Paeds · allergy-and-immunology
Cow's-milk protein allergy
Also known as Cow's milk allergy · CMPA · Cow's-milk protein hypersensitivity · Bovine protein allergy
A fellowship approach to cow's-milk protein allergy (CMPA): separate the immediate IgE-mediated phenotype from the delayed non-IgE-mediated phenotype, clear the anaphylaxis threat gate first, confirm the diagnosis clinically by elimination and planned rechallenge rather than over-relying on allergy tests, and run the stepwise elimination ladder — maternal elimination for the breastfed infant, extensively hydrolysed formula first-line for the formula-fed, amino-acid formula for severe or refractory disease — while building tolerance over time.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A four-month-old arrives with blood and mucus in the stools but looks well and is growing. Beside her is a six-month-old who turned red, vomited, and became wheezy ten minutes after a first bottle of formula. Both have cow's-milk protein allergy, but they are different diseases with different risks, different diagnostic logic, and different pathways. Holding both in the same frame — the calm delayed gut phenotype alongside the immediate anaphylaxis phenotype — is the whole skill of this topic. [1] [3]
M.I.L.K. A.L.L.E.R.G.Y.
Overview & Definition
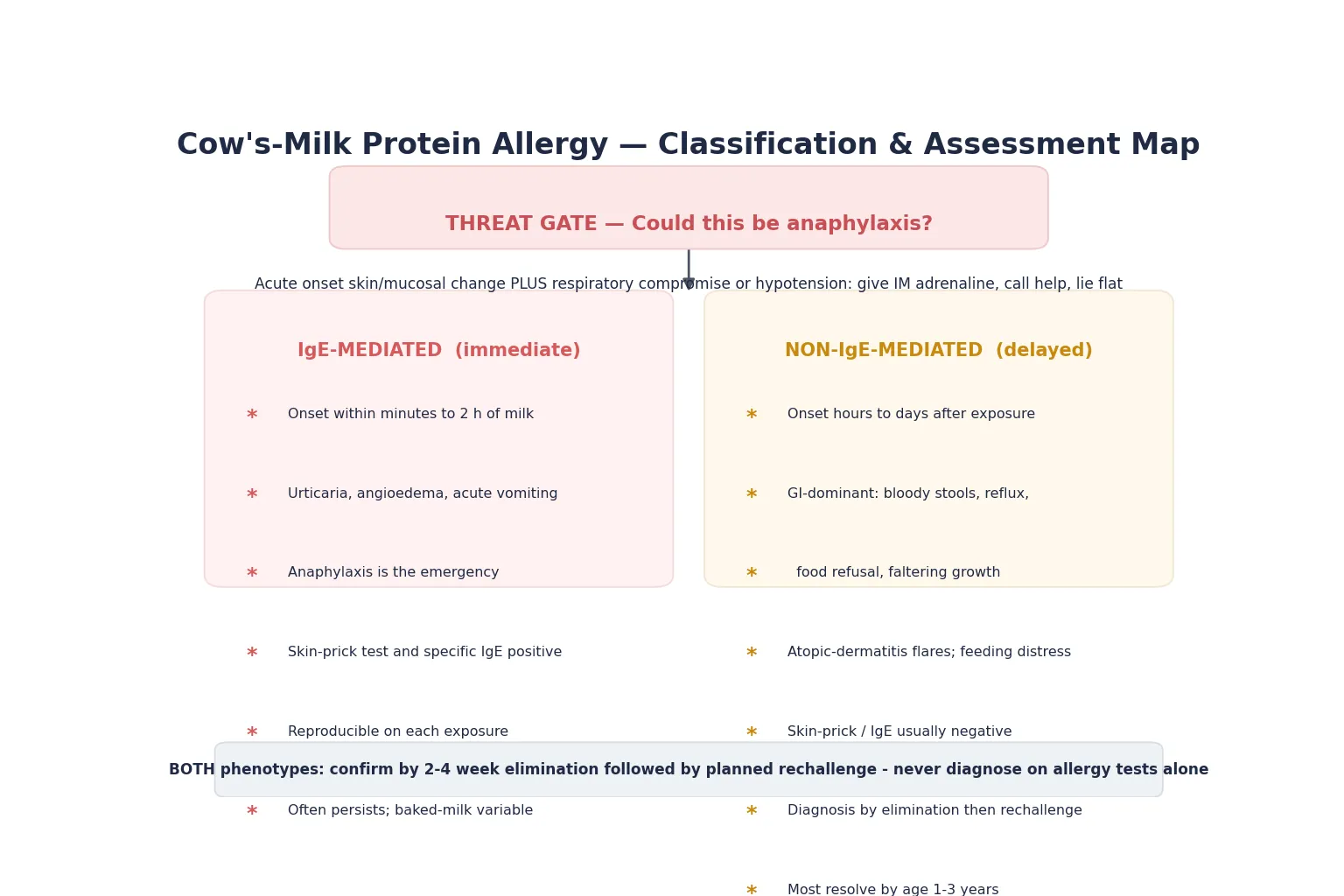
Cow's-milk protein allergy is an adverse immunological reaction to one or more of the proteins in cow's milk — most often casein and the whey proteins beta-lactoglobulin and alpha-lactalbumin. It is the commonest food allergy of infancy. The key clinical division is between IgE-mediated disease, driven by specific immunoglobulin E against milk proteins and manifesting within minutes to two hours of exposure, and non-IgE-mediated disease, driven by cellular and mixed immune mechanisms and manifesting hours to days after exposure. [1] [3]
Do not confuse CMPA with lactose intolerance, which is an enzyme deficiency (lactase) producing bloating and diarrhoea without any immune mechanism. The two are commonly conflated by families and occasionally by clinicians, and the distinction matters because lactose intolerance is not dangerous and does not need elimination of all cow's-milk protein. The vast majority of infants with CMPA tolerate lactose without issue. [2]
The decisive clinical question at first contact is never "is the skin-prick positive?" but "which phenotype is this, and could this become anaphylaxis?" A positive test in an asymptomatic child is sensitisation, not allergy. A child who reacts on exposure is allergic regardless of the test number. The ESPGHAN practical guideline makes this point explicitly: CMPA is a clinical diagnosis confirmed by elimination and rechallenge, with tests used to phenotype rather than to screen. [1]
Classification
Sort cow's-milk protein allergy by immune mechanism, because that single split predicts timing, risk, testing, and outcome. [1] [2]
IgE-mediated CMPA is immediate. Symptoms begin within minutes to two hours of ingesting cow's-milk protein. The phenotype spans cutaneous reactions (urticaria, angioedema, pruritus), gastrointestinal reactions (acute vomiting), and the life-threatening constellation of anaphylaxis — skin change plus respiratory compromise or hypotension. Skin-prick testing and serum specific IgE are positive and useful here. This phenotype carries the ongoing risk of anaphylaxis on every re-exposure. [3] [7]
Non-IgE-mediated CMPA is delayed. Symptoms emerge hours to several days after exposure and are dominated by the gastrointestinal tract and skin. The patterns include cow's-milk protein-induced proctocolitis (blood and mucus in stools of an otherwise well infant), food-protein-induced enteropathy (malabsorption, diarrhoea, faltering growth), and food-protein-induced enterocolitis syndrome (FPIES — delayed, repetitive vomiting leading to lethargy and dehydration). Atopic dermatitis that flares with exposure also sits here. Tests are typically negative, and the diagnosis rests on elimination and rechallenge. [1] [2]
A subset of infants have mixed or eosinophilic disease, including eosinophilic oesophagitis with dysphagia, reflux unresponsive to therapy, and food impaction. These overlap with both phenotypes and often need endoscopy and specialist input. [1]
Epidemiology & Risk Factors
Cow's-milk protein allergy is the commonest food allergy of infancy. European data place the prevalence of challenge-confirmed cow's-milk allergy in the range of around one to two per cent of infants, with self-reported rates considerably higher because many non-allergic conditions are mislabelled as CMPA. Nwaru and colleagues, in a European systematic review and meta-analysis, found that perceived prevalence consistently exceeded confirmed prevalence across food allergens — a reminder that over-diagnosis is as common a problem as under-diagnosis. [6]
The burden is real. Liu and colleagues, using data from the National Health and Nutrition Examination Survey, showed food allergy affects a meaningful proportion of children and associates with asthma and other atopic disease. Cow's-milk is the leading trigger in the first year of life, ahead of egg and peanut. [5]
Risk factors are the atopic cluster. A personal history of atopic dermatitis, a family history of atopy, and early disruption of the skin or gut barrier raise the probability of sensitisation. Severity of atopic dermatitis in particular correlates with the risk of developing food allergy, supporting the dual-allergen-exposure hypothesis that sensitisation occurs through broken skin before tolerance develops through the gut. [8]
The natural history favours resolution. Skripak and colleagues followed a cohort of children with IgE-mediated cow's-milk allergy and found that a substantial proportion achieved tolerance over time, though those with higher initial specific IgE and larger skin-prick wheals resolved more slowly. Non-IgE-mediated disease resolves faster still — most infants with proctocolitis tolerate cow's milk by their first birthday. [4]
Pathophysiology
The two phenotypes arise from different arms of the immune system, and the distinction explains the timing, the testing, and the prognosis. [3]
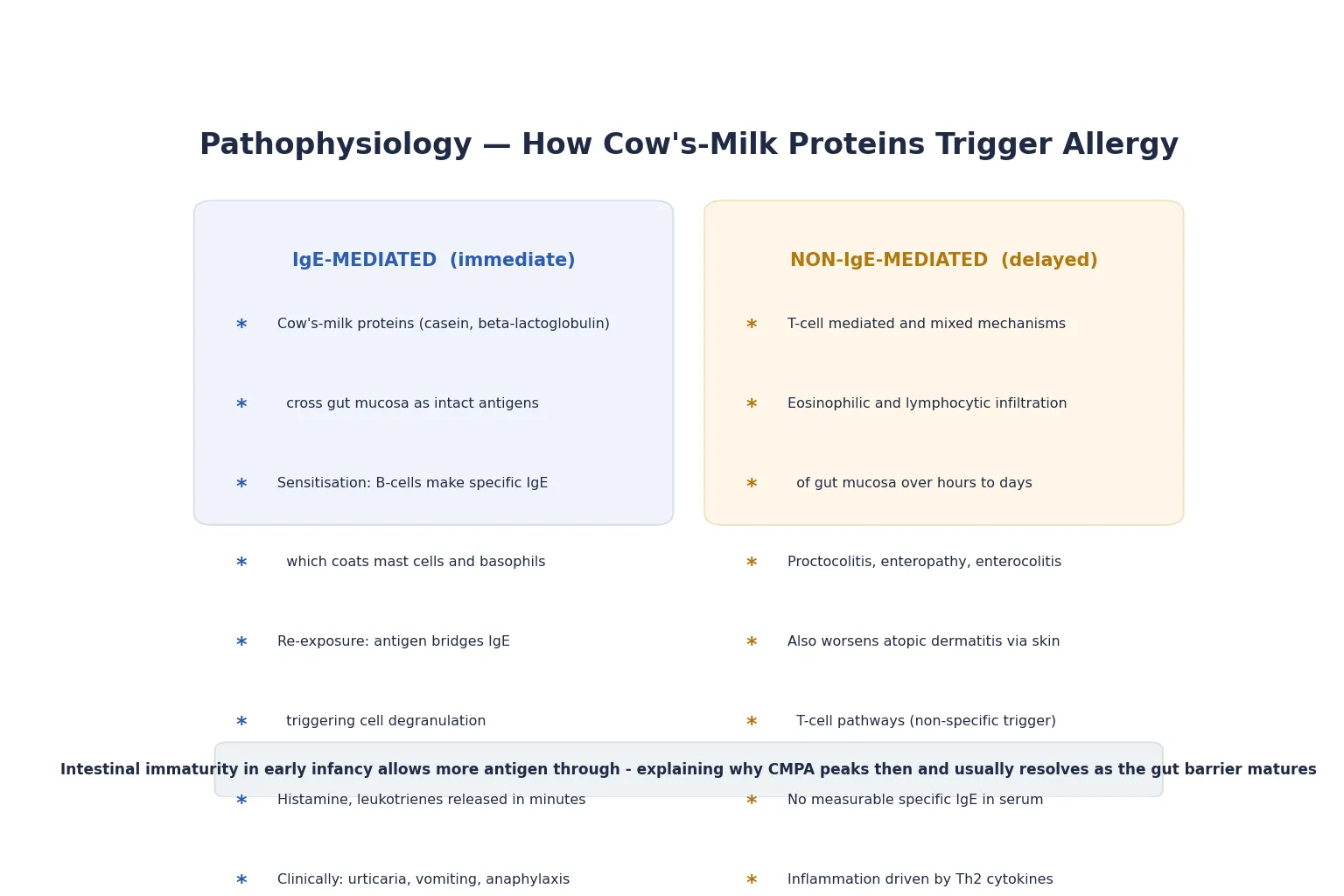
In IgE-mediated CMPA, intact cow's-milk proteins cross the gut mucosa and, in a sensitised child, are presented to T- and B-lymphocytes that drive production of specific immunoglobulin E. This IgE coats mast cells and basophils throughout the body. On re-exposure, the milk protein bridges adjacent IgE molecules, triggering immediate cell degranulation and release of histamine, leukotrienes, and prostaglandins. The clinical result appears within minutes: urticaria, angioedema, vomiting, bronchospasm, and in the most severe form, anaphylaxis with vasodilation and shock. [7]
In non-IgE-mediated CMPA, the mechanism is cellular rather than antibody-driven. T-lymphocyte and eosinophilic infiltration of the gastrointestinal mucosa produces inflammation over hours to days, seen histologically as eosinophilic proctocolitis, enteropathy, or — in FPIES — a severe delayed systemic inflammatory response. There is no measurable specific IgE in serum, which is why tests are negative here. The same non-IgE pathways can worsen atopic dermatitis by acting as a non-specific trigger on inflamed skin rather than through a classical allergic mechanism. [1]
The reason CMPA peaks in infancy and usually resolves is intestinal immaturity. The infant gut barrier is more permeable to intact antigens than the mature gut, allowing more cow's-milk protein through before oral tolerance is established. As the gut and the immune system mature, most children develop tolerance and the allergy resolves. This developmental arc is why the diagnosis is overwhelmingly an infant disease and why the prognosis is generally good. [12]
Clinical Presentation
IgE-mediated reactions declare themselves quickly. Within minutes to two hours of ingesting cow's milk — by bottle, by maternal milk in a breastfed infant, or by a hidden ingredient — the child develops urticaria, angioedema (periorbital, lip, or facial swelling), pruritus, and acute vomiting. The severe end of the spectrum is anaphylaxis: rapid-onset skin change accompanied by respiratory compromise (stridor, wheeze, respiratory distress) or cardiovascular compromise (pallor, floppiness, hypotension). Any of these after milk exposure is an emergency. [3] [7]
Non-IgE-mediated CMPA presents more subtly and later. The parents of a well-looking breastfed infant report blood and mucus in the stools — classic cow's-milk protein-induced proctocolitis, the most common pattern. Others describe persistent reflux that resists standard therapy, distress or arching on feeding, persistent diarrhoea, eczema that flares and fails to settle, or faltering growth when intake is compromised. The temporal link to cow's milk is often unclear because symptoms accumulate over days, which is why a structured elimination trial is diagnostic. [1] [2]
Food-protein-induced enterocolitis syndrome (FPIES) is the dramatic delayed pattern and is easily missed. One to four hours after ingesting the trigger — cow's milk is a common one — the infant develops repetitive, projectile vomiting that progresses to lethargy, pallor, and dehydration. There is no urticaria, no IgE, and the picture is often mistaken for sepsis or gastroenteritis. FPIES demands intravenous fluids and a careful, specialist-led approach to rechallenge because reactions can be severe. [1]
Atopic dermatitis and CMPA are tightly linked. Severe or early-onset eczema that fails to respond to first-line topical therapy in a formula-fed infant should prompt consideration of non-IgE-mediated CMPA as a contributing trigger, though eczema is multifactorial and cow's milk is not the cause of all eczema. [8]
Differential Diagnosis
Hold the benign and the dangerous together, because several non-allergic conditions mimic CMPA and several dangerous ones sit beside it. [1] [12]
Must-not-miss: anaphylaxis from any cause, sepsis presenting with vomiting and lethargy (especially in the FPIES mimic), intussusception with bloody stools and colic, eosinophilic oesophagitis with dysphagia and reflux, and surgical causes of gastrointestinal bleeding such as Meckel's diverticulum or malrotation with volvulus. These stay open until the assessment clears them. [1]
Non-allergic mimics of non-IgE CMPA: lactose intolerance (enzyme deficiency, no immune mechanism, bloating and watery diarrhoea), infectious gastroenteritis, anal fissure as the source of bright bleeding, swallowed maternal blood from cracked nipples in a breastfed neonate, and functional reflux or colic that are normal infant behaviour. These account for much of the over-diagnosis when clinicians label any unsettled formula-fed infant as CMPA. [2]
Other food-allergic conditions in the differential: eosinophilic gastrointestinal disease, coeliac disease in older infants (proximity of gluten introduction), and other food-protein-induced syndromes. The phenotype of the reaction and the temporal link to a specific food separate these. [1]
CMPA vs its commonest mimic
Clinical & Bedside Assessment
1. Clear the threat gate first. Any child with acute skin change plus respiratory compromise, pallor, floppiness, or hypotension after milk exposure is having anaphylaxis until proven otherwise. Lie the child flat, give IM adrenaline into the anterolateral thigh, call for help, and start the emergency pathway. Do not wait for tests. [3] [7]
2. History that phenotypes. Establish the timing of symptoms relative to milk exposure: minutes to two hours points to IgE-mediated; hours to days points to non-IgE-mediated. Ask about the exact trigger (formula, maternal dairy in a breastfed infant, hidden milk in solids), the reproducibility of the reaction, and any prior reactions. Capture the atopic background — eczema, asthma, allergic rhinitis, family atopy — and the feeding history including type of formula and timing of introduction. [1] [2]
3. Examination by phenotype. In the immediate reactor, look for urticaria, angioedema, wheeze, stridor, and signs of shock. In the delayed reactor, assess growth (plot weight and length — faltering growth is a red flag), examine the abdomen, inspect the perianal area and stool pattern, and grade the eczema with a validated tool. A well-looking, growing infant with blood-streaked mucus in the stool is the classic proctocolitis picture. [1]
4. Growth is a vital sign in this topic. Plot every infant with suspected CMPA on a growth chart. Faltering growth alongside gastrointestinal symptoms and eczema raises the severity and pushes the child toward specialist input and an amino-acid formula. A thriving, well infant with isolated blood in the stool can usually be managed in primary care with a planned elimination trial. [1] [12]
5. Family and social context. Confirm whether the family understands what elimination actually requires — cow's-milk protein hides in bread, biscuits, processed foods, and some medications. Check the family's capacity to access and afford specialised formula, and identify any need for dietetic, interpreter, or financial-support input, because adherence drives outcome. [2]
Investigations
Investigations in CMPA phenotypes rather than confirms — they do not screen for the disease and they never exclude it. Use them to characterise the IgE phenotype and to support the clinical picture, not to replace it. [1]
Skin-prick testing and serum specific IgE are useful only in the IgE-mediated phenotype. A wheal of three millimetres or more above the negative control on skin-prick, or an elevated serum specific IgE to cow's milk, supports sensitisation. A negative test does not exclude non-IgE-mediated disease, and a positive test in a child who tolerates milk represents asymptomatic sensitisation, not allergy. Component-resolved diagnostics (testing to specific milk proteins such as casein) can refine risk in specialist hands but do not change first-line management. [3] [7]
The oral food challenge is the gold standard for diagnosis and for assessing tolerance development, but it is rarely needed at first presentation in straightforward non-IgE disease, where elimination and rechallenge settle the question. A supervised challenge is reserved for equivocal cases, for confirming tolerance before liberalising the diet, and for IgE-mediated cases where the history is unclear. It must be done where anaphylaxis can be treated. [1] [7]
Elimination and rechallenge is the diagnostic mainstay for non-IgE disease. Remove cow's-milk protein completely for two to four weeks and assess whether symptoms resolve. If they do, reintroduce milk in a planned, supervised way: recurrence of symptoms confirms the diagnosis, and resolution without recurrence points to a non-allergic cause. This structured approach is what the ESPGHAN and BSACI guidelines both centre. [1] [2]
No routine blood panels, no routine endoscopy. Do not order a generic "allergy panel" of serum IgE tests to multiple foods in an unsettled infant — it generates false positives and anxiety. Reserve endoscopy and biopsy for suspected eosinophilic oesophagitis or enteropathy with atypical or refractory features. [12]
Management — Resuscitation
The only resuscitation in CMPA is anaphylaxis, and it is the one thing you must not be slow on. [3] [7]
Recognise anaphylaxis. The diagnostic standard is acute onset (minutes to a few hours) involving skin or mucosal tissue (urticaria, angioedema, pruritus) plus either respiratory compromise (stridor, wheeze, increased work of breathing, hypoxaemia) or reduced blood pressure (pallor, floppiness, collapse). In infants, lethargy and floppiness may be the only sign of cardiovascular involvement. Gastrointestinal features such as repetitive vomiting often accompany paediatric anaphylaxis. [7]
Treat immediately. Lie the child flat with legs raised (do not sit or stand them up — empty-vena-cava collapse is a recognised cause of death). Give intramuscular adrenaline into the anterolateral thigh at the weight-appropriate dose, repeat after five minutes if there is no improvement, and call for paediatric emergency help. Support the airway and give high-flow oxygen and intravenous fluids for shock. Bronchodilators are added for persistent bronchospasm. [7]
Adrenaline autoinjector and action plan before discharge. Any child who has had anaphylaxis to cow's milk leaves with a prescribed adrenaline autoinjector, a written anaphylaxis action plan, training of caregivers, and a clear referral to paediatric allergy. This is non-negotiable — deaths in food allergy cluster around delayed adrenaline and absent autoinjectors. [7]
Management — Definitive & Stepwise
Once the threat gate is clear, definitive management is elimination of cow's-milk protein, structured by feeding mode and severity, with a planned path back to tolerance. [1] [2]
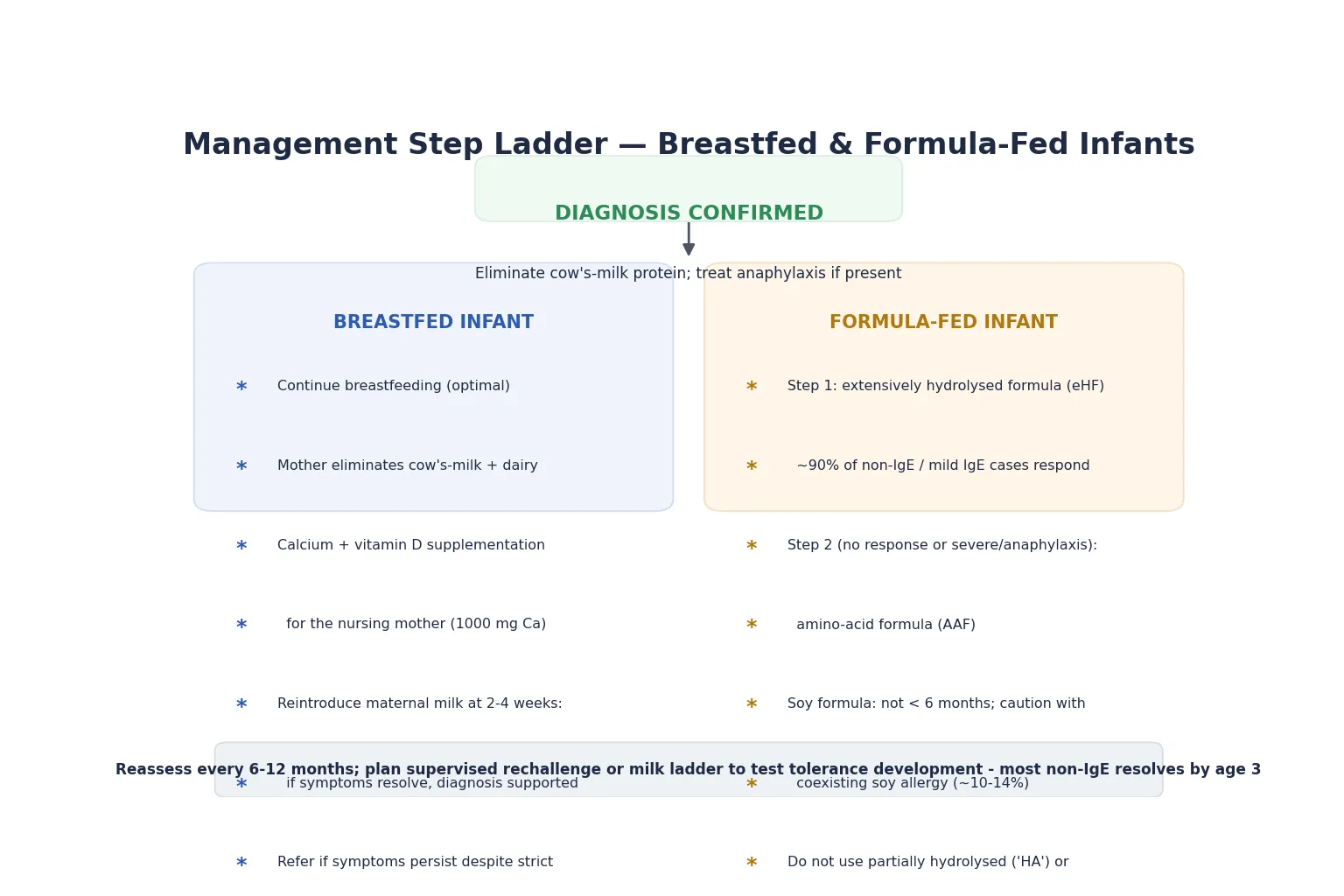
Breastfed infant — continue breastfeeding. Breastfeeding remains optimal and should not be stopped. The nursing mother eliminates all cow's-milk and dairy from her own diet for two to four weeks as both a diagnostic and a therapeutic trial. Because eliminating dairy removes the main dietary calcium source, she must take calcium and vitamin D supplementation (approximately 1000 mg calcium daily) to protect her own bone health. If symptoms resolve, the diagnosis is supported; if they persist despite strict elimination, broaden the differential and reconsider. [1] [2]
Formula-fed infant — the step ladder. First-line is an extensively hydrolysed formula (eHF), in which the proteins are broken down sufficiently that around 90 per cent of infants with CMPA tolerate them. If the infant does not respond within two to four weeks, or if the presentation is severe (anaphylaxis, faltering growth, multiple food allergies), step up to an amino-acid formula (AAF), which is non-allergenic. Soy formula is not first-line in infants under six months because of cross-reactivity (around ten to fourteen per cent react to soy as well) and its phytoestrogen content; it may be considered after six months in selected cases. [1] [2]
Never use partially hydrolysed ("HA" or hypoallergenic) formulas for confirmed CMPA — they retain enough intact protein to trigger reactions. Equally, mammalian milks from goat, sheep, or mare cross-react with cow's-milk proteins and are not safe substitutes. The degree of cross-reactivity is high enough that they are contraindicated. [1] [3]
Baked-milk tolerance. Many children with CMPA tolerate extensively heated milk (as in muffins or cakes) because heat denatures the conformational epitopes that drive most reactions. Establishing baked-milk tolerance under supervision allows a less restrictive diet and accelerates full tolerance. Leonard and colleagues reviewed the evidence for baked-milk and baked-egg diets and found that introducing baked forms is associated with faster acquisition of tolerance. This is a specialist-guided step, not a home experiment in an IgE-mediated child. [9] [10]
Formula step ladder (no invented milligram doses)
Build tolerance over time. Most children — especially the non-IgE group — outgrow CMPA. Reassess at intervals (every six to twelve months for IgE-mediated, earlier for non-IgE) and use a structured milk ladder — gradual reintroduction of milk-containing foods from baked through to uncooked forms — to test and accelerate tolerance development. A milk ladder in a non-IgE child can often begin from around nine to twelve months; an IgE-mediated child needs supervised challenge. [1] [2]
Dietetic input is essential, not optional. Eliminating cow's milk removes a major source of calories, calcium, and vitamin D. A paediatric dietitian ensures adequate nutrition for the growing infant, guides the mother on a nutritionally complete dairy-free diet, and plans the reintroduction. [1] [8]
Specific Subtypes & Scenarios
Cow's-milk protein-induced proctocolitis is the commonest non-IgE pattern and the most reassuring. A well-looking, thriving breastfed (or formula-fed) infant develops blood and mucus in the stools, usually within the first few months of life. There is no systemic illness, no anaemia, and growth is preserved. Maternal elimination (or eHF) resolves the bleeding within two to four weeks, and tolerance typically develops by age one. This can be managed in primary care without extensive investigation. [1] [2]
Food-protein-induced enterocolitis syndrome (FPIES) to cow's milk is the dangerous delayed pattern. One to four hours after milk exposure the infant develops repetitive projectile vomiting that progresses to lethargy, pallor, and dehydration — a picture that mimics sepsis. Management in the acute episode is intravenous fluids and supportive care; the long-term management is strict avoidance and a planned, supervised oral food challenge to assess tolerance, because FPIES reactions can be severe. [1]
Severe IgE-mediated CMPA with anaphylaxis drives the most stringent pathway: absolute avoidance, an adrenaline autoinjector, a written action plan, and regular allergy review. These children are at ongoing risk, and the family must be able to read and act on the early signs of a reaction. School, childcare, and any caregiver must be included in the plan. [3] [7]
Eosinophilic oesophagitis sits at the edge of the topic. Persistent reflux unresponsive to standard therapy, dysphagia, food refusal, or food impaction in an older infant or child warrants endoscopy with biopsy. Cow's milk is a leading trigger, and elimination is part of both diagnosis and treatment, but the pathway is specialist-led. [1]
The multiple-food-allergic infant. A child reacting to several foods, with faltering growth or severe eczema, needs paediatric allergy and dietetic input to avoid nutritional collapse from over-restriction. The temptation to eliminate foods one by one on the basis of positive tests is a known cause of avoidable malnutrition. [12]
Complications & Pitfalls
Over-diagnosis is the dominant modern pitfall. The combination of readily available allergy tests and the temptation to label any unsettled formula-fed infant leads to widespread over-diagnosis of CMPA, with unnecessary formula switches, maternal dietary restriction, parental anxiety, and — most seriously — nutritional compromise from extended elimination that is never challenged. Vandenplas and colleagues highlight this "remaining challenge" as a central issue in everyday practice. [12]
Under-treatment of anaphylaxis remains the catastrophic pitfall. Delayed adrenaline, absent autoinjectors, and failure to recognise that floppiness and pallor in an infant can be cardiovascular anaphylaxis all contribute to avoidable harm. Any child with a clear immediate reaction to milk must have anaphylaxis actively considered and excluded, not dismissed as "a bit of a rash." [3] [7]
Nutritional deficiency from poor elimination. Cow's milk is a major source of calcium, calories, and vitamin D. Without dietetic input, an elimination diet can cause faltering growth, rickets, and poor bone health — in the infant and in the nursing mother who eliminates dairy without calcium replacement. [1] [8]
Mislabelling lactose intolerance as CMPA leads to lifelong unnecessary restriction. Lactose intolerance is an enzyme deficiency, not an immune condition, and does not carry anaphylaxis risk; conflating the two over-restricts the diet and under-prepares the family for the real risks. [2]
FPIES mistaken for sepsis or gastroenteritis. The delayed, repetitive vomiting of FPIES can lead to extensive septic work-up before the allergic trigger is identified. Recognising the temporal pattern — vomiting one to four hours after a specific food — shortens the journey and avoids repeated iatrogenic harm. [1]
Prognosis & Disposition
The prognosis of CMPA is generally excellent, and saying so clearly is part of good care. Most children develop tolerance over time, and the arc is faster for the non-IgE phenotype than the IgE phenotype. [1] [4]
In Skripak's cohort of IgE-mediated disease, around half of the children had acquired tolerance by five years, with higher initial specific IgE and larger skin-prick wheals predicting slower resolution. Non-IgE-mediated proctocolitis resolves even earlier — typically by the first birthday. The overall message is that the majority of these infants will eat dairy freely by school age, which is why indefinite restriction without reassessment is poor practice. [4]
Disposition follows severity. A well-looking infant with proctocolitis and preserved growth can be managed in primary care with a planned elimination and rechallenge. Any child with anaphylaxis, faltering growth, FPIES, multiple food allergies, or diagnostic uncertainty is referred to paediatric allergy and dietetics. The family leaves with a clear written plan covering elimination, the rechallenge timeline, nutritional support, and — where relevant — an adrenaline autoinjector and action plan. [1] [2]
Special Populations
Breastfed infants and their mothers. Continuing breastfeeding is optimal and must be defended. The mother's elimination must be nutritionally supported with calcium and vitamin D, and she needs clear guidance that one brief trial of reintroduction at two to four weeks confirms the diagnosis rather than committing her to long-term restriction. [1] [8]
The multi-food-allergic or growth-faltering infant. These children sit at high risk of nutritional collapse from cumulative elimination and need coordinated allergy and dietetic input. Over-restriction driven by multiple positive tests is a recognised harm; the priority is to maintain growth and nutrition while confirming each true trigger. [12]
Adolescents with persistent IgE-mediated CMPA. A minority do not resolve, and the adolescent faces the burden of ongoing avoidance, anaphylaxis risk in social and restaurant settings, and the developmental task of self-managing an autoinjector. Transition to adult allergy services, peer education, and a written action plan support safety and quality of life. [3] [7]
Socioeconomically disadvantaged families. Specialised formula is expensive and may not be subsidised, and dairy-free diets cost more than standard diets. Assess affordability, signpost to financial support and subsidised formula pathways, and recognise that non-adherence to elimination is often economic, not educational. [2]
Indigenous, refugee, and migrant families. Use trained interpreters, place the diagnosis in a culturally meaningful frame, and respect that elimination of staple foods may conflict with cultural food practices. Build the plan with the family rather than for them. [2]
Evidence, Guidelines & Regional Differences
The evidence base for CMPA is guideline-rich, and the major guidelines are broadly concordant on the clinical-diagnosis principle, the elimination-rechallenge method, and the formula step ladder — but they differ in emphasis and detail. [1] [11]
The ESPGHAN practical guideline (Koletzko and colleagues, 2012) centres a structured diagnostic approach and the extensively-hydrolysed-formula-first principle, and it is the most widely adopted framework in Europe and ANZ. The BSACI guideline (Luyt and colleagues, 2014) provides the UK framework and emphasises primary-care management of mild non-IgE disease with a clear elimination-rechallenge pathway. The DRACMA guideline (Fiocchi and colleagues, 2010, with updates) offers an evidence-graded global framework; its global impact and uptake were later reviewed by Fiocchi and colleagues. The EAACI food-allergy guideline (Muraro and colleagues, 2014) covers diagnosis and management across food allergens and underpins the anaphylaxis-prevention principles. [1] [2] [3] [7] [11]
The primary prevention evidence shifted decisively with the AAP clinical report (Greer and colleagues, 2019), which concluded that there is no evidence that maternal dietary restriction during pregnancy or lactation, or delayed introduction of allergenic foods, prevents atopic disease — and that hydrolysed formula does not reliably prevent allergy. This overturned earlier advice to delay allergen introduction and moved practice toward early introduction and the dual-allergen-exposure model. [8]
Controversies persist. The boundary between CMPA and non-allergic infant distress (reflux, colic) is drawn differently by clinicians, and over-diagnosis remains a live concern. The role of component-resolved diagnostics and baked-milk protocols in primary care, versus specialist settings, is still evolving. [12]
Exam Pearls
The clinical pathway in five moves
Phenotype and threat-gate: immediate vs delayed; rule out anaphylaxis now
Confirm clinically: eliminate cow's-milk protein 2-4 weeks, assess resolution
Plan rechallenge: recurrence confirms CMPA; resolution without recurrence points elsewhere
Manage elimination: breastfeed with maternal dairy-free diet + calcium, or eHF/AAF for formula-fed
Build tolerance: reassess 6-12 monthly; milk ladder or supervised challenge; refer anaphylaxis/severe to allergy
The high-yield facts an examiner will probe: the two phenotypes and their timing windows, the clinical-not-test diagnosis, the formula step ladder (eHF then AAF), the absolute avoidance of partially hydrolysed and mammalian milks, the natural history of resolution, and the FPIES pattern. If you can state "I diagnose CMPA clinically and confirm by elimination and rechallenge, because tests phenotype but do not confirm" you have answered the core question. [1] [2]
The dangerous fact to demonstrate you own: anaphylaxis to cow's milk requires IM adrenaline immediately, an autoinjector before discharge, and a written action plan — and infants may present with floppiness and pallor rather than the classic adult picture. [3] [7]
The pitfall to name unprompted: over-diagnosis from allergy testing in unsettled infants causes unnecessary restriction and nutritional harm, and lactose intolerance is not CMPA. Naming this shows you understand the harm of the reflexive label. [12]
References
- [1]Koletzko S Diagnostic approach and management of cow's-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines. Journal of pediatric gastroenterology and nutrition, 2012.PMID 22569527
- [2]Luyt D BSACI guideline for the diagnosis and management of cow's milk allergy. Clinical and experimental allergy, 2014.PMID 24588904
- [3]Fiocchi A Diagnosis and Rationale for Action Against Cow's Milk Allergy (DRACMA): a summary report. The Journal of allergy and clinical immunology, 2010.PMID 21134569
- [4]Skripak JM The natural history of IgE-mediated cow's milk allergy. The Journal of allergy and clinical immunology, 2007.PMID 17935766
- [5]Liu AH National prevalence and risk factors for food allergy and relationship to asthma: results from the National Health and Nutrition Examination Survey 2005-2006. The Journal of allergy and clinical immunology, 2010.PMID 20920770
- [6]Nwaru BI Prevalence of common food allergies in Europe: a systematic review and meta-analysis. Allergy, 2014.PMID 24816523
- [7]Muraro A EAACI food allergy and anaphylaxis guidelines: diagnosis and management of food allergy. Allergy, 2014.PMID 24909706
- [8]Greer FR The Effects of Early Nutritional Interventions on the Development of Atopic Disease in Infants and Children: The Role of Maternal Dietary Restriction, Breastfeeding, Hydrolyzed Formulas, and Timing of Introduction of Allergenic Complementary Foods. Pediatrics, 2019.PMID 30886111
- [9]Leonard SA Baked Milk and Egg Diets for Milk and Egg Allergy Management. Immunology and allergy clinics of North America, 2016.PMID 26617232
- [10]Leonard SA Baked Egg and Milk Exposure as Immunotherapy in Food Allergy. Current allergy and asthma reports, 2016.PMID 27002516
- [11]Fiocchi A The global impact of the DRACMA guidelines cow's milk allergy clinical practice. The World Allergy Organization journal, 2018.PMID 29308116
- [12]Vandenplas Y The Remaining Challenge to Diagnose and Manage Cow's Milk Allergy: An Opinion Paper to Discuss Daily Practice Challenges. Nutrients, 2023.PMID 38004156