Paeds · adolescent-and-young-adult-medicine
Youth violence, risky behaviour and injury prevention
Also known as Youth violence prevention · Adolescent injury prevention · Teen risky behaviour and safety · Public-health approach to youth violence · Lethal means counselling in adolescents · Positive youth development
A fellowship, public-health approach to preventing youth violence, risky behaviour and injury in adolescence: how to recognise the young person at risk, screen privately across violence, road, self-harm and weapon domains, stratify by prevention tier, and deliver evidence-based prevention from graduated driver licensing and safe firearm storage to positive youth development and lethal-means counselling across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old comes in for a sports check. You ask about seatbelts because that is easy. You do not ask about weapons, because that feels awkward. A year later the same teenager is shot dead in a friend's home by an unsecured firearm. The missed work was not a rare diagnosis. It was a five-minute question nobody asked, in the domain that kills more adolescents than any disease. [3] [6]
Injury is the dominant cause of death and disability in adolescence across high-income countries. Road crashes, violence, self-harm and overdose sit at the top of the list. These are not random acts of bad luck. They cluster in predictable patterns, they follow developmental and social risk, and they respond to prevention. [1] [4]
Youth violence is the intentional use of physical force or power by or against a young person that threatens or causes harm — bullying, fighting, weapon-carrying, assault, gang involvement, and teen dating violence all sit inside this frame. Unintentional injury is the same harm arriving without intent — road crashes, drowning, poisoning, and sport and recreation injury. The two are linked because they share risk drivers: impulsivity, intoxication, peer influence, access to means, and the developmental biology of adolescence. [1] [2]
The clinical skill is to treat violence and injury as a health problem you can act on, not a character problem you can only judge. The World Health Organization frames this as a four-step public-health model: define the problem, identify its causes, design and evaluate interventions, then scale up what works. Your consultation sits inside that fourth step. [1] [3]
The prevention encounter in sequence
Engage
Greet young person first, time alone, conditional confidentiality, non-judgemental stance.
Screen
Weave violence, road, self-harm, weapon and means questions into HEeADSSS.
Stratify
Sort into universal, selective or indicated prevention tier.
Prevent
Match the tier to evidence: GDL, safe storage, SEL/PYD, targeted programs, brief advice.
Safety plan
Lethal-means restriction, written plan, who to call tonight.
Follow-up
Timed review, low-threshold way back in, close referral loops.
Classification
Sort harm two ways at once: whether it is intentional or unintentional, and which prevention tier the young person sits in. The first tells you what kind of harm you are facing; the second tells you how heavy your response needs to be. [1] [4]
Intentional versus unintentional harm
Intentional harm includes youth violence (bullying, fighting, weapon-carrying, assault), teen dating violence, and self-harm and suicide. Unintentional harm includes road crashes, drowning, poisoning and overdose, and sport and recreation injury. The line blurs in adolescence because intoxication and impulsivity turn one into the other — a drunk fight is both violence and a head injury. [1] [12]
The universal–selective–indicated tiering
Universal prevention reaches every adolescent regardless of risk — seatbelt and helmet laws, graduated driver licensing, school-based social and emotional learning, and positive youth development. Selective prevention targets higher-risk groups — mentoring for disengaged youth, targeted violence-prevention programs, intimate-partner-violence support. Indicated prevention is for young people already affected — multisystemic or functional family therapy, trauma-focused care, supervised treatment and weapons-reduction programs. The clinician mostly operates at the universal and selective end; knowing the local indicated services matters because that is where you refer. [3] [4]
Risk behaviour as the connector
A risky behaviour is something a young person does that raises their chance of harm — substance use, impaired driving, unprotected sex, non-suicidal self-injury, carrying a weapon. Risk-taking is developmentally normal in adolescence. It becomes dangerous when it is frequent, impairing, escalating, or paired with access to lethal means. [10] [3]
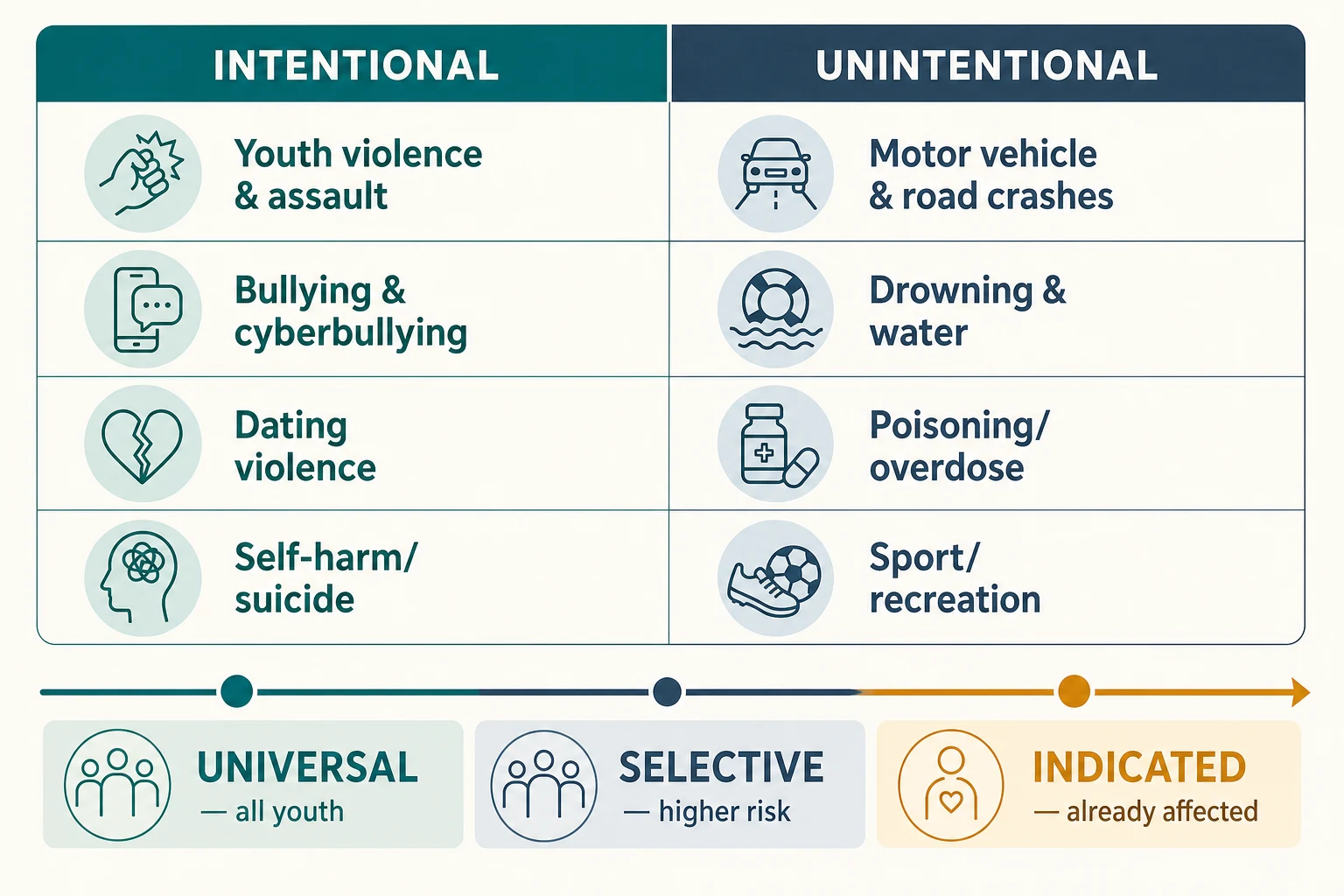
Read the figure like this: if your prevention advice never moves beyond "wear a seatbelt," you have lived entirely in one cell. The point of the matrix is to widen the brief — a single visit can touch road, weapon, self-harm and dating-violence rows at the universal tier. [3]
Universal
All youth
- GDL, seatbelt and helmet laws
- School-based SEL programs
- Positive youth development
- Safe-storage public messaging
Selective
Higher-risk groups
- Mentoring for disengaged youth
- Targeted violence-prevention programs
- Dating-violence support
- Substance-use brief intervention
Indicated
Already affected
- Multisystemic / functional family therapy
- Trauma-focused care
- Supervised treatment programs
- Weapons-reduction work
Epidemiology & Risk Factors
Injury is the leading cause of death in adolescence across high-income settings. Road crashes, violence, self-harm and overdose account for most of it, and the burden falls hardest on the young people with the fewest resources to protect themselves. [1] [12]
Risk is unevenly shared. Death and serious injury peak in the 15–24 age band and concentrate in young men, in those living in poverty, in rural and remote areas, among Indigenous and racialised groups, and in young people known to out-of-home care or youth justice. The same social forces that drive these patterns — structural inequity, racism, housing instability, community violence exposure — also reduce access to confidential, non-judgemental care. [3] [4]
Upstream drivers amplify risk in a stackable way. Adverse childhood experiences, family violence, access to firearms, substance use, peer delinquency, school disconnection and untreated mental illness each add load. When several stack, the chance of both violence perpetration and victimisation rises sharply. [2] [10]
The recent picture has shifted. Firearms have become a leading cause of adolescent death in the United States, while self-harm and mental-health burden have risen across high-income countries more broadly. These are not background trends; they change what a prevention conversation must cover. [6] [7]
Pathophysiology
You do not need a neuroscience degree to counsel an adolescent about safety. You do need one usable model of why this age group takes risks, because it explains why prevention works better than willpower and why access to means matters so much. [10]
The dual-systems model describes two developmental curves. The reward and socio-emotional system matures early and peaks through mid-adolescence. The cognitive-control system, anchored in the prefrontal cortex, matures later. The gap between them is the window of heightened risk-taking — wider under peer presence, emotional arousal, intoxication and sleep loss. [10]
This matters at the bedside. Under those loads, an adolescent may genuinely intend not to fight, not to drive drunk, not to act on a suicidal thought — and still act. Counselling that treats a broken promise as a moral failure ignores the biology. Counselling that lowers access to lethal means, delays exposure and builds skills works with the biology instead of against it. [10] [7]
Adverse childhood experiences add a second layer. They sensitise the stress-response system and raise, in a dose-response pattern, the risk of both violence perpetration and victimisation. So a young person who has grown up with violence is not "bad"; they are biologically and socially loaded toward the very harm you are trying to prevent, which is exactly why the conversation needs to be curious rather than punitive. [2] [3]
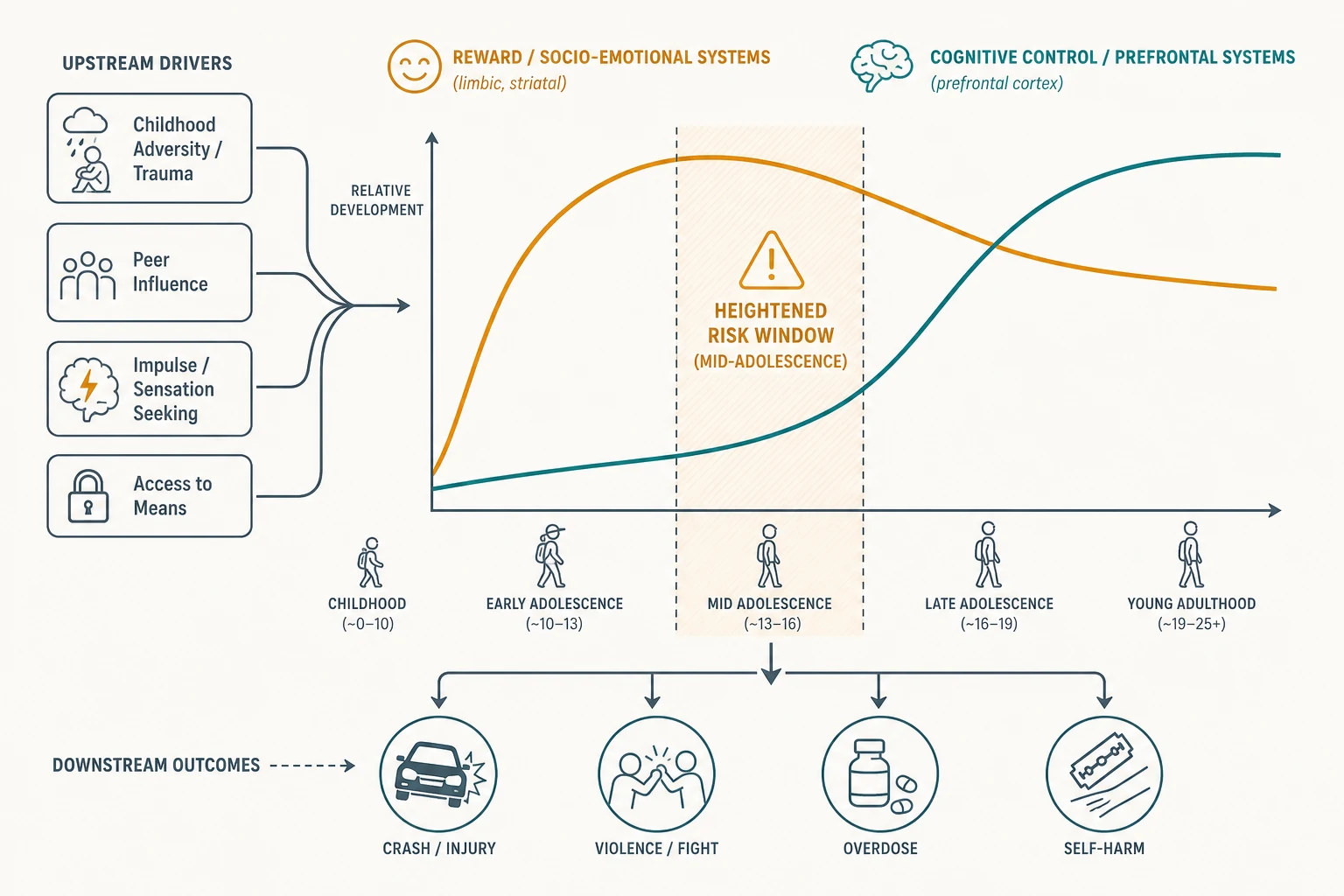
Read the figure like this: the shaded gap is not a character flaw. It is a developmental fact, widened by adversity. Your job is to shrink the harm inside the gap — by reducing access to firearms, large medication quantities and high-speed driving — not to lecture it shut. [10] [6]
Clinical Presentation
Risk and injury present across a spectrum, from openly disclosed to completely hidden. The most dangerous presentations are often the quiet ones, because nobody created the private space to find them. [9]
Organised low-risk presentation: the young person engages, private time is secured, the safety screen is negative, and protective factors are strong. The task is brief reinforcement, a strengths message, and a safety net. [3]
Higher-risk patterns hiding inside ordinary visits: unexplained or repeated injuries; frequent emergency-department attendance; school decline or sudden school refusal; sleep reversal dismissed as attitude; withdrawal or anger; a substance disclosure; or a parent who answers every question and blocks private time. Each is a door into a domain, not a reason to close the visit. [3] [12]
Violence presents on both sides. A victim may carry bruises, a weapon injury, fear, hypervigilance, or school avoidance. A perpetrator may disclose fighting, a suspension or disciplinary history, or weapon-carrying "for protection." Both need the same private, non-judgemental assessment, because today's perpetrator is often yesterday's victim. [2] [4]
Bullying and cyberbullying present as school refusal, low mood, self-harm, sudden withdrawal from a phone or device, or fear of school. Teen dating violence presents as isolation from friends, a partner who controls the phone and social media, missed appointments, unexplained injuries, anxiety, or hints at sexual coercion. Road risk hides in the ordinary — riding with an impaired driver, no helmet or seatbelt, speeding, or breaching graduated-licensing conditions. [11] [13]
Differential Diagnosis
In prevention work the differential is less "which disease" and more "what is driving the behaviour, and is it dangerous." Use function, frequency and access to means as your discriminators. [2]
| What it looks like | Safer framing question | Do not miss |
|---|---|---|
| A fighting or aggression history | Trauma exposure, family violence, mood or behavioural disorder | A treatable driver behind "delinquency" |
| Repeated or unexplained injury | Abuse, exploitation, intimate-partner violence, trafficking | Coercion hidden behind "risk-taking" |
| School refusal | Bullying or cyberbullying rather than defiance | A safeguarding concern under the label |
| Self-harm marks | Suicidal intent versus non-suicidal self-injury | Active suicide risk with means access |
| "Recreational" substance use | Frequency, dependence, impaired driving | Fentanyl exposure in counterfeit pills |
The core discriminator is function and danger. Normative experimentation sits alongside intact home, school and peer function. A behaviour accompanied by impairment, escalation, fear, or access to lethal means has crossed from normal risk into something you must act on. [10] [7]
Clinical & Bedside Assessment
1. Open and frame the visit
Greet the young person first, set a joint agenda, then secure time alone. State conditional confidentiality and its limits out loud and check understanding. Without this frame, the violence and safety screen will return false negatives — the young person will not tell you about a weapon they fear will be reported. [9] [3]
2. Weave violence and safety into HEeADSSS
HEeADSSS gives you the scaffold; the Safety domain is where violence and injury live. Ask about fighting, weapon-carrying, bullying as target and perpetrator, cyberbullying, teen dating violence, road risk (seatbelt, helmet, riding with impaired drivers), water and sport safety, and — every time — access to firearms and other lethal means. [9] [3]
3. Ask about bullying both ways
Ask "Has anyone bullied or hurt you?" and then ask "Have you ever bullied or hurt anyone else?" The second question catches the perpetrator side, which carries its own injury and legal risk and often points back to the young person's own victimisation. [11]
4. Screen teen dating violence safely and privately
Ask about conflict, control and coercion: does a partner check the phone, isolate the young person from friends, threaten them, or force sexual contact? Fear is the signal. Ask this only when you are certain you are alone and confidential. [13]
5. Assess access to lethal means
This is the single most-omitted high-yield question. Ask whether there is a firearm in the home or in the homes they visit, and how it is stored — loaded, unlocked, ammunition separate. Ask about large quantities of medication and other weapons. Counselling safe, locked, unloaded, ammunition-separated storage is a prevention act, and during a suicide-risk crisis it becomes temporary removal. [6] [7]
6. Build a safety and strengths formulation
Pull the findings into a picture that names the drivers, the protective factors, and a prevention tier. Share it with the young person in plain language. The formulation, not a screen score, drives the plan. [3] [8]
7. Document with care
Record enough for safety and continuity, and protect sensitive detail according to local record and portal rules. A portal or billing leak of confidential content — a disclosed firearm, a dating-violence disclosure — is a system-level harm that can endanger the young person. [3]
Investigations
Most prevention work needs few laboratory tests; it needs a thorough private history and the right questions. Investigation is selective and history-led. [3]
Useful adjuncts include validated screens used as triggers, not diagnoses — the ASQ or Columbia for suicide, CRAFFT or S2BI for substance use. After an injury or assault, document injuries with a body map and, where indicated, imaging and safeguarding photography. For young people who disclose injecting or escalating drug use, testing for blood-borne viruses is part of the work-up. [7]
Low-value patterns to avoid: routine broad blood panels on every asymptomatic adolescent; punitive toxicology that damages trust and suppresses disclosure; and treating a screen score as a diagnosis. [3] [12]
Management — Resuscitation
A routine prevention visit can become an emergency in one disclosure. Recognise the exit point and use it before you reach brief advice. [7]
- Stabilise physiology first: airway, breathing, circulation, glucose, and reversal of opioid toxicity with naloxone where indicated after an overdose. [7]
- Secure immediate safety for suicide risk: remove or reduce access to means (especially firearms), do not leave the young person alone, and activate the crisis or mental-health pathway. [7]
- Respond to disclosure of assault, dating violence or exploitation by following local safeguarding and mandatory-reporting duties, sharing the minimum necessary and telling the young person what must happen and why. [13] [3]
- Document the decisions, who was informed, and the safety plan. [3]
Lethal-means counselling is both a resuscitation and a prevention act: the same locked, unloaded, separated storage that lowers everyday risk is the temporary removal that may save a life during a suicide crisis. [6] [7]
Management — Definitive & Stepwise
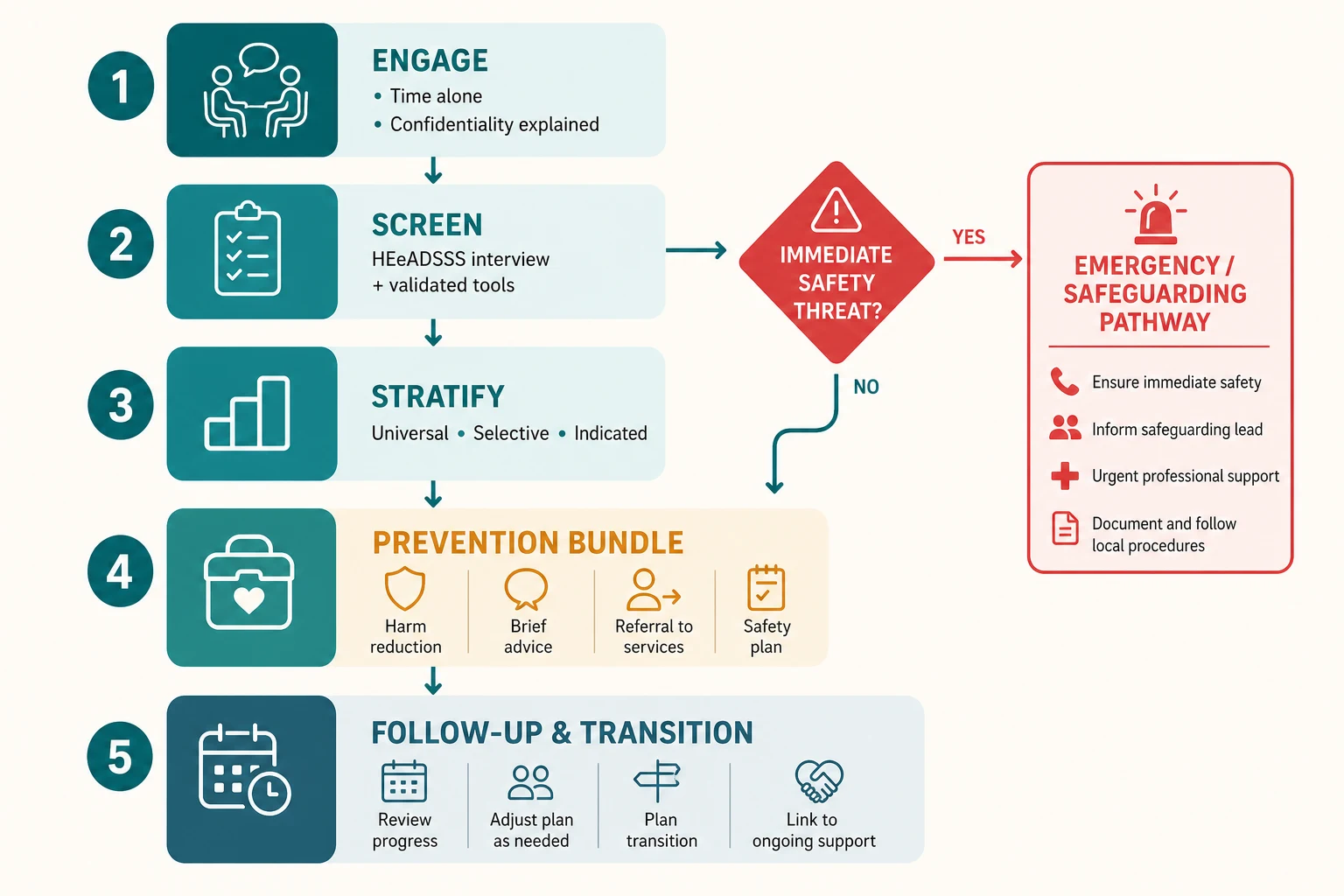
Read the figure like this: the red diamond is not decoration. Any immediate-safety finding exits the routine path before you reach brief advice. [7]
Stepwise routine pathway
- Engage and set the frame: time alone, conditional confidentiality, non-judgemental, strengths-based stance. [9]
- Screen: weave violence, road, self-harm, weapon and means questions into HEeADSSS; add ASQ or Columbia for suicide and CRAFFT for substance when a lead appears. [9] [7]
- Stratify: sort into universal, selective or indicated prevention tier. [3]
- Prevention bundle: match the tier to the evidence below, using brief, strengths-based advice and motivational-interviewing technique. [8]
- Safety plan and follow-up: a written plan, lethal-means restriction where indicated, who to call tonight, and a timed review. [7]
Match the intervention to the evidence
Road crashes fall with graduated driver licensing, seatbelt and helmet laws, and counselling against riding with an impaired driver. Firearm injury and suicide fall with safe firearm storage and lethal-means counselling — locked, unloaded, ammunition separated, and temporary removal in a crisis. Universal violence falls with school-based social-emotional learning and positive youth development, which show meta-analytic follow-up benefit. Higher-risk youth benefit from targeted programs; affected youth need indicated interventions such as multisystemic or functional family therapy. [5] [6] [8] [4]
Brief advice technique
Use motivational interviewing — open questions, affirmation, reflective listening, summaries — to help the young person articulate their own reasons for safer choices. A strengths-based, future-oriented message lands better than a fear-based lecture, and it keeps the door open for the next visit. [8] [3]
Road
Road crashes
- Graduated driver licensing
- Seatbelt and helmet every trip
- Never ride with an impaired driver
- Plan a safe way home
Firearms
Firearm injury & suicide
- Locked, unloaded, ammo separated
- Ask about homes they visit too
- Temporary removal in crisis
- Lethal-means counselling
Violence
Bullying & dating violence
- School SEL / PYD programs
- Ask bullying both ways
- Screen dating violence privately
- Safety plan for IPV
Self-harm
Suicide & NSSI
- Means restriction first
- ASQ/Columbia as a trigger
- Same-visit risk assessment
- Written safety plan + follow-up
Specific Subtypes & Scenarios
The road-safety conversation. Ask about seatbelt and helmet use, riding with impaired drivers, and graduated-licensing stages. Name the staged structure — learner, provisional or restricted, then full — and that breaching conditions (night driving, peer passengers) is where much of the risk concentrates. [5]
The firearm-in-the-home conversation. When there is a firearm, counsel safe storage: locked, unloaded, ammunition stored separately. Ask about homes the young person visits, not only their own. During a suicide-risk crisis, shift to temporary removal — the firearm leaves the home until the crisis resolves. This protects the young person without demonising the family. [6] [7]
Bullying and cyberbullying. Ask both ways. If a young person is a target, validate, assess for self-harm, and plan a safe school response — involve the school only with the young person's agreement unless safety overrides. Cyberbullying needs specific questions about online harassment, image-based abuse, and exclusion. [11]
Teen dating violence. Privately assess control, coercion and fear. Offer safety planning, confidential specialist referral, and clear information that abuse is not their fault. Do not contact the partner or family without the young person's explicit agreement. [13]
The weapon-carrying adolescent. A young person who carries a weapon "for protection" is telling you they feel unsafe. Understand the perceived threat, reduce access, and address the underlying safety need — which may be community violence, family violence, or exploitation. [2] [4]
Higher-baseline-risk settings. In youth-justice, out-of-home-care, rural-remote and chronic-disease settings, baseline risk is higher and records are fragmented. Reconstruct the history actively, clarify consent, and widen the screen. A chronic-disease clinic is not a reason to skip violence and self-harm questions. [3]
Complications & Pitfalls
- Treating risk-taking as delinquency and responding punitively, which suppresses disclosure and engagement at the next visit. [3] [2]
- Filing a weapon or violence disclosure without a safety plan or follow-up. [4]
- Missing intimate-partner violence or trafficking behind "adolescent relationship drama" or "risk-taking." [13]
- Forgetting to ask about firearms and lethal means — the single most common lethal omission in adolescent suicide prevention. [6] [7]
- Breaking confidentiality inappropriately, or refusing to break it when safety demands it; portal and billing leaks also breach trust. [3]
- Offering prevention advice in one domain (substance) while ignoring violence, road risk and self-harm. [9]
- Confusing a screen score with a diagnosis, or using toxicology punitively. [3]
Prognosis & Disposition
Prognosis here means the trajectory of risk, protective factors and connectedness, not a disease stage. [3]
Routine disposition: a complete low-risk visit with intact function and strong protective factors; brief strengths-based reinforcement, a safety net, and a planned interval. [8]
Early-review disposition: new violence exposure, dating-violence concern, school decline, or an incomplete assessment needing a return visit with trust built. [13] [11]
Urgent disposition: active suicide risk, overdose, weapon injury, assault, or medical instability — emergency department, crisis or safeguarding pathway as indicated, with follow-up loops closed. [7]
Engagement is fragile across adolescence and into young adulthood, so disposition should always name the next contact and a low-threshold way back in. Prevention succeeds when the young person returns. [3] [8]
Special Populations
Youth-justice and out-of-home-care adolescents. Highest cross-domain risk, most fragmented records, most trauma. Lead with reconstruction of the history and clarification of consent. [3]
Rural, remote and agricultural settings. Firearms are common and access differs; on telehealth, deliberately create a private audio space and ask who else is in the room. Dual relationships threaten confidentiality in small communities. [6]
Indigenous young people. Cultural safety, connection to community, and racism and colonisation as health exposures matter as much as any screening tool. Partner with local services. [3]
Migrant and refugee youth. Use a professional interpreter for confidential content; family interpreters are not equivalent. Apply trauma-informed pacing. [3]
Disabled and neurodiverse adolescents. Offer easy-read materials, longer slots, sensory adjustments, and capacity assessment. Avoid diagnostic overshadowing of violence, self-harm and substance risk. [3]
Socioeconomic disadvantage. Ask about food, transport, money and device access before attributing "non-adherence" to character. Prevention must be affordable and reachable. [3] [4]
Evidence, Guidelines & Regional Differences
The public-health model. The WHO world report on violence and health established the four-step public-health approach that frames violence as predictable and preventable, and reviews of youth violence apply it to developmental pathways and prevention challenges. [1] [2]
Road safety. Graduated driver licensing is one of the best-evidenced adolescent injury-prevention interventions; reviews show reduced crash rates through staged exposure to driving risk. [5]
Firearms and lethal means. Safe-storage and lethal-means interventions reduce firearm injury and suicide. Lethal-means counselling in emergency care is a critical opportunity for adolescent suicide prevention, and firearm-injury prevention reviews set out the clinician's role in safe-storage counselling. [6] [7]
Universal violence prevention. School-based social and emotional learning interventions show meta-analytic follow-up benefit on positive youth development, and structured positive-youth-development programs reduce violence and risk behaviour. [8]
Bullying and dating violence. Systematic reviews support family and educational strategies for cyberbullying prevention, and the Dating Matters comprehensive model shows effects on physical violence, bullying and sexual harassment in a cluster-randomised trial. [11] [13]
Unintentional injury. Behavioural risk factors — impulsivity, sensation-seeking, poor hazard perception — drive pediatric unintentional injury and point toward skills-based and environmental prevention. [12]
ANZ: youth-friendly confidential care culture; graduated-licensing schemes with night-driving and peer-passenger restrictions; expanding safe-storage messaging; RCH-linked adolescent resources; local mandatory-reporting statutes. UK: NICE safeguarding and self-harm pathways; PSHE and anti-bullying school programs; apply Gillick/Fraser capacity concepts with current local legal teaching; knife-crime-reduction context. US: AAP Bright Futures and CDC technical packages for youth violence, teen dating violence and suicide prevention; ASQ and Columbia dissemination; firearms a leading cause of adolescent death and state-variable firearm-storage and access laws; open-notes portal confidentiality tensions. Canada: CPS-aligned injury- and violence-prevention guidance; provincial consent variation; graduated-licensing and safe-storage messaging.
Exam Pearls
- Open every answer with time alone + conditional confidentiality before any violence or risk question. [9] [3]
- Define the WHO public-health approach in four steps: define the problem, identify causes, design and evaluate interventions, scale up. [1]
- Name injury as the leading cause of adolescent death; separate intentional from unintentional harm. [1] [12]
- Tier prevention: universal, selective, indicated. [3] [4]
- Match the prevention to the evidence: GDL for road, safe storage and lethal-means counselling for firearms and suicide, SEL/PYD for universal violence, targeted programs for higher risk. [5] [6] [8]
- Always ask separately about access to firearms and lethal means; never assume none. [6] [7]
- Ask about bullying both ways (target and perpetrator); ask about cyberbullying and dating violence by name. [11] [13]
- Use function, frequency and access to means to separate normative risk-taking from impairment, escalation and instability. [10]
- State that local statute governs licensing ages, reporting triggers and firearm-storage law; do not invent universal cut-offs. [3]
SAFE TEENS prevention bundle
References
- [1]Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R The world report on violence and health. Lancet, 2002.PMID 12384003
- [2]Dahlberg LL Youth violence. Developmental pathways and prevention challenges. American Journal of Preventive Medicine, 2001.PMID 11146255
- [3]Duke NN Youth Violence Prevention and Safety: Opportunities for Health Care Providers. Pediatric Clinics of North America, 2015.PMID 26318944
- [4]Santaella-Tenorio J, Wheeler K Youth Violence: Prevention and Control. American Journal of Public Health, 2021.PMID 34038157
- [5]Williams AF Graduated driver licensing (GDL) in the United States in 2016: A literature review and commentary. Journal of Safety Research, 2017.PMID 29203021
- [6]Gastineau KAB, Brantner ML, Gresham C, Lee LK Firearm Injury Prevention. Pediatric Clinics of North America, 2023.PMID 37865435
- [7]Krass P, Ballard E, Wolf A, Ranney ML Lethal Means Counseling in Emergency Care: A Critical Opportunity for Adolescent Suicide Prevention. Journal of Adolescent Health, 2026.PMID 42331501
- [8]Taylor RD, Oberle E, Durlak JA, Weissberg RP Promoting Positive Youth Development Through School-Based Social and Emotional Learning Interventions: A Meta-Analysis of Follow-Up Effects. Child Development, 2017.PMID 28685826
- [9]Cohen E, Mackenzie RG, Yates GL HEADSS, a psychosocial risk assessment instrument: implications for designing effective intervention programs for runaway youth. Journal of Adolescent Health, 1991.PMID 1772892
- [10]Steinberg L A Social Neuroscience Perspective on Adolescent Risk-Taking. Developmental Review, 2008.PMID 18509515
- [11]Tozzo P, Del Brusas F, Gennaro GD, Furlan P, Spolon R, Gabai A, Mucciaccia B, Caenazzo L Family and Educational Strategies for Cyberbullying Prevention: A Systematic Review. International Journal of Environmental Research and Public Health, 2022.PMID 36012084
- [12]Schwebel DC, Gaines J Pediatric unintentional injury: behavioral risk factors and implications for prevention. Journal of Developmental and Behavioral Pediatrics, 2007.PMID 17565295
- [13]Vivolo-Kantor AM, Niolon PH, McDugle K, Cornelius T, Le V, Giga NM, Godfrey E, Tay R, DeGue S Middle School Effects of the Dating Matters Comprehensive Teen Dating Violence Prevention Model on Physical Violence, Bullying, and Sexual Harassment: A Cluster-Randomized Controlled Trial. Prevention Science, 2021.PMID 31833020