Paeds · allergy-and-immunology
Anaphylaxis: recognition and emergency management
Also known as Anaphylactic shock · Severe allergic reaction · Anaphylactoid reaction · IgE-mediated systemic hypersensitivity · Adrenaline-requiring allergic emergency
Fellowship topic on anaphylaxis in children: the rapid, life-threatening, multisystem hypersensitivity reaction whose decisive treatment is early intramuscular adrenaline; the NIAID/FAAN definition and Brown severity grading; the IgE and non-IgE mast-cell and basophil mediator cascade producing upper-airway obstruction, bronchospasm and distributive shock; the triggers (food, drug, venom, idiopathic), the paediatric epidemiology of rising incidence and the fatal case profile (asthma, teenagers, delay in adrenaline); recognition that up to a fifth have no skin signs; the emergency algorithm — call help, remove trigger, IM adrenaline by weight/age band, positioning, oxygen and fluids, refractory management; tryptase timing; the biphasic reaction and observation periods; the discharge package of autoinjector, action plan and allergy referral; and ASCIA, EAACI, NICE and WAO regional guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Anaphylaxis in one line — and the rule that saves lives
Overview & Definition
Picture a four-year-old with a known peanut allergy who, ten minutes after biting into a biscuit at a birthday party, becomes flushed, starts to cough and wheeze, and tells his mother his throat feels funny. Within a minute his lips and tongue are swelling and he is drooling. His mother gives his adrenaline autoinjector into his thigh and calls an ambulance, and by the time help arrives he is already recovering. That sequence — a rapid multisystem reaction, an early intramuscular adrenaline, and a complete recovery — is anaphylaxis in its clearest form, and the whole fellowship answer hangs on understanding why adrenaline given early reverses everything while adrenaline given late may not. [1] [8]
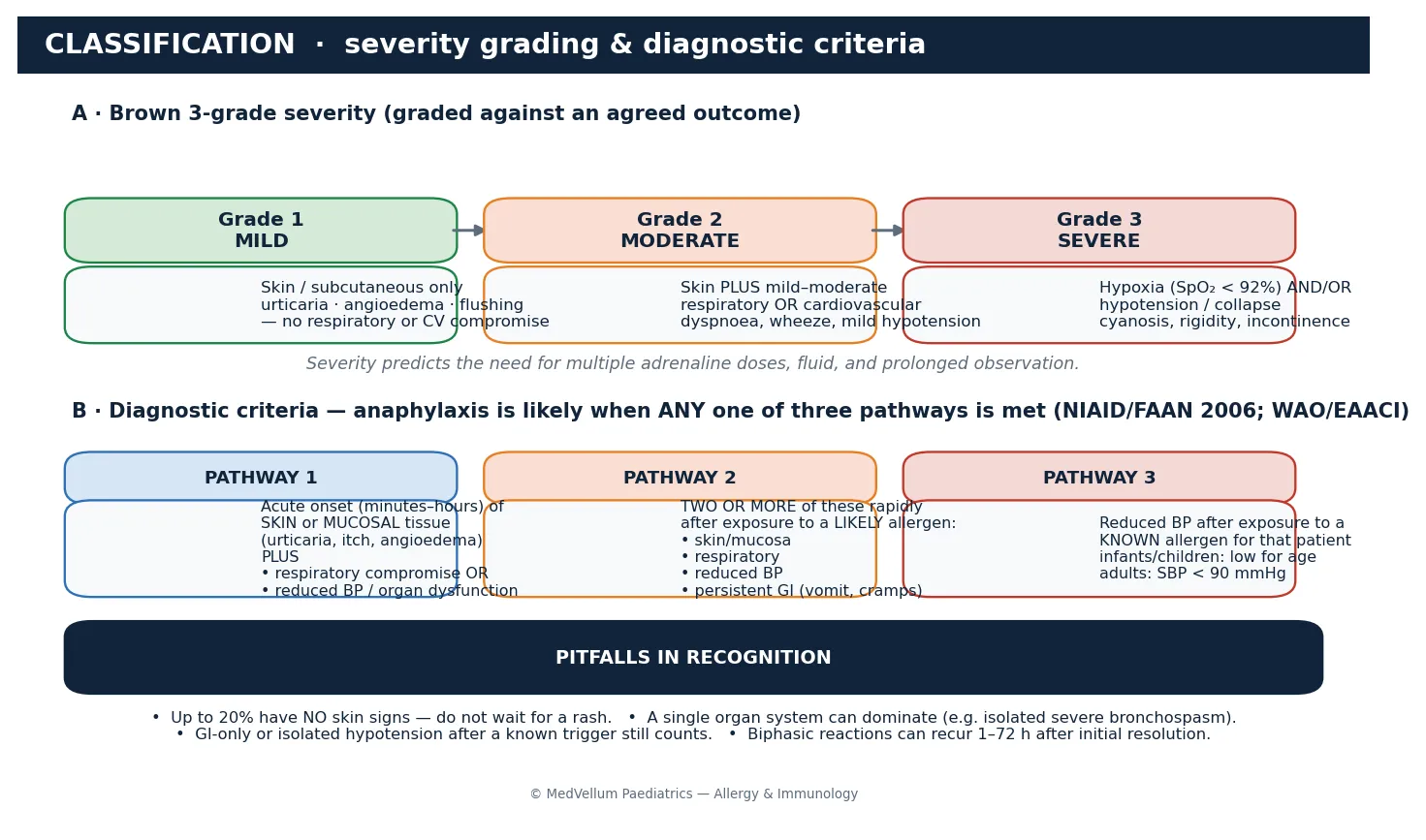
Anaphylaxis is a severe, life-threatening generalised or systemic hypersensitivity reaction. It is acute in onset, usually progressing over minutes rather than hours, and it is multisystem — the skin and mucous membranes are involved in most but not all reactions, and the danger lies in the respiratory and cardiovascular compromise that follows. The 2006 NIAID/FAAN second symposium, summarised by Sampson and colleagues, gave the operational definition that clinicians now use at the bedside, because it allows treatment to begin without waiting for laboratory confirmation. [1] [5]
The clinical task has two halves that the examination separates sharply. The first half is the emergency: recognise the reaction, give intramuscular adrenaline early, support the airway, breathing and circulation, and escalate if it does not resolve. The second half is the aftermath: confirm the trigger, prevent the next reaction, and send the child home equipped — with an autoinjector, a written action plan, an allergy referral, and a family and school who know exactly what to do. A candidate who treats only the acute event and forgets the prevention package fails the question. [3] [8]
Classification
Anaphylaxis is classified along three axes that each change what you do: by severity, by trigger, and by mechanism. The severity axis matters most at the bedside because it predicts how aggressive resuscitation must be and how long to observe. Brown's three-grade system, validated against an agreed clinical outcome, grades the reaction by how badly the respiratory and cardiovascular systems are hit. Grade one is skin and subcutaneous tissue only — urticaria, angioedema, flushing — with no respiratory or cardiovascular compromise. Grade two adds mild to moderate respiratory or cardiovascular involvement such as dyspnoea, wheeze or mild hypotension. Grade three is the severe, hypoxic or hypotensive reaction with cyanosis, collapse or incontinence, and it is the one that demands multiple adrenaline doses, fluid, and a high level of observation. [2] [5]
The second axis is the trigger, because identifying it drives prevention. In children, food is the commonest culprit — peanut, tree nuts, egg, cow's milk and seafood — followed by drugs (antibiotics, neuromuscular blockers, non-steroidal anti-inflammatory drugs) and insect venom (bee and wasp). Around a third of reactions have no identified trigger and are labelled idiopathic, which is a diagnosis of exclusion made only after a thorough allergy workup. Recognising the trigger class directs the history, the subsequent allergy testing, and the avoidance advice. [3] [4]
The third axis is the mechanism, which separates the classic IgE-mediated reaction from the non-IgE pathways that produce an identical clinical picture. In the IgE-mediated reaction, re-exposure to an allergen cross-links allergen-specific IgE bound to the high-affinity receptor on mast cells and basophils, triggering degranulation. In non-IgE anaphylaxis, the mast cell is activated directly or through complement, immune-complex, or cyclo-oxygenase pathways — opioids, radiocontrast media, vancomycin and non-steroidal anti-inflammatory drugs are the classic examples. The mechanism distinction matters for investigation (skin-prick and specific-IgE testing targets the IgE pathway) but not for treatment, because the clinical picture and the adrenaline response are the same. [3] [12]
Epidemiology & Risk Factors
Where does anaphylaxis sit in modern paediatrics, and who dies from it? The incidence of anaphylaxis has risen sharply over the past two decades, driven principally by the increase in food allergy in young children, and it is now one of the commonest reasons a child receives an adrenaline autoinjector. Hospital admissions for anaphylaxis in children have increased several-fold across high-income countries, and food has overtaken drugs and venom as the leading trigger in the paediatric age group. Understanding who is at highest risk focuses both the acute vigilance and the prevention effort. [4] [6]
The fatal case profile is narrow and important, because it tells you exactly where vigilance must be highest. Fatal food anaphylaxis is concentrated in the second decade of life — teenagers and young adults — and the recurring risk factors are poorly controlled asthma, a known food allergy (especially peanut or tree nut), a delay in giving adrenaline, and the social pressures and risk-taking that lead adolescents to eat unsafe food and to hesitate before using their autoinjector. The systematic review by Umasunthar and colleagues quantified the incidence of fatal food anaphylaxis and confirmed that, although the absolute risk to any individual child is low, the risk clusters in this identifiable group. [7] [11]
Cofactors amplify a reaction and explain why the same allergen causes a trivial reaction one day and anaphylaxis the next. Exercise, acute infection, non-steroidal anti-inflammatory drugs, alcohol and, in the perioperative setting, beta-blocker or angiotensin-converting-enzyme inhibitor therapy all lower the threshold or worsen the response. Food-dependent exercise-induced anaphylaxis is the classic cofactor combination in young people: the food alone or the exercise alone is tolerated, but together they trigger a severe reaction. Asking about cofactors is part of every allergy history because they change both the avoidance advice and the risk assessment. [4] [12]
Pathophysiology
Why does a swollen lip become a collapsed, wheezy, hypotensive child within minutes, and why does a single drug reverse all of it? The answer is the mast-cell and basophil mediator cascade and the way adrenaline maps onto every step of it. On re-exposure, the allergen cross-links allergen-specific IgE bound to the high-affinity Fc-epsilon-RI receptor on mast cells and basophils, and the cell degranulates, releasing both preformed mediators (histamine, tryptase, heparin) and newly synthesised lipid mediators (leukotrienes, prostaglandins, platelet-activating factor). [3] [12]
These mediators produce the end-organ effects that define the clinical picture and that kill. Histamine and the lipid mediators increase vascular permeability, producing the oedema that swells the lip and the larynx and that shifts fluid out of the circulation. They cause vasodilation, producing the flushing, the warmth and the distributive shock. They cause bronchospasm, producing the wheeze and the hypoxia. Platelet-activating factor is a particular villain — its level correlates with severity, and its degradation correlates with recovery. The same cascade, in a different balance, produces urticaria in one child and circulatory collapse in another. [2] [3]
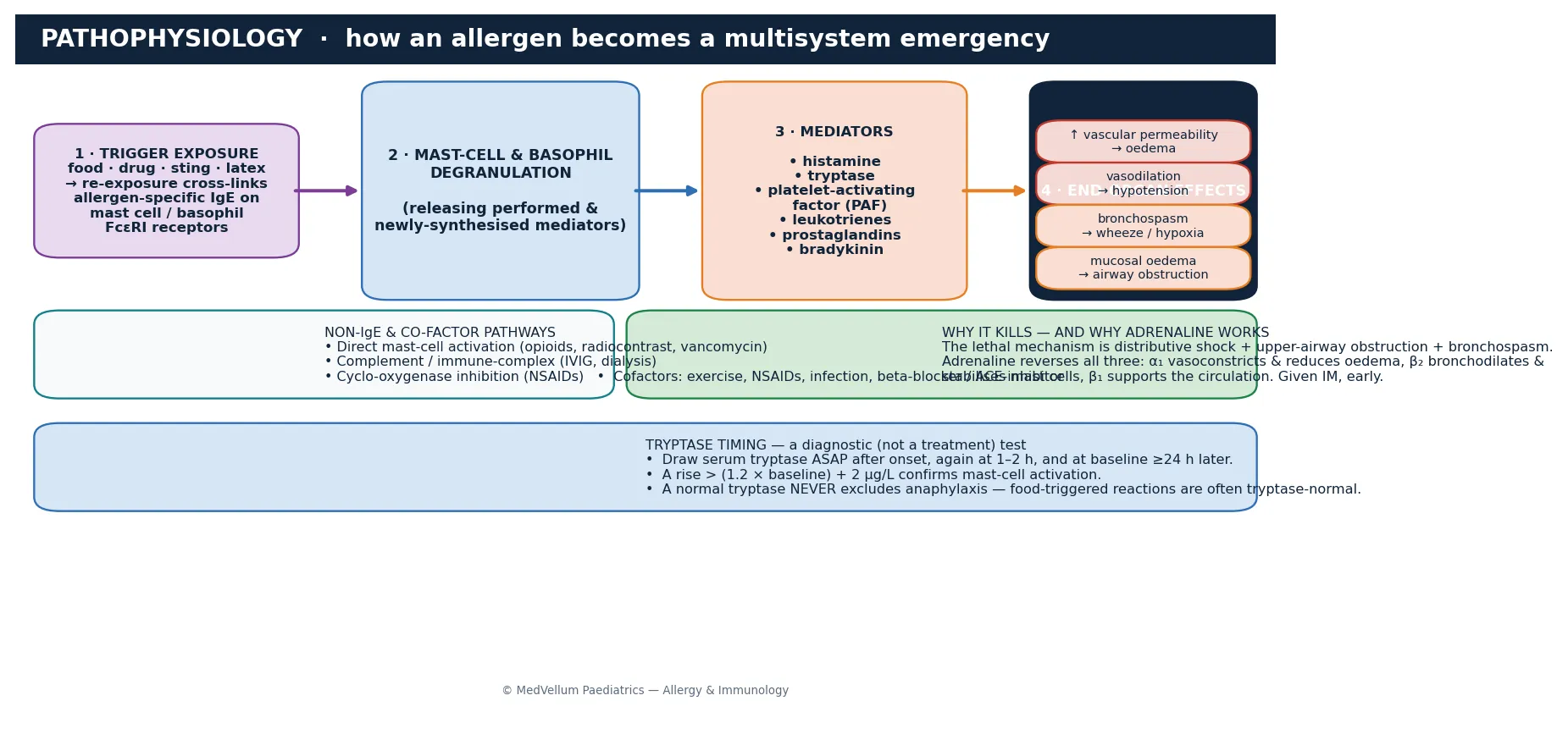
The reason adrenaline is the perfect antidote is that it acts on every limb of the cascade through its receptor profile. Alpha-1 stimulation causes vasoconstriction, reversing the oedema and the distributive shock and restoring venous return and blood pressure. Beta-2 stimulation bronchodilates and stabilises the mast cell membrane, reducing further mediator release. Beta-1 stimulation supports the heart rate and contractility. No other drug covers all three limbs, which is why antihistamines, steroids and bronchodilators are adjuncts and never substitutes for adrenaline. This receptor logic is what the examiner is probing when they ask why adrenaline and not an antihistamine. [3] [8]
The biphasic reaction is the pathophysiological reason for observation. In a proportion of patients — around three to five per cent in most series, higher in severe reactions — symptoms recur one to seventy-two hours after the initial reaction has fully resolved, without further allergen exposure. The mechanism is incompletely understood but probably reflects ongoing late-phase mediator release and a primed mast-cell population. The biphasic reaction is why a child who has apparently recovered cannot simply be sent home, and why the observation decision is a severity-graded judgement rather than a reflex. [9] [4]
Clinical Presentation
The presentation is multisystem and rapid, and the key skill is synthesising the systems into a single decision rather than waiting for each to declare itself. Most reactions begin within minutes of exposure, though the onset can be delayed by an hour or more. Skin and mucosal involvement is the commonest feature — flushing, generalised urticaria, angioedema of the lips, tongue, face and periorbital tissues, and pruritus — and it is present in around four-fifths of reactions. The danger is in assuming that the skin must be involved, because up to a fifth of reactions have no skin signs at all. [1] [2]
Respiratory compromise is the commonest system to threaten life in children, and it is the one most magnified by asthma. The child develops rhinitis and hoarseness, a sensation of throat tightness or closure, stridor and drooling from upper-airway oedema, cough, wheeze, tachypnoea, accessory-muscle use and, in the worst case, silent chest and cyanosis. Because children's airways are smaller, even modest laryngeal oedema can critically narrow the lumen, and the asthmatic child is at particular risk because the bronchospasm compounds an already reactive airway. [3] [11]
Cardiovascular compromise ranges from tachycardia and a narrowed pulse pressure through hypotension, pallor, mottling and collapse to cardiac arrest from profound distributive shock and hypoxia. Gastrointestinal features — abdominal cramps, vomiting and diarrhoea — reflect gut smooth-muscle contraction and are easily mistaken for gastroenteritis when the history of a trigger is not elicited. Neurological features — dizziness, confusion, a sense of impending doom and, in infants, sudden floppiness — reflect cerebral hypoperfusion. The synthesis is the skill: skin plus respiratory, or skin plus cardiovascular, or two or more systems after a likely allergen, is anaphylaxis. [2] [5]
The features that change disposition are the red flags: stridor or throat closure signalling impending airway obstruction; marked wheeze or hypoxia signalling severe bronchospasm; hypotension or collapse signalling shock; any reaction that needed two adrenaline doses; and any child on a beta-blocker. A child with isolated urticaria and no respiratory or cardiovascular compromise can usually be observed briefly and discharged, but a child with any red flag needs admission, observation, and a clear escalation plan. [3] [9]
Differential Diagnosis
The differential for an acute, multisystem collapse with respiratory distress is broad, and the trap is twofold: missing anaphylaxis when the cause is something else, and missing something else by labelling it anaphylaxis. The common mimics include a severe asthma exacerbation (wheeze and respiratory distress without urticaria or a trigger history), a vasovagal syncope (pallor and collapse after a trigger such as a procedure or sight of blood, with bradycardia rather than tachycardia and rapid full recovery once supine), and a panic attack (hyperventilation, paraesthesia and a sense of doom without objective hypotension, hypoxia or skin signs). [5] [4]
Other acute emergencies enter the differential when the presentation is dominated by one system. Upper-airway obstruction from a foreign body or epiglottitis can mimic the laryngeal oedema of anaphylaxis; distributive shock from sepsis can mimic the cardiovascular collapse; and hereditary angioedema — a complement-mediated, histamine-resistant swelling that runs in families and is unresponsive to adrenaline — must be considered when angioedema recurs without urticaria and is treated with C1-esterase-inhibitor replacement. A careful history of the trigger, the timing and the systems involved, together with the tryptase pattern, usually separates them. [4] [12]
The skin-only differential matters because isolated urticaria and angioedema are common and do not by themselves need adrenaline, but they coexist with anaphylaxis and can precede it. Acute urticaria from infection or a drug, and acute angioedema, must be distinguished from anaphylaxis by the presence or absence of respiratory and cardiovascular compromise. The safe rule is that any skin reaction accompanied by respiratory or cardiovascular symptoms is anaphylaxis until shown otherwise, and that a skin reaction alone is treated with antihistamines and observation. [5] [4]
Clinical & Bedside Assessment
The assessment in the acute setting is simultaneous with treatment and follows the airway, breathing, circulation, disability, exposure framework. The first move is to recognise the reaction and call for help while the airway and circulation are secured. Assess the airway for stridor, drooling and tongue or lip swelling; the breathing for wheeze, respiratory rate, effort and oxygen saturation; and the circulation for heart rate, blood pressure, capillary refill, pallor and level of consciousness. Lie the child flat with legs raised to improve venous return, sit them up if breathing is distressed, and place them in the left lateral position if pregnant or unconscious. [3] [4]
The history that anchors the diagnosis is taken in parallel, often from the parent or a witness while resuscitation proceeds. Establish the trigger and the timing — what was eaten, injected or stung, and how many minutes elapsed before symptoms began. Ask about the progression and the systems involved, the child's known allergies and atopic background (asthma, eczema, allergic rhinitis), and whether an adrenaline autoinjector was given, when, and by whom. A history of asthma is not a minor detail; it is a predictor of severity and fatal outcome, and it must be asked for explicitly. [5] [11]
Examine for the features that change the immediate plan. Confirm the site and severity of airway compromise, listen for wheeze and assess the work of breathing, and measure the blood pressure and perfusion. Look for the skin signs — flushing, urticaria, angioedema — but treat them as supportive rather than necessary. Check the medication list for beta-blockers and angiotensin-converting-enzyme inhibitors, which blunt the response to adrenaline and mark the patient out for glucagon and infusion strategies. [4] [12]
Document the essentials that drive the subsequent investigation and prevention. Record the time of onset, the suspected trigger, the number and timing of adrenaline doses, and the lowest blood pressure and oxygen saturation. Arrange the tryptase samples at the correct intervals, because a single random tryptase is far less useful than a timed series. These details determine whether the diagnosis is confirmed, whether the trigger is identified, and whether the child leaves with a correct prevention plan. [3] [4]
Investigations
Anaphylaxis is a clinical diagnosis, and treatment must never be delayed for investigations. The only laboratory test that supports the diagnosis during the acute event is the serum tryptase, and even it is not required to make the call. Tryptase should be drawn as soon as possible after the onset of the reaction, again at one to two hours, and at a baseline time point at least twenty-four hours later. A rise that exceeds 1.2 times the baseline plus 2 micrograms per litre confirms mast-cell activation. The timing matters because tryptase peaks and falls quickly, so a single late sample can be normal even in a genuine reaction. [3] [4]
The critical limitation of tryptase is that a normal value never excludes anaphylaxis. Food-triggered reactions in particular are often tryptase-normal, because gut mast cells release less tryptase than the skin and systemic mast cells targeted by venom or drug. A candidate who waits for a tryptase result, or who excludes the diagnosis on a normal tryptase, has misunderstood the test completely. Tryptase is a confirmatory and research tool, not a gatekeeper for adrenaline. [4] [12]
In Australia and Aotearoa New Zealand, ASCIA provides the emergency-management algorithm, the adrenaline autoinjector dose recommendations and the standardised ASCIA action plan that every child with confirmed anaphylaxis should carry. ASCIA's guidance specifies the weight- and age-based adrenaline doses, the observation advice, and the post-event referral to an allergy specialist, and it underpins school and childcare anaphylaxis policy across both countries. [3]
The trigger-identification workup follows once the child is stable and is usually done in the specialist allergy clinic, not in the emergency department. Skin-prick testing and allergen-specific serum IgE detect sensitisation to suspected IgE-mediated triggers, and they are interpreted in the light of the history because sensitisation alone does not prove the trigger. Component-resolved diagnostics (for example, Ara h 2 for peanut) refine the risk assessment, and a supervised oral food challenge is the gold standard when the history and tests are discordant. Baseline tryptase also guides the decision to investigate clonal mast-cell disorders in adults with recurrent unexplained anaphylaxis, though this is rare in children. [4] [5]
Management — Resuscitation
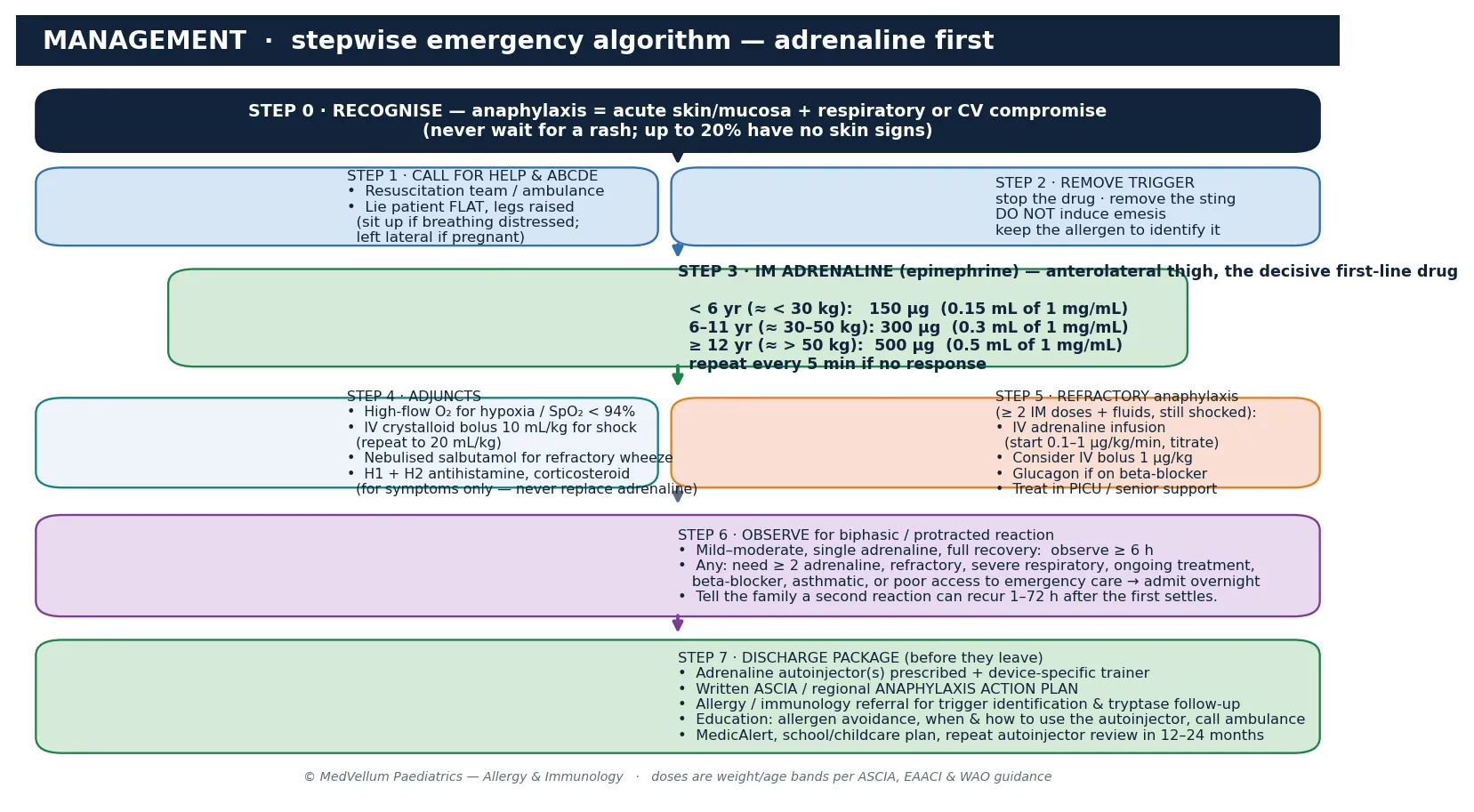
Resuscitation of anaphylaxis is a fixed, memorised algorithm in which the single decisive act is early intramuscular adrenaline. The first steps are simultaneous: recognise the reaction, call for the resuscitation team or ambulance, remove the trigger where possible, and lie the child flat with the legs raised. Positioning alone improves venous return and can prevent the circulatory collapse that kills, and sitting a hypotensive patient up can precipitate cardiac arrest — a documented and avoidable error. [3] [8]
Adrenaline is given intramuscularly into the anterolateral thigh (the vastus lateralis), where absorption is rapid and reliable, and it is dosed by weight or age band. For a child under about six years or under thirty kilograms the dose is 150 micrograms, which is 0.15 millilitres of the 1 milligram per millilitre (1 in 1000) concentration; for six to eleven years or about thirty to fifty kilograms it is 300 micrograms; and for twelve years and over or over fifty kilograms it is 500 micrograms, which is 0.5 millilitres of the 1 in 1000 concentration. The dose is repeated every five minutes if there is no response, and most autoinjectors deliver the 150 or 300 microgram doses that match these bands. [3] [4]
Adrenaline (epinephrine) — IM, first-line in anaphylaxis
Adjuncts support the adrenaline but never replace it. Give high-flow oxygen to any child with hypoxia or an oxygen saturation below 94 per cent. Give an intravenous crystalloid bolus of 10 millilitres per kilogram to the shocked child, repeating to 20 millilitres per kilogram if needed, because the vasodilation and capillary leak produce large fluid deficits. Nebulised salbutamol treats refractory bronchospasm. An H1 antihistamine relieves urticaria and pruritus, an H2 antihistamine and a corticosteroid are traditional adjuncts, but their onset is too slow and their effect too narrow to alter the acute course — they are for symptom comfort and the historical hope of preventing a biphasic reaction, never for life support. [3] [4]
Management — Definitive & Stepwise
The definitive pathway runs from the first adrenaline dose through to the discharge package, and it is the structure that earns the marks. After the resuscitation steps, the child who responds fully is stabilised and observed; the child who does not respond escalates; and every child, before discharge, receives the prevention equipment. The stepwise nature is what distinguishes a complete answer from an adrenaline-only answer, because the prevention package is what stops the next fatal reaction. [8] [4]
The stepwise anaphylaxis pathway
Recognise anaphylaxis from the NIAID/FAAN criteria and do not wait for a rash — up to a fifth of reactions have no skin signs.
Call for help, remove the trigger, and lie the child flat with legs raised; sit up if breathing is distressed, left lateral if pregnant or unconscious.
Give IM adrenaline into the anterolateral thigh by weight or age band (150 µg < 6 yr, 300 µg 6–11 yr, 500 µg ≥ 12 yr), repeating every 5 minutes if no response.
Add high-flow oxygen, an IV crystalloid bolus (10–20 mL/kg) for shock, and a bronchodilator for refractory wheeze; antihistamine and steroid for symptoms only.
If refractory — two or more IM doses, ongoing shock, or a patient on a beta-blocker — start an IV adrenaline infusion (0.1–1 µg/kg/min) and consider glucagon; treat in PICU.
Draw serum tryptase on arrival, at 1–2 hours, and at baseline after 24 hours; never let the result delay or deny treatment.
Observe for the biphasic reaction; admit overnight if severe, multiple adrenaline doses, asthma, beta-blocker, or poor access to emergency care.
Discharge with an adrenaline autoinjector, a written ASCIA action plan, allergy referral, and family and school education on avoidance and autoinjector use.
Refractory anaphylaxis is the escalation that every candidate must be able to describe. If a child has received two or more intramuscular adrenaline doses and adequate fluid yet remains shocked or hypoxic, an intravenous adrenaline infusion is started at 0.1 to 1 microgram per kilogram per minute and titrated to the response, with a peripheral intravenous bolus of about 1 microgram per kilogram reserved for the peri-arrest or arrested patient under experienced hands. A child on a beta-blocker who is refractory to adrenaline should receive glucagon, which bypasses the receptor blockade. Refractory disease is managed in the paediatric intensive care unit with senior support, because it signals a reaction that is overwhelming the catecholamine response. [4] [3]
Specific Subtypes & Scenarios
A food-triggered reaction in a young child. A preschool child with a known food allergy develops flushing, lip swelling and wheeze within minutes of eating. The response is to recognise the multisystem involvement, lie the child flat, give 150 micrograms of intramuscular adrenaline into the thigh, and call for help. The family is taught that the same food caused the reaction, the trigger is confirmed in allergy clinic, and the child leaves with an autoinjector and an action plan. Food is the commonest paediatric trigger and the model for the whole algorithm. [6] [8]
The asthmatic adolescent with no skin signs. A teenager with asthma and a peanut allergy becomes dizzy, wheezy and pale in the school yard after shared food, with no rash. This is the dangerous atypical case and the profile of the fatal paediatric reaction. The absence of skin signs must not delay adrenaline; the asthma magnifies the bronchospasm; and the adolescent hesitation before using the autoinjector is a recurring contributor to death. Early intramuscular adrenaline and oxygen are the priorities, with close attention to the asthma. [11] [6]
An insect-sting reaction. A child stung by a bee develops local swelling that generalises within minutes to urticaria, abdominal cramps and hypotension. Intramuscular adrenaline and fluids are given, and the trigger is confirmed by venom-specific IgE testing. Children with confirmed venom anaphylaxis are candidates for venom immunotherapy, which is highly effective at preventing recurrence, and this referral is part of the discharge plan. [3] [12]
A drug or perioperative reaction. A child collapses with bronchospasm and hypotension minutes after an antibiotic or a neuromuscular blocker. The non-IgE and IgE pathways overlap in the perioperative setting, the skin signs are often hidden under drapes, and the anaesthetic team gives intravenous adrenaline because access is already established. The subsequent investigation includes tryptase timing and specialist drug-allergy referral to identify the culprit and to delabel where appropriate. [4] [5]
A refractory or protracted reaction. A child who has needed two or more adrenaline doses and remains unwell is in refractory anaphylaxis and is managed in the paediatric intensive care unit with an intravenous adrenaline infusion. The search for a beta-blocker or other cofactor is urgent, glucagon is considered if a beta-blocker is present, and the observation is prolonged because these patients are at highest risk of a biphasic recurrence. [4] [9]
A biphasic recurrence. A child who fully recovered in the emergency department returns six hours later with wheeze and hypotension, without further allergen exposure. This is the biphasic reaction, and it is the reason for observation. Management is the same adrenaline-first algorithm, and the lesson for discharge is that a second reaction can recur for up to seventy-two hours and the family must know to use the autoinjector again and call an ambulance. [9] [10]
Complications & Pitfalls
The central pitfall, and the one that kills, is a delay in giving intramuscular adrenaline. Audit data and the fatal-case literature repeatedly identify delayed or absent adrenaline as the single reversible factor in fatal paediatric anaphylaxis. The reasons are familiar: waiting for a rash, attributing wheeze to asthma alone, hesitating because of the perceived danger of adrenaline, or treating with an antihistamine or a steroid first. None of these is defensible. Adrenaline given intramuscularly in correct doses is remarkably safe, and the risk of giving it when anaphylaxis is merely suspected is far smaller than the risk of withholding it when anaphylaxis is real. [11] [8]
The second pitfall is failing to recognise anaphylaxis without skin signs. Up to a fifth of reactions have no urticaria or flushing, and the child who presents with isolated bronchospasm, hypotension or collapse after a trigger is in anaphylaxis until proven otherwise. Anchoring on the skin as a required criterion closes the door to adrenaline at the moment it is most needed, and the asthmatic adolescent with food anaphylaxis and no rash is the exact patient this error harms. [1] [11]
A third pitfall is incorrect adrenaline dosing or route. Subcutaneous adrenaline is absorbed too slowly to be useful, intravenous bolus adrenaline outside the arrest setting is dangerous, and doses that are estimated rather than weight- or age-banded risk underdosing the small child or overdosing the large one. The anterolateral thigh is the correct site because absorption is fastest there, and the weight- or age-band dose (150, 300 or 500 micrograms) is the one to memorise. [3] [4]
A fourth pitfall is discharging the patient without the prevention package. A child who has had anaphylaxis and is sent home without an adrenaline autoinjector, a written action plan, and an allergy referral is set up for a recurrent reaction that may be fatal. The discharge encounter is as load-bearing as the resuscitation, and the autoinjector, the plan, the trigger identification, and the education of the family and the school are non-negotiable. [8] [4]
The fifth pitfall is over-reliance on tryptase. A normal tryptase never excludes anaphylaxis, and waiting for the result or using it to withhold treatment misunderstands the test. Tryptase confirms mast-cell activation when the timing is correct and the rise exceeds the threshold, but it is a confirmatory and research tool, not a decision rule for adrenaline. [4] [12]
Prognosis & Disposition
Most children with anaphylaxis who receive early adrenaline recover fully and completely, and the immediate prognosis is excellent when the algorithm is followed. The morbidity and mortality are concentrated in the small group in whom adrenaline is delayed, in the asthmatic adolescent with food anaphylaxis, and in the patient who has a refractory or biphasic course. For the typical child who responds to a single adrenaline dose and recovers, the prognosis is one of full recovery, with the long-term question being prevention rather than residual harm. [11] [8]
The disposition decision is a severity-graded judgement about the risk of a biphasic recurrence. A child with a mild to moderate reaction that resolved fully with a single adrenaline dose, who is well and has good access to emergency care, can be observed for around six hours and discharged with the prevention package. A child who needed two or more adrenaline doses, who had a refractory or severe course, who has asthma or is on a beta-blocker, who has ongoing symptoms, or who has poor access to emergency care is admitted overnight for observation. The Dribin cohort study of repeat epinephrine timing informs the paediatric observation logic by mapping when second doses fall, supporting risk-stratified rather than blanket observation. [9] [10]
Observation decision after anaphylaxis
Stage 3
Refractory shock or airway compromise needing an adrenaline infusion, or peri-arrest presentation
At discharge, the family is given the prevention package and a clear safety-net for return. The autoinjector is prescribed, ideally two devices, with a trainer of the same brand so the family practises with what they carry. The written ASCIA action plan names the trigger, the dose, and the steps, and it goes to the school or childcare. The family is taught allergen avoidance, when and how to use the autoinjector, and to call an ambulance immediately and use a second device if there is no response. The trigger is confirmed and the prevention plan refined in the allergy clinic, and the autoinjector and plan are reviewed annually. [8] [4]
The risk of recurrence depends on the trigger and the exposure. A child with a confirmed food allergy who continues to be exposed remains at risk, and strict avoidance with autoinjector carriage is the standard. Venom immunotherapy dramatically reduces the risk after insect-sting anaphylaxis, and drug delabelling and avoidance prevent drug-triggered recurrence. Across the life course the message is constant: the child who carries an autoinjector, knows the trigger, and has a plan is the child who survives the next reaction. [3] [4]
Special Populations
Adolescents and young adults are the group at highest risk of fatal food anaphylaxis, because risk-taking, social pressure, poorly controlled asthma and hesitation before using the autoinjector converge. The stance for this group is explicit education, encouragement to carry and to use the device without hesitation, optimal asthma control, and a transition to adult allergy care. The teenager who leaves the consultation believing that using the autoinjector is embarrassing is the teenager at risk. [11] [6]
Children with asthma are at magnified risk because the anaphylactic bronchospasm compounds an already reactive airway, and asthma is a recurring feature of fatal food anaphylaxis. Optimal asthma control, a written asthma plan, and explicit teaching that a wheeze after a food trigger may be anaphylaxis rather than an asthma attack are essential. The child with both conditions carries both the asthma reliever and the adrenaline autoinjector, and knows when each is indicated. [11] [7]
Children with complex chronic illness or who are immunocompromised may have atypical presentations and additional medication interactions, including beta-blockers for cardiac disease that blunt the adrenaline response. These children need individualised action plans and coordinated care between the allergy and the specialty teams, and glucagon must be available if a beta-blocker cannot be ceased. [4] [12]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families may face barriers to autoinjector access, to allergy services and to culturally safe education. The cost of an autoinjector is a real barrier for disadvantaged families, and an action plan in the family's language, delivered with a trained interpreter rather than a family member, is part of equitable care. Disadvantage should never be the reason a child is discharged without the means to survive a recurrence. [4] [3]
Children in out-of-home care and in schools and childcare need a written anaphylaxis plan held by the carer and the institution, staff trained in autoinjector use, and clear protocols for food avoidance and emergency response. School and childcare anaphylaxis policy is a public-health layer that protects the child who cannot yet protect themselves, and the clinician's role includes engaging with the school to ensure the plan is understood and the device is accessible. [8] [3]
Rural and remote children need timely access to adrenaline and to retrieval, because the distances and the ambulance times mean that the autoinjector and the family's competence are the first response. Telehealth links to allergy services, clear local protocols, and early mobilisation of retrieval for severe reactions are part of equitable care for the child far from the emergency department. [4] [11]
Evidence, Guidelines & Regional Differences
The definitional and severity-grading evidence underpins the whole field. The NIAID/FAAN second symposium, summarised by Sampson and colleagues in 2006, gave the operational diagnostic criteria that clinicians use at the bedside, and Brown's severity grading in the Journal of Allergy and Clinical Immunology provided the validated three-grade scale that predicts the need for multiple adrenaline doses and prolonged observation. Together they turn a syndrome that was once loosely defined into a recognisable, treatable emergency. [1] [2]
The guideline structure is now remarkably consistent across regions. The World Allergy Organization guidelines for the assessment and management of anaphylaxis, led by Simons and colleagues in 2011 and updated in 2012, set the global standard, and the European Academy of Allergy and Clinical Immunology anaphylaxis guidelines (2021 update), led by Muraro and Worm, define the European practice. The 2010 Joint Task Force practice parameter, led by Lieberman and colleagues, is the North American counterpart. All converge on the same message: recognise early, give intramuscular adrenaline first, support the circulation, observe for the biphasic reaction, and discharge with an autoinjector and a plan. [3] [4]
Paediatric anaphylaxis observation periods
Population: A multicentre retrospective cohort of paediatric emergency department anaphylaxis visits, examining the timing of repeat epinephrine to inform observation decisions.
Key finding
The timing of repeat epinephrine doses was mapped across the cohort, providing an evidence base for risk-stratified paediatric observation periods rather than a single blanket duration.
Practice change
Observation after paediatric anaphylaxis should be tailored to severity, the number of adrenaline doses and co-morbidity (especially asthma), supporting shorter observation for low-risk and longer observation or admission for high-risk presentations.
The fatal-case epidemiology defines where vigilance must be highest. The UK national data analysis by Baseggio Conrado and colleagues, covering food anaphylaxis from 1998 to 2018, documented the rising incidence and the fatal-case profile, and the systematic review by Umasunthar and colleagues quantified the incidence of fatal food anaphylaxis. The review by Anagnostou and colleagues, "Fatal Food Anaphylaxis: Distinguishing Fact From Fiction", clarified the true magnitude of risk and the avoidable factors, principally delayed adrenaline and undertreated asthma. [6] [11]
The first-aid and biphasic evidence completes the picture. The American Academy of Pediatrics guidance on epinephrine for first-aid management, by Sicherer and Simons, established the role of the lay autoinjector, and the predictors of biphasic reactions identified by Lee and colleagues define who must be observed. The regional policy instruments — the ASCIA acute-management guidelines and action plans in ANZ, the NICE guidance on assessment and referral in the UK, and the Resuscitation Council algorithms — translate the evidence into practice, and the principle is identical everywhere: adrenaline first, by the intramuscular route, early. [8] [9]
Exam Pearls
- Anaphylaxis is a rapid, multisystem, life-threatening hypersensitivity reaction; the onset is usually minutes after a trigger and the decisive treatment is intramuscular adrenaline. [1]
- The NIAID/FAAN criteria: skin or mucosa plus respiratory or cardiovascular compromise; or two or more systems after a likely allergen; or hypotension after a known allergen. [1]
- Up to 20% have no skin signs — never wait for a rash, and never exclude the diagnosis on its absence. [11]
- Brown severity grading: grade 1 skin only, grade 2 skin plus respiratory or cardiovascular, grade 3 hypoxia or hypotension. [2]
- Food is the commonest paediatric trigger (peanut, tree nut, egg, milk, seafood); drugs and venom follow; about a third are idiopathic. [6]
- IM adrenaline into the anterolateral thigh: 150 µg under about six years, 300 µg six to eleven years, 500 µg twelve years and over; repeat every 5 minutes. [3]
- Adrenaline receptor logic: alpha-1 reverses oedema and shock, beta-2 bronchodilates and stabilises mast cells, beta-1 supports the heart. [3]
- Biphasic reactions recur in 1–72 h; admit overnight if ≥ 2 adrenaline doses, refractory, severe, asthmatic, on a beta-blocker, or poor access to care. [9]
- Refractory disease (≥ 2 IM doses or beta-blocker) escalates to an IV adrenaline infusion (0.1–1 µg/kg/min) and glucagon for beta-blockade. [4]
- Tryptase is drawn on arrival, at 1–2 h, and at baseline after 24 h; a normal value never excludes anaphylaxis. [4]
- The discharge package is non-negotiable: adrenaline autoinjector, written action plan, allergy referral, and family and school education. [8]
- Fatal paediatric anaphylaxis clusters in asthmatic adolescents with food allergy and delayed adrenaline — the single reversible factor. [11]
References
- [1]Sampson HA; Muñoz-Furlong A; Campbell RL; et al Second symposium on the definition and management of anaphylaxis: summary report--second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. Ann Emerg Med, 2006.PMID 16546624
- [2]Brown SG Clinical features and severity grading of anaphylaxis. J Allergy Clin Immunol, 2004.PMID 15316518
- [3]Simons FE; Ardusso LR; Bilò MB; et al World allergy organization guidelines for the assessment and management of anaphylaxis. World Allergy Organ J, 2011.PMID 23268454
- [4]Muraro A; Worm M; Alviani C; et al EAACI guidelines: Anaphylaxis (2021 update). Allergy, 2022.PMID 34343358
- [5]Lieberman P; Nicklas RA; Oppenheimer J; et al The diagnosis and management of anaphylaxis practice parameter: 2010 update. J Allergy Clin Immunol, 2010.PMID 20692689
- [6]Baseggio Conrado A; Ierodiakonou D; Gowland MH; et al Food anaphylaxis in the United Kingdom: analysis of national data, 1998-2018. BMJ, 2021.PMID 33597169
- [7]Umasunthar T; Leonardi-Bee J; Hodes M; et al Incidence of fatal food anaphylaxis in people with food allergy: a systematic review and meta-analysis. Clin Exp Allergy, 2013.PMID 24118190
- [8]Sicherer SH; Simons FER; SECTION ON ALLERGY AND IMMUNOLOGY Epinephrine for First-aid Management of Anaphylaxis. Pediatrics, 2017.PMID 28193791
- [9]Lee S; Bellolio MF; Hess EP; et al Predictors of biphasic reactions in the emergency department for patients with anaphylaxis. J Allergy Clin Immunol Pract, 2014.PMID 24811018
- [10]Dribin TE; Sampson HA; Zhang Y; et al Timing of repeat epinephrine to inform paediatric anaphylaxis observation periods: a retrospective cohort study. Lancet Child Adolesc Health, 2025.PMID 40506197
- [11]Anagnostou A; Sharma V; Herbert L; et al Fatal Food Anaphylaxis: Distinguishing Fact From Fiction. J Allergy Clin Immunol Pract, 2022.PMID 34656799
- [12]Simons FE; Ardusso LR; Bilò MB; et al 2012 Update: World Allergy Organization Guidelines for the assessment and management of anaphylaxis. Curr Opin Allergy Clin Immunol, 2012.PMID 22744267