Paeds · allergy-and-immunology
Allergic disease in children: integrated approach
Also known as Atopic disease in children · The atopic child · Atopic march · Paediatric allergy · Integrated allergy management · Food allergy, eczema, asthma and allergic rhinitis
Fellowship guide to the integrated allergic child: the shared type-2 mechanism and atopic march linking eczema, food allergy, asthma and allergic rhinitis; IgE versus non-IgE disease; challenge-proven epidemiology and natural history; early-allergen introduction (LEAP and EAT) and the skin-barrier story (KEEP and BEEP); the anaphylaxis diagnosis and the intramuscular-adrenaline-first rule; stepwise organ treatment; shared decision-making around oral immunotherapy; and one coordinated action plan for the whole child.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the child who arrives in clinic with itchy, dry skin in infancy, a frightening reaction to egg at the high-chair, wheeze through the pre-school winters, and a constantly blocked nose at school. Each presentation looks like a separate problem to a separate organ, but they are expressions of one atopic tendency, and the integrated approach treats that tendency rather than chasing each flare in isolation.[10]
Allergic disease in childhood is an immune dysregulation in which a Th2-skewed response generates allergen-specific immunoglobulin E against otherwise harmless environmental proteins, producing reproducible inflammation across skin, gut and airway. The four diseases that dominate practice are atopic dermatitis, food allergy, asthma and allergic rhinitis, and they cluster so predictably in the same children that the older term "atopy" is still the most honest shorthand for what is going on.[9]
The unifying emergency that runs across all of them is anaphylaxis, a rapid, life-threatening reaction that demands intramuscular adrenaline before any test is drawn. A child may live for years with eczema and rhinitis and never see a hospital, yet die in minutes from a peanut, so the action plan that puts an adrenaline autoinjector in the bag is the single most important outcome of every allergy consultation.[11]
Classification
The first bedside question is whether a given reaction is driven by immunoglobulin E, because that mechanism alone decides whether adrenaline belongs in the action plan. IgE-mediated reactions are rapid, reproducible and mast-cell-dependent, producing the immediate urticaria, vomiting, bronchospasm and anaphylaxis that follow a food within minutes, whereas non-IgE reactions such as food protein-induced enterocolitis syndrome and eosinophilic oesophagitis are delayed, cell-mediated and behave clinically and therapeutically like different diseases.[11]
The second question is which organ is affected, because that decides the stepwise treatment. Skin disease is eczema or urticaria, gut disease is immediate food allergy or the delayed non-IgE food disorders, the upper airway carries allergic rhinitis, and the lower airway carries asthma. Most atopic children have disease in more than one compartment at once, which is exactly why an organ-by-organ silo approach fails them.[10]
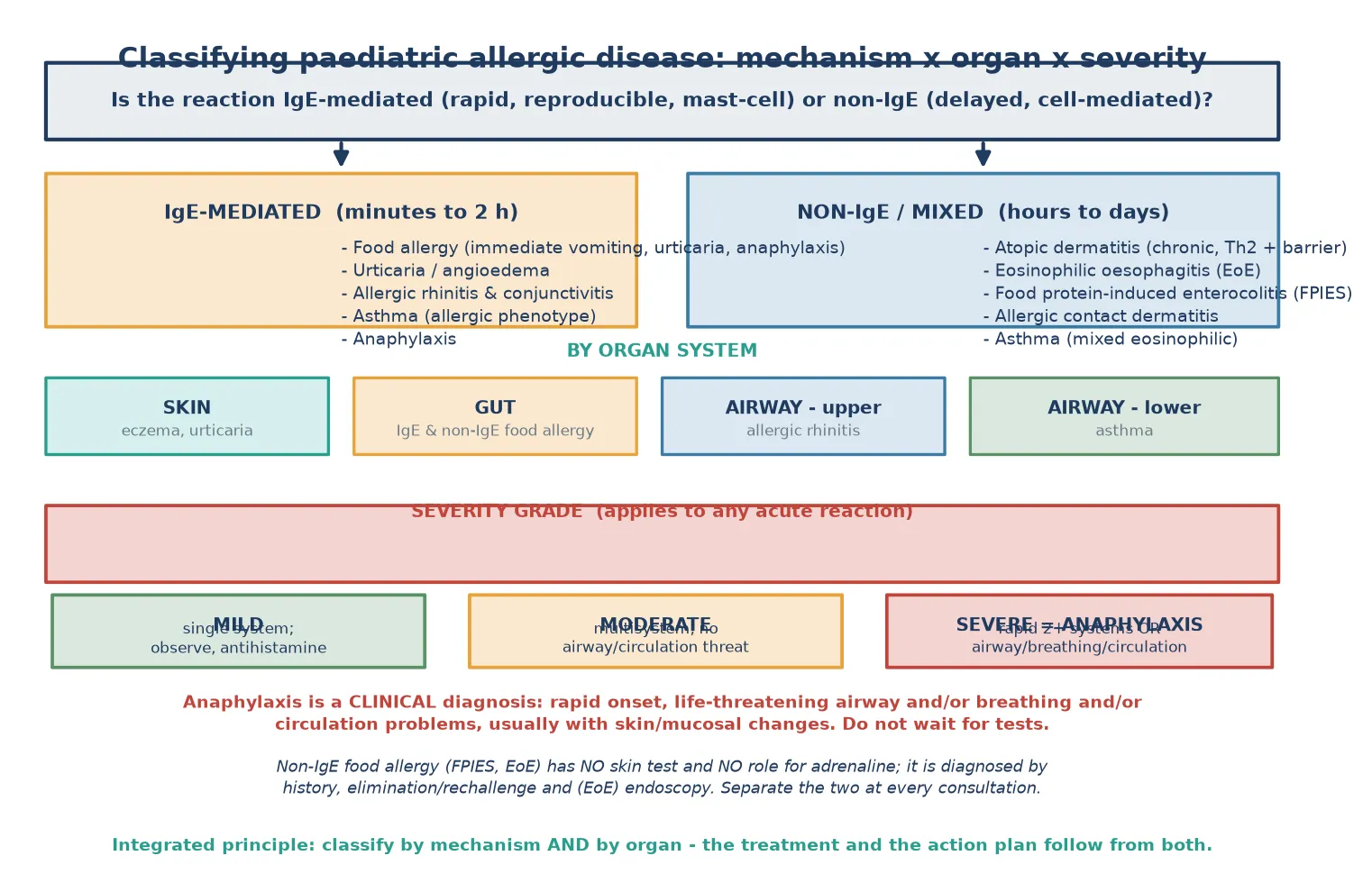
Severity is graded separately, and it is the grade that determines the disposition. A mild reaction involves a single system and is managed with observation and an antihistamine, a moderate reaction involves multiple systems without threat to airway, breathing or circulation, and a severe reaction is anaphylaxis, defined by rapid involvement of two or more systems or any threat to airway, breathing or circulation.[11]
The clinical trap is to treat every food reaction as IgE-mediated. A breast-fed infant with blood-streaked stools from non-IgE cow's-milk protein allergy does not need adrenaline, a skin-prick test or an autoinjector, and a child with eosinophilic oesophagitis needs endoscopy and dietary manipulation, not an avoidance list built on unreliable tests. Separating the two mechanisms at the first consultation is the classification skill that the exam rewards.[6]
Epidemiology & Risk Factors
Food allergy has become remarkably common in affluent countries, and the burden is clearest where challenge-proven rather than test-based diagnosis is used. The HealthNuts population-based cohort of Australian infants found challenge-proven, immunoglobulin-E-mediated food allergy in around one in ten, with peanut and egg the dominant culprits, establishing that food allergy is not a rare niche diagnosis but a routine part of general paediatric practice.[4]
The natural history is more reassuring than frightened families expect. Population-based follow-up of peanut allergy showed that roughly one in five children resolve it by four years of age, and egg allergy resolves even more readily, so a substantial minority of children will outgrow the very allergy that drove their earliest scares, which makes planned re-challenge a core skill rather than an optional extra.[5][6]
Risk factors cluster in two domains. Genetic risk is strong: a family history of atopy, a filaggrin gene loss-of-function variant producing an impaired skin barrier, and early-onset severe eczema all increase the chance of sensitisation. Environmental risk includes the modern affluent-country exposures of reduced microbial exposure, vitamin D insufficiency, delayed allergen introduction, and the skin-barrier inflammation that lets environmental allergen in through broken skin rather than through the gut.[10]
The atopic march describes the tendency for these diseases to appear in sequence in the same child, beginning with eczema and food allergy in infancy and progressing to allergic rhinitis and asthma in the pre-school and school years. The march is common but not inevitable, and the two interventions that have bent the curve are early repair of the skin barrier and early introduction of allergenic foods, both of which are covered below.[10][14]
Pathophysiology
The shared mechanism begins at a body surface. When a genetically predisposed child has an impaired skin or mucosal barrier, environmental allergen crosses that surface and meets dendritic cells, which present it to naive T cells and drive them toward the Th2 phenotype that defines atopy.[9]
The Th2 response is the engine of the whole syndrome. Interleukin-4 and interleukin-13 drive B cells to switch immunoglobulin production toward allergen-specific immunoglobulin E, which then binds the high-affinity Fc-epsilon receptor on mast cells throughout skin, gut and airway. Interleukin-5 sustains the eosinophilia that underlies both asthma and eosinophilic oesophagitis, so the same cytokine family damages multiple organs at once.[10]
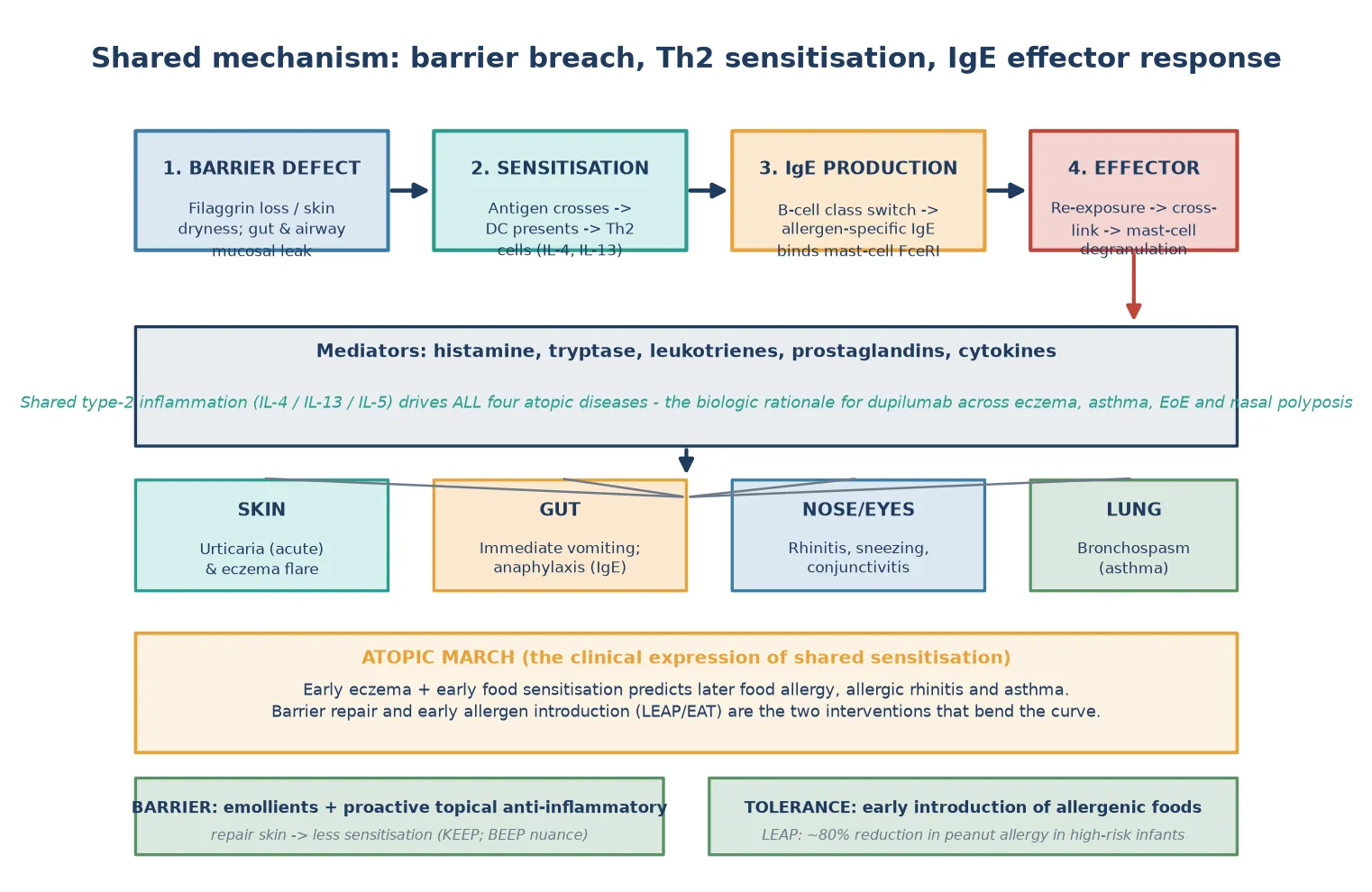
On re-exposure, the allergen cross-links adjacent immunoglobulin E molecules on the mast-cell surface, triggering degranulation and the release of histamine, tryptase, leukotrienes and prostaglandins. These mediators produce the immediate clinical picture of urticaria, bronchospasm, mucosal oedema and hypotension that the clinician recognises as the acute allergic reaction, and the speed of this cascade is the reason adrenaline must be given first.[11]
The chronic diseases use the same machinery in a lower gear. Atopic dermatitis is sustained Th2 and itch-scratch inflammation against a defective filaggrin barrier, asthma is chronic eosinophilic airway inflammation with bronchial hyper-responsiveness, and allergic rhinitis is type-2 inflammation of the nasal mucosa. This shared biology is the rationale for the monoclonal antibody dupilumab, which blocks the interleukin-4 receptor alpha chain and now treats severe eczema, severe asthma, eosinophilic oesophagitis and nasal polyposis in the one patient.[10]
The atopic march falls out of this mechanism directly. A child whose broken skin admits peanut or egg protein in infancy generates immunoglobulin E against that protein, and the sensitised mast cells then sit in the gut and later in the airway, ready to react when the allergen returns. Repairing the barrier early and introducing allergen through the gut rather than through inflamed skin is therefore the pathophysiological basis of prevention.[14]
Clinical Presentation
A practical integrated assessment works organ by organ but holds the whole child in mind. Eczema presents in infancy as itchy, dry, flexural dermatitis that disrupts sleep and is often complicated by Staphylococcus aureus colonisation and herpes simplex, and its severity in the first months of life is the single best predictor of later food allergy and asthma.[9]
Food allergy presents with reproducible reactions within minutes to two hours of the trigger, most commonly urticaria, angioedema, immediate vomiting, abdominal pain and, in the severe end of the spectrum, the airway, breathing and circulation compromise of anaphylaxis. The non-IgE food disorders present differently: cow's-milk protein allergy in infancy with blood-streaked stools, mucus and distress, and eosinophilic oesophagitis in the older child with reflux-like pain, feeding difficulty, food impaction and faltering growth.[6]
Asthma in the atopic child presents as recurrent wheeze, chest tightness, exercise limitation and nocturnal cough, with symptoms between viral colds, on exercise, on allergen exposure and overnight distinguishing true asthma from transient virus-associated wheeze. Allergic rhinitis presents with sneezing, itching, clear rhinorrhoea and congestion, often with ocular symptoms, and chronic disease brings mouth-breathing, snoring, poor sleep, the allergic salute and the facial stigmata of long-standing disease.[16]
Anaphylaxis is the presentation that overrides everything else. It is defined clinically as a rapid reaction with life-threatening airway or breathing or circulation problems, usually with skin or mucosal change, and the history of a trigger within the preceding minutes is what should make the clinician act before any test returns. The classic error is to wait for certainty in a child who is clearly deteriorating.[11]
Differential Diagnosis
The integrated approach demands a working differential for each organ while keeping the overlap in mind. An itchy rash is most often atopic dermatitis but may be seborrhoeic dermatitis in early infancy, scabies in an intensely pruritic child with burrows and family contacts, contact dermatitis where the distribution matches an exposure, or immunodeficiency-associated eczema when the child also has failure to thrive, infection and a family history of consanguinity.[9]
Recurrent wheeze is usually asthma or virus-associated wheeze but may be foreign-body aspiration when a toddler has a sudden choking event and persistent unilateral findings, cystic fibrosis when there is faltering growth and chest disease, primary ciliary dyskinesia when there is neonatal respiratory distress and situs abnormalities, or upper-airway obstruction masquerading as wheeze. The response to a bronchodilator and the pattern between episodes separate asthma from the rest.[16]
Chronic rhinitis is most often allergic but may be infectious, vasomotor, or drug-related, and the child with persistent unilateral discharge deserves suspicion for a foreign body. The food-reaction differential turns entirely on mechanism: an immediate reaction after the right food is IgE-mediated allergy until proven otherwise, but chronic loose stools, eczema flares and irritability in an infant may be non-IgE cow's-milk protein allergy, lactose intolerance, coeliac disease or eosinophilic gastrointestinal disease, each with its own confirmatory path.[6]
The most important differential skill is to separate anaphylaxis from its mimics, because the treatment differs entirely. A vasovagal faint after immunisation is pale, brief and bradycardic with immediate recovery on lying flat, whereas anaphylaxis is warm, flushed, tachycardic and progressive. Panic and vocal-cord dysfunction present with stridor or throat tightness but no skin change and normal oxygenation, and a breath-holding or seizure event can masquerade as a collapse until the history is taken carefully.[11]
Clinical & Bedside Assessment
Begin with a single history that spans every organ, because the allergic child rarely volunteers the rhinitis or the sleep disturbance when the family has come for the eczema. Ask about the onset, pattern and triggers of each complaint, the interval between exposure and reaction, the worst-ever reaction, the child's diet and growth, the family atopic history, and the social setting in which an action plan must be delivered.[10]
Examine the skin for the distribution and severity of eczema, signs of infection and the stigmata of chronic allergic disease such as the allergic salute, Dennie-Morgan folds and mouth-breathing. Examine the chest for wheeze and prolonged expirium, the nose for pale boggy turbinates and posterior drainage, and growth for the faltering that signals either an over-restricted diet or a serious non-atopic mimic.[9]
The synthesis for the exam long case is a one-sentence problem representation that names the mechanism, the organs involved and the integrated plan. A model statement is: "A four-year-old with early-onset severe eczema, challenge-confirmed peanut allergy with prior anaphylaxis, virus-triggered asthma and perennial allergic rhinitis has multisystem atopic disease and needs one coordinated plan covering skin control, an adrenaline action plan, an asthma action plan and school communication." That sentence tells the examiner you see the whole child.[10]
Assess the family's confidence and their barriers, because a plan that the family cannot execute saves no one. Ask who cares for the child, whether carers can use an autoinjector, whether the school will hold and administer it, what language the family reads, and how food is shared in their culture. The integrated assessment ends with the practical question of whether this plan can actually be carried out in this family's life.[12]
Investigations
Testing exists to confirm a history, not to screen for allergy, and over-testing is one of the commonest causes of harm in this field. A positive skin-prick test or serum-specific immunoglobulin E indicates sensitisation, not clinical allergy, and a child who eats the food without reaction is not allergic however large the number; the diagnosis rests on a clear history plus either a convincing reaction or a supervised oral food challenge.[4]
The oral food challenge remains the gold standard and the reference test against which all others are judged, and it is the only test that can confirm resolution and lift a restriction. A challenge is performed in a supervised setting with trained staff, incremental dosing, a clear stopping criterion and resuscitation equipment, and it converts the frightening label of lifelong allergy into a manageable, often temporary, diagnosis.[5]
Component-resolved diagnostics refine risk in selected cases. A child sensitised to the stable storage proteins of peanut such as Ara h 2 is more likely to have systemic allergy than one sensitised only to the labile proteins that cross-react with pollen, so component testing can spare some children a challenge while sharpening the indication for one in others. A serum tryptase taken within one to two hours of an anaphylactic reaction supports the diagnosis retrospectively when it was missed in the heat of the moment.[11]
For the non-IgE disorders the testing philosophy is entirely different. Food protein-induced enterocolitis has no role for skin testing and is confirmed by standardised oral challenge after elimination, while eosinophilic oesophagitis is confirmed by endoscopy with biopsy showing eosinophil-predominant inflammation. Atopic dermatitis and asthma are clinical diagnoses supported by pattern and, for asthma from around five years, by reversible airflow limitation on spirometry.[9]
Management — Resuscitation
The only acute allergic emergency is anaphylaxis, and its management is built around intramuscular adrenaline given without delay. The dose is 10 micrograms per kilogram of 1 in 1000 adrenaline, to a maximum of 500 micrograms in older children, delivered into the anterolateral thigh and repeated after five to fifteen minutes if there is no response.[11]
Adrenaline (epinephrine) 1:1000 IM
Dose
10 micrograms/kg (0.01 mL/kg of 1:1000)
Position and supportive care matter as much as the drug. Lie the child flat with the legs raised to preserve venous return, give high-flow oxygen, establish intravenous access for fluid if the child is shocked, and avoid the upright posture that can precipitate empty-venous cardiac arrest. Fluid boluses of 10–20 mL per kilogram of isotonic crystalloid are appropriate for the shocked child who does not respond rapidly to adrenaline.[11]
Antihistamines and corticosteroids are adjuncts, not treatment, and their main role is symptom relief for urticaria and possibly the reduction of late-phase reactions. The dangerous habit is to reach for an oral antihistamine in a child who is actually anaphylactic, because the time spent swallowing and absorbing a tablet is the time in which the airway can close. Adrenaline intramuscularly is the only drug that reverses anaphylaxis.[11]
Observe every treated child for a biphasic reaction, which can recur four to twenty-four hours after the first even without re-exposure. The standard observation is several hours of monitoring after resolution, longer for severe or refractory cases, and every child is discharged with a loaded adrenaline autoinjector, a written action plan and a clear plan for follow-up.[12]
Management — Definitive & Stepwise
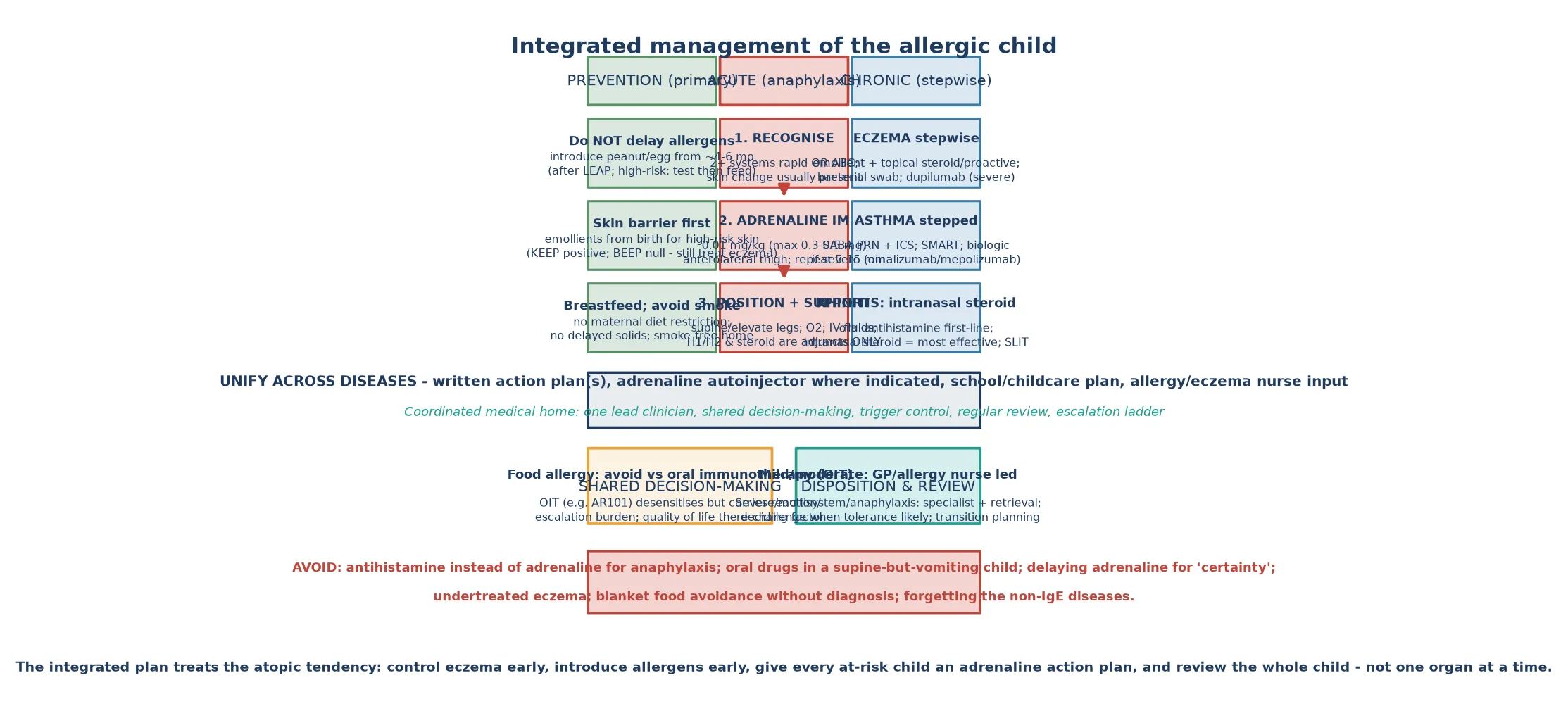
The definitive, integrated plan has three lanes that run in parallel for the whole atopic child: prevention, acute anaphylaxis readiness, and stepwise chronic control of each organ. The lane that is foregrounded depends on the child, but no integrated plan is complete until all three have been addressed.[10]
Prevention has been transformed by the early-introduction evidence. The LEAP trial showed that early peanut introduction from four to eleven months in high-risk infants reduced peanut allergy at five years by around 80 per cent, and the EAT trial showed a signal toward reduced allergy with early introduction of multiple foods in the general breast-fed population. The NIAID addendum guideline operationalised this by recommending peanut introduction from around four to six months, with testing-then-feeding for the severe-eczema or egg-allergic infant who is the highest-risk group.[1][2][3]
The skin-barrier lane is more nuanced. The Japanese KEEP trial showed that neonatal emollient application reduced eczema in a high-risk cohort, but the larger UK BEEP trial found no overall reduction in eczema at two years with daily emollient from birth, and its five-year follow-up confirmed no lasting prevention benefit. The integrated message is that aggressive treatment of established eczema is essential, but routine emollient from birth for all infants is not proven prevention.[14][15]
Chronic stepwise control is then applied organ by organ. Eczema is managed with a foundation of emollients and bleach-bath or wash decolonisation, a proactive regimen of topical corticosteroid or calcineurin inhibitor for flares and weekend proactive therapy for recurrent disease, treatment of infection, and dupilumab for the severe, unresponsive child. Asthma is stepped from a short-acting bronchodilator as needed to inhaled corticosteroid as a daily preventer, with a single-inhaler maintenance-and-reliever regimen now preferred for many children, and a biologic such as omalizumab or mepolizumab for severe disease. Allergic rhinitis is managed with an oral non-sedating antihistamine first-line and an intranasal corticosteroid, the most effective single therapy, with sublingual immunotherapy reserved for confirmed, troublesome disease.[9][16]
Anaphylaxis first-line - 'AAA'
The food-allergy lane adds the avoid-versus-immunotherapy decision. Standard management is strict allergen avoidance, an adrenaline autoinjector, a written action plan, and regular review for resolution, and this remains the right plan for most children. Oral immunotherapy with agents such as AR101 desensitises a majority of peanut-allergic children, but the PACE meta-analysis confirmed it carries a substantial burden of reactions and adrenaline use during treatment, so the decision is a shared one built around quality of life rather than a reflexive escalation.[7][8]
Anaphylaxis in the community - the child and the carer
1. Recognise: skin change + airway/breathing/circulation after a trigger
2. Give adrenaline IM into the thigh through the autoinjector
3. Lie the child flat with legs raised; call an ambulance
4. Second autoinjector at 5-15 min if no response
5. Seek medical review; never assume it is over
Specific Subtypes & Scenarios
The severe-eczema infant is the highest-yield integrated scenario because this is the child who will go on to develop the rest of the march. A six-month-old with early-onset, widespread, sleep-disrupting eczema deserves aggressive skin therapy, assessment for peanut and egg sensitisation with test-then-feed introduction, and early review for wheeze, because this single presentation predicts the next five years.[10]
The food-allergic adolescent is the highest-risk anaphylaxis scenario in practice. Risk-taking, expanded eating away from home, reluctance to carry an autoinjector and the sheer volume of novel food exposure combine to make adolescence the peak age for fatal food anaphylaxis, so the integrated plan for this age group foregrounds empowerment, a discreet autoinjector, peer awareness and transition to adult allergy care.[12][13]
The child with multiple food allergies and faltering growth is the scenario where over-restriction causes harm. A blanket elimination diet imposed on the basis of large but clinically meaningless specific immunoglobulin E numbers can deprive a growing child of calories, calcium and protein, and the integrated task is to replace avoidance with confirmed-diagnosis-led restriction, dietetic support, and planned challenges to lift unnecessary bans.[4]
The child with non-IgE food disease is easily missed because the testing paradigm of skin-prick and specific immunoglobulin E does not apply. A breast-fed infant with bloody, mucousy stools has non-IgE cow's-milk protein allergy and needs maternal dairy elimination or an extensively hydrolysed formula, with no autoinjector and no skin test; an older child with refractory reflux and food impaction may have eosinophilic oesophagitis and needs endoscopy and a proton-pump inhibitor or elimination diet. Recognising these as separate diseases with separate algorithms prevents both overtreatment and dangerous reassurance.[6]
The rural and remote atopic child faces the integrated challenge of distance. Specialist allergy services may be hundreds of kilometres away, an oral food challenge may require travel and a waiting list, and the autoinjector and action plan may be the only immediate safety net. Telehealth-supported allergy care, regional nurse-led eczema services, and a clear retrieval pathway for anaphylaxis are the structural elements that close this gap.[12]
Complications & Pitfalls
The most feared complication is fatal anaphylaxis, and it is rare but concentrated in identifiable groups. Adolescents and young adults, those with asthma, those who delay adrenaline, those who do not carry their autoinjector, and those with a previous severe reaction carry the highest risk, and the integrated plan that addresses each of these is the plan that prevents death.[12][13]
Chronic disease brings its own complications. Untreated eczema causes sleep loss, secondary infection, scarring and the sensitisation that drives the march; undertreated asthma causes exercise limitation, exacerbations and lung-remodelling; and untreated allergic rhinitis impairs sleep, school performance and worsens asthma control. The complications of the integrated disease are the sum of unmanaged disease in each organ.[10]
The iatrogenic complications are as important. Over-restricted diets cause faltering growth and nutritional deficiency, indiscriminate testing produces false positives that cascade into unnecessary avoidance, and the mislabelling of a non-IgE reaction as IgE-mediated imposes an autoinjector and an anxiety the child does not need. A confident, mechanism-based plan prevents all three.[4]
The classic exam pitfalls are worth naming because examiners return to them. Giving an antihistamine instead of adrenaline for anaphylaxis, sitting the child upright, withholding the autoinjector to confirm the diagnosis, building an avoidance diet on an unconfirmed test, and forgetting to address the asthma in the food-allergic child are the five errors that cost the most marks and the most lives.[11]
Prognosis & Disposition
The prognosis for the integrated atopic child is generally good but demands active management over years. Most children outgrow their egg and milk allergy, a substantial minority outgrow peanut allergy, asthma severity often improves into adolescence, and rhinitis becomes a manageable chronic condition, so the family should be told that the trajectory is toward improvement with the right plan rather than toward lifelong disease.[5][6]
The disposition is layered. A well child with mild single-organ disease and no history of anaphylaxis is managed in the primary-care medical home with an allergy or eczema nurse. A child with multiple allergies, prior anaphylaxis, severe asthma or faltering growth needs specialist allergy and respiratory input, a dietitian, and a coordinated plan, and a child with refractory anaphylaxis or severe asthma belongs in a service with access to biologics, desensitisation programs and retrieval.[12]
Long-term follow-up is built around planned review and re-challenge. Serial specific immunoglobulin E trends guide when to challenge, the oral food challenge confirms resolution and lifts restrictions, asthma is reviewed against a written action plan with stepped up or down therapy, and the adolescent is transitioned to adult care with the autoinjector, the plan and the confidence to use both. The integrated clinic that sees the whole child once, rather than each organ separately, is the model that delivers this trajectory.[10]
Special Populations
The food-allergic adolescent is the population in whom the stakes are highest and the engagement hardest. Autonomy, risk-taking, peer eating, alcohol and the desire not to stand out all conspire against safe management, so the integrated plan foregrounds a discreet autoinjector, peer and partner education, an unambiguous action plan, mental-health screening for the anxiety that chronic anaphylaxis risk produces, and structured transition to adult services.[13]
Migrant, refugee and asylum-seeker families may arrive with a different dietary culture, a different experience of food restriction through scarcity, and a language barrier to the written action plan. A professional interpreter, a plan translated into the family's language, and culturally appropriate food substitution are the elements that turn a generic plan into an executable one, and sensitisation patterns may differ from the host country so the history guides the testing rather than a standard panel.[12]
Indigenous and remote children carry a higher burden of skin infection and chronic disease, and the integrated approach must account for environmental health, housing crowding, hot-climate skin care and the distance to specialist services. Eczema in this context is often complicated by streptococcal and staphylococcal infection, scabies and impetigo, and the skin-control lane of the plan must be embedded in a broader primary-health and environmental-health response.[9]
Children in socioeconomic disadvantage face restricted access to autoinjectors, to the emollients and preventers that chronic control requires, and to the dietitian and specialist that complex disease needs. The integrated plan that cannot be afforded is no plan, so attention to subsidised access, to school-held autoinjectors, and to nurse-led shared-care models is part of competent paediatric allergy practice.[12]
Children with disability and neurodivergence may have sensory differences that make eczema therapy, mask use for asthma or dietary restriction particularly challenging, and their families need a plan adapted to the child's communication, sensory profile and routine. The integrated approach that works for the typically developing child is adapted, not abandoned, in this population.[9]
Evidence, Guidelines & Regional Differences
The evidence base for prevention has reshaped practice in the last decade. The LEAP trial's demonstration that early peanut introduction prevents allergy overturned decades of advice to delay allergens, and the NIAID addendum guideline, ASCIA guidance and the European EAACI guidelines all now recommend early introduction from around four to six months, with testing-then-feeding for the highest-risk infant. This is among the clearest examples in modern paediatrics of a randomised trial changing global guidance.[1][3]
The skin-barrier prevention evidence is more contested. KEEP showed benefit, BEEP did not, and the five-year BEEP follow-up confirmed no prevention signal, so the current consensus is to treat established eczema aggressively while not yet recommending universal neonatal emollient for prevention. This nuance is a common viva question because it tests whether the candidate can hold a positive and a negative trial in mind together.[14][15]
The oral-immunotherapy evidence is the area of sharpest shared decision-making. The PALISADE trial of AR101 and the PACE meta-analysis established that desensitisation is achievable but carries a reaction and adrenaline-use burden, and efficacy and safety must be weighed against the child's and family's quality of life. Guidelines therefore frame immunotherapy as an option, not a default, and the candidate who presents it as a nuanced shared decision outperforms the one who presents it as a cure.[7][8]
Regional differences are operational rather than scientific. Australasian practice uses ASCIA action plans and autoinjectors as standard, has strong school anaphylaxis legislation, and draws on population cohort data for prevalence; the United Kingdom and Europe use EAACI guidance with similar adrenaline-first messages; and North America follows the NIAID addendum with its test-then-feed pathway for high-risk infants. The shared science means the integrated plan transfers well across regions, with the variation in how the plan is delivered and funded.[16]
Exam Pearls
Carry these single-testable facts into the written and clinical exam. Anaphylaxis is a clinical diagnosis: rapid airway, breathing or circulation compromise with skin change after a trigger, treated with intramuscular adrenaline into the thigh, repeated at five to fifteen minutes, with the child laid flat. Antihistamines and steroids are adjuncts and never substitute for adrenaline. LEAP showed around 80 per cent reduction in peanut allergy with early introduction; the NIAID addendum recommends peanut from around four to six months, test-then-feed for severe-eczema or egg-allergic infants.[1][3][11]
The mechanism facts are high-yield because they explain the whole field. Atopy is Th2-skewed immunity with immunoglobulin E against harmless proteins; interleukin-4 and interleukin-13 drive class switching, interleukin-5 sustains eosinophilia, and dupilumab blocks the interleukin-4 receptor alpha chain and treats eczema, asthma, eosinophilic oesophagitis and nasal polyposis at once. The atopic march runs eczema to food allergy to rhinitis to asthma, and it is driven by barrier breakdown plus sensitisation.[10]
Finally, the integrated principle is the answer that distinguishes the fellowship candidate from the registrar. The allergic child is one child with one tendency expressed across skin, gut and airway, so the plan is one plan: control the skin, introduce the foods, carry the adrenaline, step the asthma and treat the rhinitis, with one lead clinician, one written action plan, and regular review of the whole child. That single organising idea is what the examiner is listening for.[10][11]
References
- [1]Du Toit G, Roberts G, Sayre PH, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy N Engl J Med, 2015.PMID 25705822
- [2]Perkin MR, Logan K, Tseng A, et al. Randomized Trial of Introduction of Allergenic Foods in Breast-Fed Infants N Engl J Med, 2016.PMID 26943128
- [3]Togias A, Cooper SF, Acebal ML, et al. Addendum guidelines for the prevention of peanut allergy in the United States: Report of the NIAID-sponsored expert panel J Allergy Clin Immunol, 2017.PMID 28065278
- [4]Osborne NJ, Koplin JJ, Martin PE, et al. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants J Allergy Clin Immunol, 2011.PMID 21377036
- [5]Peters RL, Allen KJ, Dharmage SC, et al. Natural history of peanut allergy and predictors of resolution in the first 4 years of life: A population-based assessment J Allergy Clin Immunol, 2015.PMID 25725989
- [6]Peters RL, Dharmage SC, Gurrin LC, et al. The natural history and clinical predictors of egg allergy in the first 2 years of life: a prospective, population-based cohort study J Allergy Clin Immunol, 2014.PMID 24373356
- [7]Vickery BP, Vereda A, Casale TB, et al. AR101 Oral Immunotherapy for Peanut Allergy N Engl J Med, 2018.PMID 30449234
- [8]Chu DK, Wood RA, French S, et al. Oral immunotherapy for peanut allergy (PACE): a systematic review and meta-analysis of efficacy and safety Lancet, 2019.PMID 31030987
- [9]Williams HC Clinical practice. Atopic dermatitis N Engl J Med, 2005.PMID 15930422
- [10]Spergel JM, Leung DYM, Calatroni A, et al. The atopic march: Where we are going? Can we change it? Ann Allergy Asthma Immunol, 2021.PMID 34479727
- [11]Sampson HA, Munoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: summary report Ann Emerg Med, 2006.PMID 16546624
- [12]Turner PJ, Jerschow E, Umasunthar T, et al. Fatal Anaphylaxis: Mortality Rate and Risk Factors J Allergy Clin Immunol Pract, 2017.PMID 28888247
- [13]Atkins D, Bock SA Fatal anaphylaxis to foods: epidemiology, recognition, and prevention Curr Allergy Asthma Rep, 2009.PMID 19348717
- [14]Horimukai K, Morita K, Narita M, et al. Application of moisturizer to neonates prevents development of atopic dermatitis J Allergy Clin Immunol, 2014.PMID 25282564
- [15]Bradshaw LE, Montgomerie AA, Glass BD, et al. Emollients for prevention of atopic dermatitis: 5-year findings from the BEEP randomized trial Allergy, 2023.PMID 36263451
- [16]Brozek JL, Bousquet J, Agache I, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines-2016 revision J Allergy Clin Immunol, 2017.PMID 28602936