Paeds · adolescent-and-young-adult-medicine
Digital media, gaming and cyberbullying
Also known as Screen time and adolescent mental health · Problematic internet use · Internet gaming disorder · Cyberbullying and online victimisation · Sexting and online sexual solicitation · Social media harm reduction
A fellowship approach to the digital life of young people: how to ask about screen time, social media, gaming, cyberbullying and online sexual risk; how to separate normative use from the use that harms; and how to build a harm-reduction plan that keeps a young person safe and engaged rather than lectured into silence.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A registrar sees a 14-year-old for acne. The phone never leaves the teenager's hand. "Sleep's fine," they say, dark-eyed at noon. The visit closes in seven minutes. Three weeks later the same young person is in the emergency department after taking pills because a group chat turned on them. The missed work was not a rare diagnosis. It was an online life that nobody asked about. [4] [8]
Digital media is now a developmental environment, not an accessory. Screen time, social media, gaming and online interaction are where adolescents form identity, build peer relationships, seek information about health and sexuality, and explore risk. The American Academy of Pediatrics frames media use as a health topic that paediatricians must discuss at every well-child visit from infancy onward, shifting the question from "how much screen time" to "what is the content, context and consequence of the use." [1] [2]
Digital-media harm is the cluster of mental-health, sleep, developmental and safety harms that arise when exposure meets vulnerability: depression and anxiety linked to heavy or comparative social-media use, sleep loss from night-time device use, compulsive or disordered gaming, and the psychological injury of cyberbullying and online sexual exploitation. The defining clinical point is that the same technology is benign for most and harmful for a vulnerable few, so the task is targeted assessment rather than blanket prohibition. [12] [5]
Cyberbullying is aggression — harassment, humiliation, threats, exclusion or rumour — delivered through digital channels, distinguished from offline bullying by its reach, permanence, perceived anonymity, and the fact that it follows the young person home and into the bedroom. [3] [4]
Core sequence of a digital-media risk encounter
Screen all
Ask every adolescent about use, content, contacts, cyberbullying, sleep and mood — without judgement.
Assess function
Impairment, mood/sleep effects, compulsive-use signs, victimisation, coercion.
Classify
Normative use vs use causing impairment, danger or instability.
Brief intervention
Motivational interviewing, personalised feedback, a family media plan.
Harm-reduction plan
Sleep-protective schedule, blocking/privacy, safer-use, parental controls.
Red-flag exit
Suicidality, exploitation, leaked images, crisis → acute safety and safeguarding.
Classification
Classify digital-media risk along four exposures, filter every finding through a function test, and run the whole picture through a content–contact–conduct–compulsion frame. The exposure tells you what to ask; the function test tells you whether to worry; the frame tells you where the harm sits. [8] [1]
The four exposures
The exposures that matter clinically are screen time and social media (amount, timing, content, comparative behaviour), gaming and internet use (compulsion, neglect, monetisation, in-game contact), cyberbullying (victimisation and perpetration), and sexting and online sexual solicitation (consensual sharing, non-consensual sharing, grooming, exploitation). Each has its own risk profile and its own intervention. [1] [3]
The function filter
Use does not equal harm. The clinical discriminator is function: does the use sit alongside intact sleep, mood, school, friendships and safety, or is it accompanied by impairment, danger and instability? Sleep loss, school decline, mood change, weight change, withdrawal and neglect of self-care are the signals that move a behaviour from normative to concerning. [5] [12]
Content, contact, conduct, compulsion
A practical classification frame splits online risk into content risks (what a young person sees — violent, sexual, pro-self-harm or extremist material), contact risks (who reaches them — predators, extremists, groomers), conduct risks (how they behave — bullying, sexting, aggression) and compulsion risks (how the technology captures attention — variable-ratio rewards that drive problematic or disordered use). This frame maps cleanly onto safeguarding language and onto interventions. [8]
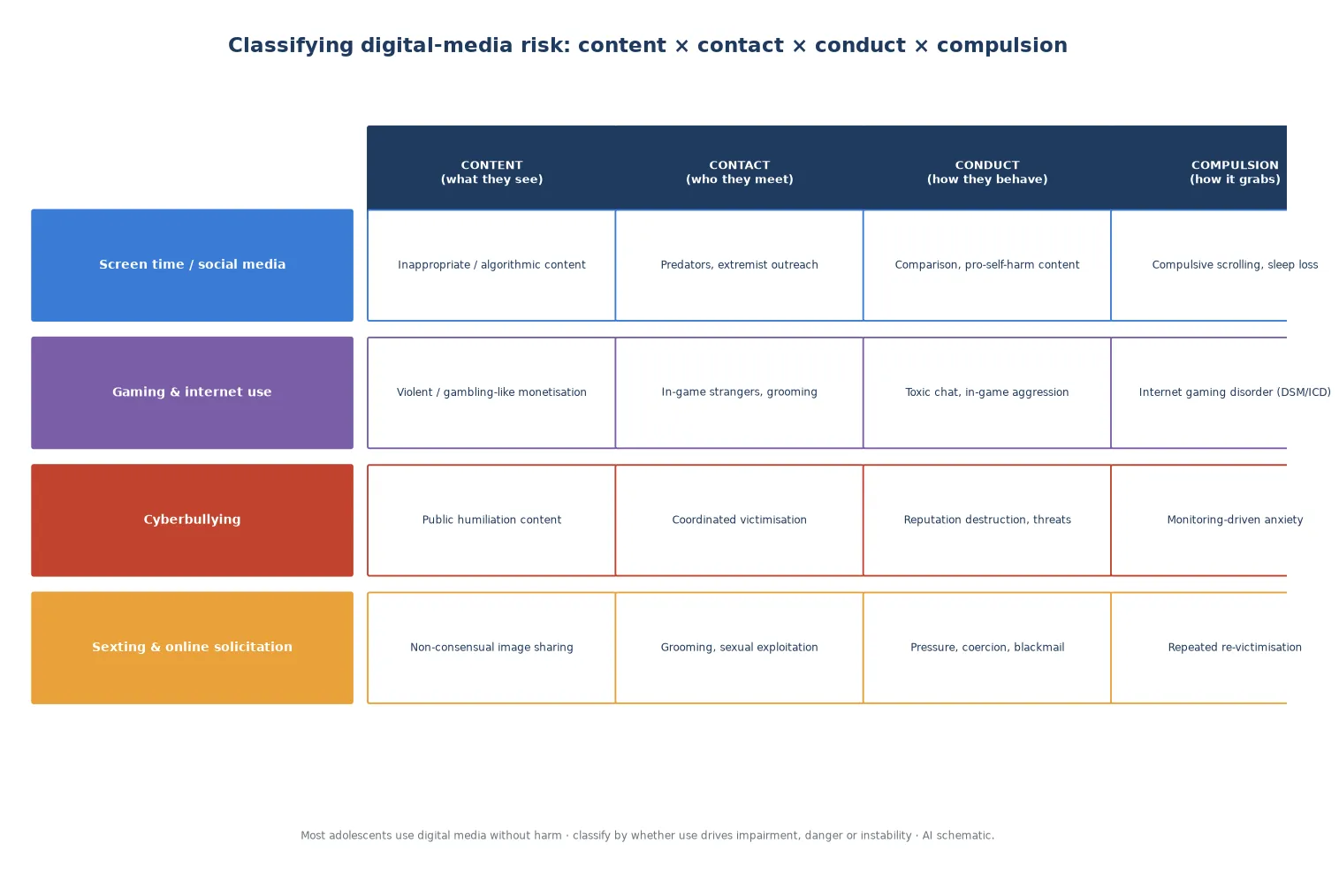
Read the figure like this: the same exposure (say, social media) generates different harm depending on whether the problem is content, contact, conduct or compulsion. A blanket "reduce screen time" instruction addresses none of them precisely. [12]
Normative use
No impairment
- Use alongside intact function
- Sleep, mood, school preserved
- Brief reinforcement and safety net
- No treatment needed
At-risk use
Function declining
- Sleep loss, mood dip, school slip
- Comparative or compulsive features
- Brief intervention + media plan
- Timed review
Harmful use
Impairment or danger
- Depression, self-harm, exploitation
- Disordered gaming, cyberbullying crisis
- Acute safety + mental-health pathway
- Safeguarding as indicated
Epidemiology & Risk Factors
Nearly every adolescent in high-income settings is online daily, and most use social media. High engagement is normal; the epidemiological question is which patterns track with harm. Systematic reviews find cyberbullying affects a substantial minority of adolescents, with US middle- and high-school prevalence estimates commonly in the 10–40 per cent range depending on definition and method. [3] [1]
Cyberbullying victimisation is strongly and consistently associated with self-harm and suicidal behaviour. A systematic review found cyber-victims and cyber-perpetrators both had roughly doubled odds of self-harm and suicidal ideation compared with non-involved peers, and the association held after accounting for offline victimisation in several studies. [4]
Screen time and mental health show a more contested picture. Longitudinal adolescent data link higher screen time — particularly social-media and device time — to increasing depressive symptoms over time, while the prospective ABCD cohort finds associations between screen time and later internalising and externalising problems. The effect sizes are modest and the field struggles to separate cause from consequence, which is exactly why function — not hours — drives clinical decisions. [5] [11]
Online sexual risk is common but under-asked. A meta-analysis found a substantial minority of youth had sent or received sexts, prevalence rising with age, and non-consensual forwarding is the point where consensual sharing becomes harm. Retrospective data confirm that online sexual solicitation and grooming of minors are genuine, recurring experiences that young people rarely disclose spontaneously. [7] [9]
Pathophysiology
You do not need a full neuroimaging lecture to counsel well. You do need a usable model of why digital exposure moves the developing adolescent brain, because it explains why harm reduction fits and why a "just delete the app" ultimatum often fails. [12]
The reward pathway. Social-media feeds, gaming rewards and notifications operate on variable-ratio reinforcement schedules — the same schedule that makes slot machines compelling. Likes, loot boxes, streaks and messages deliver unpredictable rewards that drive dopamine-mediated reinforcement. Because the adolescent prefrontal control system matures later than the reward system, the pull can outrun self-regulation, which is the mechanism behind compulsive and disordered use. [12] [10]
The sleep pathway. Night-time device use displaces and fragments sleep through blue-light exposure, arousal from content, and incoming notifications. Short and delayed sleep worsens mood, attention and impulse control, creating a feed-forward loop that looks clinically like depression or inattention but is partly sleep-driven. [5] [11]
The social-comparison and threat pathways. Curated, idealised feeds drive upward social comparison and fear of missing out, strongest in young people already vulnerable to anxiety or low self-worth. Cyberbullying and victimisation activate threat and stress systems with the added cruelty that the content persists and re-victimises — a post does not heal like a bruise. Perceived social isolation is itself elevated in the most frequent social-media users. [6] [4]
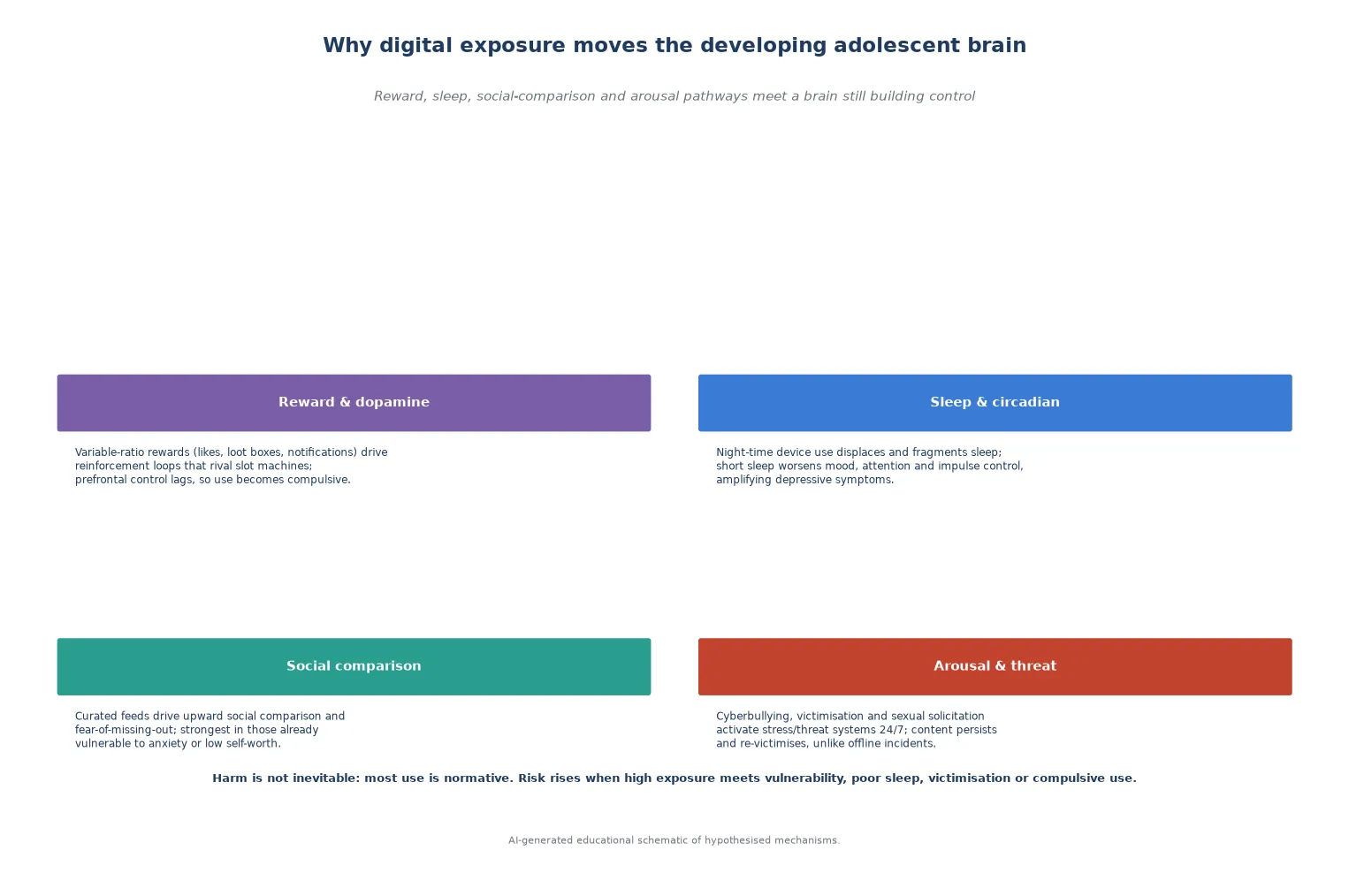
Read the figure like this: harm is not the device. It is the meeting of a persuasive technology with a vulnerable, sleep-deprived, socially-driven brain. Your interventions target the meeting point, not the hardware. [12]
Clinical Presentation
Digital-media risk presents across a spectrum, and the dangerous presentations are often quiet. A young person does not usually present with "problematic internet use" on the label — they present with the downstream effects, and the online cause has to be asked about directly. [1] [8]
Normative presentation: a young person engages, uses screens and social media, but sleep, mood, school and friendships are intact. The task is brief reinforcement, a family media plan, and a safety net. This is the most common encounter and must not be pathologised. [1]
At-risk presentations hiding in ordinary visits: the tired adolescent whose sleep reversal is blamed on laziness; mood decline with a new phone; school refusal after a social-media incident; weight loss alongside compulsive gaming; an anxious teen whose self-worth tracks their follower count; the young person who flinches at a notification. Each is a door into a digital-media assessment, not a personality flaw to be dismissed. [5] [4]
Acute and harmful presentations: a cyberbullying crisis with suicidality; self-harm triggered by online events; non-consensual sharing of an intimate image (sexting that has become a safeguarding and legal event); disclosure of online grooming or sextortion; a gaming-affected young person who has neglected food, hygiene, education and relationships; an acute mental-health presentation where the digital context is the trigger. [4] [9]
Differential Diagnosis
In this domain the differential is "what is driving the presentation, and is the digital behaviour cause, consequence, or coincidental." [12]
| What it looks like | Safer framing question | Do not miss |
|---|---|---|
| Depression with heavy screen use | Is the use driving the mood, or is a depressed teen self-soothing online? | Underlying mood disorder, suicidality |
| School refusal after online incident | Was there cyberbullying, leaked images or a relationship breakup? | Ongoing victimisation, exploitation |
| Fatigue and inattention | How much sleep, and when does the device go off? | Sleep displacement, ADHD, iron deficiency |
| Gaming all day in holidays | Is function otherwise intact, or is there neglect and compulsion? | Internet gaming disorder, depression |
| "Sexting" disclosure | Consensual sharing, or coercion and non-consensual forwarding? | Grooming, sextortion, image-based abuse |
The core discriminator is function and safety, just as in other adolescent risk domains. Use alongside intact function is normative; use with impairment, danger or instability is not. Crucially, do not let an obvious diagnosis overshadow a hidden online driver — ask about digital life even when the label looks straightforward. [12]
Clinical & Bedside Assessment
1. Open and frame
Greet the young person first, secure time alone, and state conditional confidentiality with its limits. A non-judgemental, curious stance is essential — a lecture tone shuts down disclosure about online life faster than almost any other topic. [1] [4]
2. Ask the four exposures directly
Use plain, specific questions. Screen time and social media ("What apps? How late? How does it make you feel?"); gaming ("How much? Do you play past when you meant to stop? Does it crowd out sleep or friends?"); cyberbullying ("Has anyone been cruel to you online, or shared things about you? Have you been cruel to others?"); and online sexual risk ("Has anyone asked you for pictures, or pressured you? Have you shared anything you're worried about?"). A normalised opener — "I ask every young person this" — lowers the bar to disclosure. [8] [3]
3. Run the function filter
For any positive lead, test function: sleep amount and timing, mood and anxiety, school attendance and performance, eating and weight, friendships and withdrawal, and safety. Function — not hours of use — is what moves a behaviour from normative to concerning. [5] [11]
4. Assess cyberbullying and online sexual risk in depth
When cyberbullying is disclosed, ask about content, duration, perpetrator, reach, whether images are involved, and the impact on mood and safety — then screen for suicidality. When sexting or solicitation is disclosed, distinguish consensual sharing from coercion, grooming and non-consensual forwarding; ask about adult contact, gifts, threats and blackmail; and consider exploitation and trafficking. [4] [9]
5. Screen for suicidality and assess compulsive-use features
A digital-media disclosure with any mood lead must trigger a suicide screen (ideation, plan, intent, prior attempts, means, protective factors, ability to keep safe). For gaming and internet use, probe compulsive features: preoccupation, tolerance, withdrawal, loss of control, escapism, deception about use, and functional impairment — the markers of internet gaming disorder. [4] [10]
6. Document with care
Record enough for safety and continuity while protecting sensitive detail according to local record and patient-portal rules. A portal or billing leak of confidential content about sexuality or exploitation is a system-level harm. [1]
Investigations
Digital-media risk assessment is history- and screen-led; it needs few laboratory tests. Investigation is selective and driven by the clinical picture, not by the disclosure itself. [1]
Useful adjuncts include validated mood, anxiety and suicide screens (applied when a mood lead appears), and a focused history of sleep, eating, school and function. For presentations with somatic features, targeted testing — for example iron studies in a fatigued adolescent, or pregnancy and STI testing when sexual risk is disclosed — is appropriate. There is no blood test or scan for "screen-time harm." [5] [11]
Low-value patterns: ordering broad blood panels or neuroimaging on the basis of screen-time history alone; treating self-reported hours of use as a diagnosis; punitive device-confiscation framed as "treatment"; and relying on a screen-time app's number rather than a functional assessment. The intervention is behavioural and relational, not investigative. [12]
Management — Resuscitation
A routine digital-media conversation can become an emergency in one disclosure — most often a cyberbullying crisis with suicidality, or a disclosure of exploitation. Recognise the exit point and use it. [4]
- Stabilise safety first: assess and de-escalate acute mental-health crisis, remove access to means, and do not leave a suicidal young person alone. [4]
- Act on exploitation immediately: when grooming, sextortion or image-based abuse of a minor is disclosed, treat it as a safeguarding and legal event — follow local mandatory-reporting duties, preserve evidence (do not have the family delete material without advice), and involve child-protection and law-enforcement pathways as indicated. [9] [8]
- Address the leaked image: where an intimate image of a minor has been shared, use reporting and takedown routes (for example the relevant e-safety authority or platform reporting tools) alongside safeguarding, because re-victimisation is the active harm. [9]
The common error is treating a cyberbullying crisis as a routine mental-health follow-up. Suicidality and exploitation exit the routine pathway before you reach brief intervention. [4]
Management — Definitive & Stepwise
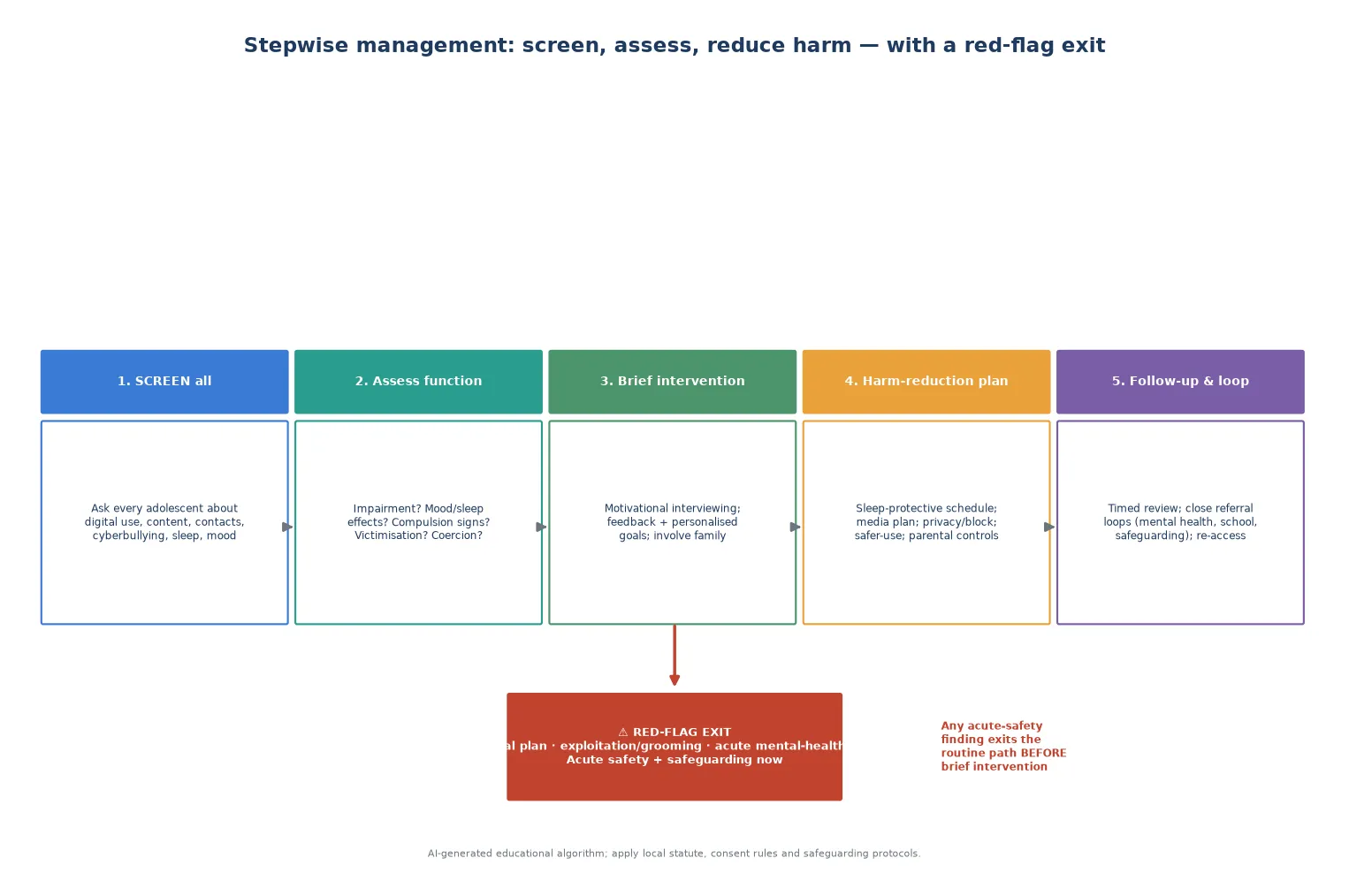
Read the figure like this: the red diamond is not decoration. Any acute-safety or exploitation finding exits the routine path before you reach brief intervention. [4]
Stepwise routine pathway
- Engage and frame: time alone, conditional confidentiality, non-judgemental stance, normalised questions. [1]
- Classify the use: normative (reinforce), at-risk (intervene), or harmful (activate pathways), using the function filter. [12]
- Deliver a brief intervention: motivational interviewing to evoke the young person's own reasons for change, with personalised feedback on sleep, mood and function. [5]
- Build a harm-reduction plan and a family media plan: negotiated, age-appropriate, and written down. [1]
Brief intervention technique
Motivational interviewing uses open questions, affirmation, reflective listening and summaries to help the young person articulate their own reasons for changing how, when and why they use screens. The skill is to evoke rather than impose — an abstinence ultimatum about a phone usually produces concealment, not change. [5] [12]
Domain-specific harm-reduction bundle
Screen time & social media
Sleep and mood
- Sleep-protective schedule: devices off and out of room at bedtime
- Curate feeds; mute or unfollow harmful accounts
- Protect time for sleep, movement and in-person contact
- Family media plan, negotiated not imposed
Gaming & internet use
Compulsion
- Set session limits with breaks for food, movement, sleep
- Address dependence and withdrawal gradually
- Open doors to parental awareness of in-game contact
- Refer for disordered use with functional impairment
Cyberbullying
Victimisation
- Do not reply; preserve evidence (screenshots)
- Block, report, and use platform/takedown tools
- Mental-health support and suicide screening
- School and safeguarding involvement as indicated
Sexting & online sexual risk
Exploitation
- Distinguish consensual from coerced sharing
- Report image-based abuse and seek takedown
- Assess for grooming, sextortion, trafficking
- Safeguarding and law-enforcement pathways
Specific Subtypes & Scenarios
Cyberbullying with suicidality. This is the highest-acuity digital-media scenario. Treat it as a crisis: assess suicide risk fully, restrict means, do not leave the young person alone, preserve evidence, involve mental-health and crisis pathways, and engage the school and safeguarding as appropriate. Remember that perpetrators, not only victims, carry elevated self-harm risk. [4]
Internet gaming disorder and problematic use. When gaming produces functional impairment, compulsive features and withdrawal, classify it as disordered rather than recreational. A systematic review highlights family factors — conflict, low monitoring, poor communication — as both risk and intervention targets. Manage with graded reduction, functional goals and referral for severe cases; do not frame sudden confiscation as treatment. [10]
Heavy screen time and depression. Longitudinal data link higher screen time to rising depressive symptoms, and the prospective ABCD cohort associates screen time with later internalising problems. The effect sizes are modest and bidirectional, so assess and treat the depression on its merits while negotiating sleep-protective and function-focused changes to the use. [5] [11]
Sexting that has gone wrong. Consensual sexting is common; the harm enters when images are forwarded without consent or when an adult is involved. Non-consensual sharing of a minor's image is image-based abuse and a safeguarding event: report, seek takedown through the relevant authority, support the young person, and involve safeguarding. [7] [9]
Online grooming and sexual exploitation. Grooming builds through attention, gifts, secrecy and escalating requests, and may progress to sextortion (threats to release images unless demands are met). Retrospective reports confirm minors rarely disclose spontaneously. Ask directly, distinguish from consensual contact, preserve evidence, and activate child-protection pathways. [9] [8]
Young children and early media. For younger children the emphasis is different: the AAP advises avoiding screen time under 18–24 months (other than video-calling), prioritising co-viewing and age-appropriate content, and protecting sleep — the building of healthy habits before adolescence. [2]
Complications & Pitfalls
- Defaulting to an abstinence lecture that drives the behaviour underground and ends disclosure. [12]
- Treating hours of use as the diagnosis while ignoring function, content and context. [5]
- Missing suicidality behind a "cyberbullying" label, or exploitation behind "risk-taking behaviour." [4] [9]
- Confiscating devices as "treatment" without a functional or safeguarding plan. [10]
- Failing to preserve evidence or seek image takedown in image-based abuse. [9]
- Overstating causation from cross-sectional screen-time data when the relationship is bidirectional. [11] [12]
Prognosis & Disposition
Prognosis here means the trajectory of function, safety and engagement, not a disease stage. Most young people use digital media without lasting harm; the dispositions below describe the responses to the subset in whom the use has become a clinical problem. [12]
Routine disposition: a complete assessment with normative use and intact function; brief reinforcement, a family media plan, a safety net, and a planned interval. [1]
Early-review disposition: at-risk use with emerging sleep, mood or school effects, or an incomplete assessment needing a return visit with trust built. Negotiate concrete changes and review function. [5]
Urgent disposition: cyberbullying with suicidality, exploitation or image-based abuse, acute mental-health crisis, or severe neglect from compulsive use — crisis, safeguarding and mental-health pathways as indicated, with follow-up loops explicitly closed. [4] [9]
Engagement is fragile, and a young person who feels judged will not return. Name the next contact and a low-threshold way back in; harm reduction succeeds when the young person comes back. [12]
Special Populations
Neurodiverse and disabled young people. Gaming and online interaction can be a genuine social lifeline, but compulsive use and exploitation risk are elevated. Adapt the assessment — longer slots, sensory considerations, easy-read materials — without overshadowing mental-health and sexual-risk assessment. [12] [10]
Gender and sexual diversity. LGBTQ+ young people frequently find affirmation and community online but also face disproportionate cyberbullying and minority stress. Tailor the assessment, affirm identity, and watch for victimisation, family rejection and exploitation. [4]
Out-of-home care and youth justice. Assume incomplete history, high trauma load, fragmented records, and elevated risk across every digital domain, including exploitation and image-based abuse. Reconstruct the story actively and clarify consent and safeguarding duties. [9]
Socioeconomic disadvantage. Device access, data limits, shared devices and parental work patterns shape what harm-reduction options are reachable. A "devices out of the bedroom" plan assumes a bedroom and a parent home at night — ask before prescribing. [12]
Indigenous young people. Cultural safety, connection to community and racism as a health exposure matter as much as any screen-time question; partner with local services and avoid deficit framing. [1]
Migrant and refugee youth. Use a professional interpreter for confidential content and apply trauma-informed pacing; family interpreters are not equivalent for sensitive online-history disclosure. [8]
Evidence, Guidelines & Regional Differences
Paediatric media guidance. The AAP recommends that paediatricians ask about media use at every well-child visit, create a family media plan, prioritise co-viewing and age-appropriate content, keep mealtimes and bedrooms screen-free, and protect sleep — shifting the focus from hours alone to content, context and consequence. Separate AAP guidance addresses media use in younger children. [1] [2]
Cyberbullying and self-harm. A systematic review of cyberbullying and self-harm in children and young people found victims and perpetrators had around twice the odds of self-harm and suicidal behaviour, supporting routine suicide screening whenever cyberbullying is disclosed. Prevalence reviews confirm cyberbullying affects a substantial minority of adolescents. [3] [4]
Screen time and mental health. Longitudinal adolescent data link higher screen and social-media use to increasing depressive symptoms, and the prospective ABCD cohort associates screen time with later internalising and externalising problems. Annual-review commentary stresses that the field must move beyond panic and hours to mechanism, vulnerability and function, and that associations are modest and partly bidirectional. [5] [11] [12]
Social media and isolation. Frequent social-media use is associated with higher perceived social isolation, supporting a mechanism in which comparative, curated feeds can worsen belonging rather than build it. [6]
Online sexual risk. A meta-analysis documents substantial youth sexting prevalence rising with age; retrospective data confirm online solicitation and grooming of minors as recurring, under-disclosed experiences. The clinical implication is to ask directly and distinguish consensual sharing from coercion and exploitation. [7] [9]
Problematic internet gaming. A systematic review identifies family factors as central to adolescent problematic gaming, framing the family as both risk and intervention target alongside individual compulsive-use features. [10]
ANZ: the eSafety Commissioner provides cyberbullying reporting, takedown and image-based-abuse pathways used routinely in Australian practice; RCH Melbourne offers screen-time guidance; apply state consent and mandatory-reporting statute. UK: UK Safer Internet Centre and "Keeping Children Safe in Education" guidance; NICE mental-health pathways; apply Gillick/Fraser capacity concepts and local safeguarding duties with current legal teaching. US: AAP media-use policy and Family Media Plan; vary state-by-state sexting, exploitation and mandatory-reporting laws; manage open-notes portal confidentiality for sensitive online-history content. Canada: CPS-aligned digital-media guidance; provincial consent variation; strong cyberbullying and image-based-abuse legislation in several provinces.
Exam Pearls
- Open every answer with time alone + conditional confidentiality before any digital-media question. [1] [4]
- Define the discriminator in one line: function, not hours — is sleep, mood, school, weight or safety affected? [12]
- Name the four exposures: screen time/social media, gaming, cyberbullying, sexting/online sexual risk. [8]
- Cite the content–contact–conduct–compulsion frame to classify where the harm sits. [8]
- State that cyberbullying roughly doubles the odds of self-harm and suicidality — so screen for suicide whenever it is disclosed. [4]
- Pair every screen-time discussion with a family media plan and a sleep-protective schedule, not an abstinence lecture. [1]
- Treat non-consensual image sharing of a minor as a safeguarding and legal event: report, seek takedown, preserve evidence. [9]
- Remember that the effect sizes for screen time and depression are modest and bidirectional — assess and treat the depression on its merits. [11] [12]
- State that local statute governs consent, mandatory reporting, sexting law and image-based-abuse pathways — do not invent universal ages. [9]
SAFE-DIGITAL risk response
References
- [1]Council on Communications and Media Media Use in School-Aged Children and Adolescents. Pediatrics, 2016.PMID 27940794
- [2]Council on Communications and Media Media and Young Minds. Pediatrics, 2016.PMID 27940793
- [3]Selkie EM, Fales JL, Moreno MA Cyberbullying Prevalence Among US Middle and High School-Aged Adolescents: A Systematic Review and Quality Assessment. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2016.PMID 26576821
- [4]John A, Glendenning AC, Marchant A, Montgomery P, Stewart A, Wood S, Lloyd K, Hawton K Self-Harm, Suicidal Behaviours, and Cyberbullying in Children and Young People: Systematic Review. Journal of medical Internet research, 2018.PMID 29674305
- [5]Boers E, Afzali MH, Newton N, Conrod P Association of Screen Time and Depression in Adolescence. JAMA pediatrics, 2019.PMID 31305878
- [6]Primack BA, Shensa A, Sidani JE, Whaite EO, Lin LY, Rosen D, Colditz JB, Radovic A, Miller E Social Media Use and Perceived Social Isolation Among Young Adults in the U.S. American journal of preventive medicine, 2017.PMID 28279545
- [7]Madigan S, Ly A, Rash CL, Van Ouytsel J, Temple JR Prevalence of Multiple Forms of Sexting Behavior Among Youth: A Systematic Review and Meta-analysis. JAMA pediatrics, 2018.PMID 29482215
- [8]Livingstone S, Smith PK Annual research review: Harms experienced by child users of online and mobile technologies: the nature, prevalence and management of sexual and aggressive risks in the digital age. Journal of child psychology and psychiatry, and allied disciplines, 2014.PMID 24438579
- [9]Greene-Colozzi EA, Winters GM, Blasko B, Jeglic EL Experiences and Perceptions of Online Sexual Solicitation and Grooming of Minors: A Retrospective Report. Journal of child sexual abuse, 2020.PMID 33017275
- [10]Schneider LA, King DL, Delfabbro PH Family factors in adolescent problematic Internet gaming: A systematic review. Journal of behavioral addictions, 2017.PMID 28762279
- [11]Nagata JM, Testa A, Ganson KT, Baker FC Screen time and mental health: a prospective analysis of the Adolescent Brain Cognitive Development (ABCD) Study. BMC public health, 2024.PMID 39370520
- [12]Odgers CL, Jensen MR Annual Research Review: Adolescent mental health in the digital age: facts, fears, and future directions. Journal of child psychology and psychiatry, and allied disciplines, 2020.PMID 31951670