Paeds · adolescent-and-young-adult-medicine
Normal puberty and adolescent development
Also known as Normal puberty · Tanner staging · Pubertal development · Adolescent growth and development · Normal variants of puberty · Gonadarche and adrenarche
A fellowship approach to normal puberty and adolescent development: the reactivated HPG axis, Tanner staging of breast/genital and pubic hair development, the sex-specific sequence and timing of events, the coupled growth spurt and brain changes, the normal variants, the referral thresholds for abnormal timing, and counselling across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 13-year-old boy is brought in because he is "the smallest in the class" and "hasn't started." His father grew late and reached his adult height at 19. You measure testicular volumes of 3 mL, plot a height that is tracking along the third centile at a normal velocity, and order a bone age that reads two years behind his chronological age. The answer is not a disease. It is the single most common reason boys present with delayed puberty: constitutional delay of growth and puberty. The skill is recognising what is normal, explaining it well, and reserving referral for the few who are not. [4] [6]
Puberty is the biological transition from a prepubertal child to a reproductively mature young adult, driven by the reactivation of the hypothalamic–pituitary–gonadal (HPG) axis. Adolescence is the broader social and developmental phase that puberty sits inside — identity formation, increasing autonomy, peer orientation and the move toward adult roles. Puberty is measurable; adolescence is lived. A clinician who can stage puberty but cannot talk to a young person about what it means has only done half the job. [10] [11]
The clinical task has three layers. First, describe what you see: which Tanner stage, in what sequence, at what age, progressing at what tempo. Second, classify whether that pattern is normal, a normal variant, or outside the band. Third, act: reassure and monitor, or refer with the right urgency. Most young people you see will sit in the first two categories. The danger is not over-calling the common — it is missing the rare one who needs a brain scan. [3] [5]
The three clinical questions of any pubertal assessment
What stage?
Tanner B/G stage and PH stage separately; Prader orchidometer in boys; growth chart and velocity.
Is the timing normal?
Girls 8–13 yr onset, boys 9–14 yr; menarche 10–15 yr; within band = reassure or variant.
Does it need referral?
Outside the band, rapid progression, CNS or endocrine red flags, or psychosocial crisis → paediatric endocrine.
Classification
Puberty is classified along two axes at once: the biological stage (how far along the Tanner pathway the young person has travelled) and the timing relative to the population (early, on-time, or late). Confusing the two is a classic error — a girl at B3 who is nine years old is at a normal stage but her timing is early; a boy at G2 who is fifteen is at an early stage and his timing is late. [15]
Tanner stages
Marshall and Tanner defined the staging system still used worldwide, describing the orderly sequence of physical changes in girls (1969) and boys (1970). Each sex is staged on a five-point scale for the gonadal/genital development and separately for pubic hair. [1] [2]
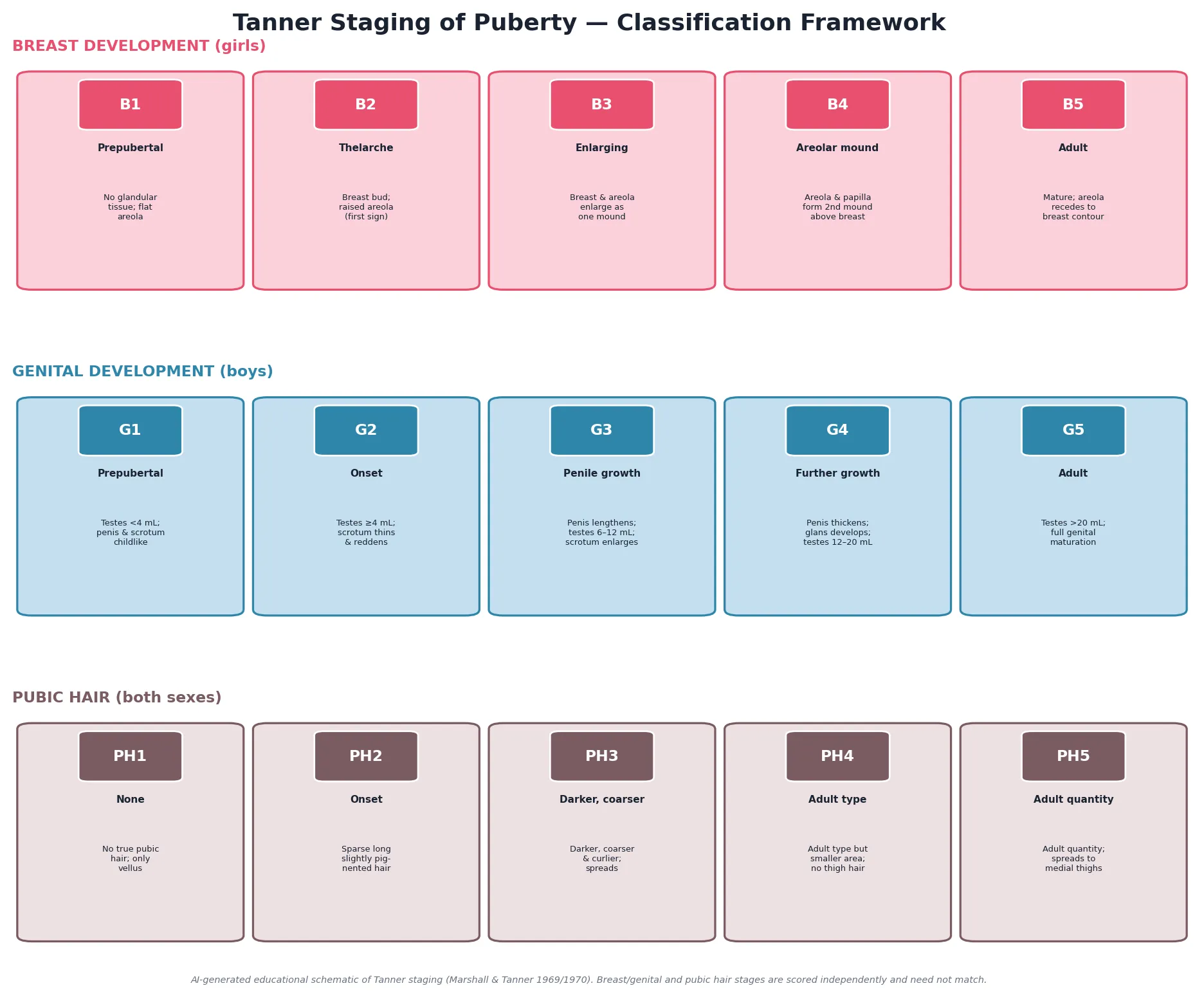
Read the figure like this: a young person at B3 but PH1 is perfectly normal — the breast is responding to estrogen while the adrenal has not yet switched on. The reverse, PH3 with B1, raises the question of an androgen source rather than true central puberty. [15]
Girls: breast (B)
Estrogen driven
- B1 prepubertal — no glandular tissue
- B2 thelarche — breast bud, first sign
- B3 enlarging mound
- B4 areolar secondary mound
- B5 mature adult contour
Boys: genital (G)
Gonadotropin driven
- G1 prepubertal — testes small, childlike
- G2 onset — testes enlarge, scrotal thinning and reddening
- G3 penile lengthening, testes further enlarge
- G4 penile thickening, glans develops
- G5 adult — full genital maturation
Both: pubic hair (PH)
Adrenal androgen driven
- PH1 none — vellus only
- PH2 sparse pigmented hair
- PH3 darker, coarser, curlier
- PH4 adult type, smaller area
- PH5 spreads to medial thighs
Timing classification
Timing is classified against population age bands, which themselves carry a caveat: the bands are statistical, not diagnostic. A girl at seven-and-a-half with isolated breast budding sits below the traditional threshold, but whether she needs a full workup depends on progression, bone age and context — not the number alone. [13] [15]
| Timing category | Girls | Boys | What it usually means |
|---|---|---|---|
| Precocious | Signs before 8 yr | Testicular growth before 9 yr | Refer for endocrine assessment |
| Early-normal | 8–9 yr | 9–10 yr | Often normal; watch tempo and bone age |
| On-time | 10–12 yr | 11–13 yr | Typical; reassure |
| Late-normal | 12–13 yr | 13–14 yr | Often constitutional delay; monitor |
| Delayed | No signs by 13 yr | No testicular growth by 14 yr | Refer; most boys have constitutional delay |
Normal variants
Three presentations are common, benign, and exist to stop you over-investigating. Premature thelarche is isolated breast budding, usually before age two or between two and six years, with prepubertal gonadotropins, no growth acceleration and no other signs. Premature adrenarche is isolated pubic or axillary hair before eight years with normal bone age and growth velocity. Constitutional delay of growth and puberty is the late bloomer — short for the family, delayed bone age that matches height age, and a normal growth velocity. Each is a diagnosis of a recognisable pattern, not a label of exclusion. [15] [6]
Epidemiology & Risk Factors
The normal age band for puberty onset is 8 to 13 years in girls and 9 to 14 years in boys, with the median age of thelarche around 10 years and of testicular enlargement around 11.5 years. Menarche typically occurs between 10 and 15 years, roughly two to two-and-a-half years after thelarche. These bands are wide because the timing of puberty is among the most variable of human traits. [13] [14]
Pubertal timing is strongly heritable: family history predicts it, and constitutional delay runs in families. Twin and family studies estimate heritability at roughly 50 to 80 per cent, meaning the largest single determinant of when a young person enters puberty is their genetic programme. Asking when parents and siblings went through puberty is not small talk — it is a diagnostic test. [4] [6]
A secular trend toward earlier puberty has been documented over decades, more strongly in girls than in boys. The age at thelarche and at menarche has fallen in many populations, linked at least in part to the rising prevalence of childhood obesity — body fat, signalled by leptin, is a permissive gate for pubertal onset. Environmental endocrine-disrupting chemicals have been proposed as an additional contributor, though the evidence quality is mixed and remains an active area of research. [13] [7] [17]
Body mass index is the modifiable factor most consistently associated with timing: higher childhood BMI correlates with earlier thelarche and earlier menarche in girls, mediated partly through leptin and insulin. The relationship is less clear-cut in boys, where the picture is more complex. Chronic under-nutrition, whether from poverty, eating disorder or inflammatory illness, delays puberty — the growth chart is the sentinel for this interaction. [16] [9]
Risk factors that shift a young person outside the typical band include low birthweight, chronic disease (inflammatory bowel disease, coeliac disease, cystic fibrosis, chronic kidney disease), intense energy-deficit athletics, and childhood adversity, which has been associated with earlier menarche. For a girl presenting at the early edge of normal, the question is not only "is this within the band?" but "what is driving it toward the early edge?" [13] [15]
Pathophysiology
To explain puberty to a family, hold one image in mind: a switch that has been off throughout childhood gets turned back on. During childhood the GnRH pulse generator is actively suppressed — the so-called childhood brake. At puberty, kisspeptin-producing neurons in the hypothalamus release that brake and the GnRH pulses resume, first at night, then increasingly through the day. [8] [9]
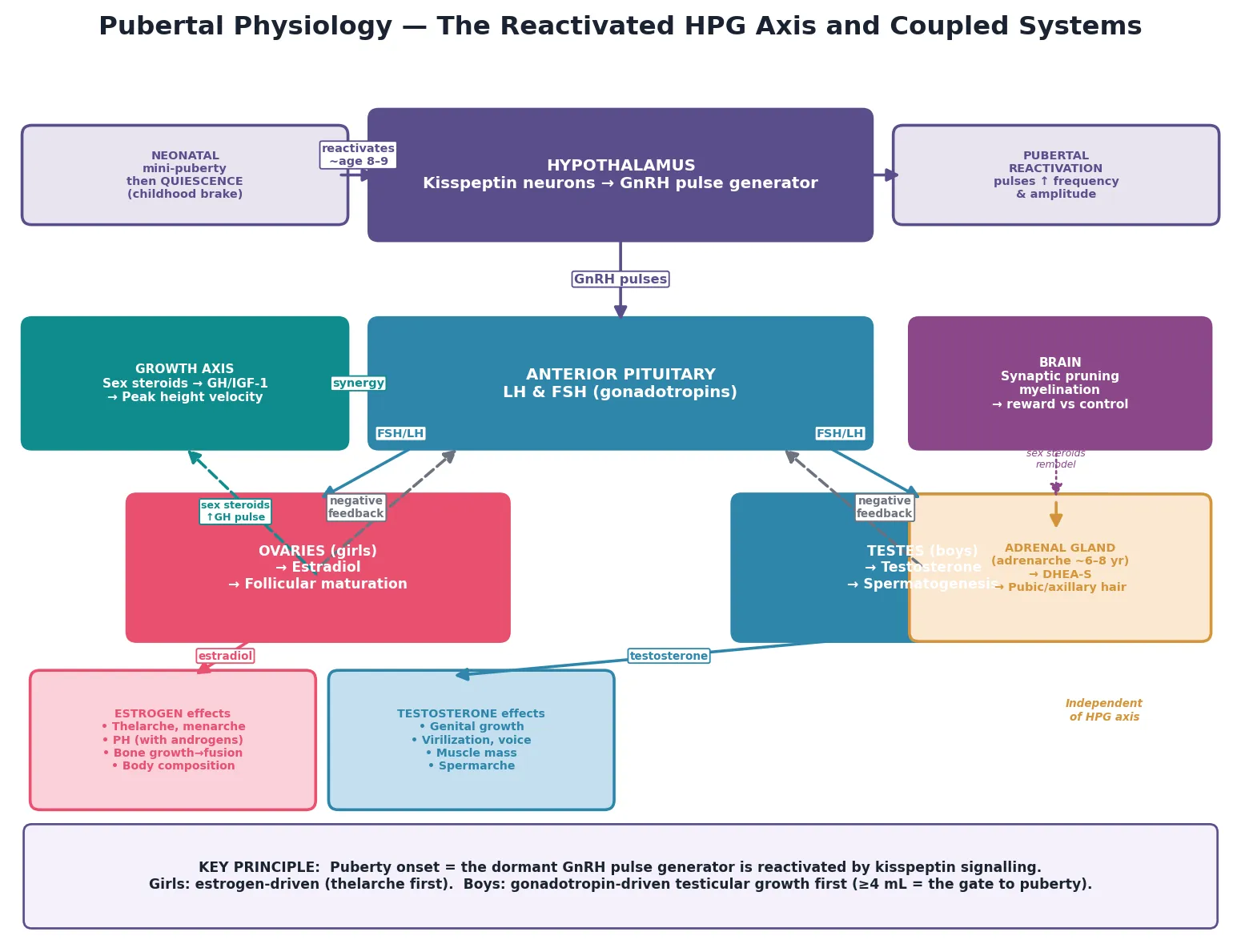
Read the figure like this: the dotted feedback arrow from the gonads back to the hypothalamus and pituitary is the loop that makes puberty self-sustaining once it starts. The adrenal box is drawn separately for a reason — it is not controlled by GnRH. [8]
The HPG axis has a developmental arc of its own. It is active in the fetus, briefly active again in the neonatal "mini-puberty" of the first months of life, then suppressed through childhood, and finally reactivated at puberty. This suppression is not a passive absence but an active restraint — which is why damage to the restraint mechanism (a hypothalamic hamartoma, for example) can release GnRH prematurely and cause central precocious puberty. [5] [8]
Kisspeptin and its receptor are now understood as the key upstream gatekeeper of GnRH neuron activity. The kisspeptin neurons of the arcuate nucleus (the KNDy population, named for their co-expression of kisspeptin, neurokinin B and dynorphin) generate the pulsatile signal that drives GnRH release. Energy balance signals — leptin from adipose tissue, insulin — modulate this pathway, which is why body fat and nutritional status influence when puberty begins. [8] [9]
Once GnRH pulses are established, they drive the pituitary to release luteinising hormone (LH) and follicle-stimulating hormone (FSH). In girls, FSH stimulates ovarian follicular development and LH drives ovarian estrogen production; the rising estrogen causes breast development, the growth spurt, and eventually menarche. In boys, LH drives the Leydig cells to produce testosterone and FSH drives the Sertoli cells and spermatogenesis; testicular enlargement is the first visible sign because the tubular growth under FSH precedes the androgen-dependent external changes. [1] [2] [14]
The growth spurt is not a separate event bolted onto puberty — it is generated by it. Sex steroids amplify growth hormone secretion and IGF-1 activity, producing the acceleration in height velocity that defines the adolescent growth spurt. Paradoxically, the same estrogen that drives the growth spurt also accelerates epiphyseal maturation and ultimately fuses the growth plates, ending growth. This is why a child who enters puberty early stops growing earlier, and why the timing of the growth spurt and of menarche are the strongest predictors of final adult height. [16]
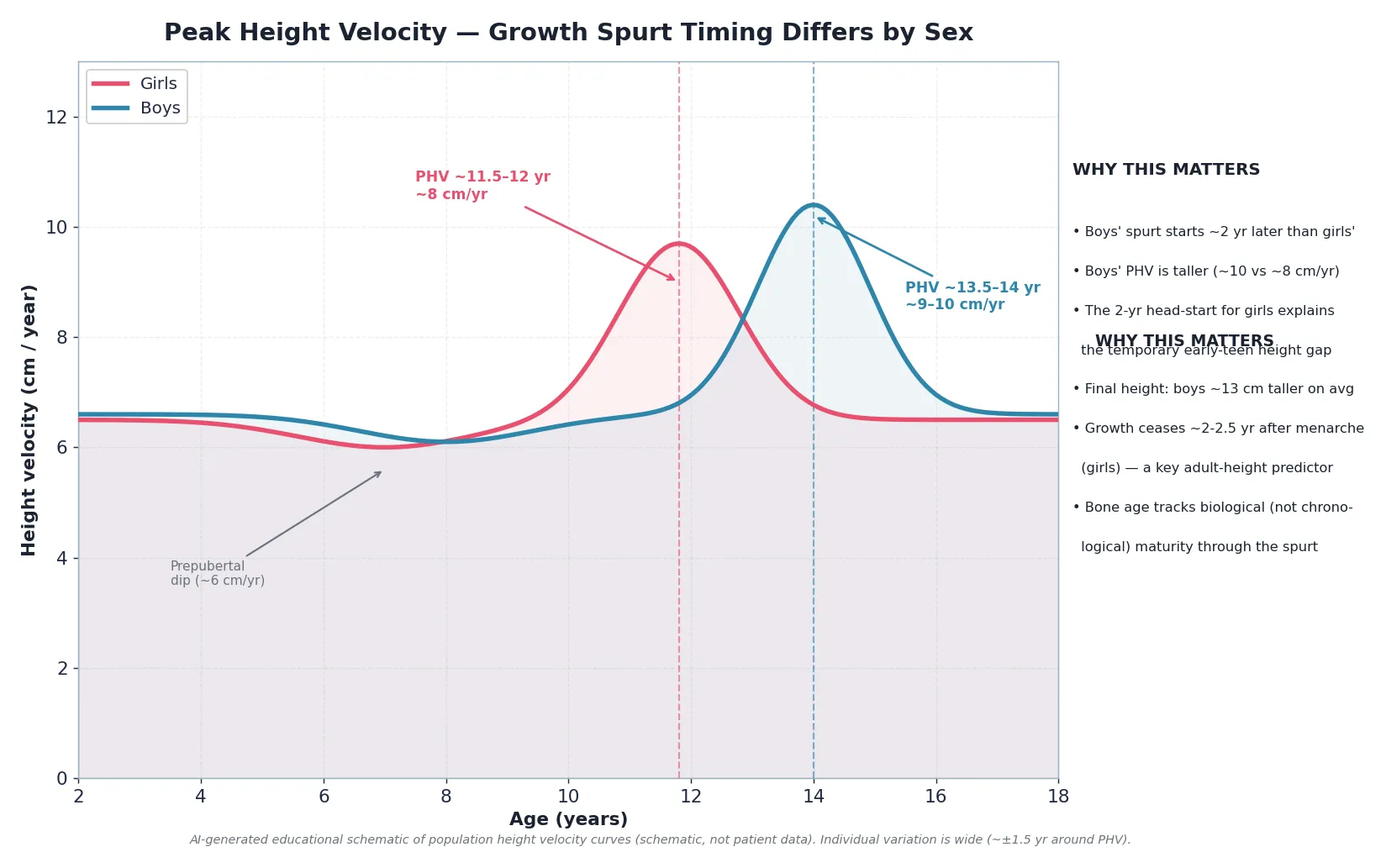
Read the figure like this: the area under each curve is roughly similar — boys grow for longer and at a faster peak, which is why their final height averages about 13 cm taller. A girl who has had menarche is near the end of her growth, not the beginning. [16]
The adolescent brain changes in parallel with the body. Synaptic pruning and myelination, especially in the prefrontal cortex and frontostriatal circuits, continue into the mid-twenties. Reward circuitry matures earlier than cognitive-control circuitry, creating a developmental window of heightened reward sensitivity alongside still-maturing impulse control. This is not a defect — it supports learning, social bonding and identity exploration — but it is the biology behind adolescent risk-taking, and it is part of why puberty is a developmental, not merely hormonal, event. [10] [11]
Clinical Presentation
A well-organised pubertal assessment looks calm and structured, but the important work is recognising that the young person in front of you is navigating the most visible biological transition of their life. Present your findings by sequence, stage and tempo. [15]
Girls
In girls the typical sequence is thelarche (breast budding, B2) first, followed over the next months to years by adrenarche-driven pubic hair (PH2), the acceleration of the growth spurt, and finally menarche. The interval from thelarche to menarche averages about two to two-and-a-half years. Body composition shifts toward a relative increase in fat mass, physiologic insulin resistance develops, and skin changes (sebum, acne, apocrine odour) appear in parallel with rising androgens. [1] [14]
Boys
In boys the sequence is testicular enlargement (the gonadotropin-driven tubular growth to at least 4 mL, G2) first, followed by scrotal thinning and reddening, pubic hair (PH2), penile growth (G3 to G4), the growth spurt, spermarche, voice deepening, and finally facial and axillary hair. The growth spurt in boys is a later event — it typically begins only after G3, which is why a boy who is "shooting up" has already been in puberty for some time. Body composition shifts toward lean and muscle mass under testosterone. [2]
Girls vs boys: what comes first and when
A young person may present not with a puberty concern at all but with anxiety about being "different" — the early-maturing girl who looks older than her peers and is treated accordingly, or the late-maturing boy who is bullied for his size. Both can sit entirely within the normal band. Recognising that the distress is real even when the biology is normal is part of the assessment. [10] [15]
Some normal presentations look alarming until you frame them. Physiologic gynaecomastia affects roughly half of boys at around G3 to G4 and resolves spontaneously in most. Irregular menstrual cycles are the norm for the first one to two years after menarche because ovulation is not yet regular. Acanthosis nigricans and a degree of insulin resistance are features of normal puberty. None of these, in isolation, is pathology. [14] [15]
Differential Diagnosis
In a topic about normal puberty, the differential is really a set of pattern-recognition rules that separate the normal and the benign variant from the presentation that must be referred. Master these four distinctions and you will rarely over- or under-investigate. [15]
Premature thelarche
Benign variant
- Isolated breast bud, usually under 6 yr
- Prepubertal gonadotropins
- No growth acceleration
- No pubic hair, no advanced bone age
- Stable or resolves; observe
Premature adrenarche
Benign variant
- Isolated pubic/axillary hair before 8 yr
- Normal bone age and growth velocity
- DHEA-S appropriate for stage
- No clitoromegaly or rapid virilisation
- Flag metabolic/PCOS surveillance
Central precocious puberty
Pathological
- Progressive breast or testicular development under 8/9 yr
- Accelerated growth, advanced bone age
- Raised basal or stimulated LH
- Brain MRI indicated (esp. boys)
Constitutional delay
Normal variant
- Family history of late blooming
- Bone age = height age, both behind chrono age
- Short for family but normal velocity
- Most common cause of delayed puberty in boys (>60%)
The hardest distinction is constitutional delay from permanent hypogonadism. Constitutional delay is a pattern: short for the family, a delayed bone age that matches the height age, and a normal growth velocity, with a family history of late maturation. Permanent hypogonadotropic hypogonadism (such as Kallmann syndrome, where anosmia accompanies the gonadotropin deficiency) or hypergonadotropic hypogonadism (gonadal failure, such as Turner or Klinefelter syndrome) lacks that pattern and often has other features. The distinction can take time and sometimes only declares itself with follow-up — which is why borderline cases are referred rather than dismissed. [4] [6]
Gynaecomastia in a pubertal boy at G3 to G4 is normal and needs only reassurance. Investigate when it is tender and progressive, gross (over 4 cm of glandular tissue), persistent beyond two years, asymmetric, or accompanied by galactorrhoea or other endocrine signs. [15]
Clinical & Bedside Assessment
1. Set up the assessment
Explain what you will examine and why, obtain the young person's assent or consent, and offer a chaperone for any sensitive examination. Pubertal staging requires looking at and gently touching the chest, genitalia and pubic region — this is clinical work that must be done with explicit, developmentally appropriate consent. [15]
2. Stage breast development (girls)
Inspect and then palpate. True thelarche is a firm, disc-like glandular bud beneath the areola, distinct from the soft, diffuse adipose of lipomastia. Inspection alone misses the distinction; gentle palpation between thumb and forefinger is essential. Record the stage B1 to B5. [1] [15]
3. Stage genital development and measure testes (boys)
Inspect the penis and scrotum and measure testicular volume with a Prader orchidometer — a series of oval beads of known volume against which each testis is compared. A volume of at least 4 mL defines the G2 threshold (the onset of puberty); adult volume is over 20 mL. Record the stage G1 to G5 and the measured volume. [2] [15]
4. Stage pubic hair (both sexes)
Inspect and record PH1 to PH5 separately from the gonadal stage. The two are scored independently because they reflect different physiology. [1] [2]
5. Measure and plot growth
Measure height (using a stadiometer), weight, and calculate body mass index, then plot all on age- and sex-appropriate growth charts. Calculate the height velocity over the preceding six to twelve months — normal prepubertal velocity is roughly 5 to 6 cm per year. A child whose velocity has fallen below 4 to 5 cm per year before puberty needs investigation regardless of pubertal stage. [4] [16]
6. Targeted general examination
Look for features that shift a normal assessment toward pathology: a focused neurological examination including visual fields and fundoscopy (central causes), skin for café-au-lait spots or neurofibromas (McCune-Albright, neurofibromatosis), the thyroid, any abdominal or pelvic mass, and in girls any clitoromegaly (an androgen source). These findings change the frame from "reassure" to "refer." [3] [5]
7. Take the history that frames the stage
Ask when each change was first noticed, in what order, and how fast it has progressed. Ask about the parents' and siblings' timing of puberty and their adult heights. Ask about general health, growth, BMI trajectory, chronic illness, medications, and any headaches, visual change or other neurological symptoms. The history of tempo and family timing is often more diagnostic than any single hormone level. [6] [15]
8. Synthesise
Combine the stage, the timing, the tempo, the growth chart trajectory and the family history into one of three impressions: on-time and normal (reassure), a recognisable normal variant (reassure with a safety-net), or outside the band or atypical (refer). The synthesis — not the individual numbers — is what the family needs from you. [15]
Investigations
Most young people with normal puberty need no investigations at all. Investigation is reserved for those whose timing falls outside the band, whose progression is atypical, or in whom the clinical picture does not fit a normal variant. Over-investigating a normal child is a harm: it medicalises a normal process and can surface incidental findings. [15]
For suspected precocious puberty (girls under 8 years or boys under 9 years with progressive signs), the first-line panel is a bone age radiograph (left hand and wrist) and basal gonadotropins (LH, FSH) with the relevant sex steroid (estradiol in girls, testosterone in boys). A bone age advanced by more than two years and a raised basal LH suggest central precocious puberty, which may be confirmed with a GnRH- or agonist-stimulation test. Pelvic ultrasound in girls and brain MRI are second-line, guided by the biochemical picture. [3] [5]
For suspected delayed puberty (girls with no signs by 13 years, boys with no testicular growth by 14 years, or a gap of more than five years from onset to completion), the first-line panel is a bone age and basal gonadotropins with sex steroids, plus screening for chronic disease (full blood count, coeliac serology, thyroid function, inflammatory markers, renal function). A low LH and FSH point to hypogonadotropic causes (constitutional delay or permanent hypogonadism); a raised FSH and LH point to hypergonadotropic (gonadal) causes. [4] [6]
Bone age
Maturation marker
- Left hand and wrist radiograph
- Greulich-Pyle or Tanner-Whitehouse
- Advanced in early/precocious puberty
- Delayed in constitutional delay
- Interpret with the clinical picture, never alone
Basal LH/FSH
Axis localiser
- Low = hypogonadotropic (constitutional, Kallmann)
- High = hypergonadotropic (gonadal failure)
- Pubertal-range LH supports central puberty
- May need stimulation test if equivocal
Brain MRI
Structural cause
- All boys with central precocious puberty
- Girls under 6 yr or with neurological signs
- Not routinely for girls 6–8 yr with isolated CPP
- Looks for hamartoma, tumour, malformation
Brain MRI deserves a specific rule because the yield differs by sex and age. All boys with central precocious puberty warrant imaging, because a higher proportion have an identifiable central nervous system cause. Girls under six years, and any child of any age with central precocious puberty plus neurological signs, also warrant imaging. Girls between six and eight years with isolated, slowly progressive central precocious puberty can often be managed without immediate imaging, weighed against the clinical context. [5]
For the normal variants, investigations are minimal or none. Premature thelarche with no growth acceleration needs no hormonal panel. Premature adrenarche with normal bone age and growth velocity may need only a DHEA-S and 17-hydroxyprogesterone to exclude non-classic congenital adrenal hyperplasia, then surveillance. The discipline is to match the investigation to the pattern, not to screen reflexively. [15]
Management — Resuscitation
A pubertal assessment is rarely a resuscitation, but a small number of presentations that look like "early puberty" are time-critical and must be recognised on the spot. The principle is simple: a pubertal sign plus a red flag exits the routine pathway. [3] [5]
Rapidly progressive precocious puberty — crossing more than two Tanner stages within six to twelve months, with marked growth acceleration and a substantially advanced bone age — risks premature epiphyseal fusion and a significantly reduced adult height. This is not a "watch and wait" scenario; it needs prompt paediatric endocrine referral to consider GnRH-analogue suppression. [3] [5]
Central nervous system red flags accompanying a pubertal finding mandate urgent neuroimaging, not routine referral. These include new or worsening headache, visual field loss, gelastic (laughing) seizures suggesting a hypothalamic hamartoma, morning vomiting, or papilloedema on fundoscopy. A child with central precocious puberty and any of these needs same-day assessment and imaging. [5]
Peripheral androgen excess presenting as sudden virilisation in a girl — clitoromegaly, deepening voice, rapid muscle bulk, severe acne — signals an androgen source (non-classic congenital adrenal hyperplasia or, rarely, an adrenal or ovarian tumour) rather than central puberty, and needs urgent endocrine workup. A hypertensive crisis or electrolyte disturbance raises congenital adrenal hyperplasia to an emergency. [3]
Management — Definitive & Stepwise
Once red flags are excluded, management is longitudinal and developmental. The young person who is within the normal band or who has a recognisable variant is managed with explanation, growth monitoring, anticipatory guidance and a clear safety-net — not investigation or treatment. [15]
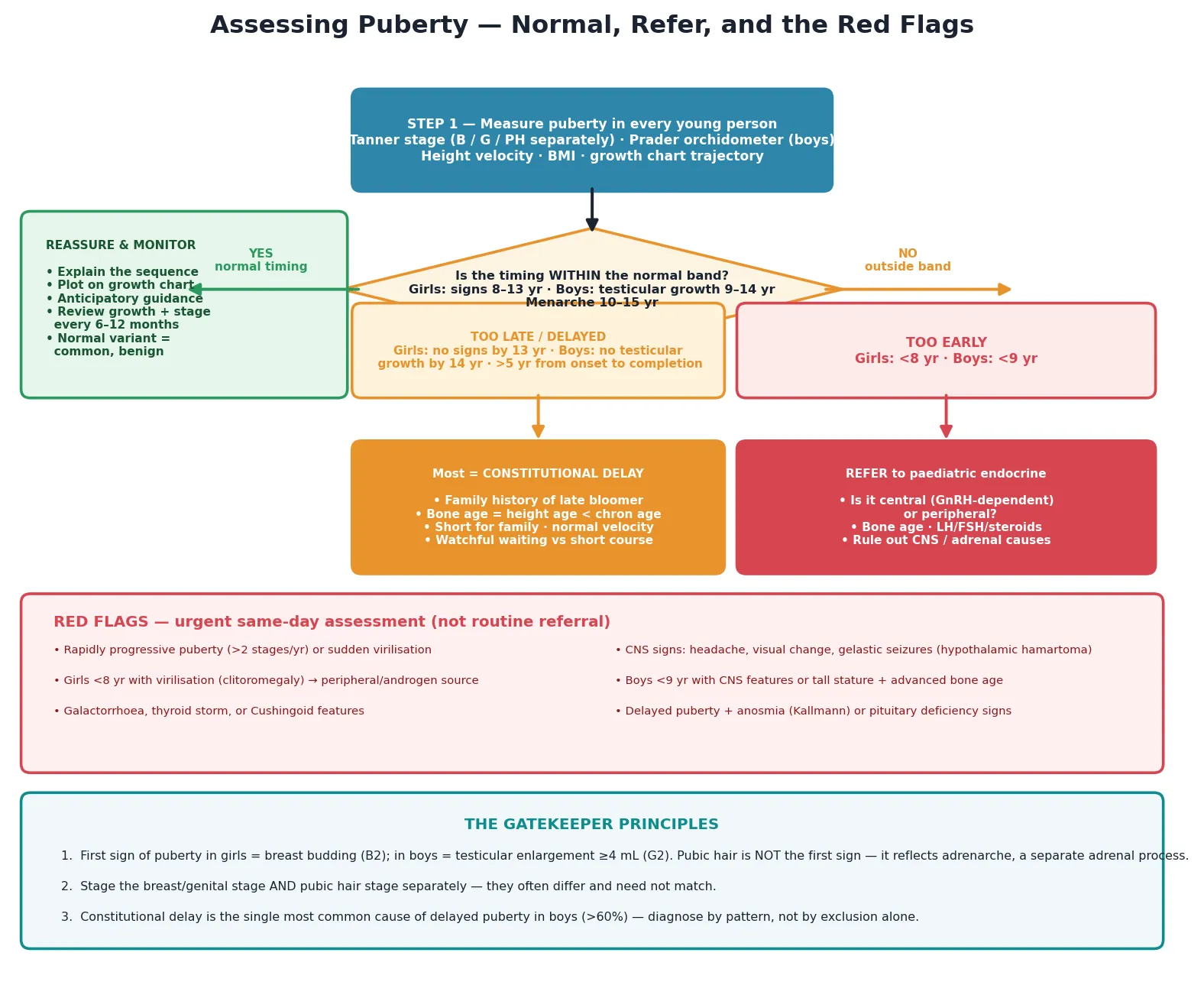
Read the figure like this: the green branch (reassure) is where most young people belong. The amber and red branches are smaller but carry the consequences — missing them is the error that matters. [15]
Step 1 — Reassure and explain the sequence
For the on-time young person and for those with a normal variant, the most powerful intervention is a clear, jargon-free explanation of what puberty is, what comes next, and roughly when. Plot the growth chart with the family, show them the trajectory, and name the variant (premature thelarche, premature adrenarche, constitutional delay) in plain language. Anxiety about "being different" often dissolves once the pattern is named and normalised. [15]
Step 2 — Monitor growth and stage over time
Arrange review every six to twelve months, re-measuring height, weight and Tanner stage, and re-plotting the trajectory. For constitutional delay, the bone age catching up and the eventual onset of puberty confirm the diagnosis prospectively. For premature thelarche, stability or regression confirms the benign course. Monitoring is diagnostic as well as reassuring. [6] [15]
Step 3 — Refer at the agreed thresholds
Refer to paediatric endocrinology when the timing is outside the band (girls under 8 years or no signs by 13 years; boys under 9 years or no testicular growth by 14 years), when progression is rapid, when bone age is markedly discordant, or when any red flag is present. State the referral threshold and the urgency clearly in the letter. [3] [4]
Step 4 — Address the psychosocial impact
For the early-maturing girl and the late-maturing boy, the psychosocial burden can outweigh the biological one. Acknowledge it, support the young person, and involve the school or a psychologist when bullying, withdrawal or risk behaviour is present. Constitutional delay in boys may warrant discussion of a short, low-dose testosterone course to "kick-start" puberty and relieve distress — a decision made with endocrine input, not in isolation. [6] [10]
Step 5 — Anticipatory guidance at each stage
At each visit, give developmentally timed guidance: hygiene and body odour as apocrine glands activate, acne management with rising androgens, menstrual preparation before menarche is expected, growth expectations and final-height discussion, and the mood, sleep and peer changes that accompany brain maturation. Puberty is teachable medicine. [14] [15]
Step 6 — Integrate with the broader adolescent visit
Pubertal assessment sits inside the adolescent preventive visit — do not stage puberty and forget the HEADSS psychosocial screen, mental health, sleep, nutrition, immunisation and sexual health. The two are one encounter. [15]
Step 7 — Safety-net
Give the family clear instructions on when to return sooner: rapid progression of signs, new neurological symptoms, growth that has stopped or fallen off the centile, menstrual abnormalities beyond expected early irregularity, or any distress. A good safety-net converts a single visit into a safe longitudinal plan. [15]
Specific Subtypes & Scenarios
Premature thelarche. A girl under two, or between two and six years, presents with an isolated breast bud, no pubic hair, no growth acceleration and no advanced bone age. Basal gonadotropins are prepubertal. The course is benign — stable or regressing — and management is reassurance with monitoring for any progression to true central puberty. [15]
Premature adrenarche. A child presents with isolated pubic or axillary hair before eight years, with normal bone age and a normal growth velocity. The androgen (DHEA-S) is appropriate for the clinical stage. Exclude non-classic congenital adrenal hyperhalasia with a 17-hydroxyprogesterone, then reassure and surveil — premature adrenarche flags an increased later risk of metabolic syndrome and polycystic ovary syndrome that is worth naming to the family. [15]
Constitutional delay of growth and puberty. The most common cause of delayed puberty in boys (over 60 per cent) and a common cause in girls. The triad is a family history of late blooming, a delayed bone age that matches the height age (both behind the chronological age), and a normal growth velocity with the child short for the family. Management is reassurance, monitoring, and — for boys with significant distress — discussion of a short low-dose testosterone course. Final adult height is normal for the family. [4] [6]
The early-maturing girl within the normal band. A girl who enters puberty at eight or nine years is within the normal band but faces real risks: an older peer group, vulnerability from being treated as older than her years, and lower self-esteem. Support without pathologising — she is not diseased, but she is at a developmental disadvantage that deserves attention. [10] [15]
The late-maturing boy within the normal band. A boy at fourteen with minimal testicular growth and a family history of delay may be entirely on a constitutional-delay trajectory, but the psychosocial cost — bullying, withdrawal, sport disadvantage, identity strain — can be significant. Name the pattern, support the young person, and consider endocrine input for a kick-start. [6]
Chronic disease and puberty. Inflammatory bowel disease, coeliac disease, cystic fibrosis, chronic kidney disease and eating disorders can delay or arrest puberty. The growth chart is the sentinel: a child whose growth falters alongside delayed puberty has disease activity or nutritional deficiency until proven otherwise. Disease control restores the pubertal trajectory. [4] [6]
Puberty in disability and neurodiversity. Staging puberty in a non-verbal young person or one with sensory sensitivities requires a trauma-informed, capacity-aware approach. Assess the capacity to consent to examination, allow extra time and trusted support people, and avoid diagnostic overshadow — endocrine concerns are real even when communication is hard. [15]
Gender-diverse young people. For a young person with gender dysphoria, endogenous puberty can be profoundly distressing. GnRH analogues offer a reversible pause at Tanner stage 2 to 3, buying time while identity consolidates, within a multidisciplinary, affirming care model. The endocrine assessment of pubertal stage is the entry point to that pathway. [15]
Athletes and energy deficit. Intense training with inadequate energy intake — relative energy deficiency in sport (RED-S) — delays puberty and stunts growth. Recognise the interaction of training load and the growth spurt, and address the energy deficit early. [4]
Migrant and refugee young people. When the chronological age is uncertain, bone age and clinical staging become the practical surrogates. Cultural framing of puberty and menstruation varies; use an interpreter when needed and approach the topic with cultural humility. Early-life nutrition and stress influence timing. [13] [15]
Complications & Pitfalls
The most common error is confusing lipomastia (adipose tissue under the areola in a larger child) with true thelarche (glandular breast bud). The distinction is by palpation, not inspection alone — a soft, diffuse, non-disc-like feel is fat; a firm, disc-like feel is gland. Calling fat a breast bud over-diagnoses early puberty. [15]
Treating pubic hair as the first sign of puberty is the second classic error. Because adrenarche is independent of gonadarche, pubic hair can appear before any breast or testicular change. A young person presenting with pubic hair alone has begun adrenarche, not necessarily central puberty — and the assessment must stage the two systems separately to read the picture correctly. [1] [2]
Missing testicular enlargement as the first male sign is easy to do because parents and young people notice pubic hair or a growth spurt before they notice testicular size. Unless you measure testicular volume with a Prader orchidometer, you can under-stage a boy and misclassify his timing. [2] [15]
Over-investigating normal variants is a harm in its own right. Premature thelarche with no growth acceleration does not need a hormone panel, a pelvic ultrasound or an MRI. Premature adrenarche with normal bone age and growth needs minimal testing. The discipline is to match the workup to the pattern. [15]
Under-investigating central precocious puberty in boys is the converse error. Boys with central precocious puberty have a higher proportion of identifiable central nervous system causes than girls, and all warrant brain MRI. Assuming a boy's early puberty is benign is a mistake. [5]
Misinterpreting bone age in isolation is a frequent trap. A single advanced bone age does not equal pathology, and a delayed bone age does not alone confirm constitutional delay. Bone age is interpreted with the clinical picture, the growth velocity and the family history — never as a standalone test. [4] [6]
Failing to recognise that growth ceases roughly two to two-and-a-half years after menarche leads to false reassurance about remaining growth. A girl who has menarche at ten years is near the end of her growth, not the beginning — a key adult-height predictor that changes counselling. [16]
Confusing physiologic gynaecomastia in a pubertal boy with a pathological breast mass causes unnecessary anxiety and investigation. Roughly half of boys develop some glandular breast tissue at G3 to G4; it resolves in most within one to two years. [15]
Assuming irregular menstrual cycles in the first one to two post-menarchal years are pathological leads to over-investigation. Anovulatory cycles are the norm early on; regularity usually emerges within two years. [14]
Prognosis & Disposition
For the young person with normal puberty, the prognosis is straightforward: progression to full reproductive maturity over three to five years, with a final adult height predicted by the timing of the growth spurt and of menarche. The disposition is primary care follow-up with growth monitoring and anticipatory guidance until completion. [15]
The normal variants carry an excellent prognosis when correctly identified. Premature thelarche is stable or regresses. Premature adrenarche is benign in itself but flags metabolic and polycystic ovary syndrome surveillance into later life. Constitutional delay reaches full puberty and a normal adult height for the family — the only lasting cost is usually psychosocial. [6] [15]
Disposition splits into three tiers. The on-time or normal-variant young person is reassured and followed in primary care with a safety-net. The borderline-timing young person who does not yet meet a referral threshold but whose pattern is uncertain is monitored closely, with a planned review that will declare the trajectory. The outside-the-band or red-flag young person is referred to paediatric endocrinology, with urgency tiered to the clinical concern. [3] [4]
Long-term outcomes worth naming during counselling include bone density, which accrues substantially during the growth spurt and is compromised if puberty is delayed or suppressed untreated; the metabolic risk carried by early maturers and by premature adrenarche; and the psychosocial outcomes of mistimed puberty, which are often more burdensome than the biological ones. [13] [16]
Safety-net the family explicitly: return sooner if signs progress rapidly, if new neurological symptoms appear, if growth stops or falls off the centile, if menstrual bleeding is heavy or persistent beyond expected early irregularity, or if the young person is in distress. [15]
Special Populations
Girls enter puberty earlier and more body-fat-dependently than boys, and the early-maturing girl within the normal band faces heightened psychosocial vulnerability — older peer groups, earlier sexualisation, and lower self-esteem. Menstrual preparation and cycle education are part of her care. [14] [13]
Boys enter puberty later, and constitutional delay dominates the delayed-puberty presentations. The psychosocial cost of being short or physically immature among peers — bullying, withdrawal, sport and identity strain — is real and deserves direct support. [6]
Gender-diverse young people may experience endogenous puberty as deeply distressing. The pubertal assessment is the entry point to a multidisciplinary, affirming pathway in which GnRH analogues can offer a reversible pause. Approach with clinical humility and without prejudice. [15]
Chronic disease (inflammatory bowel disease, coeliac disease, cystic fibrosis, chronic kidney disease, eating disorders) delays or arrests puberty. The growth chart is the sentinel; disease control restores the trajectory. [4] [6]
Disability and neurodiversity require capacity-aware consent, trauma-informed staging, and vigilance against diagnostic overshadow of endocrine concerns. Extra time, trusted support people and sensory adjustments make the assessment possible. [15]
Athletes face relative energy deficiency in sport, which delays puberty and stunts growth when training outstrips intake. Address the energy deficit early. [4]
Indigenous, migrant and refugee young people may have uncertain chronological ages, making bone age and clinical staging the practical surrogates. Cultural framing of puberty and menstruation varies; early-life nutrition and stress influence timing, and childhood adversity has been associated with earlier menarche. Use interpreters and approach with cultural humility. [13] [15]
Evidence, Guidelines & Regional Differences
Marshall and Tanner's original 1969 and 1970 studies defined the staging framework still used worldwide and remain the reference standard for the orderly sequence of pubertal changes in girls and boys. The criteria have been validated and refined in many populations since, but the core five-stage scheme is unchanged. [1] [2]
The secular trend toward earlier puberty, particularly earlier thelarche and menarche in girls, is well documented and is linked at least partly to rising childhood obesity; the contribution of endocrine-disrupting chemicals is biologically plausible but remains an active area of research with mixed evidence quality. Modern population-specific reference ranges, such as those from the Copenhagen Puberty Study, complement the original Tanner data and reflect contemporary timing. [13] [7] [17]
The kisspeptin model has reshaped the modern understanding of puberty physiology, locating the gate to GnRH-pulse reactivation in kisspeptin signalling and integrating energy-balance signals (leptin, insulin) into the timing mechanism. This is the framework a fellowship candidate should hold when explaining why body fat and nutritional status matter. [8] [9]
ANZ: Royal Children's Hospital Melbourne clinical resources and local youth-health frameworks frame adolescent pubertal assessment within youth-friendly, confidential care; referral thresholds follow the standard bands with local endocrine protocols.
UK: RCPCH Progress+ maps growth and pubertal staging to training levels; BSPED guidelines guide the management of delayed puberty; local consent and safeguarding frameworks apply.
US: Bright Futures periodicity and AAP guidance frame pubertal assessment within the adolescent preventive visit; a debate continues on whether the evaluation threshold for girls should be 7 versus 8 years, with adjustment by ethnicity and progression.
Canada: the Canadian Paediatric Society and the Greig Health Record frame adolescent preventive care including pubertal assessment, with provincial variation in referral pathways.
The threshold debate is worth knowing. Some guidelines have proposed evaluating African-American girls from 6 years and white girls from 7 years, on the grounds that early thelarche is more common in some populations and that the traditional 8-year cut-off over-medicalises normal variation. The concern is that lowering thresholds pathologises healthy children. The defensible fellowship position is to use the standard bands as a screen but to individualise: a girl at seven with isolated, non-progressive thelarche, a normal bone age and no growth acceleration is managed differently from one at seven with rapid progression and advanced bone age. [13] [15]
The Pubertal Development Scale, a self-report measure developed by Petersen and colleagues, is widely used in research and school settings as a non-clinical proxy for Tanner staging; a recent systematic review confirms reasonable reliability but reaffirms that clinician-assessed staging remains the standard for clinical decisions. [12] [18]
Exam Pearls
- First sign of puberty: girls = breast budding (B2); boys = testicular enlargement to at least 4 mL (G2). Pubic hair is not the first sign in either sex. [1] [2]
- Normal age band: girls 8 to 13 years, boys 9 to 14 years; menarche 10 to 15 years, roughly two to two-and-a-half years after thelarche. [13] [14]
- Peak height velocity: girls about 8 cm per year at 11.5 to 12 years; boys about 9 to 10 cm per year at 13.5 to 14 years. Boys' spurt is later and taller. [16]
- Adrenarche (about 6 to 8 years) and gonadarche are independent — adrenal DHEA-S drives pubic and axillary hair separately from the HPG axis. [8] [14]
- Kisspeptin neurons (KNDy) reactivate the GnRH pulse generator at puberty onset; energy-balance signals (leptin, insulin) modulate timing. [8] [9]
- Growth ceases about two to two-and-a-half years after menarche — a key adult-height predictor. [16]
- Constitutional delay is the most common cause of delayed puberty in boys (over 60 per cent): the triad is family history, delayed bone age equal to height age, and normal growth velocity. [4] [6]
- Stage breast/genital and pubic hair separately — they often differ and need not match. [1] [2]
- Prader orchidometer: each oval is a known volume; at least 4 mL defines the G2 threshold; adult volume is over 20 mL. [2] [15]
- All boys with central precocious puberty warrant brain MRI (higher yield of a central cause); girls 6 to 8 years with isolated, slowly progressive central precocious puberty may be managed without immediate imaging. [5]
- Physiologic gynaecomastia is normal in about half of boys at G3 to G4; reassure unless tender, progressive, gross, persistent, or asymmetric. [15]
- Irregular anovulatory cycles are normal for one to two years post-menarche. [14]
- Physiologic insulin resistance and acanthosis nigricans are features of normal puberty. [14]
- The adolescent brain: synaptic pruning and myelination; reward circuitry matures before cognitive control — the biology of adolescent risk-taking. [10] [11]
ORDER of puberty — girls
References
- [1]Marshall WA, Tanner JM Variations in pattern of pubertal changes in girls. Archives of disease in childhood, 1969.PMID 5785179
- [2]Marshall WA, Tanner JM Variations in the pattern of pubertal changes in boys. Archives of disease in childhood, 1970.PMID 5440182
- [3]Carel JC, Leger J Clinical practice. Precocious puberty. The New England journal of medicine, 2008.PMID 18509122
- [4]Palmert MR, Dunkel L Clinical practice. Delayed puberty. The New England journal of medicine, 2012.PMID 22296078
- [5]Latronico AC, Brito VN, Carel JC Causes, diagnosis, and treatment of central precocious puberty. The lancet diabetes & endocrinology, 2016.PMID 26852255
- [6]Harrington J, Palmert MR An Approach to the Patient With Delayed Puberty. The Journal of clinical endocrinology and metabolism, 2022.PMID 35100608
- [7]Lopez-Rodriguez D, Franssen D, Heger S, Parent AS Endocrine-disrupting chemicals and their effects on puberty. Best practice & research. Clinical endocrinology & metabolism, 2021.PMID 34563408
- [8]Herbison AE Control of puberty onset and fertility by gonadotropin-releasing hormone neurons. Nature reviews. Endocrinology, 2016.PMID 27199290
- [9]Navarro VM Metabolic regulation of kisspeptin - the link between energy balance and reproduction. Nature reviews. Endocrinology, 2020.PMID 32427949
- [10]Casey BJ, Jones RM, Hare TA The adolescent brain. Annals of the New York Academy of Sciences, 2008.PMID 18400927
- [11]Steinberg L A Social Neuroscience Perspective on Adolescent Risk-Taking. Developmental review, 2008.PMID 18509515
- [12]Petersen AC, Crockett L, Richards M, Boxer A A self-report measure of pubertal status: Reliability, validity, and initial norms. Journal of youth and adolescence, 1988.PMID 24277579
- [13]Sorensen K, Mouritsen A, Aksglaede L, Hagen CP, Mogensen SS, Juul A Recent secular trends in pubertal timing: implications for evaluation and diagnosis of precocious puberty. Hormone research in paediatrics, 2012.PMID 22508036
- [14]Apter D, Hermanson E Update on female pubertal development. Current opinion in obstetrics & gynecology, 2002.PMID 12401974
- [15]Smith CE, Biro FM Pubertal Development: What's Normal/What's Not. Clinical obstetrics and gynecology, 2020.PMID 32482957
- [16]Sorensen K, Hagen CP, Aksglaede L, Juul A Higher peak height velocity in early maturing girls depends on insulin rather than fat mass or IGF-I. European journal of endocrinology, 2024.PMID 39292994
- [17]Lopez-Rodriguez D, Franssen D, Delbaere J, Naveau C, Evrard A, Gerard A, Parent AS Cellular and molecular features of EDC exposure: consequences for the GnRH network. Nature reviews. Endocrinology, 2021.PMID 33288917
- [18]Pan D, Lin C A systematic review and meta-analysis of the self-reported Pubertal Development Scale's applicability. Journal of pediatric endocrinology & metabolism, 2025.PMID 40256953