Paeds · adolescent-and-young-adult-medicine
Sexual orientation, identity and inclusive care
Also known as Inclusive care for sexual minority youth · LGBTQ+ adolescent care · Affirming paediatric care · Sexual orientation history-taking in adolescents · Minority stress in young people · SOGI data collection in paediatrics · Affirming clinical environment
Fellowship-level approach to sexual orientation, identity and inclusive care for adolescents: distinguishing sexual orientation from gender identity, expression and sex assigned at birth; the three components of orientation (attraction, behaviour, identity); the minority-stress model and why sexual minority youth carry excess depression, anxiety, suicidality and substance-use burden; affirming history-taking (HEEADSSS sexuality module), SOGI data collection and documentation; building an affirming environment and confidentiality; acute risk management (suicidality, family rejection, disclosure crisis); family acceptance; the harms of sexual orientation and gender identity change efforts; and care for Aboriginal and Torres Strait Islander, Maori, culturally diverse, rural, out-of-home-care and neurodiverse sexual minority youth.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A fifteen-year-old sits in your consulting room with her mother for a "check-up." The mother does most of the talking. Once you ask the mother to wait outside, the young person tells you she has a girlfriend, that she has been called slurs at school for months, and that she has thought about killing herself. What you do in the next twenty minutes — what you ask, how you ask it, what you keep private, and what you connect her to — is the whole of this topic. An affirming clinician in that moment is not being polite. They are delivering a protective intervention. [1] [8]
Sexual orientation is a person's pattern of emotional, romantic and sexual attraction to others. Inclusive care is care that actively welcomes and affirms sexual diversity and works to dismantle the health disparities that stigma creates. The two ideas belong together, because the disparities faced by sexual minority youth are not caused by who they are attracted to — they are caused by how they are treated for it. Grasp that single point and the rest of the topic falls into place. [1] [3]
The clinician's job is not to diagnose or "confirm" an orientation. It is to build an environment safe enough that a young person can disclose what is relevant, to screen for the consequences of stigma, to treat what you find, to protect confidentiality, and to broker acceptance and connection. Nothing here changes who the young person is. Everything here changes how much harm stigma is allowed to do to them. [8] [9]
Classification
Before you can take a history you have to be clear about what you are asking, because the vocabulary is routinely muddled. Sex assigned at birth is the label given at delivery. Gender identity is a person's internal sense of their own gender. Gender expression is how a person presents to the world. Sexual orientation is who a person is attracted to. These are four different axes, and collapsing any two of them is the single most common error clinicians make. A person's gender identity tells you nothing reliable about their sexual orientation, and vice versa. [2] [8]
Within sexual orientation itself, the useful frame is that orientation has three components, and they often do not align. Attraction is who you are drawn to — emotional, romantic and sexual. Behaviour is who you are actually sexually active with, which may be constrained by opportunity, safety or stage of life. Identity is the word you use for yourself — lesbian, gay, bisexual, queer, pansexual, asexual, questioning, or something else. Asking only one of these three produces wrong care: a young woman who identifies as bisexual but has only had male partners still needs pregnancy-prevention counselling and an affirming environment; a young man with male partners who calls himself heterosexual still needs behaviour-based screening. [2] [4]
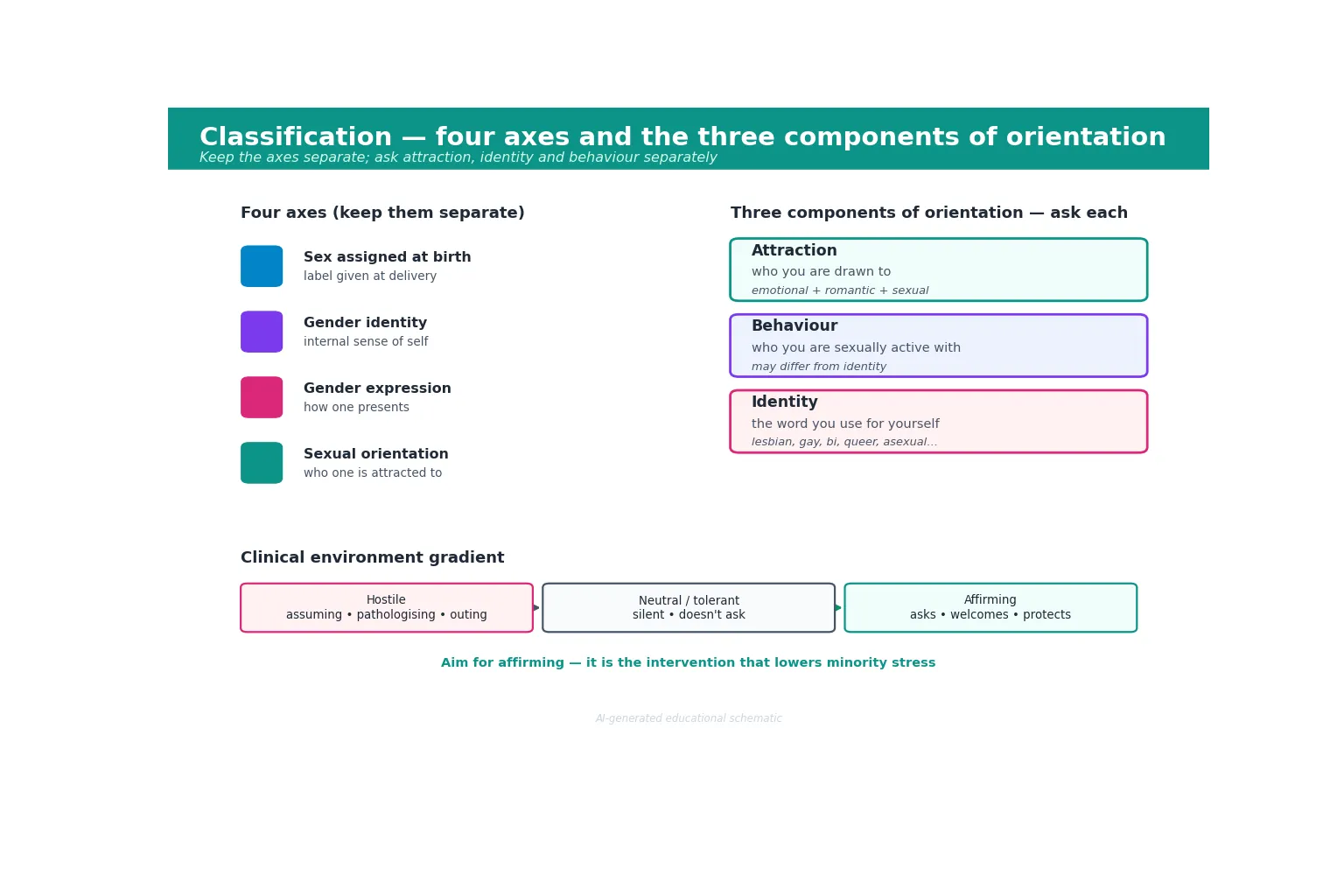
Finally, classify the clinical environment itself, because where you sit on this gradient changes everything downstream. A hostile environment assumes, pathologises or outs. A neutral or tolerant environment is silent and never asks, so it forces the young person to carry all the risk of disclosure. An affirming environment asks well, welcomes diversity, and protects confidentiality — and it is the only one of the three that measurably lowers minority stress. [4] [9]
| Axis | What it is | Common error to avoid |
|---|---|---|
| Sex assigned at birth | Label given at delivery | Assuming it predicts orientation |
| Gender identity | Internal sense of one's own gender | Conflating it with orientation |
| Gender expression | How one presents to the world | Reading expression as orientation |
| Sexual orientation | Pattern of attraction to others | Treating it as one indivisible thing |
Epidemiology & Risk Factors
A sizeable and growing minority of adolescents identify as something other than heterosexual, and population-level data has made the health gap visible. The clearest finding is that sexual minority youth carry higher rates of depression, anxiety, self-harm, suicidal ideation, substance use and care avoidance than their heterosexual peers — and that suicide ideation and behaviour begin earlier in this group. These are not small differences, and they are the reason this topic is high-yield and high-stakes. [2] [6]
The risk factors are overwhelmingly social, not intrinsic. Rejection by family, bullying and peer victimisation, an unsafe school environment, lack of an accepting adult, rural or cultural isolation, and exposure to change efforts each add load to the same stress system. Intersectionality matters: a young person who is also navigating racism, ableism, faith-based condemnation or poverty carries compounded stress, and the disparities are largest exactly where support is thinnest. [7] [9]
Pathophysiology
There is no disease of being queer. The pathophysiology here is the body and mind reacting to chronic, identity-based social stress — a mechanism Ilan Meyer set out as the minority stress model and that decades of data have since supported. Understanding the cascade tells you exactly why inclusive care works and where to intervene. [1] [3]
The stress splits into two layers. Distal stressors are external and happen to the young person: prejudice events, bullying, discrimination, family rejection, violence. Proximal stressors are internal and grow within them: internalised stigma (believing the hostile messages), expectation of rejection (bracing for it everywhere), and concealment (the exhausting work of hiding). A young person can carry heavy proximal stress even when nothing visibly bad is happening, because hypervigilance is itself corrosive. [1] [3]
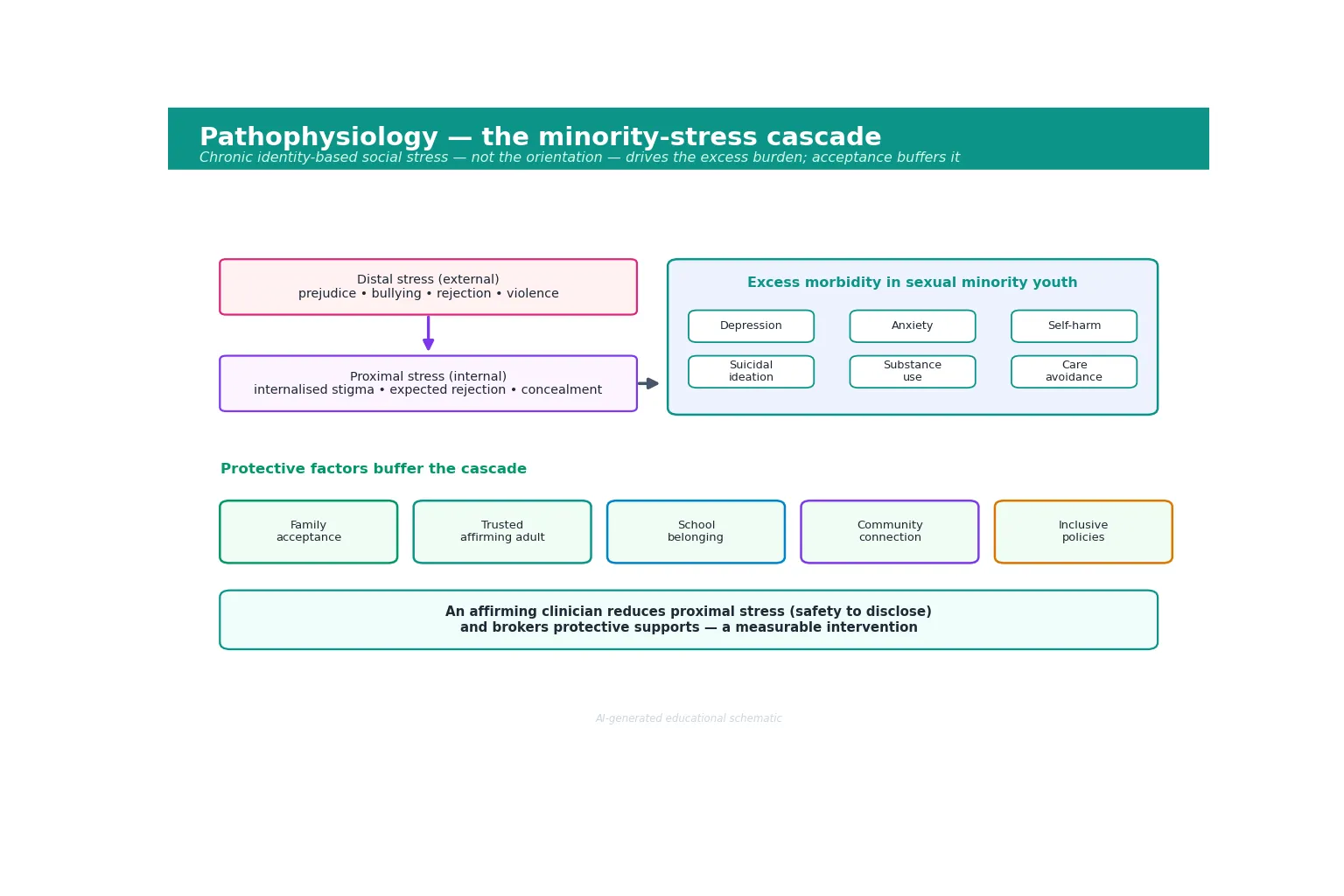
The cascade then converts stress into the morbidity you see in clinic. Chronic activation of threat systems drives low mood, anxiety, sleep disturbance, dysphoria and maladaptive coping such as substance use or self-harm. Crucially, the same model explains recovery: acceptance, visibility, community, pride and a safe clinical relationship each buffer the pathway, and an affirming clinician lowers proximal stress simply by making disclosure safe. That is why a single, well-asked question can be protective — it tells the nervous system this room is not a threat. [3] [7]
Clinical Presentation
Sexual minority youth present to paediatric services in two registers, and you have to recognise both. The first is the direct presentation: a young person discloses an orientation, asks a question about identity, or raises concern about bullying, family reaction or a relationship. The second is indirect and far more common — the orientation is invisible, and what you see are the downstream effects: depression, anxiety, self-harm, suicidal ideation, substance use, disordered eating, school refusal, or avoidance of care altogether. [2] [8]
The high-yield presentations of distress worth holding in mind are these. A young person who avoids the doctor, delays presenting, or withholds any sexuality-relevant history. A teenager with new depression or self-harm in whom no one has asked about attraction or victimisation. A "crisis of disclosure" — being outed, or feeling pressure to come out before they are ready. Pregnancy or STI risk mis-framed because behaviour was assumed rather than asked. And the most dangerous: acute suicidal ideation after bullying, family rejection, or exposure to change efforts. [6] [9]
The trap is to wait for the young person to volunteer their orientation before you start asking. Most will not, in a clinical environment that has not signalled safety. So treat the environment itself as the first presentation you must manage: if your forms, language and body language have not announced that this is a safe room, the relevant history stays hidden and you will manage only the fallout. [4] [8]
Differential Diagnosis
When a sexual minority young person presents with distress, the first job is to work out what is driving it, because the management differs entirely. Resist the reflex to attribute everything to "being LGBTQ+". Several contributors often overlap, and untangling them changes the plan. [3] [9]
| Surface picture | Likely dominant driver | What changes in the plan |
|---|---|---|
| Low mood, withdrawal, self-blame | Cumulative minority stress + possible comorbid depression | Affirmation, connection, screen and treat mood, safety plan |
| Distress spikes at school | Peer bullying or victimisation | Safety planning, school advocacy, involve counsellor |
| Distress worst at home | Family rejection or conflict | Family-engagement work, assess home safety, supports |
| Dysphoria, body unease | Undisclosed gender dysphoria (a separate axis) | Screen gender identity; see the gender-affirming-care topic |
| Substance use escalating | Self-medication for stress vs primary use disorder | Motivational work, treat use disorder, reduce stress load |
| Acute distress after "therapy" | Past or current change efforts | Explicitly affirm, name the harm, safeguard, refer |
Distinguish a situational crisis — a disclosure gone wrong, being outed, an acute bullying episode — from chronic minority stress that has ground the young person down over years. The first needs immediate containment and a safety plan; the second needs sustained affirmation, connection and treatment of entrenched mood disorder. Both can coexist, and both can present as the same flat affect in your consulting room. [1] [7]
Clinical & Bedside Assessment
The encounter starts before you ask a single question. Establish who is in the room, what is and is not shared with parents, and that there is a private space for a one-to-one conversation. Confidentiality is not a courtesy here — it is the precondition for an honest history, because a young person who fears you will tell their parents will simply not tell you. Explain the limits of confidentiality up front, in plain language, before you get anywhere near sexuality. [4] [8]
Use the young person's name and pronouns, and ask rather than assume. Then take the HEEADSSS sexuality module properly — which means asking attraction, identity and behaviour as three separate questions rather than one. A reliable, low-key sequence is: "Are you attracted to guys, girls, both, or neither?" then "What word, if any, do you use for yourself?" then "Have you been sexually active, and with partners of what gender?". Each answer drives different care, so do not let one stand in for another. [2] [8]
Screen routinely and without fanfare for the consequences of stigma. Use a validated adolescent depression screen such as the PHQ-A, ask directly about anxiety and suicide, and ask about safety — bullying, the family's reaction, whether home and school feel safe, and any intimate partner or sexual violence. Balance the risk questions with protective-factor questions: is there an adult who knows and accepts them, a peer group or community where they belong, a school that is inclusive? The protective factors tell you where to build. [6] [9]
Minimum affirming assessment: [4] [8]
- Establish confidentiality and its limits before the history. [8]
- Use the young person's name and pronouns; do not assume orientation. [2]
- Ask attraction, identity and behaviour separately. [2]
- Screen mood (PHQ-A), anxiety, suicide risk and substance use. [6]
- Ask about safety: bullying, family reaction, home, school, violence. [9]
- Ask about protective factors: an accepting adult, belonging, community. [3]
Investigations
You do not order blood tests to confirm an orientation. The "investigations" in inclusive care are the structured tools that make risk visible and the documentation that makes the young person count in the system. [2] [4]
Mental-health screening is central. The PHQ-A screens for adolescent depression; the GAD-7 and SCARED screen anxiety; and any positive screen, any disclosure of self-harm, or any mention of suicide demands a structured suicide-risk assessment — not a passing question. Screen for substance use with a validated adolescent tool. These are the instruments that convert "she seems a bit flat" into a defensible, documented risk picture. [6] [9]
Screen for sexually transmitted infections on the basis of behaviour and anatomy, never assumed orientation. A young man who has sex with men needs STI screening that includes pharyngeal and rectal sites as appropriate; a young woman with male partners needs pregnancy-prevention counselling regardless of how she identifies. Collect and document sexual orientation and gender identity (SOGI) in the electronic health record using structured fields — this is how disparities become measurable, and it lets the system flag the right care. Patients, including adolescents, report high acceptability for being asked, provided it is done respectfully and with control over disclosure. [4] [2]
Management — Resuscitation
Some disclosures carry immediate danger, and in those moments you manage safety first and inclusivity second — exactly as you would in any resuscitation. Acute suicidal ideation is a medical emergency: complete a structured risk assessment, build a safety plan with the young person, reduce access to means, and escalate to crisis or mental-health services. Do not let the affirmation of identity substitute for the management of risk. [6] [3]
An acute disclosure crisis — being outed, or coming out to a family whose reaction makes home unsafe — can precipitate homelessness, self-harm or family violence. Your job is to separate the young person's immediate safety from the family's reaction: confirm where they will sleep tonight, whether they are safe there, and whether emergency accommodation or a child-protection response is needed. Throughout, hold confidentiality: do not involuntarily out a young person, and recognise that a breach can itself be the trigger for harm. [9] [5]
Management — Definitive & Stepwise
Once safety is secured, the definitive work is an inclusive-care bundle: build the environment, take the history well, screen accurately, protect confidentiality, build acceptance, and connect the young person to durable support. Run it as a sequence you can recite under viva pressure. [4] [8]
The inclusive-care bundle
Build an affirming environment — inclusive language, intake forms, signage, private space, trained staff
Establish and explain confidentiality and its limits before the history
Ask attraction, identity and behaviour separately, using the young person's words
Screen mood, suicide risk, safety, substance use and behaviour-based sexual health
Build family acceptance where it is safe — the strongest buffer a clinician can broker
Connect the young person to affirming peer, community and mental-health supports
Plan longitudinal follow-up, a safety plan for high-stress periods, and repeat screening
Family acceptance is the lever that matters most. Because the family is usually the largest single source of either stress or protection, working with the family — when the young person consents and when it is safe — changes outcomes more than anything else you do in the consulting room. Offer family education, correct misinformation, and connect parents to support organisations. Where acceptance grows, minority stress falls and the young person's trajectory moves toward their peers'. Where the family cannot or will not accept, shift effort to building an alternative accepting adult and to keeping the young person safe. [3] [7]

Document your plan in a way that is both clinically useful and protective. Record the history you took, the screens and their results, the safety plan, the supports connected, and the follow-up arranged — while respecting what the young person has agreed may be shared. Good documentation makes the care continuous across clinicians and makes the young person's needs visible to the system over time. [4] [9]
Specific Subtypes & Scenarios
The questioning or exploring adolescent. Many young people are mid-exploration and resist a label. Affirm the exploration, avoid premature closure, and make clear that not having a word yet is fine. The risk to manage is not the uncertainty — it is the stigma they may meet while uncertain. [2] [8]
The young person who is not "out." Concealment is a rational response to an unsafe environment, not a problem to be solved. Respect it, protect confidentiality absolutely, and help the young person plan any future disclosure on their own terms. Never push someone out before they are ready. [8] [9]
Bisexual and pansexual youth. These young people face "bisexual erasure" — the assumption that they are really gay or really straight, depending on their current partner — and the evidence shows erasure is not benign: bisexual youth often carry a higher mental-health burden than their exclusively same-attracted peers. Name their identity as they name it, and screen accordingly. [2] [9]
Asexual and ace-spectrum youth. Distinguish a sexual orientation (little or no sexual attraction) from anxiety, trauma or a medical cause; affirm the identity without pathologising it, and address any genuine distress on its own merits. A young person who is asexual is not broken and does not need fixing. [8]
Rural, remote, religious or conservative settings. Isolation amplifies minority stress: there may be no visible community, no affirming adult, and a real risk that disclosure travels fast. Lower the threshold for confidential telehealth, for safety planning, and for connecting the young person to online or distant affirming supports. [7] [9]
Out-of-home care and youth-justice populations. Sexual minority youth are over-represented in care and justice settings, carry high trauma loads, and have acute confidentiality needs. Screen sensitively, recognise that disclosure may carry specific risks in these systems, and advocate for placement and case planning that does not punish the orientation. [8] [9]
Survivors of sexual orientation and gender identity change efforts. Some young people have been subjected to "conversion practices" — by family, faith leaders or clinicians — which are associated with significant mental-health harm. Ask gently whether anyone has tried to change their orientation or identity, name the harm plainly, affirm the young person as they are, and link them to trauma-informed, affirming support. [5] [10]
Complications & Pitfalls
- Assuming orientation from appearance, behaviour, anatomy, relationship status or gender expression. [2] [8]
- Conflating sexual orientation with gender identity — two separate axes, often wrongly merged. [8]
- Bisexual erasure: assuming a same-sex partner means gay, or a different-sex partner means heterosexual. [2] [9]
- Breaching confidentiality by disclosing orientation without the young person's consent — an act that can trigger the crisis. [8] [6]
- Behaviour-blind screening: withholding pregnancy or STI care because of an orientation assumption. [2] [4]
- Sexual orientation and gender identity change efforts ("conversion practices") — harmful, condemned, and never to be offered or referred for. [5] [10]
- Curiosity-driven history-taking that is clinical neither in purpose nor in tone. [4] [8]
Prognosis & Disposition
With family acceptance, a trusted affirming adult, and connection to community, sexual minority youth move toward the outcomes of their peers. Without those, the minority-stress disparities persist and can worsen across adolescence as social demands and visibility increase. The prognosis, in other words, is largely socially determined — which is exactly why inclusive care is a clinical intervention rather than a gesture. [3] [7]
Disposition is longitudinal, not a single referral. Arrange affirming follow-up, connect the young person to peer and mental-health supports, give them a safety plan for predictable high-stress periods (a bullying flare, a family conflict, an anniversary), and repeat screening as their circumstances evolve. Connection to a trusted adult is the single most modifiable protective factor you can broker — find it, build it, and document it. [9] [6]
Special Populations
Aboriginal and Torres Strait Islander and Maori sexual minority youth. Many First Nations cultures hold long-standing frameworks for sexual and gender diversity that predate colonisation; imposed Western labels can sit awkwardly with these. Practise cultural safety alongside inclusive care, let the young person use the language that fits them, and recognise the compounded load of racism and colonisation alongside minority stress. [9]
Culturally and linguistically diverse, and migrant, refugee and asylum-seeker youth. The intersection of racism, faith-based stigma and minority stress is heavy, and disclosure may carry specific risks within family or community. Use interpreters appropriately, never use family members to interpret sexuality history, and weigh the safety of any disclosure carefully. [9] [8]
Rural and remote youth. Distance, visibility and the scarcity of affirming services amplify isolation. Lower the threshold for confidential telehealth, safety planning, and referral to distant or online supports. [7]
Out-of-home care and youth justice. High prevalence, high trauma load, and acute confidentiality needs — screen sensitively and advocate for case planning that does not punish the orientation. [8]
Disability and neurodivergence. The orientation of young people with disability or neurodivergence is often overlooked or presumed absent. Affirm their autonomy, ask the same questions, and guard against the assumption that disability precludes sexuality. [8]
Gender-diverse youth who are also sexual minority. These young people carry intersecting minority stress on two axes; manage orientation here and refer to the companion topic on gender-diversity and gender-affirming paediatric care for gender-related needs. [2] [8]
Evidence, Guidelines & Regional Differences
Practice anchors: Meyer's minority-stress model; Baams and colleagues on the mechanisms of risk for depression and suicidal ideation; Bradford and Mustanski on why population data is essential to see the disparities; Luk on the earlier age of suicide-ideation onset; and Cahill's "do ask, do tell" finding that patients — including adolescents — find routine SOGI data collection highly acceptable when done respectfully. [1] [3] [2] [6] [4]
On change efforts, the New Zealand work of Fenaughty and colleagues documented who suggests sexual orientation and gender identity change efforts to young people and the mental-health harms that follow, and Yu and colleagues have produced an interview tool to identify exposure to such efforts in queer youth — clinically useful because survivors rarely volunteer it. [5] [10]
The RACP positions LGBTQIA+ inclusive care within professional and cultural-safety obligations, and several Australian states and New Zealand have legislated against sexual orientation and gender identity change efforts. A GP Mental Health Treatment Plan and state-based services (for example Q-Life and the equivalent state youth services) support referral, and headspace offers youth-friendly, often telehealth-based, affirming mental-health care. [8]
Exam Pearls
AFFIRMS
Self-test: a young man with male partners calls himself heterosexual
This is common, and it is not for you to relabel him. His identity is his to name; his behaviour is what drives his clinical care. So affirm his identity, and offer behaviour-based screening and counselling — STI screening appropriate to the sites and acts involved, PrEP discussion where relevant, and the same attention to mental-health and safety screening you would give any sexual minority youth. The error is letting the identity label override the behaviour when you choose what care to offer. [2] [4]
References
- [1]Meyer IH Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological Bulletin, 2003.PMID 12956539
- [2]Bradford J, Mustanski B Health disparities among sexual minority youth: the value of population data. American Journal of Public Health, 2014.PMID 24328630
- [3]Baams L, Grossman AH, Russell ST Minority stress and mechanisms of risk for depression and suicidal ideation among lesbian, gay, and bisexual youth. Developmental Psychology, 2015.PMID 25751098
- [4]Cahill S, Singal R, Grasso C, King D, Mayer K, Baker K, Makadon H Do ask, do tell: high levels of acceptability by patients of routine collection of sexual orientation and gender identity data in four diverse American community health centers. PLoS One, 2014.PMID 25198577
- [5]Fenaughty J, Tan KK, Ker A, Craig J, Fisher C, Greaves L, Sutch S Sexual Orientation and Gender Identity Change Efforts for Young People in New Zealand: Demographics, Types of Suggesters, and Associations with Mental Health. Journal of Youth and Adolescence, 2023.PMID 36301377
- [6]Luk JW, Goldstein RB, Yu S, Rotheram-Borus MJ, Kuo SI, Striley CW, Cottler LB Sexual Minority Status and Age of Onset of Adolescent Suicide Ideation and Behavior. Pediatrics, 2021.PMID 34580171
- [7]Lea T, de Wit J, Reynolds R Minority stress in lesbian, gay, and bisexual young adults in Australia: associations with psychological distress, suicidality, and substance use. Archives of Sexual Behavior, 2014.PMID 24573397
- [8]Diana P, Esposito S LGBTQ+ Youth Health: An Unmet Need in Pediatrics. Children, 2022.PMID 35884011
- [9]Ream GL Minority Stress and Intersectionality in LGBTQIA+ Youth Mental Health Disparities. American Journal of Public Health, 2024.PMID 38662974
- [10]Yu L, Dalke K, Eckstrand K An Interview Tool for Identifying Sexual Orientation or Gender Identity and Expression Change Efforts in Queer Youth. Journal of the American Academy of Child and Adolescent Psychiatry, 2025.PMID 40912505