Paeds · allergy-and-immunology
Allergic rhinitis and rhinoconjunctivitis
Also known as hay fever · AR · SAR · PAR · seasonal allergic rhinitis · perennial allergic rhinitis · allergic rhinoconjunctivitis
An IgE-mediated inflammation of the nasal and ocular mucosa driven by aeroallergen exposure, presenting with sneezing, itch, rhinorrhoea and congestion in children; classified by the ARIA framework and managed with a stepwise allergen-avoidance and pharmacotherapy ladder culminating in disease-modifying immunotherapy.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A school-aged child who rubs the tip of their nose upwards, sneezes in bursts each spring morning, and breathes through their mouth at night is the classic picture of allergic rhinitis. The problem is an immunoglobulin-E-mediated inflammation of the nasal mucosa triggered by inhaled aeroallergens, producing the quartet of sneezing, nasal itch, anterior rhinorrhoea and congestion. [3]
When the same allergic process inflames the conjunctiva, the term allergic rhinoconjunctivitis is used, reflecting how often the nose and eyes are affected together. The 2024–2025 ARIA-EAACI guideline reaffirms allergic rhinitis as the most common chronic allergic disease of childhood and a major driver of impaired school attendance, sleep disturbance and reduced quality of life. [1]
Epidemiology & Risk Factors
Allergic rhinitis affects roughly one in four children worldwide, and a 2023 systematic review and meta-analysis confirmed it is among the most prevalent chronic conditions of childhood, with pooled estimates climbing over recent decades in both high- and low-income settings. [2]
The atopic march describes the typical temporal sequence: atopic dermatitis and food allergy in infancy, followed by allergic rhinitis and then asthma through the preschool and school-age years, underpinned by shared Th2-skewed immunological pathways and filaggrin-related barrier defects. Children with allergic rhinitis have a roughly threefold higher risk of developing asthma than children without it, which is why the United Airway Disease concept places rhinitis and asthma on a single management continuum. [10]
Major risk factors include a family history of atopy, early sensitisation to aeroallergens (especially house-dust mite), urban versus rural residence, exposure to second-hand smoke, and reduced exposure to microbial diversity in early life — the hygiene hypothesis framing the protective effect of farm living and vaginal delivery. The prevalence of both allergic rhinitis and asthma is higher in children exposed to household pets under some circumstances and lower under others, depending on dose, timing and the specific animal. [2]
Pathophysiology
Allergic rhinitis is a type I, IgE-mediated hypersensitivity reaction that unfolds in two phases. In the sensitisation phase, inhaled allergen is taken up by antigen-presenting cells in the nasal mucosa, processed, and presented to naïve CD4-positive T cells, which polarise toward a T-helper-2 phenotype. These Th2 cells release interleukin-4 and interleukin-13, which drive B-cell immunoglobulin class-switching to allergen-specific IgE. [3]
The newly formed IgE coats mast cells and basophils in the nasal mucosa by binding high-affinity Fc-epsilon-RI receptors, and the child is now sensitised but asymptomatic. On re-exposure, allergen cross-links adjacent IgE–Fc-epsilon-RI complexes, triggering immediate mast-cell degranulation within minutes and the release of histamine, tryptase, prostaglandin-D2 and leukotrienes. [3]
This immediate reaction produces the classic symptoms: histamine drives sneezing, itch and watery rhinorrhoea, while leukotrienes and vasodilator mediators produce nasal congestion. A late-phase reaction follows four to eight hours later, marked by eosinophil and Th2-cell infiltration of the mucosa, which sustains congestion and renders the nose hyper-reactive to non-specific irritants like cold air and perfume. [14]
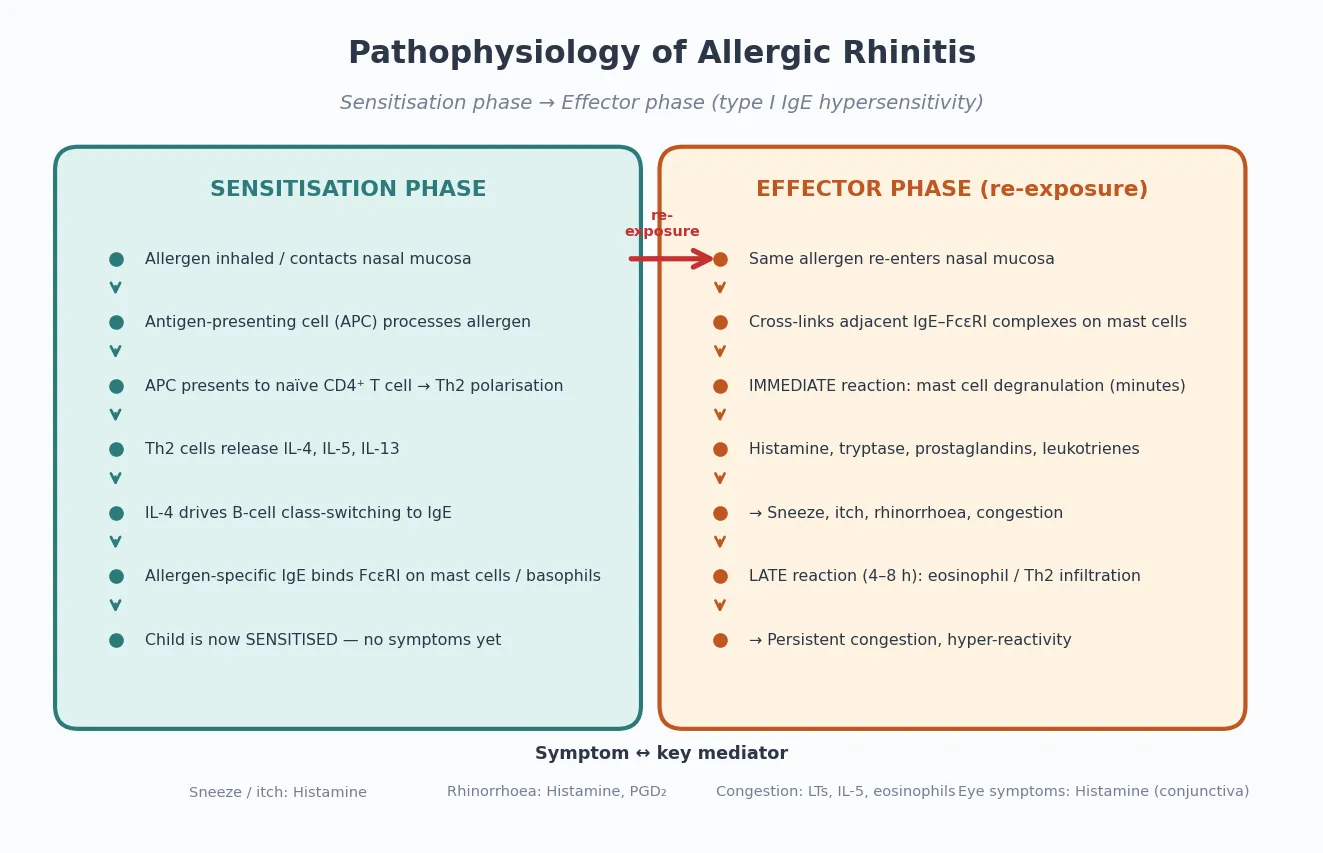
ALLERGIC — the mediators that matter
Classification
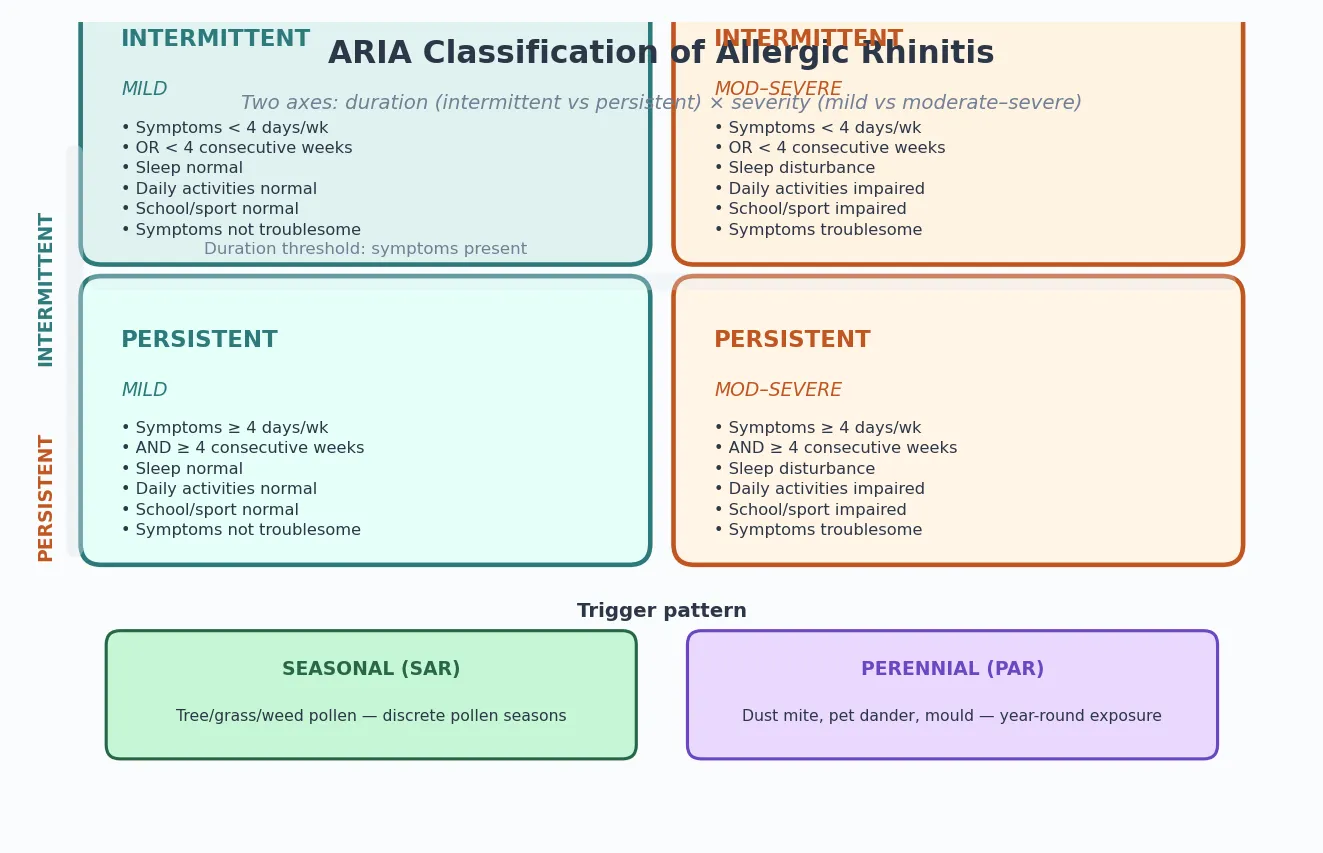
The universally taught classification is the ARIA framework, which grades allergic rhinitis along two axes: duration and severity. By duration, symptoms are intermittent if they occur on fewer than four days per week or for fewer than four consecutive weeks, and persistent if they meet both thresholds. By severity, symptoms are mild when they do not disturb sleep, daily activities, school or sport and are not troublesome, and moderate-to-severe when any of these domains is impaired. [1]
The second useful axis is the trigger pattern. Seasonal allergic rhinitis is driven by pollen — tree pollen in early spring, grass pollen in late spring and early summer, and weed pollen in late summer and autumn — producing discrete symptomatic windows. Perennial allergic rhinitis is driven by year-round indoor allergens such as house-dust mite, animal dander, cockroach and mould, producing continuous or fluctuating symptoms without a clear seasonal pattern. [3]
Episodic allergic rhinitis, a third subtype, describes symptoms triggered by exposure that is not normally encountered in the environment, such as a child who sneezes only when visiting a grandparent with a cat. The distinction matters because seasonal disease suits pre-emptive antihistamine or intranasal corticosteroid courses timed before the pollen season, while perennial disease demands year-round controller therapy and aggressive allergen-avoidance measures. [14]
Clinical Presentation
The hallmark is the nasal symptom quartet of paroxysmal sneezing, anterior watery rhinorrhoea, nasal itch and congestion, often accompanied by itchy, watery, red eyes in allergic rhinoconjunctivitis. Symptoms are reproducible on allergen exposure, bilateral, and classically spare the systemic features of fever and malaise that point toward infection. [3]
On examination, the classic signs are the allergic salute and transverse nasal crease, pale violaceous nasal turbinates (contrasting with the erythematous turbinates of viral infection), clear nasal discharge, and infraorbital venous congestion producing the "allergic shiner" and Dennie-Morgan lines (extra folds below the lower eyelids). A child with chronic disease may also show mouth breathing, a high-arched palate and the "adenoid face" of long-standing nasal obstruction. [3]
School and quality-of-life impact is substantial and often under-recognised. Children with allergic rhinitis have impaired sleep from nocturnal congestion, daytime somnolence, reduced attention and lower school performance, and they participate less in sport and social activity during symptomatic periods. Quantifying this impact with a validated paediatric quality-of-life instrument is part of a thorough assessment. [14]
Differential Diagnosis
The first task is to separate allergic from infectious rhinitis. Viral upper-respiratory infections produce acute onset, fever, thicker or mucopurulent discharge, and resolution within seven to ten days, whereas allergic rhinitis is afebrile, produces clear rhinorrhoea, and persists or recurs with exposure. A course lasting beyond ten days without improvement should raise the question of bacterial rhinosinusitis rather than allergy. [12]
Structural and mechanical causes must also be considered, particularly in a child with unilateral symptoms: a nasal foreign body (classic in toddlers, producing unilateral foul-smelling discharge), a deviated nasal septum, nasal polyps (rare in children and prompting consideration of cystic fibrosis when present), and midline masses such as juvenile nasopharyngeal angiofibroma in adolescent boys. [12]
Drug-induced and vasomotor forms round out the differential: rhinitis medicamentosa from overuse of topical decongestants, gustatory rhinitis triggered by spicy foods, and cold-air-induced or vasomotor rhinitis triggered by temperature change. Primary ciliary dyskinesia and immunodeficiency enter the differential when rhinitis is complicated by chronic or recurrent sino-pulmonary infection. [14]
Clinical & Bedside Assessment
Assessment begins with a focused history that establishes the symptom pattern, triggers, seasonality, and impact on sleep, school and quality of life, together with a personal and family atopic history (eczema, asthma, food allergy). The timing of symptoms relative to specific exposures — worse in spring, worse in the bedroom, worse after contact with animals — frequently identifies the culprit allergen before any testing. [3]
Examination of the nose uses anterior rhinoscopy or, where available, nasendoscopy, looking at the colour and texture of the inferior turbinates, the character of any discharge, and the presence of polyps or a deviated septum. The examination extends to the eyes (conjunctival injection, Dennie-Morgan lines), the oropharynx (cobblestoning from post-nasal drip), the ears (a retracted tympanic membrane or effusion suggesting Eustachian-tube dysfunction) and the chest (wheeze confirming coexisting asthma). [12]
A peak nasal inspiratory flow measurement and a validated symptom or quality-of-life score (such as the paediatric Rhinoconjunctivitis Quality of Life Questionnaire) provide objective tracking of severity and response to treatment over time, anchoring the stepwise escalation of therapy. [14]
Investigations
The diagnosis of allergic rhinitis is primarily clinical, and testing confirms sensitisation rather than disease. Skin-prick testing is the first-line investigation because it is inexpensive, rapid, and demonstrates the presence of allergen-specific IgE bound to mast cells in the skin through a wheal-and-flare reaction read at 15 to 20 minutes. A wheal at least 3 mm larger than the negative control indicates sensitisation, and the panel is selected to match the child's likely exposures — house-dust mite, pollens relevant to the region, cat and dog dander, moulds and cockroach. [12]
Serum-specific IgE testing is the alternative when skin-prick testing is contraindicated — severe dermatographism or eczema, ongoing antihistamine use that cannot be withheld, or a history of anaphylaxis to a skin-prick allergen — and component-resolved diagnosis can distinguish true sensitisation from cross-reactivity in selected cases. A normal total IgE does not exclude allergic rhinitis, and total IgE alone is not a diagnostic test. [14]
Nasal smear for eosinophils, nasal peak flow and rhinomanometry are rarely needed in routine practice. Imaging is reserved for suspected structural disease, chronic rhinosinusitis or complications: a plain sinus radiograph has limited value, and contrast-enhanced CT or MRI is the modality of choice when a complication such as orbital cellulitis or a nasal mass is suspected. [12]
CONFIRM — when to test
Management — Resuscitation
Allergic rhinitis is rarely a resuscitation problem, but the acute scenario to recognise is severe exacerbation complicated by asthma — a child whose allergic trigger has provoked bronchospasm and respiratory distress. The first priority in that situation is the asthma: supplementary oxygen, inhaled bronchodilator and systemic corticosteroid per the child's asthma action plan, because allergic rhinitis and asthma share a common inflammatory pathway and one can tip the other into crisis. [1]
For isolated severe nasal symptoms — distressing sneezing, obstruction or rhinorrhoea in the clinic — an oral second-generation antihistamine gives rapid relief within one to two hours, and saline nasal irrigation clears mucus and allergen from the nasal cavity while definitive therapy is established. [13]
Acute management never stops at symptom relief: the opportunity is taken to assess the child's asthma control, review inhaler technique and adherence, and arrange a structured follow-up plan, because treating rhinitis improves asthma outcomes and vice versa. [1]
Management — Definitive & Stepwise
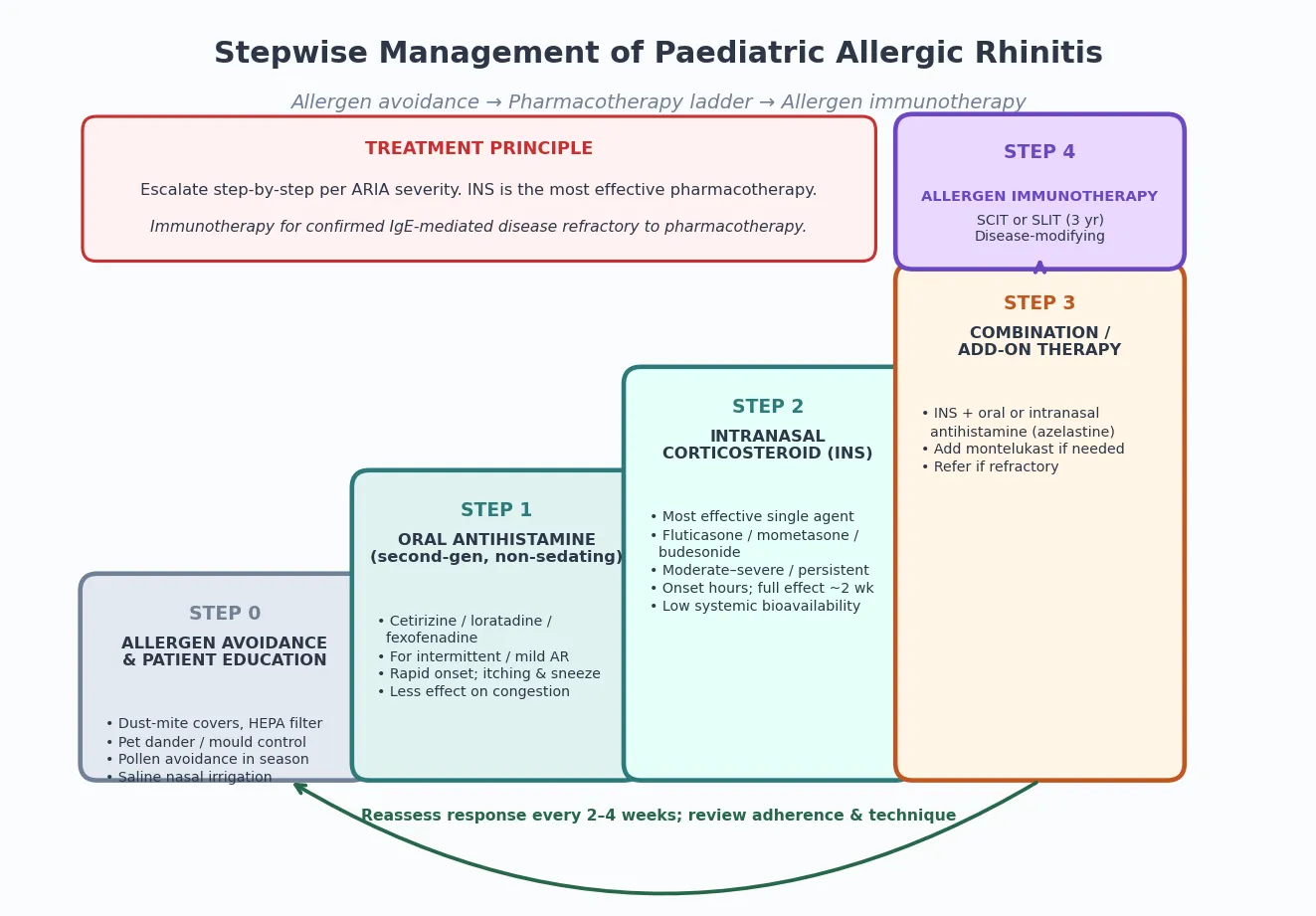
Definitive care follows the ARIA stepwise ladder, beginning with allergen avoidance and patient education and escalating according to symptom severity and control. Allergen-avoidance measures include dust-mite-impermeable mattress and pillow covers, washing bedding in hot water, reducing humidity, removing carpets from the bedroom, HEPA air filtration, and keeping pets out of the child's sleeping area — though the evidence for individual measures is variable, bundled interventions reduce symptom burden in sensitised children. [12]
ARIA stepwise management ladder
Step 0: allergen avoidance and education (dust-mite covers, HEPA, saline irrigation)
Step 1: oral second-generation antihistamine (cetirizine, loratadine, fexofenadine) for mild / intermittent AR
Step 2: intranasal corticosteroid (fluticasone, mometasone, budesonide) for moderate-severe / persistent AR
Step 3: combination — INS + intranasal or oral antihistamine; add montelukast if needed
Step 4: allergen immunotherapy (SCIT or SLIT) for refractory, IgE-confirmed disease
Reassess: every 2-4 weeks; review adherence and spray technique
The pharmacotherapy ladder places a second-generation oral antihistamine at step one for mild or intermittent disease, chosen over first-generation agents because it avoids the sedation, anticholinergic effects and impaired learning associated with chlorphenamine and promethazine. Cetirizine, loratadine, fexofenadine and desloratadine are all effective, with a 2023 evidence-based review confirming their efficacy for itching, sneezing and rhinorrhoea, though they have limited effect on nasal congestion. [7]
Intranasal corticosteroids are the single most effective pharmacotherapy and form step two for moderate-to-severe or persistent disease. A 2024 review of corticosteroid efficacy in children confirms that fluticasone propionate, mometasone furoate, budesonide, triamcinolone and ciclesonide all reduce total nasal symptom scores more effectively than antihistamines, with onset over hours and a full effect after about two weeks of continuous use. [5]
Safety of intranasal corticosteroids is a common parental concern, and the evidence is reassuring: a 2022 safety review confirms minimal systemic bioavailability for mometasone and fluticasone, no clinically meaningful effect on the hypothalamic-pituitary-adrenal axis at recommended paediatric doses, and local side effects limited to mild epistaxis, dryness and irritation. Correct spray technique — directing the nozzle away from the nasal septum — minimises local adverse effects. [6]
A 2025 network meta-analysis of intranasal treatments in preschool- and school-age children ranks intranasal corticosteroids and the combination of intranasal corticosteroid plus intranasal antihistamine (such as azelastine) as the most effective options, supporting combination therapy as step three when monotherapy is inadequate. Leukotriene-receptor antagonists (montelukast) are a useful add-on, particularly in children with coexisting asthma, though behavioural side effects warrant counselling. [4]
Saline nasal irrigation is a valuable adjunct at every step. A 2025 trial in children aged 6 to 12 years demonstrated significant symptom improvement with isotonic saline irrigation as an adjunct to standard pharmacotherapy, and it carries essentially no risk, making it an ideal first-line measure and add-on in young children. [13]
Topical decongestants (oxymetazoline, xylometazoline) have no place in chronic management because of rebound congestion and rhinitis medicamentosa beyond three to five days of use, and first-generation sedating antihistamines impair learning and school performance and should be avoided in children. [12]
Specific Subtypes & Scenarios
Rhinoconjunctivitis, in which ocular symptoms accompany the nasal quartet, is the most common scenario in seasonal disease and often requires topical ocular antihistamine or mast-cell stabiliser (olopatadine, ketotifen) in addition to nasal therapy. Failure to address the ocular component leaves a child who is still symptomatic and functionally impaired despite an adequate nasal regimen. [14]
The atopic-march scenario frames allergic rhinitis as part of a multisystem atopic phenotype that begins with eczema and food allergy in infancy and progresses to rhinitis and asthma. A 2019 review characterises multiple trajectories and pathways, including the "pre-atopic march" driven by early filaggrin-related barrier defects, and confirms that early sensitisation predicts a more severe and persistent allergic trajectory. [10]
Local allergic rhinitis is an under-recognised variant in which the child has a negative skin-prick test and serum IgE but a positive nasal allergen challenge, indicating local IgE production within the nasal mucosa. It explains why some children with a classic allergic phenotype test negative systemically and should be suspected when the clinical picture is convincing but skin-prick testing is unrevealing. [14]
Complications & Pitfalls
The most common complications are the downstream effects of uncontrolled nasal inflammation on the ears, sinuses and lower airway. Eustachian-tube dysfunction produces otitis media with effusion, conductive hearing loss and speech or learning delay; chronic rhinosinusitis develops from persistent mucosal oedema and impaired sinus drainage; and asthma control deteriorates as the shared Th2 inflammation drives bronchial hyper-reactivity. A study of children with otitis media with effusion found a high prevalence of allergic rhinitis, supporting aggressive treatment of the allergic component. [11]
The iatrogenic pitfall is over-reliance on first-generation sedating antihistamines or topical decongestants. Sedating antihistamines impair cognition, reaction time and school performance, and prolonged topical decongestant use produces rebound congestion and rhinitis medicamentosa that is difficult to reverse. Both should be actively deprescribed. [12]
The diagnostic pitfall is anchoring on an allergic label in a child who has a structural, infectious or immunodeficient cause. Unilateral discharge should prompt examination for a foreign body; bilateral nasal polyps in a child should prompt cystic-fibrosis testing; and recurrent sino-pulmonary infection from childhood should prompt consideration of primary ciliary dyskinesia, humoral immunodeficiency or HIV. [14]
Prognosis & Disposition
Allergic rhinitis is a chronic condition with a variable long-term course: many children improve or remit in adulthood, while a substantial proportion progress to asthma or persistent multi-allergen disease. The prognosis is best in children whose sensitisation is limited and whose symptoms are well controlled with a simple regimen, and worst in those with early multi-allergen sensitisation, a strong family history and coexisting asthma. [10]
Disposition is outpatient in virtually all cases, with follow-up every two to four weeks when escalating therapy and then every six to twelve months for stable disease. Referral to a paediatric allergist is appropriate for severe or refractory disease, when allergen immunotherapy is being considered, when the diagnosis is uncertain, or when there is coexisting asthma, food allergy or anaphylaxis that complicates management. [12]
Disease-modifying therapy is the long-term promise of allergen immunotherapy. A 2023 comparison of sublingual versus subcutaneous immunotherapy in children confirmed that both routes reduce symptom scores and medication use, with sublingual therapy offering a better safety profile and convenience for children, and a three-to-five-year course producing sustained remission in a proportion of treated children. [9]
Special Populations
Children with neurodevelopmental disability or autism may be unable to articulate nasal symptoms, presenting instead with behavioural change, sleep disturbance, mouth breathing or self-injury; a high index of suspicion and a structured examination are needed to detect treatable rhinitis in this group. Adherence to intranasal therapy is often challenging and benefits from a simplified regimen and caregiver training. [14]
Refugee, migrant and asylum-seeking children may have had limited prior access to allergy care and may present with advanced, untreated disease complicated by chronic complications such as otitis media with effusion and speech delay. The allergen panel must be matched to the child's country of origin and current environment, because sensitisation patterns differ geographically — a child sensitised to subtropical grasses in their country of origin may not be captured by a temperate-climate panel. [2]
In children with coexisting asthma, allergic rhinitis is not a bystander but an active contributor to asthma morbidity, and the two conditions are managed together under the United Airway Disease model. Aggressive rhinitis control is part of asthma step-up, and poor asthma control in a child with rhinitis should prompt a review of nasal therapy before escalating asthma medication. [1]
Evidence, Guidelines & Regional Differences
The 2024–2025 ARIA-EAACI guideline is the current international standard, integrating evidence on diagnosis, the stepwise pharmacotherapy ladder and the role of allergen immunotherapy, and placing strong emphasis on the united-airway concept and on digital, patient-centred care pathways. It reaffirms intranasal corticosteroids as the most effective pharmacotherapy and allergen immunotherapy as the only disease-modifying intervention. [1]
The EAACI 2018 guideline on allergen immunotherapy for allergic rhinoconjunctivitis sets the indications, contraindications and safety framework for both subcutaneous (SCIT) and sublingual (SLIT) routes, and remains the reference standard for immunotherapy practice, with sublingual therapy increasingly preferred in children because of its superior safety profile and home-based convenience. [8]
The American Academy of Otolaryngology clinical practice guideline focuses on the otolaryngological dimension, offering criteria for referral, imaging and surgical consideration, and is the key reference when the question turns to structural disease, chronic rhinosinusitis or surgical intervention. [12]
Regional differences centre on the dominant aeroallergens and the intensity of pollen seasons: temperate regions contend with tree, grass and weed pollens in discrete seasons, while tropical and subtropical regions contend with year-round dust-mite exposure and subtropical grass pollens. The Melbourne 2016 thunderstorm asthma event demonstrated how a high grass-pollen load combined with a thunderstorm can trigger fatal asthma epidemics in sensitised populations, a phenomenon now part of public-health warning systems. [1]
Exam Pearls
For written and viva exams, allergic rhinitis is a high-yield topic because it is common, has a clean IgE mechanism, and tests whether you can apply the ARIA classification, justify a stepwise pharmacotherapy ladder, and articulate the link to asthma. Be ready to draw the two-phase mechanism: sensitisation through Th2-driven IgE class-switching, and effector mast-cell degranulation producing immediate and late-phase symptoms. [3]
Examiners love the pharmacotherapy ladder and the safety of intranasal corticosteroids. State that intranasal corticosteroids are the most effective single therapy with minimal systemic bioavailability at paediatric doses, that second-generation oral antihistamines replace sedating first-generation agents, and that allergen immunotherapy is the only disease-modifying option, reserved for refractory IgE-confirmed disease. [5]
The red flags and differentials are equally high-yield: unilateral discharge means foreign body, bilateral polyps in a child mean cystic fibrosis, purulent discharge means infection rather than allergy, and coexisting asthma means the two conditions must be managed together under the United Airway Disease model. Name the atopic march and explain how treating rhinitis improves asthma outcomes. [12]
References
- [1]Sousa-Pinto B, Bousquet J, Vieira RJ Allergic Rhinitis and Its Impact on Asthma (ARIA)-EAACI Guidelines-2024-2025 Revision: Part I-Guidelines. Allergy, 2026.PMID 41324154
- [2]Licari A, Magri P, De Silvestri A Epidemiology of Allergic Rhinitis in Children: A Systematic Review and Meta-Analysis. J Allergy Clin Immunol Pract, 2023.PMID 37236349
- [3]Skoner DP Allergic rhinitis: definition, epidemiology, pathophysiology, detection, and diagnosis. J Allergy Clin Immunol, 2001.PMID 11449200
- [4]Gil-Mata S, Vieira RJ, Borowiack E Intranasal Treatments for Allergic Rhinitis in Preschool- and School-Age Children: Network Meta-Analysis. J Allergy Clin Immunol Pract, 2025.PMID 40675325
- [5]Li Y, Xiong J, Zhang Z Efficacy and safety of various corticosteroids in the treatment of children with allergic rhinitis. J Evid Based Med, 2024.PMID 39313999
- [6]Zhang M, Ni JZ, Cheng L Safety of intranasal corticosteroids for allergic rhinitis in children. Expert Opin Drug Saf, 2022.PMID 35199623
- [7]Linton S, Hossenbaccus L, Ellis AK Evidence-based use of antihistamines for treatment of allergic conditions. Ann Allergy Asthma Immunol, 2023.PMID 37517656
- [8]Roberts G, Pfaar O, Akdis CA EAACI Guidelines on Allergen Immunotherapy: Allergic rhinoconjunctivitis. Allergy, 2018.PMID 28940458
- [9]Yang J, Lei S Efficacy and safety of sublingual versus subcutaneous immunotherapy in children with allergic rhinitis. Front Immunol, 2023.PMID 38162647
- [10]Paller AS, Spergel JM, Mina-Osario P The atopic march and atopic multimorbidity: Many trajectories, many pathways. J Allergy Clin Immunol, 2019.PMID 30458183
- [11]Norhafizah S, Salina H, Goh BS Prevalence of allergic rhinitis in children with otitis media with effusion. Eur Ann Allergy Clin Immunol, 2020.PMID 31668057
- [12]Seidman MD, Gurgel RK, Lin SY Clinical practice guideline: Allergic rhinitis. Otolaryngol Head Neck Surg, 2015.PMID 25644617
- [13]Yadegari B, Houshmand H, Ghaemi MR Effectiveness of the Nasal Irrigation in Treating Allergic Rhinitis in Children 6 to 12 Years. Iran J Allergy Asthma Immunol, 2025.PMID 40052885
- [14]Schuler CF, Montejo JM Allergic Rhinitis in Children and Adolescents. Immunol Allergy Clin North Am, 2021.PMID 34602232