Paeds · adolescent-and-young-adult-medicine
Medication adherence and treatment fatigue
Also known as Medication adherence in adolescents · Treatment fatigue · Treatment burnout · Non-adherence in chronic adolescent disease · Self-management support in young people · Concordance and persistence
A fellowship approach to assessing and promoting medication adherence in adolescents living with chronic disease, recognising treatment fatigue as an expected phase, measuring adherence with the right tool, mapping modifiable barriers, and applying a non-judgemental, engagement-preserving stepwise intervention across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A registrar inherits a 16-year-old liver-transplant recipient whose tacrolimus level has been subtherapeutic for three visits. The bloods are fine, the graft is quiet, and the family is "managing." At the next appointment the young person is jaundiced, and a biopsy shows rejection. The missed work was not a rare complication. It was a teenager who had quietly stopped taking a medicine that marked him out as different from his friends — and nobody had asked the question in a way he could answer. [10] [1]
Medication adherence is the extent to which a person's behaviour in taking medication corresponds to agreed recommendations from a health-care provider. The word agreed does the heavy lifting: adherence is a shared, negotiated behaviour, which is why the older term compliance — implying obedience to an instruction — has been retired in favour of language that does not blame. [1] [5]
Adherence is not one behaviour but three phases. Initiation is whether the young person ever starts the medicine. Implementation is whether they take it as prescribed day to day. Persistence is whether they keep taking it over the months and years the condition demands. A teenager who starts dutifully, drifts into missed doses at exam time, and stops altogether at university has failed implementation first and persistence second — and each phase needs a different conversation. [4] [1]
Treatment fatigue (sometimes called treatment burnout) is the experiential and developmental state in which the cumulative burden of a regimen — the pill count, the monitoring, the identity it confers, the future it promises but never delivers — erodes the motivation to keep going. It is the long shadow of a chronic illness in a young person whose brain is wired to value today over a distant tomorrow. Fatigue is the precursor to most non-adherence, and meeting it with a lecture only accelerates the disengagement it warns of. [1] [9]
The adherence conversation, in six moves
Frame
Curious, non-judgemental, time alone; normalise that everyone misses doses.
Measure
Self-report to open; refill records and objective data to triangulate.
Map barriers
Patient, regimen, family, system — probe the darkest first.
Agree goals
Shared decision-making aligned with the young person's values.
Tailor & simplify
Regimen change, reminders, family support, technology.
Re-measure & re-engage
Named next contact and a low-threshold way back in.
Classification
Classify non-adherence by phase, by intention, and by barrier domain. The phase tells you what is happening; the intention tells you why; the domain tells you where to intervene. [1] [4]
Phase of behaviour
Initiation, implementation, and persistence are distinct failures. A young person who never fills the first prescription, one who takes doses erratically, and one who stops at the two-year mark each need a different assessment. Collapsing all three into a single "non-adherent" label hides the intervention. [4] [5]
Intentional versus unintentional
Unintentional non-adherence is practical: forgetting, regimen complexity, cost, access, formulation. Intentional non-adherence is a reasoned decision to stop or reduce, usually built on a beliefs calculus — the perceived necessity of the medicine weighed against its perceived concerns or harms. The split matters because a reminder app does nothing for a teenager who has decided the medicine is unnecessary, and a beliefs conversation does nothing for one who simply cannot afford the refill. [1] [11]
Barrier domains
The barriers cluster into four interacting domains. Patient and development covers the adolescent neuroscience of delayed reward, emerging autonomy, mood, and neurodiversity. Regimen and disease covers pill burden, side-effects, the asymptomatic-on-treatment trap, cost and formulation. Family covers the parent–teen supervision conflict and the household's necessity–concerns beliefs. System covers transition, fragmented records, access, and confidentiality leaks. Behaviour emerges from all four, so a plan that fixes only one rarely holds. [1] [8]
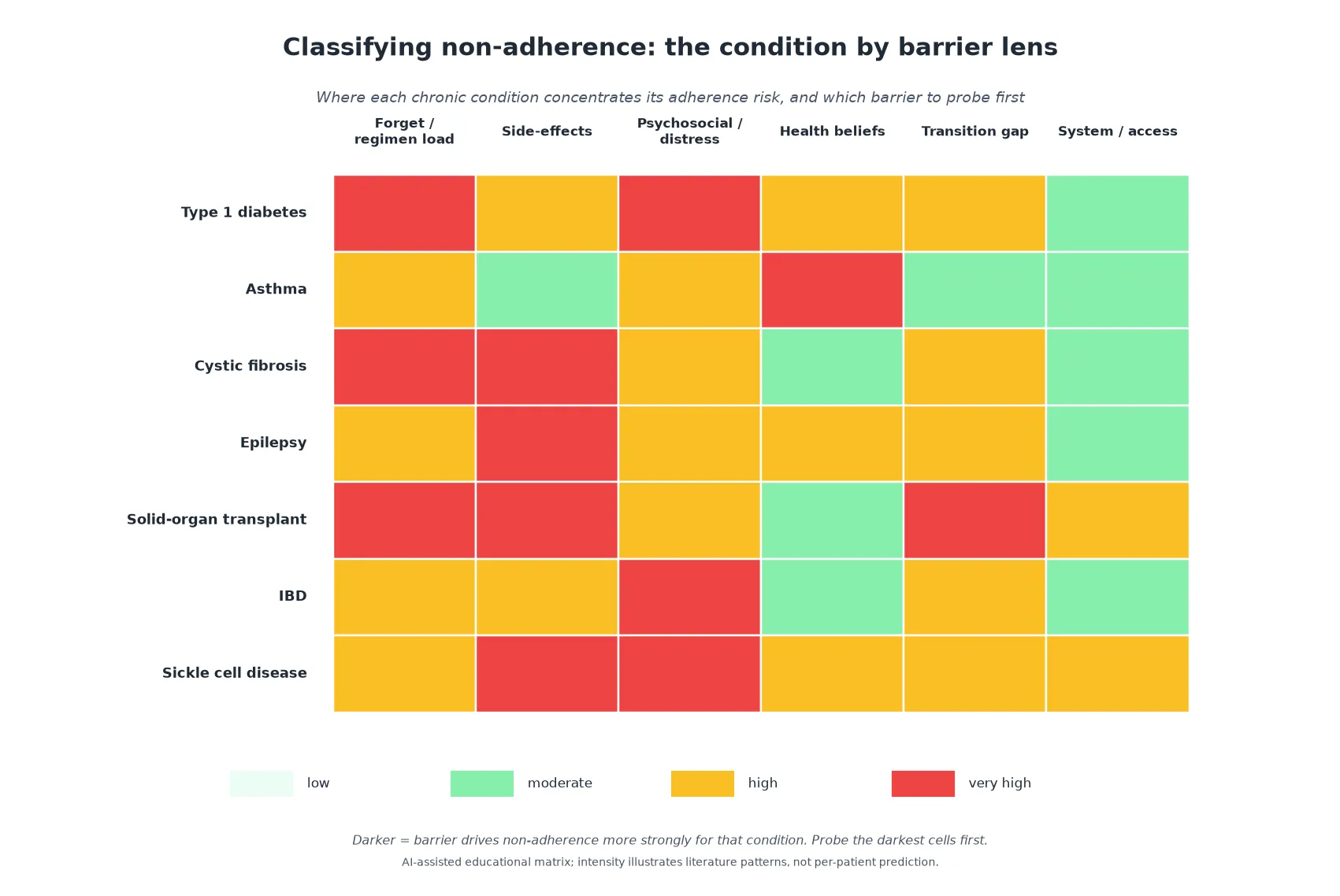
Read the figure like this: the pattern tells you the entry point. For transplant and cystic fibrosis, the burden and side-effect columns dominate; for asthma, beliefs; for IBD and diabetes, psychosocial distress. The first question you ask should follow that gradient. [8] [11]
Unintentional
Practical failure
- Forgetting, complex regimen, cost, access
- Reminder tools, simplification, supply solve it
- Behaviour change not the core issue
- Often the easier fix
Intentional
Reasoned decision
- Necessity–concerns calculus
- Asymptomatic so feels cured
- Identity, stigma, peer burden
- Needs beliefs work and shared goals
Treatment fatigue
Cumulative burnout
- Years of burden erode motivation
- Asks 'when can I stop'
- Resentment of the regimen
- Needs re-engagement, not a lecture
Epidemiology & Risk Factors
Adherence is the single largest reversible determinant of outcome in chronic adolescent disease — larger than most drug choices. Reviews across conditions converge on the same uncomfortable number: roughly half of young people take their long-term medication suboptimally, and the dip steepens across the teenage years and around transfer to adult care. [2] [6]
In adolescents and young adults with cancer and other chronic conditions, systematic review evidence links non-adherence to measurable harm — relapse, graft loss, worse survival and psychological outcomes — and identifies predictors that are almost identical across diseases: regimen complexity, side-effects, psychiatric comorbidity, poor family functioning, and weak transition support. The drivers travel together because the biology of being an adolescent does. [2] [4]
The developmental risk is real and explainable. The adolescent reward and socio-emotional system matures well before the prefrontal control system that values a distant future, so a medicine whose only reward is "something bad will not happen in twenty years" is neuro-developmentally hard to prioritise. Add mood disorder, neurodiversity, stigma, cost, or a fragmented care system, and adherence drifts toward lapse. [1] [9]
Social determinants amplify every domain. Poverty, housing instability, food insecurity, racism, out-of-home care, youth-justice involvement, and refugee or migrant status reduce access, intensify stigma, and fracture continuity. When a young person cannot reliably store a refrigerated medicine or charge a device, non-adherence is structural, not behavioural, and no amount of counselling will fix it. [1] [5]
Pathophysiology
Adherence fails for understandable reasons, and a clinician who knows the mechanism counsels without blame. [9]
The dual-systems model of adolescent brain development describes two curves on different clocks. The reward and socio-emotional circuitry matures early and runs hot through mid-adolescence; the prefrontal cognitive-control circuitry matures later. In the gap between them, present reward consistently outbids future benefit — precisely the trade-off a daily chronic-disease medication demands. A teenager who genuinely intends to take every dose and still misses some is not lying or lazy; they are running the neurobiology of their age. [1] [9]
Treatment fatigue is the clinical expression of that gap accumulating over years. The regimen never rewards, the side-effects always cost, the identity it confers (the sick kid, the different one) keeps hurting, and the asymptomatic present whispers that the medicine is no longer needed. Fatigue is not a single event but a slow erosion: the dose moved from morning to "later," the later to "tomorrow," the tomorrow to a quiet stop. Meeting it with escalation of monitoring usually confirms the young person's suspicion that the system values the drug level more than them. [1] [9]
The downstream pathophysiology is condition-specific but follows one logic — the disease returns. Missed insulin drives hyperglycaemia and diabetic ketoacidosis; withdrawn antiseizure medication lowers seizure threshold and raises sudden unexpected death in epilepsy risk; lapsed immunosuppression invites rejection and graft loss; interrupted hydroxyurea invites sickle cell crisis; stopped controller therapy invites asthma exacerbation. The mechanism of harm is the disease the treatment was suppressing, now unopposed. [4] [12]
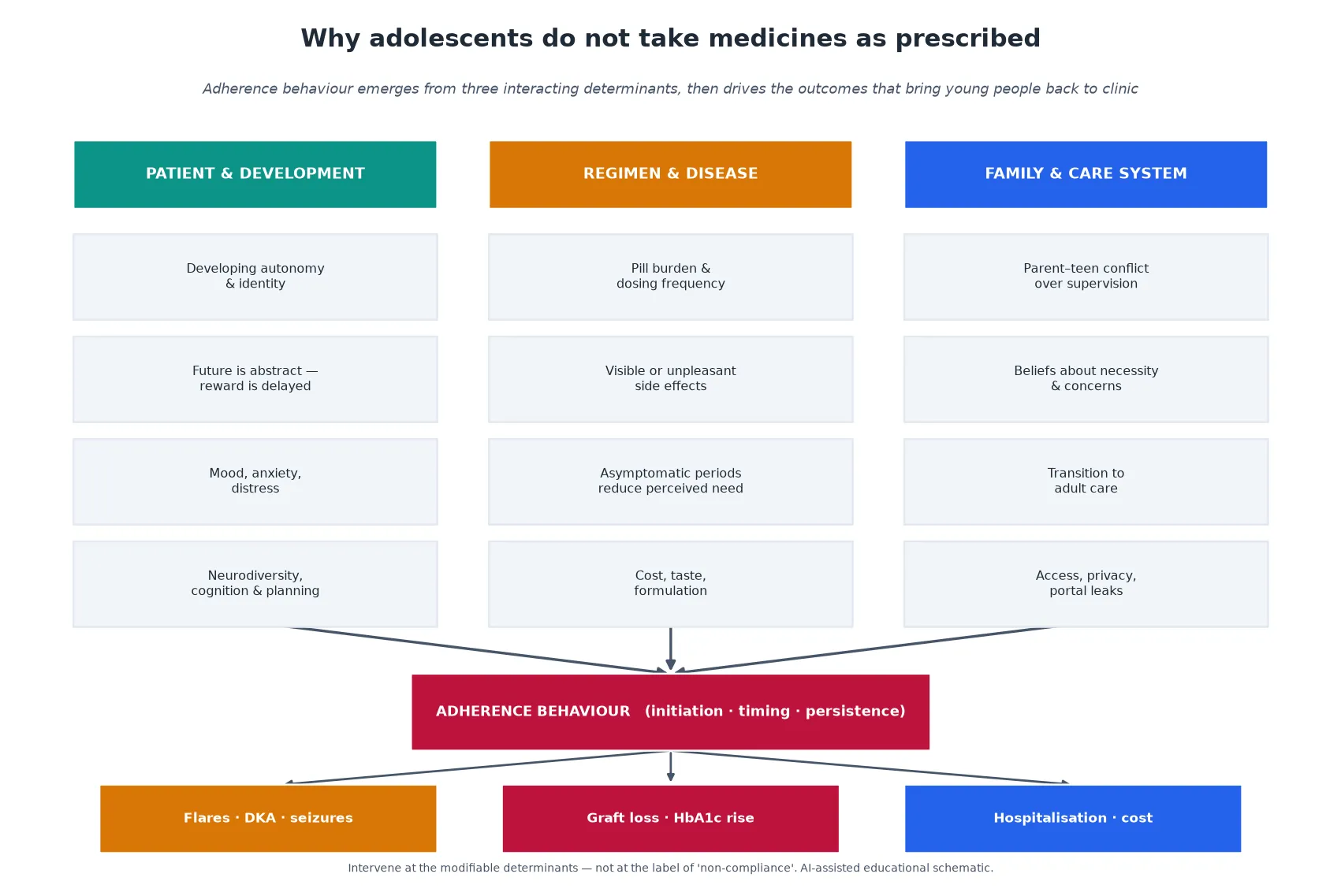
Read the figure like this: the arrow runs from determinants through behaviour to outcomes. If you intervene only at the behaviour — demanding the dose — you have ignored the upstream drivers that will reproduce the lapse. The durable fix sits in the determinant columns. [5]
Clinical Presentation
Non-adherence rarely walks in announcing itself. It presents across a spectrum from the obvious to the carefully hidden, and the hidden end is the more dangerous one. [1]
Overt presentations are the easy cases: missed refills, prescriptions never collected, erratic clinic attendance, and disease control that has quietly deteriorated. The young person may name the problem directly if they trust you — "I've been rubbish with my tablets" — and the work is then straightforward. [7] [12]
Covert presentations are where harm hides. Self-report can be near-perfect while objective data tell another story; a parent may confidently report the doses they watched weeks ago but not the ones they assumed this week; a teenager ashamed of stopping may nod through every review. A request to stop a visible medication — the acne-causing steroid, the weight-gaining insulin, the immunosuppressant that marks transplant — is a covert disclosure of fatigue wearing the costume of a clinical question. [9] [1]
Treatment fatigue presenting before non-adherence has its own tell-tale signs: boredom with the regimen, the recurring question of "when can I stop," resentment of the monitoring, and a growing conflict between the young person's identity and the sick-role the treatment enforces. These are not gripes to manage; they are the prodrome of lapse. [1]
Acute presentations arrive in emergency departments: diabetic ketoacidosis from missed or omitted insulin, a seizure cluster after withdrawn antiseizure medicine, a sickle cell pain crisis after lapsed hydroxyurea, or jaundice and graft tenderness heralding transplant rejection. Here the immediate task is resuscitation and stabilisation — the adherence cause is dissected afterwards, in safety. [4] [12]
Differential Diagnosis
When control deteriorates, non-adherence is the leading explanation — but it is a diagnosis of exclusion built on evidence, not a default label for an inconvenient patient. [4]
| What it looks like | Safer framing question | Do not miss |
|---|---|---|
| "Non-compliant" with rising HbA1c | Is the regimen right, and is a new co-morbidity present? | Coeliac disease, thyroid disease, evolving diabetes type |
| Erratic antiseizure levels | Is this adherence, absorption, or an interacting new drug? | Enzyme-inducing interaction, true pharmacoresistance |
| Rejection after stable graft | Is this fatigue, access to tacrolimus, or rejection despite adherence? | Adherence-independent rejection, infection |
| "Won't take" hydroxyurea | Is the dosing tolerable and the monitoring reachable? | Cytopenia on current dose, access to blood counts |
| Poor asthma control | Is the technique, the device, or the belief the problem? | Wrong inhaler technique, parent withholding controller |
The core discriminator is whether the deterioration fits a behavioural pattern or a disease pattern. A sudden step-up in requirements after years of stability, with subtherapeutic drug levels and a young person nearing transition, points to adherence; a gradual rise across every measure with therapeutic levels points to progression or a new driver. Test the hypothesis both ways before settling. [4] [7]
Always separate the driver from the consequence. A teenager labelled "non-compliant" may have depression, an unsafe home, a formulation they cannot swallow, or a parent withholding the controller on belief grounds. Blaming the patient for a family or system driver is the cardinal error of this topic, and it closes the door on the disclosure that would reveal it. [1] [11]
Clinical & Bedside Assessment
1. Open and frame
Greet the young person first, secure time alone, and open the adherence conversation with a normalising, non-judgemental line — "Most people miss doses; I'd rather hear the real story than the tidy one." The frame determines whether the rest of the assessment returns truth or performance. [1] [13]
2. Take a structured adherence history
Probe the three phases separately. Ask about initiation (did you ever start it?), implementation (how do you actually take it day to day — mornings, weekends, when you're out?), and persistence (have you ever stopped for a while?). A specific, behavioural question — "of the last seven days, how many did you take all the doses?" — beats a global "do you take your medicine?". [1] [14]
3. Map the barriers across the four domains
Work through patient and development, regimen and disease, family, and system. Ask about mood, sleep and distress; about side-effects, taste and burden; about who supervises and whether that causes conflict; about cost, access, privacy and the portal. Where a domain lights up, that is the intervention target. [8] [5]
4. Screen for the adherence suppressors
Depression, anxiety and diabetes distress directly suppress self-management behaviour, and they are common. A brief mood screen is part of the adherence assessment, not a separate referral. Screen for insulin omission for weight control, for substance use, and for the "why now" behind any change. [9] [1]
5. Explore identity, stigma and the meaning of the medicine
Ask what the medicine means to the young person — does it mark them out, remind them they are sick, threaten a body they are trying to build? The identity load of a regimen is an adherence determinant that no app can fix, and naming it often loosens it. [1] [9]
6. Involve the family while protecting autonomy
Bring the family in to map the supervision dynamic and the household beliefs, but keep the adolescent's voice central and protect confidential content. A parent who polices every dose can be the very thing pushing the young person toward covert non-adherence. [11] [1]
Investigations
Adherence is assessed primarily by conversation triangulated with objective data — not by a single laboratory number. No measure captures the whole behaviour, so measure multimodally and read the pattern. [7] [14]
Self-report is where the conversation begins. Validated brief scales and patient-reported outcome instruments open the door without surveillance, and they correlate only modestly with objective truth — which is exactly why they are a starting point, not a verdict. Their strength is that they invite honesty rather than punish it. [14] [6]
Refill and claims records — medication possession ratio and proportion of days covered from pharmacy data — estimate implementation over time without relying on memory. They miss free samples, shared supplies, and doses bought but not taken, but they are among the most practical longitudinal measures in real clinics. [6] [2]
Objective measures triangulate the story. Therapeutic drug levels (tacrolimus, antiseizure drugs) catch both under-dosing and white-coat adherence — the burst of good behaviour before a clinic visit. Electronic monitoring caps, pump and continuous-glucose-monitor downloads, and biomarkers such as HbA1c each capture a different facet: levels confirm exposure, downloads confirm behaviour, biomarkers confirm effect. Read them together, because each can mislead alone. [7] [10]
Low-value patterns to abandon: surprise or punitive drug-level testing; relying on a single uncorroborated metric; treating a self-reported "fine" as proof; and using objective data as evidence for a lecture rather than a prompt for curiosity. When self-report and objective data disagree, the discordance is the conversation, not the indictment. [7] [1]
Management — Resuscitation
A routine adherence review can turn into an emergency in one disclosure or one set of results. Recognise the exit point and take it. [4]
- Stabilise physiology first. For DKA, follow the standard paediatric fluid, insulin and electrolyte protocol; for seizure cluster, abort with first-line rescue therapy and protect the airway; for sickle crisis or acute chest, give analgesia, oxygen and hydration per protocol; for suspected rejection, involve the transplant team urgently for biopsy and immunosuppression. [12] [10]
- Do not leave the young person alone with a crisis and a lecture. The disclosure that follows an adherence-related emergency is the most valuable moment you will get — protect it with psychological safety, not blame. [1] [13]
- Involve the specialist team early for high-stakes regimens (transplant, insulin, antiseizure), because the acute plan and the adherence plan must be built together. [10] [5]
The adherence cause is dissected after physiology is safe, never instead of it. [4]
Management — Definitive & Stepwise
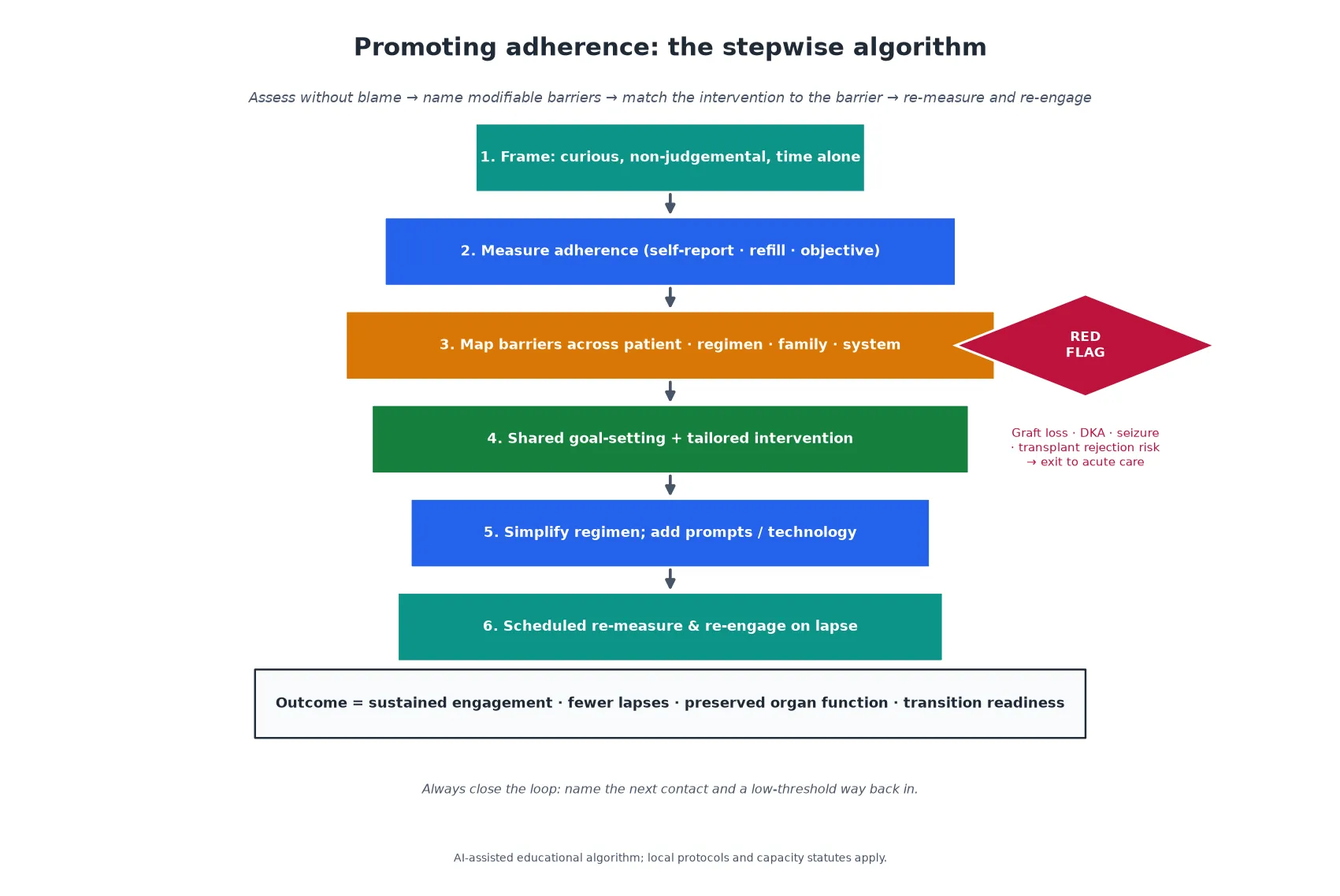
Read the figure like this: the red diamond overrides every step. Any acute consequence of non-adherence exits the routine pathway before you reach the intervention — and when you return to the pathway, you return without blame. [4]
Step 1 — Frame, then measure
Open with a non-judgemental, normalising line and time alone. Add the measurement that fits the condition — self-report plus refill or objective data — so the conversation is grounded in pattern, not impression. [1] [14]
Step 2 — Map barriers and probe the darkest first
Use the four-domain map to find where the risk concentrates, then lead the intervention there. A regimen-burden problem wants simplification; a beliefs problem wants a necessity–concerns conversation; a system problem wants access and continuity fixes. [8] [5]
Step 3 — Agree shared goals with motivational interviewing
Shared decision-making aligns the regimen with what the young person actually wants — to play sport, to fit in, to finish school, to feel normal. Motivational interviewing, with its open questions, affirmations, reflective listening and summaries, has meta-analytic support for improving adherence, and the skill is to evoke the young person's own reasons for taking the medicine rather than to impose yours. [13] [3]
Step 4 — Simplify the regimen, with the specialist team
Where licensed and safe, simplify — once-daily dosing, combination formulations, route or device changes. This is a specialist-team decision, not a registrar improvisation, because simplifying a transplant, insulin or antiseizure regimen wrongly can cause the very crisis you are trying to prevent. [5] [10]
Step 5 — Add prompts, reminders and technology
Pill organisers, timed reminders, app-based trackers and device downloads support implementation, especially for the unintentional, forgetting end of the spectrum. Their effect is modest and person-dependent, so match the tool to the barrier rather than prescribing an app reflexively. [14] [3]
Step 6 — Behavioural and family-based support
Problem-solving therapy, behavioural family systems approaches and group programmes have evidence in paediatric chronic disease, and they target the family and psychosocial drivers that no pill or app reaches. Involve psychology early, not only after a crisis. [3] [9]
Step 7 — Re-measure and re-engage
Name the next contact, schedule re-measurement, and build a low-threshold way back in. Re-engagement after a lapse is the default plan, because lapses are expected — the outcome is sustained engagement, not perfect compliance. [5] [1]
Specific Subtypes & Scenarios
Type 1 diabetes. Insulin adherence collides with diabetes distress, body image and the risk of insulin omission for weight control. Device downloads from pump and continuous glucose monitoring give an honest, granular picture; diabetes distress must be screened for directly because it suppresses self-management more powerfully than most regimens. [9] [1]
Asthma. Controller adherence fails most often on beliefs — the household conviction that inhaled corticosteroids are dangerous or unnecessary — and on technique rather than intention. Watching the young person use the inhaler is part of the assessment, and addressing parent beliefs is part of the plan. [11]
Cystic fibrosis. The regimen burden is among the highest in paediatrics, and the modulator era has shifted but not removed it. Multi-method assessment is essential because self-report, refill and electronic monitoring diverge widely in this population. [7]
Epilepsy. The asymptomatic-on-treatment trap is sharpest here: a young person seizure-free for years concludes the medicine is no longer needed, and withdrawal invites seizure cluster and raises the risk of sudden unexpected death in epilepsy. Driving, autonomy and the developmental timing of the question make this a recurrent flashpoint. [12]
Solid-organ transplant. The stakes are existential — lapsed immunosuppression drives rejection and graft loss, and the risk clusters at transfer to adult care. Transition readiness, confidential adolescent-only time, and an honest relationship with the transplant team are the protective triad. [10]
Inflammatory bowel disease and sickle cell disease. In IBD, steroid and biologic burden and body-image concerns drive fatigue, and anxiety and depression compound the barrier. In sickle cell disease, hydroxyurea adherence falters on the asymptomatic trap and on access to monitoring, and the transition window again concentrates risk. [8] [6]
Complications & Pitfalls
- A punitive or shaming response to non-adherence destroys the future disclosure on which everything depends. [1] [13]
- The label "non-compliant" is a self-fulfilling harm; reframe it as "struggling with adherence," because language shapes whether the young person will tell you the truth next time. [1] [5]
- Taking self-report at face value misses the cohort who report perfection while their drug levels and downloads tell another story. [7] [10]
- Surprise or punitive drug-level testing breaches trust and confidentiality and suppresses honest conversation for years. [1] [14]
- The transition cliff — transfer to adult care with poor handover — is a predictable, preventable cause of graft loss, DKA and disengagement, and leaving it unmanaged is a system error dressed as a patient one. [10]
- Focusing only on the patient misses the family beliefs and system gaps that keep the behaviour in place. [11] [5]
Prognosis & Disposition
Prognosis here is the trajectory of engagement and disease control, not a single adherence score read on one day. [4]
Routine disposition follows a complete assessment with intact engagement, an agreed tailored plan, and a named next contact: brief reinforcement, scheduled re-measurement, and a planned interval. [5]
Early-review disposition is for new fatigue, rising but not crisis-level discordance, unstable housing or family conflict, or an incomplete assessment needing a return visit with trust built. [1] [9]
Urgent disposition is for the acute consequences — DKA, seizure cluster, sickle crisis, suspected rejection — and for sudden disengagement from a life-sustaining regimen. Emergency care, specialist involvement, and closed follow-up loops apply. [4] [10]
Disposition should always name the next contact and a low-threshold way back in. Engagement across adolescence into young-adult transition is itself the outcome: the young person who returns after a lapse is the success case, not the failure. [1] [10]
Special Populations
Gender-diverse and sexual-minority youth. Minority stress compounds the identity load of a chronic regimen; affirm identity, watch for bullying and family rejection, and tailor the conversation to how the medicine sits with the young person's sense of self. [1] [9]
Indigenous young people. Cultural safety, connection to community, and racism as a health exposure matter as much as any scale; partner with local services and avoid a surveillance stance that recalls historic harm. [1]
Migrant and refugee youth. Use a professional interpreter for the adherence conversation — family interpreters are not equivalent — and pace the work with trauma-informed care. [5]
Neurodiverse and disabled young people. Executive function, sensory load and formulation drive implementation; offer easy-read materials, longer slots, and scaffolded routines rather than assuming motivation is the problem. [5] [14]
Socioeconomic disadvantage and out-of-home care. Ask about food, transport, money, device charging and a stable place to store medicine before attributing non-adherence to character; options must be reachable and affordable, and continuity of prescriber is often the single biggest lever. [1] [5]
Youth-justice and child-protection settings. Confidentiality, supervision and continuity of medication are structurally constrained; reconstruct the history actively, clarify consent, and build a bridge to ongoing care on release or placement change. [1]
Evidence, Guidelines & Regional Differences
Rates, outcomes and predictors. Systematic review evidence in adolescents and young adults with cancer, and parallel reviews across chronic disease, converge on suboptimal adherence in roughly half, with measurable harm to disease control, graft survival and psychological outcomes, and predictable predictors in regimen complexity, side-effects, psychiatric comorbidity, family functioning and transition support. [2] [4]
Barriers. The systematic review of self-reported barriers among chronically ill adolescents found a consistent cluster of forgetfulness, regimen complexity, side-effects, lack of perceived necessity, and psychosocial and family factors — the same domains this topic organises assessment around. [1]
Interventions. The meta-analysis of psychological interventions to promote adherence in paediatric chronic conditions found a small but reliable benefit, strongest for behavioural and family-based approaches; motivational interviewing has separate meta-analytic support for improving medication adherence. [3] [13]
Measurement. Multi-method assessment — self-report, refill records and objective measures together — is the evidence-based standard, because each method captures a different facet and each misleads alone. Patient-reported outcome instruments function as conversation triggers rather than surveillance. [7] [14]
Condition-specific evidence. Sickle cell disease adherence, cystic fibrosis multi-method assessment, IBD barriers and their interaction with anxiety and depression, transplant transition readiness, asthma parent beliefs, and epilepsy barriers across the age span each reinforce the same cross-cutting message: the barrier pattern is condition-specific, the engagement-first stance is universal. [6] [7] [8] [9] [10] [11] [12]
ANZ: RCH clinical guidelines and youth-friendly confidential-care culture; local capacity and consent statutes govern a mature-minor assessment; strong transition frameworks but variable rural access and device-charging realities. UK: NICE medicines adherence guidance (CG76) centres shared decision-making and patient involvement; apply Gillick/Fraser capacity concepts with current local legal teaching; local safeguarding duties apply. US: AAP transition-in-the-medical-home policy; strong device-download infrastructure but portal-confidentiality tensions with open notes; variable insurance and cost barriers shape which regimens are reachable. Canada: CPS-aligned chronic-disease and transition guidance; provincial consent variation; strong transition infrastructure in many regions but rural and remote access gaps persist.
Exam Pearls
- Open every adherence answer with a non-judgemental, normalising frame and time alone before any adherence question. [1] [13]
- Define adherence in one line: the extent to which behaviour matches the agreed plan — agreed, not imposed. [1]
- Name the three phases — initiation, implementation, persistence — because lapses in each look different and need different conversations. [4]
- Match the measure to the setting: self-report opens the conversation; objective data (drug level, device download, refill) triangulate it. [7] [14]
- Probe the darkest barrier domain first (regimen burden, side-effects, beliefs, transition, system) rather than blaming the patient. [8]
- Cite the dual-systems model to justify why future benefit loses to present cost in adolescence. [1] [9]
- Treat the transition cliff as a predictable, preventable high-risk period for graft loss, DKA and disengagement. [10]
- Reframe "non-compliant" as "struggling with adherence" — language shapes disclosure. [1]
- State that local capacity and consent rules are jurisdiction-specific — assess capacity and support the mature minor without inventing universal consent ages. [5]
- Remember ADHERE: Assess without blame, Determine barriers across domains, Help with shared goals, Ease the regimen, Reminders and technology, Exit red flags to acute care. [5] [13]
ADHERE — the adherence-promotion sequence
References
- [1]Hanghøj S, Boisen KA Self-reported barriers to medication adherence among chronically ill adolescents: a systematic review. Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2014.PMID 24182940
- [2]McGrady ME, Pai ALH A Systematic Review of Rates, Outcomes, and Predictors of Medication Non-Adherence Among Adolescents and Young Adults with Cancer. Journal of adolescent and young adult oncology, 2019.PMID 31038372
- [3]Kahana S, Drotar D, Frazier T Meta-analysis of psychological interventions to promote adherence to treatment in pediatric chronic health conditions. Journal of pediatric psychology, 2008.PMID 18192300
- [4]Pai AL, Drotar D Treatment adherence impact: the systematic assessment and quantification of the impact of treatment adherence on pediatric medical and psychological outcomes. Journal of pediatric psychology, 2010.PMID 19710252
- [5]Drotar D Strategies of adherence promotion in the management of pediatric chronic conditions. Journal of developmental and behavioral pediatrics : JDBP, 2013.PMID 24247913
- [6]Loiselle K, Lee JL, Szulczewski L, Drake S, Crosby LE, Pai AL Systematic and Meta-Analytic Review: Medication Adherence Among Pediatric Patients With Sickle Cell Disease. Journal of pediatric psychology, 2016.PMID 26384715
- [7]Modi AC, Lim CS, Yu N, Geller D, Wagner MH, Quittner AL A multi-method assessment of treatment adherence for children with cystic fibrosis. Journal of cystic fibrosis : official journal of the European Cystic Fibrosis Society, 2006.PMID 16679071
- [8]Ingerski LM, Baldassano RN, Denson LA, Hommel KA Barriers to oral medication adherence for adolescents with inflammatory bowel disease. Journal of pediatric psychology, 2010.PMID 19776229
- [9]Gray WN, Denson LA, Baldassano RN, Hommel KA Treatment adherence in adolescents with inflammatory bowel disease: the collective impact of barriers to adherence and anxiety/depressive symptoms. Journal of pediatric psychology, 2012.PMID 22080456
- [10]Fredericks EM, Dore-Stites D, Well A, Magee JC, Freed GL, Shieck V Assessment of transition readiness skills and adherence in pediatric liver transplant recipients. Pediatric transplantation, 2010.PMID 20598086
- [11]Conn KM, Halterman JS, Lynch K, Cabana MD The impact of parents' medication beliefs on asthma management. Pediatrics, 2007.PMID 17766496
- [12]Gutierrez-Colina AM, Smith AW, Mara CA, Modi AC Adherence barriers in pediatric epilepsy: From toddlers to young adults. Epilepsy & behavior : E&B, 2018.PMID 29433948
- [13]Palacio A, Garay D, Langer B, Taylor J, Wood BA, Tamariz L Motivational Interviewing Improves Medication Adherence: a Systematic Review and Meta-analysis. Journal of general internal medicine, 2016.PMID 27160414
- [14]Plevinsky JM, Gutierrez-Colina AM, Carmody JK, Hommel KA, Crosby LE, McGrady ME Patient-Reported Outcomes for Pediatric Adherence and Self-Management: A Systematic Review. Journal of pediatric psychology, 2020.PMID 31845997