Paeds · adolescent-and-young-adult-medicine
School refusal, bullying and social exclusion
Also known as Anxious school refusal in adolescence · Bullying victimisation and school disengagement · Cyberbullying and school avoidance · Peer exclusion and attendance collapse · School absenteeism in young people
A fellowship approach to the adolescent whose school attendance collapses, where school refusal, bullying victimisation and social exclusion overlap. Covers Kearney functional analysis adapted to adolescence, bully-role assessment, school belonging, exposure-based CBT with graded return, whole-school anti-bullying response, and SSRI evidence for the underlying anxiety or depression — across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 14-year-old stops going to school after a term of name-calling that moved to group chats. She tells her GP she has "stomach migraines." Her mother, exhausted, asks for "a few weeks off." Nobody mentions the bullying. Six weeks later she is in the emergency department after an overdose. The missed work was not a single diagnosis. It was three drivers that nobody connected. [9] [11]
School refusal is a behaviour, not a freestanding diagnosis: difficulty attending school with emotional distress, usually with caregiver knowledge of the absence. In adolescence it rarely travels alone. It blends with bullying victimisation (face-to-face or cyber) and social exclusion — the loss of belonging and peer connection that makes school feel unbearable. The clinical skill is to see all three and treat the whole picture rather than chasing one label. [1] [2]
The fellowship-level point is simple but load-bearing: return to learning is a mental-health intervention. Attendance is the outcome of feeling safe enough, connected enough and well enough to walk through the gate. A plan that targets attendance without safety, belonging and treatment of the underlying distress will fail the young people at greatest risk. [9] [10]
Core sequence for the school-disengaged adolescent
Secure
Time alone, conditional confidentiality, non-judgemental stance, greet the young person first.
Assess
Multi-informant attendance map, HEEADSSS, bully role, belonging, suicide screen.
Exclude red flags
Suicide risk, safeguarding/abuse, medical red flags in somatic symptoms.
Formulate
Kearney functions + bully dynamic + co-morbidity + readiness.
Act this week
Graded return + CBT, whole-school anti-bullying response, re-connection.
Treat and review
SSRI if moderate–severe anxiety/depression; dated certificates; timed review.
Classification
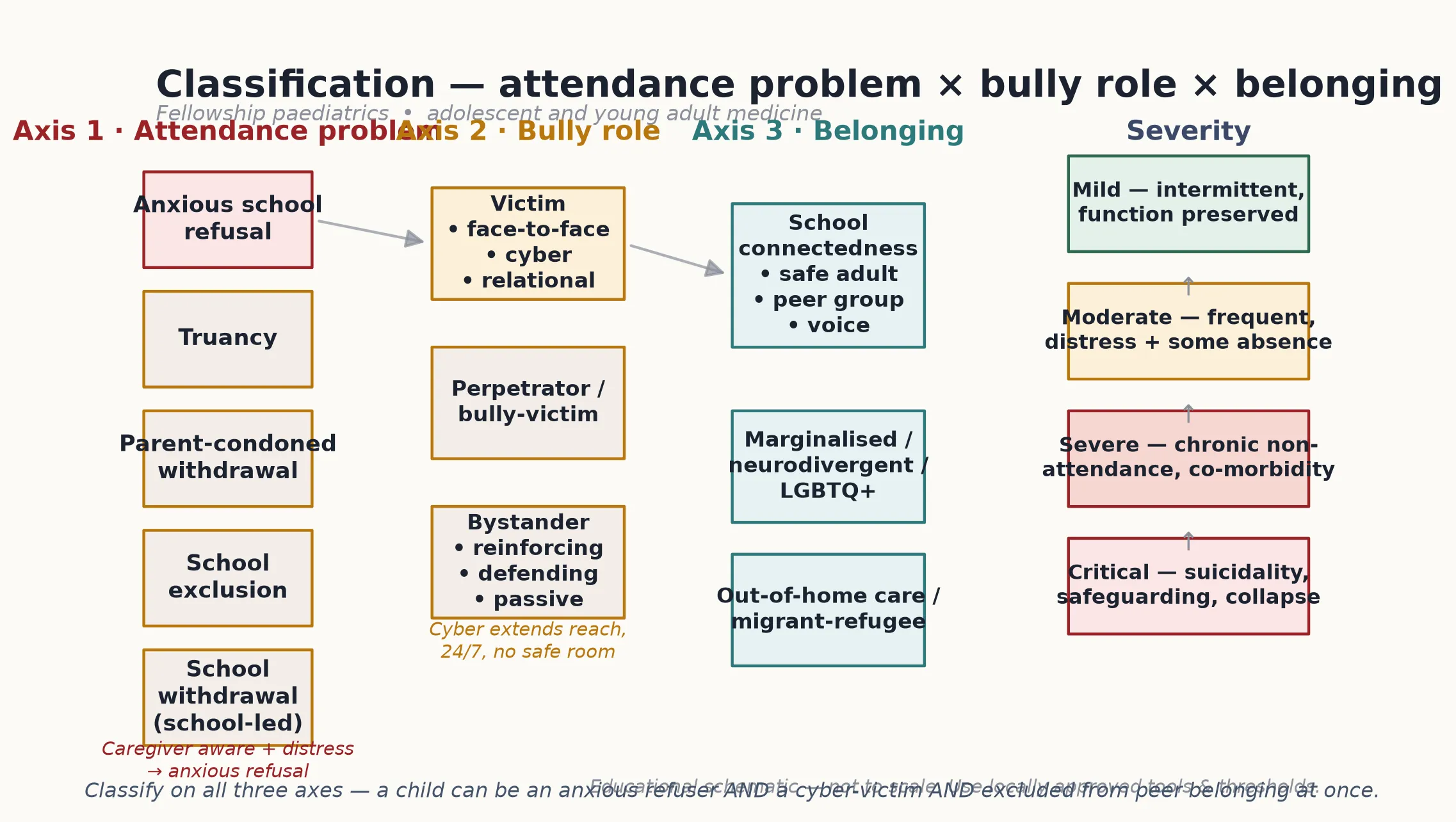
Classify the adolescent's presentation on three axes at once. The attendance axis tells you what the behaviour looks like; the bully-role axis tells you who is doing what to whom; the belonging axis tells you what the school feels like from the inside. A single child can sit differently on each axis, and the combination drives the plan. [1] [2]
Attendance problem
Anxious school refusal is distress-driven non-attendance and the caregiver usually knows. Truancy is often covert, with less anxiety and more externalising or peer-linked skipping. Parent-condoned withdrawal and school-led withdrawal describe carers or schools keeping the young person out, and school exclusion is a formal disciplinary or safeguarding removal. These carry different drivers and different pathways, so name the one in front of you. [2]
Bully role
A young person can be a victim, a perpetrator, a bully-victim (both), or a bystander. Victimisation splits further into face-to-face, cyber and relational forms. Cyber is its own category because it removes the safe-room effect — the harm is 24/7, public and permanent, and it follows the young person home. [9] [10]
Belonging and severity
Belonging is the protective scaffold: a trusted adult, a peer group and a sense of voice. Map it alongside severity — mild (intermittent, function preserved), moderate (frequent, distress with some absence), severe (chronic non-attendance with co-morbidity), or critical (suicidality, safeguarding concern, collapse). Severity decides intensity, not whether to act. [9] [8]
Anxious refusal
Distress-driven
- Caregiver aware of absence
- Weekday somatic symptoms, weekend recovery
- Fear, panic, tears at the gate
- Negative reinforcement from escape
Truancy
Covert absence
- Caregiver often unaware
- Less school-related anxiety
- Externalising or peer-linked skipping
- Different psychiatric profile
Bully-driven avoidance
Threat-driven
- Specific peers or locations feared
- Cyber harm may extend 24/7
- Disclosed or hidden
- School becomes the site of harm
Exclusion / withdrawal
School- or carer-led
- Formal or informal removal
- Safeguarding or discipline drivers
- Needs reintegration pathway
- Structural rather than purely clinical
Epidemiology & Risk Factors
Bullying victimisation is one of the most common adverse exposures in adolescence, and its mental-health footprint is large and durable. Across high-income settings, victimised adolescents carry a markedly higher burden of depression, anxiety, psychosomatic symptoms and self-harm than non-victimised peers. [9] [10]
The suicide signal is the one to hold onto. A meta-analysis linking bullying and suicidal ideation and behaviours found victimisation associated with excess suicidal thoughts and attempts — a signal that holds after accounting for other psychiatric risk. Among suicidal adolescents, bullying perpetration and victimisation during the school years raise the odds of later depression and suicidality. [9] [11]
Risk is not evenly distributed. Prior anxiety or depression, neurodivergence, disability, LGBTQ+ minority stress, out-of-home care, migrant or refugee status, family conflict and the absence of a trusted adult all amplify exposure and reduce access to confidential, safe care. Socioeconomic disadvantage and rural isolation narrow the choices a family has. [9] [10]
Pathophysiology
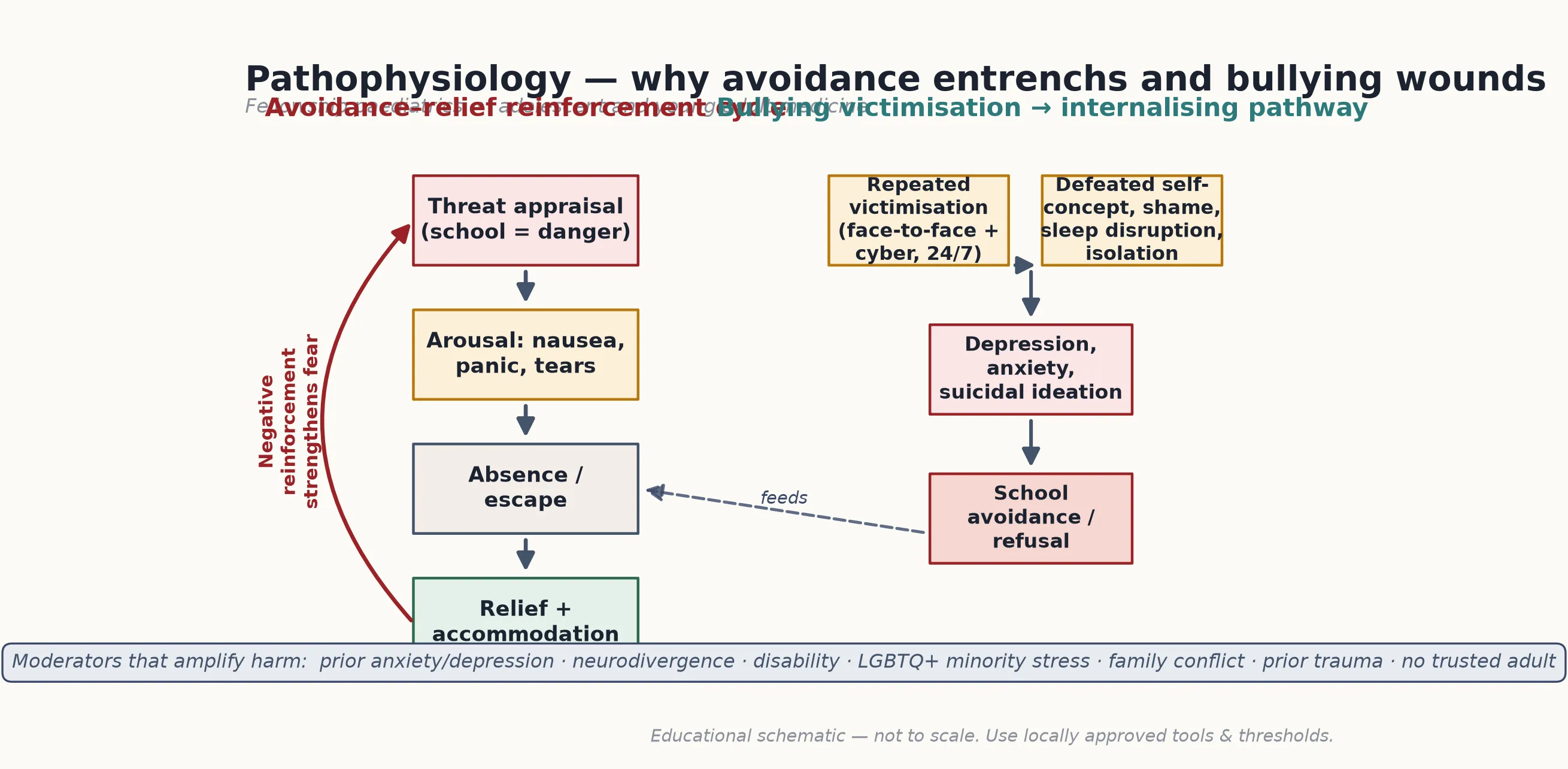
A usable model of mechanism explains why a few mornings of "feeling sick" become months of absence, and why a bullied teenager spirals rather than shrugs it off. Two pathways run in parallel and feed each other. [1] [9]
The avoidance–relief reinforcement cycle is the engine of school refusal. School triggers a threat appraisal. Arousal follows — nausea, panic, tears. The young person stays home, and the distress falls. Relief plus caregiver accommodation rewards the avoidance and teaches the brain that school is genuinely dangerous. Each successful escape strengthens the fear, so the next morning is harder, not easier. [1]
The bullying-to-internalising pathway explains the wound. Repeated victimisation — amplified when cyber follows the young person home — erodes self-concept, drives shame and sleep disruption, and isolates the adolescent from the peer group. That combination feeds depression, anxiety and suicidal ideation, which in turn makes school feel more threatening and harder to face. [9] [10]
The dual-systems model of adolescent brain development matters here. The reward and socio-emotional system matures earlier and peaks through mid-adolescence, while cognitive control lags behind. Under social and emotional load, an adolescent can genuinely intend to attend and still not manage it. The peer environment weighs more in this window than it ever will again, which is why belonging is not a soft variable — it is the load-bearing wall. [1] [9]
Clinical Presentation
School disengagement presents across a spectrum, from the openly disclosed bully victim to the completely hidden anxious refuser. The most dangerous presentations are often the quiet ones, because nobody looked past the attendance label. [1] [9]
Somatic pattern. Weekday-morning nausea, abdominal pain or panic that remits when school is avoided, with recovery at weekends and holidays, is the classic school-refusal signature. It still needs a medical red-flag screen — nocturnal waking, progressive pain, weight loss and systemic features change the story. [1]
Bullying hidden inside ordinary distress. A bullied adolescent may never name the bullying. They present as withdrawal, declining marks, sleep reversal, self-harm, a sudden change in online identity, or a quiet request to change schools. Phone-guarding and a mood drop after device use are cyber signs worth asking about directly. [9] [10]
Acute risk. Overdose, self-harm, an assault disclosure, or a positive suicide screen with plan and intent all exit the routine pathway immediately and enter safety care. Among suicidal adolescents, bullying is a clear and modifiable contributor — so treating it is part of the acute response, not a later add-on. [9] [11]
[9] [10]Differential Diagnosis
The differential in this presentation is less "which disease" and more "what is driving the disengagement, and is it dangerous." A structuring table keeps the encounter honest. [1] [9]
| What it looks like | Safer framing question | Do not miss |
|---|---|---|
| Weekday-morning stomach pain | Is this school-related anxiety after a red-flag screen? | Medical disease with nocturnal or progressive features |
| Withdrawal and declining marks | Is there undisclosed bullying or cyber harm? | Active suicide risk needing same-day action |
| Refusal to attend specific days | Which lesson, peer, teacher or route is the trigger? | Safeguarding or abuse underneath the attendance label |
| "Just lazy" or "bad attitude" | Has anyone built private time to ask? | Untreated anxiety, depression, ADHD or learning disorder |
| Requests to change schools | What is the young person escaping? | Exploitation or trafficking masquerading as choice |
The core discriminator is function. Does the behaviour sit alongside intact home, school and peer function, or is it accompanied by impairment, danger and instability? Normative exploration and ordinary teen friction do not need treatment. Impairment, danger and a lost sense of safety do. [1] [9]
Clinical & Bedside Assessment
1. Secure the frame
Greet the young person first, set a joint agenda, then secure time alone. State conditional confidentiality with its limits out loud and check understanding. Without this frame the assessment returns false negatives — a parent who answers every question has not been tested for risk. [1] [8]
2. Build the attendance map
Pull data from school records, caregiver and youth: days missed in the last term, the pattern, the triggers, and what recovery looks like at weekends. Attendance is multi-informant; a single source hides the picture. Convert the map into a symptom-and-attendance diary that captures triggers, avoidance, relief and maintaining factors. [2] [1]
3. Run HEEADSSS with focused probes
Work the domains with open then focused questions — Home, Education/Employment, Eating, Activities, Drugs, Sexuality, Suicide/mood, Safety — and add a strengths pass. Follow every positive lead deeper rather than ticking the box. [1] [8]
4. Ask about bullying and belonging directly
Ask separately about face-to-face and cyber victimisation, who the perpetrator is, who the bystanders are, and whether a trusted adult exists at school. Belonging is the protective scaffold; its absence is a finding, not a soft note. A young person who cannot name a safe adult is at higher risk. [9] [10]
5. Screen suicide and safety
Use a brief instrument such as the Ask Suicide-Screening Questions (ASQ) or Columbia protocol as a trigger, then move immediately to a full clinical assessment of intent, plan, means and protection if positive. Anxiety does not protect against suicide — among victimised adolescents it raises the risk. [9] [11]
[1] [8] [9]Investigations
There is no blood test for school refusal. Investigations are targeted medical red-flag exclusion for somatic symptoms — not a blanket workup. Repeated normal panels that delay return entrench the avoidance cycle and teach the young person that something dangerous is being hunted. [1] [8]
Use validated screens where a lead appears. CRAFFT or S2BI stratify substance use; ASQ or Columbia act as suicide triggers; locally approved mood and anxiety scales such as the PHQ-A or GAD-7 track severity and response. A screen is a prompt for clinical thinking, never a diagnosis on its own. [8]
Functional analysis is the real investigation. A diary that captures the triggers, the avoidance, the relief and the maintaining factors does more to guide treatment than any laboratory panel, because it locates the mechanism you will treat. [1] [2]
Management — Resuscitation
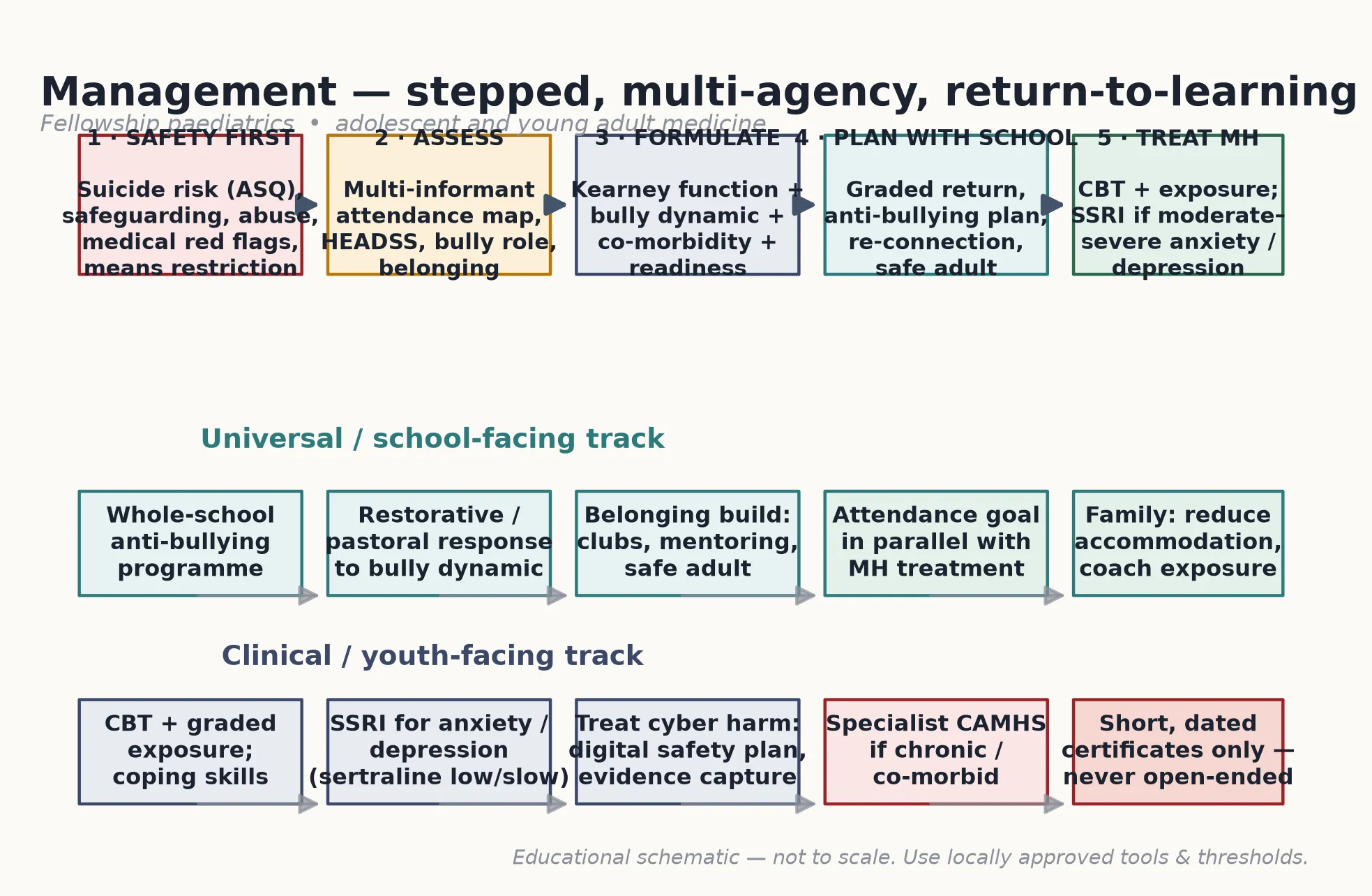
Safety comes before any attendance plan. First exclude active suicide risk, a safeguarding concern and medical instability — each of these exits the routine pathway. Means-restriction safety planning happens the same day if there is any suicidal ideation, plan or recent attempt, with carers involved and the plan documented. [9] [11]
Stabilise the acute mental state — severe agitation, self-harm or intoxication — before graded return is even discussed. For cyberbullying that involves images, threats or criminal content, capture and preserve evidence safely and escalate to police or child protection as the disclosure requires. [9] [10]
Frame this for the family clearly: safety first, then return-to-learning runs in parallel with treatment. The two are not sequential — an adolescent can begin a graded return while depression and the bully dynamic are being actively treated, and waiting for perfect symptom remission before any attendance goal usually deepens the entrenchment. [8] [1]
Management — Definitive & Stepwise
Exposure-based CBT and graded return
First-line treatment is exposure-based CBT with a fear hierarchy, graded school exposures, cognitive work on catastrophic beliefs and contingency management. Graded return moves the same week, with school: the gate, a short classroom visit, a partial timetable, then a full day. Attendance is measured weekly, and high-value home leisure is not available during school hours. [4] [3]
Caregiver training supports outcomes. The job is to reduce excessive reassurance and accommodation and to coach planned exposures rather than open-ended staying home. Families who cancel school "to settle" the young person are inadvertently strengthening the avoidance cycle, so the work names that pattern without blame. [3] [1]
Whole-school anti-bullying response and re-connection
A meta-analysis of randomised school anti-bullying trials found whole-school programmes reduce victimisation — so school intervention is clinical care, not someone else's job. Pair a whole-school programme with a specific, restorative response to the bully dynamic, and actively rebuild belonging through clubs, mentoring and a named safe adult. [12] [9]
SSRI for the underlying anxiety or depression
Medication treats the underlying moderate–severe anxiety or depression, not "school refusal." The CAMS trial supports CBT, sertraline and especially combination for childhood separation, social and generalised anxiety — each beat placebo, with combination highest. The Melvin trial is the cautionary anchor: adding fluoxetine to CBT in anxious school-refusing adolescents did not clearly beat CBT alone for attendance outcomes, so do not overclaim SSRI superiority for attendance specifically. [6] [5]
Start low and titrate slowly — for example sertraline 25 mg oral daily or fluoxetine 10 mg oral daily — and counsel activation and suicidality. Bridge's meta-analysis found a small absolute increase in reported suicidal ideation and attempts with paediatric antidepressants, so review early and document the monitoring plan. [7] [8]
Certificates and the home-schooling request
Short, dated medical certificates are acceptable only if the young person is truly unfit, and each one is paired with a written reintegration date and a graded plan. Indefinite home schooling without a reintegration pathway entrenches avoidance through negative reinforcement. Decline open-ended certificates; offer a structured return instead. [1] [3]
Specific Subtypes & Scenarios
Cyberbullying with school refusal
Digital harm follows the young person home, so the plan rebuilds safety both online and on-site. A digital safety plan sets device boundaries, captures and preserves evidence, reports through the platform, and escalates to police or child protection where criminal content is involved. Graded return runs in parallel, because the on-site and online environments are the same threat now. [9] [10]
Neurodivergent and disabled adolescents
ASD and ADHD raise both bullying exposure and school distress. Keep the same graded-return principles and adapt the load: sensory plans, visual schedules, predictable transitions and communication supports. Do not abandon exposure for phobic avoidance, and do not force "just try harder" without adapting the environmental demand. [8] [9]
LGBTQ+ victimisation and exclusion
Minority stress and targeted victimisation drive a distinct presentation. Affirming the young person's identity is part of the treatment, not separate from it. Name the bully dynamic, address the minority stress, and build a safe-adult scaffold the young person trusts. [9] [10]
Out-of-home care and migrant-refugee youth
Mobility disrupts school connection, trauma multiplies risk, and access to confidential care is often narrower. Trauma-informed return planning respects the prior adversity while still moving toward attendance and belonging. [9] [11]
The bully-victim
A young person who both perpetrates and is victimised sits on both sides of the dynamic. Address externalising co-morbidity, use restorative over purely punitive responses, and treat the victimisation the adolescent also experiences. [9] [12]
[8] [10]Complications & Pitfalls
Open-ended medical certificates and indefinite home schooling are the commonest iatrogenic harm. Each day of unstructured absence strengthens the avoidance cycle and pushes reintegration further away. A dated certificate paired with a reintegration date is the safe alternative. [1] [3]
Treating the bully dynamic as pure school discipline misses the victim's mental-health need and the perpetrator's drivers. Diagnostic overshadowing does similar damage — attributing distress to ASD, ADHD or disability and missing co-morbid anxiety, depression or abuse. Both errors leave the load-bearing problem untreated. [9] [8]
Two evidence pitfalls trap candidates. The first is anchoring on anxiety and missing medical red flags in somatic presentations. The second is overclaiming SSRI benefit for attendance: the Melvin trial did not show fluoxetine clearly beating CBT alone for school-refusal attendance, and Bridge reminds us antidepressants carry a small suicide-signal that demands active monitoring. [5] [7]
Prognosis & Disposition
Most young people improve with timely exposure-based CBT, a graded return and a whole-school anti-bullying response. Earlier return predicts a better outcome, which is why the plan moves the same week rather than waiting for perfect symptom remission. [4] [3]
Chronic non-attendance, untreated co-morbidity and the absence of a trusted adult predict poorer academic, social and mental-health outcomes. Disposition follows severity: a routine primary-care and school pathway for mild-to-moderate presentations, and specialist child and adolescent mental-health services for severe, chronic or high-risk cases. [8] [9]
Plan for transition where disorder persists into late adolescence, and give a clear safety net: low-threshold re-access, a written plan, a timed review, and a named person to call if risk rises. The young person should leave the visit knowing the next step and the escape route if things worsen. [9] [11]
Special Populations
Neurodivergent and disabled young people face higher bullying exposure and greater school distress, so adapt the return with sensory and communication supports without abandoning exposure. LGBTQ+ youth carry minority stress and targeted victimisation; affirming care is part of treatment. [9] [10]
Out-of-home care and migrant, refugee or asylum-seeking youth face mobility, trauma and disrupted belonging that multiply risk, and they often have narrower access to confidential care. Youth-justice-involved and socioeconomically disadvantaged adolescents carry structural drivers that a clinical plan alone cannot fix — advocacy and service linkage are part of the disposition. [9] [11]
Indigenous and culturally diverse young people need culturally safe engagement, language-accessible assessment and school connection that respects identity. A plan that ignores culture and language fails the very adolescents most at risk of disengagement. [9] [10]
Evidence, Guidelines & Regional Differences
The anxiety-treatment evidence anchors the SSRI decision. The CAMS trial showed CBT, sertraline and combination each beat placebo for childhood anxiety, with combination highest for acute response. The Melvin trial is the school-refusal-specific caution: fluoxetine did not clearly beat CBT alone for attendance outcomes, so medication is for the anxiety or mood driver, not a magic school pill. [6] [5]
The AACAP anxiety practice guideline places CBT first-line and considers an SSRI for moderate-to-severe or non-responsive anxiety. Bridge's meta-analysis quantifies the small absolute increase in reported suicidal ideation and attempts with paediatric antidepressants, which is why monitoring is part of the prescription. [8] [7]
The bullying evidence is what makes school intervention clinical care. Holt's meta-analysis links victimisation to suicidal ideation and behaviours; Moore's systematic review maps the durable internalising and psychosomatic morbidity; and the Fraguas meta-analysis of randomised trials shows whole-school anti-bullying programmes reduce victimisation. [9] [10] [12]
Regional service models differ. In Australia and New Zealand, school attendance and welfare teams link with CAMHS or youth mental-health pathways. In the UK, pastoral support and Early Help sit alongside Child and Adolescent Mental Health Services. In the US, school counsellors, 504 plans and Individualized Education Programs frame the response. In Canada, school-board and mental-health linkage drives the pathway. The clinical principles are constant; the levers you pull depend on the system you work in. [1] [8]
Evidence anchors at a glance
Exam Pearls
The school-disengagement stack — FUNCTION + SCREEN + RETURN + TREAT
School refusal is a behaviour, not a diagnosis — and in adolescence it blends with bullying victimisation and social exclusion. [1] [2]
Anxious refusal is not truancy: distress and caregiver awareness set them apart, and the psychiatric profiles differ. [2]
Hold the evidence straight: CAMS supports combination treatment for childhood anxiety; Melvin does not support fluoxetine over CBT alone for school-refusal attendance. [6] [5]
Bullying victimisation carries a real suicide signal and durable morbidity — so asking about it and acting on it is clinical care, not pastoral work. [9] [10]
References
- [1]Kearney CA, Albano AM The functional profiles of school refusal behavior. Diagnostic aspects. Behavior Modification, 2004.PMID 14710711
- [2]Egger HL, Costello EJ, Angold A School refusal and psychiatric disorders: a community study. Journal of the American Academy of Child and Adolescent Psychiatry, 2003.PMID 12819439
- [3]Heyne D, King NJ, Tonge BJ, Rollings S, Young D, Pritchard M, Ollendick TH Evaluation of child therapy and caregiver training in the treatment of school refusal. Journal of the American Academy of Child and Adolescent Psychiatry, 2002.PMID 12049443
- [4]King NJ, Tonge BJ, Heyne D, Pritchard M, Rollings S, Young D, Myerson N, Ollendick TH Cognitive-behavioral treatment of school-refusing children: a controlled evaluation. Journal of the American Academy of Child and Adolescent Psychiatry, 1998.PMID 9549960
- [5]Melvin GA, Dudley AL, Gordon MS, Klimkeit E, Gullone E, Taffe J, Tonge BJ Augmenting Cognitive Behavior Therapy for School Refusal with Fluoxetine: A Randomized Controlled Trial. Child Psychiatry and Human Development, 2017.PMID 27485100
- [6]Walkup JT, Albano AM, Piacentini J, Birmaher B, Compton SN, Sherrill JT, Ginsburg GS, Rynn MA, McCracken J, Waslick B, Iyengar S, March JS, Kendall PC Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. New England Journal of Medicine, 2008.PMID 18974308
- [7]Bridge JA, Iyengar S, Salary CB, Barbe RP, Birmaher B, Pincus HA, Ren L, Brent DA Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA, 2007.PMID 17440145
- [8]Walter HJ, Bukstein OG, Abright AR, Keable H, Ramtekkar U, Ripperger-Suhler J, Rockhill C, Stock S, Python NV, Wolraich M Clinical Practice Guideline for the Assessment and Treatment of Children and Adolescents With Anxiety Disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 2020.PMID 32439401
- [9]Holt MK, Vivolo-Kantor AM, Polanin JR, Holland KM, DeGue S, Matjasko JL, Wolfe M, Reid G Bullying and suicidal ideation and behaviors: a meta-analysis. Pediatrics, 2015.PMID 25560447
- [10]Moore SE, Norman RE, Suetani S, Thomas HJ, Sly PD, Scott JG Consequences of bullying victimization in childhood and adolescence: A systematic review and meta-analysis. World Journal of Psychiatry, 2017.PMID 28401049
- [11]Klomek AB, Kleinman M, Altschuler E, Marrocco F, Amakawa L, Gould MS Suicidal adolescents' experiences with bullying perpetration and victimization during high school as risk factors for later depression and suicidality. Journal of Adolescent Health, 2013.PMID 23790199
- [12]Fraguas D, Díaz-Caneja CM, Ayora M, Hernández-Álvarez F, Rodríguez-Quiroga A, Recio S, Álvarez-Solano I, Galaro JC, Tabar-Seisdedos R, Arango C Assessment of School Anti-Bullying Interventions: A Meta-analysis of Randomized Clinical Trials. JAMA Pediatrics, 2021.PMID 33136156