Paeds · adolescent-and-young-adult-medicine
Dysmenorrhoea and heavy menstrual bleeding
Also known as Dysmenorrhoea and heavy menstrual bleeding · Adolescent menstrual pain and menorrhagia · Period pain and heavy periods in adolescents · Primary and secondary dysmenorrhoea · Abnormal uterine bleeding in the adolescent
A fellowship approach to the adolescent with menstrual pain and heavy bleeding: separating primary from secondary dysmenorrhoea, applying the FIGO PALM-COEIN classification with the adolescent-dominated COEIN causes, the bleeding-disease screen, and the stepwise NSAID-to-hormonal-to-LNG-IUS management ladders, run in parallel with iron repletion, school and sport reintegration, and the HEEADSSS and confidentiality frame.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
The adolescent who comes to clinic with "bad periods" is describing one of two separable problems, and the first task is to tell them apart. Dysmenorrhoea is cyclic pelvic pain that comes with menstruation; heavy menstrual bleeding is blood loss the young person finds excessive or disruptive. The two often travel together, but they have different mechanisms, different red flags, and different management ladders. [1]
Both are common, and both are under-treated. A large majority of menstruating adolescents report some menstrual pain, and a substantial minority describe pain that limits activity and misses school. Heavy menstrual bleeding brings a meaningful proportion to adolescent gynaecology, and in this age group it is most often driven by anovulatory cycles from the still-maturing hypothalamic–pituitary–ovarian axis, or by an underlying bleeding disorder such as von Willebrand disease. [2] [4]
Classification
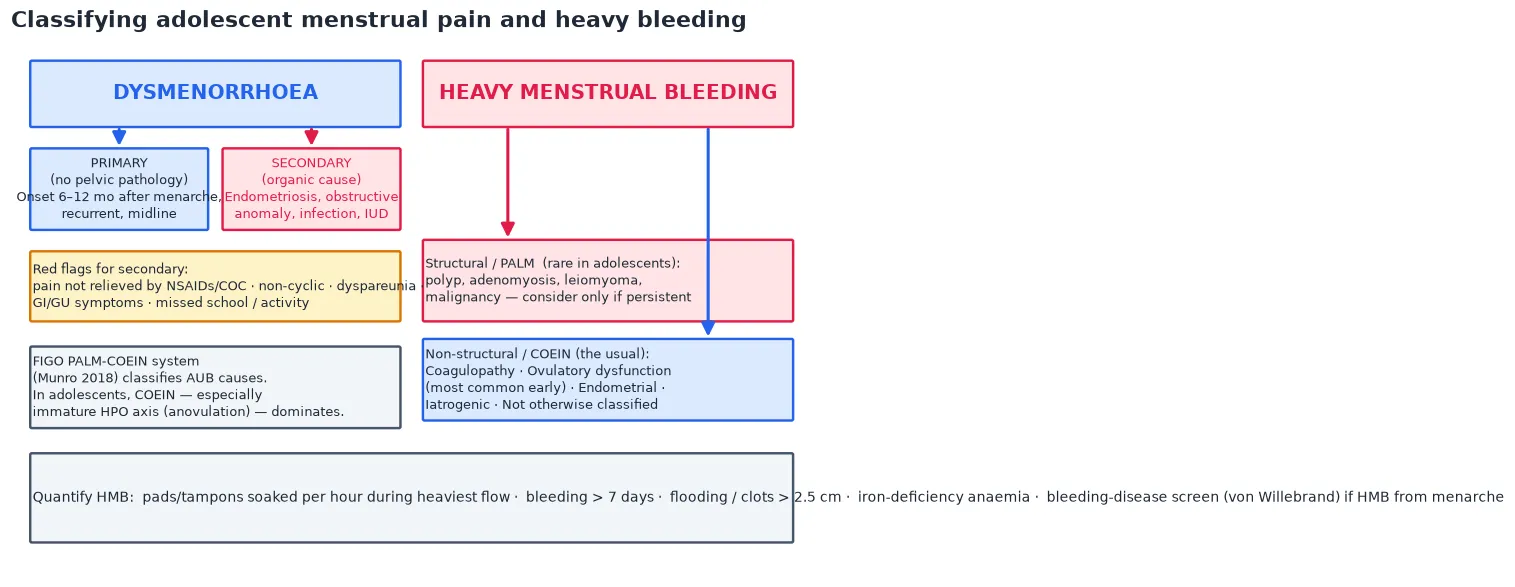
Menstrual pain is classified by whether a cause is found. Primary dysmenorrhoea is cyclic pelvic pain with no pelvic pathology; it begins only once ovulatory cycles establish, typically 6 to 12 months after menarche, and it is driven by excess prostaglandins. Secondary dysmenorrhoea is menstrual pain with an identifiable organic cause — endometriosis in the adolescent most often, but also pelvic infection, an obstructive Müllerian anomaly, or an intrauterine device. The discriminator is the history: primary pain is midline, cyclic, and predictable; secondary pain breaks through standard therapy or carries features such as non-cyclic pain, dyspareunia, dyschezia, or GI/GU symptoms. [1]
Heavy menstrual bleeding sits inside the FIGO system for abnormal uterine bleeding. The 2018 FIGO revision classifies causes into the structural PALM arm (Polyp, Adenomyosis, Leiomyoma, Malignancy) and the non-structural COEIN arm (Coagulopathy, Ovulatory dysfunction, Endometrial, Iatrogenic, Not otherwise classified). In the adolescent the arms invert: the COEIN arm dominates, because the immature hypothalamic–pituitary–ovarian axis produces anovulatory cycles, and coagulopathy — especially von Willebrand disease — is over-represented. The structural PALM causes are rare in this age group and are pursued only when the picture is atypical or persistent. [3] [4]
Epidemiology & Risk Factors
Dysmenorrhoea is the most common menstrual complaint in adolescence. The large majority of menstruating adolescents report some menstrual pain, and roughly a third to a half describe pain that limits daily activity; a smaller but important proportion miss school or sport because of it. Despite this, dysmenorrhoea is under-reported and under-treated, partly because adolescents and families normalise it. [1]
Heavy menstrual bleeding is a leading reason for adolescent gynaecology referral. In the first 1 to 2 years after menarche, most cycles are anovulatory, so irregular and sometimes heavy bleeding is the expected background. Beyond that window, persistent heavy bleeding prompts the search for a cause. An underlying bleeding disorder is found in a meaningful proportion of adolescents with heavy menstrual bleeding — von Willebrand disease is the commonest, with platelet function disorders and thrombocytopenia also represented — and heavy menstrual bleeding from menarche is the single most common presentation of a bleeding disorder in females. [4]
The risk factors for secondary dysmenorrhoea are the things that add an organic driver: endometriosis (which has a long diagnostic delay in adolescents), a sexually transmitted infection, an obstructive Müllerian anomaly, and an intrauterine device. A family history of a bleeding disorder, bleeding after dental work or surgery, epistaxis, easy bruising, and a mother or sister with menorrhagia all raise the likelihood of a coagulopathy behind the heavy bleeding. [1] [4]
Pathophysiology
The two problems have two mechanisms, and the mechanisms explain the treatment. Primary dysmenorrhoea is a prostaglandin problem. As the menstruating endometrium sheds, it releases an excess of prostaglandins — PGF2α and PGE2 — and leukotrienes. These drive myometrial contraction and vasoconstriction, producing uterine ischaemia and the cramping pain the young person feels. The same mediators generate the systemic symptoms that ride with the pain: nausea, diarrhoea, headache, and fatigue. This is why a non-steroidal anti-inflammatory drug works — it blocks prostaglandin synthesis at the source. [6]
Primary dysmenorrhoea appears only after ovulatory cycles establish, typically 6 to 12 months after menarche. The reason is progesterone: the secretory-phase progesterone of an ovulatory cycle primes the endometrium to synthesise prostaglandins and leukotrienes. A newly menarcheal, anovulatory cycle has not built up that prostaglandin load, so the very first periods are often painless — a point examiners probe, because candidates misremember primary dysmenorrhoea as starting from the first ever period. [1]
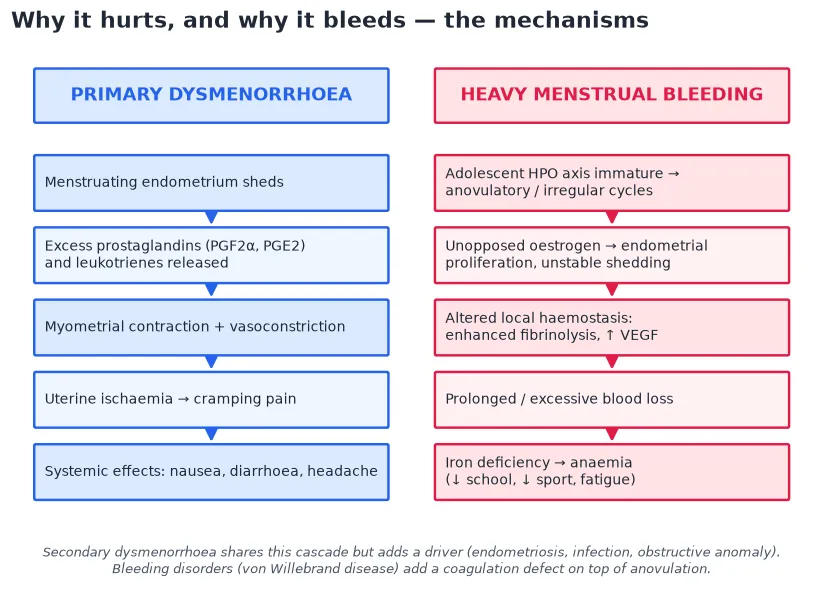
Adolescent heavy menstrual bleeding is usually an anovulation problem. The immature hypothalamic–pituitary–ovarian axis fails to ovulate, so the cycle runs on unopposed oestrogen. Oestrogen drives endometrial proliferation without the organised, progesterone-mediated shedding of an ovulatory cycle. The endometrium becomes thick and unstable and sheds irregularly, with altered local haemostasis and enhanced fibrinolysis that prolong the bleeding. This is the mechanism behind the irregular, sometimes heavy periods of early adolescence. [4]
A coagulation defect stacks on top of the anovulatory mechanism. In von Willebrand disease the deficient or dysfunctional von Willebrand factor cannot support platelet adhesion at the endometrial vessels, so the already-unstable anovulatory bleeding becomes heavier and starts from menarche. Platelet function defects and thrombocytopenia do the same. This is why heavy menstrual bleeding from menarche earns a bleeding-disease screen. [4]
Clinical Presentation
The classic presentation of primary dysmenorrhoea is suprapubic cramping pain that begins just before or with the onset of menses, lasts one to three days, sits in the midline, recurs each cycle in a predictable pattern, and comes with systemic symptoms such as nausea, diarrhoea and headache. Crucially, it does not progress or change character between cycles. A history of predictable, midline, cyclic pain that the young person can forecast is the pattern of primary dysmenorrhoea. [1]
Secondary dysmenorrhoea shows a different shape. The pain is not relieved by NSAIDs and the combined oral contraceptive, or it becomes non-cyclic, or it persists as chronic pelvic pain between periods. Dyspareunia, dyschezia, and GI/GU symptoms accompany it. It limits activity and school attendance out of proportion to a "normal period." These are the features that move the assessment from primary to secondary, and in the adolescent they most often point to endometriosis or an anatomic cause. [1]
Heavy menstrual bleeding is a clinical, not a laboratory, diagnosis at first contact. The defining features come from the history: soaking a pad or tampon more often than every 1 to 2 hours on the heaviest days, bleeding that runs longer than 7 days, flooding through protection, and clots larger than about 2.5 cm. The sequelae of iron deficiency follow — fatigue, pallor, reduced exercise tolerance, and missed school or sport. Quantifying these features, rather than accepting "heavy" at face value, is the discriminator between the well adolescent with anovulatory cycles and the one who needs investigation. [2] [4]
Differential Diagnosis
The differential for dysmenorrhoea separates primary pain from the secondary causes. Endometriosis is the commonest secondary cause in the adolescent and carries a long diagnostic delay, so it is actively considered when standard therapy fails. Pelvic infection from a sexually transmitted pathogen causes pain and bleeding, and a sexually active adolescent is screened. An obstructive Müllerian anomaly produces progressive, often severe dysmenorrhoea with a haematocolpos. An intrauterine device can cause or worsen pain. Pregnancy-related pain — ectopic or miscarriage — is excluded with a pregnancy test in the sexually active. [1]
The differential for heavy menstrual bleeding separates the anovulatory default from a bleeding disorder and from other medical causes. Von Willebrand disease is the commonest inherited bleeding disorder in females, with platelet function disorders and carriership of haemophilia also represented; thrombocytopenia and anticoagulant use are iatrogenic or acquired contributors. Pregnancy-related bleeding, thyroid disease, and a structural cause (polyp, rarely malignancy) round out the list. In the adolescent the structural PALM causes are uncommon, but they are pursued when the picture is atypical or the bleeding persists despite first-line therapy. [3] [4]
[3] [4]Menstrual pain also has non-gynaecological mimics that cause chronic pelvic pain in the adolescent: functional abdominal pain, irritable bowel syndrome, urinary tract pathology, and musculoskeletal pain. The menstrual cycle — its timing, its relationship to the pain, and its response to cycle-suppressing therapy — separates a gynaecological cause from a gastrointestinal or functional one. A dysmenorrhoea that does not track the cycle, and that does not improve when the cycle is suppressed, points away from a pure menstrual mechanism. [1]
Clinical & Bedside Assessment
The assessment starts with the menstrual history, taken with the young person alone after confidentiality is framed. The key elements are the age at menarche, the cycle length and regularity, the duration and heaviness of flow, and the pain — its onset, timing, severity, and what relieves it. A menstrual calendar or app is the single most useful tool, because it converts a vague "heavy" into a quantified pattern over time. The sexual and contraceptive history, the bleeding-disease screen questions (bleeding after dental work, epistaxis, easy bruising, a parent or sibling with heavy periods), and the impact on school and sport complete the picture. [1] [2]
Seeing the young person alone is both a clinical and an ethical step. The menstrual history sits inside the HEEADSSS psychosocial assessment, and the parts of it that matter most — sexual activity, contraception, coercion, substance use — only surface when the parent is not in the room. Framing confidentiality up front, with its limits, is what allows the history to be complete. The same visit is the place to integrate the menstrual cycle as a vital sign, because an irregular or absent cycle is often the first sign of an eating disorder, over-training, or a thyroid problem. [2]
The examination is tailored. The abdomen is examined for tenderness and masses. The external genitalia are examined when an obstructive anomaly, trauma, or a foreign body is suspected. Signs of iron deficiency (pallor) and a bleeding disorder (bruising, petechiae, mucosal bleeding) are sought. A pelvic or speculum examination is not routine in the adolescent and is reserved for the sexually active young person with a specific indication, or when an anatomic cause is suspected; a pelvic ultrasound is the preferred first imaging step when a secondary cause is in play. [1] [4]
Investigations
The first-line investigations for heavy menstrual bleeding are few and high-yield. A full blood count and ferritin establish the degree of iron deficiency and anaemia. A pregnancy test is done in the sexually active adolescent. A sexually transmitted infection screen is done when the history or examination raises infection. These run in parallel with the decision to start medical therapy — treatment does not wait for the bleeding-disease screen to return. [4]
The bleeding-disease screen is ordered when heavy menstrual bleeding presents from menarche or the history suggests a coagulopathy. The core panel is von Willebrand factor antigen and activity (ristocetin cofactor), factor VIII, and a blood-group-aware interpretation — von Willebrand factor levels rise with blood group O and with oestrogen, and fall during acute bleeding, pregnancy, and the menstrual state, so a level drawn during active heavy bleeding is interpreted in that context. A platelet count and a platelet function screen complete the work-up. Haematology is involved when a disorder is confirmed or the screen is equivocal. [4]
Pelvic ultrasound is the first imaging step when a secondary cause is suspected — an obstructive anomaly, an ovarian endometrioma, or a structural cause — or when heavy menstrual bleeding is persistent or atypical. Endometrial biopsy and hysteroscopy are rarely indicated in the adolescent; they become relevant only for refractory disease, a structural lesion, or a much older young person in whom malignancy enters the differential. [1] [4]
Management — Resuscitation
The resuscitation lane is for the adolescent with acute severe heavy menstrual bleeding and haemodynamic compromise. Intravenous access is established, and the young person is resuscitated with isotonic fluids while a full blood count, group-and-hold, and coagulation screen are sent. A hormonal taper regimen — a combined oral contraceptive or oral progestogen, tapered as the bleeding settles — together with tranexamic acid is the first pharmacological step. Escalation to transfusion follows when the haemoglobin is critically low or the young person remains unstable. [1] [4]
The immediate work-up of the sexually active adolescent with pain or bleeding runs in parallel with resuscitation. A pregnancy test and a sexually transmitted infection screen are part of the first contact, because pregnancy-related bleeding and pelvic infection are both in the differential and both change management. Attributing the presentation to a benign menstrual cause before excluding them is a classic error. [1]
Iron-deficiency anaemia is treated at the first visit, not filed for later. Oral iron repletion is first-line for the stable adolescent; the young person with severe symptomatic anaemia is referred for consideration of intravenous iron. The safety-net is explicit: return if the bleeding increases, if there is dizziness or presyncope, or if the pain becomes severe. [4]
Immediate management of acute severe heavy menstrual bleeding
Assess haemodynamics; establish intravenous access
Resuscitate with isotonic fluids; send FBC, group-and-hold, coagulation
Pregnancy test and STI screen if sexually active
Start a hormonal taper regimen (COC or oral progestogen) plus tranexamic acid 1 g three times daily
Transfuse if critically anaemic or unstable; refer for intravenous iron if severe symptomatic anaemia
Refer to paediatric gynaecology and haematology; arrange follow-up
Management — Definitive & Stepwise
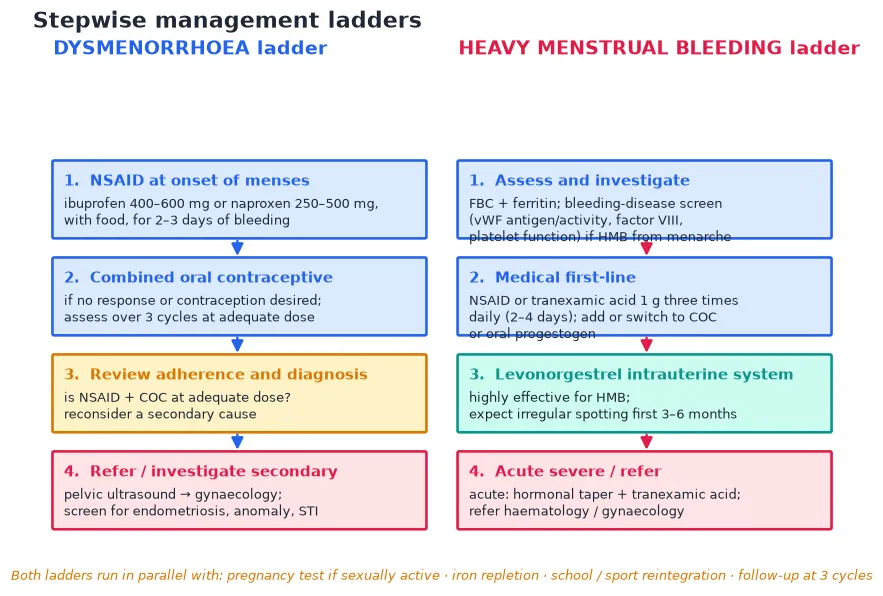
The definitive management runs on two ladders, one for each problem, and they often run together. For dysmenorrhoea, the first step is a non-steroidal anti-inflammatory drug at the onset of menses — ibuprofen 400 to 600 mg or naproxen 250 to 500 mg, taken with food, for 2 to 3 days of bleeding. NSAIDs are more effective than placebo for dysmenorrhoea, and they work because they block prostaglandin synthesis. The second step is the combined oral contraceptive, added if the NSAID does not give adequate relief or contraception is desired, and assessed over three cycles at an adequate dose. The oral contraceptive pill improves dysmenorrhoea over placebo. The third step is to review adherence and reconsider a secondary cause — is the young person actually taking an adequate dose? The fourth step is referral for pelvic ultrasound and gynaecology, to pursue endometriosis, an anomaly, or infection. [5] [6]
For heavy menstrual bleeding, the first step is a non-steroidal anti-inflammatory drug or tranexamic acid 1 g three times daily for 2 to 4 days of bleeding; NSAIDs reduce heavy menstrual bleeding more than placebo. The second step is to add or switch to the combined oral contraceptive or an oral progestogen. The third step is the levonorgestrel intrauterine system, the most effective long-term option for heavy menstrual bleeding — more effective than oral medical therapies — with the caveat that irregular spotting is expected in the first 3 to 6 months. The fourth step, for acute severe bleeding, is a hormonal taper plus tranexamic acid, with referral to haematology and gynaecology. [7] [8]
NSAID / tranexamic acid / hormonal
Iron repletion runs in parallel with both ladders wherever iron-deficiency anaemia is present. School and sport reintegration is an explicit goal — the measure of success is not just less bleeding but the young person back in class and on the field. Follow-up at three cycles confirms response and catches the secondary cause that the first treatment has masked. A confirmed bleeding disorder moves the young person into shared care with haematology, where the choice of agent is adjusted — for example, tranexamic acid is central and some non-steroidal agents are used with caution in certain platelet disorders. [4] [9]
ACOG (US) frames the menstrual cycle as a vital sign and uses the FIGO PALM-COEIN system, with the stepwise NSAID-to-combined-oral-contraceptive ladder for dysmenorrhoea and the NSAID-or-tranexamic-acid-to-hormonal-to-LNG-IUS ladder for heavy menstrual bleeding. NICE NG88 (UK) defines heavy menstrual bleeding by patient impact and follows a pharmacological-then-LNG-IUS pathway, with the LNG-IUS as the preferred long-term option. ANZ adolescent gynaecology practice aligns with both and emphasises the HEEADSSS framework, conditional confidentiality, and a low threshold for the bleeding-disease screen. [1] [2] [4]
Specific Subtypes & Scenarios
The newly menarcheal adolescent with anovulatory irregular bleeding is the commonest scenario. For the well, well-cycled young person, reassurance and a menstrual calendar are enough — the pattern matures over 2 to 3 years as the axis settles. Hormonal cycling is offered when the bleeding is heavy, disruptive, or causing iron deficiency. The bleeding-disease screen is reserved for the heavy-from-menarche picture or a positive bleeding history. [4]
The adolescent with heavy menstrual bleeding from menarche moves into a specific lane. The bleeding-disease screen is done; a non-steroidal anti-inflammatory drug or tranexamic acid is started; the combined oral contraceptive is added or switched to; and haematology liaison is arranged when a disorder is confirmed. The levonorgestrel intrauterine system is an excellent long-term option for the confirmed bleeding disorder, because it both controls the bleeding and avoids oestrogen. [4] [8]
Suspected endometriosis is managed empirically first. Hormonal suppression — the combined oral contraceptive or a progestogen — is first-line, because the goal in the adolescent is symptom control and the avoidance of the long diagnostic delay that has historically characterised this disease. Pelvic ultrasound and gynaecology referral follow refractory or atypical disease, and laparoscopy is reserved for disease that does not respond to medical therapy. [1]
The adolescent with an obstructive Müllerian anomaly presents with progressive dysmenorrhoea and a haematocolpos — the pain is severe, progressive, and often out of proportion to the apparent cycle. Pelvic ultrasound confirms the obstructed outflow tract, and urgent gynaecology referral follows. This is one of the few menstrual-pain scenarios that is both anatomic and time-sensitive. [1] [4]
Complications & Pitfalls
The complications are the consequences of under-treatment. Iron-deficiency anaemia is common and erodes school attendance, exercise tolerance, and concentration. School absenteeism and reduced quality of life are the lived experience of the adolescent with untreated dysmenorrhoea. The long diagnostic delay for endometriosis and the missed bleeding disorder are the failures of attribution — the presentation is normalised as "just bad periods" until the underlying cause declares itself. [1] [4]
The common errors cluster around attribution and under-dosing. Attributing pain or bleeding to normal periods without quantifying the impact is the first error; failing to test for pregnancy and sexually transmitted infection in the sexually active adolescent is the second; and ordering a bleeding-disease screen during active heavy bleeding without interpreting it in that context is the third, because acute bleeding lowers von Willebrand factor levels. The non-steroidal pitfalls are giving the dose too late (after the prostaglandin cascade has run), under-dosing, or persisting with an agent the young person has already found ineffective. Gastritis, and the caution in asthma and renal disease, are the safety considerations. [4] [6]
The combined oral contraceptive pitfalls are inadequate counselling of side-effects and the need for three cycles to assess benefit, missing the von Willebrand work-up behind the bleeding, and over-reliance on imaging when the history points to a functional cause. The levonorgestrel intrauterine system pitfall is not warning the young person about the irregular spotting of the first 3 to 6 months, which leads to early discontinuation of an otherwise excellent therapy. [1] [8]
Prognosis & Disposition
Primary dysmenorrhoea has an excellent prognosis. The large majority respond to a non-steroidal anti-inflammatory drug with or without the combined oral contraceptive, and only a minority need evaluation for a secondary cause. The measure of success is functional — the young person back at school and sport, with a cycle that no longer governs the month. [1]
Adolescent heavy menstrual bleeding from anovulation matures with the axis over 2 to 3 years, and hormonal control is effective in the interim. The early recognition and treatment of iron deficiency and of a bleeding disorder protects both the immediate quality of life and the long-term iron stores, and prevents the cycle of recurrent anaemia. [4]
Disposition follows severity and cause. Most adolescents are managed in primary care or general paediatrics, with simple first-line therapy and follow-up at three cycles. Paediatric gynaecology, adolescent medicine, and haematology referral follow refractory disease, a confirmed bleeding disorder, or an anatomic cause. Structured follow-up confirms response, and the young person transitions to adult care as she moves through adolescence. [1] [4]
Special Populations
The adolescent with a confirmed bleeding disorder moves into shared care with haematology. Tranexamic acid is central to control, the levonorgestrel intrauterine system is a highly effective long-term option that avoids oestrogen, and some non-steroidal agents are used with caution in certain platelet function disorders because of their effect on platelet aggregation. The plan is built around the specific disorder, the bleeding phenotype, and the young person's goals. [4] [9]
The young person with a developmental disability or an autistic young person who finds menstruation distressing is offered menstrual suppression tailored to goals, capacity, and consent. The options — the combined oral contraceptive, a progestogen, or the levonorgestrel intrauterine system — are weighed against the cognitive and sensory impact of menstruation, the capacity to manage hygiene, and the principle of the least restrictive effective option. Consent is assessed in the framework of the young person's capacity and best interests. [9]
The gender-diverse young person on testosterone who continues to menstruate needs specific handling. Testosterone-induced amenorrhoea is not immediate, and bleeding can persist for months. The levonorgestrel intrauterine system or a progestogen controls bleeding without oestrogen, which matters for a young person on gender-affirming testosterone. The approach is affirming, consent-based, and integrated with the gender service. [9]
The rural or remote adolescent is supported by telehealth-delivered adolescent gynaecology, with first-line therapy initiated locally and a clear referral pathway for refractory disease, a confirmed bleeding disorder, or an anatomic cause. Distance is not a reason to defer the bleeding-disease screen or the simple, high-yield first steps. [1] [4]
Evidence, Guidelines & Regional Differences
The evidence base is strong for the first-line therapies. Non-steroidal anti-inflammatory drugs are more effective than placebo for dysmenorrhoea (Marjoribanks 2010, Cochrane), and they reduce heavy menstrual bleeding more than placebo (Bofill Rodriguez 2019, Cochrane). The oral contraceptive pill improves dysmenorrhoea over placebo (Wong 2009, Cochrane). The levonorgestrel intrauterine system is more effective than oral medical therapies for heavy menstrual bleeding (Bofill Rodriguez 2020, Cochrane). Together these underwrite the stepwise ladders. [5] [6] [7] [8]
The key guidelines converge on a small set of principles. ACOG Committee Opinion 760 frames dysmenorrhoea and endometriosis in the adolescent and recommends the NSAID-to-combined-oral-contraceptive ladder with referral for refractory disease. ACOG Committee Opinion 651 frames the menstrual cycle as a vital sign, so that an irregular or absent cycle is read as a signal, not a nuisance. The ACOG clinical guidance on abnormal uterine bleeding in the adolescent (Hernandez and Dietrich 2020) sets out the FIGO-based assessment and the bleeding-disease screen. NICE NG88 defines heavy menstrual bleeding by patient impact and follows a pharmacological-then-LNG-IUS pathway. [1] [2] [4]
The evidence in four lines
The controversies live at the edges. The optimal timing and components of the bleeding-disease screen — whether to screen all or only the heavy-from-menarche group, and how to interpret a level drawn during active bleeding — is still refined in practice. The balance of empirical hormonal suppression versus early laparoscopy for suspected endometriosis is weighed toward medical therapy first in the adolescent. Menstrual suppression for convenience rather than medical necessity raises an ethical question, especially in the young person with a disability, and the long-term bone-density consideration of prolonged progestogen suppression in the adolescent is real and monitored. [1] [4] [9]
Exam Pearls
PALM-COEIN — the FIGO causes of abnormal uterine bleeding
References
- [1]ACOG Committee on Adolescent Health Care ACOG Committee Opinion No. 760: Dysmenorrhea and Endometriosis in the Adolescent. Obstet Gynecol, 2018.PMID 30461694
- [2]ACOG Committee on Adolescent Health Care ACOG Committee Opinion No. 651: Menstruation in Girls and Adolescents: Using the Menstrual Cycle as a Vital Sign. Obstet Gynecol, 2015.PMID 26595586
- [3]Munro MG; Critchley HOD; Fraser IS; FIGO Menstrual Disorders Committee The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. Int J Gynaecol Obstet, 2018.PMID 30198563
- [4]Hernandez A; Dietrich JE Abnormal Uterine Bleeding in the Adolescent. Obstet Gynecol, 2020.PMID 32028485
- [5]Wong CL; Farquhar C; Roberts H; Proctor M Oral contraceptive pill for primary dysmenorrhoea. Cochrane Database Syst Rev, 2009.PMID 19821293
- [6]Marjoribanks J; Proctor M; Farquhar C; Derks RS Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev, 2010.PMID 20091521
- [7]Bofill Rodriguez M; Lethaby A; Farquhar C Non-steroidal anti-inflammatory drugs for heavy menstrual bleeding. Cochrane Database Syst Rev, 2019.PMID 31535715
- [8]Bofill Rodriguez M; Lethaby A; Jordan V Progestogen-releasing intrauterine systems for heavy menstrual bleeding. Cochrane Database Syst Rev, 2020.PMID 32529637
- [9]Altshuler AL; Hillard PJ Menstrual suppression for adolescents. Curr Opin Obstet Gynecol, 2014.PMID 25110977