Paeds · adolescent-and-young-adult-medicine
Chronic disease self-management in young people
Also known as Adolescent self-management · Self-management of chronic illness in adolescence · Adherence in young people · Transition readiness skills · Chronic disease empowerment in youth · Supported self-management in adolescents
A fellowship approach to chronic-disease self-management in young people: what self-management is and its three task-domains; why it breaks down in adolescence through developmental, psychosocial and system mechanisms; how to assess skills and transition readiness with the TRAQ; how to measure adherence objectively rather than trust self-report; and how to build a stepwise self-management plan with motivational interviewing, shared goals, written action plans and technology — across type 1 diabetes, asthma, sickle cell disease, cystic fibrosis, IBD, JIA, CKD and transplant, for ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 16-year-old with type 1 diabetes is admitted in diabetic ketoacidosis for the third time in a year. His HbA1c has climbed, his clinic letters say "non-compliant", and the team is frustrated. The real problem is rarely that he has decided not to look after himself. It is that nobody has built, with him, the skills to manage a demanding condition through the hardest developmental years of his life. That skill — helping a young person own their chronic illness — is chronic-disease self-management. [2] [6]
Self-management is the tasks and confidence a person develops to live with a long-term condition: taking treatment reliably, monitoring for trouble, acting on a flare, navigating appointments, and coping with how the illness feels. The clinician's job is self-management support — the partnership, education, tools and coaching that make those tasks possible. The two ideas travel together: self-management is what the young person does, self-management support is what you do with them. [6] [24]
It matters because chronic disease now dominates the health of young people. Asthma, type 1 diabetes, cystic fibrosis, inflammatory bowel disease, juvenile idiopathic arthritis, sickle cell disease, chronic kidney disease and transplant survivors increasingly survive into adolescence and beyond — and adolescence is exactly when control tends to slip, when adherence dips, and when preventable complications cluster. Get self-management right and you change a life trajectory. Get it wrong and you see the recurring admissions, the graft loss, the retinopathy, and the young person lost to follow-up at transfer. [2] [24] [1]
Classification
Begin with the patient, then sort what kind of self-management work they need. Self-management is best held as three task-domains, the long-standing framework that still organises the field: the medical work of the regimen, the role work of fitting the condition into life, and the emotional work of carrying it. [6]
The medical-management domain is the obvious one — taking medicines, checking glucose or peak flow, recognising and treating a flare, and turning up to appointments. The role-management domain is the life around it: reorganising school, sport, friendships and work around the condition, telling the people who need to know, and paying for and sourcing treatment. The emotional-management domain is the most overlooked and the most predictive of outcome: processing the grief and anger of diagnosis, fighting stigma and isolation, managing anxiety and low mood, and building an identity that is bigger than the illness. A plan that only ever talks about tablets has missed two-thirds of the work. [6] [17]
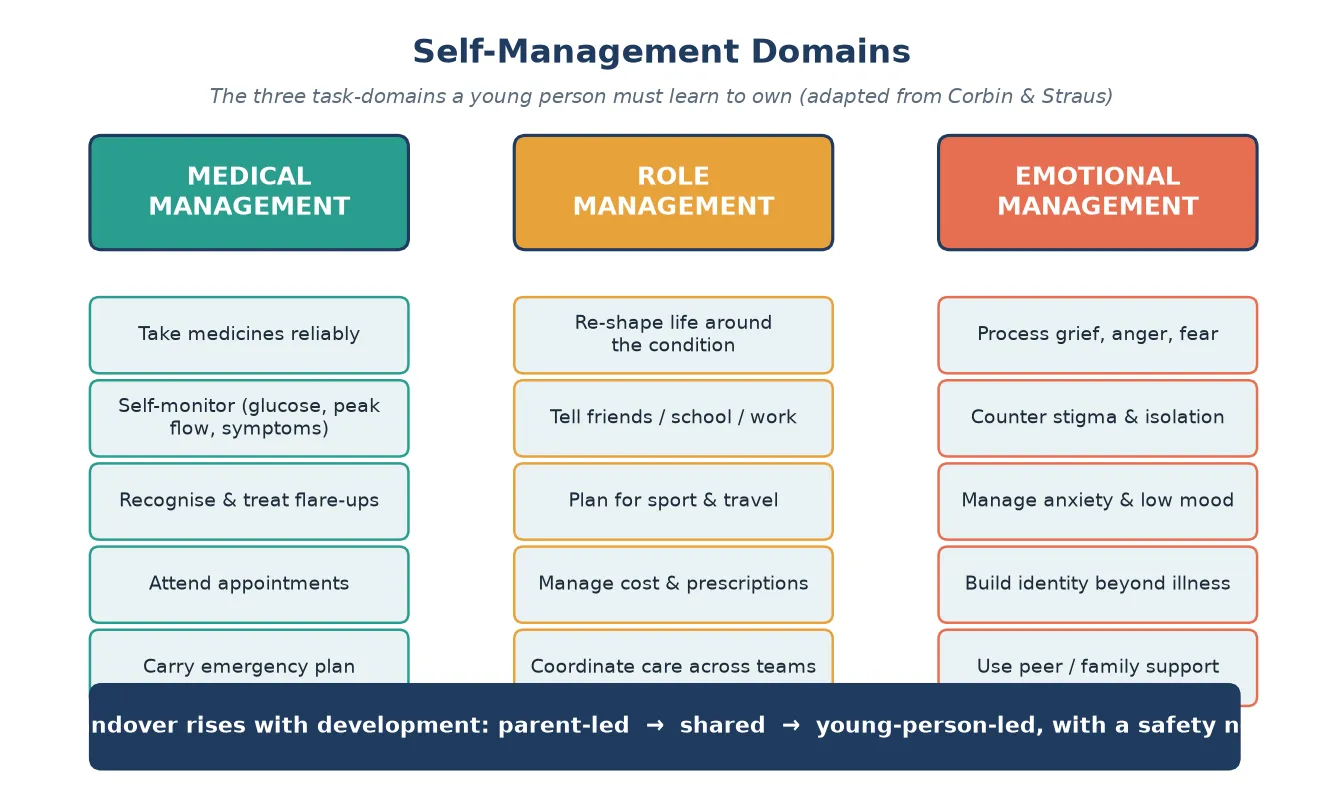
Self-management is also a developmental process, not a switch. In childhood the parent is the manager. Across adolescence responsibility is handed over in a graded way — parent-led, then genuinely shared, then young-person-led — with a safety net held underneath the whole time. Where a young person sits on that arc is what you assess at the bedside, and it is not the same as their age, their diagnosis, or their transition-readiness score. [4] [6]
Epidemiology & Risk Factors
Roughly one in four adolescents lives with a chronic health condition, and a substantial share of adolescent morbidity and mortality is concentrated in this group. The headline statistic that shapes practice is adherence: around half of adolescents with a chronic condition take their treatment sub-optimally, and non-adherence peaks in the transition years before partly recovering in the mid-twenties. [2] [24]
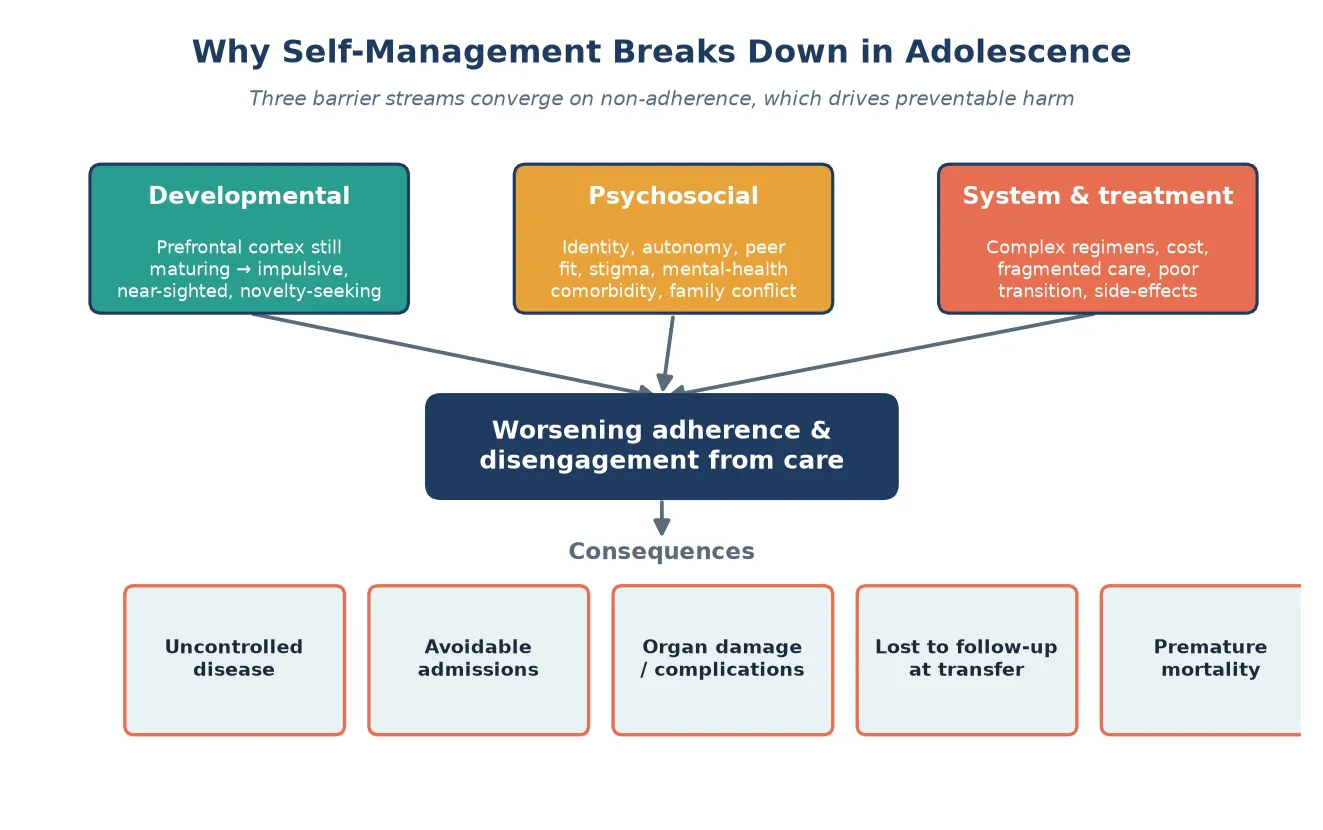
The factors that predict a breakdown cluster into three streams. Developmental factors — the still-maturing prefrontal cortex, reward-seeking, and the weighting of now over a distant complication — are nearly universal in adolescence. Psychosocial factors are the strongest modifiable drivers: comorbid depression and anxiety, family conflict, bullying, stigma, and the normal drive for autonomy. System factors are the ones clinicians can fix: regimen complexity and side-effect burden, the cost and accessibility of treatment, fragmented care, and a poorly managed transfer to adult services. [7] [2]
Disparities amplify the risk. Indigenous, rural-remote, out-of-home-care, justice-involved, migrant and refugee young people, and those living in socioeconomic disadvantage, carry heavier self-management burdens — cost of medicines, transport, food security, digital access, and culturally unsafe care all conspire. Left unaddressed, these produce the recurring admissions and the graft losses that mark inequity, not biology. [18] [6]
Pathophysiology
There is no single lesion behind self-management failure in adolescence. Three converging streams push a young person toward non-adherence, and you need to see all three because they call for different fixes. [7] [6]
The first is developmental. The prefrontal cortex — the seat of planning, impulse control and weighing long-term consequence — continues to mature into the mid-twenties. Meanwhile the reward system is exquisitely sensitive to peer approval and novelty. So a teenager is neurobiologically tilted toward the immediate reward of fitting in over the distant, invisible benefit of a tablet taken today. This is not a character flaw; it is developmental neuroscience, and it is why a judgemental response fails. [7] [13]
The second is psychosocial. The normal drive for autonomy collides with a regimen still run by parents, generating conflict and covert non-adherence — the teenager who says they have injected when they have not. Stigma and identity threat push a young person to hide the condition and its treatment, especially at school and with peers. Comorbid depression and anxiety directly blunt the cognitive and motivational machinery of self-care, so mental illness is both a consequence and a cause of poor control. [9] [17]
The third is systemic. Regimens that are complex, burdensome or carry visible side-effects erode adherence over years. Fragmented care and a cold transfer to adult services create a "care cliff" — the moment a young person leaves a familiar paediatric team, receives no warm handover, and simply vanishes, reappearing in an adult emergency department months later. The acute chest syndrome, the DKA, the graft rejection at 19 — these are system failures as much as patient failures. [1] [11]
A recurring trap compounds all three: self-reported adherence is systematically overestimated. Asked how they are doing, most young people — and most parents — give the answer they think the clinician wants. A landmark review put it plainly: across chronic disease, self-report substantially overstates true adherence. The implication is operational. Never rely on self-report alone. Pair it with an objective marker, every time. [2] [8]
Clinical Presentation
Failing self-management rarely announces itself as "I have stopped my tablets". It arrives sideways, through the disease. A rising HbA1c. Increasing reliever use and nocturnal waking. More pain crises or exacerbations. A cluster of repeat admissions. A young person who stops coming to clinic. Your job is to read these signals as self-management problems, not just as disease activity. [2] [11]
Covert non-adherence has a signature: the report and the reality do not agree. The young person (or parent) insists the regimen is followed perfectly, yet the objective marker — the glucose downloads, the pharmacy refill gap, the low tacrolimus level, the empty pill count — tells another story. When control is mysteriously poor despite an "escalating" drug ladder, stop escalating and start measuring adherence. [8] [7]
Psychological distress often presents through the chronic condition. Worsening control in an adolescent with previously stable disease is a flag for anxiety, depression, bullying, family conflict or abuse — not only for a change in the disease. The HbA1c that climbs after parental separation, or the asthma that worsens when school refusal begins, are communications as much as they are physiology. [9] [14]
The transfer cliff presents as absence: a young person with a complex condition is discharged from paediatric care, no adult appointment is secured, and they are lost to follow-up — until they re-present to adult services in crisis years later. This is one of the most preventable presentations in adolescent medicine, and it is a failure of the system, not the patient. [1]
Differential Diagnosis
When control deteriorates, the central diagnostic question is: is this true refractory disease, or unrecognised non-adherence masquerading as treatment failure? The two coexist more often than either alone, so consider both every time rather than forcing a choice. [8] [2]
The most important split is "won't" from "can't". A young person may look non-adherent when the real barrier is something they cannot fix alone: the cost of the medicine, a health-literacy gap, an undiagnosed learning or neurodevelopmental disability, a swallowing or dexterity problem, an unrecognised side-effect, or untreated depression. Before you label behaviour, you rule out barriers. [6] [7]
A short differential of mimics keeps you from overcalling non-adherence. Poor inhaler technique, a blocked or empty device, the wrong diagnosis (asthma masquerading as something else), a drug interaction, or an absorption problem can all look like non-adherence. A young person with rising creatinine after transplant may be non-adherent — or may have a drug interaction, recurrence, or infection. Measure, do not assume. [8]
True refractory disease
- Objective markers fall despite verified, dosed, absorbed therapy
- Pharmacy refills and downloads confirm full adherence
- Re-assess diagnosis and escalate therapy
Unrecognised non-adherence
- Self-report claims perfect adherence
- Objective markers (refills, levels, downloads) tell another story
- Stop escalating drugs; measure and support
Hidden barrier ('can't')
- Cost, literacy, neurodevelopmental disability, side-effect, depression
- Technique, device, or absorption problem
- Remove the barrier before judging the behaviour
Finally, distinguish a system failure from a patient failure. A young person who never makes it to adult clinic may have chosen not to attend — or may never have been given an appointment, a summary, or a warm handover. The fix is very different. [1] [22]
Clinical & Bedside Assessment
Assessment happens in the room, with the young person, in confidence. Start by seeing the young person alone for part of the visit — this is the frame that makes an honest self-management assessment possible, because it removes the pressure to perform for a parent. Run a brief HEEADSSS to place the condition in the context of their actual life. [13] [6]
Then assess skills directly, not by report. Ask the young person — not the parent — to describe their regimen in their own words, to show you their technique (inhaler, injection, blood-glucose checking), and to talk you through what they would do if things went wrong: a hypo, a pain crisis, a missed dose, a flare. The gap between what a parent reports and what a young person can actually demonstrate is the single most useful finding in this assessment. [11] [4]
Bring a transition-readiness tool to structure the conversation. The Transition Readiness Assessment Questionnaire (TRAQ) is the best-evidenced and most widely used; its domains cover managing medications and keeping appointments, among the everyday tasks of self-care. Use it to find the specific gaps, not to generate a single number that justifies or blocks transfer — no readiness score alone decides when a young person moves to adult care. [4] [3]
Assess the family system: who actually does what, where the conflict sits, and whether the young person is being given room (or too much, too soon) to take charge. Screen for the mental illness that silently drives self-management failure — a brief PHQ-A for depression and a GAD-7 for anxiety take minutes and change the plan. Map the supports — school, peers, extended family, apps, community — and name the gaps. [14] [7]
Investigations
"Investigations" in self-management means measuring adherence objectively, because self-report will mislead you. Each condition has its own window onto the truth, and you combine them. [2] [8]
For type 1 diabetes, HbA1c reflects glycaemia over weeks and continuous-glucose monitoring adds time-in-range and glycaemic variability. For asthma, electronic inhaler and dispenser downloads reveal actual reliever and preventer use, and prescription-refill data show whether preventer is even being collected. For transplant and chronic kidney disease, trough drug levels (such as tacrolimus) and the gap between prescribed and dispensed immunosuppression expose non-adherence that drives graft loss. For sickle cell disease, hydroxyurea refill records sit alongside pain and attendance data. [8] [17]
No single measure is enough. A multimethod approach — objective marker plus self-report plus a validated questionnaire — catches more non-adherence than any one method alone, and it guards against both over- and under-diagnosis. Where the picture is confusing, re-assess the diagnosis and check for the mimics: drug interactions, absorption issues, and alternative explanations for poor control. [8] [2]
Layer in mental-health screening as part of the work-up, because depression and anxiety are both cause and consequence of poor control. Routine monitoring of disease control — the HbA1c, the lung function, the blood pressure, the graft function — must accompany every self-management assessment, so that deterioration is caught early rather than at the next crisis. [9] [14]
Management — Resuscitation
The immediate priority when a self-management failure presents as an acute crisis is the crisis itself, not the failure. A young person in diabetic ketoacidosis, a severe asthma exacerbation, acute chest syndrome, or with suspected graft rejection needs resuscitation and stabilisation first. Manage the emergency by protocol. [2] [17]
Hold the self-management conversation for the recovery phase. Conducting a blaming "why didn't you take your insulin?" interrogation in the emergency department destroys the relationship and worsens future engagement. The stance in the acute event is non-punitive, curious and supportive — "this is really hard, let's get you safe, and we will work on the rest together once you are well". [13] [11]
Recognise when a mental-health crisis overrides the chronic-disease plan. Disclosure of suicidality, an act of serious self-harm, or acute psychosis is a psychiatric emergency that takes precedence over everything else; secure the young person's safety first, then re-weave the chronic-disease plan around the mental-health treatment. [14] [9]
After any acute self-management-related admission, build a tighter safety-net: closer follow-up within days, a simplified regimen, a written flare plan, and wrap-around supports — adolescent health, psychology, a diabetes or asthma nurse, and the family. The readmission you prevent is the one that matters most. [2] [1]
Management — Definitive & Stepwise
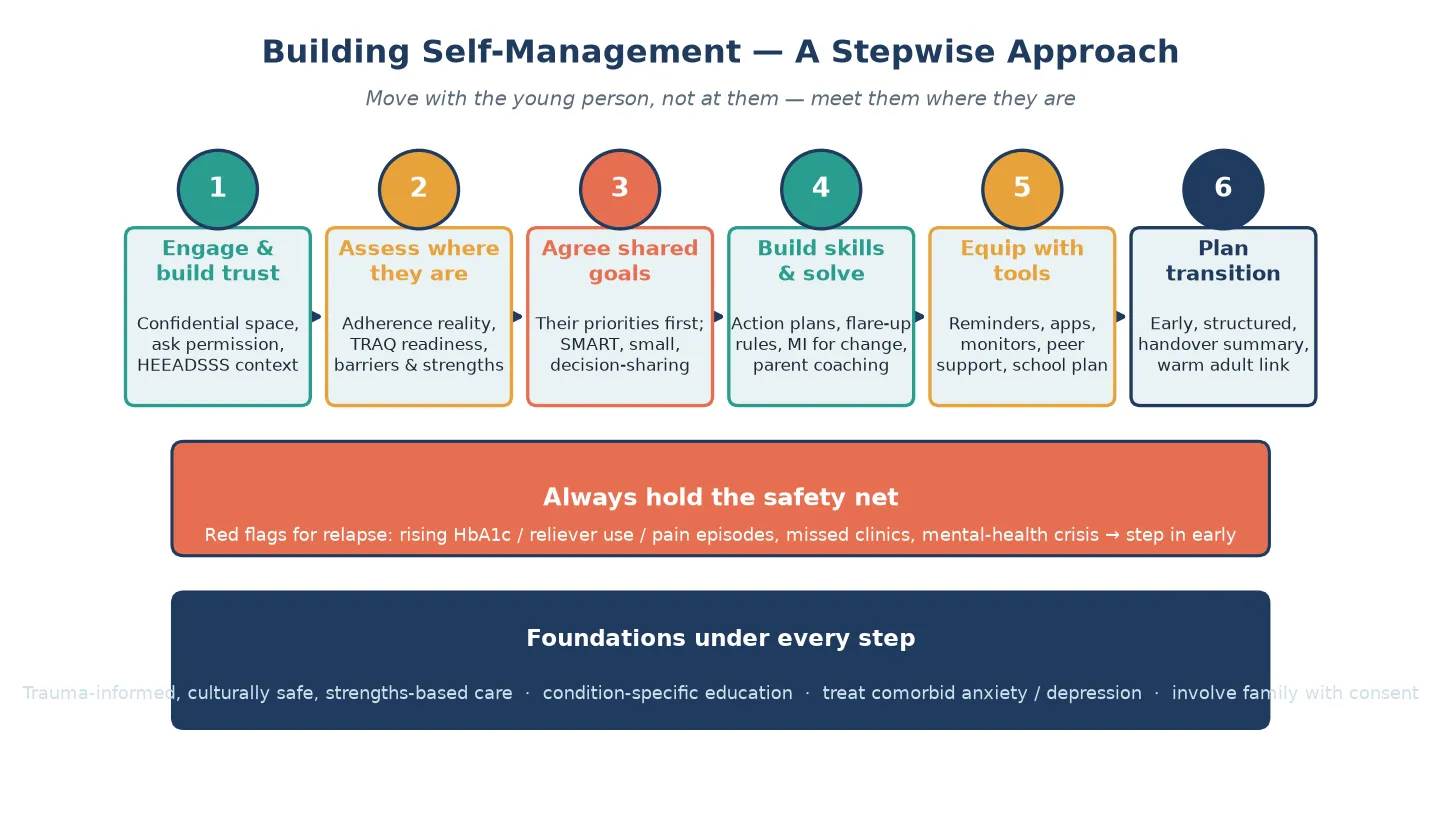
Once the young person is safe, the work is to build self-management deliberately, in steps that move with them rather than at them. The framework is sequential, though in practice you cycle through it at every visit. [6] [12]
Building self-management — the six steps
Engage and build trust: a confidential, non-judgemental space; ask permission; place the condition in their life with HEEADSSS
Assess where they are: the real adherence, the TRAQ readiness, the barriers and the strengths
Agree shared goals: their priorities first, written as SMART goals, small and achievable, with shared decision-making
Build skills and solve problems: co-created action plans, flare-up rules, motivational interviewing for change, parent coaching
Equip with tools: reminders, apps, continuous monitors, telehealth, peer support, a school plan
Plan the transition: early and structured, with a handover summary and a warm adult link
Motivational interviewing — the engine of behaviour change
Most adolescents with a chronic condition are ambivalent, not unmotivated. Motivational interviewing (MI) works with that ambivalence rather than against it. The frame is OARS — Open questions, Affirmations, Reflective listening, and Summaries — used to draw out the young person's own reasons to change ("change talk") and to roll with resistance rather than argue it down. A systematic review of MI in adolescents and young adults with chronic illness found improvements in adherence and symptom severity, and it is the behavioural tool examiners expect you to name and demonstrate. [12] [13]
Shared goals, written plans, and a simpler regimen
Set goals the young person actually owns. SMART goals — Specific, Measurable, Achievable, Relevant, Time-bound — anchored to their priorities (playing sport, going out with friends, not collapsing an exam) outperform clinician-imposed targets. Co-create a written, condition-specific action plan they carry: the asthma plan with its reliever-and-steroid ladder, the sickle-cell pain plan, the diabetes sick-day rules. And before you ever escalate a drug, simplify the regimen — the fewest doses, combination and once-daily options where possible — so that adherence becomes the path of least resistance. [19] [23]
Technology, family coaching, and escalation
Technology now sits inside self-management support — reminders, smartphone apps, continuous monitors and telehealth — and the evidence base is growing, with systematic reviews reporting usability and effectiveness gains for eHealth and mHealth tools that support self-management and transition. Use technology to support skills, never to replace them, and watch for the equity trap when device and app access follow socioeconomic lines. A gamified app may engage one young person and exclude another who cannot afford the data. [22] [20]
Coach the parents to shift from manager to coach, handing over with the young person's consent rather than holding on. Build the school and community plan so the regimen survives the real world. And escalate when self-management support exceeds the generalist's scope: a structured disease-specific self-management program, peer support, specialist adolescent health, or psychology. Peer-led programs have shown durable effectiveness — a peer-led asthma self-management trial demonstrated long-term benefit on asthma outcomes in urban adolescents. [14] [16]
OARS
Specific Subtypes & Scenarios
Each chronic condition shapes self-management in its own way, and examiners probe these scenarios directly. The principles are constant; the details are condition-specific, so cross-link the dedicated topic for exact dosing. [6] [2]
Type 1 diabetes carries the steepest self-management burden in adolescence: carbohydrate counting, insulin titration, continuous-glucose monitoring, and fear of hypoglycaemia, every day. The risk that crystallises is diabetic ketoacidosis — the recurring admission that signals disengagement or a mental-health problem underneath. Resilience-building programs (such as PRISM) have shown benefit in randomised trials, and the adolescent's experience of taking over diabetes self-management is itself the subject of systematic review. Cross-link the diabetes topic for insulin regimens. [9] [10] [11]
Asthma turns on inhaler technique, action-plan ownership, and preventer adherence masked by reliever over-reliance. School-based self-management programs and peer-led models improve outcomes; a peer-led program delivered long-term benefit in urban adolescents. The single most common fix is technique correction plus a written plan the young person actually carries. [15] [16] [23]
Sickle cell disease asks the young person to manage pain at home, take hydroxyurea reliably, and avoid triggers (cold, dehydration, infection). Patients describe the daily-life impact and the self-management strategies they rely on in international surveys, and structured self-management programs improve confidence and outcomes. Cross-link the sickle-cell topic for hydroxyurea and transfusion detail. [17] [18]
Cystic fibrosis, inflammatory bowel disease, and juvenile idiabetic arthritis share a theme: a heavy, lifelong regimen (airway clearance, enzymes, modulators; immunosuppression; injections or infusions) colliding with adolescence, with relapsing-remitting courses that tempt a young person to stop treatment the moment they feel well. The protective factors are the same — a trusted team, a simplified regimen, mental-health support, and family coaching. [6] [14]
Transplant and chronic kidney disease carry the highest-stakes scenario of all: immunosuppression non-adherence is the leading modifiable driver of graft loss in adolescent transplant recipients. Monitor proactively with trough drug levels and refill data, and executive-function and caregiver-monitoring research in adolescents with chronic kidney disease shows exactly the cognitive and family mechanisms that put the graft at risk. [7] [8]
Technology-dependent and complex chronic illness — home ventilation, enteral feeding, complex medication regimens — demands the most carefully staged handover of all. The young person may never fully take over every task, so the plan defines who holds each responsibility, who is the back-up, and how adult services will inherit a device-dependent young person without a gap. [6] [1]
Complications & Pitfalls
The complications of chronic non-adherence are the chronic complications of the disease itself, arriving early and avoidably: retinopathy and nephropathy in diabetes, fixed airflow obstruction and exacerbation deaths in asthma, organ damage and stroke in sickle cell disease, and graft loss and return to dialysis after transplant. These are not rare — they are the predictable cost of unsupported adolescence. [2] [24]
The clinician pitfalls are the ones examiners love to expose. Trusting self-report is the cardinal error. Lecturing rather than asking closes down disclosure. Escalating drugs before assessing adherence drives toxicity without benefit. Blaming the young person shatters the relationship and worsens engagement. And diagnostic overshadowing — dismissing real deterioration as "just non-adherence" — can hide a relapse, an interaction, or a new diagnosis. [8] [7]
The transfer cliff is the single most preventable system complication: loss to follow-up, no handover summary, a cold adult clinic, and fragmentation. And technology, for all its promise, can widen inequity when the young people who would benefit most cannot afford the device, the data, or the language the app speaks. [1] [22]
Prognosis & Disposition
Long-term outcome in a young person with chronic disease is set by a handful of things: the control achieved, the adherence trajectory, the mental health, the social support, and above all the quality of the transition. The natural history of adherence across adolescence is the dip around the transfer years and a partial recovery in the mid-twenties — so a deteriorating 18-year-old is not a lost cause, they are a person passing through the hardest stretch. [2] [1]
Most young people with a stable chronic condition are managed in the primary-care medical home with specialist support; complex, multisystem or technology-dependent disease belongs in a specialist adolescent or integrated multidisciplinary clinic. Step up the intensity when control slips, adherence flags, or mental-health or social complexity mounts. [6] [14]
The safety-net after any self-management plan is concrete: close follow-up, objective control monitoring at every visit, a low threshold for the young person to re-contact the team, and a written crisis plan. Successful transition to adult care changes long-term outcomes — but the Cochrane review of transition interventions is candid that the evidence is diverse and of limited certainty, which is itself a high-yield exam point. [1]
Special Populations
Self-management is never one-size-fits-all. For a young person with a neurodevelopmental disability or intellectual disability, the plan defines who holds each responsibility and builds in supported decision-making rather than handing over tasks the young person cannot yet do alone. For gender- and sexuality-diverse young people, fragmented or stigmatising care can drive disengagement; an inclusive, confidential stance is therapeutic in itself. [6] [13]
For young people in out-of-home care, youth justice, or who are homeless, unstable guardianship and disrupted records make continuity almost impossible — the self-management plan must travel with the young person and name a single accountable clinician. For Indigenous, migrant, refugee and asylum-seeking young people, culturally safe care, interpreter use, and attention to the social determinants are not optional add-ons; they are the intervention. [18] [6]
Socioeconomic disadvantage shapes every layer of self-management — the cost of medicines, transport to clinic, food security, and digital access — and the response is practical: subsidised supply, telehealth, outreach, and an explicit refusal to blame behaviour that is really poverty. In rural and remote settings, telehealth and regional outreach bring specialist support to a self-management plan that otherwise could not exist. [22]
Evidence, Guidelines & Regional Differences
The evidence base for self-management support in young people is real but uneven, and a fellowship candidate must hold both its strengths and its gaps. The Cochrane review of transition of care (Campbell 2016) is the anchor citation: it found that interventions are diverse, study quality is variable, and the evidence for any single model remains of limited certainty. Name this honestly; do not overclaim. [1]
For specific tools, the evidence is stronger. Motivational interviewing in adolescents and young adults with chronic illness improves adherence and symptom severity (Schaefer 2017). Psychological interventions for parents of children and adolescents with chronic illness reduce parental distress and can improve child outcomes (Law 2019, Cochrane). Peer-led and peer-support programs show durable benefit — the peer-led asthma self-management trial (Rhee 2021) demonstrated long-term effectiveness in urban adolescents, and technology-based peer support is an active field. [12] [14] [16] [21]
Transition of care (Campbell 2016, Cochrane)
Systematic review of randomised and non-randomised studies
Population: Adolescents with chronic disease transferring from paediatric to adult services
Key finding
Interventions are diverse and the certainty of evidence is limited; no single transition model is clearly superior. Structured, coordinated, early transition with a named coordinator and preparation shows promise but is not yet proven.
Practice change
Plan a structured, early, person-centred transition with a coordinator and a warm handover — and tell the examiner the evidence is still maturing.
The digital evidence base is growing fast: systematic reviews report usability and effectiveness gains for eHealth and mHealth tools that support self-management and transition (Li 2024), and gamification shows engagement promise (Stutvoet 2024). The gaps are honest: short follow-up, single-condition apps, limited equity data, and a tendency to measure process (app opens) rather than outcomes (control, admissions, quality of life). [22] [20]
Regional transition frameworks differ, and examiners expect you to name the local one. [3] [5]
ANZ (RACP)
- RACP transition position statement and 'Moving On' resources
- Capacity-based consent, mature-minor principle
- Adolescent medicine as a recognised subspecialty pathway
UK (RCPCH/NICE)
- Ready Steady Go and Got It transition tools
- NICE transition guidance (NG43)
- Gillick competence governs adolescent consent
US (AAP/Got Transition)
- Got Transition Six Core Elements framework
- AAP/AAFP/ACP clinical report on transition
- Insurance and access shape the adult-care handover
Exam Pearls
- Adherence is not compliance. Adherence is an active, agreed collaboration; compliance is passive obedience. The word you choose signals your model of care — pick the collaborative one. [2] [24]
- Self-report overstates adherence. Always pair it with an objective marker — refills, downloads, drug levels, HbA1c — or you will be fooled. [2] [8]
- TRAQ measures managing medications and appointment-keeping, among other self-care domains. No readiness score alone justifies or blocks transfer. [4] [3]
- The Campbell 2016 Cochrane review found transition evidence is diverse and uncertain — say so, do not overclaim. [1]
- Motivational interviewing is OARS — Open questions, Affirmations, Reflective listening, Summaries — and you may be asked to demonstrate it at the table. [12] [13]
- The adherence dip deepens around the transfer years and partly recovers in the mid-twenties — a deteriorating 18-year-old is passing through, not lost. [2]
- Treat the crisis first. Have the self-management conversation in the recovery phase, never punitively in the acute event. [17]
- Simplify before you escalate. Fewest doses, combination devices, once-daily options where possible. [23] [19]
- Immunosuppression non-adherence is the leading modifiable driver of adolescent graft loss — monitor proactively. [7] [8]
- Name the regional transition tool the examiner expects: Ready Steady Go (UK), Got Transition Six Core Elements (US), RACP position statement (ANZ). [3] [5]
References
- [1]Campbell F, Biggs K, Aldiss SK, et al. Transition of care for adolescents from paediatric services to adult health services. Cochrane Database Syst Rev, 2016.PMID 27128768
- [2]Osterberg L, Blaschke T. Adherence to medication. N Engl J Med, 2005.PMID 16079372
- [3]Zhang LF, Ho J, Yeh GM, et al. A systematic review of the psychometric properties of transition readiness assessment tools in adolescents with chronic disease. BMC Pediatr, 2014.PMID 24405982
- [4]Wood DL, Sawicki GS, Miller MD, et al. The Transition Readiness Assessment Questionnaire (TRAQ): its factor structure, reliability, and validity. Acad Pediatr, 2014.PMID 24976354
- [5]Yi T, Wu X, Jiang Y, et al. Instruments to Assess Transition Readiness Among Adolescents With Chronic Disease: A COSMIN Systematic Review of Measurement Properties. Child Care Health Dev, 2025.PMID 39629862
- [6]Camp-Spivey LJ, Berenson S, Riddell K, et al. Theoretical and contextual considerations for self-management strategies of children and adolescents with chronic diseases: An integrative review. J Child Health Care, 2022.PMID 33913767
- [7]Eaton CK, Gutierrez-Colina AM, Quast LF, et al. Executive functioning, caregiver monitoring, and medication adherence over time in adolescents with chronic kidney disease. Health Psychol, 2020.PMID 32202823
- [8]Pruette CS, Iyengar MS, Kshirsagar AV, et al. Does a multimethod approach improve identification of medication nonadherence in adolescents with chronic kidney disease? Pediatr Nephrol, 2019.PMID 30116892
- [9]Winkley K, Ismail K, Landau S, Eisler I. Psychological interventions to improve self-management of type 1 and type 2 diabetes: a systematic review. Health Technol Assess, 2020.PMID 32568666
- [10]Yi-Frazier JP, Tapia C, Smith RE, et al. Promoting Resilience in Stress Management for Adolescents With Type 1 Diabetes: A Randomized Clinical Trial. JAMA Netw Open, 2024.PMID 39158914
- [11]Leocadio P, Maatouk I, Saleh S, Phung M, Jones A, Greenfield G, Hayward J, Huynh-Hua B, King A, Phelan H, Cohen N. Adolescents' Experiences of Transition to Self-Management of Type 1 Diabetes: Systematic Review and Future Directions. Sci Diabetes Self Manag Care, 2023.PMID 37927049
- [12]Schaefer MR, Kavookjian J. The impact of motivational interviewing on adherence and symptom severity in adolescents and young adults with chronic illness: A systematic review. Patient Educ Couns, 2017.PMID 28619271
- [13]Desai N, Braganza S. The Role of Motivational Interviewing in Children and Adolescents in Pediatric Care. Pediatr Ann, 2019.PMID 31505012
- [14]Law E, Fisher E, Eccleston C, Palermo TM. Psychological interventions for parents of children and adolescents with chronic illness. Cochrane Database Syst Rev, 2019.PMID 30883665
- [15]Harris K, Kneale D, Lasserson TJ, McDonald VM, Grigg J, Thomas J. School-based self-management interventions for asthma in children and adolescents: a mixed methods systematic review. Cochrane Database Syst Rev, 2019.PMID 30687940
- [16]Rhee H, Belyea MJ, Brasch J. Long-term Effectiveness of a Peer-Led Asthma Self-management Program on Asthma Outcomes in Adolescents Living in Urban Areas: A Randomized Clinical Trial. JAMA Netw Open, 2021.PMID 34874404
- [17]Crosby LE, Joffe NE, Peugh J, Ware MA, Shook L, Robins DL, Britto MT, Quinn CT. Improving self-management in adolescents with sickle cell disease. Pediatr Blood Cancer, 2020.PMID 32697889
- [18]Osunkwo I, Andemariam B, Minniti CP, et al. Impact of sickle cell disease on patients' daily lives, symptoms reported, and disease management strategies: Results from the international Sickle Cell World Assessment Survey (SWAY). Am J Hematol, 2021.PMID 33264445
- [19]Krockow EM, Zermatten CAV, Buyck JF. Improving shared health decision making for children and adolescents with chronic illness: A narrative literature review. Patient Educ Couns, 2019.PMID 30578102
- [20]Stutvoet MD, Geerling S, Scholten N, van Os-Medendorp H, Kelders SM. Gamification in eHealth for Chronic Disease Self-Management in Youth: A Systematic Review. Games Health J, 2024.PMID 38900649
- [21]Berkanish P, Mawn B, Mahieu L, Hussain N, Browning K. Technology-Based Peer Support Interventions for Adolescents with Chronic Illness: A Systematic Review. J Clin Psychol Med Settings, 2022.PMID 35147830
- [22]Li Z, Wang Y, Meng Y, et al. Usability and Effectiveness of eHealth and mHealth Interventions That Support Self-Management and Health Care Transition in Adolescents and Young Adults With Chronic Disease: Systematic Review. J Med Internet Res, 2024.PMID 39589770
- [23]Gibson PG, Powell H, Coughlan J, et al. Self-management education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev, 2003.PMID 12535399
- [24]Dunbar-Jacob J, Mortimer-Stephens MK. Adherence in chronic disease. Annu Rev Nurs Res, 2000.PMID 10918932