Paeds · adolescent-and-young-adult-medicine
Sleep, fatigue and circadian disorders in adolescents
Also known as Adolescent sleep problems · Delayed sleep-wake phase disorder in adolescents · Teenage insomnia · The tired teenager · Adolescent circadian rhythm disorder · Insufficient sleep in adolescents
A fellowship approach to sleep, fatigue and circadian disorders in adolescents: the biologically delayed sleep phase, the two-process model, the differential of the 'tired teenager' (insufficient sleep, insomnia, delayed sleep-wake phase disorder, central disorders of hypersomnolence, obstructive sleep apnoea, depression and medical fatigue), a sleep-history and sleep-diary assessment, and stepped-care management (sleep hygiene, CBT-I, timed light and melatonin) across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old is sent to the clinic because she "can't get up" and is falling asleep in morning classes. Her mother thinks she is depressed or lazy; the school thinks she is disengaged. Ask one question — what time does she actually fall asleep, and what time does she wake on a weekend when left alone — and the picture changes. On weeknights she is in bed by 23:00 but awake until 01:30; she rises at 06:45 for school, getting about five hours. On weekends she sleeps from 02:00 until 11:00, feeling well. The answer is not laziness. It is the single most common adolescent sleep pattern: a biologically delayed clock colliding with a socially fixed morning. [10] [1]
Sleep is the reversible state of reduced consciousness and motor activity the brain needs for memory consolidation, emotional regulation and metabolic recovery. Fatigue is a subjective lack of energy, and it is not the same as sleepiness, the tendency to fall asleep. The tired teenager sitting in front of you may be sleepy (a sleep problem), fatigued (a mood or medical problem), or both, and conflating the two is the commonest diagnostic error on this topic. [11]
The clinical task has three steps. First, name the dominant mechanism: insufficient sleep, insomnia, a circadian timing disorder, a central disorder of hypersomnolence, sleep-disordered breathing, or fatigue from another cause. Second, exclude the can't-miss mimics — narcolepsy, obstructive sleep apnoea, depression with self-harm risk. Third, match the management to the mechanism. The trap is reaching for a "sleeping tablet" before you know which problem you are treating. [10] [16]
[1] [8]Classification
Group adolescent sleep and fatigue presentations by their dominant mechanism, because the mechanism drives the treatment. A classification that lists diagnoses without naming the mechanism produces a "try everything" plan that fails. [10]
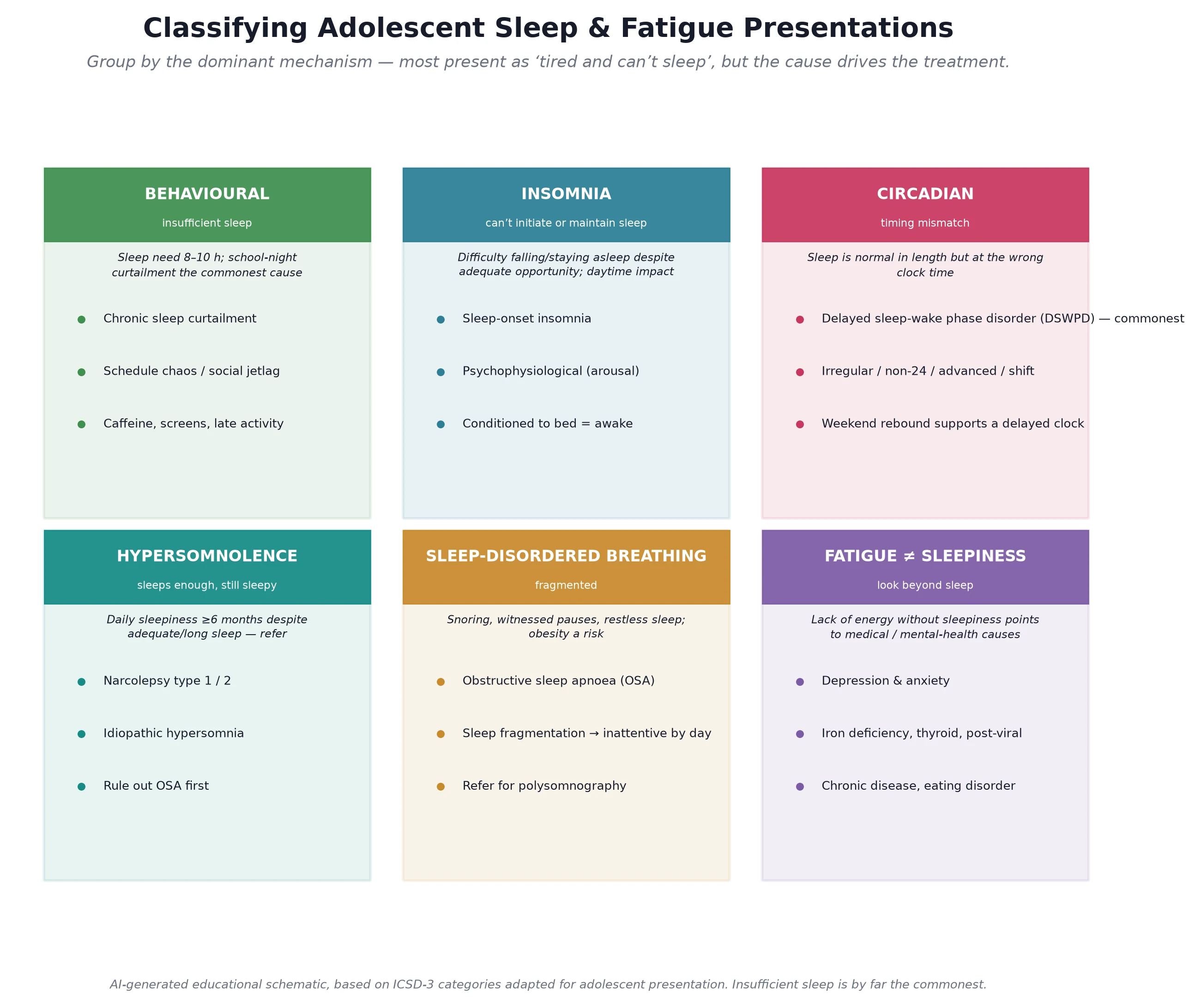
Read the figure like this: most teenagers you see sit in the first three boxes. The discipline is to confirm which one, because a teenager who sleeps only six hours because they are on their phone is managed very differently from one who has eight hours of opportunity but lies awake for two of them, or one who sleeps soundly from 02:00 to 10:00 whenever allowed. [9]
Insufficient sleep
Not enough opportunity
- In bed too late, up too early
- Normal ability to sleep when given the chance
- Weekday–weekend gap in rise time
- First-line: schedule, not sedation
Insomnia
Enough opportunity, cannot sleep
- Sleep latency over ~30 min or frequent waking
- Conditioned arousal: bed = awake
- Daytime fatigue more than true sleepiness
- First-line: CBT-I, not hypnotics
Delayed sleep-wake phase
Sleep at the wrong clock time
- Very late onset, cannot rise early
- Normal length and quality when allowed
- Marked weekend rebound
- First-line: light + melatonin phase advance
Hypersomnolence
Sleeps enough, still sleepy
- Daily irresistible sleep over 3 months
- Cataplexy = narcolepsy type 1
- Refer for MSLT
- Specialist pharmacotherapy
Key distinctions within the classification
The two distinctions examiners probe hardest are insufficient sleep versus insomnia and sleepiness versus fatigue. Insufficient sleep means the young person sleeps well when given the chance but rarely gets the chance — the fix is more opportunity, structured by a consistent schedule. Insomnia means the opportunity is there but the brain will not switch off, often because the bed has become a cue for wakefulness and worry — the fix is CBT-I, not more time in bed. Sleepiness is the tendency to doze in boring situations and points to a sleep problem; fatigue is low energy without dozing and points to mood or medical causes. [11]
Circadian and hypersomnolence subtypes
Within the circadian group, delayed sleep-wake phase disorder (DSWPD) dominates adolescence: sleep is normal in length and quality but starts and ends two or more hours later than socially desired, with marked weekend rebound. Rarer circadian patterns — irregular sleep-wake, non-24-hour, advanced, or shift-related — occur in specific contexts (neurodevelopmental disability, shift-working older adolescents, severe visual impairment). The central disorders of hypersomnolence — narcolepsy type 1 (with cataplexy, due to orexin deficiency), narcolepsy type 2, and idiopathic hypersomnia — are uncommon but devastating when missed, and they all share daily irresistible sleepiness despite adequate overnight sleep for at least three months. [16]
Epidemiology & Risk Factors
Adolescents need more sleep than they get. The American Academy of Sleep Medicine recommends 9 to 12 hours for 6- to 12-year-olds and 8 to 10 hours for 14- to 17-year-olds, a range endorsed by the National Sleep Foundation. The worldwide meta-analysis by Gradisar and colleagues showed that across regions most adolescents sleep less than this on school nights, with a consistent pattern of short weekday sleep and long weekend catch-up. [4] [5] [12]
The phase delay is driven by puberty rather than chronological age: a girl at Tanner stage 3 has a later dim-light melatonin onset than she did at stage 1, irrespective of her exact age. The biological changes are a longer intrinsic circadian period, a later evening rise of melatonin, and a slower build-up and dissipation of homeostatic sleep pressure across the day, all of which push the brain toward a later schedule. [8] [9]
The modifiable risk factors for insufficient sleep are the social and environmental ones the "perfect storm" names. Early school start is the single largest structural driver — a school day beginning at 08:00 forces a wake-time incompatible with a biologically delayed onset. Screens compound this: the Carter meta-analysis found that access to or use of a portable screen-based device around bedtime is associated with shorter sleep, poorer sleep quality and excessive daytime sleepiness, plausibly through blue-light suppression of melatonin and through the arousal of social content. Caffeine (including energy drinks), late-night homework, paid work, long commutes, and unstructured autonomy all add to the deficit. [3] [17]
Groups carrying the highest sleep risk include young people with depression and anxiety (the relationship is bidirectional), neurodiverse young people with autism or ADHD, those with chronic disease, obese adolescents at risk of obstructive sleep apnoea, out-of-home-care and trauma-exposed youth for whom sleep disturbance may be a sentinel of distress, and Indigenous, remote and rural young people whose long travel times collide hardest with early starts. [11] [12]
Pathophysiology
To explain adolescent sleep, hold two processes in mind at once. Process S is homeostatic sleep pressure: it builds up steadily from the moment you wake and dissipates while you sleep, so the longer you are awake the sleepier you become. Process C is the circadian alerting signal: a roughly 24-hour internal clock that sends a wake-promoting signal through the day and withdraws it at night. We fall asleep when rising Process S meets a falling circadian alerting signal, and we wake when the circadian signal reasserts itself even if Process S has not fully discharged. This is the Borbély two-process model, and it is the framework a fellowship candidate should hold. [8]
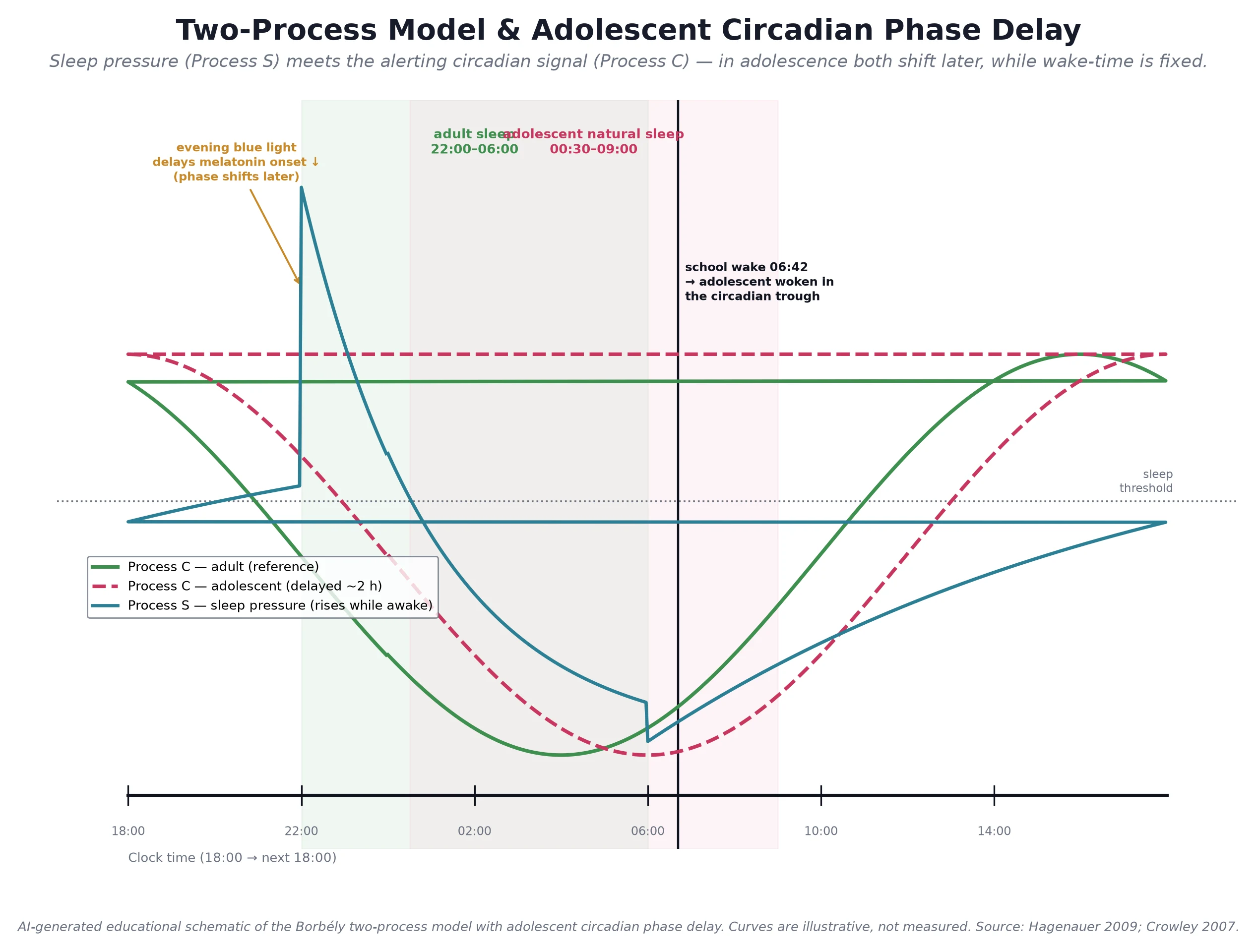
Read the figure like this: the shaded rose window is where an adolescent's brain wants to sleep — about 00:30 to 09:00. The fixed school wake at 06:45 cuts that window in half, leaving roughly five or six hours in place of the eight to ten the brain needs. The green window is where an adult's clock sits, only an hour or two earlier, which is why parents and adolescents argue about "a sensible bedtime". [10]
At puberty the circadian system genuinely shifts later. The dim-light melatonin onset (DLMO) — the moment the brain's melatonin begins to rise in the evening — moves about one to two hours later relative to clock time, and this is tied to pubertal stage rather than age. The intrinsic circadian period lengthens slightly (the brain's day gets longer than 24 hours, which biases it toward delay), and homeostatic sleep pressure may accumulate and dissipate more slowly, so an adolescent feels alert later into the evening and sleepier for longer into the morning. [8] [9]
Evening light reinforces the delay. Blue-wavelength light from phones, tablets and overhead lighting suppresses melatonin secretion and pushes DLMO later still, so the very devices an adolescent uses to wind down biologically wind them up. Weekend catch-up sleep completes the trap: sleeping until late morning on Saturday and Sunday means the young person receives their light exposure late in the day, which re-anchors the clock to a delayed phase and makes Monday's early rise even harder — the phenomenon of social jetlag, the mismatch between the social clock and the biological clock. [8] [17]
The consequences of chronic partial sleep loss track the brain systems that sleep supports. The prefrontal cortex, still maturing through adolescence, is exquisitely sleep-sensitive: attention, working memory, response inhibition and emotional regulation all degrade. Reward circuitry is amplified, increasing risk-taking. Consolidation of learning is impaired, and mood regulation falters, which is why sleep loss and depression reinforce one another. Mechanistically, narcolepsy type 1 is different again: it reflects loss of hypothalamic orexin (hypocretin) neurons, usually autoimmune, producing the inability to sustain stable wakefulness and the intrusion of REM-sleep phenomena into waking that we recognise as cataplexy. [11] [16]
Clinical Presentation
The teenager rarely presents with a "sleep complaint" of their own. They present through school (lateness, sleeping in class, falling grades), through parents (cannot get them out of bed, "lazy"), through mental-health services (low mood, anxiety, self-harm), or through primary care ("always tired"). The skill is recognising sleep as the common thread. [10]
Chronic insufficient sleep presents as daytime sleepiness, irritability, inattention, falling or erratic grades, weekend catch-up of two or more hours, and a widening weekday–weekend rise-time gap. The young person can sleep when given the chance. Insomnia presents differently: a long sleep-onset latency (lying awake for more than 30 minutes), frequent night waking or early awakening, mounting anxiety about sleep itself, and daytime fatigue that is often more "wired-tired" than true doziness. The bed has become a cue for wakefulness rather than sleep. [11]
Delayed sleep-wake phase disorder presents as an extreme inability to fall asleep before 01:00 to 03:00 and an extreme difficulty rising before late morning, with completely normal, refreshing sleep once it begins. The discriminating feature is the weekend: given a free schedule, the young person sleeps a normal length and feels well — they are not insomniac, they are mis-timed. Narcolepsy, by contrast, presents with irresistible sleep attacks across the day despite an adequate overnight sleep, and type 1 adds cataplexy — sudden bilateral loss of muscle tone triggered by emotion (laughter most classically) — with sleep paralysis and hypnagogic hallucinations. Narcolepsy is frequently misattributed to laziness, depression or substance use, and the delay to diagnosis averages years. [9] [16]
Obstructive sleep apnoea in an adolescent may present as snoring, witnessed pauses, restless or mouth-breathing sleep, morning headache, enuresis, daytime sleepiness and inattention that resembles ADHD; obesity and adenotonsillar hypertrophy raise the likelihood. Fatigue from non-sleep causes — the teenager who is "tired" but never actually dozes — most often signals depression or anxiety (anhedonia, low mood, worry, withdrawal, somatic complaints), and must also prompt consideration of iron deficiency, hypothyroidism, post-viral fatigue, coeliac disease, an eating disorder or an undiagnosed chronic disease. [11]
[16]Differential Diagnosis
The differential turns on the two questions you have already framed: is this sleepiness or fatigue, and if it is a sleep problem, which mechanism dominates? Build the list around the mechanism, and for each entry name the feature that separates it from the others. [10]
| Differential | Distinguishing feature |
|---|---|
| Insufficient sleep | Inadequate opportunity; sleeps well when allowed; short weekday, long weekend |
| Insomnia disorder | Adequate opportunity but cannot sleep; conditioned arousal; fatigue over sleepiness |
| Delayed sleep-wake phase disorder | Normal sleep at a delayed clock time; marked weekend rebound |
| Narcolepsy type 1 / idiopathic hypersomnia | Daily irresistible sleep despite adequate overnight sleep; cataplexy in type 1 |
| Obstructive sleep apnoea | Snoring, witnessed apnoea; obesity or adenotonsillar hypertrophy |
| Depression or anxiety | Fatigue with anhedonia, low mood, worry; no true sleep attacks |
| Medical fatigue | Iron deficiency, hypothyroidism, post-viral, coeliac, eating disorder, chronic disease |
| Substance or medication effect | Caffeine, nicotine/vaping, alcohol, SSRIs, stimulants, corticosteroids, isotretinoin |
The discrimination is largely in the history and the sleep diary, not in tests. A teenager who sleeps nine sound hours whenever the schedule allows is not insomniac; a teenager who lies awake for two hours every night despite nine hours in bed is not simply "not tired"; a teenager who dozes through afternoon classes despite nine sound hours overnight needs investigation for a central disorder of hypersomnolence. Fatigue without dozing, especially with mood change, points you to the mental-health history, the full blood count and ferritin, and thyroid function before it points you to a sleep clinic. [11] [16]
[9]Clinical & Bedside Assessment
A focused adolescent sleep assessment rests on a two-week sleep diary completed by the young person (not the parent) and embedded inside the broader HEEADSSS interview. Ask for bedtime, sleep-onset latency, number and duration of night wakings, final wake time and rise time, separately for weeknights and weekends, plus naps, caffeine, screens in the hour before bed, exercise timing, and a rating of daytime sleepiness. Where available, wrist actigraphy objectifies the timing and total sleep that diaries approximate. [10]
The history must also cover mood (depression and anxiety screen, self-harm risk), substance use (caffeine, energy drinks, nicotine and vaping, alcohol, recreational drugs), medications (stimulants, SSRIs, isotretinoin, corticosteroids), school (start time, travel time, homework load), and the young person's own goals — because behaviour change depends on their motivation, not the parent's. Ask specifically about snoring, witnessed apnoea, morning headache, sleep paralysis, hypnagogic hallucinations and, crucially, any emotion-triggered weakness (cataplexy). [11] [16]
The sleep assessment in five moves
Mechanism
Use the diary to separate insufficient sleep (short opportunity), insomnia (long latency / conditioned arousal) and DSWPD (normal sleep, delayed clock, weekend rebound).
Sleepiness vs fatigue
Epworth Sleepiness Scale for doziness; if fatigue dominates without dozing, screen mood and medical causes first.
Red flags
Cataplexy, snoring with witnessed apnoea, daily irresistible sleep despite adequate sleep, new neurology, self-harm.
Function and goals
Grades, mood, driving, relationships; the young person's own goals drive adherence.
Name the dominant problem
Document one mechanism as primary — the plan follows from it.
Validated tools are useful but do not replace the diary. The Epworth Sleepiness Scale measures the tendency to doze across situations and helps separate sleepiness from fatigue. The Insomnia Severity Index quantifies insomnia and its impact. The BEARS screen (Bedtime problems, Excessive daytime sleepiness, Awakenings, Regularity and duration, Snoring) and the Adolescent Sleep Wake Scale offer structure for busy clinics. The focused examination looks for obesity and adenotonsillar hypertrophy (OSA risk), neurological signs (narcolepsy, raised intracranial pressure), and the physical and mental-state stigmata of depression, anxiety, an eating disorder or chronic disease. [11] [16]
Investigations
Most adolescent sleep problems need no tests beyond the diary. The discipline is to reserve investigation for the mechanism that demands it. Polysomnography is indicated for suspected obstructive sleep apnoea (snoring with witnessed apnoea, especially with obesity or adenotonsillar hypertrophy), for parasomnias of concern, and to document adequate sleep before a multiple sleep latency test — not for straightforward insufficient sleep or insomnia. [16]
The multiple sleep latency test (MSLT) diagnoses the central disorders of hypersomnolence. It follows an overnight polysomnogram that confirms adequate preceding sleep and the absence of other sleep disorders, and requires withdrawal of REM-suppressing medications; a mean sleep latency of eight minutes or less with two or more sleep-onset REM periods supports narcolepsy or idiopathic hypersomnia. Any adolescent with daily irresistible sleepiness despite an adequate and well-documented overnight sleep deserves this pathway via a sleep specialist. [16]
For fatigue, a targeted medical screen is reasonable when the history or examination suggests an organic cause: full blood count and ferritin, thyroid function, coeliac serology, inflammatory markers, renal and liver function, and consideration of vitamin D and a monospot or post-viral screen. Dim-light melatonin onset is a research and specialist tool for confirming circadian phase in difficult DSWPD and is rarely needed in primary care. [11] [7]
The common error is over-investigating a behavioural problem. A teenager with short weekday sleep, long weekend catch-up, a normal examination and a clear diary does not need polysomnography, an MSLT or an extensive blood panel — they need a schedule. The converse error, equally serious, is missing narcolepsy or OSA by attributing sleepiness to "not enough sleep" without ever asking whether the sleep, when present, was adequate. [16]
Management — Resuscitation
Sleep presentations rarely need acute resuscitation, but a handful of scenarios are urgent. Cataplexy with sleep attacks is narcolepsy type 1 until proven otherwise and warrants prompt referral to a sleep specialist, both because untreated narcolepsy carries real functional and driving risk and because early treatment changes lives. Suspected obstructive sleep apnoea with significant desaturation, obesity-hypoventilation or cardiorespiratory concern needs prompt polysomnography and ENT or sleep referral rather than routine behaviour change. [16]
The most important "resuscitation" on this topic is the hidden mental-health crisis. A tired teenager may be depressed and at risk of self-harm, and the sleep complaint can be the only signal. Screen mood and safety at the first visit: if there is active suicidal ideation, recent self-harm or severe functional decline, the immediate priority is mental-health assessment and safety planning, not a sleep diary. Treat the sleep problem and the mood disorder together, because they reinforce one another — but the safety risk comes first. [11]
Severe sleep deprivation itself can carry acute risk: drowsy driving, falls and risk-taking. Counsel explicitly around driving — a sleep-deprived adolescent behind the wheel has reaction times comparable to intoxication — and address the schedule urgently while the underlying problem is being treated. [3] [6]
Management — Definitive & Stepwise
Management is stepped: start with measures that help every mechanism, then add the mechanism-specific therapy, then refer when red flags or refractory symptoms appear. The universal first step is a consistent rise time, seven days a week, which anchors the circadian clock; an adequate eight to ten hour sleep opportunity; bright light on waking; no screens for an hour before bed; a caffeine cap (and none after mid-afternoon); regular daytime exercise; and a bed reserved for sleep. These measures alone resolve a large fraction of adolescent sleep problems. [4] [14]
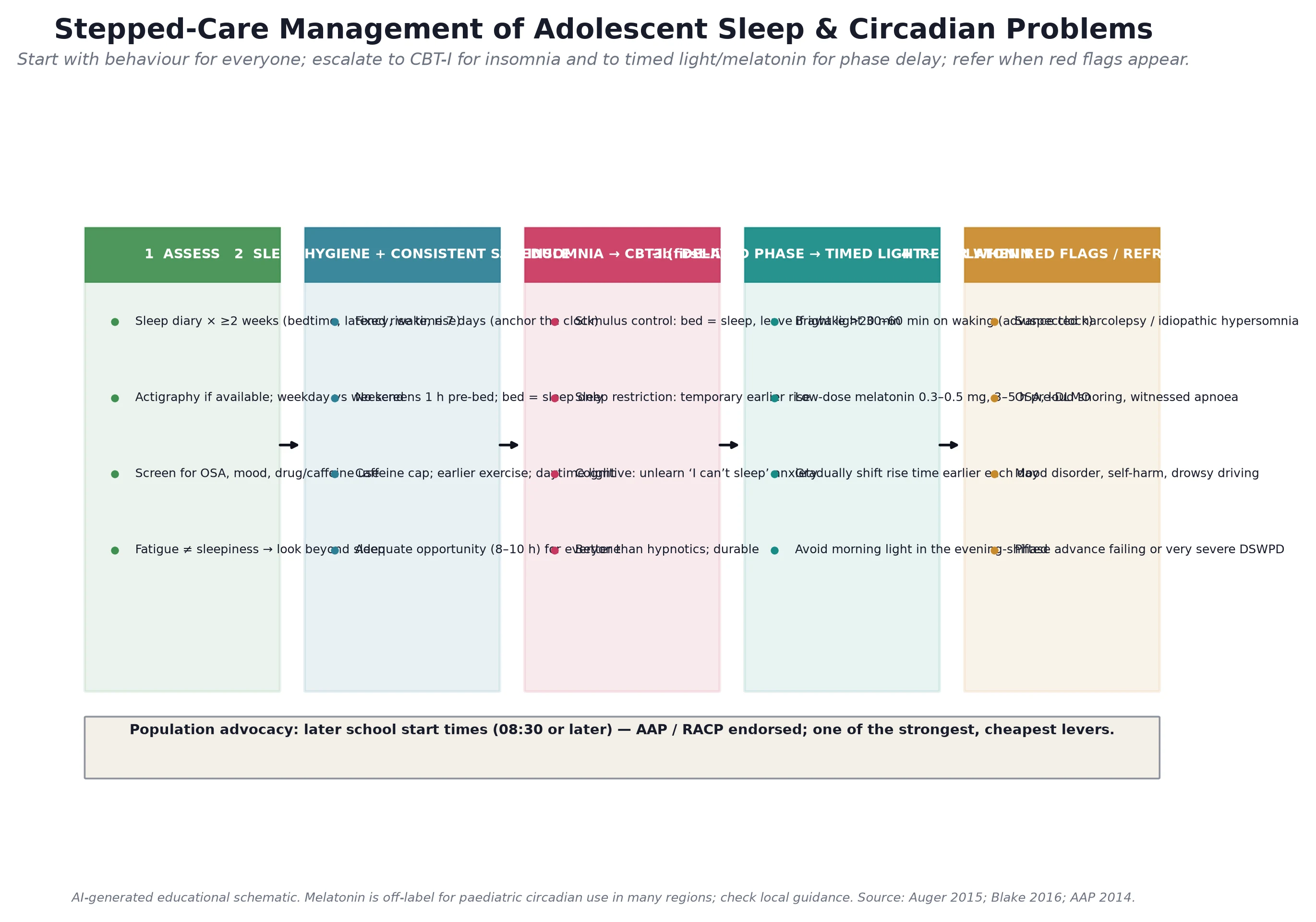
Insomnia — cognitive-behavioural therapy
For insomnia, first-line treatment is CBT-I, not a hypnotic. Its components are stimulus control (bed is for sleep only; if awake for more than 20 minutes, leave the bed and return only when sleepy), sleep restriction (temporarily reducing time in bed to build sleep pressure and consolidate sleep, then expanding it), cognitive therapy (addressing the unhelpful beliefs about sleep that drive arousal), sleep hygiene, and relapse prevention. The SENSE trial and related work show that cognitive-behavioural and mindfulness-based sleep interventions improve adolescent sleep and mood, and the gains are durable — a property hypnotics lack. [13] [14]
Delayed sleep-wake phase disorder — phase advance
For DSWPD, the goal is to move the clock earlier. Combine a gradual earlier rise time (15 to 30 minutes every few days, held seven days a week), bright light on waking (30 to 60 minutes of daylight or a light box), and low-dose melatonin taken about three to five hours before habitual sleep onset to pull DLMO earlier, while protecting the eyes from bright evening light. The AASM circadian guideline gives weak recommendations for both timed light and melatonin in DSWPD, reflecting an emerging evidence base; a recent meta-analysis confirms that melatonin meaningfully improves sleep parameters in young people with sleep or mental-health comorbidity and is generally well tolerated. [7] [15]
A typical phase-shifting melatonin dose is in the low range of roughly 0.3 to 5 mg, taken three to five hours before the current habitual sleep onset and gradually moved earlier with the schedule; in many regions paediatric melatonin use is off-label and should involve specialist input, and over-the-counter preparations vary in content. Chronotherapy — progressively delaying sleep around the clock until the desired time is reached — can work but carries a real risk of slipping into a non-24-hour pattern and is best supervised by a sleep specialist. [7] [15]
Population advocacy and follow-up
At the population level, delaying middle- and high-school start times to 08:30 or later is endorsed by the AAP and is among the strongest, cheapest levers in adolescent medicine: it has been shown to increase total sleep, improve mood and attendance, and reduce motor-vehicle crashes in adolescents. Advocating for it is part of management, not a sideshow. Follow up with a diary at four to eight weeks, adjust the plan, and safety-net the family to return sooner if cataplexy, loud snoring with pauses, mood or functional decline, or drowsy driving appears. [3] [6]
Specific Subtypes & Scenarios
Chronic insufficient sleep is the commonest scenario. Contract a consistent schedule and an adequate opportunity with the young person, framing the eight to ten hours as non-negotiable biology rather than parental control, and addressing screens, caffeine and homework timing as practical levers. Insomnia is managed with CBT-I delivered in an adolescent-friendly format; a sleeping tablet is rarely the answer and carries its own risks. [10] [13]
Delayed sleep-wake phase disorder is the adolescent who "cannot get up". The combined morning-light, low-dose evening melatonin and gradual schedule-advance approach works for many, but relapse is common if the schedule is not maintained once the clock has moved. Suspected narcolepsy or idiopathic hypersomnolence requires referral for an MSLT; the stimulant, sodium oxybate and other pharmacotherapy that may follow belongs to specialist sleep medicine and is beyond first-line general paediatric practice. [7] [16]
Obstructive sleep apnoea in the obese adolescent is recognised through snoring, witnessed apnoea and daytime sleepiness, confirmed with polysomnography, and managed with weight management alongside ENT or sleep input. Fatigue from depression or anxiety is the commonest non-sleep cause of a "tired teenager"; screen, treat the mood disorder, and resist over-investigating sleep. Sleep disturbance in neurodiverse young people (autism, ADHD) and in chronic disease demands tailored behavioural approaches, attention to sensory and routine factors, and coordination with the treating team. [11] [16]
The shift-working or early-start older adolescent (apprentices, fast-food workers, rural young people with long commutes) and the screen-bound teenager represent the hardest collision of social and biological clocks. Practical schedule negotiation, screen-boundary discussions that protect a therapeutic alliance, and realistic goal-setting matter more than rigid rules. [12] [17]
Complications & Pitfalls
The commonest error is confusing fatigue with sleepiness. They have different causes and different workups: fatigue most often points to mood or medical causes, sleepiness to a sleep problem, and treating a depressed teenager's fatigue with a sleep-hygiene leaflet misses the diagnosis entirely. The mirror error is treating insomnia with a hypnotic when CBT-I is the evidence-based, safer and more durable option, and chronic hypnotic use in adolescents is to be avoided. [11] [13]
Prescribing melatonin for "poor sleep" without clarifying the mechanism is a frequent trap. Melatonin phase-shifts a delayed clock; it is not a general sedative for insomnia or for simple insufficient sleep, and using it as one exposes the young person to an off-label agent without addressing the real problem. Equally, morning bright light applied without protecting the wake time can fail or even delay the clock further, and evening light can undo a day of phase advance. [7] [15]
Missing narcolepsy by attributing daytime sleepiness to laziness, depression or insufficient sleep delays diagnosis for years and harms education, safety and mental health. Missing obstructive sleep apnoea in an inattentive "ADHD-like" teenager, or over-diagnosing it without polysomnography, are the two ends of the same error. Over-investigating a straightforward behavioural problem with polysomnography and extensive bloods causes cost and anxiety for no benefit, and failing to address the mental-health comorbidity that drives or maintains the sleep complaint guarantees the plan will fail. Finally, ignoring the school context — an early start will defeat any individual schedule change unless the school start is addressed. [16] [3]
Prognosis & Disposition
Adolescent insufficient sleep has a good prognosis when the young person engages with a consistent schedule and the school start permits adequate sleep — but it relapses readily when the schedule slips. CBT-I for insomnia produces durable improvement in sleep onset, total sleep and daytime function, comparable to or better than medication, and the gains often persist at follow-up. DSWPD responds to combined light and melatonin phase-advance in many, with the caveat that relapse is common if the schedule is not maintained. [13] [7]
Narcolepsy and idiopathic hypersomnolence are chronic but manageable with specialist treatment; cataplexy in type 1 may respond to targeted therapy. When sleep disturbance is comorbid with depression or anxiety, the prognosis tracks the mood disorder — treat both, and sleep and mood improve together. Untreated adolescent sleep loss carries long-term costs in academic attainment, mental health, metabolic risk and drowsy-driving crashes, which is why this topic matters well beyond the clinic. [11] [6]
Disposition splits into tiers. The common behavioural problems (insufficient sleep, uncomplicated insomnia, mild DSWPD) are managed in primary care or general paediatrics with a diary, a plan and a safety-net. Refractory insomnia, moderate-to-severe or diagnostically unclear DSWPD, suspected central disorders of hypersomnolence, and obstructive sleep apnoea are referred to a sleep service, with urgency tiered to the red flags. Safety-net every family to return sooner if cataplexy, loud snoring with pauses, mood or functional decline, drowsy driving or self-harm emerges. [16]
Special Populations
Adolescents with depression and anxiety sit at the centre of this topic: the relationship between sleep and mood is bidirectional, and the principle is to treat both. Neurodiverse young people (autism, ADHD) have higher rates of sleep disturbance shaped by sensory and routine factors, and need tailored, consistent behavioural approaches and careful review of stimulant timing. [11]
Young people with chronic disease (cystic fibrosis, inflammatory bowel disease, chronic kidney disease, epilepsy) face disease-related sleep disruption and fatigue; coordinate with the treating team and remember that disease activity is often the driver. Obese adolescents carry increased OSA risk and the metabolic consequences of short sleep; weight management runs alongside sleep care. [11] [16]
Out-of-home-care and trauma-exposed youth may present with nightmares, hypervigilance and fragmented sleep as a sentinel of distress; a trauma-informed approach and screening for maltreatment and mental-health need take precedence over a rigid sleep schedule. Indigenous, remote and rural young people face long travel times colliding with early starts and real access barriers to specialist sleep services; culturally safe care and telehealth-based sleep support matter. Shift-working or early-start older adolescents need practical schedule negotiation, and young people on sleep-disturbing medication (stimulants, SSRIs, isotretinoin, corticosteroids) need a review of timing and alternatives as part of the plan. [12] [17]
Evidence, Guidelines & Regional Differences
The AASM consensus statement (Paruthi, 2016) sets the sleep-duration benchmarks used worldwide — 9 to 12 hours for school-age children and 8 to 10 hours for teenagers — and the National Sleep Foundation recommendations (Hirshkowitz, 2015) align closely. These are the figures a fellowship candidate should quote when asked "how much sleep does a teenager need". [4] [5]
The AAP 2014 policy statement on school start times, and the Owens school start-time study, established delaying middle- and high-school start to 08:30 or later as evidence-based public health, with demonstrable gains in sleep, mood, attendance and adolescent driving safety. The AASM 2015 circadian rhythm guideline (Auger) gives weak-but-real recommendations for timed light and melatonin in DSWPD, and the AASM 2021 hypersomnolence guideline (Maski) frames specialist pharmacotherapy for narcolepsy and idiopathic hypersomnia. [3] [6] [7] [16]
The behavioural evidence is growing. The SENSE trial (Blake, 2016) showed post-intervention benefits of a cognitive-behavioural and mindfulness-based group sleep intervention in at-risk adolescents, and the Dewald-Kaufmann trial (2014) showed that sleep extension plus sleep-hygiene advice improved sleep and depressive symptoms. The Carter meta-analysis (2016) quantified the association between portable screens and adverse sleep outcomes, with the usual caveats of cross-sectional, self-reported data. [13] [14] [17]
ANZ: the Sleep Health Foundation and RACP position statements frame adolescent sleep within youth-friendly preventive care and support later school start times; melatonin is available but paediatric off-label use is guided by specialist input.
UK: RCPCH Progress+ maps adolescent sleep to behavioural and mental-health training levels; NICE guidance on sleep does not endorse routine pharmacotherapy for paediatric insomnia, favouring behavioural approaches; melatonin is prescription-only and used selectively, often via paediatric services.
US: the AAP and AASM are the dominant voices; the AAP endorses 08:30 or later school starts; the AASM circadian and hypersomnolence guidelines shape management; melatonin is sold over the counter with documented variability in content, prompting caution.
Canada: the Canadian Paediatric Society and the Greig Health Record frame adolescent preventive care including sleep; provincial variation governs school start times and access to paediatric sleep services.
The open controversies are worth knowing. The real-world effect of school start delays at scale, the regulation and purity of over-the-counter melatonin, and the boundary between a normal adolescent phase delay and clinical DSWPD are all active areas of debate. The defensible fellowship position is to treat the mechanism in front of you, to use behavioural first-line therapy, and to reserve pharmacotherapy and specialist referral for the indications the guidelines name. [7] [15]
Exam Pearls
- Sleep need: 9 to 12 hours for 6–12 year olds; 8 to 10 hours for 14–17 year olds (AASM 2016; NSF 2015). [4] [5]
- The adolescent change is a circadian phase DELAY of about 1–2 hours, driven by puberty (later DLMO), not laziness. [8] [9]
- Three mechanisms drive the plan: insufficient sleep (not enough opportunity) vs insomnia (enough opportunity, cannot sleep) vs DSWPD (sleep at the wrong clock time). [10]
- Fatigue is NOT sleepiness — fatigue points to mood or medical causes; sleepiness points to a sleep problem. [11]
- CBT-I (stimulus control, sleep restriction, cognitive therapy) is first-line for adolescent insomnia, not hypnotics. [13]
- DSWPD management: morning bright light + low-dose melatonin about 3–5 h before DLMO + gradual earlier rise; protect the wake time. [7]
- Melatonin phase-shifts a delayed clock — it is not a general sleeping tablet for insomnia. [15]
- Later school start times (08:30 or later) are AAP-endorsed and improve sleep, mood, attendance and driving safety. [3] [6]
- Suspect narcolepsy type 1 when sleep attacks coexist with cataplexy; confirm with MSLT after documented adequate sleep. [16]
- Screen for OSA with snoring, witnessed apnoea and daytime sleepiness — especially in the obese adolescent; confirm with polysomnography. [16]
- Always screen for depression, anxiety and self-harm in the tired teenager — mood disorder is the commonest non-sleep cause. [11]
- Two-process model: Process S (homeostatic) rises while awake; Process C (circadian alerting) gates sleep; in adolescence both move later. [8]
- Social jetlag (the weekday–weekend sleep-timing gap) is a clinical marker of a delayed clock fighting an early start. [9]
- A 2-week sleep diary (and actigraphy if available) is the core investigation; polysomnography is reserved for suspected OSA and before MSLT. [10]
SLEEP for adolescent insomnia — first-line management
References
- [1]Carskadon MA, Wolfson AR, Acebo C, Tzischinsky O, Seifer R Adolescent sleep patterns, circadian timing, and sleepiness at a transition to early school days. Sleep, 1998.PMID 9871949
- [2]Wolfson AR, Carskadon MA Sleep schedules and daytime functioning in adolescents. Child development, 1998.PMID 9768476
- [3]Adolescent Sleep Working Group, Committee on Adolescence, Council on School Health School start times for adolescents. Pediatrics, 2014.PMID 25156998
- [4]Paruthi S, Brooks LJ, D'Ambrosio C, Hall WA, Kotagal S, Lloyd RM, Malow BA, Maski K, Nichols C, Quan SF, Rosen CL, Troester MM, Wise MS Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. Journal of clinical sleep medicine : JCSM, 2016.PMID 27250809
- [5]Hirshkowitz M, Whiton K, Albert SM, Alessi C, Bruni O, DonCarlos L, Hazen N, Herman J, Katz ES, Kheirandish-Gozal L, Neubauer DN, O'Donnell AE, Ohayon M, Peever J, Rawding R, Sachdeva RC, Setters B, Vitiello MV, Ware JC, Adams Hillard PJ National Sleep Foundation's updated sleep duration recommendations: final report. Sleep health, 2015.PMID 29073398
- [6]Owens JA, Belon K, Moss P Impact of delaying school start time on adolescent sleep, mood, and behavior. Archives of pediatrics & adolescent medicine, 2010.PMID 20603459
- [7]Auger RR, Burgess HJ, Emens JS, Deriy LV, Thomas SM, Sharkey KM Clinical Practice Guideline for the Treatment of Intrinsic Circadian Rhythm Sleep-Wake Disorders: Advanced Sleep-Wake Phase Disorder (ASWPD), Delayed Sleep-Wake Phase Disorder (DSWPD), Non-24-Hour Sleep-Wake Rhythm Disorder (N24SWD), and Irregular Sleep-Wake Rhythm Disorder (ISWRD). An Update for 2015: An American Academy of Sleep Medicine Clinical Practice Guideline. Journal of clinical sleep medicine : JCSM, 2015.PMID 26414986
- [8]Hagenauer MH, Perryman JI, Lee TM, Carskadon MA Adolescent changes in the homeostatic and circadian regulation of sleep. Developmental neuroscience, 2009.PMID 19546564
- [9]Crowley SJ, Acebo C, Carskadon MA Sleep, circadian rhythms, and delayed phase in adolescence. Sleep medicine, 2007.PMID 17383934
- [10]Carskadon MA Sleep in adolescents: the perfect storm. Pediatric clinics of North America, 2011.PMID 21600346
- [11]Beebe DW Cognitive, behavioral, and functional consequences of inadequate sleep in children and adolescents. Pediatric clinics of North America, 2011.PMID 21600347
- [12]Gradisar M, Gardner G, Dohnt H Recent worldwide sleep patterns and problems during adolescence: a review and meta-analysis of age, region, and sleep. Sleep medicine, 2011.PMID 21257344
- [13]Blake M, Waloszek JM, Schwartz O, Abbey B, Raniti M, Simmons JG, Dudgeon P, Belcher J, Trinder J, Kaestner E, Klinck J, O'Brien L, Allen NB, Tractenberg S, Lewinsohn PM, Hickie IB, Toumbourou JW The SENSE study: Post intervention effects of a randomized controlled trial of a cognitive-behavioral and mindfulness-based group sleep improvement intervention among at-risk adolescents. Journal of consulting and clinical psychology, 2016.PMID 27775416
- [14]Dewald-Kaufmann JF, Oort FJ, Meijer AM The effects of sleep extension and sleep hygiene advice on sleep and depressive symptoms in adolescents: a randomized controlled trial. Journal of child psychology and psychiatry, and allied disciplines, 2014.PMID 24252173
- [15]Salanitro M, Wrigley T, Ghabra H, de Luquero Pascual MT, Farez M, Scalco MZ, Wu C, Peker Y, Owusu J, Khosh-Chasenar F, Fillbrunn M, Rickards H, Curtis C, Fox S, Mehta M, Petrides G, Fusar-Poli P Efficacy on sleep parameters and tolerability of melatonin in individuals with sleep or mental disorders: A systematic review and meta-analysis. Neuroscience and biobehavioral reviews, 2022.PMID 35691474
- [16]Maski K, Trotti LM, Kotagal S, Robert M, Friederich Murray C, Gordon CR, Chervin RD, Loccock L, Moore L, Wilson M, Rogers AE Treatment of central disorders of hypersomnolence: an American Academy of Sleep Medicine clinical practice guideline. Journal of clinical sleep medicine : JCSM, 2021.PMID 34743789
- [17]Carter B, Rees P, Hale L, Bhattacharjee D, Paradkar MS Association Between Portable Screen-Based Media Device Access or Use and Sleep Outcomes: A Systematic Review and Meta-analysis. JAMA pediatrics, 2016.PMID 27802500