Paeds · allergy-and-immunology
Anaphylaxis prevention, action plans and autoinjectors
Also known as ASCIA anaphylaxis action plan · Adrenaline autoinjector · EpiPen · Anapen · Anaphylaxis first-aid · School anaphylaxis management · Biphasic anaphylaxis
Fellowship topic on the complete community prevention and first-aid package for a child at risk of anaphylaxis: trigger identification and avoidance, the written personalised ASCIA action plan (green for the mild-to-moderate allergic reaction, red for anaphylaxis), prescribing and teaching the weight-appropriate adrenaline autoinjector (0.15 mg device for 7.5-20 kg, 0.3 mg for 20 kg and over, 0.5 mg for 50 kg and over where available), correct intramuscular technique into the outer mid-thigh, family and school education, the biphasic reaction and the mandatory observation pathway, the fatal-risk triad of adolescence with peanut or tree-nut allergy and uncontrolled asthma, and adolescent transition planning. The page names ASCIA, EAACI, WAO and the US 2020 practice parameter guideline positions and the regional deltas, and defends the adrenaline-first principle.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The numbers that shape the prevention package
Overview & Definition
Imagine a six-year-old with a peanut allergy sitting in a school lunch area. In the next ten minutes one of two things will happen: either nothing, because everyone knew the trigger, carried the plan and the device, and the food was kept away — or a collapse, and in that collapse the difference between life and death is whether a written plan and an adrenaline autoinjector exist on site and whether someone present can use them. This page is about building that package so reliably that the second scenario is survivable. [10]
Anaphylaxis prevention in children is the structured, longitudinal package that converts a potentially fatal allergic emergency into a treatable community event. It rests on five pillars: identification and avoidance of the trigger, a written personalised action plan, a prescribed adrenaline autoinjector, education of the child and every carer, and a medical alert plus a second device. The package is global, but its drugs, weight bands and named documents are regional — in Australia and Aotearoa New Zealand it is delivered through the ASCIA plans and devices, in Europe through the EAACI framework, and in North America through the AAAAI/ACAAI 2020 practice parameter. [5] [4]
In Australasia, the written documents are the ASCIA Action Plan for Anaphylaxis (red) and the ASCIA Action Plan for Allergic Reactions (green). Adrenaline autoinjector devices available include EpiPen and Anapen. The weight bands are 7.5 to 20 kg for the 0.15 mg device and 20 kg and over for the 0.3 mg device, with a 0.5 mg Anapen available for 50 kg and over.
The concept to hold is that prevention here is layered. Primary prevention is stopping food allergy from developing in the first place — the LEAP trial proved that early rather than delayed peanut introduction in high-risk infants cuts peanut allergy, and that upstream work reduces the downstream population this page's package exists to protect. [14] Secondary prevention is what happens after the diagnosis: avoidance, preparedness, the plan and the device. Tertiary prevention is preventing the next reaction from killing once anaphylaxis has already occurred — adrenaline without delay, the second dose, the ambulance, the observation. Every paragraph below sits inside one of these three layers. [9]
Classification
The package classifies along two axes that the examiner tests directly. The first is the written document, and there are two of them, distinguished by colour and by whether they trigger adrenaline. The second is the autoinjector device, distinguished by dose and by the child's weight. [10]
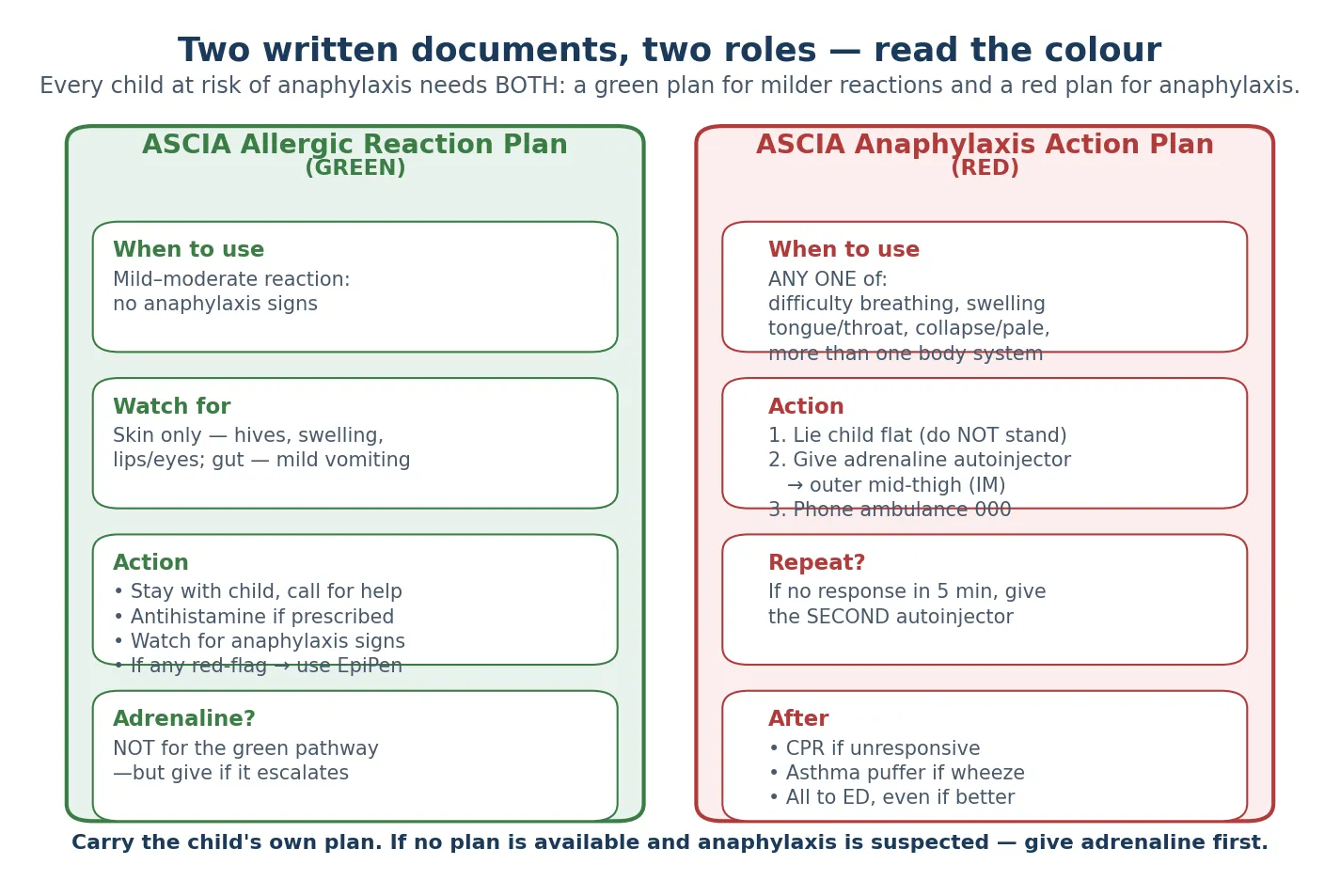
The green plan (Allergic Reaction Plan) covers mild to moderate reactions: skin symptoms such as hives, localised swelling of the lips or eyes, and mild gut symptoms such as a single vomit. The plan says stay with the child, give an antihistamine if prescribed, and watch closely for any sign that the reaction is escalating into anaphylaxis. Adrenaline is not given on the green pathway — but the moment any red-flag feature appears, the carer crosses immediately to the red plan. [10]
The red plan (Anaphylaxis Action Plan) triggers adrenaline the moment anaphylaxis is recognised — any one of difficulty breathing, swelling of the tongue or throat, collapse or pallor, or a rapid reaction involving skin plus any other body system. The plan is explicit and rehearsed: lie the child flat, give the adrenaline autoinjector into the outer mid-thigh, call the ambulance, and repeat the dose after five minutes if there is no response. The genius of the colour-coded plan is that it removes deliberation at the moment of crisis; the carer does not diagnose, they read the colour. [10]
[10]Epidemiology & Risk Factors
Paediatric anaphylaxis and the dispensing of adrenaline autoinjectors have risen sharply across Australia, the United Kingdom and North America over the past two decades. Food is the dominant trigger in children — peanut, tree nuts, egg, cow's milk, sesame and seafood — with insect venom and medication (antibiotics and non-steroidal anti-inflammatory drugs) rising as children move into adolescence. Liew and colleagues documented the rising trend of anaphylaxis admissions and fatalities in Australia, and Mullins and colleagues showed that anaphylaxis fatalities in Australia continued to increase through 2013, particularly in the food-allergic, adolescent age band. [7] [8]
Fatal anaphylaxis in children is rare in absolute terms, but the case-fatality of a recurrent reaction in a high-risk child is preventable and is driven overwhelmingly by delayed or absent adrenaline. Turner and colleagues synthesised the fatal-anaphylaxis literature and identified the recurring risk factors: adolescence and young adulthood, peanut or tree-nut allergy, co-existing asthma — especially uncontrolled asthma — a prior severe reaction, and the absence of an in-date or available autoinjector at the moment of need. [11]
The undertreatment problem is the dominant public-health issue. Many children with a clear anaphylaxis history are never prescribed an autoinjector, or never carry it, or carry a device that is expired, and the family and school often cannot demonstrate correct technique when tested. Simons documented this gap in first-aid treatment of food anaphylaxis, and the AAP clinical report reinforced that prescribing a device without teaching and rehearsing technique is incomplete prevention. [9] [10]
Pathophysiology
Anaphylaxis is an acute IgE-mediated mast-cell and basophil degranulation. The trigger cross-links allergen-specific IgE on the surface of mast cells and basophils, releasing a torrent of preformed and newly synthesised mediators — histamine, tryptase, leukotrienes, prostaglandins and platelet-activating factor. These mediators act in synergy to produce the cardiovascular collapse (vasodilation, increased capillary permeability, third-spacing, hypotension) and the respiratory compromise (bronchospasm, upper-airway mucosal oedema) that together characterise the syndrome. [1] [2]
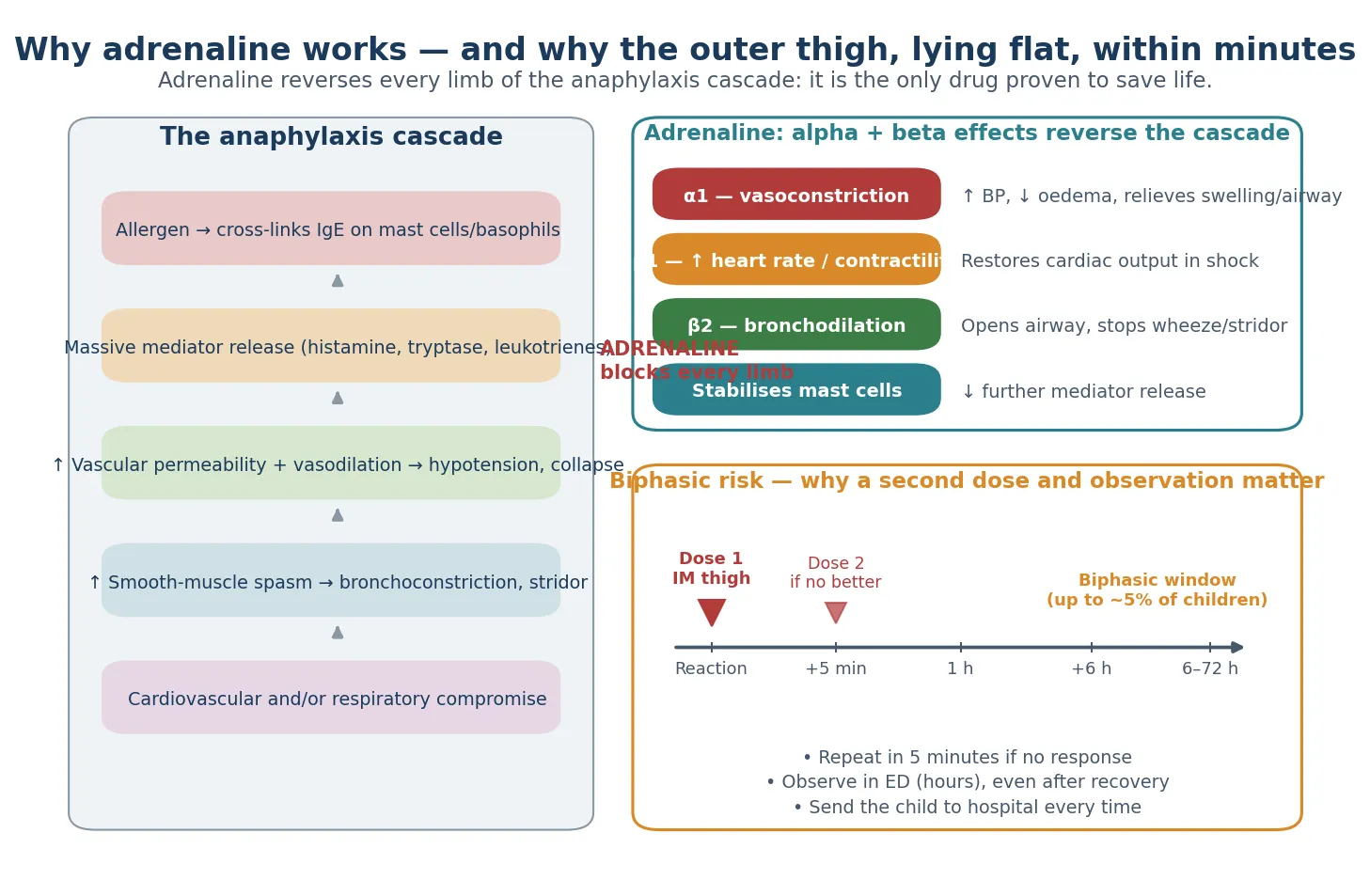
Adrenaline is the single drug that reverses every limb of that cascade, which is why no other drug substitutes for it. Its alpha-1 agonism vasoconstricts, restoring blood pressure and shrinking the mucosal oedema that threatens the airway; its beta-1 agonism increases heart rate and contractility to restore cardiac output in shock; its beta-2 agonism bronchodilates to relieve the wheeze and stridor; and it stabilises the mast cell to slow further mediator release. Antihistamines, steroids and bronchodilators are adjuncts only — none reverses the haemodynamic collapse, and none saves a life in the first minutes. [9] [4]
The route and the site matter and are heavily tested. Intramuscular adrenaline into the vastus lateralis — the outer middle third of the thigh — produces the fastest and most reliable peak concentration, far faster and more predictable than subcutaneous injection, because absorption from subcutaneous tissue in a shock state is erratic and slow. The deltoid and the buttock are inferior sites for first-aid adrenaline. The autoinjector is engineered around this pharmacology: a fixed-dose, spring-loaded, pre-filled device that deposits adrenaline intramuscularly at the right depth when pressed against the outer thigh. [9] [3]
The biphasic reaction is the late recurrence of symptoms hours after the initial reaction has settled, driven by persistent mediator release and the long tissue half-life of leukotrienes. Lee and colleagues' systematic review and meta-analysis found that biphasic reactions occur in a small but real fraction of anaphylaxis presentations, typically within the first hours, and Mehr and colleagues identified the paediatric predictors — a severe initial reaction, the need for more than one dose of adrenaline, and a wide initial pulse pressure. The biphasic risk is the reason a second autoinjector is prescribed and why hospital observation is mandatory after every community device use. [12] [13]
Clinical Presentation
The child who needs the plan may present across any combination of body systems. The skin features — urticaria, angioedema, flushing, itch — are the most visible but are the least dangerous. The dangerous features are airway (a sense of throat closing, hoarseness, drooling, stridor), breathing (wheeze, cough, respiratory distress, hypoxia), circulation (pallor, floppiness, hypotension, collapse) and gut (vomiting, abdominal pain, diarrhoea), often with a neurological sense of impending doom or dizziness. [1]
For the community plan, anaphylaxis is defined operationally as any acute reaction with airway or breathing compromise, or collapse and pallor, or a rapid progressive reaction involving skin plus another body system. This operational definition is the one the carer uses — and the plan is explicit that the correct response to it is to treat, not to deliberate. The hardest teaching point is that a child with a known food allergy who develops acute wheeze after an allergen has anaphylaxis until proven otherwise, and adrenaline treats both the anaphylaxis and the wheeze. [4]
Atypical presentations are the ones that catch families and clinicians out. A child may simply become pale and quiet without any rash; an infant may present with floppiness and lethargy; a teenager may collapse at a party after alcohol without offering a clear history. Any of these in a child with a known allergy, or after a plausible allergen exposure, is anaphylaxis until proven otherwise, and the adrenaline-first principle applies. [11]
Differential Diagnosis
The single differential the plan hinges on is whether the reaction is a mild allergic reaction (green plan, no adrenaline) or anaphylaxis (red plan, adrenaline now). The discriminating features are airway or breathing compromise, cardiovascular compromise, or rapid multi-system involvement. A reaction that involves only the skin stays on the green plan; the moment any other system is involved, or the airway or circulation is threatened, the carer crosses to the red plan. [10]
Acute asthma is the most dangerous mimic because it is also a genuine alternative treatment target. The asthmatic with known food allergy who becomes acutely wheezy after an allergen has anaphylaxis until proven otherwise; adrenaline treats both, and the cost of giving adrenaline to a child who "only" has asthma is small and reversible, while the cost of withholding it in anaphylaxis is death. [4] [11]
REASONS
Vasovagal syncope separates itself by pallor and collapse without urticaria, airway or gut features, and by rapid full recovery on lying flat — the opposite tempo of anaphylaxis. Panic attacks present with breathlessness and tingling but no urticaria, no hypotension, and normal oxygenation. Breath-holding and choking events are brief and self-limiting. The teaching point is unchanged: when anaphylaxis is genuinely possible, adrenaline is safer than withholding it, so the cost of a diagnostic error in the safe direction is small. [4]
Clinical & Bedside Assessment
The structured allergy history at the prevention visit establishes the foundation for the whole package. Establish the confirmed trigger or triggers from the reaction history and testing; the most severe past reaction and how it was managed; the interval since the last reaction; the child's asthma status and how well it is controlled; comorbidities; and every setting the child spends time in — home, school, childcare, the other parent's house, grandparents, sport, holiday care. Each of these settings is a place the device and the plan must reach. [10]
The device check is a bedside manoeuvre the candidate must perform and teach. Confirm the device is in date (check both the printed expiry and the viewing window), that it is the correct dose for the child's current weight, that the family can demonstrate the technique on a trainer device (correct site on the outer mid-thigh, cap off, three-second hold, and that it can be given through clothing), and that they know the five-minute repeat rule. The child's weight against the device dose band is checked at every visit — a child who has grown past 20 kg needs the 0.3 mg device, and the prescribing doctor must drive that check, because families rarely raise it themselves. [10]
The risk synthesis is where fellowship reasoning shows. The teenager who does not carry the device, the child with uncontrolled asthma and peanut allergy, the family with limited health literacy or a language barrier, the school without a trained staff member, and the rural child with long ambulance times each need a different, escalated plan. The plan is not "here is a prescription"; it is "here is how this specific child stays alive in this specific context". [11]
Investigations
The diagnosis of anaphylaxis is clinical, and no test is needed to treat. Adrenaline must not be delayed for tryptase or any investigation in the community or the emergency setting. The 2006 international definition (Sampson and the NIAID/FAAN symposium) codified anaphylaxis as a clinical diagnosis, and every subsequent guideline has held that line — the plan triggers on bedside recognition, not on a laboratory value. [1]
Serum tryptase has a confirmatory role when drawn within the first one to two hours of a reaction: a level rising from the individual's baseline supports mast-cell activation and helps with retrospective confirmation, especially when the diagnosis is uncertain. A baseline tryptase is taken at follow-up, both to interpret the acute level and to screen (rarely, in children) for underlying systemic mastocytosis, which is associated with more severe recurrent anaphylaxis. [5]
The allergen workup that follows a confirmed reaction is what closes the prevention loop. Skin-prick testing and specific serum IgE to the suspected trigger confirm sensitisation; a supervised oral food challenge is the gold standard where the trigger is uncertain or tolerance is being reassessed; and component-resolved diagnostics (for example Ara h 2 for peanut) refine the risk of a true systemic reaction versus cross-reactivity. The written action plan and the autoinjector are prescribed at this clinical review — the "investigation" of community readiness is whether the device is present, in date, and the plan is distributed to every carer. [4]
Management — Resuscitation
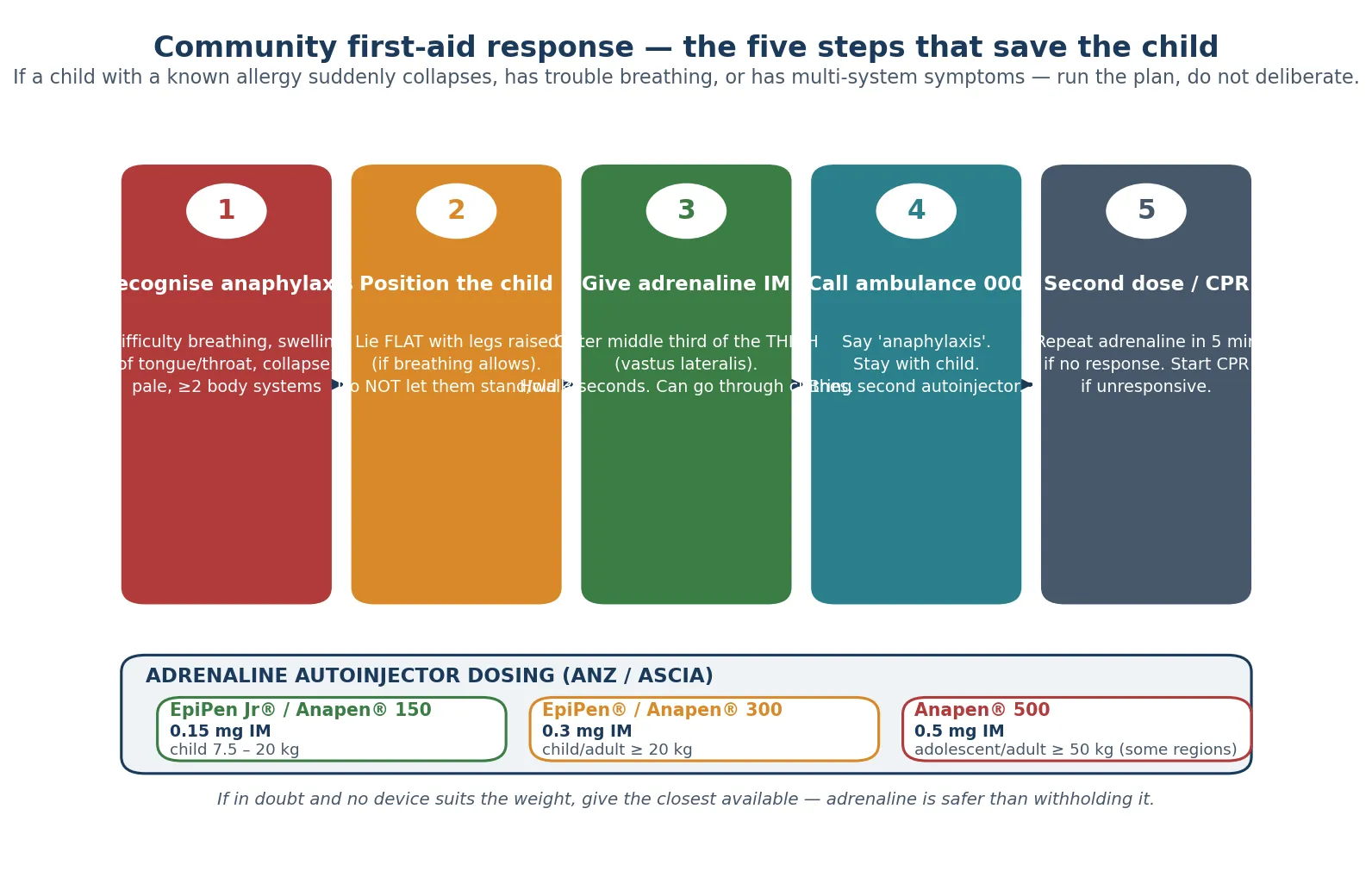
The immediate community first-aid bundle is fixed and rehearsed. The moment anaphylaxis is recognised: position the child flat with legs raised (do not let them stand or walk — sudden standing provokes fatal empty-vena-cava collapse); give the adrenaline autoinjector into the outer middle third of the thigh; and call the ambulance, stating "anaphylaxis". These three actions are the resuscitation, and the order matters. [10]
The exact autoinjector technique is heavily examined and frequently done wrong under stress. Remove the safety cap. Place the orange end — the needle end — against the outer middle third of the thigh (the vastus lateralis). Push firmly until it clicks, and hold for three seconds. Remove and massage the site for ten seconds. The device can be given through clothing, which removes a reason for delay. The "blue to the sky, orange to the thigh" mnemonic (EpiPen) and "fist around the device, red end down" (Anapen) encode the orientation so the needle enters the child, not the thumb. [10]
Adrenaline (epinephrine) autoinjector, intramuscular, outer mid-thigh
The repeat-dose rule is the safety net. A second dose is given after five minutes if there is no response, or if symptoms recur after an initial response — which is why a second device and the ambulance are essential. The child is sent to hospital by ambulance every time, even after apparent full recovery, because of the biphasic window. If the child becomes unresponsive at any point, cardiopulmonary resuscitation is started. [12]
Management — Definitive & Stepwise
The definitive prevention prescription is what the general paediatrician writes at the review after a reaction or on first diagnosis. It has six components: confirmed trigger avoidance with label-reading and cross-contamination advice; the green and red ASCIA plans; the weight-appropriate adrenaline autoinjector; two devices (one for home and one for school or childcare); a planned review date; and explicit, rehearsed education. Each component is testable, and each is incomplete without the others. [10]
The prevention prescription — what to write at the review
Confirm the trigger(s) from history and testing; give avoidance and label-reading advice for the specific allergen
Issue the green ASCIA Allergic Reaction Plan AND the red ASCIA Anaphylaxis Action Plan, dated, with a photo
Prescribe the weight-appropriate adrenaline autoinjector — 0.15 mg for 7.5-20 kg, 0.3 mg for 20 kg and over, 0.5 mg for 50 kg and over where available
Prescribe TWO devices — one for home, one for school/childcare — and a trainer device
Teach and rehearse technique with the parents, the child (age-appropriate) and a named school staff member
Optimise asthma control; set a review date — at least annually, at every reaction, and at every weight-band transition
The education ladder is where prevention lives or dies. Teach the child and every carer — parents, grandparents, school, childcare, sport, close friends — the recognition cues and the device technique using a trainer device, and re-teach at every visit. Technique decays: a family shown the device once at diagnosis will not reliably reproduce it a year later, and the school staff member trained in term one may have moved on by term three. The school-readiness package provides the school with the action plan and device, confirms a trained staff member, agrees on storage that is accessible rather than locked away, and rehearses the response. In Australia the ASCIA school training program underpins this and is the backbone of community paediatric anaphylaxis prevention. [10]
Asthma control is a non-negotiable part of the anaphylaxis prevention plan, because uncontrolled asthma multiplies anaphylaxis fatality risk and because beta-agonist-only management of an allergic wheeze delays adrenaline. Optimise preventer therapy, confirm the child has and uses an asthma action plan, and rehearse the crossover scenario: the child who is wheezy after an allergen gets adrenaline first, salbutamol as adjunct. [11]
The transition pathway for adolescents is built around behaviour, not just biology. An explicit device-carrying plan, autonomy over the action plan, mental-health-aware counselling that addresses risk-taking and eating out without stigma, alcohol advice (alcohol impairs recognition and judgement of a reaction), and a named adult physician handover before independent living are the elements that distinguish the adolescent plan from the child plan. The adolescent years are when fatal anaphylaxis clusters, and the prevention package must be rebuilt for that reality. [11] [4]
Specific Subtypes & Scenarios
The school-age child newly diagnosed with peanut anaphylaxis is the flagship scenario. The full prevention package is deployed — the two plans, the 0.15 mg or 0.3 mg device by weight, two devices, school liaison, and an early connection with an allergy service for component testing (Ara h 2) to refine whether the reactivity reflects a true systemic peanut allergy. The family is taught to read labels and to manage the everyday risk of shared tables, birthday parties and travel. [4]
The insect-venom-allergic child is the one subtype with a disease-modifying option. Venom immunotherapy is highly effective for bee and wasp venom allergy and is offered to children with a systemic reaction confirmed on testing; until immunotherapy has taken hold, the child carries an adrenaline autoinjector for an untreated sting, and summer-lifestyle advice — shoes outside, avoidance of soft drinks and picnics where wasps gather — is part of the plan. [5]
The child with multiple food allergies in a complex social setting — out-of-home care, shared households, travel — needs a prioritised avoidance plan that identifies the highest-risk allergens, a single master action plan rather than competing documents, and additional devices for each setting so the device is never the missing element. These families benefit from a dietitian and from explicit, rehearsed plans for travel, including carrying devices and a translated plan. [4]
The adolescent transitioning to independence is addressed in the management section and is the highest-risk subtype. The package is rebuilt around device-carrying behaviour, alcohol and eating out, the move from parent-managed to self-managed care, and a structured handover to adult allergy services before the young person leaves paediatric care. [11]
Complications & Pitfalls
The fatal pitfall is delayed adrenaline. Attributing airway compromise to asthma, a skin-only reaction, anxiety, or a gastrointestinal upset, and treating with antihistamine, bronchodilator or observation instead of adrenaline, is the single recurring error in fatal paediatric anaphylaxis. The prevention plan exists to remove that deliberation: the red plan triggers adrenaline without a diagnostic step. [11] [9]
The device errors are the next tier. Injecting into the thumb rather than the thigh (digit injection from holding the wrong end), injecting into the subcutaneous buttock, not holding for the full three seconds so the dose is not fully delivered, and using an expired or never-replaced device are all documented. Each is preventable by rehearsal with a trainer device and by orientation training at every visit. [10]
The planning errors are the system failures that kill. No second device at school, the device left at home by the adolescent, the plan never given to the school, and the dose not up-titrated as the child grows past 20 kg are all documented contributors to fatal outcomes. The follow-up errors compound them: no allergy review after the first reaction, no adrenaline prescription despite a clear history, and no biphasic-risk observation after a community device use. [8] [11]
Prognosis & Disposition
With an in-date device, a distributed plan and trained carers, the child at risk of anaphylaxis has an excellent prognosis — the preventable cause of death is system failure, not biology. The package works because it is engineered around human factors: the colour-coded plan removes diagnostic deliberation, the fixed-dose device removes calculation, the rehearsed technique removes performance failure, and the second device plus ambulance removes the consequence of a biphasic reaction. [10]
Every community autoinjector use mandates ambulance transfer to hospital for observation because of the biphasic window, which extends over the hours after the initial reaction. The child who looks fully recovered in the kitchen may relapse in the emergency department, and the observation period is the safety net that catches that relapse. [12] [13]
The review cycle is the longitudinal backbone. Annual review at minimum, review at every reaction, and review at every weight-band transition are the three scheduled touchpoints. The device expires (typically twelve to eighteen months) and must be replaced before the expiry date; an expired device may be used only if no other device is available and adrenaline is genuinely needed, and the family should be told to replace it before that situation arises. [10]
The long-term outlook for food allergy itself is variable. Cow's milk and egg allergy frequently resolve through childhood; peanut and tree-nut allergy more often persist. The allergy review reassesses tolerance over time and answers the question of whether the autoinjector is still required, which is part of preventing both undertreatment and unnecessary lifelong device carriage. [5]
Special Populations
The infant and small child under 7.5 kg is the group where device choice is hardest and the evidence thinnest. Anaphylaxis in this age group is recognised on collapse, pallor and floppiness as much as on airway signs; the 0.15 mg device is the smallest available, and specialist advice is essential to weigh the very small infant against the device. The teaching point is unchanged: adrenaline must not be withheld because the infant is small. [4]
The adolescent is the highest-risk group for fatal anaphylaxis. Non-carrying of the device, risk-taking, alcohol, uncontrolled asthma and unstructured eating cluster in this group. The prevention plan must be rebuilt around adolescent behaviour — explicit device-carrying plans, autonomy, mental-health-aware counselling, and a structured transition to adult services. [11]
The child with developmental disability or neurodiversity, and the child in out-of-home care, needs simplified plans, multiple trained carers, robust school liaison, and device distribution that does not depend on a single adult. These children are at higher risk of both reaction and undertreatment because of the complexity of their care environments. [4]
The rural and remote child faces longer ambulance times and fewer trained bystanders. Additional devices, explicit ambulance-triage language ("anaphylaxis" brings the right response), and local community training are the elements that close the gap. [10]
The child with comorbid asthma is the one whose asthma must be optimised, because asthma multiplies anaphylaxis fatality risk. The child on beta-blockers is rare in paediatrics but important: beta-blocker-related refractory anaphylaxis may need glucagon under specialist guidance, and the prevention plan must flag the interaction. [11]
Evidence, Guidelines & Regional Differences
The ASCIA position in Australia and Aotearoa New Zealand is the regional standard for this page: every child at risk of anaphylaxis has a written ASCIA plan and a prescribed adrenaline autoinjector, with weight bands of 7.5 to 20 kg for the 0.15 mg device and 20 kg and over for the 0.3 mg device. The ASCIA school and childcare training program is the community backbone, and the ASCIA plans are the named documents that travel with the child. [10]
The European position is set by the EAACI anaphylaxis guideline (2021 update, Muraro and colleagues), which endorses written plans, intramuscular adrenaline as first-line treatment, the weight-appropriate device, and structured school and community education. The 2014 EAACI guideline (Muraro and colleagues) established the framework the 2021 update refined. [5] [6]
The World Allergy Organization guidelines (Simons and colleagues, 2012 update) codified adrenaline as first-line, intramuscular, into the thigh, and recommended community availability of adrenaline for those at risk — the global consensus that underpins every regional plan. [3]
[4]The UK position is set by the Resuscitation Council UK emergency treatment of anaphylaxis and by BSACI, with intramuscular adrenaline, the child flat, written plans, and — in some regions — school access to spare unassigned autoinjectors. [5]
The primary-prevention evidence is the LEAP trial (Du Toit and colleagues, 2015), a randomised trial showing that early rather than delayed peanut introduction in high-risk infants markedly reduced peanut allergy at five years. This is the upstream work that reduces the downstream population this page's package exists to protect, and it is the evidence base for early-allergen introduction guidance. [14]
LEAP — Learning Early About Peanut Allergy
PMID 25705822
Randomised, controlled trial in 640 infants at high risk of peanut allergy (severe eczema, egg allergy, or both)
Key finding
Early sustained peanut consumption from 4-11 months reduced peanut allergy at 5 years by about 80% relative to avoidance.
The controversies are real and examined. The weight band at which the child moves from the 0.15 mg to the 0.3 mg device differs slightly between ASCIA (20 kg) and some international labelling; whether schools should hold spare unassigned autoinjectors is debated and varies by jurisdiction; and the optimal route and dose in infants below 7.5 kg has thin evidence. In each case the safe principle holds: when anaphylaxis is possible, give adrenaline rather than withhold it. [4] [11]
Exam Pearls
The single most tested paediatric fact is the 20 kg weight band. Below 20 kg the 0.15 mg device; at 20 kg and over the 0.3 mg device. Check the child's weight at every visit, because the family will not raise it. [10]
The "adrenaline is safer than withholding" principle is the ethical and clinical spine of the whole topic. The harm of an unnecessary dose — transient tachycardia, pallor, anxiety — is small, recognised and reversible. The harm of a missed dose in genuine anaphylaxis is death. When in doubt, the safe direction is to give. [9]
Two documents, two colours, two devices, two carers trained, two settings covered — the "two" of the package is a memory hook that ensures redundancy at every failure point. The candidate who can reproduce the prevention prescription and defend the adrenaline-first principle has the topic. [10]
References
- [1]Sampson HA; Muñoz-Furlong A; Campbell RL; Adkinson NF Jr; Bock SA; Branum A; Brown SG; Camargo CA Jr; Cydulka R; Galli SJ; Gidudu J; Gruchalla RS; Harlor AD Jr; Jopner DL; Kaplan AP; Levy JH; Lisenby WF; Méndez-Inocencio J; Nowak-Węgrzyn A; Oppenheimer JJ; Sclar DA; Sheffer AL; Sferdeen L; Yocum MW Second symposium on the definition and management of anaphylaxis: summary report--Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol, 2006.PMID 16461139
- [2]Brown SG Clinical features and severity grading of anaphylaxis. J Allergy Clin Immunol, 2004.PMID 15316518
- [3]Simons FE; Ardusso LR; Bilò MB; El-Gamal YM; Ledford DK; Ring J; Sanchez-Borges M; Senna GE; Sheikh A; Thong BY; Worm M; World Allergy Organization 2012 Update: World Allergy Organization Guidelines for the assessment and management of anaphylaxis. Curr Opin Allergy Clin Immunol, 2012.PMID 22744267
- [4]Shaker MS; Wallace DV; Golden DBK; Oppenheimer J; Bernstein JA; Campbell RL; Dinakar C; Ellis A; Greenhawt M; Khan DA; Lang DM; Lierl MB; Padial A; Rank MA; Stukus DR; Wang J; Cassidy-Smith M; Cush J; Hershey MS; Hogue SL; Kachru R; Kanaley J; Portnoy JM; Schilling LH; Stahl AL; Tadigotla V; Vargas PA; Wasserman R; Zampelli A Anaphylaxis-a 2020 practice parameter update, systematic review, and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) analysis. J Allergy Clin Immunol, 2020.PMID 32001253
- [5]Muraro A; Worm M; Alviani C; Cardona V; DunnGalvin A; Gowland MH; language review team; Angood E; Arroyave-Sánchez L M; Beck S; Belohlávek J; Bindslev-Jensen C; Bøgh KL; Brockow K; Fernández-Rivas M; Garvey LH; Gómez C; Halken S; Jensen BM; Khaleva E; Knol EF; Kolkhir P; Kurowski M; Lopata AL; Lozoya I; Michaelis LJ; Mohapatra A; Oude Elberink H N G; Panesar SS; Pavão R; Regent A; Ribeiro C; Santos A F; Silva R; Sokolova E; Søndergaard KB; Stensgaard A; Söderström L; Tedner M; Tøttenborg SS; Trautmann A; Turner PJ; Uyttebroek A; Vazquez-Ortiz M; Vlieg-Boerstra B; Weritz N; Yazdanbakhsh M; Zawadzka-Krajewska A; EAACI Guidelines Committee EAACI guidelines: Anaphylaxis (2021 update). Allergy, 2022.PMID 34343358
- [6]Muraro A; Roberts G; Worm M; Bilò MB; Brockow K; Fernández Rivas M; Santos AF; Zolkipli ZQ; Bellou A; Beyer K; Bindslev-Jensen C; Cardona V; DunnGalvin A; Foucard T; de Groot H; Garvey LH; Hourihane J; Kowalski M; Kuitunen M; Lebens AF; McBride D; Oude Elberink H; Papi A; Rancé F; Riemer A; Ring J; Sampson H; Slapke I; Sturm G; Vlieg-Boerstra B; Wöhrl S; Wickman M; Sheikh A; EAACI Food Allergy and Anaphylaxis Guidelines Group Anaphylaxis: guidelines from the European Academy of Allergy and Clinical Immunology. Allergy, 2014.PMID 24909803
- [7]Liew WK; Williamson E; Tang ML Anaphylaxis fatalities and admissions in Australia. J Allergy Clin Immunol, 2009.PMID 19117599
- [8]Mullins RJ; Wainstein BK; Barnes EH; Liew WK; Campbell DE Increases in anaphylaxis fatalities in Australia from 1997 to 2013. Clin Exp Allergy, 2016.PMID 27144664
- [9]Simons FE First-aid treatment of anaphylaxis to food: focus on epinephrine. J Allergy Clin Immunol, 2004.PMID 15131564
- [10]Sicherer SH; Simons FER; SECTION ON ALLERGY AND IMMUNOLOGY Epinephrine for First-aid Management of Anaphylaxis. Pediatrics, 2017.PMID 28193791
- [11]Turner PJ; Jerschow E; Umasunthar T; Lin R; Campbell DE; Boyle RJ Fatal Anaphylaxis: Mortality Rate and Risk Factors. J Allergy Clin Immunol Pract, 2017.PMID 28888247
- [12]Lee S; Bellolio MF; Hess EP; Erwin P; Silber MC; Campbell RL Time of Onset and Predictors of Biphasic Anaphylactic Reactions: A Systematic Review and Meta-analysis. J Allergy Clin Immunol Pract, 2015.PMID 25680923
- [13]Mehr S; Liew WK; Tey D; Tang ML Clinical predictors for biphasic reactions in children presenting with anaphylaxis. Clin Exp Allergy, 2009.PMID 19486033
- [14]Du Toit G; Roberts G; Sayre PH; Bahnson HT; Radulovic S; Santos AF; Brough HA; Phippard D; Basting M; Feeney M; Turcanu V; Sever ML; Gomez Lorenzo M; Plaut M; Lack G; LEAP Study Team Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med, 2015.PMID 25705822