Paeds · adolescent-and-young-adult-medicine
Tobacco, vaping and nicotine dependence
Also known as Adolescent nicotine dependence · Youth e-cigarette and vaping use · Adolescent smoking cessation · Vaping and EVALI · Youth tobacco use disorder · Pod-device and e-liquid dependence
A fellowship approach to adolescent nicotine and tobacco use across combustible, electronic, pod and smokeless products: faster-onset dependence in the developing brain, validated dependence assessment, the 5 A's and motivational interviewing, evidence-based pharmacotherapy, EVALI recognition, and prevention across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old tells you they "just vape sometimes." Three months later they are using a pod device every hour, craving it on waking, irritable without it, and failing classes. The missed signal was not the product — it was the assumption that "sometimes" means "not dependent." [13]
Nicotine dependence is the brain adaptation that follows repeated nicotine exposure: tolerance, craving, withdrawal and a loss of control over use. In adolescents it can appear within days to weeks of first use, often before a young person becomes a daily user, because the developing brain is exquisitely sensitive to nicotine. [5] [7]
The products that deliver nicotine to young people are now far broader than the cigarette. Combustible cigarettes remain the most lethal; e-cigarettes and vapes aerosolise nicotine with solvents and flavourants; pod and nicotine-salt devices (such as JUUL-type products) deliver high doses discreetly; heated tobacco products heat rather than burn leaf; waterpipe (hookah) delivers high carbon-monoxide exposure in shared sessions; and smokeless tobacco carries oral and cancer risk. Asking only about "smoking" misses most modern use. [14] [15]
The clinical task is threefold: detect use and dependence early, treat with evidence-based behavioural and pharmacological support, and prevent uptake. The first two require a clinician who asks routinely and without judgement; the third requires advocacy. [12]
The core sequence of adolescent tobacco and nicotine care
Engage
Time alone, conditional confidentiality, non-judgemental stance, ask about all products.
Detect
Screen every adolescent; quantify use; ask about craving, withdrawal, quit attempts.
Grade
Apply DSM-5 criteria; use a validated tool (HONC, mFTQ) to measure dependence.
Assist
5 A's, motivational interviewing, behavioural support, pharmacotherapy matched to readiness.
Arrange
Follow-up within 1–2 weeks; frame relapse as practice; close referral loops.
Safety
Recognise EVALI and nicotine toxicity; escalate acute presentations immediately.
Classification
Classify by product, stage of use, and degree of dependence. The product tells you what toxins the young person is exposed to; the stage tells you where they sit on the experimentation-to-dependence continuum; the degree of dependence tells you how hard quitting will be and how aggressive treatment should be. [13]
Products and what they deliver
The product spectrum runs from burned tobacco at one end to aerosolised nicotine and smokeless leaf at the other. Combustible cigarettes deliver thousands of toxins and tar; e-cigarettes and vapes deliver aerosolised nicotine with propylene glycol, glycerine and flavouring chemicals, producing far fewer combustion toxins but not "harmless water vapour." Pod and nicotine-salt devices use benzoic acid to deliver high nicotine doses smoothly and discreetly, which is why they drove the surge in youth use. [15] [14]
Stages of use
Use moves from experimentation (trying, typically social and infrequent), to regular use (repeated, often weekly), to problematic use (interfering with function or accompanied by dependence features), to established dependence (daily use, withdrawal, failed control). A young person can skip straight from experimentation to dependence with a high-delivery pod device, which is why the stage model is a guide, not a ladder every adolescent climbs one rung at a time. [13]
Grading dependence
Dependence is graded with the DSM-5 tobacco use disorder criteria — craving, withdrawal, tolerance, using more or longer than intended, persistent desire or failed efforts to cut down, and continued use despite harm — applied with the understanding that an adolescent need not be a daily user to meet criteria. Validated instruments such as the Hooked on Nicotine Checklist (HONC) and the modified Fagerström Tolerance Questionnaire (mFTQ) quantify severity and, importantly, give the young person language for what they are experiencing. [7]
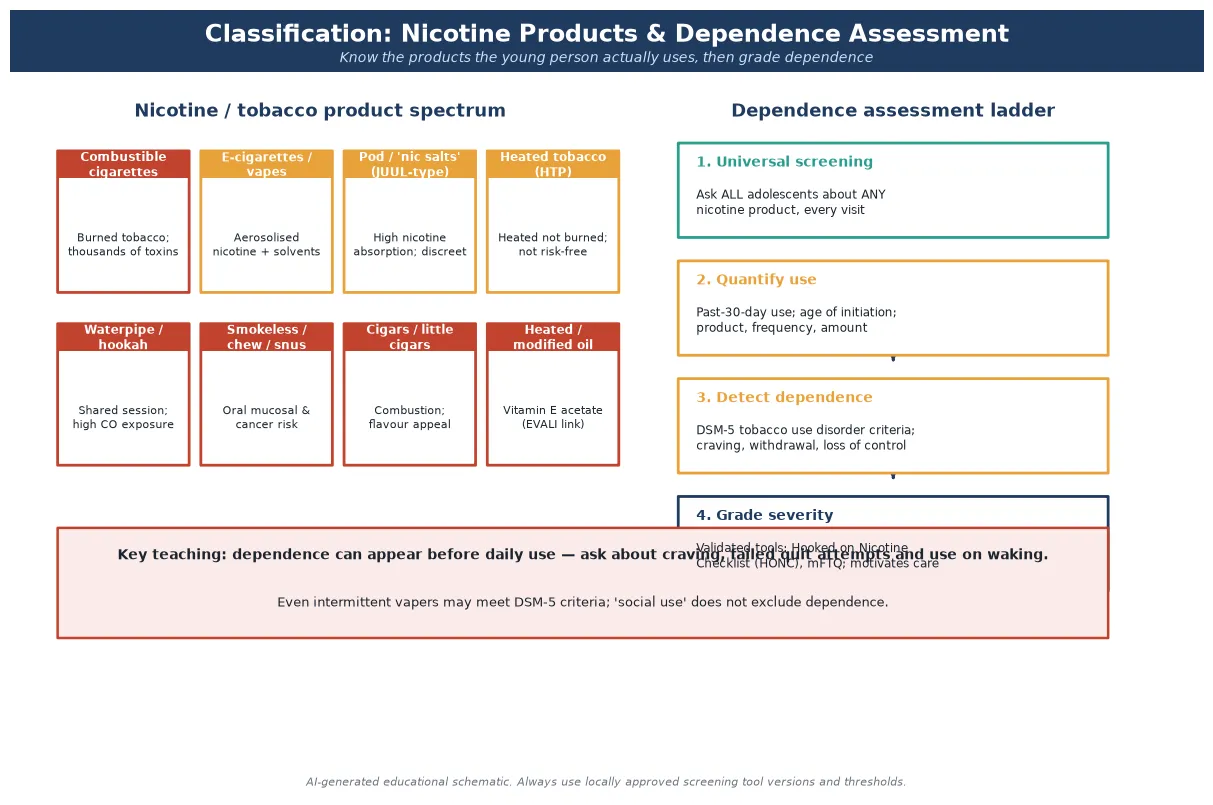
Read the figure like this: if you ask only about cigarettes, you will classify a daily pod-device user as a non-smoker. Always map the actual product before grading dependence. [15]
Cigarette smoker
Combustible
- Thousands of combustion toxins and tar
- Highest long-term mortality profile
- Often the end-point of a vaping gateway
- Strong smell — easier to detect
Vape / pod user
Aerosolised nicotine
- High nicotine absorption, discreet, flavoured
- Can drive dependence faster than cigarettes
- Fewer combustion toxins but not harmless
- Odourless — easy to miss clinically
Waterpipe / hookah
Shared combustion
- High carbon-monoxide exposure per session
- Shared mouthpiece — infection risk
- Perceived as safer; uptake is social
- Large inhaled volume per session
Smokeless / chew
Oral tobacco
- Oral mucosal disease and cancer risk
- Nicotine dependence without inhalation
- Region-specific products and prevalence
- Often overlooked in 'do you smoke?' screening
Epidemiology & Risk Factors
E-cigarette and vape use among adolescents rose sharply through the late 2010s, driven by flavoured pod devices and social-media marketing, and it now dominates youth nicotine exposure in many high-income countries even as combustible cigarette smoking has fallen. [1]
The United States National Youth Tobacco Survey documents the current pattern: a substantial minority of middle and high school students report current tobacco product use, with e-cigarettes the most commonly used product, and a meaningful proportion reporting frequent or daily use. [1]
Risk is not evenly distributed. LGBTQ+ youth, those with depression, anxiety or ADHD, young people with low family or school connectedness, those exposed to peer or family smoking, and adolescents in out-of-home care or socioeconomic disadvantage all carry higher rates of vaping and smoking. These are also the young people most likely to be missed if screening is selective rather than universal. [13]
The gateway association is central to why paediatricians care: adolescents who use e-cigarettes are more likely to subsequently take up combustible cigarettes than those who do not, and the evidence from meta-analysis and systematic review is consistent in direction even as it is debated in mechanism. [4] [3]
Pathophysiology
You do not need a neuroscience lecture to counsel well. You do need a working model of why a young person who "just vapes sometimes" is already on a biological track toward dependence, because that model explains why early detection and non-judgemental treatment matter. [5]
When nicotine is inhaled — whether in smoke or in aerosol — it reaches the brain within seconds and binds to alpha-4-beta-2 nicotinic acetylcholine receptors in the ventral tegmental area. That binding triggers dopamine release into the nucleus accumbens, the brain's reward centre, and the dopamine surge encodes "do that again." Repeated exposure drives tolerance, craving, withdrawal and the loss of control that defines dependence. [5] [6]
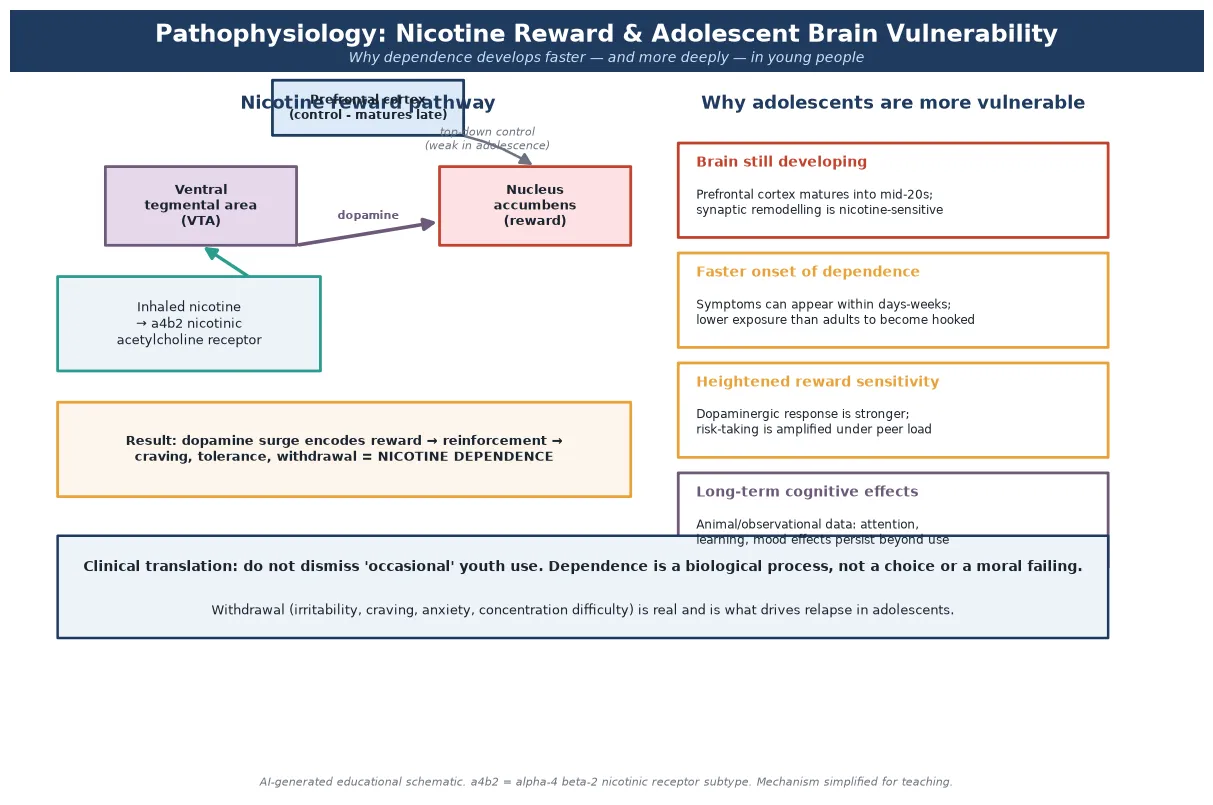
The adolescent brain is more vulnerable for three reasons. The prefrontal cortex — the seat of impulse control and forward planning — is still maturing into the mid-twenties, so top-down control over reward is weak. The dopaminergic reward system is at peak sensitivity through mid-adolescence, so nicotine feels more rewarding. And the brain is undergoing active synaptic remodelling, so nicotine leaves longer-lasting imprints on attention, learning and mood than it does in an adult brain. [5] [6]
The clinical consequence is that dependence develops faster and at lower cumulative exposure in adolescents than in adults. A young person can experience craving, withdrawal and failed quit attempts while still describing their use as "occasional." Withdrawal itself — irritability, anxiety, low mood, poor concentration, craving — is real and is exactly what drives relapse, so a teenager who "keeps failing" to quit is not weak-willed; their brain is demanding the chemical it has adapted to. [8] [6]
Clinical Presentation
Nicotine dependence presents across a spectrum, from the openly disclosed experimenter to the completely covert daily user. The most dangerous presentations are the hidden ones, because nobody asked the right question. [13]
Organised low-risk presentation: the young person engages, private time is secured, and the only finding is infrequent experimentation with intact mood, sleep, school and social function, and no dependence features. The task is brief, personalised advice, reinforcement of non-use, and a safety net. [12]
High-risk patterns hiding inside ordinary visits: mood or attention decline attributed to "adolescence"; school disengagement; concealed odourless pod-device use; escalating use of the device on waking or between classes; money spent on pods or e-liquid; recurrent respiratory symptoms; and a young person with a chronic illness whose condition is worsening without obvious cause. Each is a door into a dependence assessment, not a closed file. [13] [14]
Acute presentations arrive in the emergency department. EVALI — e-cigarette or vaping product use-associated lung injury — presents with respiratory distress, cough, chest pain or shortness of breath, often with gastrointestinal symptoms and fever, in a young person with recent vaping; it was recognised as a major outbreak and demands emergency assessment and reporting. Acute nicotine toxicity arises most often from ingestion of e-liquid, causing nausea, vomiting, tachycardia and, in severe cases, seizures or reduced consciousness. [2] [14]
Differential Diagnosis
In nicotine care the differential is less "which disease" and more "what is driving the presentation, and is there an acute complication." [13]
| What it looks like | Safer framing question | Do not miss |
|---|---|---|
| "Occasional" vaping | Craving, use on waking, failed quit attempts | Emerging dependence before daily use |
| Low mood, anxiety, poor concentration | Nicotine withdrawal versus a primary disorder | Both can co-exist; withdrawal is real |
| Cough and dyspnoea in a vaper | EVALI versus asthma exacerbation or infection | EVALI needs exclusion and reporting |
| Worsening chronic illness | Is nicotine use undermining control (e.g. asthma) | Concealed vaping as the driver |
| Cannabis or other-substance vaping | What else is in the device? | Co-occurring substance use and dependence |
The core discriminator is function and control: does the use sit alongside intact mood, sleep and school performance with no dependence features, or is it accompanied by craving, withdrawal, escalating use and impairment? Experimentation without dependence needs brief advice. Dependence and impairment need treatment. [7]
A second discriminator is whether an acute complication is present. Respiratory distress with recent vaping is EVALI until proven otherwise, and mood collapse in a heavy user may be withdrawal, a co-occurring mental-health disorder, or both — each shifts the immediate plan. [2] [8]
Clinical & Bedside Assessment
1. Open and frame
Greet the young person first, set a joint agenda, then secure time alone and state conditional confidentiality with its limits out loud. Without this frame, the assessment will return false negatives, because the young person will not disclose use in front of a parent. [12]
2. Take a product-specific history
Ask about all products — not just "do you smoke." Which product (cigarette, vape, pod, waterpipe, smokeless)? How old when they started? How many days in the last month? How many times a day? What triggers use (stress, friends, waking)? Use open then focused questions and follow every lead deeper. [13] [15]
3. Screen and quantify use
Determine any use, past-30-day use, daily use, and age of initiation. These four anchors stratify risk and track change over time. Frequency alone underestimates dependence, so always pair it with dependence-feature questioning. [12]
4. Assess dependence
Apply the DSM-5 tobacco use disorder criteria and a validated tool such as the Hooked on Nicotine Checklist. Ask directly about craving, use on waking, tolerance, withdrawal, and failed quit attempts. A positive dependence screen is a trigger for a treatment plan, never just a label. [7]
5. Assess readiness and co-morbidities
Explore the young person's own reasons for and against change (their readiness), because the right intervention for a precontemplative experimenter is not the right one for someone asking to quit. Screen for co-occurring depression, anxiety, ADHD, other substance use, and — in any young person who vapes or smokes — pregnancy risk. [13]
6. Examine when harm is suspected
If vaping-related illness is suspected, perform a focused respiratory examination, check oxygen saturation, and look for signs of systemic illness. The exam is guided by the presentation; routine asymptomatic screening does not need a physical work-up. [2]
Investigations
Most adolescent tobacco and nicotine assessment needs few laboratory tests; it needs a thorough history and the right screens. Investigation is selective and presentation-led. [13]
For suspected EVALI, the work-up includes a chest radiograph (which typically shows bilateral opacities), inflammatory markers, and an infectious work-up to exclude alternative diagnoses — because EVALI is a diagnosis of exclusion supported by a consistent exposure history. The severity guides whether imaging, bloods or hospital admission are needed. [2] [14]
Validated instruments — the Hooked on Nicotine Checklist, the modified Fagerström, and the DSM-5 criteria — function as triggers for clinical action, not as diagnoses. Their value is that they quantify dependence and give the young person shared language, which improves engagement and treatment matching. [7]
Cotinine or urine nicotine testing has a narrow, consent-governed role — for example, confirming exposure in specific research or forensic contexts — and is never a substitute for a confidential interview. Punitive or surprise testing damages trust and suppresses future disclosure. [13]
Low-value patterns to avoid include routine broad blood panels on every asymptomatic adolescent vaper, treating a screen score as a diagnosis, and punitive toxicology. [13]
Management — Resuscitation
A routine tobacco visit can become an emergency in one disclosure or one examination. Recognise the exit point and use it. [2]
- Suspected EVALI: assess airway, breathing and circulation; give supplemental oxygen as needed; perform the diagnostic work-up and exclude infection; and arrange admission or transfer for progressive respiratory failure. EVALI can deteriorate quickly, so a low threshold for escalation protects the patient. [2] [14]
- Acute nicotine toxicity (e-liquid ingestion): this is a poisonings emergency — assess and support airway, breathing and circulation, manage seizures, and seek urgent toxicology or poisons-centre guidance, because ingestion of concentrated nicotine liquid can be life-threatening. [14]
- Co-occurring mental-health crisis: if heavy nicotine use sits alongside suicidality or self-harm, address the safety risk first — remove means, do not leave the young person alone, and activate the crisis pathway before turning to cessation. [13]
The principle is simple: acute threats to life or safety come before a quit plan, every time. [2]
Management — Definitive & Stepwise
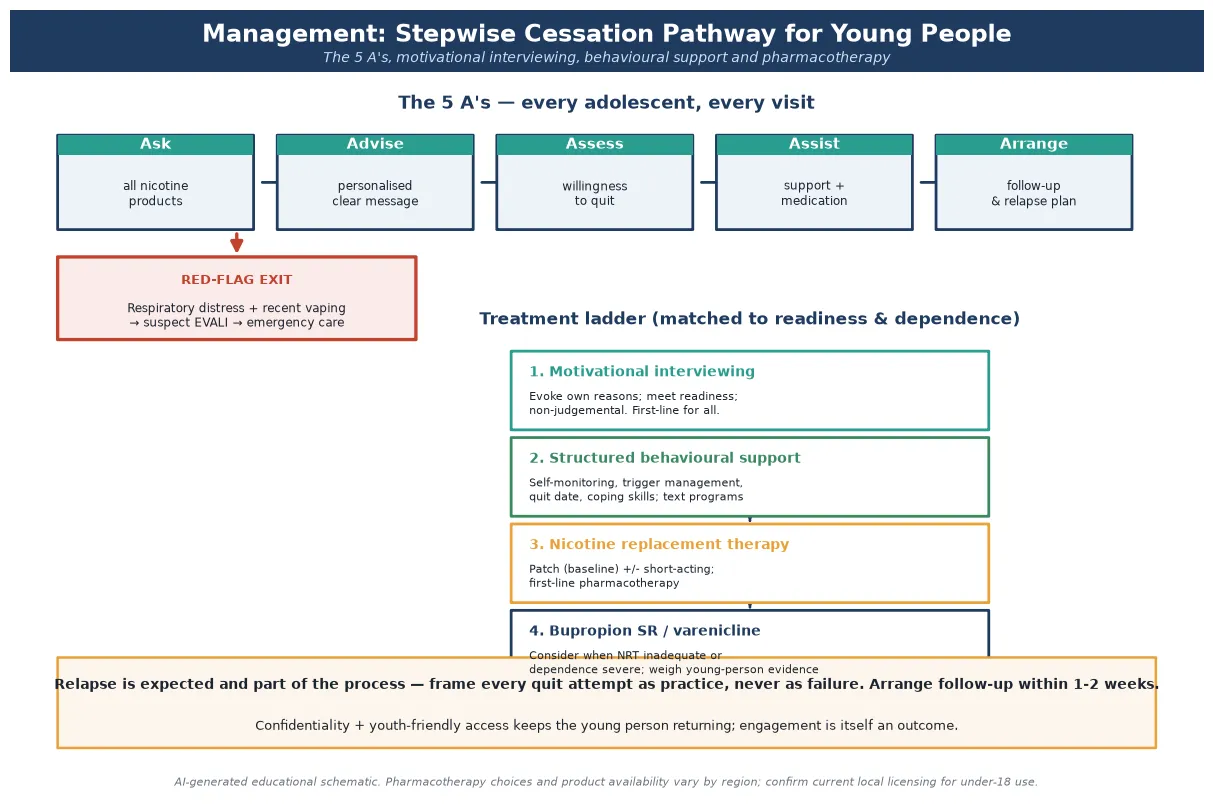
Read the figure like this: the EVALI red-flag exit sits before the treatment ladder for a reason. Any acute-respiratory finding exits the routine cessation path before you reach brief intervention. [2]
The 5 A's — universal workflow
The 5 A's — Ask, Advise, Assess, Assist, Arrange — is the evidence-based tobacco-care workflow that should run on every adolescent at every visit. Ask about all products; Advise with a clear, personalised message; Assess willingness to quit and dependence; Assist with counselling and, where indicated, pharmacotherapy; and Arrange follow-up. [12]
Brief intervention: motivational interviewing
Motivational interviewing uses open questions, affirmation, reflective listening and summaries to help the young person articulate their own reasons for change rather than being lectured. The skill is to evoke, not to impose. For a precontemplative teenager, the goal of the conversation is not abstinence today — it is moving them one step toward readiness. [13]
Behavioural support
Structured behavioural support includes setting a quit date, identifying and managing triggers, building coping skills, arranging social support, and using digital tools. A randomised trial showed that a tailored text-message cessation program increased abstinence in adolescent e-cigarette users, making digital support a practical, low-cost, high-reach option. [16]
Pharmacotherapy
Pharmacotherapy is matched to dependence severity and willingness. Nicotine replacement therapy is first-line: a patch provides baseline nicotine and a short-acting form (gum, lozenge, spray) handles breakthrough craving. Bupropion SR and varenicline are considered where NRT is inadequate or dependence is severe, recognising that the evidence base and licensing for under-18 use vary by region — a recent randomised trial examined varenicline specifically for youth vaping cessation. [9] [11]
Varenicline for youth nicotine vaping cessation (Evins et al., JAMA 2025)
Randomised clinical trial of varenicline in young people seeking to quit vaping.
Key finding
Provides current, trial-level evidence on varenicline for youth vaping cessation; interpret alongside regional licensing and the wider Cochrane review of vaping-cessation interventions.
Practice change
Pharmacotherapy options for adolescent vaping cessation are expanding, but product licensing and guideline endorsement for under-18 use remain region-specific — confirm local status before prescribing.
Motivational interviewing
First-line for all
- Evoke the young person's own reasons
- Matched to stage of change
- Non-judgemental, youth-friendly
- No medication, no age limit
Behavioural support
Structured quitting
- Quit date and trigger management
- Coping skills and social support
- Text-message and app programs
- Builds skills for repeated attempts
Nicotine replacement
First-line medication
- Patch baseline plus short-acting
- Reduces withdrawal and craving
- Regional licensing governs under-18 use
- Caution in pregnancy and cardiac disease
Bupropion / varenicline
Second-line consider
- When NRT inadequate or dependence severe
- Evidence and licensing vary by region
- Monitor for neuropsychiatric effects
- Varenicline trialled in youth vaping
Arrange follow-up and manage relapse
Arrange follow-up within one to two weeks of a quit attempt, because the early period carries the highest relapse risk. Frame relapse as part of the quitting process, not as failure — most successful quitters made multiple attempts — and use each relapse to refine the trigger and coping plan. Engagement is fragile across adolescence, so always name the next contact and a low-threshold way back in. [12] [13]
Specific Subtypes & Scenarios
Pod and nicotine-salt device dependence. Pod devices deliver high doses of nicotine smoothly and discreetly, which is why they drove the youth surge and why their users can develop dependence faster than cigarette smokers. Treat the dependence seriously even when the young person "only" uses a pod, and match pharmacotherapy intensity to the dependence grade rather than the product. [15]
Suspected EVALI. In any adolescent with respiratory distress and recent vaping, treat EVALI as the working diagnosis, exclude infection, perform chest imaging and inflammatory markers, provide supportive respiratory care, counsel immediate cessation, and report as required. The 2019 outbreak was strongly linked to vitamin E acetate and illicit or modified products, particularly those containing THC, so ask exactly what was in the device. [2] [14]
Wants to quit vaping but not cigarettes (or vice versa). Meet the young person where they are: support the change they want to make first, while gently opening the conversation about the other product. Demanding total abstinence as a precondition for any help disengages the very young people most at risk. [13]
Chronic illness. Young people with asthma, cystic fibrosis, diabetes or mental-health disorders still need nicotine screening and cessation support — and often more urgently, because vaping can worsen their underlying disease. Do not let the chronic condition overshadow the nicotine use. [13]
Waterpipe (hookah). Shared-session waterpipe use delivers large inhaled volumes and high carbon-monoxide exposure, and young people often perceive it as safer than cigarettes. Screen for it specifically, because it is easy to miss with a "do you smoke cigarettes?" question. [14]
Pregnancy in an adolescent who smokes or vapes. This is a high-stakes scenario: nicotine harms fetal development, and cessation is urgent. Prioritise behavioural support, use NRT only with careful, region-specific guidance and supervision, and arrange close, multidisciplinary follow-up. [13]
Complications & Pitfalls
- Dismissing "occasional" youth use as harmless, and missing dependence that has already begun. [7]
- Asking only about cigarettes, and classifying a daily pod-device user as a non-smoker. [15]
- Assuming e-cigarettes are "safe" or produce "harmless water vapour" — they deliver fewer combustion toxins but are not harmless, and EVALI can be fatal. [14] [2]
- Missing EVALI behind a diagnosis of "asthma exacerbation" or "viral infection" in a young person who vapes. [2]
- A punitive or judgemental stance that suppresses disclosure at the next visit. [13]
- Forgetting that bupropion and varenicline carry neuropsychiatric monitoring requirements and that licensing for under-18 use is region-specific. [9]
- Failing to frame relapse as part of quitting, so the young person disengages after a "failure." [12]
- Offering cessation help to only one domain while ignoring co-occurring cannabis, alcohol or mental-health needs. [13]
Prognosis & Disposition
Prognosis here means the trajectory of dependence, quit attempts and engagement, not a disease stage. [13]
Routine disposition: a complete low-risk assessment with experimentation but no dependence, intact function and strong protective factors; give personalised brief advice, reinforce non-use, and plan the next routine contact. [12]
Early-review disposition: established or emerging dependence, a recent quit attempt, unstable mood without crisis, or an incomplete assessment needing a return visit with trust built. Arrange follow-up within one to two weeks and a low-threshold way back in. [13]
Urgent disposition: suspected EVALI, acute nicotine toxicity, or a co-occurring mental-health crisis — emergency department or crisis pathway as indicated, with cessation and follow-up loops closed. [2]
Most successful quitters made several attempts, so disposition should normalise repeated tries and keep the young person engaged. The single best predictor of eventual success is that the young person keeps coming back. [12] [13]
Special Populations
LGBTQ+ youth. Vaping rates are higher among sexual- and gender-minority young people, layered with minority stress, bullying and family rejection. Tailor counselling to identity and context, and watch for co-occurring mental-health needs. [13]
Mental-health comorbidity and ADHD. Young people with depression, anxiety or ADHD vape and smoke at higher rates, and nicotine is sometimes self-medication for concentration or mood. Treat the nicotine dependence and the mental-health condition together, because each worsens the other. [13]
Pregnant adolescents. Nicotine harms fetal development, making cessation urgent. Lead with behavioural support, use NRT only with region-specific guidance and supervision, and arrange close multidisciplinary follow-up. [13]
Indigenous young people. Deliver culturally safe counselling, partner with local services, and recognise that connection to community and addressing racism are part of tobacco care as much as any screening tool. [13]
Neurodiverse and disabled young people. Offer longer slots, sensory adjustments, easy-read materials and capacity assessment, and avoid overshadowing the nicotine dependence behind the disability. [13]
Socioeconomic disadvantage. Ask about cost, transport and clinic access before attributing "non-adherence" to character, because NRT cost and clinic reach shape which cessation options are actually available to the young person. [13]
Evidence, Guidelines & Regional Differences
Pharmacotherapy evidence in adolescents. Evidence for NRT, bupropion and varenicline in adolescent cessation is weaker than in adults, partly because adherence and trial design are harder in young people. NRT remains first-line; bupropion and varenicline are considered second-line where dependence is severe, and a recent randomised trial examined varenicline specifically for youth vaping cessation. [9] [11]
Vaping cessation interventions. A Cochrane review of interventions for quitting vaping is synthesising this fast-moving evidence, and a randomised trial confirmed that a tailored text-message program increased abstinence in adolescent e-cigarette users, supporting digital, low-threshold delivery. [10] [16]
The gateway association. A meta-analysis and a recent systematic review both find that e-cigarette use is associated with subsequent combustible cigarette smoking in young people. The association is consistent in direction; the causal mechanism remains debated, but the clinical implication is clear: prevent and detect vaping early. [4] [3]
EVALI. The 2019 outbreak of e-cigarette or vaping product use-associated lung injury clarified that vaping can cause severe, sometimes fatal acute lung injury, most strongly linked to vitamin E acetate and illicit or THC-containing products. It reshaped how clinicians assess respiratory illness in any young person who vapes. [2] [14]
Adolescent brain vulnerability. Reviews of nicotine's effects on the adolescent brain establish that dependence develops faster and at lower exposure in young people, with potential long-term effects on cognition, attention and mood. [5] [6]
Controversy: harm reduction versus youth prevention. A central policy tension is whether e-cigarettes are a harm-reduction tool for adult smokers or a youth gateway that should be heavily restricted. For paediatricians the priority is fixed: prevent uptake, detect dependence early, and treat with evidence-based support. [13]
ANZ: Australia restricts recreational e-cigarette access and requires prescription for nicotine vaping products; Aotearoa New Zealand has moved through successive smokefree and vaping regulation. Confirm current local statute before advising on product legality or prescribing. UK: NICE guideline NG209 covers preventing uptake, promoting quitting and treating dependence, and the UK has historically framed e-cigarettes as a harm-reduction tool for adult smokers while restricting youth access and advertising. US: The CDC and Surgeon General frame youth e-cigarette use as an epidemic; the 2008 Public Health Service clinical practice guideline underpins tobacco-dependence treatment; state laws govern age of sale, flavours and pharmacotherapy access. Canada: Health Canada regulates vaping product promotion, nicotine concentration and flavours, with provincial variation; smoking-cessation counselling and pharmacotherapy align with national guidance.
Exam Pearls
- Open every answer with time alone and conditional confidentiality before any tobacco or nicotine question. [12]
- Define adolescent nicotine dependence as a biological process that can begin before daily use — not a choice or moral failing. [5] [7]
- Name the actual product the young person uses (vape, pod, cigarette, waterpipe, smokeless) — never ask only about "smoking." [15]
- Cite that dependence develops faster and at lower exposure in adolescents because the brain is still developing. [5] [6]
- Frame every quit attempt as practice; relapse is expected and part of the process, never a failure. [12]
- State that NRT is first-line pharmacotherapy; bupropion and varenicline are considered where NRT is inadequate or dependence is severe, with region-specific licensing caution. [11] [9]
- Suspect EVALI in respiratory distress with recent vaping; exclude infection and report. [2] [14]
- Remember the 5 A's — Ask, Advise, Assess, Assist, Arrange — every adolescent, every visit. [12]
- Name the gateway association: e-cigarette users are more likely to subsequently smoke combustible cigarettes. [4] [3]
- State that local statute and licensing govern product age-of-sale, nicotine caps and pharmacotherapy availability — do not invent universal cut-offs. [13]
ASK AGAIN — adolescent nicotine care
References
- [1]Jamal A, Park-Lee E, Birdsey J, et al. Tobacco Product Use Among Middle and High School Students - National Youth Tobacco Survey, United States, 2024. MMWR Morbidity and mortality weekly report, 2024.PMID 39418216
- [2]Kalininskiy A, Bach CT, Nacca NE, et al. E-cigarette, or vaping, product use associated lung injury (EVALI): case series and diagnostic approach. The Lancet Respiratory medicine, 2019.PMID 31711871
- [3]Begh R, Conde M, Fanshawe TR, et al. Electronic cigarettes and subsequent cigarette smoking in young people: A systematic review. Addiction (Abingdon, England), 2025.PMID 39888213
- [4]Soneji S, Barrington-Trimis JL, Wills TA, et al. Association Between Initial Use of e-Cigarettes and Subsequent Cigarette Smoking Among Adolescents and Young Adults: A Systematic Review and Meta-analysis. JAMA Pediatrics, 2017.PMID 28654986
- [5]Yuan M, Cross SJ, Loughlin SE, Leslie FM Nicotine and the adolescent brain. The Journal of physiology, 2015.PMID 26018031
- [6]Leslie FM Unique, long-term effects of nicotine on adolescent brain. Pharmacology, biochemistry, and behavior, 2020.PMID 32738256
- [7]Scragg R, Wellman RJ, Laugesen M, DiFranza JR Diminished autonomy over tobacco can appear with the first cigarettes. Addictive behaviors, 2008.PMID 18207651
- [8]Rubinstein ML, Benowitz NL, Auerback GM, Jacob P 3rd Rate of nicotine metabolism and withdrawal symptoms in adolescent light smokers. Pediatrics, 2008.PMID 18762498
- [9]Evins AE, Cather C, Reeder HT, et al. Varenicline for Youth Nicotine Vaping Cessation: A Randomized Clinical Trial. JAMA, 2025.PMID 40266580
- [10]Butler AR, Lindson N, Livingstone-Banks J, et al. Interventions for quitting vaping. The Cochrane database of systematic reviews, 2025.PMID 39777614
- [11]Rubinstein ML, Benowitz NL, Auerback GM, Jacob P 3rd A randomized trial of nicotine nasal spray in adolescent smokers. Pediatrics, 2008.PMID 18762494
- [12]Pbert L, Farber H, Horn K, et al. State-of-the-art office-based interventions to eliminate youth tobacco use: the past decade. Pediatrics, 2015.PMID 25780075
- [13]Kaliamurthy S, Camenga DR Clinical approach to the treatment of e-cigarette use among adolescents. Current problems in pediatric and adolescent health care, 2022.PMID 35534404
- [14]Cao DJ, Aldy K, Hsu S, et al. Review of Health Consequences of Electronic Cigarettes and the Outbreak of Electronic Cigarette, or Vaping, Product Use-Associated Lung Injury. Journal of medical toxicology, 2020.PMID 32301069
- [15]McKelvey K, Baiocchi M, Halpern-Felsher B Adolescents' and Young Adults' Use and Perceptions of Pod-Based Electronic Cigarettes. JAMA network open, 2018.PMID 30646249
- [16]Graham AL, Cha S, Jacobs MA, et al. A Vaping Cessation Text Message Program for Adolescent E-Cigarette Users: A Randomized Clinical Trial. JAMA, 2024.PMID 39110436