Paeds · adolescent-and-young-adult-medicine
Consent and confidential care for adolescents
Also known as Adolescent consent · Mature minor · Gillick competence · Confidentiality in adolescent care · Conditional confidentiality · Adolescent decision-making capacity
A fellowship approach to consent and confidential care for adolescents: informed consent, assent and parental permission; bedside capacity assessment using the Gillick/mature-minor principle; conditional confidentiality with lawful limits and how to override ethically; protecting sensitive records, portals and billing; and consent for contraception, STI care, mental health, vaccination, gender-affirming care and research across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old wants the contraceptive implant but says, "Please don't tell my mum." A 14-year-old admitted with an overdose begs you to keep it secret. A 16-year-old with a chronic illness refuses a treatment the parents want. These are not exotic edge cases. They are the everyday work of adolescent medicine, and the clinical skill they test is consent and confidential care. [10] [4]
Informed consent is permission given by someone who has the capacity to decide, has received the information a reasonable person would need, and is free from coercion. In children and adolescents this single idea splits into three linked concepts. Consent is the decision of someone with capacity. Parental permission is the authorisation of a parent or guardian for a child who lacks capacity. Assent is the age-appropriate agreement of the child, which you seek even when a parent gives permission. Mixing these up is the commonest exam and bedside error. [10] [11]
Decision-making capacity is the ability to understand the proposed care, retain the information, weigh the risks and benefits in your own situation, and communicate a choice. In many jurisdictions a young person who can do this — the Gillick competent minor in the United Kingdom, the mature minor in Australia, Canada and parts of the United States — may give valid consent in their own right. This is a capacity-based principle, not a magic birthday. [12] [13] [14]
Confidentiality is the duty to keep what a patient tells you private. With adolescents that duty is conditional, not absolute. You promise privacy, and you are honest about its limits: you will act if the young person is at serious risk of harm, if someone else is being hurt, or if the law requires you to report. Promising total secrecy you cannot keep is a trust injury waiting to happen. [4] [5] [2]
The skill in this topic is not reciting statutes. It is running an encounter where a young person feels safe enough to tell you the truth, while you hold the lawful limits and act when safety demands it. [1] [9]
Classification
Begin with the patient in front of you, then classify who can consent, what kind of consent it is, and how confidential the content is. [10]
Who can consent
Capable minor
Mature minor / Gillick
- Understands, retains, weighs, communicates
- Can consent in their own right
- Capacity is task-specific
- Still seek assent-style engagement and offer family involvement
Minor lacking capacity
Permission + assent
- Parent or guardian gives permission
- Seek the child's age-appropriate assent
- Give developmentally matched information
- Re-assess capacity as the young person matures
Statute-based minor consent
Service-specific
- Some services allow minor consent by law
- Commonly contraception, STI, mental health, substance use
- No capacity test needed for that service
- Local statute governs the detail — check it
Emancipated / looked-after
Special status
- Legal status may grant consent authority
- Looked-after children have a guardian or state authority
- Clarify who holds consent before treating
- Document the basis clearly
The categories overlap. A young person may be capable for a contraception decision and still benefit from a parent's input on a complex chronic-illness choice the same afternoon. Judge each decision on its own merits. [12] [13]
The kind of consent and the kind of content
- Routine low-risk care (a blood pressure, an immunisation offered routinely): standard consent with information and capacity. [10]
- Sensitive care (contraception, STI testing, mental health, substance use, gender-affirming care, pregnancy): raises both consent and confidentiality stakes together. [4] [17]
- High-stakes or contested care (a capable minor refusing life-sustaining treatment, or a parent–adolescent conflict): slow down, assess capacity in detail, and seek ethics and legal advice. [12] [14]
- Research: generally needs the young person's assent plus parental permission, with capacity-based exceptions for mature minors in some jurisdictions and study types. [11] [12]
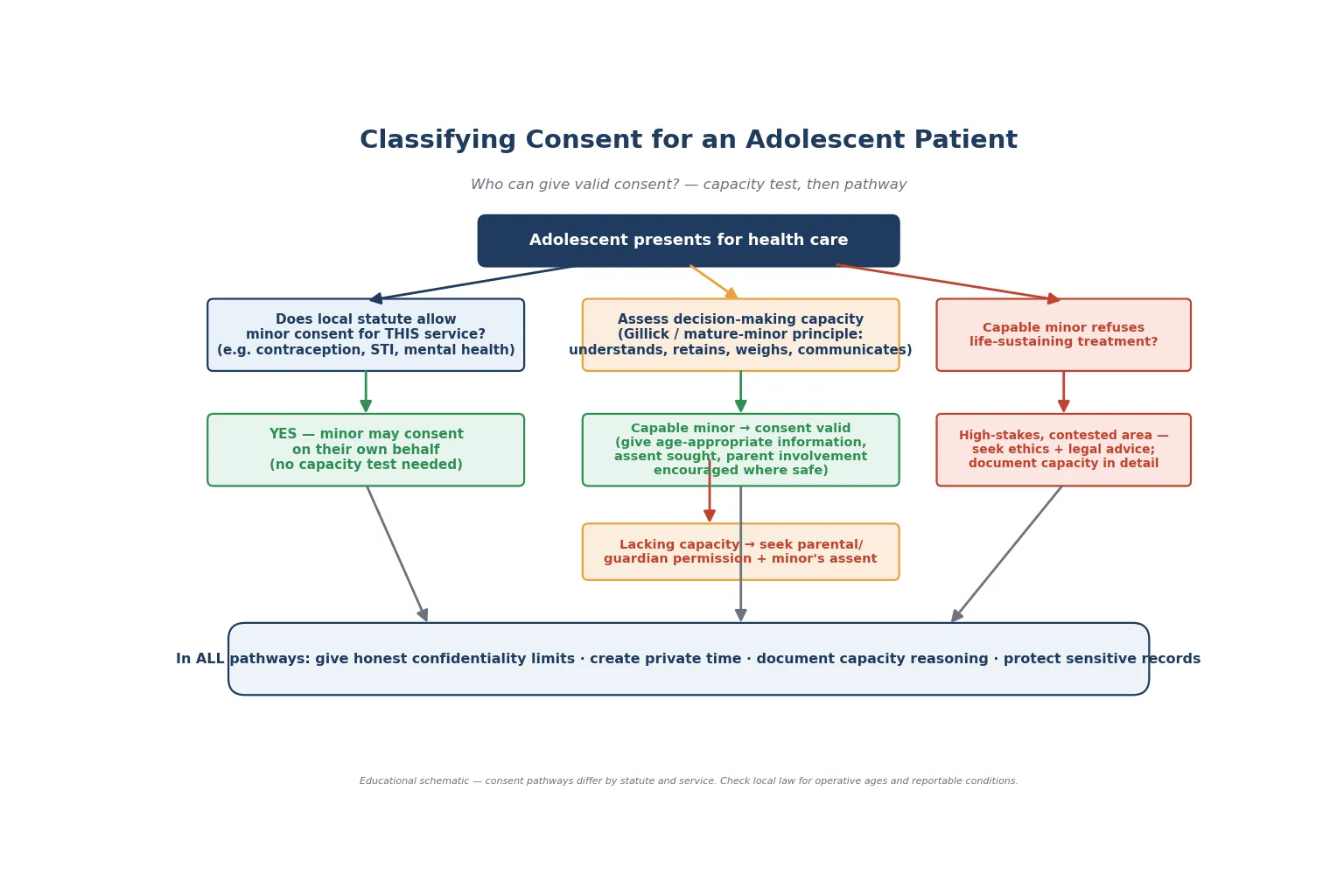
Read the figure like this: every pathway still demands an honest confidentiality statement and protected records. Capacity routes the decision; confidentiality protects the relationship. [4] [10]
Epidemiology & Risk Factors
Confidentiality failure is common, and it is measurable. When Ford randomised adolescents to receive an explicit confidentiality assurance, the young people were more willing to disclose sensitive information and to say they would seek future health care. The assurance changed behaviour, not just comfort. [1] [2]
The flip side is the risk. When a young person expects that parents or the system will see everything, sexual activity, substance use, suicidality and abuse stay hidden. Delayed and avoided care follow. The mechanism is simple: trust enables disclosure, and disclosure enables appropriate care. [1] [4]
Some groups carry extra risk when confidentiality is weak. Sexual minority and gender-diverse youth, young people seeking sexual and reproductive care, those with mental-health or substance concerns, and those experiencing abuse are all disproportionately exposed to the consequences of a breach. [4] [5]
Modern electronic records have added new failure modes. Patient portals, after-visit summaries, billing statements and insurance explanation-of-benefit letters can surface contraception, mental-health and sexual-health content to a parent's view by default. The open-notes era and the 21st Century Cures Act in the United States have made this a live clinical problem. [6] [7]
Parent attitudes matter too. Many parents accept private time when its purpose is explained as normal developmental care. Skipping private time is not efficiency — it is a quality failure that suppresses disclosure. [3] [8]
Pathophysiology
You do not need a neuroscience lecture to consent a young person well. You do need a working model of why capacity and confidentiality behave the way they do. [13]
Adolescent development brings rising autonomy alongside still-maturing cognitive control. The reward system matures ahead of the prefrontal regulatory system, which supports identity and exploration and also explains why young people can reason soundly yet still act on impulse under peer or affective pressure. This is why capacity is judged on understanding and reasoning, not on a single age. [13]
Capacity is task-specific. The same 14-year-old may be able to consent to a course of antibiotics and yet not to a complex bariatric procedure. Stakes, complexity, reversibility and the time available to decide all shift the bar. Re-assess at each new decision rather than stamping "capable" once. [12] [14]
The trust–disclosure chain is the real mechanism. A young person who trusts that sensitive content stays private will tell you about a coercive partner, daily vomiting, or a suicide plan. Strip away that trust — through a breach, a parent in the room, or a portal leak — and the information stops. You cannot treat what you never hear. [1] [4]
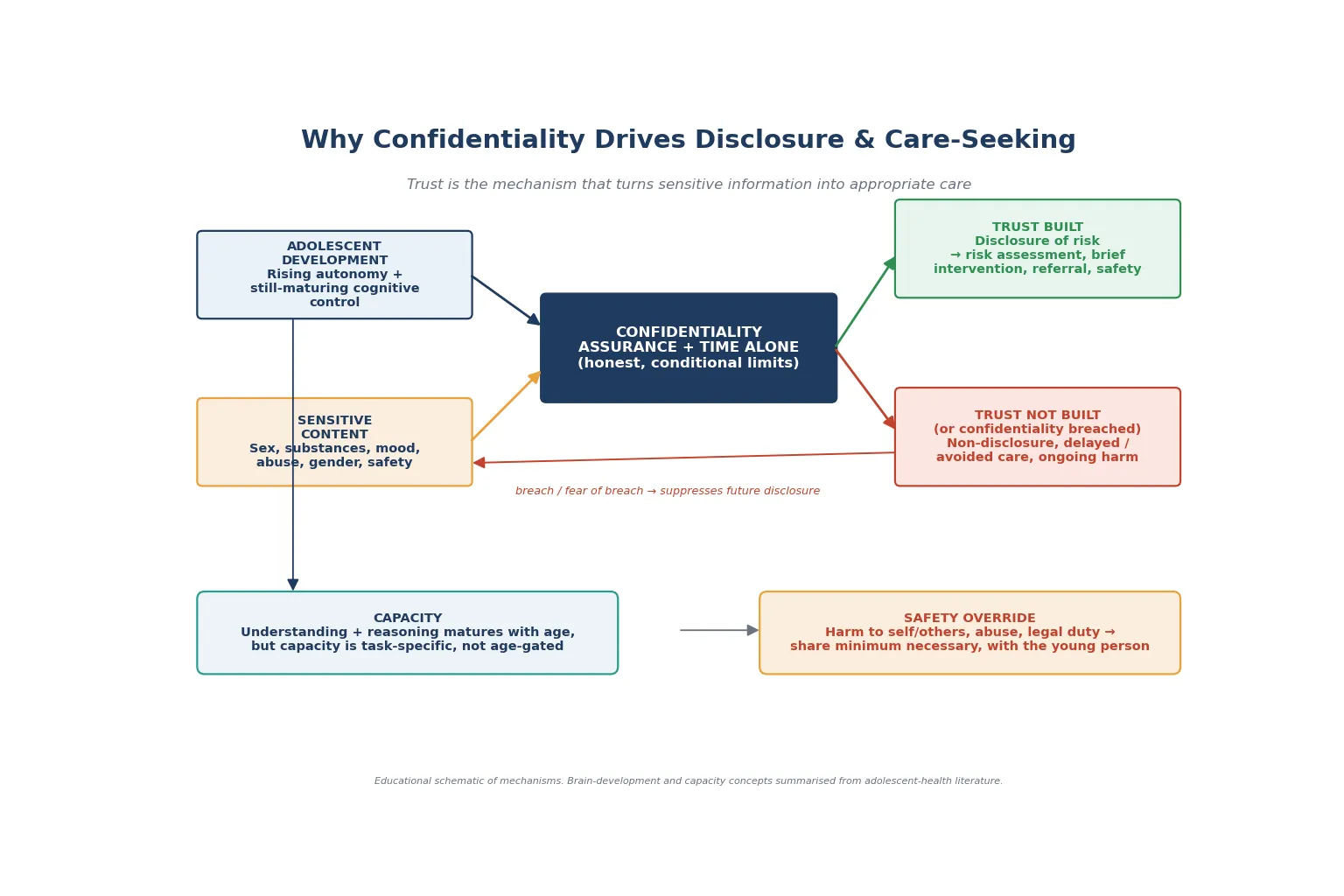
Read the figure like this: the override arrow does not undo the trust arrow. An ethical override, told to the young person and kept proportionate, can preserve the relationship. A silent, avoidable leak destroys it. [4] [7]
Trauma and adversity change how authority and information-giving feel. A young person who has been controlled or abused may experience even routine consent questions as a threat. Trauma-informed pacing — explaining why you ask, giving choices where you can — is part of consent skill, not a separate niceness module. [4] [9]
Clinical Presentation
Consent and confidentiality rarely announce themselves. They surface as small moments inside an ordinary visit. [10]
The organised encounter looks calm. You greet the young person first, set a joint agenda, explain the plan for private time, state the confidentiality limits, assess capacity for the decision at hand, give information with teach-back, and close with a shared plan. [2] [3]
The high-risk patterns hide inside "well" visits. A parent answers every question. A young person is vague about why they came, or asks that something "not go in the notes." A capable adolescent suddenly refuses a treatment the parent wants. A portal message about contraception lands in a parent's inbox. Each is a presentation of a consent or confidentiality problem. [1] [6] [12]
A covert confidentiality worry may show as reluctance to examine, refusal of a test, or a whispered request that a parent not be told. These are cues to create private space and ask, gently, what the worry is. [4]
The capacity question presents as a decision a young person is making — or refusing — that you are unsure they fully understand. Your job is to assess, not to assume. A neat school uniform and a cooperative manner do not prove capacity any more than a disability proves its absence. [12] [14]
Differential Diagnosis
In this topic the differential is less "which disease" and more "what is really going on with this decision or this secrecy." [14]
| What it looks like | The real question to answer | Do not miss |
|---|---|---|
| "They won't engage" | Capacity, fear, or unmet information need? | Coercion, untreated mental illness |
| "They want secrecy" | Appropriate privacy, or secrecy hiding risk? | Abuse, self-harm, exploitation |
| Adolescent refuses treatment | Capable autonomous refusal, or decision driven by illness? | Depression, delirium, intoxication |
| Parent opposes minor's choice | Is this service one the minor can lawfully consent to? | Statute-based minor consent rights |
| "Non-adherent teen" | A consent or voluntariness problem? | Coercion, side-effect fear, cost |
| Apparent "breach" | A lawful, proportionate disclosure, or an avoidable leak? | Portal and billing defaults |
Separate genuine lack of capacity from disagreement, fear and unmet information needs. A young person who refuses may be exercising autonomy, may be terrified, or may simply not have been told what they needed. The remedy differs for each. [12] [14]
Separate appropriate privacy-seeking from secrecy that signals risk. Wanting contraception kept from a parent can be healthy autonomy; wanting fresh self-harm marks kept secret is a safety signal that may need an override. [4] [1]
Clinical & Bedside Assessment
1. Open and set the frame
Greet the young person first, then the parent. Set a joint agenda. Explain that you will spend time with everyone, then private time with the young person, then bring the plan back together. [2] [3]
2. Say the confidentiality script aloud
"What we talk about privately stays private, unless I become worried that you are not safe, that someone else is being hurt, or the law says I must act. If that happens, I will tell you what I need to do and we will plan it together as much as possible." Then check the young person understands. [4] [5] [2]
3. Create time alone
Ask the parent to step out. If they resist, normalise it: this is standard adolescent care, like teaching self-management. Parent perspectives research shows many will accept private time when its purpose is explained. [3] [8]
4. Assess decision-making capacity at the bedside
Walk the young person through the decision and check four things: do they understand the proposed care and its alternatives, retain the information long enough to decide, weigh it in their own situation, and communicate a stable choice? Use teach-back — "tell me in your own words what will happen." Capacity is task-specific, so judge this decision, not the whole person. [12] [10] [14]
5. Assess voluntariness
Ask gently who else is involved in the decision and whether anyone is pressuring them. Screen for coercion and intimate partner violence without destroying rapport. A capable choice made under threat is not voluntary. [4] [9]
6. Give information and check understanding
Use plain language matched to the young person's stage. Cover what the care is, the main benefits, the real risks, the alternatives, and what happens if they do nothing. Confirm understanding before you accept consent. [10] [11]
7. Involve interpreters and support people correctly
Use trained interpreters for any language need. Family members are not equivalent interpreters for sensitive or confidential content, because they are the people the young person may be keeping things from. [4] [9]
8. Document the reasoning
Record that you assessed capacity and on what basis, what information you gave, that consent (or assent plus permission) was obtained, and your confidentiality reasoning. Documentation is part of the medicine, not paperwork. [10] [5]
Investigations
There are no laboratory tests for capacity or confidentiality. The "investigations" here are structured aids and the contextual assessments that surround a capacity judgement. [12]
Capacity assessment is primarily a clinical interview, as above. In a few situations a mental-state or cognitive assessment helps — for example, when depression, intoxication, delirium or an acute psychiatric illness may be clouding the decision. Treat the reversible driver where you can, then re-assess. [12] [14]
Validated screening tools sit around the capacity work without replacing it. A positive mood, substance or safety screen tells you a young person needs help; it does not by itself prove or disprove capacity for a separate decision. [9] [4]
Pregnancy, STI and drug testing are indicated by the history and follow local consent rules for that service. Order entry, portal results and billing can themselves leak confidential content, so consider how the result will be returned before you order it. [4] [6]
Ethics and legal consultation is the right "investigation" when the stakes are high — a capable minor refusing life-sustaining treatment, or a genuine dispute between a capable adolescent and parents. Do not absorb that risk alone. [12] [14]
Management — Resuscitation
A confidential encounter can become an emergency in one sentence of disclosure. [1]
- Stabilise physiology first if needed: ABCDE, glucose, intoxication, overdose complications. [9]
- Secure immediate safety for suicidality: do not leave a high-risk young person alone; remove means if you safely can; escalate to ED or crisis teams per your local pathway. [4]
- Break confidentiality ethically when a lawful threshold is crossed. Tell the young person what you must share and why. Share the minimum necessary with the people who need it. [4] [5]
- Run the safeguarding pathway for abuse, assault or coercive control in parallel with the medical care. [4]
- Do not negotiate away urgent transfer just because the visit was booked as routine. [9]
In an emergency where usual consent cannot be obtained, provide life-saving treatment under the emergency or best-interests doctrine, then return to consent and information-sharing as soon as the young person can engage. [10] [11]
Management — Definitive & Stepwise
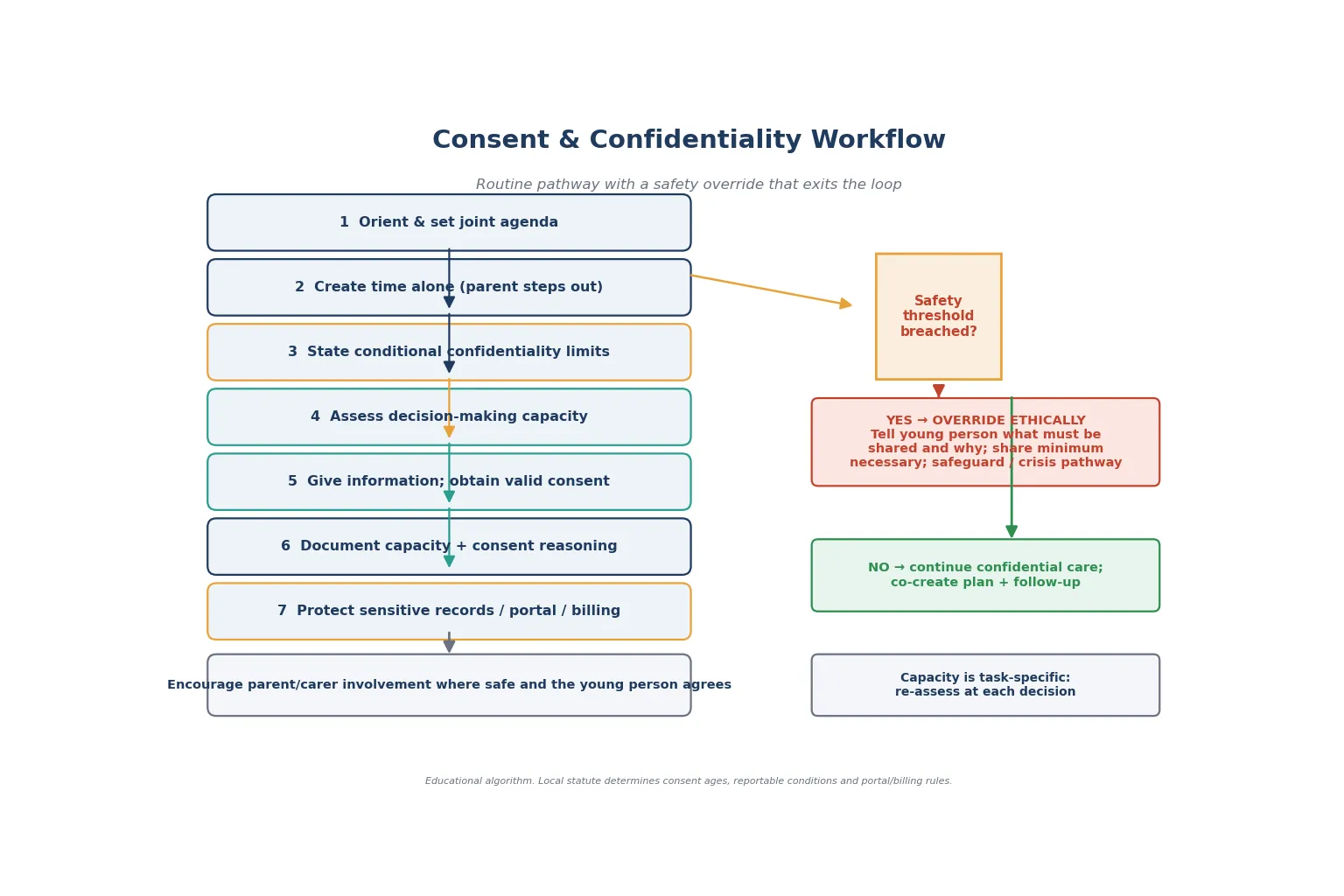
Read the figure like this: the override is a branch, not a betrayal. Done well — told, proportionate, documented — it can preserve the relationship. [4]
The routine consent and confidentiality pathway
- Orient and agenda-set with both parties. Greet the young person first. [2] [3]
- Create time alone and say the conditional confidentiality script. [4] [2]
- Assess capacity for the decision at hand, task by task. [12] [10]
- Give information matched to the young person's stage; confirm with teach-back. [10] [11]
- Obtain valid consent from the young person if capable, or parental permission plus assent if not. [10] [11]
- Encourage parent or carer involvement wherever it is safe and the young person agrees. Confidentiality and family are not opposites. [3] [8]
- Document capacity, consent and confidentiality reasoning. [5] [10]
- Protect the records. Use local sensitive-note and confidential-content workflows so that portals, after-visit summaries, billing and insurance letters do not leak. [6] [7]
- Build a shared plan the young person can own, with follow-up and an after-hours safety-net. [4] [9]
Service-specific consent
- Contraception and sexual health: minors can often consent in their own right under statute for contraception, STI testing and treatment. Assess capacity where the statute does not cover the service. Use local prescribing protocols for product detail rather than fabricating doses. [4] [17]
- Vaccination: minor-consent models can improve adolescent vaccine uptake, but consent rules vary by jurisdiction and vaccine. When an adolescent wants to consent and a parent disagrees, apply your local statute and document the reasoning. [16] [17] [15]
- Mental health and substance use: many jurisdictions allow minors to consent to mental-health and substance-use treatment. Capacity may be impaired by the illness itself, so re-assess as the young person recovers. [4] [12]
- Gender-affirming care: follow the current local clinical pathway, with careful capacity assessment, valid consent, and confidentiality protected from family where rejection is a risk. [4]
- Research: seek the young person's assent plus parental permission, with capacity-based exceptions for mature minors where your jurisdiction and ethics committee allow. [11] [12]
Follow-up intensity
- Low-risk, clear decision, safe young person: routine confidential follow-up. [10]
- New disclosure or contested decision: early review (days to weeks) to re-confirm understanding and the plan. [4]
- High risk or recent override: same-day or next-day crisis, ED or safeguarding pathway as above. [4] [9]
Specific Subtypes & Scenarios
Capable minor refuses life-sustaining treatment. This is the hardest scenario. Assess capacity in detail — understanding, retention, weighing, voluntariness, stability over time. Even a clearly capable refusal of death-preventing care is high-stakes and contested across jurisdictions. Slow down, involve ethics and legal teams, and treat any treatable driver of the refusal. Do not collapse the case into "because they are under 18 they cannot refuse." [12] [14] [10]
Parent disagrees with a minor's choice. First ask whether this is a service the minor can lawfully consent to. If yes, the capable minor's consent stands, but good practice is to keep negotiating with the family wherever it is safe. If the minor lacks capacity, parental permission governs — yet the young person's assent and views still carry weight. [17] [10]
Reproductive and sexual-health care. Contraception, STI testing and treatment, pregnancy and emergency contraception commonly fall under statute-based minor consent. Capacity still matters for services the statute does not cover. Plan how results and any prescribing will be returned confidentially before you act. [4] [17]
Vaccination consent. The same adolescent may be able to consent to vaccination under a minor-consent model in one jurisdiction and need parental consent in another. The evidence base on adolescent autonomy and minor consent for vaccines spans HPV through COVID-19 and shows that consent design changes uptake. [15] [16] [17] [18]
Gender-affirming care. Valid consent, careful capacity assessment and confidentiality are central, especially where family rejection is a real risk. Follow the current local clinical pathway and keep the young person's chosen name and pronouns in the record appropriately. [4]
Mental-health and substance-use treatment. Many jurisdictions allow minor consent for these services. Watch for the illness itself impairing capacity — an adolescent in a severe depressive episode may not be weighing the decision freely. Re-assess as they recover. [12] [4]
Emergency, ward and inpatient settings. In an emergency treat first under best interests, then return to consent. On the ward, create private time deliberately — parents and roommates are usually present, and confidential content will not surface on its own. [10] [4]
Looked-after, justice-involved, migrant and refugee youth. Clarify who holds consent authority before treating — it may be a guardian, a state authority or the young person themselves. Reconstruct history actively. Never use family members or carers as interpreters for sensitive content. [4] [9]
Research. Obtain the young person's assent plus parental permission, with capacity-based exceptions for mature minors where your ethics committee and jurisdiction permit. Pay the same attention to confidentiality of research data. [11] [12]
Complications & Pitfalls
- Skipping private time and the confidentiality statement "because they seem fine." [2] [3]
- Promising absolute secrecy you cannot keep. [4]
- Treating capacity as age-gated rather than task-specific. [12] [14]
- Parent present for the sexual, substance or safety history. [1] [4]
- Portal, billing or insurance letters disclosing contraception, mental-health or sexual-health visits. [6] [7]
- Failing to re-assess capacity after a change in mental state or circumstance. [12]
- An avoidable or disproportionate breach that deters future disclosure. [4] [1]
- Conflating capacity with the legal authority to decide. [14]
- Missing coercion or intimate partner violence that overrides voluntariness. [4] [9]
- Failing to involve a parent when it is safe and the young person agrees, missing a source of support. [3] [8]
Prognosis & Disposition
In this topic, prognosis means the trajectory of trust, safety and autonomy, not a disease stage. [10]
Routine disposition: a clear, low-risk decision made by a capable young person who is safe, understands the plan, and can re-access care. Plan routine confidential follow-up. [10]
Early-review disposition: a new disclosure, a contested decision, or an incomplete assessment that needs return with trust built. Bring them back in days to weeks, not months. [4]
Urgent disposition: active suicide risk, assault, abuse, medical instability, or severe intoxication with impaired capacity. Use ED, crisis or safeguarding pathways the same day. [4] [9]
Safety-net explicitly: who to call tonight, when to come back sooner, and how confidentiality will work with parents after any override. Close the loop after ethics, legal, mental-health, sexual-health or social-work involvement. [5] [4]
Over time, disposition should build the young person's capacity and autonomy. Late-adolescent care should include planning for consent to transfer information to adult services at transition. [12] [10]
Special Populations
Indigenous adolescents. Cultural safety and respect for family and community decision-making norms belong in the consent conversation. Racism is a health exposure. Use local pathways and culturally safe services. [4]
Migrant and refugee youth. Use trained interpreters, never family members, for sensitive content. Trauma-informed pacing and catch-up of missed care matter. [4] [9]
Out-of-home care and youth justice. Clarify consent authority, assume incomplete records and higher mental-health and sexual-health risk, and reconstruct history actively. [4]
Gender and sexual diversity. Confidentiality, chosen name and pronouns, and tailored care are central. Watch for family rejection, bullying and minority stress. [4]
Disability and neurodiversity. Adapt communication and capacity assessment to ability, and use supported decision-making. Avoid the diagnostic overshadowing that wrongly assumes incapacity. [12] [14]
Chronic disease and technology dependence. Build autonomy and plan the transition of consent authority and information-sharing to adult care over years, not in a birthday letter. [10]
Rural and remote. Small-community dual relationships threaten confidentiality. Create private space deliberately, including on telehealth where a parent may be off-camera. [4]
Pregnant and parenting adolescents. Layered capacity applies: they may be deciding for themselves and, after birth, for their own child. Keep safeguarding assessment in view. [4]
Evidence, Guidelines & Regional Differences
The confidentiality assurance evidence. Ford's randomised trial showed that an explicit assurance increased adolescents' willingness to disclose sensitive information and to seek future care. This is the empirical backbone for treating confidentiality as clinical quality. [1] [2]
Contemporary guidance. The American Academy of Pediatrics 2024 confidentiality policy and technical report set out the modern practice standard, including electronic-record confidentiality. The open-notes and 21st Century Cures Act literature maps the new failure modes. [4] [5] [6] [7]
The consent framework. The AAP clinical report on informed consent in paediatric decision-making, and the older Committee on Bioethics statement on consent, parental permission and assent, remain the conceptual scaffolding. [10] [11]
Capacity and the mature minor. Weithorn maps when a minor's legal competence to make health-care decisions matters. Steinberg asks whether adolescent brain-development research actually informs the mature-minor doctrine. Salter argues the field has conflated capacity with authority — a useful viva-level point. [12] [13] [14]
Vaccination consent. The SAHM position paper, Ford on minor consent and vaccine delivery, Zimet on HPV consent, and Mihaly tracing adolescent autonomy from HPV to COVID-19 together show how consent design changes uptake. [16] [17] [15] [18]
ANZ: the mature-minor principle applies; capacity is assessed at the bedside, with state and territory statutes governing operative consent ages and mandatory-reporting duties. Trained interpreters are required for language needs. UK: Gillick competence and the Fraser guidelines frame capacity-based consent for under-16s in relevant services; those aged 16 and over are generally presumed competent to consent. GMC 0–18 years guidance applies. Apply current local legal teaching. US: mature-minor doctrines vary by state; minor-consent statutes commonly cover reproductive, mental-health and substance-use services. The Cures Act and open notes reshape electronic-record confidentiality. Canada: provincial consent legislation varies; the Greig Health Record and CPS guidance frame preventive care. Check the relevant province.
State the principle, and check local law. Do not invent a universal consent age or a universal reporting threshold — they do not exist. [12] [4]
Exam Pearls
- Open every answer with capacity + information + voluntariness, then the conditional confidentiality script. [10] [4]
- Capacity is task-specific, not age-gated. Assess at the bedside. [12] [14]
- Gillick competence (UK) and the mature-minor doctrine (US/Canada/AU) are principles, not fixed ages — state the principle, check local statute. [12] [13]
- Assent is sought from the child; permission from the parent; valid consent needs capacity, information and voluntariness. [11] [10]
- Confidentiality limits: serious harm to self or others, abuse, and other legal mandates. [4]
- An override is told to the young person, kept to the minimum necessary, and documented — ethical, not silent. [4] [5]
- Portal, billing and insurance explanation-of-benefit letters are modern confidentiality traps examiners reward. [6] [7]
- Never use family members as interpreters for sensitive content. [4] [9]
- Encourage parent involvement where safe and agreed — confidentiality and family are not opposites. [3] [8]
- A capable minor refusing life-sustaining treatment is high-stakes — seek ethics and legal advice. [12] [14]
CIVIC for a confidential adolescent encounter
References
- [1]Ford CA Influence of physician confidentiality assurances on adolescents' willingness to disclose information and seek future health care. A randomized controlled trial. JAMA, 1997.PMID 9307357
- [2]Ford CA Delivery of confidentiality assurances to adolescents by primary care physicians. Archives of pediatrics & adolescent medicine, 1997.PMID 9158445
- [3]Miller VA Adolescents Spending Time Alone With Pediatricians During Routine Visits: Perspectives of Parents in a Primary Care Clinic. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2018.PMID 29887486
- [4]Chung RJ Confidentiality in the Care of Adolescents: Policy Statement. Pediatrics, 2024.PMID 38646690
- [5]Chung RJ Confidentiality in the Care of Adolescents: Technical Report. Pediatrics, 2024.PMID 38646698
- [6]English A Adolescent Consent and Confidentiality: Complexities in Context of the 21st Century Cures Act. Pediatrics, 2022.PMID 35531643
- [7]Pasternak RH 21st Century Cures Act ONC Rule: Implications for Adolescent Care and Confidentiality Protections. Pediatrics, 2023.PMID 37010402
- [8]McKay EA Parents' Perspectives on Confidentiality in Clinical Preventive Services for Adolescents. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2025.PMID 40580168
- [9]Cohen E HEADSS, a psychosocial risk assessment instrument: implications for designing effective intervention programs for runaway youth. Journal of adolescent health : official publication of the Society for Adolescent Medicine, 1991.PMID 1772892
- [10]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [11]American Academy of Pediatrics Committee on Bioethics Informed consent, parental permission, and assent in pediatric practice. Pediatrics, 1995.PMID 7838658
- [12]Weithorn LA When Does A Minor's Legal Competence To Make Health Care Decisions Matter? Pediatrics, 2020.PMID 32737229
- [13]Steinberg L Does recent research on adolescent brain development inform the mature minor doctrine? Journal of medicine and philosophy, 2013.PMID 23607975
- [14]Salter EK Conflating Capacity & Authority: Why We're Asking the Wrong Question in the Adolescent Decision-Making Debate. The Hastings Center report, 2017.PMID 28074581
- [15]Zimet GD Adolescent Consent for Human Papillomavirus Vaccine: Ethical, Legal, and Practical Considerations. The Journal of pediatrics, 2021.PMID 33484694
- [16]English A Adolescent consent for vaccination: a position paper of the Society for Adolescent Health and Medicine. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2013.PMID 24054082
- [17]Ford CA Minor consent and delivery of adolescent vaccines. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2014.PMID 24074605
- [18]Mihaly LK From Human Papillomavirus to COVID-19: Adolescent Autonomy and Minor Consent for Vaccines. Journal of pediatric health care : official publication of National Association of Pediatric Nurse Associates & Practitioners, 2022.PMID 35941049