Paeds · adolescent-and-young-adult-medicine
Menstrual disorders in adolescents
Also known as Abnormal uterine bleeding in adolescents · Adolescent menstrual problems · Heavy menstrual bleeding in adolescents · Dysmenorrhoea in adolescents · Amenorrhoea in adolescents · Adolescent gynaecology
A fellowship approach to menstrual disorders in adolescents: what is normal after menarche, how to classify abnormal uterine bleeding (PALM-COEIN), the work-up for heavy bleeding, dysmenorrhoea and amenorrhoea, stepwise management with combined hormonal contraception, the levonorgestrel intrauterine system, tranexamic acid and iron, and red flags across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 14-year-old presents with “heavy periods” since menarche a year ago. Her mother says everyone in the family has them. The registrar notes she looks pale and prescribes iron. Eighteen months later she is admitted overnight with a haemoglobin in the 60s and a von Willebrand panel no one ever sent. The miss was not a rare syndrome. It was treating bleeding as an annoyance rather than as a vital sign. [1] [5]
Menstrual disorders in adolescents are any departure from the normal cycle range, volume, timing or associated symptoms that warrants assessment or treatment. The umbrella covers three symptom clusters that overlap in real life: abnormal uterine bleeding (too heavy, too long, too frequent, too infrequent, or absent), dysmenorrhoea (painful menses, primary or secondary), and amenorrhoea (primary or secondary). ACOG framed the cycle as a vital sign precisely so that clinicians would not wave away irregular, heavy or absent menses as “just being a teenager.” [1] [9]
The exam skill is to recognise what is normal for the developmental stage, name the abnormal pattern in objective FIGO terms, and pursue the mechanism rather than the label. An adolescent whose cycles are 40 to 90 days apart two years after menarche is not “stressed.” She has ovulatory dysfunction that needs a cause. [1] [4]
Classification
Begin with the person in front of you, then sort the problem along two axes: what is the pattern of bleeding, and what is the structural or medical cause. [3] [9]
What is a normal adolescent cycle?
After menarche the cycle is allowed to be irregular while the hypothalamic–pituitary–ovarian axis matures. ACOG gives the operational thresholds examiners expect you to recite. [1]
If cycles fall outside these ranges, or stay irregular beyond three years post-menarche, or become heavier, more painful or absent, classify the abnormal pattern before chasing a diagnosis. [1] [9]
FIGO objective descriptions of bleeding
Drop the vague words. FIGO asks you to describe bleeding by frequency, regularity, duration and volume so the next clinician knows exactly what you saw. [4]
| Term | Definition |
|---|---|
| Heavy menstrual bleeding (HMB) | Increased volume interfering with quality of life |
| Prolonged bleeding | Duration over 7–10 days |
| Frequent | Cycle less than 21 days |
| Infrequent | Cycle more than 45 days (adolescent oligomenorrhoea threshold commonly used) (over 90 days needs work-up) |
| Irregular | Variation more than 7 to 9 days between cycles |
| Absent (amenorrhoea) | No bleeding — primary or secondary |
PALM-COEIN — the cause framework
Once the pattern is named, attach a cause using FIGO's two-tier system, which separates what you can see structurally from what is medical. [3] [4]
PALM (structural)
Seen on imaging, hysteroscopy or histology
- Polyp
- Adenomyosis
- Leiomyoma
- Malignancy / hyperplasia — uncommon in early adolescence
COEIN (non-structural)
Most adolescent bleeding lives here
- Coagulopathy (von Willebrand disease)
- Ovulatory dysfunction (immaturity, PCOS, thyroid)
- Endometrial (primary disorder of endometrial haemostasis)
- Iatrogenic (hormonal, anticoagulants)
- Not yet classified
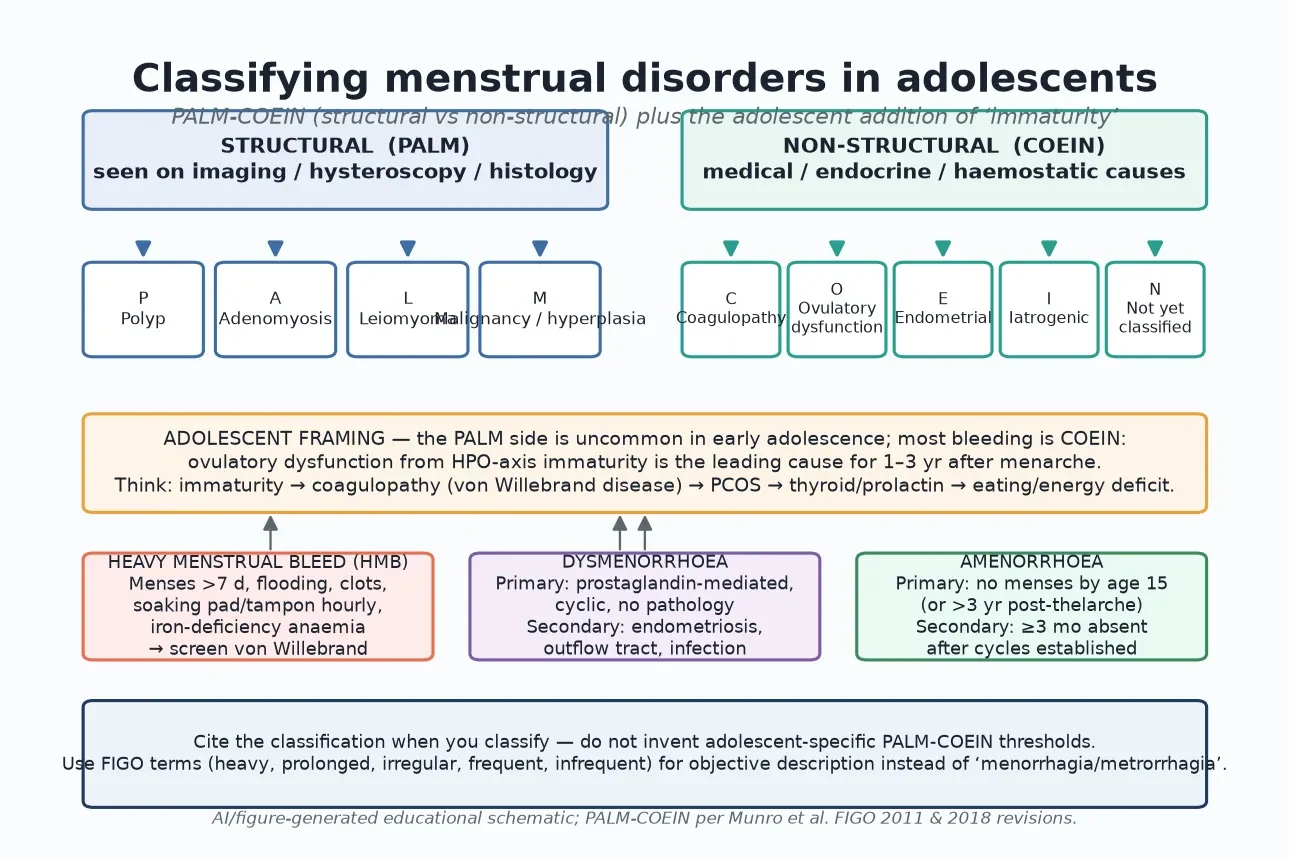
Read the figure like this: the structural side is uncommon in early adolescence, so a young adolescent with heavy bleeding has coagulopathy or ovulatory dysfunction until shown otherwise — not a fibroid. [5] [6]
Epidemiology & Risk Factors
Menstrual complaints are among the most common reasons an adolescent sees a doctor, and they are under-recognised. [12]
A systematic review of adolescents found heavy menstrual bleeding and dysmenorrhoea to be highly prevalent, with substantial impact on school attendance, sport and quality of life, and a persistent unmet need for both effective treatment and respectful education. [12]
Heavy menstrual bleeding affects a meaningful minority of adolescents, and among those referred for evaluation roughly one in five has an underlying bleeding disorder — von Willebrand disease is the single most common. [5] [6] Dysmenorrhoea is the most frequent gynaecological complaint of adolescence, yet many young people never receive effective treatment. [7] [8]
Risk amplifiers for an organic or serious cause: bleeding or bruising history (epistaxis, gum bleeding, family history of bleeding disorder); heavy bleeding from the very first period; cycles that remain erratic beyond three years post-menarche; severe dysmenorrhoea refractory to NSAIDs and hormonal therapy; low body weight, restriction, over-exercise or eating disorder; features of hyperandrogenism (hirsutism, acne, central adiposity); thyroid symptoms;recent pregnancy or sexual coercion; and chronic disease or medication affecting haemostasis or the HPO axis. [5] [6] [10] [9]
Pathophysiology
You do not need a reproductive endocrinology lecture to manage an adolescent. You need a working model of how a normal cycle is built and where the common adolescent breaks happen. [11]
How a normal cycle is built
The cycle runs as a chain with feedback. The hypothalamus releases gonadotropin-releasing hormone in pulses, the pituitary responds with follicle-stimulating hormone and luteinising hormone, the ovary produces oestradiol and progesterone, and the endometrium proliferates then sheds if no pregnancy occurs. Each level feeds back on the one above it. A regular cycle is proof that this chain is intact, well-nourished and unblocked by thyroid, prolactin or cortisol disturbance. [1] [11]
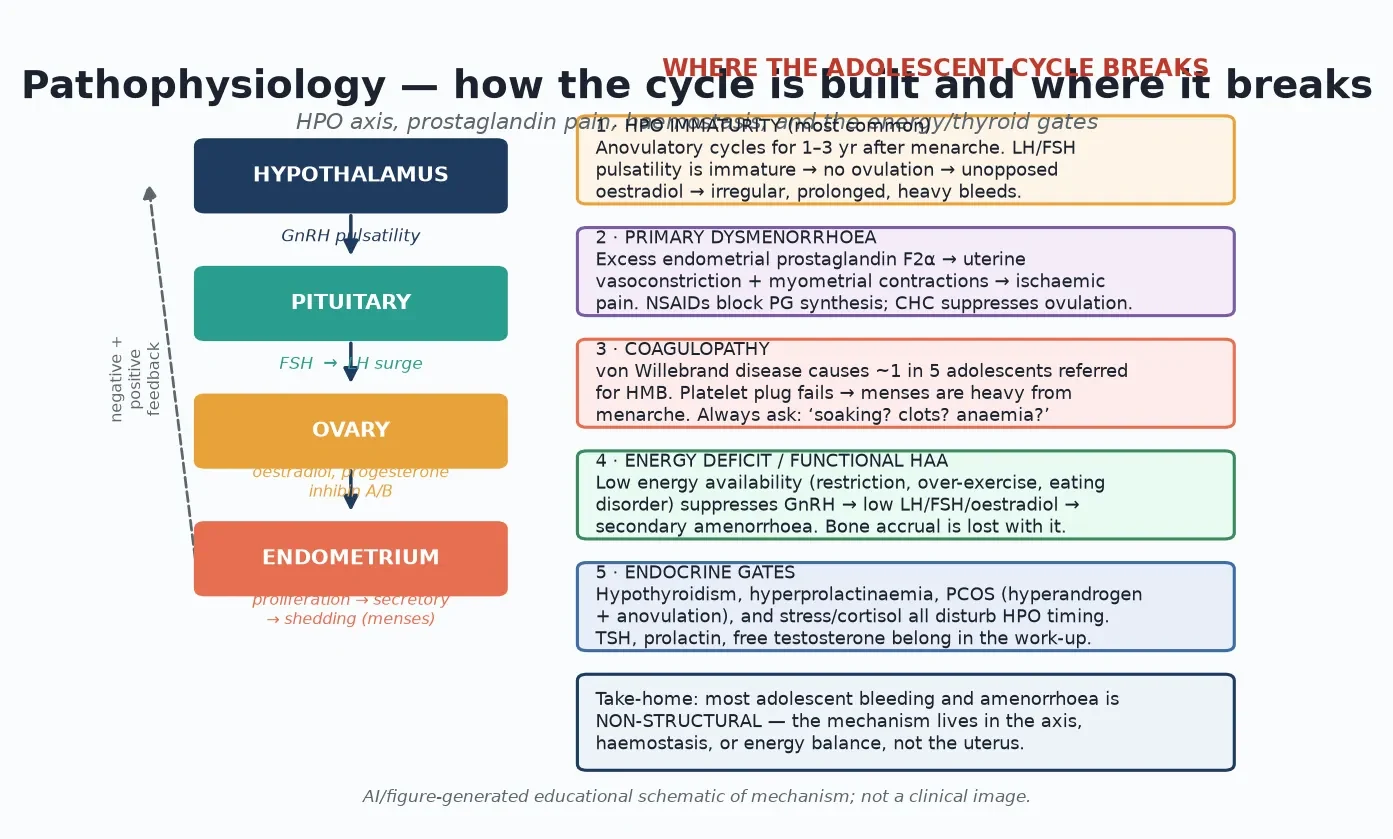
Read the figure like this: most adolescent menstrual disorders are non-structural. The mechanism lives in the axis, the prostaglandins, the clotting, or the energy balance — not usually the uterus. [3] [9]
The five adolescent breaks
HPO-axis immaturity is the leading cause of irregular and heavy bleeding for one to three years after menarche. The pulsatility of luteinising hormone is not yet mature, so ovulation does not happen reliably. Without the progesterone of a corpus luteum, the endometrium sees unopposed oestradiol, builds up, and sheds unpredictably and heavily. [11] [1]
Primary dysmenorrhoea is pain caused by excess endometrial prostaglandin F2α. The prostaglandin drives myometrial contractions and vasoconstriction, producing ischaemic pain that typically begins just before or with the bleed and is worst on the first one to two days. NSAIDs work because they block prostaglandin synthesis; combined hormonal contraception works because it suppresses ovulation and thins the endometrium. [7] [8]
Coagulopathy matters because von Willebrand disease is common among adolescents referred for heavy bleeding. Platelet plug formation fails, so the bleeding is heavy from the very first period and tends to come with other bleeding history. [5] [6]
Energy deficit and the functional hypothalamic amenorrhoea spectrum suppress gonadotropin-releasing hormone when energy availability is too low — from restriction, over-exercise, or an eating disorder. Luteinising hormone, follicle-stimulating hormone and oestradiol fall, ovulation stops, and bone accrual is lost with it. [9] [10]
Endocrine gates — hypothyroidism, hyperprolactinaemia, and polycystic ovary syndrome — disturb the timing of the axis. PCOS in adolescence is an ovulatory disorder with hyperandrogenism; read its criteria carefully and do not over-diagnose on a single blood test. [10] [9]
Clinical Presentation
Most adolescents with a menstrual disorder do not arrive with a FIGO descriptor. They arrive with the impact the cycle is having on their life, and your job is to translate that into a pattern and then a mechanism. [1] [9]
Heavy menstrual bleeding presents as flooding, clots, soaking a pad or tampon every one to two hours for several hours, or bleeding lasting longer than seven to ten days. Often the adolescent has normalised it; the giveaway is pallor, fatigue, breathlessness on exertion, or missed school. Ask directly about bleeding from the very first period and about bruising, epistaxis and family history. [5] [6]
Irregular or infrequent bleeding presents as unpredictable cycles, prolonged intervals of forty to ninety days or more, or bleeding that comes and goes without a pattern. For the first one to three years after menarche this is usually HPO immaturity; beyond that, suspect PCOS, thyroid, prolactin, or an energy-deficit state. [11] [10]
Dysmenorrhoea presents as cramping lower abdominal and back pain beginning just before or with the bleed and peaking on the first one to two days, often with nausea, diarrhoea or fatigue. Primary dysmenorrhoea fits this pattern and responds to NSAIDs. Pain that is non-cyclic, deep, breaks through hormonal therapy, or causes school absence despite adequate treatment points to a secondary cause such as endometriosis or an outflow obstruction. [2] [7]
Amenorrhoea presents either as no menses by age fifteen (or within three years of thelarche) — primary — or as three or more missed cycles after regular menses were established — secondary. Pregnancy is the first thought in secondary amenorrhoea, always. [1] [9]
Differential Diagnosis
In this topic the differential is the list of mechanisms above, applied to the pattern the adolescent brings. The table pairs the common presentation with the distinguishing features and the thing you must not miss. [9] [5]
| Presentation | Distinguishing features | Do not miss |
|---|---|---|
| Irregular, infrequent bleeding | HPO immaturity, PCOS, thyroid, prolactin, energy deficit | Pregnancy; PCOS over-diagnosis on one test |
| Heavy bleeding from menarche | von Willebrand disease, platelet disorder, anticoagulant | Coagulopathy; symptomatic anaemia |
| Severe dysmenorrhoea, NSAID-resistant | Endometriosis, outflow obstruction (imperforate hymen, vaginal septum), pelvic infection | Structural obstruction; endometriosis |
| Secondary amenorrhoea | Pregnancy, functional hypothalamic, PCOS, thyroid, prolactin, premature ovarian insufficiency | Pregnancy (always); eating disorder |
| Mid-cycle / postcoital bleeding | Cervical or vaginal cause, infection, retained foreign body, (rarely) malignancy | STI, foreign body, coercion |
| Sudden heavy bleed, unwell | Pregnancy complication, bleeding disorder flare, iatrogenic | Haemodynamic instability; ectopic |
Clinical & Bedside Assessment
1. Confidential adolescent frame first
Greet the young person, set a joint agenda, then create time alone. State conditional confidentiality — what stays private, and the limits of serious harm, abuse and legal duties. The sexual and bleeding history that drives this work is impossible with a parent answering. [1] [9]
2. Menstrual history with objective terms
Ask for cycle length, days of bleeding, number of pads or tampons per day, flooding, clots, and days missed from school or sport. Use the FIGO descriptors: frequency, regularity, duration, volume. Ask whether the bleeding has been heavy from the very first period — that points to coagulopathy. [1] [4]
Practical volume prompts: soaking a pad or tampon every one to two hours for several hours, passing clots larger than a grape, bleeding lasting longer than seven to ten days, and any anaemia symptoms (fatigue, breathlessness, dizziness). These mark heavy menstrual bleeding. [5]
3. Pain history
For dysmenorrhoea, establish the timing (just before and first one to two days of menses is typical of primary), the response to NSAIDs and heat, and any non-cyclic pelvic pain, deep dyspareunia, or pain that breaks through hormonal therapy — those shift you toward a secondary cause. [2] [7]
4. Bleeding, systemic and psychosocial screen
Ask about other bleeding (epistaxis, gum bleeding, easy bruising, family history), thyroid symptoms, galactorrhoea, androgen symptoms, weight and exercise, eating patterns, sleep, mood, sexual activity, contraception, and coercion. A full HEADSS-style sweep belongs here because menstrual disorders often surface alongside mental health, eating and safety concerns. [5] [9]
5. Examination matched to the question
Measure height, weight, body mass index, blood pressure, and puberty (Tanner) stage. Examine for acne, hirsutism, acanthosis nigricans, and thyroid. Inspect the external genitalia when there is pain, obstruction or foreign body suspicion; a speculum or bimanual pelvic exam is rarely needed in a young adolescent and should be performed only when indicated, with consent and a chaperone, by an experienced clinician. [9] [2]
Investigations
Most stable adolescents need a focused, mechanism-led panel — not a blanket work-up. [9] [5]
Core panel for abnormal bleeding
A pregnancy test, full blood count, and ferritin cover the essentials in nearly every adolescent with abnormal bleeding: exclude pregnancy, quantify anaemia, and reveal iron deficiency. [1] [5]
Add thyroid-stimulating hormone, prolactin, and free or total testosterone when cycles are irregular or infrequent, when there are androgen features, or when bleeding persists. These catch the endocrine gates. [9] [10]
Add a coagulation screen and a von Willebrand panel (von Willebrand factor antigen, activity or ristocetin cofactor, and factor VIII) when bleeding has been heavy from menarche or there is a bleeding history. About one in five adolescents referred for heavy menstrual bleeding has an underlying bleeding disorder. [5] [6]
Selective imaging and specialist tests
Reserve pelvic ultrasound for suspected structural cause — obstruction, mass, persistent concern after normal labs — and interpret adolescent pelvic ultrasound with the help of someone who reads paediatric and adolescent scans. Polycystic ovarian morphology on ultrasound is not diagnostic of PCOS in early adolescence. [9] [10]
Karyotype, pelvic MRI, or serum follicle-stimulating hormone and oestradiol are reserved for amenorrhoea work-up when primary, when müllerian or chromosomal anomaly is suspected, or when premature ovarian insufficiency is on the differential. [9]
In Australia and Aotearoa New Zealand, the RCH Melbourne clinical guidelines and local adolescent-gynaecology pathways shape the work-up; reference local laboratory reference ranges and adolescent-specific von Willebrand interpretation, because levels vary with blood group and age. [9] [5]
Low-value patterns to avoid
Do not order a universal von Willebrand panel on every well adolescent; do not diagnose PCOS on a single androgen level in early adolescence; do not image every irregular cycle; and do not treat a number without treating the person. [9] [10]
Management — Resuscitation
A menstrual visit can turn into an emergency when bleeding is torrential or anaemia is severe. Stabilise before you classify. [5]
- Assess and resuscitate: airway, breathing, circulation; intravenous access; fluid resuscitation if shocked. [5]
- Investigate in parallel: full blood count, blood group and hold, coagulation, von Willebrand panel, ferritin, and a pregnancy test. [5] [6]
- Stop the bleeding: intravenous tranexamic acid is first-line medical haemostasis for acute heavy bleeding; high-dose oral or intravenous oestrogen is used for acute severe bleeding that does not settle, with dosing per your local adolescent-gynaecology or haematology protocol. [5]
- Transfuse for instability or symptomatic severe anaemia, not for a number alone. [5]
- Admit if bleeding is uncontrolled, haemodynamics are unstable, or the diagnosis and disposition need inpatient coordination. [5]
Document the volume of bleeding, the interventions and their timing, who was informed, and the disposition. Override confidentiality only where safety thresholds require it, and tell the young person what you must share. [5] [1]
Management — Definitive & Stepwise
Once stable, treat by mechanism and build a plan the adolescent can own. [9] [5]
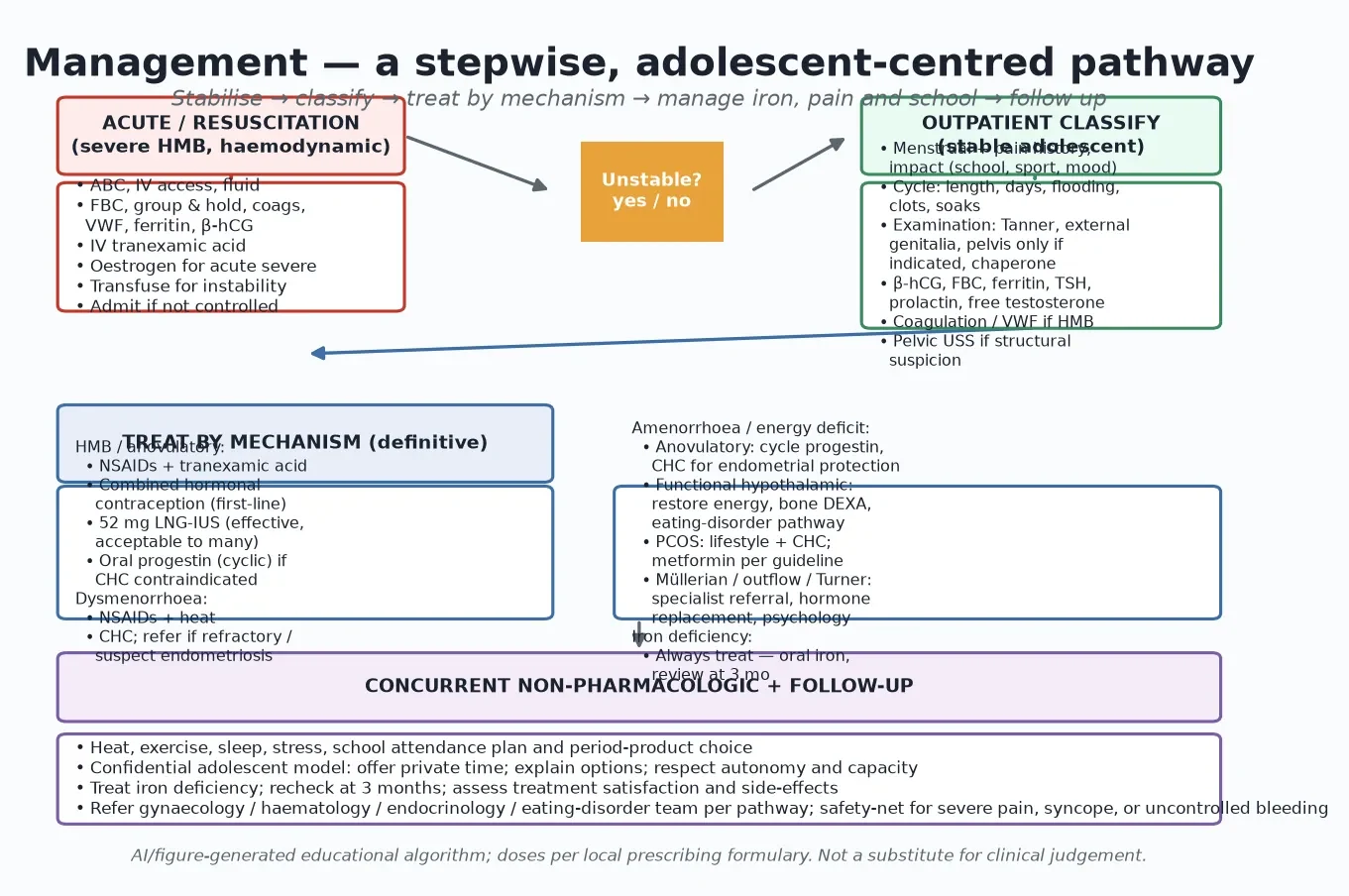
Read the figure like this: the unstable branch exits the routine path immediately. For everyone else, classification drives a mechanism-based ladder, and iron, school and confidentiality are not optional add-ons. [5] [9]
Heavy menstrual bleeding and anovulatory bleeding
Treat heavy bleeding with a layered, mechanism-based approach. [5] [6]
- Combined hormonal contraception (combined oral contraceptive pill, patch, or ring) is first-line for cycle control in adolescents without contraindication. It suppresses ovulation, regularises withdrawal bleeds, and reduces volume; product and dosing follow the local adolescent-gynaecology protocol. [5]
- The 52 mg levonorgestrel intrauterine system is effective for heavy menstrual bleeding in adolescents, including those with inherited bleeding disorders, and is acceptable to many; it also provides contraception. [5]
- Tranexamic acid, taken during menses, reduces menstrual loss by inhibiting plasminogen activation; use it when hormonal methods are declined or contraindicated, with dosing per formulary. [5] [6]
- Cyclic oral progestin (for example norethisterone or medroxyprogesterone for a set number of days each cycle) protects the endometrium and induces withdrawal bleeds when combined hormonal contraception is contraindicated. [9]
- Always treat iron deficiency — oral iron with recheck at around three months, and address the underlying cause. [5]
Dysmenorrhoea
First-line for primary dysmenorrhoea is an NSAID (for example ibuprofen or naproxen at age-appropriate dosing started at the onset of menses) plus heat and, where appropriate, combined hormonal contraception. [7] [8] If pain is refractory to adequate NSAID trials and hormonal therapy, suspect a secondary cause — endometriosis, outflow obstruction, or pelvic infection — and refer. [2]
Endometriosis in adolescents is real and under-diagnosed; laparoscopic diagnosis and excision belong to the specialist, but the recognition and the referral are yours. [2]
Amenorrhoea
Manage by cause. Exclude pregnancy first in any secondary amenorrhoea. [1] [9]
- Anovulatory or PCOS-related: cycle the endometrium with cyclic progestin or combined hormonal contraception to prevent unopposed oestrogen and reduce long-term endometrial risk; address lifestyle, weight, and hyperandrogenism per PCOS pathways. [10] [9]
- Functional hypothalamic / energy deficit: the treatment is restoration of energy balance, not hormones alone — involve the eating-disorder team, monitor weight and bone density, and only then consider hormone replacement for bone protection. [9]
- Müllerian, outflow, or Turner syndrome: refer to adolescent gynaecology and endocrinology; hormone replacement, surgery for obstruction, and psychological support are coordinated by specialists. [9]
Tranexamic acid (oral)
Antifibrinolytic for heavy menstrual bleeding
Dose
Age- and weight-appropriate dosing, during menses only (local formulary)
Concurrent, non-pharmacologic care
Heat, regular exercise, adequate sleep and stress reduction all help dysmenorrhoea and quality of life. [7] [12] Address period-product choice, school attendance, and sport participation explicitly. Run the visit as confidential adolescent care: explain the options, respect autonomy and capacity, and document sensitively so portals and billing do not leak content. [1]
Specific Subtypes & Scenarios
Early-adolescent irregular cycles. Cycles 21 to 45 days apart for the first one to three years are usually HPO immaturity. Reassure, give anticipatory guidance, treat heavy bleeding, and re-evaluate if irregularity persists beyond three years. [11] [1]
Heavy bleeding from menarche with bruising. Send a von Willebrand panel and coagulation screen; involve haematology early. Do not settle for “runs in the family.” [5] [6]
Severe dysmenorrhoea refractory to NSAIDs and combined hormonal contraception. Suspect endometriosis or outflow obstruction; inspect the external genitalia and refer to adolescent gynaecology. [2]
Functional hypothalamic amenorrhoea / eating disorder. This is medical instability risk, not a contraception issue. Restore energy, involve the eating-disorder team, monitor bone density, and safety-net for electrolyte and refeeding concerns. [9]
PCOS suspicion. Use accepted adolescent criteria — ovulatory dysfunction plus clinical or biochemical hyperandrogenism, with other causes excluded — and avoid over-diagnosis on a single test or ultrasound morphology. [10]
Sexually active adolescent with abnormal bleeding. Confidential pregnancy test, sexual health screen matched to practices, contraception, and explicit assessment of coercion. [1] [9]
Disability and neurodiversity. Accessible communication, longer slots, sensory adjustment, capacity assessment, and a chaperoned, consent-led sensitive exam. Carers help, but private time may still be possible. [9]
Transgender and gender-diverse young people on testosterone. Testosterone may reduce but does not reliably stop menses; the underlying menstrual disorder still needs confidential, affirming management. [9]
Complications & Pitfalls
- Treating heavy bleeding as “normal for teenagers” and missing von Willebrand disease. [5] [6]
- Reassuring irregular cycles without a three-year review point. [1] [11]
- Diagnosing PCOS on a single androgen level or on ultrasound morphology in early adolescence. [10]
- Treating functional hypothalamic amenorrhoea with hormones alone instead of restoring energy. [9]
- Dismissing dysmenorrhoea as “part of being a woman” and missing endometriosis. [2] [7]
- Forgetting a pregnancy test in any adolescent with abnormal bleeding or amenorrhoea. [1]
- Failing to treat iron deficiency alongside the bleeding. [5]
- Taking the full sensitive history with a parent present. [1]
- Over-investigating the well adolescent with mild cycle variation. [9]
- Letting portals or billing disclose confidential adolescent content. [1]
Prognosis & Disposition
Most adolescent menstrual disorders improve with mechanism-based treatment and mature into regular cycles as the HPO axis stabilises. [11] [1]
Routine disposition: stable adolescent, normal haemoglobin, bleeding controlled with medical therapy, clear follow-up and safety-net. Early review disposition: new treatment started, anaemia under treatment, eating-disorder or PCOS pathway opened — review within weeks to a few months. Urgent disposition: haemodynamic instability, severe anaemia, uncontrolled bleeding, suspected obstruction or endometriosis crisis, or safeguarding concern — admit or same-day specialist review. [5] [9]
Long-term outcomes that matter: resolution of anaemia, return to school and sport, satisfaction with the chosen method, preserved bone health in energy-deficit states, and reduced long-term endometrial risk in chronic anovulation. Reassess treatment at three months and at every method change. [5] [9]
Special Populations
Indigenous and migrant or refugee adolescents. Provide interpreter-supported, culturally safe care; reconstruct vaccination and gynaecology history; address trauma-informed pacing and confidential access. [9]
Socioeconomic disadvantage. Ask about cost of products, transport, and access to follow-up before blaming non-attendance; period poverty is a real driver of school absence and under-treatment. [12]
Gender and sexual diversity. Use chosen name and pronouns, tailor sexual health to anatomy and practices, and provide affirming care; testosterone does not guarantee amenorrhoea. [9]
Chronic disease and disability. Integrate disease-specific goals without dropping menstrual and sexual health; watch for diagnostic overshadowing of pain or bleeding. [9]
Athletes. Screen for relative energy deficiency in sport and functional hypothalamic amenorrhoea; do not equate thinness with health. [9]
Evidence, Guidelines & Regional Differences
ACOG Committee Opinion 651 established the menstrual cycle as a vital sign for girls and adolescents, giving the operational normal ranges that anchor adolescent assessment. [1] ACOG Committee Opinion 760 guides dysmenorrhea and endometriosis in the adolescent, including the recognition that refractory pain warrants specialist referral. [2]
The FIGO two-systems framework (Munro and colleagues, 2011 and 2018 revisions) separates structural PALM causes from non-structural COEIN causes and standardises the objective description of bleeding — frequency, regularity, duration and volume. [3] [4]
Heavy menstrual bleeding and bleeding disorders are addressed by the JAMA Pediatrics review of Borzutzky and Jaffray and by ACOG Committee Opinion 785, both of which make the case for routine von Willebrand screening in adolescents with heavy bleeding from menarche. [5] [6]
Primary dysmenorrhoea is synthesised by the Iacovides critical review and the SOGC consensus guideline of Burnett and Lemyre, covering prostaglandin mechanism and NSAID plus hormonal first-line therapy. [7] [8]
PCOS in adolescents is covered in the Joham Lancet primer; the take-home for adolescent practice is to use accepted adolescent criteria and avoid over-diagnosis on a single test. [10] The classic Mansfield and Emans paper frames adolescent menstrual irregularity as expected immaturity with defined limits. [11] A 2024 systematic review quantifies the burden and unmet need of heavy bleeding and dysmenorrhoea in adolescents. [12]
ANZ: RCH Melbourne clinical guidelines and local adolescent-gynaecology pathways; local laboratory adolescent reference ranges.
UK: NICE guidance on heavy menstrual bleeding (NG88) for adults, adapted for adolescent presentation; MRCPCH adolescent-health framing.
US: ACOG Committee Opinions 651, 760, and 785; Bright Futures adolescent preventive care.
Canada: SOGC primary dysmenorrhoea consensus guideline; provincial adolescent-gynaecology pathways.
Exam Pearls
- Recite the normal adolescent cycle: 21 to 45 days, fewer than eight days of flow, regular within three years of menarche, menarche by age 15. [1]
- Use FIGO objective terms (heavy, prolonged, frequent, infrequent, irregular, absent) — not “menorrhagia” or “metrorrhagia.” [4]
- PALM-COEIN names structural versus non-structural causes; most adolescent bleeding is non-structural (COEIN). [3]
- Heavy bleeding from menarche → screen for von Willebrand disease; about one in five referred adolescents has a bleeding disorder. [5] [6]
- Pregnancy test for any adolescent with abnormal bleeding or amenorrhoea, confidentially. [1]
- First-line dysmenorrhoea: NSAID plus heat, and combined hormonal contraception; refractory pain → refer, suspect endometriosis. [7] [2]
- Do not diagnose PCOS on a single androgen level or ultrasound morphology in early adolescence. [10]
- Functional hypothalamic amenorrhoea is treated by restoring energy, not hormones alone; protect bone. [9]
- Always treat iron deficiency alongside the bleeding. [5]
- Run every visit through confidential adolescent care; mind portals and billing. [1]
CLASSIFY an adolescent's bleeding
References
- [1]American College of Obstetricians and Gynecologists ACOG Committee Opinion No. 651: Menstruation in Girls and Adolescents: Using the Menstrual Cycle as a Vital Sign. Obstetrics and gynecology, 2015.PMID 26595586
- [2]American College of Obstetricians and Gynecologists ACOG Committee Opinion No. 760: Dysmenorrhea and Endometriosis in the Adolescent. Obstetrics and gynecology, 2018.PMID 30461694
- [3]Munro MG, Critchley HO, Fraser IS, FIGO Menstrual Disorders Working Group The FIGO classification of causes of abnormal uterine bleeding in the reproductive years. Fertility and sterility, 2011.PMID 21496802
- [4]Munro MG, Critchley HOD, Fraser IS, FIGO Menstrual Disorders Committee The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. International journal of gynaecology and obstetrics, 2018.PMID 30198563
- [5]Borzutzky C, Jaffray J Diagnosis and Management of Heavy Menstrual Bleeding and Bleeding Disorders in Adolescents. JAMA pediatrics, 2020.PMID 31886837
- [6]American College of Obstetricians and Gynecologists Screening and Management of Bleeding Disorders in Adolescents With Heavy Menstrual Bleeding: ACOG Committee Opinion, Number 785. Obstetrics and gynecology, 2019.PMID 31441825
- [7]Iacovides S, Avidon I, Baker FC What we know about primary dysmenorrhea today: a critical review. Human reproduction update, 2015.PMID 26346058
- [8]Burnett M, Lemyre M No. 345-Primary Dysmenorrhea Consensus Guideline. Journal of obstetrics and gynaecology Canada, 2017.PMID 28625286
- [9]Kabra R, Fisher M Abnormal uterine bleeding in adolescents. Current problems in pediatric and adolescent health care, 2022.PMID 35525787
- [10]Joham AE, Norman RJ, Stener-Victorin E, Legro RS, Franks S, Moran LJ Polycystic ovary syndrome. The lancet. Diabetes and endocrinology, 2022.PMID 35934017
- [11]Mansfield MJ, Emans SJ Adolescent menstrual irregularity. The Journal of reproductive medicine, 1984.PMID 6379175
- [12]Pouraliroudbaneh S, Marino J, Riggs E, Saber A, Jayasinghe Y, Peate M Heavy menstrual bleeding and dysmenorrhea in adolescents: A systematic review of self-management strategies, quality of life, and unmet needs. International journal of gynaecology and obstetrics, 2024.PMID 38654586