Paeds · adolescent-and-young-adult-medicine
Transition readiness and transfer from paediatric to adult health services
Also known as Health-care transition · Transition to adult care · Transfer of care · Transition readiness · Got Transition Six Core Elements · TRAQ transition readiness assessment · Paediatric to adult handoff
A fellowship approach to transition readiness and transfer from paediatric to adult health services: defining transition as a purposeful staged process distinct from transfer; applying the Got Transition Six Core Elements; assessing readiness across self-management, navigation, communication, legal and psychosocial domains with tools such as the TRAQ; building a portable medical summary and emergency plan; organising a warm handoff to a named adult primary and specialty home; managing chronic-condition populations (diabetes, congenital heart disease, cystic fibrosis, IBD, sickle cell disease, complex/technology-dependent and neurodevelopmental disability); re-engaging youth lost to follow-up; and comparing ANZ, UK, US and Canadian service models.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 17-year-old with type 1 diabetes has not seen an adult team and has no transition plan. At 18 the paediatric service sends a referral letter and stops. Eight months later he presents in diabetic ketoacidosis, having run out of insulin and never made it to adult clinic. This is the failure mode the whole topic exists to prevent, and it is common wherever transfer is treated as an administrative event rather than a clinical process. [12]
Health-care transition is the purposeful, planned movement of a young person from child-centred to adult-oriented health care, with continuous services before, during and after the move. Transfer is only one event inside that process — the administrative handoff of care and records to a named adult provider. Conflating the two is the central error. Transition can succeed with a transfer that is well prepared, and it can fail badly with a transfer that happens on a birthday with no preparation. [1] [2]
Why does the boundary matter so much? Adolescence is when a young person must take over the work their family has been doing — booking appointments, carrying the diagnosis, managing medicines, navigating an adult system — while also completing growth, education and identity formation. A chronic condition layers onto that developmental task. The paediatric model is family-led and coordinator-rich; the adult model expects the patient to lead and offers far less scaffolding. Without a bridge, the young person falls into the gap between two models that were never designed to meet. [1] [4]
The evidence is clear on two points. First, structured transition programmes improve engagement, disease-specific knowledge, satisfaction and self-management skills compared with usual care. Second, the unstructured default — age-based discharge with no adult home — produces loss to follow-up, relapse, and avoidable acute presentations, particularly in the youngest, most complex and least-supported young people. [6] [9]
The arc of a good transition
Introduce early
Start a transition policy by 11–12 years; normalise the idea with the young person and family.
Assess readiness
Use a validated tool (TRAQ) yearly as a teaching map, not a pass/fail gate.
Plan & document
Portable summary, emergency plan, adult provider search, legal and insurance preparation.
Transfer with a warm handoff
Named adult primary and specialty home; joint visit or direct introduction, not a cold letter.
Confirm integration
Verify first adult visit happened; short post-transfer follow-up; rescue if lost to follow-up.
Classification
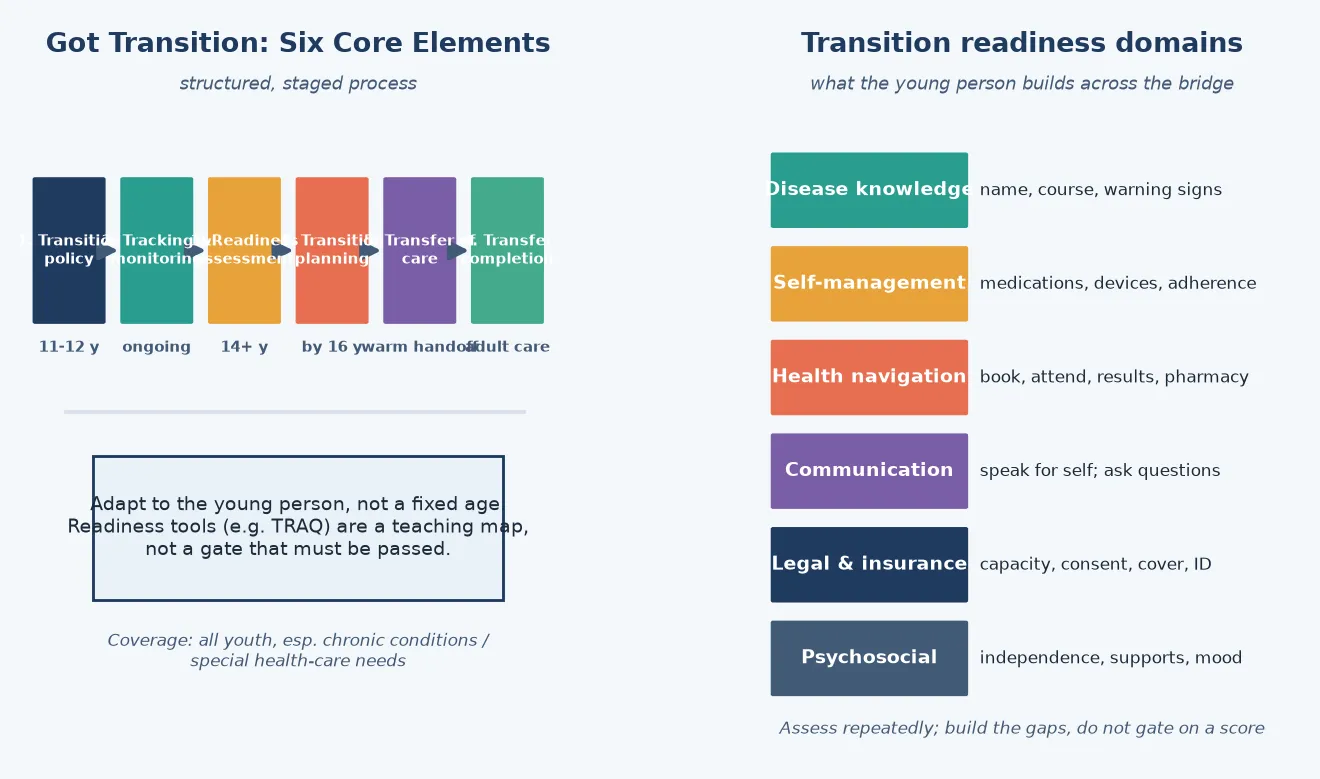
Classify transition work on two axes that change what you do next: the stage the young person has reached, and the readiness domains they have or have not yet built. Neither is a fixed age. [1]
The stage axis is the Got Transition Six Core Elements pathway, which gives the clinic a checklist-shaped spine. It begins with a written transition policy and ends only when the young person is settled in adult care. The readiness axis is the set of skills the young person must develop — knowing their condition, managing their own medicines, booking and attending appointments, speaking for themselves, handling insurance and legal status, and holding the psychosocial resilience to do all of this. A young person can be late in the pathway (stage 5, ready to transfer) but weak in several readiness domains, and that mismatch is exactly what the planning step exists to fix. [1] [3]
- Introduce transition policy
- Begin health knowledge at developmental level
- Start readiness tracking
- Low transfer pressure — build the base
- Active readiness assessment yearly
- Skill-building and adult-provider search
- Begin legal and insurance education
- Gradual shift of visit leadership to youth
- Finalise portable summary and emergency plan
- Warm handoff to named adult home
- Confirm first adult visit
- Post-transfer follow-up and rescue
The Six Core Elements are the most widely adopted structure internationally, but local tools differ. ANZ services often use hospital-based transition coordinators and the RCH Melbourne TRACe framework; the UK codifies transition in NICE NG43 and the RCPCH 'Coming of Age' principles; Canada uses CPS guidance; the US anchors on Got Transition with AAP/AAFP/ACP backing. The principle — a staged, documented, person-centred process with a warm handoff — is the same everywhere. [1]
Epidemiology & Risk Factors
Roughly one in five adolescents lives with a chronic condition, and a large and growing cohort with childhood-onset disease — type 1 diabetes, congenital heart disease, cystic fibrosis, inflammatory bowel disease, sickle cell disease, chronic kidney disease and transplants, complex and technology-dependent conditions, and neurodevelopmental disability — now survives into adulthood and needs an adult system that did not previously expect them. [1] [6]
The striking finding is not the size of the cohort but how few receive structured preparation. National data repeatedly show that only a minority of youth with special health-care needs report receiving the transition support they should — counselling on eventual adult care, help taking responsibility, and a written plan. The preparation gap is largest for those with the most complex needs, the least insurance, and the least system access. [10]
Disparities are the rule, not the exception. Transition preparation is unevenly distributed across race and ethnicity, insurance type, socioeconomic position, rurality and condition. The young people who need the most support — the most complex, the least resourced — are typically the least likely to receive a structured plan. This is a system-failure signal, not a patient-failure one, and it is the reason structured pathways, coordinators and active outreach are recommended rather than relying on the motivated family to navigate alone. [10] [9]
Pathophysiology
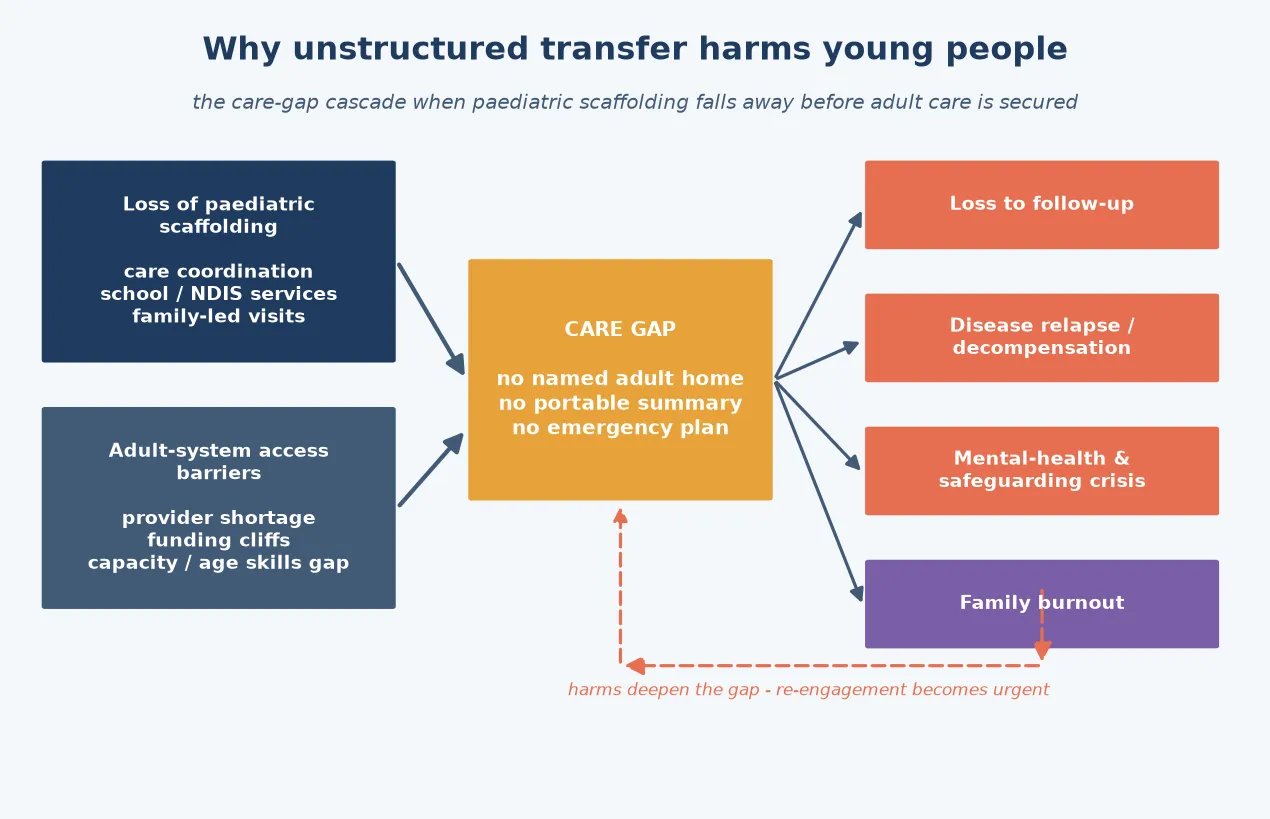
There is no single disease mechanism here, but there is a reliable harm mechanism: the care-gap cascade. It begins when the paediatric scaffolding that held the young person's care together is removed before adult care is secured. [1]
The paediatric model supplies a lot of invisible labour — a coordinator who chases no-shows, a family that holds the history, a school liaison, funded allied health and equipment. Adult care expects the patient to do most of that themselves and offers thinner coordination. When the move is unstructured, several things vanish at once: no named adult provider, no portable summary, no emergency plan, and no one whose job it is to notice the young person has gone quiet. [4] [7]
That vacuum collides with adult-system access barriers. Adult providers with the skills and capacity to take on complex childhood-onset disease are scarce. Insurance and funding may change abruptly at the age boundary. The appointment model is less family-friendly, and a young person who has never booked their own appointment may simply not arrive. Loss to follow-up is the predictable result, and once it happens, the young person's disease control, mental health and adherence can deteriorate silently until an acute crisis — ketoacidosis, a seizures, a transplant rejection, a mental-health emergency — surfaces the failure. [12] [7]
Two mediators determine whether the cascade is arrested or completed. The first is family and carer readiness: parents who are prepared, given a timeline and included in joint planning transfer responsibility more smoothly, while unsupported or burned-out families are associated with disengagement. The second is active re-engagement: a system that detects the no-show and chases it can rescue the young person before harm is done, whereas a system that waits for them to present loses them. The harm is not random — it concentrates in exactly the young people the default system was never built to catch. [5] [7]
Clinical Presentation
Transition problems present in a few recognisable shapes, and the presenting shape tells you which part of the pathway broke. [1]
The first is the unplanned adolescent: an older teenager still fully managed in paediatric services with no transition plan, no adult providers identified, and a family who has never been told this transition is coming. This is the latent failure — everything looks fine because the paediatric team is still providing excellent care, but the cliff is months away. [1] [2]
The second is the lost young adult: a patient in their late teens or early twenties presenting acutely to an adult or emergency service — diabetic ketoacidosis, a transplant or graft complication, a sickle-cell pain crisis, uncontrolled epilepsy or a mental-health crisis — who has had no health contact since paediatric discharge. The history of a recent paediatric "transfer" is the clue. [12] [11]
The third is the age-boundary crisis: a family in distress as legal, financial or decision-making arrangements change at the age of majority, with questions about capacity, guardianship or supported decision-making that were never addressed. The fourth is worsening control during the window: dropping adherence, rising HbA1c or disease activity, emerging anxiety or depression, or a young person who stops attending during the handover itself. [1] [4]
A fifth, subtler presentation is the administrative request: a form for a transition summary, an adult-service referral, a capacity or guardianship letter, or a disability or insurance application. Treating these as routine paperwork misses that they are often the first time the boundary problem becomes visible to the family. [7]
Differential Diagnosis
When a young person with a chronic condition deteriorates around the transition window, four explanations compete, and they change the management entirely. [1]
The first is true transition failure: the care gap described above, with loss to follow-up and loss of structure as the driver. The second is disease progression or a new adult-onset comorbidity that happens to coincide with the boundary — a progression that would have occurred anyway, or a genuine new problem. These two are not mutually exclusive, and a deterioration is often disease progression that was accelerated by loss of care. [6] [12]
- Care gap / loss to follow-up
- No adult home or summary
- Fix: re-engage + secure adult care
- Disease control drops with structure loss
- Natural history or new comorbidity
- Occurs with or without transition
- Fix: disease-specific escalation
- May be accelerated by the gap
- Insurance, cost, transport, time
- Cognitive or communication mismatch
- Fix: remove the barrier
- Not wilful non-adherence
- Depression, anxiety, self-harm
- Behavioural expression of unmet need
- Fix: mental-health + safeguarding
- Treat as urgent
The third is an access or adherence barrier masquerading as non-compliance: the young person who "won't take their insulin" may not be able to afford it, may not have a pharmacy, or may not understand adult instructions delivered without family present. Calling this non-compliance blames the patient for a system failure. The fourth is a mental-health or safeguarding crisis — depression, anxiety, self-harm, or exploitation of a dependent young person — which may present as behavioural disturbance or deteriorating control. Each of these needs a different response, and the job is to work out which driver (or combination) is in front of you before reaching for a disease-only fix. [4] [1]
Clinical & Bedside Assessment
Assess transition at a dedicated visit, not in the last five minutes of a routine clinic. Bring the young person and their carers together, then carve out protected time alone with the young person — this single change surfaces information families never hear. [1]
Take a structured self-management history: can the young person name their condition, list and take their own medicines, describe their warning signs and emergency plan, book and attend their own appointments, read a result, fill a prescription, and explain their insurance and legal status? Map this against the readiness domains, and the gaps become the curriculum for the next year. [3]
Use a validated readiness tool — most commonly the Transition Readiness Assessment Questionnaire (TRAQ) — to structure this. Treat the score as a developmental teaching map that tells you which skills to build, never as a gate the young person must pass before they are allowed to transfer. A low score is a reason to increase support, not to withhold a move that will eventually happen regardless. [3] [9]
Three further assessments complete the picture. Medication reconciliation ensures the drug, dose, supply and emergency plan are accurate and transportable. A legal and decision-making assessment establishes capacity, any supported-decision or guardianship arrangements, and insurance cover at the boundary. And a psychosocial assessment — mental health, housing, education or employment, family supports, and any safeguarding concern — identifies the young people who will need a heavier handoff. [1] [5]
Investigations
There is no "transition blood test," and that is the point: investigations at transition are condition-specific and purposeful, not a routine panel ordered for its own sake. [1]
Before transfer, update the disease-specific baselines the adult team will need — for example a recent HbA1c and screening for diabetes complications, a current echocardiogram and ECG for congenital heart disease, lung function and microbiology for cystic fibrosis, disease activity and surveillance for IBD, or transplant function and immunosuppression levels for a graft recipient. The goal is that the adult team inherits an up-to-date, complete picture and is not forced to repeat years of work or, worse, to miss a surveillance gap. [1] [12]
A second class of "investigation" is the readiness questionnaire itself, used as a structured assessment that produces a shareable record of where the young person is and what still needs building. A third is the documentation package, which functions as the investigation product of the whole process: a portable medical summary, problem list, medication and allergy list, emergency plan, care plans, key contacts, and the young person's preferences and goals. [1] [4]
A common trap is the endless deferral — "let's just do one more paediatric test before we transfer." Delaying transfer to complete marginal investigations is itself a form of transition failure, because it consumes the planning window and can push the young person past the age at which paediatric services can legally or contractually see them. Order what the adult team genuinely needs, then move. [1] [9]
Management — Resuscitation
Most transition work is planned and routine, but a small set of situations are urgent and need the same instinct as any resuscitation: secure the airway-equivalent first, which here means securing continuous care before the young person is harmed by its absence. [1]
The first is acute decompensation at the boundary: a young adult presenting in diabetic ketoacidosis, a transplant complication, a sickle-cell crisis, status epilepticus or a mental-health emergency after loss to follow-up. Resuscitate the acute problem as for any patient, then treat the loss of care as the underlying cause and re-engage adult services before discharge — do not resuscitate, discharge, and leave the same cliff in place. [12] [11]
The second is the medication or device failure after an unstructured transfer: insulin running out, a pump or home-ventilation issue, a feeding tube problem, or immunosuppression lapsing, with no adult team to call. Resolve the immediate issue, then make the portable summary and emergency plan exist before the next encounter. The third is a mental-health or safeguarding crisis surfacing at the boundary — assess risk, ensure safety, and involve mental-health and safeguarding services, recognising that the loss of paediatric supports may itself have precipitated the crisis. [1] [4]
The fourth urgent situation is lost-to-follow-up re-engagement, and it deserves resuscitation-grade urgency rather than a routine re-referral. A young person with a chronic condition who has dropped out of care is at predictable risk. Active outreach — phone, letter, a named coordinator — to bring them back is the rescue, and it should not wait for them to present acutely. [1] [6]
Management — Definitive & Stepwise
The definitive intervention is a structured, staged, documented process built around the Six Core Elements, applied to every young person with a chronic condition and intensified for the complex. It is not a form to complete at 17. [1]
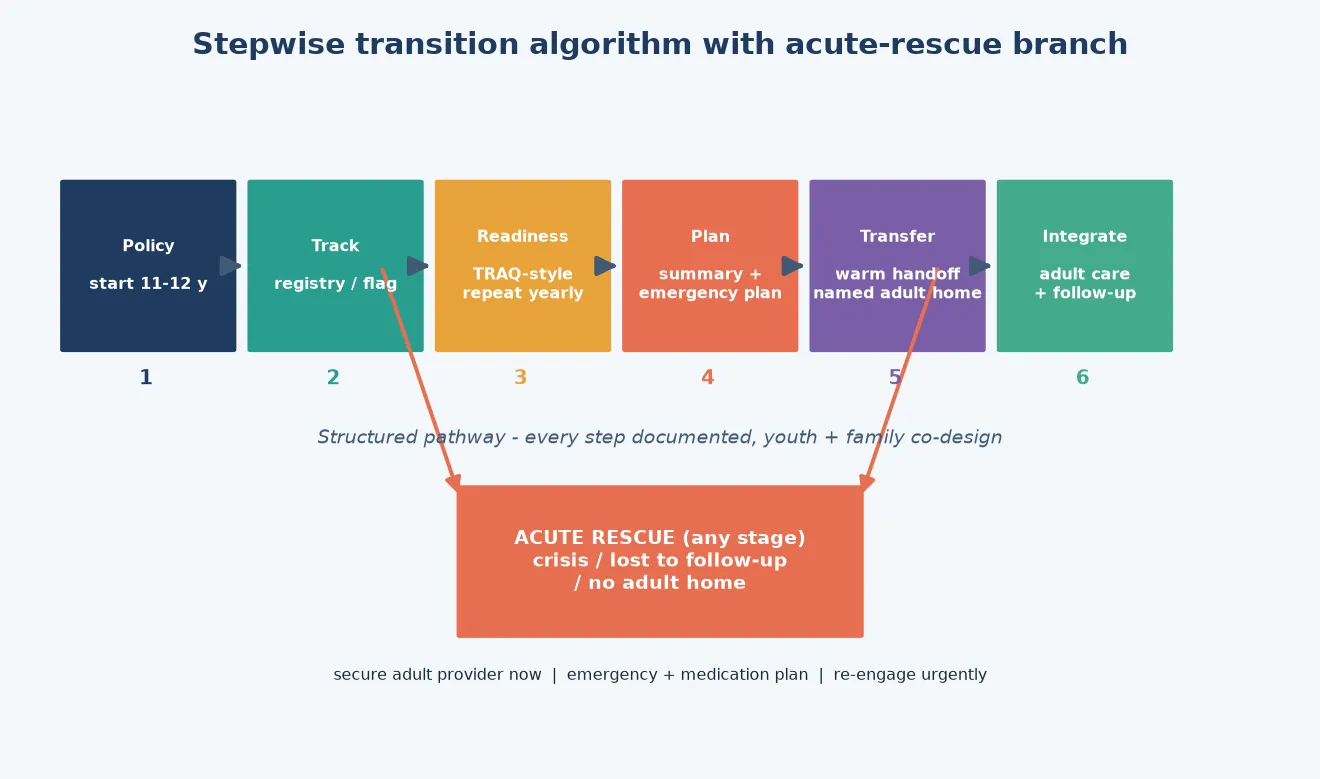
Begin with a transition policy introduced by early adolescence — a written statement, shared with the family, that care will move to adult services and that planning starts now. This normalises the move years before it happens and stops it landing as a surprise. Track every eligible young person on a registry or flag in the record so no one ages out unseen. [1] [2]
Assess readiness yearly with a validated tool, and use the result to teach — building the specific self-management, navigation and communication skills the score shows are missing. Then plan: produce a portable medical summary and a written emergency or safety plan, begin the search for adult primary and specialty providers, and start the legal, insurance and decision-making work the boundary will demand. [3] [4]
The transfer itself should be a warm handoff — a joint visit, a direct introduction, or a coordinator-warm handover to a named adult provider — never a cold letter into the void. Confirm the first adult appointment is booked, and ideally attended, before paediatric care steps back. Finally, complete the transfer with a defined period of post-transfer follow-up: a check that the young person arrived, is engaged, and has not fallen through. [1] [9]
The transfer package — what must travel with the young person
Portable summary
Diagnoses, problem list, past history, baseline results, family and social context.
Medications & allergy list
Current drugs, doses, supply, recent changes, allergies and adverse reactions.
Emergency / safety plan
What to do in a crisis — sick-day rules, seizure or pain plan, device failure, who to call.
Care plans & surveillance
Condition-specific plans, outstanding surveillance, next due investigations.
Key contacts & preferences
Named adult primary and specialty providers, coordinator, family contacts, goals and preferences.
Two cross-cutting supports make the pathway work. Family and carer preparation — a timeline, joint planning, gradual shift of visit leadership to the young person — is consistently associated with smoother transfer, because parents carry much of the invisible labour and their readiness mediates the young person's. Supported decision-making and capacity planning addresses the legal and ethical boundary directly: assess capacity, put supported-decision arrangements in place where needed, and prepare the documentation, without assuming capacity or incapacity. [5] [1]
Specific Subtypes & Scenarios
Each chronic-condition population carries a transition signature — the specific self-management skill, the specific adult home, and the specific failure mode the team must anticipate. [1]
Type 1 diabetes is the archetypal transition risk. The young person must own insulin self-management, carbohydrate counting and sick-day rules, and the adult endocrinology and diabetes-educator team must be identified before transfer. The documented failure mode is sharp: loss to follow-up after paediatric discharge with rising HbA1c and presentations in diabetic ketoacidosis. The handoff must be early, warm, and confirmed. [12]
Congenital heart disease requires transfer to a dedicated adult congenital heart disease (ACHD) service, not a general cardiology clinic. The lapse-of-care signal is strong and clinically important: gaps between paediatric and adult cardiac care are associated with worse outcomes, and the fix is an explicit, named ACHD referral tracked to attendance. [1] [6]
Cystic fibrosis is a success story of survival that created a transition challenge: many patients now reach adulthood and must move to an adult CF centre, with continued attention to infection-control segregation, adherence to complex therapies, and the developmental task of taking over an intensive daily regimen. Inflammatory bowel disease and solid-organ transplant recipients need continuity of immunosuppression, monitoring and a named adult subspecialist to avoid lapses. [6] [9]
Sickle cell disease and other haemoglobinopathies carry a high lapse-to-adult-care risk with serious consequences. Structured quality-improvement collaboratives — such as the sickle-cell transition learning collaborative model — have shown that coordinated transition support can improve adult-care engagement, and they illustrate how transition is as much a systems intervention as a clinical one. [11]
Complex chronic, technology-dependent and neurodevelopmental disability populations need the most intensive pathway. They often have multiple specialists, devices (home ventilation, feeding tubes, pumps), communication differences, and legal and capacity complexities, and they are served least well by the default adult system. The dedicated neurodevelopmental-disability transition leaf handles the detail; here the principle is the same but the intensity — coordinator involvement, supported decision-making, adult primary and specialty homes willing and able to accept the complexity — must be greater. [7] [1]
Finally, rural and remote transfer magnifies every barrier: thin adult specialist availability, distance, and thinner coordination. The out-of-home care and youth-justice interface adds safeguarding, advocacy and continuity dimensions that demand a named adult home and active outreach, because these young people are the most likely to be lost. [10] [1]
Complications & Pitfalls
The complications of transition are mostly the consequences of doing it badly, and they cluster into recognisable pitfalls. [1]
The cardinal pitfall is the abrupt birthday discharge: the 18-year-old sent with a letter and no adult clinic, who then disappears until an acute presentation. This is the failure the whole pathway is designed to prevent, and it remains common wherever transfer is treated as the endpoint. Closely related is transferring without a portable summary or emergency plan, so the adult team inherits a blank page and the young person has no safety net. [1] [6]
A second group is cognitive and ethical errors. Assuming capacity — or assuming incapacity — without a proper assessment mishandles the legal boundary and can deny a capable young person their autonomy or leave a vulnerable one unprotected. Using a low readiness score as a reason to withhold transfer, rather than to build skills and supports, abandons the young person at the cliff. And ignoring the young person's voice — especially when communication is atypical — replicates in transition the exclusion that disabled and complex young people face throughout care. [3] [7]
A third group is system and family errors. Misreading family burnout as non-engagement blames carers for the consequences of an unsupported system. Failing to chase the no-show completes the care-gap cascade. And allowing adult-system ableism, capacity assumptions or funding cliffs to block access turns a planned transfer into a refusal of care. Each pitfall has the same antidote: structure, documentation, a named adult home, and active outreach. [5] [10]
TRANSFER
Prognosis & Disposition
The prognosis of transition is the prognosis of the process, not of a disease. Structured programmes improve the outcomes that matter: engagement with adult care, disease-specific knowledge, self-management skills, satisfaction, and reduced loss to follow-up. The unstructured default predictably produces the opposite. [6] [9]
Markers of success are concrete and trackable: the young person attends their first adult appointment, retains a named primary and specialty home, demonstrates the self-management skills the readiness map targeted, reports confidence and continuity, and does not present acutely with a lapse-related complication. Family confidence and reduced carer stress are markers too, because the family carries much of the work. [1] [5]
Two disposition judgements recur. The first is when to delay transfer for clinical instability: if the young person is medically or mentally unstable, it is reasonable to hold them in paediatric or shared care and stabilise first — but this is a deliberate, documented decision, not drift, and it should not be extended indefinitely by marginal investigations. The second is what happens in the gap between services: a named coordinator, a transition nurse, a shared-care bridge or a navigator model should hold the young person during the handover, and someone's job must be to chase the no-show. [1] [4]
Disposition is ultimately about accountability: who holds this young person, who is responsible for confirming they arrived in adult care, and who notices when they do not. A pathway without a named owner is the pathway most likely to lose them. [9]
Special Populations
Some groups need the pathway intensified and adapted, because the default system serves them least well. [1]
Youth with intellectual and developmental disability and complex communication needs are at the sharpest end. They carry medical complexity, communication differences, legal and capacity questions, and adult services that are often not structured to accept them. The dedicated neurodevelopmental-disability transition leaf handles the detail; here the principles are intensified — supported decision-making, an adult primary home willing and able, coordinator involvement, and a refusal to gate transfer on a readiness score the young person's disability makes unattainable without support. [7]
Indigenous and culturally and linguistically diverse young people, and migrant and refugee families, face language, health-literacy, trust and system-navigation barriers that compound the transition gap. Culturally safe care, interpreter use, and outreach through trusted community and primary-care pathways are not optional add-ons but core to equitable transition. [10]
Gender-diverse youth may have specific health and psychosocial needs intersecting with their chronic condition; an inclusive, affirming adult service matters to engagement. Youth in out-of-home care and youth justice carry safeguarding, continuity and advocacy dimensions — they are among the most likely to be lost, and they need a named adult home and active outreach by default. [1] [4]
Socioeconomic disadvantage and insurance or funding cliffs at the age boundary can turn a planned transfer into an unaffordable one. Anticipating the financial and coverage change, and connecting the family to social work and entitlement support before the boundary, prevents cost from becoming the reason care lapses. Rural and remote young people face the same barriers magnified by distance and thin specialist availability, where telehealth-supported shared care and outreach can bridge gaps that geography otherwise widens. [10] [1]
Evidence, Guidelines & Regional Differences
The transition evidence base is real but maturing. The foundational guidance is the AAP/AAFP/ACP clinical report — originally 2011, updated in 2018 by White and Cooley — which defines transition as a process, endorses the medical home, and codifies the structured pathway. The Got Transition Six Core Elements operationalise that guidance and are the most widely used implementation tool internationally. [1] [2]
On outcomes, a Cochrane review of transition interventions found the evidence for specific models was developing, with limited but growing high-quality data. Subsequent systematic reviews — Gabriel 2017 and the Schmidt 2020 update — concluded that structured transition programmes show positive effects on engagement, disease knowledge, satisfaction and self-management, even while calling for more rigorous evaluation of disease-specific outcomes. [8] [6]
Regional models share the same spine but differ in scaffolding. The US anchors on Got Transition with AAP/AAFP/ACP backing and national surveys that track (and expose) the preparation gap. The UK codifies transition in NICE NG43 and RCPCH 'Coming of Age', emphasising a person-centred, staged process with continuity. ANZ services lean on hospital transition coordinators and frameworks such as the RCH Melbourne TRACe. Canada uses CPS guidance and condition-specific pathways. The principle is identical everywhere; the intensity of coordinator support and the funding structures differ. [1] [9]
Three controversies remain. The ideal transfer age is not fixed — it should be functional (readiness and stability), not chronological, though services inevitably have age limits. Mandatory readiness scores are debated: proponents value standardisation, but using a score as a gate risks abandoning the unready, and most guidance treats readiness tools as teaching maps. And adult provider capacity is the binding system constraint — you cannot complete a warm handoff to a home that does not exist, which is why transition is as much a health-system design problem as a clinical one. [4] [10]
The most useful recent evidence is the disparities and quality-improvement work. National data now quantify how unevenly transition support is distributed, and disease-specific learning collaboratives — the sickle-cell ST3P-UP model is a clear example — demonstrate that coordinated, measured transition support can move real outcomes. These reinforce that transition is a systems intervention measurable in engagement and lapse rates, not only in patient satisfaction. [10] [11]
Exam Pearls
The single highest-yield idea: transition is a process, transfer is an event, and the dangerous default is treating the event as the whole process. [1]
Start planning early (introduce a policy by 11–12 years) and transfer later, but only once a named adult primary and specialty home is secured and a portable summary plus emergency plan exists. A warm handoff, not a cold letter, is the standard. If an examiner asks what to send with the young person, answer with the transfer package — diagnoses, medications, emergency plan, surveillance, contacts and preferences. [1] [4]
Readiness tools (TRAQ) are a curriculum and support map, never a gate. A low score means build the skills and the adult supports, not withhold the move. Capacity is assessed, not assumed, and parents and carers need a transition too — their preparation mediates the young person's. [3] [5]
When asked to outline a plan, use the Six Core Elements as your skeleton: policy, tracking, readiness, planning, transfer, completion. When asked for the failure mode, name birthday discharge and loss to follow-up. When asked what is urgent, name re-engagement of the lost young adult. When asked about equity, name the disparities — preparation is the privilege of the supported, and structured pathways exist to close that gap. [1] [10] [6]
References
- [1]White PH; Cooley WC Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home. Pediatrics, 2018.PMID 30348754
- [2]American Academy of Pediatrics; American Academy of Family Physicians; American College of Physicians Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics, 2011.PMID 21708806
- [3]Sawicki GS; Lukens-Bull K; Yin X; Demars N; Huang IC; Livingood W; Reiss J; Wood D Measuring the transition readiness of youth with special healthcare needs: validation of the TRAQ--Transition Readiness Assessment Questionnaire. Journal of pediatric psychology, 2011.PMID 20040605
- [4]Suris JC; Akre C Key elements for, and indicators of, a successful transition: an international Delphi study. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2015.PMID 26003575
- [5]Suris JC; Larocca S; Akre C; Ambresin AE; Bel M; Kaufmann M; Paglia L; Roux N; Vidal C Transition from paediatric to adult care: what makes it easier for parents? Child: care, health and development, 2017.PMID 27625071
- [6]Gabriel P; McManus M; Rogers G; White P Outcome Evidence for Structured Pediatric to Adult Health Care Transition Interventions: A Systematic Review. The Journal of pediatrics, 2017.PMID 28668449
- [7]Fortune J; Cowan K; McClean L; Stelfox L; Stebbins A; Westrop C; Morris C Transition to adulthood: Perspectives from young people with cerebral palsy, parents, and health professionals. Developmental medicine and child neurology, 2026.PMID 42277597
- [8]Campbell F; Biggs K; Aldiss SK; O'Neill PM; Clowes M; McDonagh J; While A; Gibson F Transition of care for adolescents from paediatric services to adult health services. Cochrane Database of Systematic Reviews, 2016.PMID 27128768
- [9]Schmidt A; Ilango SM; McManus MA; Rogers KK; White PH Outcomes of Pediatric to Adult Health Care Transition Interventions: An Updated Systematic Review. Journal of pediatric nursing, 2020.PMID 31981969
- [10]Ilango SM; Schmidt A; McManus MA; Lemke KW; White PH Disparities in Health Care Transition Preparation Among US Youth. Pediatrics, 2025.PMID 40953840
- [11]Osunkwo I; Andemariam B; Beebe D; Mvula I; Riel R; Tanabe P; Walker A; Coyne I; Joshi S; Sharma D; Enderis M; Peugh J; Adams RJ; Britto MT; Anderson LM Results of a healthcare transition learning collaborative for emerging adults with sickle cell disease: the ST3P-UP study transition quality improvement collaborative. BMJ quality & safety, 2025.PMID 39577868
- [12]Lotstein DS; Seid M; Klingensmith G; Case D; Lawrence JM; Pihoker C; Cruz E; Anderson A; Peters AL; Wysocki T; Waitzfelder B; Bell RA; Todd L; Donnelly T; Dabelea D; Beck RW; Ponder S; Majcher S; Sivaprasad L; Deeb L; Laffel L; Holmbrook J; Greenbaum C; Blevins P; Goyer S; Fox LA; D'Agostino J; Foster N; Kollman C; Libman I; Lipman TH; Massias C; Maturo AC; Nadeau K; Petitti DB; Rodriguez-Vega D; Simmons JH; Tfayli H; Willi SM; Writing Group for the SEARCH for Diabetes in Youth Study Transition from pediatric to adult care for youth diagnosed with type 1 diabetes in adolescence. Pediatrics, 2013.PMID 23530167