Paeds · adolescent-and-young-adult-medicine
Eating disorders: recognition and medical instability
Also known as Anorexia nervosa · Bulimia nervosa · Binge-eating disorder · ARFID · Atypical anorexia nervosa · Refeeding syndrome risk · Medically unstable anorexia
A fellowship approach to recognising eating disorders in adolescents and deciding who is medically unstable: DSM-5 categories including anorexia, bulimia, binge-eating disorder and ARFID; SCOFF and HEEADSSS-based screening; physiological red flags and Junior MARSIPAN-style triage; focused assessment of weight, vital signs, posture and ECG; emergency stabilisation; and the threshold for admission — across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old girl is brought in because she has stopped eating meat, runs every morning before dawn, and fainted at school. Her mother thinks it is "just a phase." It is not. The pattern of food restriction, driven exercise and collapse is the textbook opening of an eating disorder, and the faint is the sign that physiology has started to fail. This topic is about recognising that pattern early, and deciding — at the bedside — whether the young person is medically unstable. [4] [6]
Eating disorders are persistent disturbances of eating behaviour and body preoccupation that impair health. The DSM-5 separates them by behaviour: anorexia nervosa is restriction that drives weight below a healthy minimum with an intense fear of gaining weight and a disturbed body image; bulimia nervosa is recurrent binge eating followed by inappropriate compensation; binge-eating disorder is recurrent binges without regular compensation; and avoidant/restrictive food intake disorder (ARFID) is restriction driven by sensory sensitivity, fear of aversive consequences or lack of interest — explicitly not body-image distress. [4] [13]
The clinical question that organises everything else is medical instability. Starvation and purging injure the heart, the metabolism, the endocrine system and the bone. A young person can look well and still be on the edge of a dangerous arrhythmia. The job of the paediatrician at first contact is to find the adolescent who must come into hospital now, before refeeding even begins. [5] [7] [14]
Classification
Start with the behaviour the young person describes, then place it in a DSM-5 category — the category tells you what complications to expect and where the weight sits. [4]
Separate the diagnoses by behaviour and weight
Anorexia nervosa
Restriction + low weight
- Intense fear of weight gain
- Disturbed body image
- Weight below minimum expected
- Subtypes: restricting vs binge-purge
- Highest medical-instability risk
Bulimia nervosa
Binge + compensate
- Recurrent binges with loss of control
- Vomiting, laxatives, fasting, exercise
- Weight often normal or slightly raised
- Electrolyte risk from purging
- One episode weekly for 3 months
Binge-eating disorder
Binge, no compensation
- Recurrent binges with distress
- No regular compensatory behaviour
- Often higher weight
- Metabolic comorbidity
- Guilt and eating rapidly
ARFID
Avoidance, not body image
- Sensory, fear, or low interest
- No drive for thinness
- Can be any weight; growth may falter
- Common in neurodivergent youth
- Recognised medical complications
The single most dangerous misclassification is atypical anorexia nervosa. The young person meets every criterion for anorexia — restriction, fear of weight gain, disturbed body image, physiological shutdown — but their weight has not fallen below the "low weight" threshold. They carry the same bradycardia, the same prolonged QTc, the same refeeding risk, and they are repeatedly reassured because they "don't look anorexic." Do not be reassured. [4] [14]
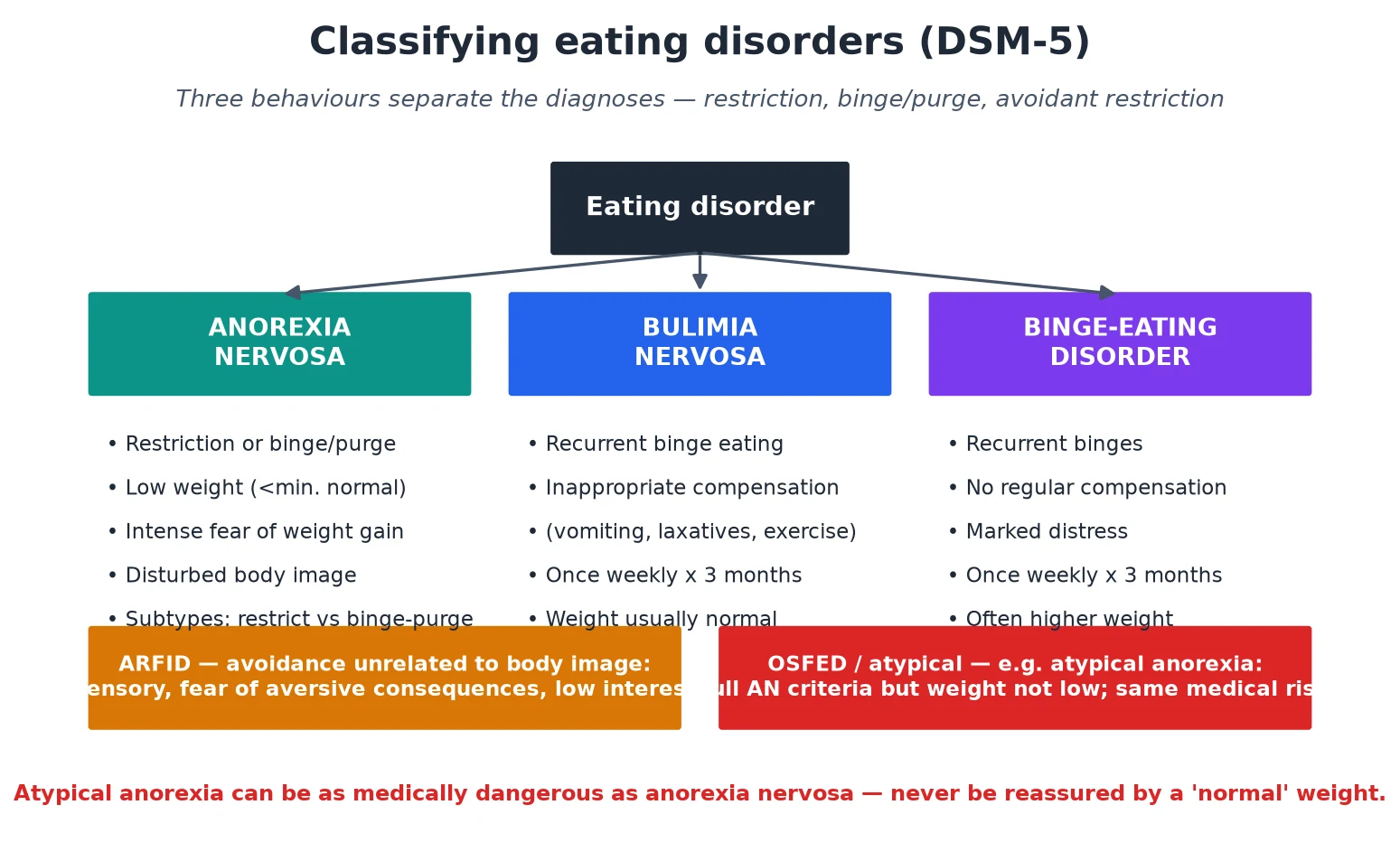
Read the figure like this: weight tells you the diagnosis name; behaviour and physiology tell you the danger. A normal-weight adolescent who is restricting, fainting and bradycardic has anorexia-grade risk regardless of the label. [14]
Epidemiology & Risk Factors
Eating disorders are common, they begin in adolescence, and they have become more visible since the COVID-19 pandemic. Hartman-Munick and colleagues showed that the volume of adolescents and young adults presenting for eating-disorder care rose sharply through the pandemic, so a candidate today is more, not less, likely to meet these patients in clinic and in the emergency department. [12]
Girls are diagnosed more often, but boys are under-recognised, and presentations in males, in higher-weight adolescents, and in gender-diverse youth are frequently missed because they do not match the thin-female stereotype. ARFID is over-represented in neurodivergent children and in those with chronic medical or gastrointestinal conditions. [13] [6]
Mortality is the headline number that should change your threshold. In Arcelus's meta-analysis of 36 studies, anorexia nervosa carried one of the highest standardised mortality ratios of any psychiatric illness — deaths come from medical complications of starvation and from suicide. That mortality is why recognition and medical-instability assessment cannot be deferred to "a specialist appointment next month." [2]
The risk factors cluster in three groups. Biological — female sex, puberty, family history. Psychological — perfectionism, anxiety, low self-esteem, neurodivergence. Social — weight-based teasing, sport or performance pressures, social-media body ideals, transitions and loss. No single factor causes the illness; the skill is noticing the pattern. [6] [12]
Pathophysiology
To assess instability you need a working model of why starvation injures the body. The body responds to under-fuelling with a protective shutdown — heart rate and blood pressure fall, reproductive hormones switch off, metabolism slows — and that shutdown, sustained, becomes the disease. [4] [14]
The heart is the organ most likely to kill the patient. The myocardium thins, the resting heart rate drops (bradycardia), blood pressure falls, and electrolyte shifts from purging or refeeding prolong the QT interval. A long QT in a starved, hypokalaemic adolescent is a setup for a fatal arrhythmia, and it is why an ECG is a first-line investigation, not an afterthought. [14] [7]
The metabolism depletes intracellular ions. Phosphate, potassium and magnesium fall — partly from purging, partly because refeeding shifts them into cells as insulin rises. Blood glucose can be low. The starved body runs on ketones. This is the substrate for refeeding syndrome, in which feeding the starved patient drives phosphate and thiamine into cells and can drop serum phosphate dangerously within the first three days. [9] [4]
The endocrine system closes down the reproductive axis to conserve energy: hypothalamic amenorrhoea, low oestrogen and testosterone, and — in growing adolescents — stunted growth and bone loss. Osteoporosis in a teenager is a direct consequence of energy deficit, not a late complication. [4] [14]
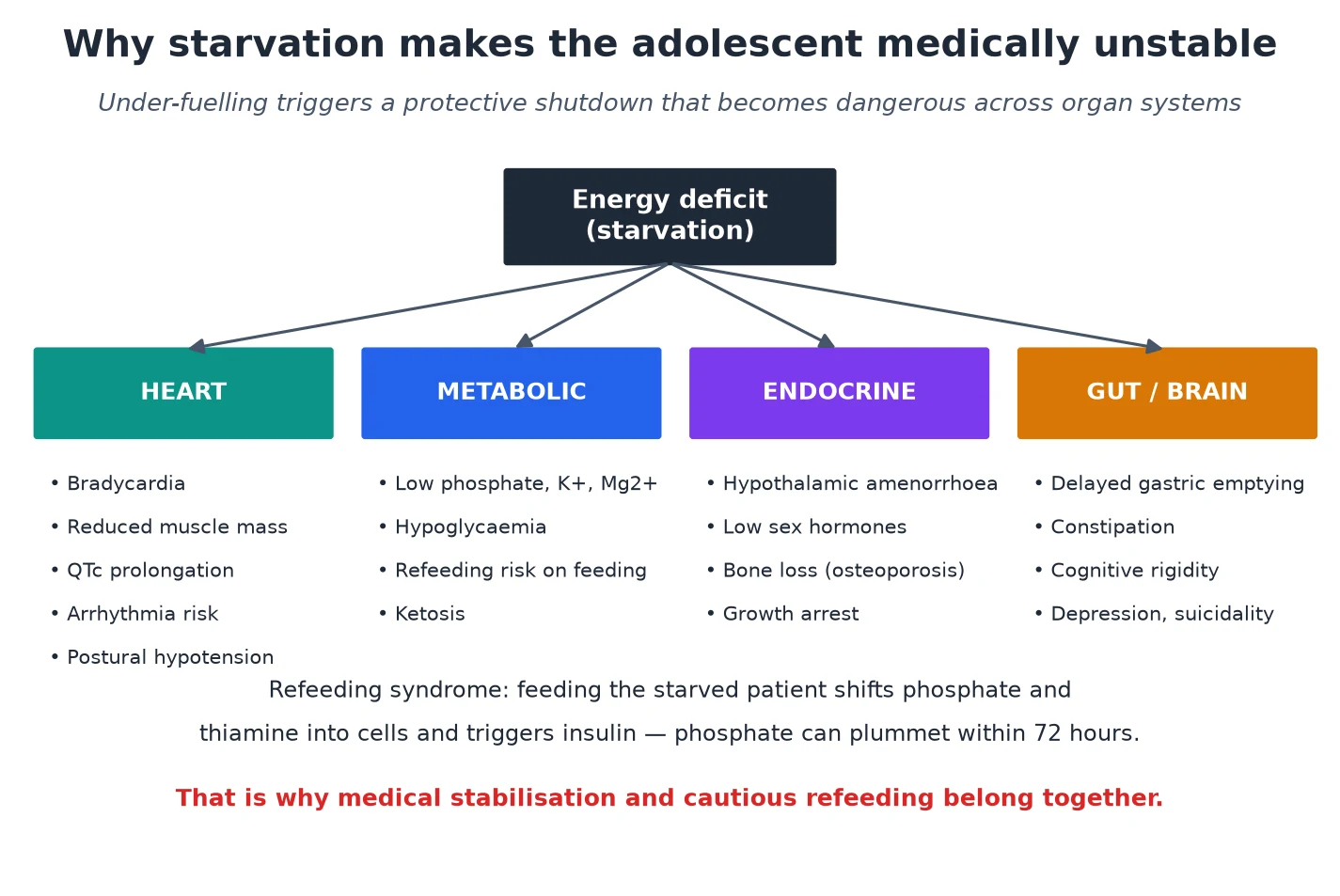
Read the figure like this: every arrow begins at energy deficit, which is why restoring nutrition is the definitive treatment — and why it must be done carefully, because feeding is itself the trigger for refeeding syndrome. [9]
Clinical Presentation
Eating disorders rarely present as "I think I have an eating disorder." They present as weight loss, food rules, missed periods, fainting, abdominal pain, or a parent who is frightened. The first clinical skill is to hear the pattern behind a vague complaint. [4] [11]
The restrictive picture is food avoidance dressed up as virtue — vegetarianism that tightens weekly, cutting out carbohydrates, eating alone, secret exercise, withdrawal from family meals. Weight falls, growth stalls, menses stop. The young person is often cold, tired, irritable and convinced they are "fine" or even "overweight." [6] [4]
The binge-purge picture hides better because weight is often normal. Look for calluses on the back of the hand (Russell's sign from inducing vomiting), parotid enlargement, dental erosion, sore throat, and electrolyte-driven symptoms — palpitations, weakness, muscle cramps, fainting. Bulimia can present as a first seizure or arrhythmia from hypokalaemia. [4] [14]
The ARFID picture is restriction without body-image distress — a child who eats only three foods, gags on textures, or stopped eating after a choking episode, with faltering growth and nutritional deficiency. It overlaps heavily with autism spectrum and anxiety. The medical complications are real and increasingly documented. [13]
The red-flag presentation is physiological. Dizziness on standing, syncope, chest pain, palpitations, cold intolerance with lanugo hair, and rapid weight loss are signals that starvation has reached the cardiovascular system. Any of these in a restricting adolescent is an emergency assessment, not a routine referral. [5] [7]
Differential Diagnosis
The differential for weight loss and food avoidance in an adolescent is long, and an eating disorder is a diagnosis of behaviour reached after reasonable exclusion of organic causes — but never delay instability assessment while you work through the list. [4]
| Presentation | Also consider | Distinguishing feature |
|---|---|---|
| Rapid weight loss, food refusal | Inflammatory bowel disease, coeliac disease, type 1 diabetes | Organic disease has diarrhoea, blood, pain, raised inflammatory markers; eating disorder has body-image distress and food fear |
| Amenorrhoea with weight loss | Hyperthyroidism, adrenal insufficiency, hypothalamic tumour | Endocrine causes lack the body-image and behaviour pattern; check thyroid and consider imaging if atypical |
| Vomiting and electrolyte disturbance | Gastro-oesophageal reflux, cyclic vomiting, pregnancy | Purging is self-induced, covert, and paired with body dissatisfaction |
| Faltering growth and restricted diet | ARFID vs food allergy, autism-related restriction, swallow disorder | ARFID has no drive for thinness; assess neurodevelopment and fear responses |
| Syncope and bradycardia | Vasovagal syncope, congenital long-QT, postural orthostatic tachycardia | In an eating disorder the bradycardia is structural, with weight loss and purging history |
Separate functional from organic weight loss: organic illness usually wants to eat but cannot, or loses weight despite eating; an eating disorder avoids or hides food while fearing weight gain. The exception is ARFID, where the young person genuinely cannot eat certain foods — but again without body-image drive. [13]
Separate primary eating disorders from disordered eating secondary to another condition — diabetes (insulin restriction for weight loss, sometimes called diabulimia), inflammatory bowel disease, or depression. The primary illness must be treated alongside the eating behaviour. [4]
Clinical & Bedside Assessment
The assessment has two jobs: confirm the behaviour, and quantify the physiological danger. Do both in the same visit, and see the adolescent alone for part of it — disclosure collapses the moment a parent answers for them. [6] [11]
1. Take a focused eating and weight history alone
Ask what is eaten, what is avoided, portion sizes, secrecy, binges, vomiting, laxatives, and driven exercise. Ask about menstruation, mood, self-harm and substance use. Use a structured psychosocial frame (HEEADSSS) so sensitive material surfaces in a predictable, safe sequence. [6]
2. Apply a screening tool
The SCOFF questionnaire is five questions — Sick (do you make yourself sick?), Control (do you worry you have lost control?), One stone (have you lost more than one stone, about six kilograms, recently?), Fat (do you believe yourself to be fat when others say you are thin?), Food (does food dominate your life?). Two or more positive answers is a positive screen and warrants full assessment. [1] [10]
3. Weigh and plot
Weigh in a gown after voiding, with the patient facing away from the number if seeing it distresses them. Plot weight and body-mass index against population references and express as a percentage of median body mass index for age and sex. A single weight is a snapshot; the rate of change often tells you more than the absolute number. [4] [7]
4. Measure vital signs — including a standing test
Record resting heart rate, blood pressure and temperature lying down, then stand the patient up and repeat the heart rate and blood pressure after two minutes. A marked postural heart-rate rise, a systolic blood-pressure drop, or a resting bradycardia are the cardiovascular red flags that flag instability. The standing test is the most often omitted and the most informative. [5] [7]
5. Examine for physical signs
Look for bradycardia, hypotension, cold and blue peripheries, lanugo hair, parotid enlargement, Russell's sign, dental erosion, and — in restrictive disease — the loss of secondary sexual characteristics or stunting. Measure growth and pubertal stage. [4] [14]
6. Keep the family engaged without breaching trust
Bring the family back in for the plan. Frame the illness as serious but treatable, agree who needs to know what, and follow the consent and confidentiality principles for adolescents — conditional confidentiality, with safety thresholds that override. [6]
Investigations
There is no single test that diagnoses an eating disorder, but a focused panel quantifies how unstable the patient is and what must be corrected before and during refeeding. [4]
Bedside and bloods. A 12-lead ECG for QTc and rhythm is non-negotiable in any restricting or purging adolescent. Bloods include full blood count, urea and electrolytes, magnesium, phosphate, calcium, glucose, liver function, thyroid function, and a venous blood gas if acutely unwell. Low potassium, low phosphate, low magnesium, hypoglycaemia or a raised urea from dehydration each change the management. [4] [14]
Baseline refeeding markers. Because refeeding shifts phosphate, potassium and magnesium into cells, measure them at baseline and recheck within the first days of feeding. A low baseline phosphate or a rapid fall after feeding is refeeding syndrome until proven otherwise. [9] [4]
Body composition and bone. A bone-density scan (DEXA) is indicated in persistent low-weight restrictive disease to detect osteoporosis, a common and under-recognised complication. Sit-up and exercise tolerance, and markers of growth, round out the assessment. [4] [14]
Rule out organic mimics. Inflammatory markers, coeliac serology, thyroid function and — where the picture is atypical — targeted endocrine or imaging tests exclude the differentials listed above, so that an eating disorder is confirmed rather than assumed. [4] [13]
SCOFF — five-question eating-disorder screen
Management — Resuscitation
When an adolescent with an eating disorder becomes medically unstable, the resuscitation priorities are the heart, the glucose and the electrolytes — and that starts with deciding they are unstable. [5] [7]
- Recognise and admit. Any physiological red flag — severe bradycardia, hypotension, prolonged QTc, syncope, hypoglycaemia — triggers admission to a paediatric inpatient setting with eating-disorder experience. Do not manage instability as an outpatient. [5]
- Cardiac monitoring. Continuous cardiac monitoring for the bradycardic, prolonged-QTc or hypokalaemic patient. Correct potassium and magnesium to shorten repolarisation; avoid medications that further prolong the QT. [14] [4]
- Correct electrolytes and glucose. Treat hypoglycaemia and replace potassium, magnesium and phosphate intravenously per local protocol before and during refeeding. Dehydration from purging or restriction needs careful fluid correction — aggressive fluids can precipitate heart failure in a starved myocardium. [4] [9]
- Begin cautious refeeding. Start nutrition at a conservative starting energy intake and advance carefully, because feeding is the trigger for refeeding syndrome. The detailed refeeding protocol — calories, phosphate and thiamine prophylaxis, monitoring frequency — belongs to the companion refeeding and multidisciplinary-care topic. [9] [4]
In an emergency — cardiac arrest from arrhythmia, severe hypoglycaemia with collapse, or a suicide attempt — treat under the emergency or best-interests doctrine, stabilise first, then return to consent and capacity as soon as the young person can engage. [4] [5]
Management — Definitive & Stepwise
The routine pathway for a stable adolescent
- Confirm the diagnosis and rule out mimics with history, SCOFF, examination and the targeted blood and ECG panel. [4] [1]
- Assess instability with vital signs including a standing test, weight and percentage of median body mass index. If unstable, exit to admission. [5] [7]
- Engage the adolescent and family. Name the illness as serious and treatable, agree confidentiality boundaries, and recruit the family as allies — family-based treatment is first-line for adolescent anorexia. [3] [6]
- Refer to a multidisciplinary specialist service — paediatric medicine, child and adolescent mental health, dietetics, and a therapist trained in family-based or evidence-based treatment. [3] [4]
- Set follow-up intensity by risk. Stable adolescent with engaged family: close specialist follow-up. Any instability or rapid loss: same-day review or admission. [5]
Escalation triggers
- New bradycardia, hypotension or postural change: admit. [5]
- Prolonged QTc or arrhythmia: cardiac monitoring and electrolyte correction. [14]
- Persistent weight loss despite outpatient care: step up to day-patient or inpatient. [3]
- Suicidal ideation or self-harm: urgent mental-health and safety pathway. [4]
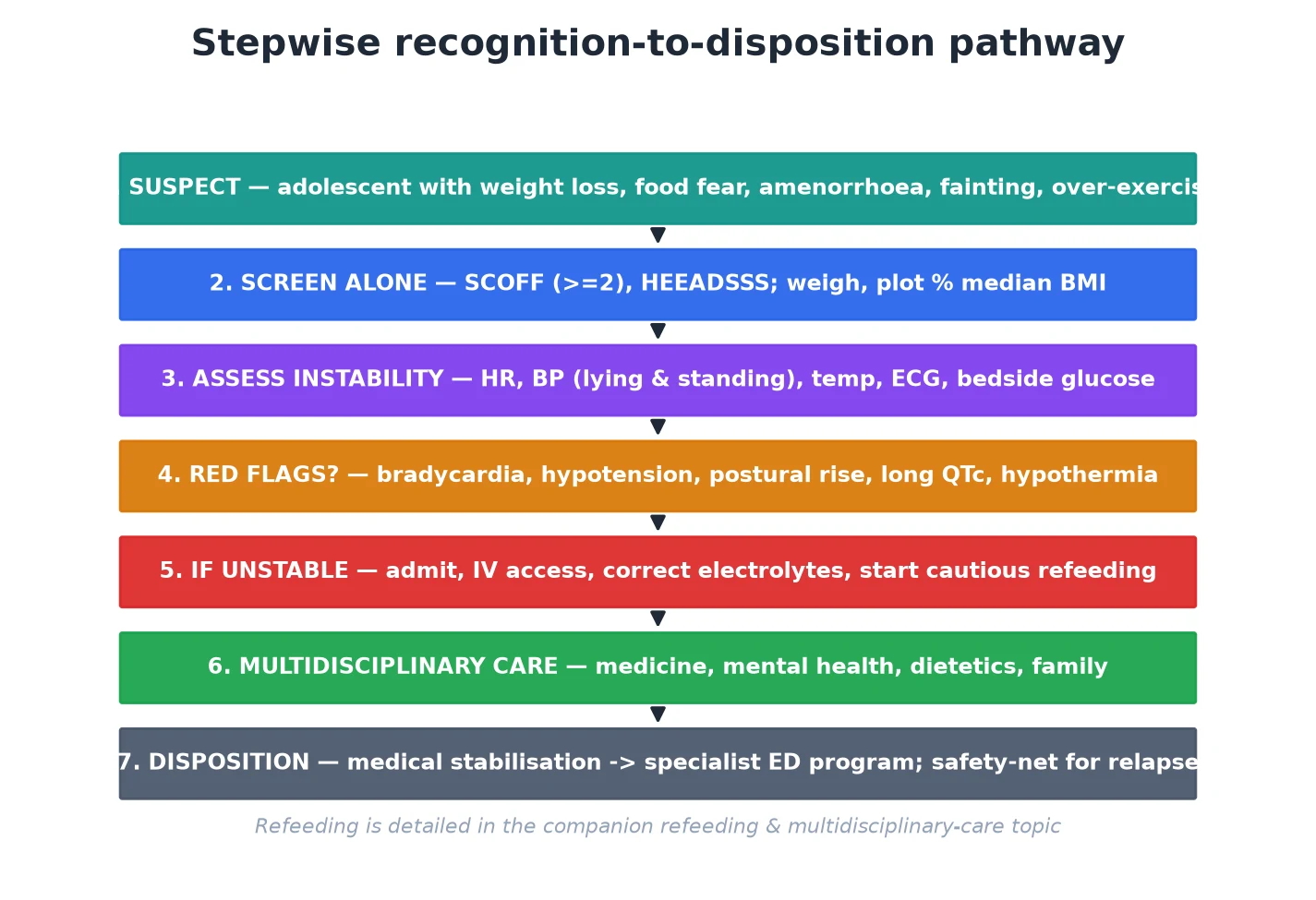
Triage decision in the first visit
Suspect
Weight loss, food rules, missed periods, fainting, over-exercise
Screen alone
SCOFF two-or-more positive; HEEADSSS
Quantify risk
Weight, percentage median BMI, vitals lying and standing, ECG
Red flag?
Bradycardia, hypotension, postural change, long QTc, hypothermia, hypoglycaemia
Stable
Multidisciplinary outpatient care with close follow-up
Unstable
Admit, monitor, correct electrolytes, cautious refeeding
Specific Subtypes & Scenarios
Anorexia nervosa, restricting type is the highest-risk subtype. Present with restriction and driven exercise without regular binge or purge. The danger is cardiovascular: bradycardia, hypotension, prolonged QTc, and — on feeding — refeeding syndrome. Family-based treatment is first-line; medical stabilisation precedes and runs alongside it. [4] [9]
Anorexia nervosa, binge-purge type adds vomiting and laxative use to restriction, so electrolyte disturbance (hypokalaemia, metabolic alkalosis) compounds the cardiac risk. Check potassium and magnesium before and during treatment. [14] [4]
Bulimia nervosa sits at normal or higher weight with cycles of binge and compensation. The medical risk is electrolyte-driven — arrhythmia and seizure from hypokalaemia — rather than starvation per se. Evidence-based psychotherapy (cognitive-behavioural therapy adapted for eating disorders) is first-line; antidepressant prescribing is a specialist decision. [3] [4]
Binge-eating disorder presents with distressing binges and no regular compensation, often at higher weight. The medical focus shifts to metabolic comorbidity and to avoiding weight-stigmatising care, while specialist psychotherapy addresses the binge behaviour. [4] [6]
ARFID restricts food without body-image drive — sensory sensitivity, fear of choking or vomiting, or low interest. Complications include faltering growth, nutritional deficiency and, in low-weight cases, refeeding risk. It overlaps with autism and anxiety, and management is distinct from body-image-focused therapies. The systematic evidence on its physical complications is now mature. [13]
Atypical anorexia meets full anorexia criteria at a non-low weight and is repeatedly missed. It carries the same bradycardia, prolonged QTc, amenorrhoea and bone loss; assess and admit on the same red flags. [4] [14]
The athlete (Relative Energy Deficiency in Sport). Driven training with insufficient fuelling produces low energy availability, menstrual dysfunction and impaired bone health — the RED-S spectrum, which overlaps with anorexia in the competitive adolescent. The IOC consensus frames assessment and return-to-play. [8]
Purging without an eating-disorder diagnosis (OSFED). Disordered eating that does not meet full criteria is still dangerous; assess behaviour and physiology, and do not discharge on a technicality. [4] [13]
Complications & Pitfalls
- Missing atypical anorexia because the weight is "normal" — the commonest lethal error. [4] [14]
- Omitting the standing test — the postural sign is the instability marker most often skipped. [5] [7]
- Not doing an ECG — a prolonged QTc is silent until it causes an arrhythmia. [14]
- Refeeding too fast — precipitates refeeding syndrome with hypophosphataemia; start conservative and monitor. [9]
- Overlooking suicide risk — death in anorexia is as much from suicide as from medical causes. [2]
- Failing to engage the family — family-based treatment needs the family as the therapeutic agent. [3] [6]
- Weight-stigmatising higher-weight adolescents — delays diagnosis of bulimia and atypical anorexia. [6] [4]
- Treating only the body — an eating disorder is a mental illness; medical stabilisation without mental-health care relapses. [3]
Prognosis & Disposition
Prognosis in eating disorders is the trajectory of weight restoration, medical stability, mental recovery and relapse risk — and early, intensive, multidisciplinary care improves it. [3] [4]
Routine disposition: a stable, engaged adolescent with no red flags, a normal ECG, stable electrolytes and a supportive family moves to specialist multidisciplinary outpatient care with close follow-up. [4] [6]
Early-review disposition: a borderline adolescent — mild bradycardia, early postural change, rapid recent loss — needs review within days, explicit weight and safety-netting, and a low threshold to admit. [5] [7]
Urgent disposition: any red flag, prolonged QTc, syncope, hypoglycaemia, or suicidality means same-day admission. [5] [14]
Safety-net explicitly at every contact: what to do if dizziness, fainting, palpitations or rapid weight loss occur; who to call tonight; and when to return. The riskiest windows are the first weeks of refeeding and any period of acute psychosocial stress. Relapse is common and is not a moral failure — plan for it. [3] [9]
Over the longer arc, restoration of weight, menstruation and bone health, alongside mental recovery, defines a good outcome. Transition planning to adult services belongs in late adolescence for persistent illness. [4] [3]
Special Populations
Males. Under-diagnosed because presentations do not match the female stereotype; often focus on muscularity and leanness rather than thinness. Ask directly about body-image and supplement use. [6] [4]
Gender-diverse youth. Higher rates of eating disorders and body distress; affirming, non-stigmatising care is essential, with attention to how gender-affirming care and nutritional status interact. [6]
Higher-weight adolescents. Atypical anorexia and bulimia are missed here; assess on behaviour and physiology, never on size. [4] [6]
Athletes. RED-S overlaps with eating disorders; coordinate with coaches and use the IOC framework for return-to-play. [8]
Neurodivergent young people. ARFID is over-represented in autism and attention-deficit disorders; adapt communication and recognise sensory-driven restriction distinct from body-image illness. [13]
Young people in out-of-home care, migrant and refugee backgrounds, and socioeconomic disadvantage. Higher psychosocial risk and poorer access; reconstruct history actively, use interpreters, and remove practical barriers to specialist care. [6]
Young people with chronic illness. Diabetes (insulin restriction for weight loss), inflammatory bowel disease and other conditions raise disordered-eating risk; treat both the primary illness and the eating behaviour. [4]
Evidence, Guidelines & Regional Differences
Mortality evidence. Arcelus's meta-analysis of 36 studies established that anorexia nervosa carries one of the highest standardised mortality ratios in psychiatry — a number that should anchor every clinician's threshold to admit. [2]
Medical management. Golden and colleagues' update on the medical management of eating disorders in adolescents is the core generalist reference for assessing and stabilising these patients, and the higher-calorie refeeding randomised trial reframed how aggressively nutrition can be restored under monitoring. [4] [9]
Risk frameworks. The Junior MARSIPAN framework and the structured fifteen-minute consultation on medically unstable anorexia give an operational, traffic-light approach to triaging physiological risk in young people; they are widely used across the UK and adopted in adapted form elsewhere. [5] [7]
Screening. The SCOFF questionnaire and the US Preventive Services Task Force recommendation on screening for eating disorders define how to find cases early in primary care; the primary-care review by Peat and colleagues maps the practical gaps. [1] [10] [11]
Guidelines. The Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines, NICE guidance, and the IOC RED-S consensus frame treatment and the athlete-specific pathway. [3] [8]
ANZ: the RANZCP clinical practice guidelines and state-based child and adolescent eating-disorder services frame care; Junior-MARSIPAN-style triage is widely adopted in adapted form, with hospital protocols governing admission cut-offs. UK: NICE eating-disorders guidance and the Junior MARSIPAN framework (RCPsych CR168) define recognition and the red-flag admission criteria; specialist community eating-disorder services for children and young people are the treatment pathway. US: the AAP clinical reports and the USPSTF screening recommendation frame primary care; higher-calorie refeeding protocols originate largely from US centres, and admission criteria follow unit protocols. Canada: the Canadian Paediatric Society and provincial eating-disorder programmes frame care; the Greig Health Record supports adolescent preventive assessment. Check local protocols for operative thresholds.
State the principle and check local protocol: admission cut-offs, refeeding calorie starts and screening instruments vary between units and jurisdictions, so name the guideline you are quoting. [4] [9]
Exam Pearls
- Open every answer with behaviour and physiology, not weight: a normal-weight restricting adolescent can be the sickest in the room. [4] [14]
- Quote SCOFF with its five letters and the two-or-more threshold; it is the single most testable screening fact. [1] [10]
- Know the red flags cold — bradycardia, hypotension, postural heart-rate rise, prolonged QTc, hypothermia, hypoglycaemia — and that any one warrants admission. [5] [7]
- Always stand the patient up. The postural sign is the instability marker examiners reward you for remembering. [5]
- An ECG is mandatory in any restricting or purging adolescent — quote a prolonged QTc as the arrhythmia substrate. [14]
- Refeeding syndrome is feeding-triggered hypophosphataemia within about 72 hours; cite the refeeding RCT for conservative starts. [9]
- Mortality in anorexia is high — quote the Arcelus meta-analysis; death is from cardiac causes and suicide. [2]
- Family-based treatment is first-line for adolescent anorexia; the family is the treatment, not an obstacle. [3] [6]
- Atypical anorexia is not milder. Same red flags, same admission threshold. [4]
Self-test: which adolescent must be admitted?
A 14-year-old runner has lost eight kilograms over three months, eats only salad, and her resting heart rate is 38 with a postural heart-rate rise to 110 on standing. Her weight is within the "healthy" band. Answer: admit now. The bradycardia and marked postural rise are red flags, and atypical anorexia at a non-low weight carries the same danger as anorexia nervosa. Outpatient follow-up is unsafe. [5] [7] [4]
References
- [1]Morgan JF; Reid F; Lacey JH The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ, 1999.PMID 10582927
- [2]Arcelus J; Mitchell AJ; Wales J; Nielsen S Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Archives of general psychiatry, 2011.PMID 21727255
- [3]Hay P; Chinn D; Forbes D; Madden S; Newton R; Sumer-Kallio J; Touyz S; Ward W Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of eating disorders. Australian and New Zealand journal of psychiatry, 2014.PMID 25351912
- [4]Golden NH; Katzman DK; Sawyer SM Update on the medical management of eating disorders in adolescents. Journal of adolescent health, 2015.PMID 25659201
- [5]Marikar D; Reynolds S; Moghrabi O; Dave M; Snook J; Harris J Junior MARSIPAN (Management of Really Sick Patients with Anorexia Nervosa). Archives of disease in childhood. Education and practice edition, 2016.PMID 26407730
- [6]Golden NH; Schneider M; Wood C Preventing Obesity and Eating Disorders in Adolescents. Pediatrics, 2016.PMID 27550979
- [7]Allison E; Nana M; O'Dea C; Spettigue W; Norris M Fifteen minute consultation: A structured approach to the management of children and adolescents with medically unstable anorexia nervosa. Archives of disease in childhood. Education and practice edition, 2017.PMID 28193620
- [8]Mountjoy M; Sundgot-Borgen J; Burke L; Ackerman KE; Blauwet C; Constantini N; Lebrun C; Lundy B; Melin A; Meyer N; Mountjoy M International Olympic Committee (IOC) Consensus Statement on Relative Energy Deficiency in Sport (RED-S): 2018 Update. International journal of sport nutrition and exercise metabolism, 2018.PMID 29771168
- [9]Golden NH; Katzman DK; Glasofer DR; Attia E; Yager J; Lynch T; Stryjecki C; Mensah J; Vaccaro J; Long M; Schek E; Mahr E; Kreipe HE Higher-Calorie Refeeding in Anorexia Nervosa: 1-Year Outcomes From a Randomized Controlled Trial. Pediatrics, 2021.PMID 33753542
- [10]US Preventive Services Task Force Screening for Eating Disorders in Adolescents and Adults: US Preventive Services Task Force Recommendation Statement. JAMA, 2022.PMID 35289876
- [11]Peat CM; Huang S; Ranzenhofer LM; Cohen NR Addressing eating disorders in primary care: Understanding screening recommendations and opportunities to improve care. The International journal of eating disorders, 2022.PMID 35903970
- [12]Hartman-Munick SM; Silverstein S; Volpe-Krecker K; Zhang F; Hadland SE; Purtell N; Goncalves A; Richmond TK Association of the COVID-19 Pandemic With Adolescent and Young Adult Eating Disorder Care Volume. JAMA pediatrics, 2022.PMID 36342721
- [13]James RL; Khalsa S; Sharma A; Faruqi A; Sidiq M; Warnick J; Gallego J; Spettigue W; Norris MD; Katzman DK Physical health complications in children and young people with avoidant restrictive food intake disorder (ARFID): a systematic review and meta-analysis. BMJ paediatrics open, 2024.PMID 38977355
- [14]Trapani S; Mencaroni E; Rocchi A; Marciano C; Belli S; Di Donato M; Rigante D; Stagi S Medical Complications of Anorexia Nervosa. Pediatrics, 2025.PMID 40659363