Paeds · adolescent-and-young-adult-medicine
Sexually transmitted infection screening and management
Also known as STI screening in adolescents · Sexually transmitted infection testing · Chlamydia and gonorrhoea screening · Adolescent sexual health screening · 5 P's sexual history · STI treatment in young people · Expedited partner therapy
A fellowship approach to confidential, youth-friendly STI care in adolescents: time alone and conditional confidentiality, the 5 P's sexual history, risk- and anatomy-based screening (universal CT/GC for sexually active females under 25, selective extragenital testing, syphilis/HIV by risk), syndrome recognition, guideline-based treatment with local-dose verification, partner services and expedited partner therapy, ~3-month rescreening, and prevention across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 16-year-old asks you for "the check." You order a urine test, pronounce her "clear," and move on. You never created private time, never asked about partners or coercion, and never sampled the rectal or pharyngeal sites her history would have revealed. Three months later she returns with pelvic inflammatory disease. The missed work was not a rare pathogen. It was an STI visit without a youth-friendly process. [19] [13]
Sexually transmitted infection (STI) screening means testing asymptomatic people whose age, anatomy, practices or exposures put them at risk. It is distinct from diagnostic testing, which is triggered by symptoms, signs or a known exposure. This distinction changes the conversation: screening is opportunistic prevention; diagnostic workup is clinical problem-solving. [1] [4]
STI management spans recognition, investigation, treatment, partner services, rescreening and prevention. For an adolescent, every step is mediated by confidentiality, capacity and access. The clinical skill is not memorising a regimen. It is running a confidential, non-judgemental encounter that surfaces the truth, samples the right sites, treats correctly and brings the young person back. [3] [19]
Core sequence of an adolescent STI encounter
Engage in private
Greet the young person first, set a joint agenda, create time alone, state conditional confidentiality.
5 P's history
Partners, Practices, Protection, Past STI, Pregnancy intention — plus a coercion check.
Risk-stratify and examine
Decide sites by anatomy and exposure; offer chaperoned exam or self-collection.
Screen or diagnose
NAAT by site, syphilis/HIV serology by risk, pregnancy test before treatment.
Treat + partner services
Guideline regimen, pregnancy-aware; expedited partner therapy where lawful.
Rescreen + prevent
Retest at ~3 months, layer condoms/HPV vaccine/PrEP/contraception, safety-net.
Classification
Classify the encounter by history framework, screening tier and anatomical site, because each determines the next test. [4]
The 5 P's sexual history
A brief, structured sexual history frames risk in under three minutes. The 5 P's are Partners, Practices, Protection, Past history and Pregnancy intention. Ask each directly, then follow the positive answers. [3] [4]
| Domain | Example opening question | What it decides |
|---|---|---|
| Partners | "In the last year, how many partners — any new ones? Men, women, or both?" | Screening tier, partner services |
| Practices | "What kinds of sex — vaginal, oral, anal?" | Which anatomical sites to sample |
| Protection | "How often do you use condoms or barriers?" | Risk, PrEP/contraception counselling |
| Past history | "Any previous STI, and when were you last tested?" | Rescreening cadence, reinfection risk |
| Pregnancy intention | "Are you trying to avoid pregnancy now?" | Contraception, pregnancy test before treatment |
Screening tiers
Risk drives the testing strategy. Universal screening applies to broad groups by age and activity; selective screening adds higher-risk groups; diagnostic testing is for symptoms, signs or a known contact. [1] [5]
- Universal: sexually active females under 25 for chlamydia and gonorrhoea; HIV at least once; syphilis by local risk profile. [1]
- Selective / risk-based: young men who have sex with men, transgender and gender-diverse youth, anonymous or multiple partners, prior STI, pregnancy, and youth in detention or out-of-home care. [14] [13]
- Symptomatic / diagnostic: discharge, dysuria, pelvic pain, genital ulcer or rash move you from screening to syndrome-led workup. [3] [16]
Confidentiality classification
Conditional confidentiality means: what you say stays private unless I am worried you are unsafe, someone else is being hurt, or the law requires me to act. That honest frame lets a young person disclose sexual activity, coercion and risk behaviour. Absolute secrecy you cannot keep is a trust injury waiting to happen. [19] [4]
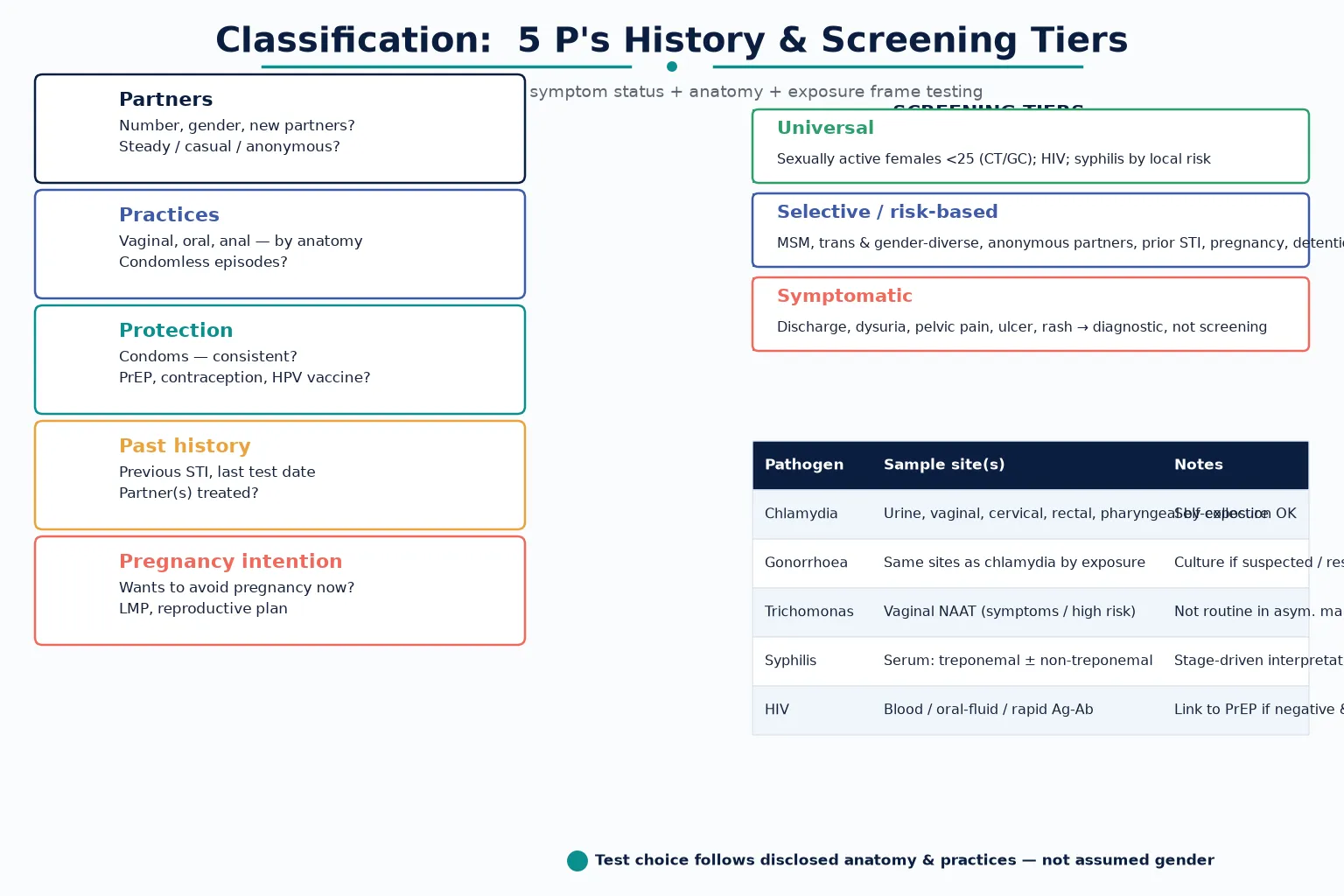
Read the figure like this: if you only sent a urine sample and never asked about anal or oral practices, you may have missed the infection that matters. Test by exposure, not by gender. [14]
Screening
Asymptomatic
- Risk-based detection
- Universal CT/GC <25 females
- Syphilis/HIV by risk
- Self-collection welcome
Diagnostic
Symptomatic/exposure
- Syndrome-led workup
- Cervicitis / urethritis / PID / ulcer
- Add culture for resistance
- Pregnancy test before treatment
Rescreening
After treatment
- Retest at ~3 months
- Reinfection, not relapse
- Partner treatment is assumed incomplete
- Test-of-cure only if indicated
Epidemiology & Risk Factors
Adolescents and young adults carry the highest STI burden of any age group. Chlamydia, gonorrhoea and syphilis have risen globally in this cohort over the past decade, with marked disparities by gender, sexuality, race and geography. [13] [20]
The drivers are biological and behavioural. Adolescent females have cervical ectopy, which exposes columnar epithelium and increases susceptibility to chlamydia and gonorrhoea. Behaviourally, condom use is inconsistent, partner networks are dense, and partner notification is often incomplete. [16] [13]
A prior STI predicts a new one. In the year after a diagnosed STI, the incidence of further infection is high, which is the evidence base for routine rescreening around three months after treatment. Reinfection usually reflects an untreated partner, not treatment failure. [18]
Gonococcal antimicrobial resistance is a worsening global threat. Cephalosporin susceptibility is falling, which makes correct first-line therapy, culture for surveillance, and partner treatment more important than ever. [20]
Access barriers suppress the whole cascade. Confidentiality fears, cost, transport, stigma, judgemental staff and the absence of private time in clinic keep young people away from testing and away from return visits. Youth-friendly, confidential services measurably increase testing and treatment uptake. [19]
Pathophysiology
Most adolescent STIs are silent at the mucosa. Chlamydia and gonorrhoea infect cervical, urethral, rectal and pharyngeal columnar epithelium and frequently cause no symptoms. Asymptomatic infection is the engine of onward transmission and of late sequelae. [2] [20]
The dangerous downstream event is ascending infection. Cervicitis can climb to endometritis and salpingitis, producing pelvic inflammatory disease (PID). Tubal inflammation scars the fallopian tubes and raises the lifetime risks of infertility, chronic pelvic pain and ectopic pregnancy. Prompt treatment of chlamydia and gonorrhoea is, in effect, fertility preservation. [16]
Cervical ectopy is why adolescent females are more susceptible than older women. The exposed columnar epithelium is a ready target for chlamydia and gonorrhoea, which is one biological reason the universal screening age band exists. [16]
Neisseria gonorrhoeae acquires resistance determinants readily. Reduced cephalosporin susceptibility is a global concern and shapes treatment and surveillance strategy. [20]
Treponema pallidum progresses in stages — primary chancre, secondary rash, latent seropositivity, and tertiary or neurosyphilis — with serological correlates that drive both diagnosis and the choice of regimen. Ulcerative STIs (syphilis, herpes) also amplify HIV acquisition and transmission through mucosal disruption. [5] [6]
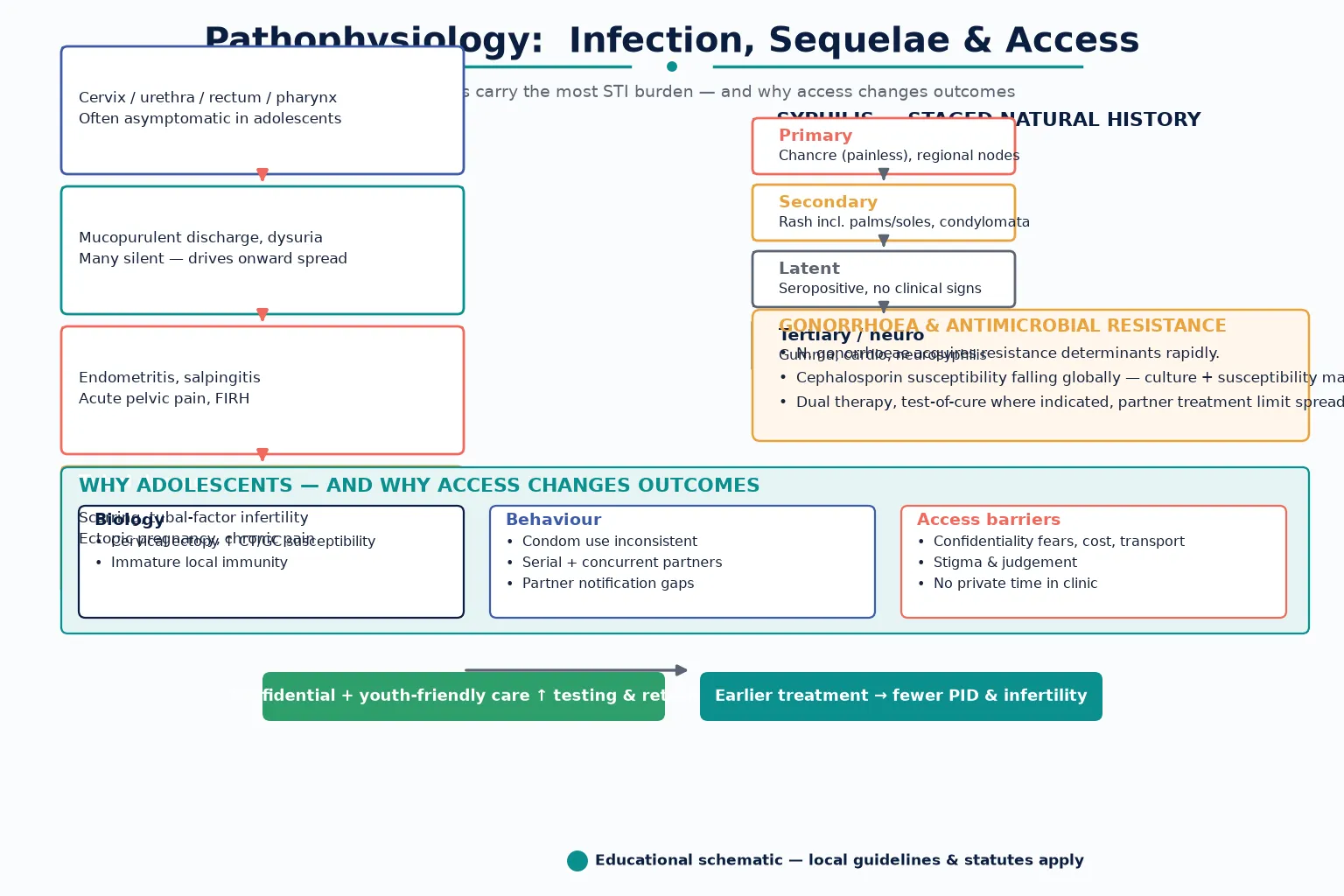
Read the figure like this: the cascade from silent infection to infertility is preventable, and access sits upstream of all of it. Confidential, youth-friendly care changes biology by changing behaviour and timing. [19] [16]
Clinical Presentation
The cardinal presentation of an adolescent STI is no presentation at all. Most chlamydial and gonococcal infections are asymptomatic, which is why screening exists and why waiting for symptoms fails. [1] [2]
Urethritis and cervicitis present with urethral or vaginal discharge, dysuria and post-coital bleeding. Many cases are silent, and the young person often attributes symptoms to a "urine infection" or thrush. [3]
Pelvic inflammatory disease presents with lower abdominal pain, deep dyspareunia, cervical motion tenderness, adnexal tenderness and sometimes fever. Severe disease with systemic toxicity, rigors, peritoneal signs or haemodynamic instability is a same-day emergency. [16]
Genital ulcers raise a focused differential. A painless indurated chancre points to primary syphilis; painful grouped vesicles that ulcerate point to herpes simplex. Less common causes (chancroid, donovanosis) depend on epidemiology. [3]
Proctitis presents with rectal pain, discharge or bleeding in a young person with anal exposure. It is missed if the practice question is never asked. Epididymitis presents with unilateral testicular pain and swelling; the trap is missing testicular torsion, which is surgical. [14] [3]
Secondary syphilis presents weeks later with a diffuse rash that classically involves the palms and soles, mucous patches, condyloma latum and lymphadenopathy. A young person with an unexplained rash may have an STI. [5]
Safeguarding presentations run alongside STIs. Coercion, an age-discordant partner, trafficking indicators or non-consensual contact may surface as a request for testing, emergency contraception or simply as fear. Ask about consent quietly and without judgement. [19]
Differential Diagnosis
Frame the differential by syndrome, and always exclude the surgical and pregnancy emergencies first. [3] [16]
| Syndrome | Distinguish from | Do not miss |
|---|---|---|
| Cervicitis / urethritis | UTI, candidiasis, bacterial vaginosis, physiologic discharge | Pregnancy before treatment; PID |
| Pelvic inflammatory disease | Appendicitis, ectopic pregnancy, ovarian torsion, endometriosis | Ectopic pregnancy, severe PID/FIRH |
| Genital ulcer | Syphilis, HSV, fixed drug eruption, trauma | HIV co-infection; syphilis staging |
| Epididymitis | Testicular torsion | Torsion (surgical emergency) |
| Proctitis | Inflammatory bowel disease, anal fissure, haemorrhoids | Gonococcal/LGV proctitis in MSM |
In any adolescent with abdominal pain or abnormal bleeding, exclude pregnancy before attributing the picture to an STI. A urine pregnancy test is fast, cheap and decisive, and it changes both the differential and the treatment. [3]
Separate reinfection from treatment failure. A positive test soon after treatment usually means an untreated partner rather than resistant organism, which is why rescreening and partner services travel together. [18]
Discordant syphilis serology needs careful reading. A treponemal-positive, non-treponemal-negative pattern can represent treated past infection, early primary syphilis before seroconversion, or a false positive. Stage clinically and repeat if uncertain. [5] [6]
Clinical & Bedside Assessment
1. Open and create private time
Introduce yourself to the young person first. Set a joint agenda with whoever has come, then ask the parent or companion to step out. Normalise private time: this is standard adolescent care, not suspicion of wrongdoing. [19]
2. State conditional confidentiality
Say the limits aloud: "What we discuss privately stays private, unless I am worried you are not safe, someone else is being hurt, or the law requires me to act. If that happens, I will tell you what I need to do." Check understanding before you start. [19] [4]
3. Take the 5 P's history
Work through Partners, Practices, Protection, Past history and Pregnancy intention with open then focused questions. Use inclusive, non-judgemental language. Do not assume gender, anatomy or partner gender. [3] [4]
4. Ask about coercion
A single respectful question — "Have any of your sexual experiences been unwanted, or have you ever felt pressured?" — opens the safeguarding pathway when needed. Ask it quietly and take the answer seriously. [19]
5. Examine by indication, offer self-collection
Offer a chaperoned examination when symptoms or signs are present. For asymptomatic screening, self-collected vaginal, urine, pharyngeal and rectal samples are acceptable and often preferred by adolescents, improving uptake. [1] [4]
6. Assess severity at the bedside
In suspected PID, check vital signs, perform an abdominal and (with consent) speculum and bimanual examination, and look for features in serious illness (FIRH): fever, rigors, peritoneal signs, vomiting, haemodynamic instability. Send a pregnancy test. Severe disease needs same-day inpatient parenteral therapy. [16]
7. Document with care
Record enough for safety and continuity while protecting sensitive detail from portal and billing disclosure. Note the sites sampled, results, treatment, partner plan and follow-up. Local record and portal rules govern how confidential content is stored and shared. [4] [19]
Investigations
Investigations are site- and risk-led, not panel-led. Choose tests from the sexual history and examination, not from a fixed "STI screen" habit. [3]
Nucleic acid amplification tests (NAATs) are the backbone for chlamydia and gonorrhoea. Sample by disclosed exposure: urine and vaginal/cervical for vaginal practices, and add pharyngeal and rectal sites when oral or anal exposure is reported. Self-collection is acceptable for most sites. [1] [14]
Extragenital testing matters because urogenital-only sampling misses infection. Rectal and pharyngeal gonorrhoea and chlamydia are common in men who have sex with men and in others with relevant exposure, and they are invisible to a urine test alone. [14]
Syphilis serology pairs a treponemal test (EIA or CIA) with a non-treponemal test (RPR or VDRL). Interpret the titre alongside the clinical stage to decide treatment and to monitor response. [5] [6]
HIV testing (fourth-generation antigen/antibody or rapid test) belongs in the panel for sexually active adolescents and is mandatory when an STI is diagnosed. A negative HIV test is the entry point to a PrEP conversation for those at ongoing risk. [7]
Trichomonas NAAT is indicated in symptomatic or high-risk females and is not routine in asymptomatic males. Mycoplasma genitalium NAAT is reserved for persistent or recurrent urethritis and cervicitis, with resistance-guided therapy when positive. [3]
Pregnancy testing is mandatory before treatment in any female adolescent. Doxycycline is contraindicated in pregnancy, and syphilis treatment differs by pregnancy status. A single urine hCG prevents teratogenic error. [3]
Culture gonorrhoea when you suspect resistance, when treating extragenital disease, on treatment failure, and for public-health surveillance, because NAAT cannot report susceptibility. [20]
Rescreen at about three months, not test-of-cure, after uncomplicated chlamydia or gonorrhoea. Reserve test-of-cure for pregnancy, suspected treatment failure or resistance, or when symptoms persist. [18]
Management — Resuscitation
Most STI visits are routine, but a handful become emergencies in a single sentence of history or one abnormal vital sign. [16]
- Stabilise physiology first: ABCDE, fluid resuscitation, analgesia and antipyretics in severe PID with sepsis or peritoneal signs. [16]
- Exclude surgical emergencies: testicular torsion masquerading as epididymitis needs urgent ultrasound and surgical review, not antibiotics. Ectopic pregnancy must be excluded before attributing pelvic pain to PID. [3]
- Treat severe PID inpatient with parenteral therapy, obstetric or gynaecology liaison, and close monitoring. Pregnancy, intolerance, non-adherence risk or diagnostic uncertainty all push toward admission. [16]
- Manage pregnancy with an STI with pregnancy-specific regimens: replace doxycycline, stage and treat syphilis to prevent congenital infection, and break confidentiality as required for safety. [3]
- Activate safeguarding for coercion, trafficking or non-consensual contact, parallel to medical care and following local mandatory-reporting law. [19]
- Link newly diagnosed HIV urgently to confirmatory testing, specialist care, partner notification and PEP/PrEP pathways. [7]
Document the decisions, who was informed, and the safety plan after any urgent escalation or confidentiality override. [4] [19]
Management — Definitive & Stepwise
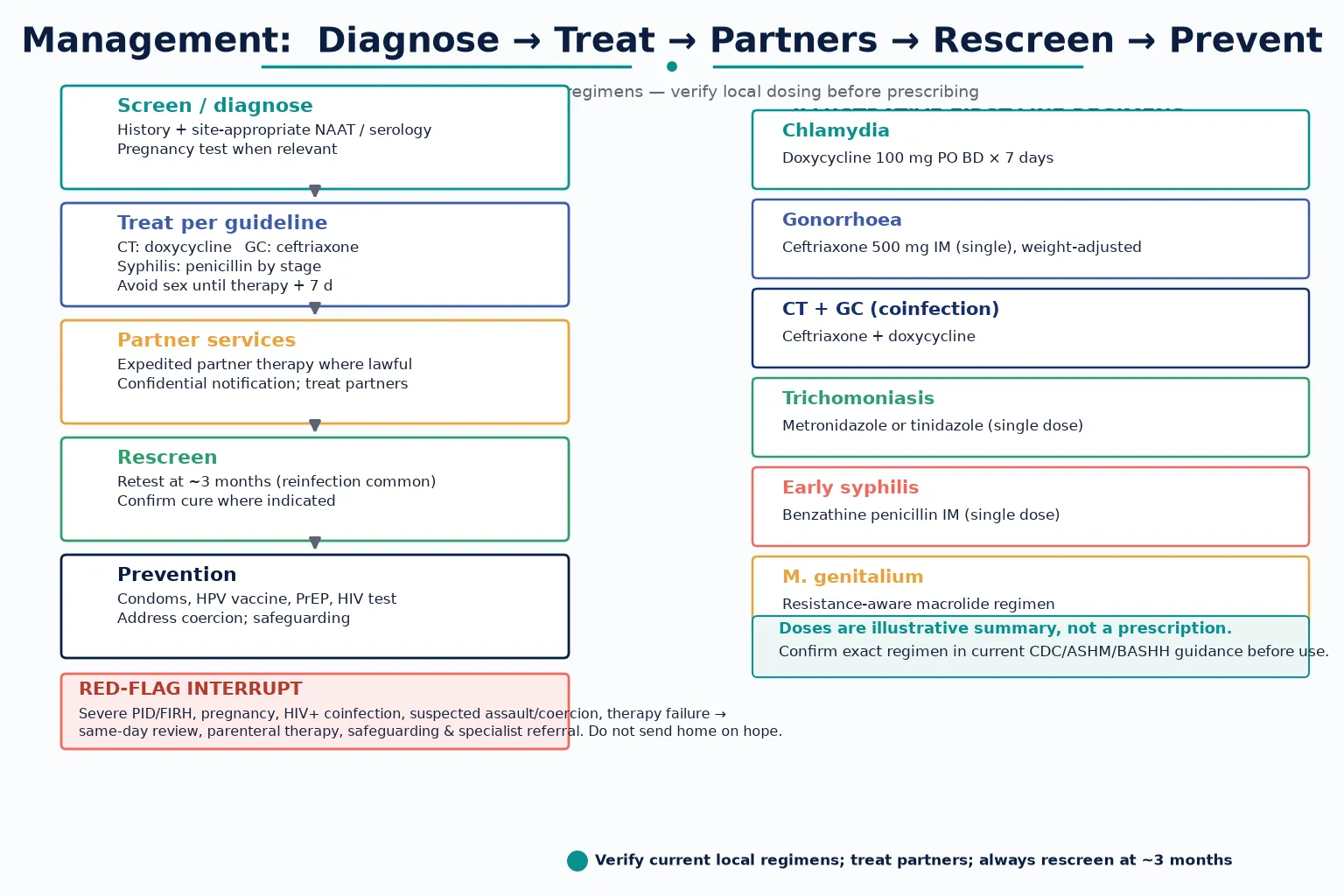
Read the figure like this: the red diamond is not decoration. Severe PID, pregnancy, suspected coercion or treatment failure exits the routine path and goes to same-day escalation. [16]
Stepwise routine pathway
- Confirm the diagnosis and stage by syndrome and site. Pregnancy-test any female adolescent before therapy. [3]
- Treat per current guideline. For uncomplicated chlamydia the standard non-pregnant first line is doxycycline 100 mg by mouth twice daily for 7 days; gonorrhoea is treated with weight-adjusted ceftriaxone intramuscularly; coinfection combines both. Verify the exact current dose in your local guideline before prescribing. [3] [21]
- Treat syphilis by stage. Early syphilis receives single-dose benzathine penicillin; late or unknown-duration disease needs weekly doses for three weeks; pregnancy and neurosyphilis differ. Manage penicillin allergy per protocol. [5] [3]
- Counsel abstinence until therapy is completed plus seven days and until symptoms resolve. [3]
- Arrange partner services. Where lawful, expedited partner therapy delivers treatment to partners without a clinical visit and reduces reinfection. Where unlawful, use provider- or patient-referral notification. [10] [11] [17]
- Rescreen at about three months after treatment. Reinfection, not relapse, is the usual cause of a recurrent positive result. [18]
- Layer prevention. Promote consistent condom use, ensure HPV vaccination and catch-up, refer for HIV PrEP when at risk, address contraception, and check hepatitis B status. [7] [12]
- Co-create a confidential plan. Agree what the young person will do, what you will do, when to return, and how to get help after hours. [19]
Follow-up intensity
- Uncomplicated infection, treated correctly: rescreen at about three months and routine preventive review. [18]
- Pelvic inflammatory disease: clinical review at 48–72 hours and rescreen at about three months. [16]
- Severe PID, pregnancy, HIV coinfection or treatment failure: same-day escalation and close specialist follow-up. [3] [16]
Specific Subtypes & Scenarios
Sexually active 16-year-old female, asymptomatic. Offer universal chlamydia and gonorrhoea screening, HIV testing, and syphilis by risk. Self-collected vaginal swabs and urine are acceptable and improve uptake. Integrate contraception. [1] [19]
Young man who has sex with men. Screen at three anatomical sites (urine or urethral, pharyngeal, rectal), add syphilis and HIV, and discuss PrEP. Be alert to gonococcal resistance and the need for culture. [14] [7]
Transgender and gender-diverse youth. Test by anatomy and disclosed practices, not registered gender. Use chosen names and pronouns, and watch for minority stress, bullying and family rejection. [19]
Genital ulcer. Work up syphilis and herpes, consider empiric cover where indicated, and check HIV. Stage before treating syphilis. [3] [5]
Suspected pelvic inflammatory disease. Apply outpatient criteria carefully; admit those who are pregnant, systemically unwell, unable to tolerate oral therapy, or whose diagnosis is uncertain. Review at 48–72 hours. [16]
Pregnant adolescent with an STI. Use pregnancy-safe regimens, treat syphilis to prevent congenital infection, and coordinate with antenatal and public-health services. Confidentiality may need to be overridden for safety. [3]
Out-of-home care and youth justice. Assume higher prevalence, fragmented records and incomplete prior screening. Clarify capacity and consent, and reconstruct the history actively. [13] [19]
Self-collected and digital/e-testing pathways. Online and mail-in testing reach young people who avoid clinic settings and support 3-month rescreening, though partner-notification outcomes can differ from clinic care. [15]
Disclosure of coercion or assault. Switch to safeguarding-first care: a forensic pathway alongside STI management, specialist referral, and mandatory reporting per local statute. [19]
Rural, remote and telehealth. Create private audio space deliberately; if a companion is off-camera, ask. Self-collection and mailed samples extend access where clinic visits are hard. [19]
Complications & Pitfalls
- Sampling only urogenital sites in a young person with oral or anal exposure, missing extragenital infection. [14]
- Prescribing doxycycline to a pregnant adolescent because pregnancy testing was omitted. [3]
- Failing to arrange partner treatment, leading to prompt reinfection. [18] [11]
- Waiting for symptoms before testing, missing the asymptomatic majority. [1] [2]
- Promising absolute secrecy you cannot keep. [19]
- Portal and billing disclosure leaking confidential STI content to parents or carers. [4] [19]
- Treating syphilis without staging or pregnancy assessment. [5] [6]
- Missing testicular torsion while working up "epididymitis." [3]
- Using first-line gonococcal therapy without culture or surveillance as resistance rises. [20]
- Stigmatising language that suppresses return visits and onward prevention. [19]
Prognosis & Disposition
Prognosis in STI care means the trajectory of cure, reinfection and sequelae, not a tumour stage. [1]
Routine disposition: uncomplicated infection treated correctly, partner services arranged, rescreening booked at about three months, and a clear after-hours safety-net. [18]
Early-review disposition: pelvic inflammatory disease needs review at 48–72 hours to confirm clinical response; new disclosures or unstable social circumstances shorten the interval. [16]
Urgent disposition: severe PID or FIRH, pregnancy with an STI, suspected coercion or assault, and treatment failure or suspected resistance all need same-day escalation, safeguarding and specialist input. [16] [19]
Untreated chlamydia and gonorrhoea carry real long-term costs: PID, tubal-factor infertility, chronic pelvic pain and ectopic pregnancy. Prompt, correct treatment is fertility preservation. [16]
The outcomes that matter are cure, reinfection rate, partner-treatment coverage, rescreen completion, HIV/PrEP linkage and HPV vaccination. Plan ongoing preventive care with a screening cadence matched to risk. [7] [12] [18]
Special Populations
Sexually active adolescent females under 25. Universal chlamydia and gonorrhoea screening, pregnancy-aware treatment, contraception integration and a 3-month rescreen. [1]
Young men who have sex with men. Three-site NAAT, syphilis and HIV, PrEP discussion, and resistance-aware gonorrhoea management. [14] [7]
Transgender and gender-diverse youth. Anatomy-based testing, affirming language and vigilance for minority stress and family rejection. [19]
Pregnant adolescents. Pregnancy-safe regimens, congenital syphilis prevention and an integrated antenatal pathway. [3]
Out-of-home care and youth justice. High prevalence, fragmented records and consent complexity; reconstruct the history and screen generously. [13]
Migrant and refugee youth. Interpreter use (never family for confidential content), trauma-informed pacing, and catch-up screening and vaccination. [19]
Indigenous youth. Cultural safety, community-led services and screening cadence calibrated to local burden. [13]
Youth with disability or neurodiversity. Accessible communication, chaperoned examination and capacity assessment, with private time still pursued. [19]
Rural and remote youth. Telehealth with deliberate private space, and self-collection and mailed-sample pathways. [19]
Survivors of coercion or assault. Safeguarding-first care, a forensic pathway alongside STI management and specialist referral. [19]
Evidence, Guidelines & Regional Differences
USPSTF chlamydia and gonorrhoea screening (2021) recommends screening sexually active females aged 24 and younger, with the evidence base detailed in the accompanying systematic review. The recommendation highlights evidence gaps for males, men who have sex with men, and older adults, which is why selective screening fills those gaps. [1] [2]
USPSTF syphilis screening is reaffirmed for non-pregnant adolescents and adults at increased risk, building on the original 2016 recommendation. [5] [6]
USPSTF HIV pre-exposure prophylaxis (2023) carries a grade A recommendation for those at increased risk, including eligible adolescents, which makes PrEP referral a defined preventive service. [7]
CDC STI Treatment Guidelines (Workowski 2021) are the US treatment backbone, with the 2015 edition as the historical reference; always verify the current regimen and any updates before prescribing. [3] [21]
Extragenital NAAT screening evidence shows that urogenital-only testing misses rectal and pharyngeal infection in men who have sex with men and in others with relevant exposure, supporting site-based testing. [14]
Expedited partner therapy improves partner treatment and reduces reinfection where it is lawful, with practical prescription-delivery evidence from public-health settings; legality varies by jurisdiction. [10] [11] [17]
Doxycycline post-exposure prophylaxis (IPERGAY 2018; DOXYVAC 2024) reduces bacterial STIs in men who have sex with men. The evidence is selective and is not a universal adolescent recommendation; stewardship concerns persist. [8] [9]
Reinfection and rescreening. The high incidence of new STIs in the year following a diagnosed infection underpins routine rescreening at about three months. [18]
Pelvic inflammatory disease in adolescents. Adolescent-specific PID evidence frames why prompt, correct treatment protects fertility and why severe disease needs inpatient parenteral care. [16]
HPV vaccination. Adolescent vaccination trends improved through 2020, with catch-up remaining important; national schedules and one-dose policy positions vary. [12]
Gonorrhoea overview. The disease primer frames pathogenesis and the worsening cephalosporin-resistance picture that shapes surveillance and therapy. [20]
Digital and self-collection pathways. Online and mail-in STI testing expands access for youth and supports rescreening, with partner-notification outcomes that differ from clinic care. [15]
Adolescent-friendly services. A dedicated review frames how confidentiality, non-judgemental care, self-collection and youth-friendly settings raise adolescent STI testing and treatment rates. [19]
ANZ: ASHM Australian STI Management Guidelines for primary care, state-based notification statutes, and youth-health services emphasising confidential care; cervical screening commences at 25 under the renewed National Cervical Screening Program. UK: BASHH guidelines for chlamydia, gonorrhoea, syphilis and PID; the National Chlamydia Screening Programme context; Gillick/Fraser capacity concepts for adolescent consent — apply with current local legal teaching. US: CDC STI Treatment Guidelines, USPSTF screening and PrEP recommendations, state variability in expedited partner therapy legality, and open-notes/portal confidentiality challenges. Canada: Canadian Guidelines on Sexually Transmitted Infections, provincial consent and partner-notification variation, and online testing pathways such as GetCheckedOnline.
Exam Pearls
- Open every STI answer with time alone + conditional confidentiality + the 5 P's history. [19] [3]
- Screening is not diagnosis: universal CT/GC for sexually active females under 25; risk-based and extragenital for MSM, trans and gender-diverse youth and others by exposure. [1] [14]
- Test by disclosed anatomy and practices, not assumed gender — add pharyngeal and rectal NAAT when oral or anal exposure exists. [14]
- Always pregnancy-test a female adolescent before STI treatment; doxycycline is contraindicated in pregnancy. [3]
- PID: lower abdominal pain plus cervical motion or adnexal tenderness — treat promptly; severe disease or FIRH needs inpatient parenteral therapy. [16]
- Stage syphilis before treating; early syphilis is single-dose benzathine penicillin, with pregnancy and late disease differing. [5] [6]
- Rescreen at about three months (reinfection, not relapse); reserve test-of-cure for pregnancy, failure or resistance. [18]
- Treat partners: expedited partner therapy where lawful; provider or patient referral otherwise. [10] [17]
- Prevention stack: condoms + HPV vaccination and catch-up + HIV PrEP for those at risk + contraception + hepatitis B status. [7] [12]
- Red flags: severe PID/FIRH, pregnancy with an STI, suspected coercion or assault, a torsion mimic, treatment failure — escalate today, and verify the local dose from current guidelines. [16] [19]
SCREEN for adolescent STI care
References
- [1]US Preventive Services Task Force; Davidson KW; Barry MJ Screening for Chlamydia and Gonorrhea: US Preventive Services Task Force Recommendation Statement. JAMA, 2021.PMID 34519796
- [2]Cantor A; Dana T; Griffin JC Screening for Chlamydial and Gonococcal Infections: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA, 2021.PMID 34519797
- [3]Workowski KA; Bachmann LH; Chan PA Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep, 2021.PMID 34292926
- [4]Barrow RY; Ahmed F; Bolan GA Recommendations for Providing Quality Sexually Transmitted Diseases Clinical Services, 2020. MMWR Recomm Rep, 2020.PMID 31899459
- [5]US Preventive Services Task Force; Mangione CM; Barry MJ Screening for Syphilis Infection in Nonpregnant Adolescents and Adults: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA, 2022.PMID 36166020
- [6]US Preventive Services Task Force (USPSTF); Bibbins-Domingo K; Grossman DC Screening for Syphilis Infection in Nonpregnant Adults and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA, 2016.PMID 27272583
- [7]US Preventive Services Task Force; Barry MJ; Nicholson WK Preexposure Prophylaxis to Prevent Acquisition of HIV: US Preventive Services Task Force Recommendation Statement. JAMA, 2023.PMID 37606666
- [8]Molina JM; Charreau I; Chidiac C Post-exposure prophylaxis with doxycycline to prevent sexually transmitted infections in men who have sex with men: an open-label randomised substudy of the ANRS IPERGAY trial. Lancet Infect Dis, 2018.PMID 29229440
- [9]Molina JM; Bercot B; Assoumou L Doxycycline prophylaxis and meningococcal group B vaccine to prevent bacterial sexually transmitted infections in France (ANRS 174 DOXYVAC): a multicentre, open-label, randomised trial with a 2 x 2 factorial design. Lancet Infect Dis, 2024.PMID 38797183
- [10]Jamison CD; Coleman JS; Mmeje O Improving Women's Health and Combatting Sexually Transmitted Infections Through Expedited Partner Therapy. Obstet Gynecol, 2019.PMID 30741802
- [11]Oliver A; Rogers M; Schillinger JA The Impact of Prescriptions on Sex Partner Treatment Using Expedited Partner Therapy for Chlamydia trachomatis Infection, New York City, 2014-2015. Sex Transm Dis, 2016.PMID 27893595
- [12]Lu PJ; Yankey D; Fredua B Human Papillomavirus Vaccination Trends Among Adolescents: 2015 to 2020. Pediatrics, 2022.PMID 35730334
- [13]Boyer CB; Agenor M; Willoughby JF A Renewed Call to Action for Addressing the Alarming Rising Rates of Sexually Transmitted Infections in U.S. Adolescents and Young Adults. J Adolesc Health, 2021.PMID 34099391
- [14]Bamberger DM; Graham G; Dennis L Extragenital Gonorrhea and Chlamydia Among Men and Women According to Type of Sexual Exposure. Sex Transm Dis, 2019.PMID 30676485
- [15]Zamanpour A; Grennan T; Ablona A Treatment and Partner Notification Outcomes for Clients Diagnosed With Chlamydia and Gonorrhea Through GetCheckedOnline Compared With Sexually Transmitted Infection Clinics in British Columbia, Canada. Sex Transm Dis, 2023.PMID 36367543
- [16]Gray-Swain MR; Peipert JF Pelvic inflammatory disease in adolescents. Curr Opin Obstet Gynecol, 2006.PMID 16932044
- [17]Hogben M Partner notification for sexually transmitted diseases. Clin Infect Dis, 2007.PMID 17342669
- [18]Peterman TA; Tian LH; Metcalf CA High incidence of new sexually transmitted infections in the year following a sexually transmitted infection: a case for rescreening. Ann Intern Med, 2006.PMID 17043338
- [19]Friedman JC; Cannon B; Tyson N Providing adolescent-friendly sexually transmitted infection screening and treatment services. Curr Opin Obstet Gynecol, 2024.PMID 39109588
- [20]Unemo M; Seifert HS; Hook EW 3rd Gonorrhoea. Nat Rev Dis Primers, 2019.PMID 31754194
- [21]Workowski KA; Bolan GA; Centers for Disease Control and Prevention Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep, 2015.PMID 26042815