Paeds · allergy-and-immunology
Atopic dermatitis and the atopic march
Also known as atopic eczema · atopic dermatitis · childhood eczema · infantile eczema · the atopic march · atopic march
A chronic, itchy, relapsing inflammatory skin disease of childhood driven by epidermal barrier failure and Th2-skewed immunity, presenting with age-pattern eczema; managed with a stepwise emollient-and-topical-steroid ladder and linked to the atopic march of food allergy, asthma and rhinitis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A baby who sleeps badly, scratches until the cheeks weep, and develops crusted red plaques on the extensor surfaces of the arms is the everyday face of atopic dermatitis in primary care. The disease is a chronic, intensely itchy, relapsing inflammatory skin disorder that begins in infancy in most children and follows a fluctuating course of flares and remissions, driven by a defective epidermal barrier and a Th2-skewed immune response. [1]
Atopic dermatitis is the most common chronic skin disease of childhood, affecting up to one in five children worldwide, and it is the first and most frequent manifestation of atopy. The term atopic march describes the typical temporal progression from atopic dermatitis and food allergy in infancy to allergic rhinitis and asthma through the preschool and school-age years, reflecting how a single barrier-and-immune defect can seed disease across multiple organ systems. [2]
Classification
Atopic dermatitis is classified along three complementary axes that together capture how the disease looks, how severe it is, and how it confirms its identity. The UK Working Party diagnostic criteria provide the case-definition gate, the age-based morphological pattern frames the clinical picture, and the validated severity scores quantify disease burden for treatment decisions and follow-up. [1]
The UK Working Party criteria require an itchy skin condition (or parental report of rubbing in a child) plus at least three of five supporting features: a history of involvement of the skin creases, a personal or immediate-family history of atopy, a history of generally dry skin, visible flexural dermatitis on examination, and onset before the age of two years. These criteria carry high sensitivity and specificity in population studies and remain the standard diagnostic anchor taught in paediatric exams. [1]
The age-based morphological pattern evolves predictably. Infants present with acute, weepy, crusted eczema on the cheeks, scalp and extensor surfaces, often sparing the nappy area, while children from about two years onward shift to chronic, lichenified, flexural eczema of the antecubital and popliteal folds, wrists, ankles and neck. Adolescents and adults may show a more localised, lichenified pattern on the hands, feet and periorbital skin. [10]
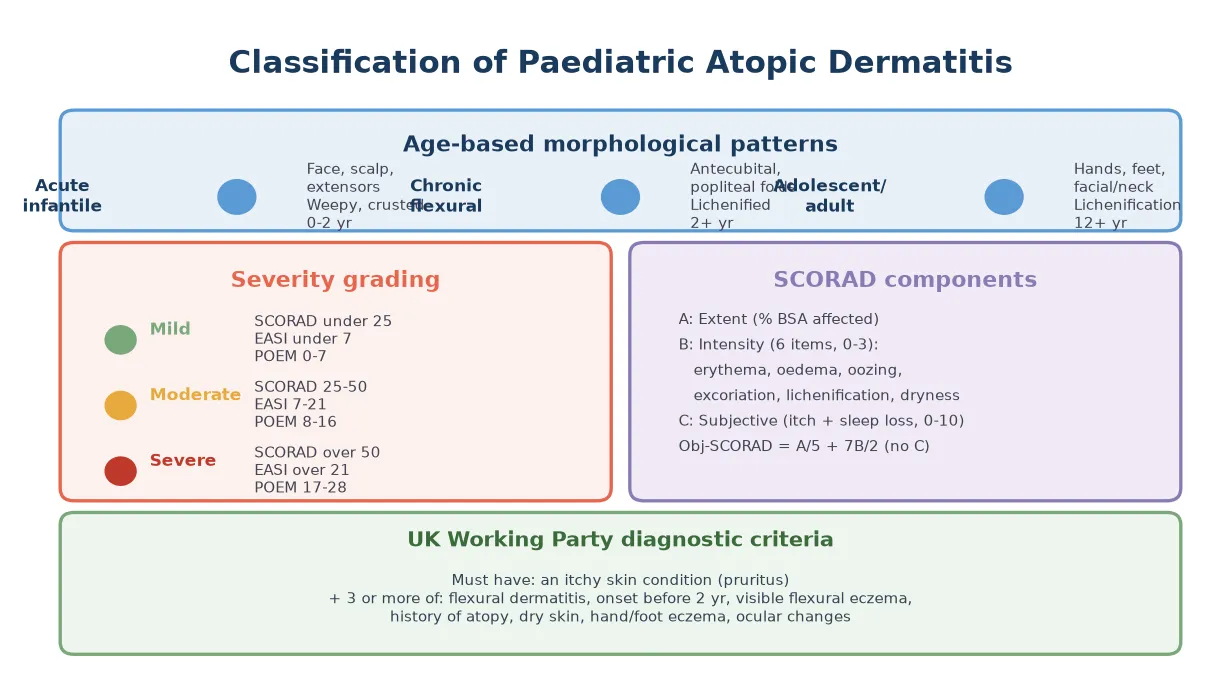
Severity is graded with validated instruments such as SCORAD (which combines extent, six clinical signs and subjective itch-and-sleep scores), EASI (a physician-assessed area-and-severity index), and POEM (a patient-reported seven-item score), with a parent-completed CDLQI capturing quality-of-life impact. A 2015 study confirmed that the objective SCORAD and the three-item severity score correlate well, and that parent-completed PO-SCORAD tracks physician assessment, supporting their combined use in clinic. [11]
Epidemiology & Risk Factors
Atopic dermatitis affects up to 20 per cent of children in high-income countries, with onset before the age of one year in roughly half of cases and before five years in the vast majority, making it both the most common skin disease and the most common atopic presentation of childhood. Prevalence has risen over recent decades, particularly in urban and high-income settings, tracking with the broader rise in allergic disease. [1]
The strongest risk factor is a family history of atopy: a child with one atopic parent has roughly a doubled risk, and a child with two atopic parents has a risk above 60 per cent. Loss-of-function variants in the filaggrin gene are the best-characterised genetic risk factor, identified by Palmer and colleagues in 2006 as a major predisposing factor, and they amplify both the severity of dermatitis and the likelihood of progression along the atopic march. [3]
Environmental factors act on the genetic substrate: urban living, reduced microbial exposure in early life, pollution, second-hand smoke, hard water, and a dry or cold climate all increase risk, while farm living, vaginal delivery, breastfeeding and early diverse microbial exposure appear protective — the hygiene-hypothesis framework that unites the rise of atopic dermatitis with the rise of allergic disease broadly. [1]
Pathophysiology
Atopic dermatitis arises from a primary defect in the epidermal barrier that allows environmental antigens, irritants and microbes to penetrate the skin and ignite a Th2-dominant inflammatory response. The two pillars — barrier failure and immune dysregulation — reinforce each other in a vicious cycle that sustains chronic, relapsing disease and opens the door to the atopic march. [13]
The barrier defect centres on filaggrin, a structural protein whose breakdown products form the natural moisturising factor that keeps the stratum corneum hydrated and acidic. Loss-of-function mutations in filaggrin, first linked to atopic dermatitis in 2006, reduce ceramide synthesis, raise transepidermal water loss, and produce a dry, cracked skin surface that admits antigens and supports Staphylococcus aureus colonisation. [3]
Once antigens breach the barrier, Langerhans and dendritic cells take them up and present them to naïve T cells, which polarise toward a Th2 phenotype secreting interleukin-4, interleukin-13 and interleukin-31. These cytokines drive B-cell immunoglobulin class-switching to allergen-specific IgE, recruit eosinophils, suppress antimicrobial peptide production (worsening infection risk), and — through interleukin-31 — directly stimulate itch, completing the itch-scratch cycle that further damages the barrier. [13]
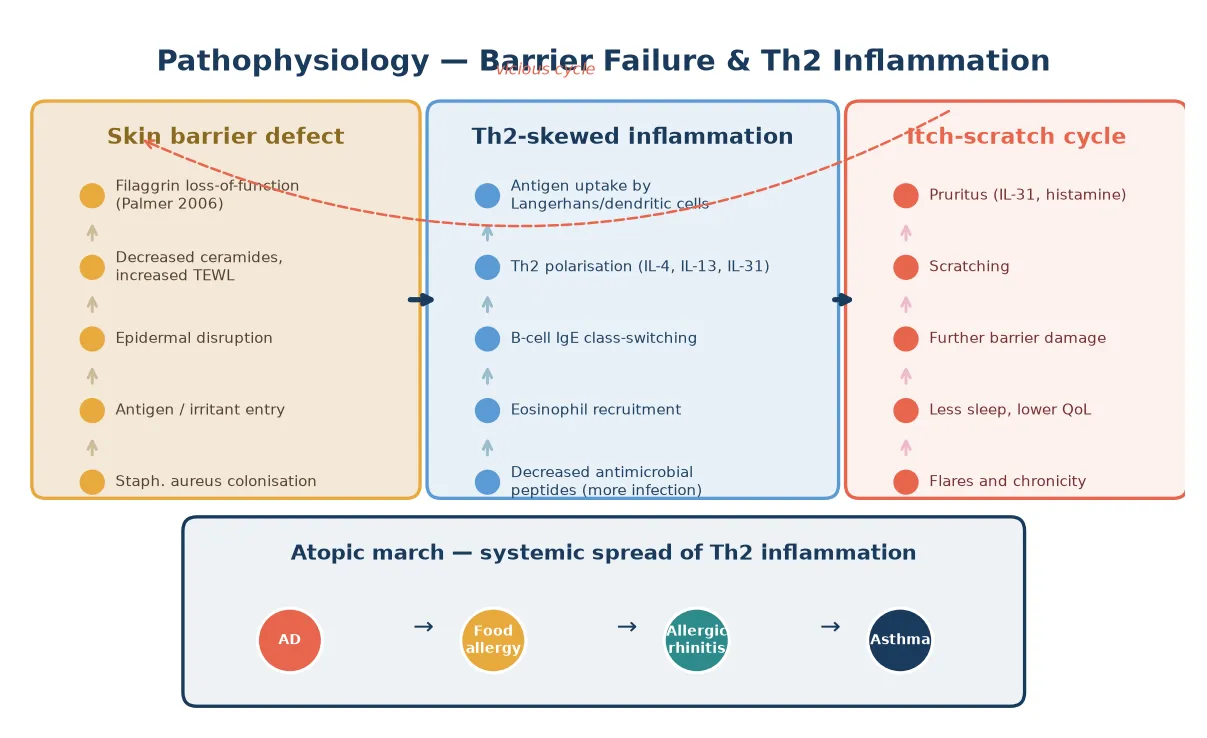
The itch-scratch cycle is the engine of chronicity. Pruritus, amplified by interleukin-31 and histamine, drives scratching that physically disrupts the barrier, triggers further inflammation and recruits more Th2 cells, so that each flare lowers the threshold for the next. Sleep is fragmented, quality of life falls, and the systemic Th2 spread that defines the atopic march gains momentum. [2]
BARRIER — why atopic dermatitis persists
Clinical Presentation
The cardinal symptom is itch, and in an infant this manifests as irritability, sleep disruption and rubbing rather than the verbal report of pruritus that an older child can give. The rash itself is eczematous — erythematous, dry, poorly demarcated patches and plaques that become weepy and crusted in acute flares and lichenified and fissured in chronic disease, distributed in the age-typical patterns described above. [1]
Examination reveals dry skin (xerosis) generally, with active eczema in the characteristic sites: the cheeks, scalp and extensor limbs in infants, and the antecubital and popliteal folds, wrists, ankles and neck in older children. Secondary changes include excoriation, impetiginisation with golden crusting from Staphylococcus aureus, and, in chronic disease, lichenification and pigmentary change. Associated features include infraorbital folds (Dennie-Morgan lines), keratosis pilaris, ichthyosis and palmar hyperlinearity, the so-called atopic stigmata. [10]
The impact extends well beyond the skin. Children with moderate-to-severe atopic dermatitis have fragmented sleep, impaired growth, reduced school attendance and concentration, behavioural disturbance and substantially reduced quality of life, and their parents carry significant caregiving burden, sleep loss and lost productivity. A 2013 review of the Children's Dermatology Life Quality Index confirmed that dermatitis ranks among the most quality-of-life-impairing chronic diseases of childhood. [9]
Differential Diagnosis
The first task is to separate atopic dermatitis from the other common eczematous and inflammatory rashes of childhood. Seborrhoeic dermatitis of infancy produces greasy yellow scales on the scalp (cradle cap), eyebrows and folds with relative sparing of the cheeks, and is less itchy; irritant and allergic contact dermatitis have a distribution matching the contactant; and juvenile plantar dermatosis produces glazed fissured soles in school-age children. [1]
Infective and infestive mimics must not be missed: scabies causes intense nocturnal itch with burrows in the finger-web spaces, axillae and genitalia and is highly contagious; tinea produces annular, scaly, slowly extending plaques with central clearing; and impetigo produces honey-coloured crusted erosions that may complicate or mimic eczema. A child whose "eczema" is unilateral, sharply demarcated or unresponsive to therapy should prompt consideration of these. [1]
The rarer but serious differentials matter when eczema is severe, early-onset, atypical or refractory. Immunodeficiency syndromes — severe combined immunodeficiency, Wiskott-Aldrich syndrome, hyper-IgE (Job) syndrome, Netherton syndrome and IPEX — can present with an eczematous eruption in early infancy, and failure to thrive, recurrent infection, thrombocytopenia or an intractable rash should trigger immunological referral. Cutaneous T-cell lymphoma is vanishingly rare in children but enters the differential of an atypical, persistent, treatment-resistant plaque. [10]
Clinical & Bedside Assessment
Assessment begins with a focused history that establishes the onset, distribution, itch severity, sleep disturbance, trigger factors, response to treatment and the impact on the child and family, alongside a personal and family atopic history. A 2014 cohort confirmed that structured history and the use of a written flare action plan improve control, and that documenting trigger factors — heat, sweat, soaps, woollen clothing, specific foods and aeroallergens — directs practical advice. [4]
Examination documents the distribution and morphology of the eczema, the presence of xerosis and atopic stigmata, and any signs of secondary infection or complication. The distribution is mapped to estimate body-surface-area involvement for severity scoring, and particular attention is paid to the flexural folds, the face and periorbital skin, the hands and the nappy area, because these sites drive both severity and quality-of-life scores. [10]
Severity is quantified with a validated instrument — SCORAD, EASI or POEM — at baseline and at each review, and quality of life is captured with the CDLQI or infant equivalent. This objective tracking is what allows rational step-up and step-down of therapy and distinguishes stable disease from a treatable flare, and it anchors the conversation with families about whether the current regimen is working. [9]
Investigations
The diagnosis of atopic dermatitis is clinical, and laboratory testing confirms neither the diagnosis nor the activity of disease. Total serum IgE and allergen-specific IgE or skin-prick testing may demonstrate sensitisation but are frequently positive in children without active disease and correlate poorly with severity, so they should not be ordered routinely to "confirm eczema". [1]
Allergy testing has a selective role. It is worth pursuing when there is a convincing history of a specific food or aeroallergen trigger, when a child has coexisting immediate-type food allergy or anaphylaxis, or when eczema is severe and refractory and a specific allergen is suspected as an aggravating factor. Serum-specific IgE or skin-prick testing can identify sensitisation, but only an oral food challenge confirms clinical allergy, and over-interpreting positive tests leads to unnecessary and harmful elimination diets. [8]
Skin biopsy is reserved for atypical, refractory or suspected-malignant disease, and emerging non-invasive tools such as electrical impedance spectroscopy can detect early subclinical barrier dysfunction, as demonstrated in a 2024 study of childhood atopic dermatitis, though these remain research-grade rather than routine clinical tools. Swabs of weeping or crusted eczema identify Staphylococcus aureus or herpes simplex during suspected secondary infection and guide antimicrobial therapy. [14]
ECZEMA — when to investigate
Management — Resuscitation
Atopic dermatitis is rarely a resuscitation problem, but two acute scenarios demand immediate action. The first is eczema herpeticum — disseminated herpes simplex infection presenting as rapidly worsening, painful, clustered, punched-out vesicles or erosions with fever and malaise — which requires same-day systemic aciclovir and admission because secondary bacterial sepsis, dehydration and dissemination can be fatal. [1]
The second is widespread, weeping, secondarily infected eczema with systemic upset, where Staphylococcal or Streptococcal infection drives a toxic, febrile child. The priority is systemic antibiotic therapy directed at the likely organism (a flucloxacillin-based regimen), antipyresis, fluid management if dehydration is present, and escalation of topical anti-inflammatory therapy once the infection is controlled. [10]
Neither scenario should be managed with topical therapy alone; both require systemic treatment and a low threshold for admission, particularly in infants and in children who are systemically unwell. The opportunity is taken to review the maintenance regimen, identify the trigger for the flare, and arrange structured follow-up to prevent recurrence. [1]
Management — Definitive & Stepwise
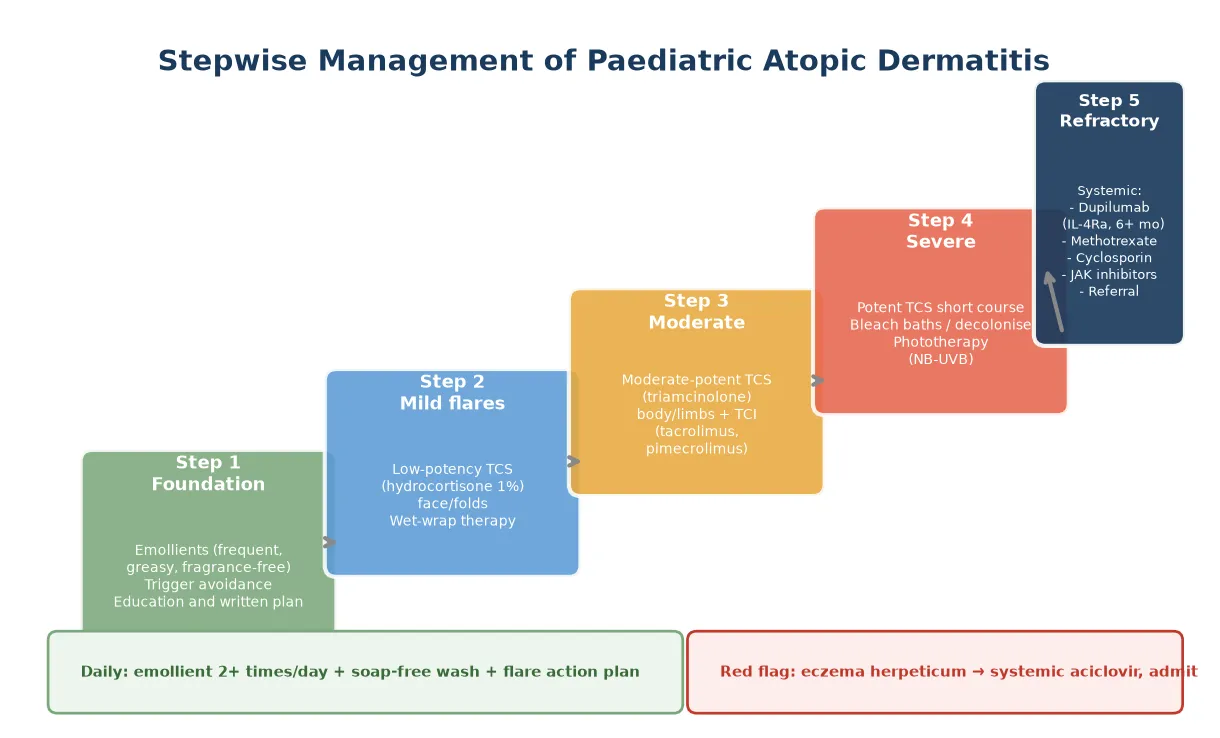
Definitive care follows a stepwise ladder that begins with foundation therapy for every child and escalates according to severity and response. The foundation is emollient therapy applied generously and frequently (at least twice daily), a soap-free wash, trigger avoidance, and a written eczema action plan that empowers families to step up treatment at the first sign of a flare. The American Academy of Dermatology guidelines reaffirm emollients as the indispensable base of every regimen. [6]
Stepwise management ladder
Step 1 foundation: emollient (greasy, fragrance-free) at least twice daily; soap-free wash; trigger avoidance; written action plan
Step 2 mild flares: low-potency topical corticosteroid (hydrocortisone 1%) to face and folds for short courses
Step 3 moderate: moderate-potency corticosteroid (triamcinolone) to body and limbs; topical calcineurin inhibitor (tacrolimus, pimecrolimus) to face and folds
Step 4 severe: potent corticosteroid short course; wet-wrap therapy; bleach baths and decolonisation; consider phototherapy (NB-UVB)
Step 5 refractory: systemic therapy (dupilumab, methotrexate, cyclosporin) under specialist supervision
Reassess: severity score (SCORAD/EASI/POEM) every 2-4 weeks during escalation; review adherence and technique
Topical corticosteroids are the mainstay of acute flare management and are selected by potency and site: a low-potency agent such as hydrocortisone 1% for the face, eyelids and folds; a moderate-potency agent such as triamcinolone for the trunk and limbs; and a potent agent such as mometasone for short courses on thick, lichenified limb skin. The fear of steroid side-effects ("steroid phobia") is the commonest cause of under-treatment, and the evidence — including the AAD guidelines — supports their safety when used at appropriate potency, for defined courses, with fingertip-unit dosing and clear instructions. [6]
Topical calcineurin inhibitors — tacrolimus ointment and pimecrolimus cream — are non-steroid anti-inflammatory agents particularly valuable for the face, eyelids and flexures where prolonged corticosteroid use risks atrophy and skin lightening. They do not cause skin thinning and are licensed for intermittent use in children from two years of age, and a common early burning sensation can be reduced by refrigerating the tube or applying to damp skin. [10]
For severe or refractory disease, systemic therapy is indicated and should be initiated under specialist supervision. Dupilumab, a monoclonal antibody blocking the interleukin-4 receptor alpha subunit and thereby both interleukin-4 and interleukin-13 signalling, is licensed from six months of age and has transformed the management of severe paediatric atopic dermatitis, with a 2023 post-hoc analysis of randomised trials confirming efficacy and safety even in the erythrodermic phenotype. Methotrexate, cyclosporin and the newer JAK inhibitors are alternatives or temporising agents. [12]
Adjuvant measures include wet-wrap therapy for severe flares, dilute bleach baths (sodium hypochlorite) to reduce staphylococcal colonisation in recurrently infected eczema, and narrowband UVB phototherapy in older children with widespread disease. The 2015 ETFAD/EADV position paper integrates these into a comprehensive stepwise framework for both adult and paediatric patients. [10]
Specific Subtypes & Scenarios
The atopic march is the central unifying scenario. A 2019 review characterises it not as a single linear pathway but as multiple trajectories and pathways, in which early-onset, severe atopic dermatitis with early sensitisation predicts the most aggressive progression to food allergy, allergic rhinitis and asthma. Recognising this risk frames aggressive early skin control not merely as symptom relief but as a strategy to interrupt the march. [2]
Food allergy coexists with atopic dermatitis in a complex bidirectional relationship. Severe early-onset eczema is a major risk factor for developing IgE-mediated food allergy, because allergens entering through broken skin sensitise the immune system, while foods themselves are uncommon direct triggers of eczema flares. The LEAP trial established that early introduction of peanut in high-risk infants prevents peanut allergy, overturning the earlier practice of delayed introduction and underscoring that dietary restriction is rarely an eczema treatment. [8]
Secondary infection is a recurring scenario. Staphylococcus aureus colonises virtually all eczematous skin and drives flares through superantigen-mediated inflammation, while clinical infection with weeping, crusting and honey-coloured lesions requires topical or systemic antibiotic therapy combined with antiseptic washes and decolonisation. Eczema herpeticum, described above, is the infective emergency. [10]
Complications & Pitfalls
The cutaneous complications are infection and treatment side-effects. Staphylococcal and streptococcal infection drive flares and, in severe cases, cellulitis or sepsis; eczema herpeticum is a medical emergency; and molluscum contagiosum and viral warts are more common in atopic skin. The treatment side-effects are those of corticosteroids — skin atrophy, telangiectasia and striae with overuse of potent agents — and these are preventable by matching potency to site and using defined courses. [1]
The systemic complication is the atopic march itself. A 2022 review tracing the path from skin barrier dysfunction to systemic impact frames atopic dermatitis as a systemic disease rather than a purely cutaneous one, with the Th2 inflammation that begins in the skin spreading to the gut, the airways and the eyes, producing food allergy, asthma, rhinitis and conjunctivitis in a substantial proportion of children. The comorbidity burden is documented in the AAD comorbidity guidelines. [7]
Complications of atopic dermatitis
The major pitfall is steroid phobia — the unfounded fear of topical corticosteroids that leads parents to under-treat, undertreatment that in turn perpetuates flares, the itch-scratch cycle and the march. Equally common is the over-investigation pitfall: ordering panels of food-specific IgE tests in a child with eczema and then eliminating foods on the basis of sensitisation rather than proven allergy, producing nutritional deficiency without improving the eczema. Both pitfalls are addressed by education and a clear written plan. [6]
Prognosis & Disposition
The prognosis is favourable for most children: roughly half of childhood cases resolve by adolescence, and many more improve substantially, though a subset — particularly those with filaggrin mutations, severe early-onset disease and early sensitisation — follow a persistent course into adult life. The risk of progressing along the atopic march is highest in children with severe, early-onset dermatitis, in whom up to half may develop asthma. [2]
Disposition is overwhelmingly outpatient, with regular review during escalation and then maintenance review every six to twelve months for stable disease. Admission is reserved for eczema herpeticum, severe secondary infection with systemic upset, and occasionally for intensive wet-wrap therapy in a child whose disease cannot be managed at home. Referral to paediatric dermatology is appropriate for severe or refractory disease, when systemic therapy is being considered, and when the diagnosis is uncertain. [1]
The long-term outlook is shaped by whether the atopic march is interrupted. Aggressive early control of the skin, identification and management of coexisting food allergy, and co-management of emerging asthma and rhinitis all modify the trajectory, and the disease-modifying potential of early intervention — including early allergen introduction and proactive emollient use — is an active and evolving area of research. [8]
Special Populations
Indigenous children, particularly in remote Australian and New Zealand settings, may experience severe atopic dermatitis compounded by high rates of streptococcal and staphylococcal skin infection, scabies and the downstream risks of acute rheumatic fever and post-streptococcal glomerulonephritis. Community-based, culturally safe Healthy Skin programmes that integrate eczema management with the treatment of infectious skin disease address this burden and are the model for care in these settings. [7]
Children with neurodevelopmental disability or autism may be unable to articulate itch and may present with behavioural disturbance, sleep disruption, self-injury or agitation driven by uncontrolled dermatitis; a high index of suspicion, a structured skin examination and a simplified, sensory-tolerable regimen are needed. Adherence to complex topical regimens is challenging and benefits from caregiver training and a stepwise, low-sensory application approach. [9]
Refugee, migrant and asylum-seeking children may have had limited access to dermatological care and may present with advanced, untreated disease complicated by chronic infection, sleep disturbance and school disengagement. Cultural and language factors shape the consultation, the emollient must be acceptable and affordable, and a focus on practical, sustainable self-management — reinforced by interpreters and written materials in the family's language — underpins success. [9]
Evidence, Guidelines & Regional Differences
The American Academy of Dermatology guidelines series is the current comprehensive standard, with the topical-therapy guideline establishing the stepwise ladder of emollients, corticosteroids and calcineurin inhibitors and the comorbidity guideline cataloguing the associations — food allergy, asthma, rhinitis, cardiovascular and mental-health comorbidity — that frame atopic dermatitis as a systemic disease. These guidelines anchor evidence-based practice across paediatric and adult care. [6]
The European ETFAD/EADV 2015 position paper integrates diagnosis and treatment for both adult and paediatric patients and is the key European reference, complementing the AAD guidelines with a practical stepwise algorithm. The 2005 Williams review in the New England Journal of Medicine remains the single most cited clinical overview and a readable entry point to the evidence base. [10]
The most contested question is whether early emollient application from birth prevents atopic dermatitis. A 2014 Japanese study and the BEEP pilot suggested benefit, but the large BEEP randomised trial reported in 2024 found that daily emollient from birth did not prevent eczema in high-risk infants, tempering enthusiasm and redirecting prevention efforts toward early allergen introduction and aggressive early treatment rather than barrier supplementation alone. [5]
Regional differences centre on climate, dominant allergens and access to care. Tropical and subtropical regions contend with heat- and sweat-triggered flares and high rates of secondary infection; temperate regions contend with winter dryness; and remote and Indigenous settings contend with the infectious complications of eczema and limited access to specialist care. The evidence base is international, but the practical implementation must be adapted to local resources and the family's circumstances. [1]
Exam Pearls
For written and viva exams, atopic dermatitis is a high-yield topic because it is extremely common, has a clean barrier-and-immune mechanism, and tests whether you can apply diagnostic criteria, justify a stepwise topical-therapy ladder, and articulate the atopic march. Be ready to state the UK Working Party criteria — an itchy skin condition plus at least three of five supporting features — and to describe the age-typical distribution from infantile extensor disease to childhood flexural disease. [1]
Examiners expect you to name filaggrin as the key barrier protein, to describe the Th2-skewed inflammation with interleukin-4, interleukin-13 and interleukin-31 driving IgE and itch, and to explain the itch-scratch cycle. State the management ladder clearly: emollient foundation, then topical corticosteroids matched by potency to site, then topical calcineurin inhibitors for face and folds, then systemic therapy with dupilumab for refractory disease. Reassure on corticosteroid safety and address steroid phobia directly. [6]
The atopic march is the high-yield concept that ties dermatitis to the rest of the atopic diathesis. Name the sequence — atopic dermatitis and food allergy in infancy, allergic rhinitis and asthma in childhood — and explain that early severe eczema predicts later asthma, that foods sensitise through broken skin, and that the LEAP trial showed early peanut introduction prevents allergy. Finally, name eczema herpeticum as the cutaneous emergency requiring systemic aciclovir. [2]
References
- [1]Williams HC Clinical practice. Atopic dermatitis. N Engl J Med, 2005.PMID 15930422
- [2]Paller AS, Spergel JM, Mina-Osorio P The atopic march and atopic multimorbidity: Many trajectories, many pathways. J Allergy Clin Immunol, 2019.PMID 30458183
- [3]Palmer CN, Irvine AD, Terron-Kwiatkowski A Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat Genet, 2006.PMID 16550169
- [4]Simpson EL, Chalmers JR, Hanifin JM Emollient enhancement of the skin barrier from birth offers effective atopic dermatitis prevention. J Allergy Clin Immunol, 2014.PMID 25282563
- [5]Bradshaw LE, Wyatt LA, Brown SJ Emollient application from birth to prevent eczema in high-risk children: the BEEP RCT. Health Technol Assess, 2024.PMID 39021147
- [6]Sidbury R, Alikhan A, Bercovitch L Executive summary: American Academy of Dermatology guidelines of care for the management of atopic dermatitis in adults with topical therapies. J Am Acad Dermatol, 2023.PMID 36623556
- [7]Davis DMR, Drucker AM, Alikhan A American Academy of Dermatology Guidelines: Awareness of comorbidities associated with atopic dermatitis in adults. J Am Acad Dermatol, 2022.PMID 35085682
- [8]Du Toit G, Roberts G, Sayre PH Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med, 2015.PMID 25705822
- [9]Salek MS, Jung S, Brincat-Ruffini LA Clinical experience and psychometric properties of the Children's Dermatology Life Quality Index (CDLQI), 1995-2012. Br J Dermatol, 2013.PMID 23679682
- [10]Wollenberg A, Oranje A, Deleuran M ETFAD/EADV Eczema task force 2015 position paper on diagnosis and treatment of atopic dermatitis in adult and paediatric patients. J Eur Acad Dermatol Venereol, 2016.PMID 27004560
- [11]van Oosterhout M, Janmohamed SR, Spierings M Correlation between Objective SCORAD and Three-Item Severity Score used by physicians and Objective PO-SCORAD used by parents/patients in children with atopic dermatitis. Dermatology, 2015.PMID 25660989
- [12]Paller AS, Silverberg JI, Cork MJ Efficacy and Safety of Dupilumab in Patients With Erythrodermic Atopic Dermatitis: A Post Hoc Analysis of 6 Randomized Clinical Trials. JAMA Dermatol, 2023.PMID 36723913
- [13]Maintz L, Bieber T, Simpson HD From Skin Barrier Dysfunction to Systemic Impact of Atopic Dermatitis: Implications for a Precision Approach in Dermocosmetics and Medicine. J Pers Med, 2022.PMID 35743678
- [14]Sasaki M, Sundberg M, Frei R Electrical impedance spectroscopy detects skin barrier dysfunction in childhood atopic dermatitis. Allergy, 2024.PMID 37753955