow-up loop: name the next contact, give a low-threshold way back in, and confirm referrals were received. Longitudinal data show adolescent SBIRT shapes subsequent health-care use, so build the trajectory deliberately. [14] [11]
Specific Subtypes & Scenarios
Fentanyl-era opioid exposure in a young person who did not intend opioid use
A 17-year-old took a pill they believed was a benzodiazepine or stimulant; fentanyl exposure is possible. Offer take-home naloxone and overdose education immediately, assess for opioid-use disorder and linkage to MOUD, test for blood-borne viruses if injecting, and bundle sexual-health and mental-health care. The stance is pragmatic and non-judgemental: lower the consequences today while keeping the door open. [8] [7]
Vaping and nicotine dependence with a cut-down approach
A 15-year-old vapes daily, has morning cravings, and has tried to quit twice. Confirm dependence, offer a structured cut-down plan with step-down nicotine and behavioural support, and consider varenicline under specialist guidance where locally approved. Frame relapse as data, not failure. [12] [15]
Cannabis use with co-occurring mood disturbance
A 16-year-old uses high-potency cannabis daily and describes emerging low mood and declining school function. Screen for the mood disorder and any psychotic features, reduce cannabis frequency and potency, and link to cannabis-use-disorder treatment (behavioural therapy) alongside mental-health care. Avoid diagnostic overshadowing of either condition by the other. [13] [10]
Injecting drug use with shared equipment
A young person discloses injecting with shared gear. Offer needle–syringe access and safe-disposal advice, test for hepatitis B and C and HIV, check and offer hepatitis B vaccination, assess for opioid-use disorder and MOUD linkage, and offer take-home naloxone. Needle–syringe provision reduces blood-borne-virus transmission — this is evidence-based public health, not moral endorsement. [9] [8]
Youth-justice and out-of-home-care adolescents
These young people carry high substance-use and trauma loads with fragmented records. Use trauma-informed pacing, accept that disclosure may take several visits, screen at every contact, and coordinate across systems. Confidentiality is complex — clarify who holds what information and why. [11] [10]
Complications & Pitfalls
Demanding abstinence as the only outcome and labelling relapse as failure harms engagement. The dual-systems model shows why willpower-only demands fail; harm reduction keeps the highest-risk young people in contact. [7] [10]
Running a screen but filing a positive lead without action is a common and dangerous failure. A positive S2BI or CRAFFT that is documented but never followed by a brief intervention, assessment, or harm-reduction bundle is screening theatre. Pair every positive screen with same-visit clinical action. [1] [14]
A judgemental or punitive stance suppresses future disclosure. The young person who felt judged does not return, or returns having learned to lie. The relationship is the intervention. [11] [7]
Confusing a screen score with a diagnosis, or using urine toxicology punitively, is dangerous. Screens are triggers; toxicology is consent-governed and narrow. Misuse erodes trust and misses the real clinical question. [1] [2]
Missing exploitation, trafficking, or coercion behind "risk-taking behaviour" is a safeguarding failure. Ask about coercion and exploitation separately, in private, and act on disclosure under local safeguarding duties. [7] [11]
Prognosis & Disposition
Prognosis is framed as the trajectory of risk and engagement, not a disease stage. A young person who keeps attending and keeps reducing harm is on a better trajectory than one who disengaged after an abstinence ultimatum, regardless of whether they are still using. [10] [7]
Routine disposition: low-risk screen, brief reinforcement, safety net, re-screen next visit. Early review: moderate risk with a brief intervention and harm bundle in place, named next contact. Urgent disposition: high risk — overdose history, suicidal plan, dependence, instability — same-day pathway and tight follow-up. [1] [14]
Disposition must always name the next contact and a low-threshold way back in. Engagement across adolescence into young adulthood is itself a harm-reduction outcome — a young person who trusts the service will return when the risk escalates. Close the follow-up loops after substance-use, mental-health, and social-work referral. [11] [14]
[1] [10]Special Populations
Youth-justice-involved and out-of-home-care young people carry the highest substance-use and trauma loads. Use trauma-informed pacing, screen at every contact, coordinate across systems, and clarify confidentiality across agencies. [11] [7]
Gender-diverse and sexual-minority youth face minority stress that elevates substance-use risk. Tailor the screen and the harm-reduction bundle without assuming substance use is "just coping," and screen for co-occurring mental-health and sexual-health needs together. [10] [7]
Indigenous young people require culturally safe assessment that acknowledges the legacy of colonisation, systemic racism, and intergenerational trauma, and that draws on community-controlled services wherever available. Substance-use risk is inseparable from social and cultural context. [11] [10]
Migrant and refugee youth may need professional interpreters (never family), trauma-informed pacing, and attention to pre-arrival exposures and acculturation stress. Avoid assumptions about substance norms. [11]
Neurodiverse and disabled young people are at elevated substance-use risk that is often missed through diagnostic overshadowing. Adapt the assessment to communication style, screen directly, and do not attribute use to "the diagnosis" without assessment. [10]
Socioeconomic disadvantage shapes which harm-reduction options are reachable and affordable. A naloxone kit, nicotine replacement, or transport to treatment that is unaffordable is not a plan. Build the bundle around what the young person can actually access. [7] [11]
Evidence, Guidelines & Regional Differences
The AAP SBIRT policy (Levy 2016) endorses universal adolescent substance-use screening, brief intervention, and referral to treatment as routine paediatric care. It names SBIRT as a core competency, not an optional add-on. [1]
CRAFFT (Knight 2002) remains the most-validated adolescent substance-use screen. S2BI (Levy 2021/2023) is the validated frequency-based screen that tiers response and performs well against DSM-5 substance-use disorder criteria. [2] [3] [4]
Motivational interviewing has meta-analytic support for adolescent substance-use behaviour change (Jensen 2011) and for adolescent health behaviour more broadly (Cushing 2014). It is the brief-intervention method of choice. [5] [6]
Harm reduction for young people who use drugs (Kimmel 2021) and the public-health-prevention case (Winer 2022) set out the principles: pragmatic, non-judgemental, youth-centred, evidence-based, and rights-respecting. Naloxone access for youth (Chadi 2019) and needle–syringe and opioid-substitution evidence (MacArthur 2014) anchor the overdose and blood-borne-virus arms of the bundle. [7] [8] [9] [10]
Vaping pharmacotherapy advanced with a 2025 randomised trial of varenicline for youth nicotine vaping cessation (Evins 2025), and cannabis-use-disorder treatment remains behavioural (Adams 2023). EVALI (Cao 2020) grounded the acute-pulmonary-harm case against unregulated vaping products. [12] [13] [15]
[1] [8] [11]Exam Pearls
- Open with time alone and conditional confidentiality before any substance question. [1]
- S2BI tiers by past-year frequency; CRAFFT (Car, Relax, Alone, Forget, Friends, Trouble) is the deeper screen. [2] [3]
- Pair every positive screen with same-visit clinical action — never file and refer. [1] [14]
- Name the harm bundle concretely: naloxone, needle–syringe, cut-down/varenicline, BBV testing, means restriction. [7] [8] [12]
- Brief intervention = motivational interviewing (OARS: open questions, affirmation, reflective listening, summaries); meta-analytic support. [5] [6]
- Cite the dual-systems model to justify why harm reduction fits adolescent biology. [10]
- Fentanyl era: naloxone and overdose education for any opioid-exposure risk, even when the young person did not intend opioid use. [8]
- Ask about coercion and exploitation separately from "risk-taking behaviour." [7] [11]
- State that local statute governs consent ages, reporting triggers, and naloxone access — do not invent universal cut-offs. [1]
- Remember SBIRT-H: Screen (S2BI/CRAFFT), Brief intervention (MI), Indicated assessment, Referral to treatment, Treat co-occurring, Harm-reduction bundle.
References
- [1]Levy SJL, Williams JF, Committee on Substance Use and Prevention Substance Use Screening, Brief Intervention, and Referral to Treatment. Pediatrics, 2016.PMID 27325634
- [2]Knight JR, Sherritt L, Shrier LA, Harris SK, Chang G Validity of the CRAFFT substance abuse screening test among adolescent clinic patients. Archives of pediatrics & adolescent medicine, 2002.PMID 12038895
- [3]Levy S, Kass NE, O'Malley T, Wisk LE, Grant RWC, Harris SK Assessment of Screening Tools to Identify Substance Use Disorders Among Adolescents. JAMA network open, 2023.PMID 37213103
- [4]Levy S, Weiss R, Sherritt L, et al Sensitivity and specificity of S2BI for identifying alcohol and cannabis use disorders among adolescents. Substance abuse, 2021.PMID 32814009
- [5]Cushing CC, Jensen CD, Miller MB, Leffingwell TR Meta-analysis of motivational interviewing for adolescent health behavior: efficacy beyond substance use. Journal of consulting and clinical psychology, 2014.PMID 24841861
- [6]Jensen CD, Cushing CC, Aylward BS, Craig JT, Sorell DM, Steele RG Effectiveness of motivational interviewing interventions for adolescent substance use behavior change: a meta-analytic review. Journal of consulting and clinical psychology, 2011.PMID 21728400
- [7]Kimmel SD, Gaeta JM, Hadland SE, Hallett E, Marshall BDL Principles of Harm Reduction for Young People Who Use Drugs. Pediatrics, 2021.PMID 33386326
- [8]Chadi N, Hadland SE Youth Access to Naloxone: The Next Frontier? The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2019.PMID 31648752
- [9]MacArthur GJ, van Velzen E, Palmateer N, Kimber J, Pharris A, Hope V, et al Interventions to prevent HIV and Hepatitis C in people who inject drugs: a review of reviews to assess evidence of effectiveness. The International journal on drug policy, 2014.PMID 23973009
- [10]Winer JM, Yule AM, Hadland SE, Bagley SM Addressing adolescent substance use with a public health prevention framework: the case for harm reduction. Annals of medicine, 2022.PMID 35900132
- [11]Bagley SM, Hadland SE, Schoenberger SF, Gai MJ, Topp D, Hallett E Integrating substance use care into primary care for adolescents and young adults: Lessons learned. Journal of substance abuse treatment, 2021.PMID 34080547
- [12]Evins AE, Hoeppner BB, Pachas GN, et al Varenicline for Youth Nicotine Vaping Cessation: A Randomized Clinical Trial. JAMA, 2025.PMID 40266580
- [13]Adams ZW, Wilson JJ, Livingston NA, et al Treatment of Adolescent Cannabis Use Disorders. The Psychiatric clinics of North America, 2023.PMID 37879838
- [14]Sterling S, Kline-Simon AH, Jones A, et al Health Care Use Over 3 Years After Adolescent SBIRT. Pediatrics, 2019.PMID 31018988
- [15]Cao DJ, Aldy K, Hsu S, McGetrick M, Nguyen W, Hieger C, et al Review of Health Consequences of Electronic Cigarettes and the Outbreak of Electronic Cigarette, or Vaping, Product Use-Associated Lung Injury. Journal of medical toxicology : official journal of the American College of Medical Toxicology, 2020.PMID 32301069