Paeds · allergy-and-immunology
Drug allergy and delabelling in children
Also known as Antibiotic allergy in children · Penicillin allergy · Beta-lactam allergy · Drug hypersensitivity · Penicillin allergy delabelling · Drug provocation testing in children
Fellowship topic on drug allergy and delabelling in children. Penicillin allergy is the prototype: 5-10% of children carry the label, but more than 90% are not truly allergic when tested. The false label drives broader-spectrum antibiotics, longer admissions and resistance. Covers Gell-Coombs classification (immediate IgE vs delayed T-cell), why most labels are wrong (viral exanthem, especially amoxicillin-EBV, waning IgE, non-allergic symptoms), the structured allergy history, PEN-FAST risk stratification, skin-prick/intradermal testing and drug provocation, the direct oral amoxicillin challenge pathway, the severe never-re-challenge reactions (anaphylaxis, SJS/TEN, DRESS, AGEP), antibiotic stewardship, and family communication across ANZ/UK/US/Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Drug allergy in five words — and the trap
Overview & Definition
Picture an eight-year-old girl in your clinic with community-acquired pneumonia. Her mother says firmly, "She's allergic to penicillin — she had a rash as a toddler." The label has followed her for six years. The question you must answer is not "what antibiotic can I use instead?" but "is this allergy even real?" In the great majority of cases it is not, and recognising that transforms her care from a second-line workaround into first-line therapy. Drug allergy, and the epidemic of false penicillin-allergy labels, is one of the highest-yield topics in general paediatrics because it sits at the intersection of allergy, antimicrobial stewardship and patient safety. [3] [10]
A drug allergy is an adverse drug reaction with a demonstrated or confirmed immunologic mechanism. The term matters because it separates true immune-mediated reactions from the much larger group of adverse drug reactions that are not immunological — expected side-effects such as gastrointestinal upset, intolerance, overdose, and pseudoallergy from direct mast-cell activation. When a parent says a child is "allergic" to amoxicillin because it caused diarrhoea, or because a grandparent was allergic, that is not a drug allergy; it is a mislabel, and mislabels are the heart of the problem. [4] [11]
The clinician's work has two halves. The acute half is to recognise and treat the genuine immune reaction — anaphylaxis, the severe delayed skin reactions, and the milder immediate and delayed rashes. The longitudinal half is to evaluate the label: to take a structured history, risk-stratify the child, and either confirm and document a true allergy or remove the false label through a safe delabelling pathway so the child can receive first-line therapy again. Both halves are examined, and both are common. [3] [8]
Classification
Classify a drug reaction along the two axes that decide everything you do next: the timing of the reaction, and its severity. Timing splits reactions into immediate and delayed, and the dividing line is one hour from exposure. Immediate reactions — appearing within minutes to one hour — are IgE-mediated (Gell-Coombs Type I): urticaria, angiooedema, bronchospasm, rhinitis, gastrointestinal symptoms and anaphylaxis. Delayed reactions — appearing after one hour, often days into a course — are T-cell mediated (Type IV): the maculopapular exanthem that dominates paediatrics, fixed drug eruptions, and the severe blistering and systemic syndromes. [4] [11]
The other Gell-Coombs types round out the framework but are far less common in children. Type II is cytotoxic antibody-mediated, causing drug-induced immune haemolysis or thrombocytopenia. Type III is immune-complex-mediated, producing serum-sickness-like reactions — rash, fever and arthralgia days to weeks after exposure, classically seen with cefaclor in young children. Knowing these names matters for the exam, but in day-to-day paediatric allergy the Type I/Type IV split and the severity axis do most of the work. [4] [11]
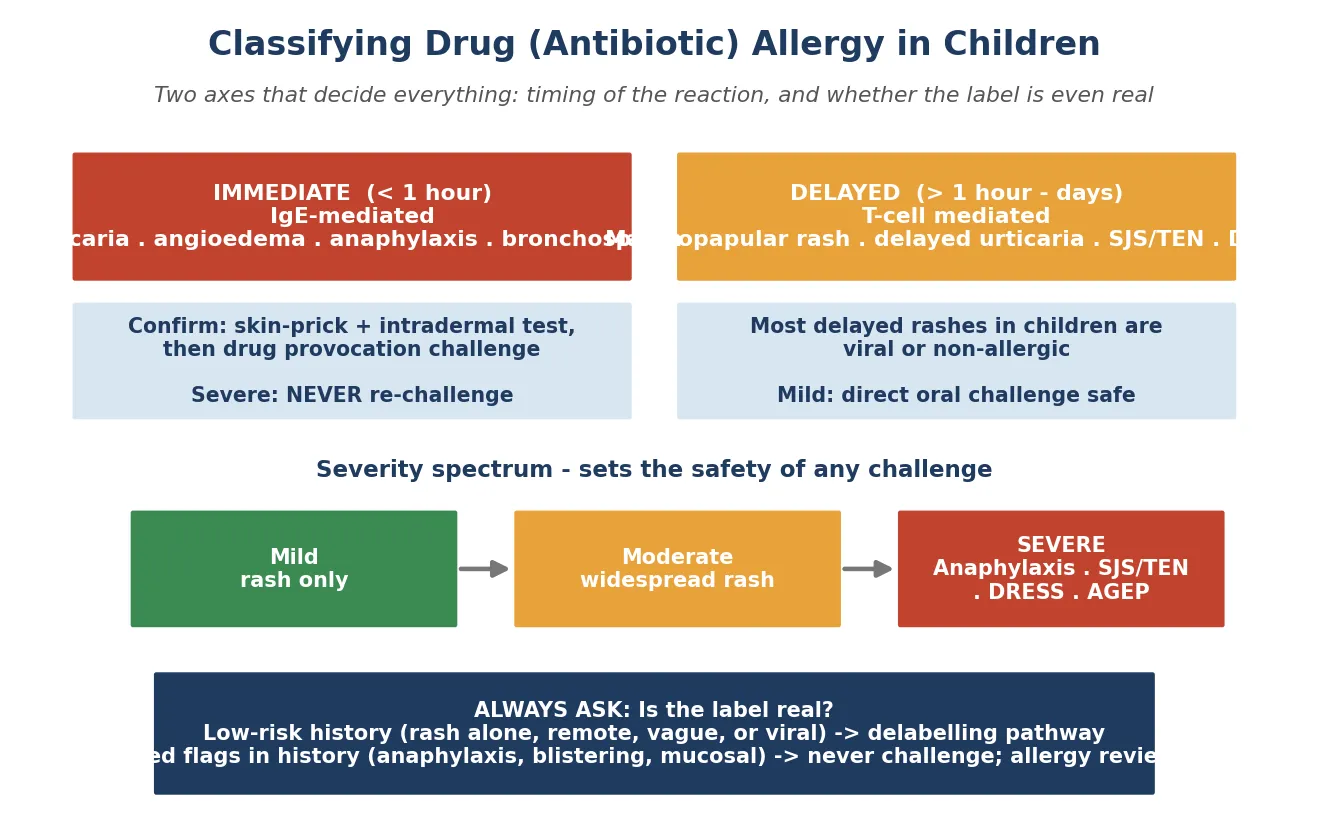
Severity is the safety axis. A mild reaction — an isolated rash, a few hives — is compatible with evaluation and, if low-risk, with a direct oral challenge. A severe reaction — anaphylaxis, blistering with mucosal involvement, multi-organ disease — is a permanent contraindication to re-challenge. The clinical decision at the bedside is almost always about reading these two axes from a historical account, which is why the structured history is the single most important skill in this topic. [3] [10]
Finally, classify the label itself: is it a true, verified allergy, or an unverified label? An unverified label is the default state of most paediatric penicillin-allergy records, and it is the target of delabelling. This distinction — verified allergy versus unverified label — reframes the whole encounter from "avoid penicillin" to "evaluate and, where safe, remove the label." [10] [8]
Epidemiology & Risk Factors
Where does drug allergy sit in children, and who carries the label? Self-reported drug allergy is common in the community: a systematic review and meta-analysis by Sousa-Pinto and colleagues found that roughly 5% of the general population report a drug allergy, with antibiotics and non-steroidal anti-inflammatory drugs the most frequently named. Penicillin is the commonest drug-allergy label in children by a wide margin, simply because penicillins are the most frequently prescribed antibiotics in paediatrics. [15] [3]
The defining epidemiological fact of this topic is that the vast majority of these labels are false. Around 5–10% of children carry a penicillin-allergy label, but when formally evaluated with skin testing and drug provocation, more than 90% cannot be confirmed as allergic. They are either not allergic and never were, or they were allergic once and the allergy has resolved. This is not a marginal finding — it is one of the most consistent results in paediatric allergy, and it is the foundation of the delabelling movement. [3] [8]
In Australia and Aotearoa New Zealand, penicillin-allergy delabelling is increasingly delivered through antimicrobial-stewardship programmes and specialist allergy services, supported by ASCIA guidance. The emphasis is on proactive evaluation of low-risk labels rather than passive avoidance, and on updating every record so the label does not resurface. The pathway aligns with the international PEN-FAST direct-challenge evidence. [1] [2]
The drivers of false labelling are worth understanding because they are preventable. The commonest is a rash that coincided with a viral illness — the amoxicillin-EBV rash is the classic, but any childhood exanthem can be misattributed to the antibiotic that happened to be on board. Add recall drift over years, second-hand labels ("my mother said I was allergic"), non-allergic symptoms recorded as allergy, and the absence of any verification at the time, and the false label propagates through every subsequent encounter. [10] [9]
The clinical groups in whom the label does the most harm are children who need beta-lactams repeatedly: those with cystic fibrosis, oncology, complex chronic disease and recurrent infection. In these children a false label funnels them into second-line agents again and again, with cumulative harm. They are the priority candidates for proactive delabelling, and a label in a child with complex disease should trigger evaluation, not resignation. [8] [11]
Pathophysiology
Why does a drug cause an immune reaction at all — and why do most childhood labels have no immune basis? Penicillins and other beta-lactams are small molecules that cannot trigger an immune response on their own. They act as haptens: they covalently bind host proteins to form larger immunogenic complexes, which can then generate drug-specific IgE or drug-specific T-cell responses. This haptenisation is the molecular event that lies beneath both the immediate and the delayed pathways. [4] [5]
In the immediate (Type I) pathway, drug-specific IgE attaches to mast-cell Fc-epsilon receptors. On re-exposure, the antigen cross-links the IgE, the mast cell degranulates, and released histamine and lipid mediators produce urticaria, angiooedema, bronchospasm and — at its most severe — anaphylaxis, all within minutes to one hour. This is the mechanism that makes skin-prick and intradermal testing relevant: they look for the IgE that drives this cascade. [4] [7]
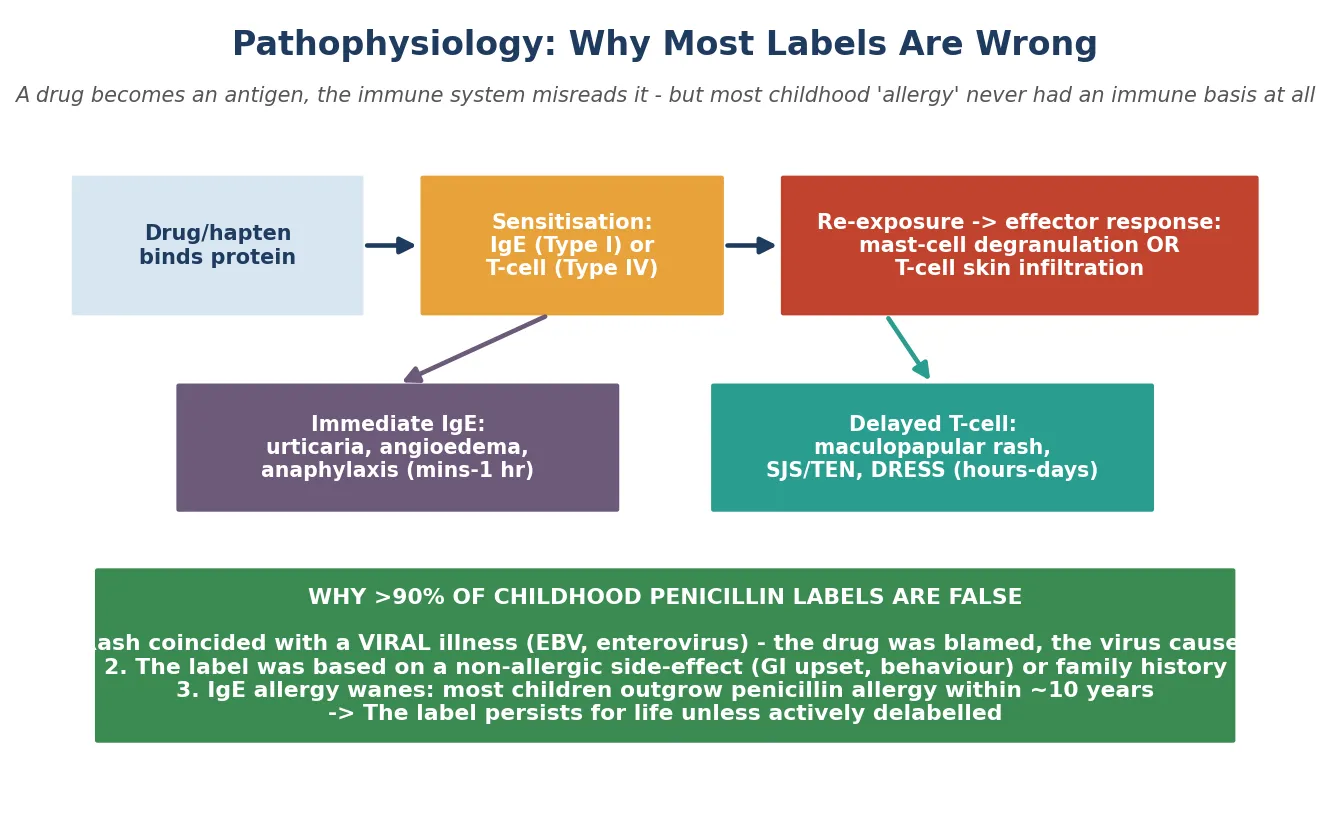
In the delayed (Type IV) pathway, drug-specific cytotoxic and helper T-cells infiltrate the skin or mucosa hours to days after exposure, producing the maculopapular exanthem that is by far the commonest delayed paediatric reaction. In its severe forms the same T-cell machinery drives Stevens-Johnson syndrome and toxic epidermal necrolysis, DRESS and acute generalised exanthematous pustulosis. These severe delayed syndromes share the T-cell mechanism with the benign rash, which is why severity — not mechanism alone — must drive the never-re-challenge decision. [4] [11]
The reason most childhood penicillin labels are false flows directly from this biology. First, the rash attributed to the antibiotic was usually caused by an intercurrent viral illness — virologically documented for EBV and amoxicillin, and plausible for the many other childhood exanthems — so no immune mechanism to the drug ever existed. Second, where a true IgE allergy once existed, it wanes: most children who were genuinely allergic tolerate penicillin again within roughly ten years. That decay of IgE sensitivity is the biological fact that makes delabelling not merely possible but medically necessary. [5] [10]
Clinical Presentation
The immediate (Type I) presentation is the one you must never miss. Within minutes to one hour of exposure, the child develops urticaria, angiooedema, pruritus, rhinitis, wheeze or gastrointestinal symptoms, and this can progress to anaphylaxis with airway compromise, respiratory distress and circulatory collapse. The close temporal link to the dose is the clue, and the speed is the danger: an immediate reaction demands immediate cessation of the drug and readiness to treat anaphylaxis. [7] [11]
The delayed presentation is the one you will see most often, and the one that generates most labels. A maculopapular or morbilliform exanthem begins hours to days into a course — commonly around day five to ten — and is usually mild and non-toxic. The child is well apart from the rash. This is the commonest 'allergy' presentation in children, and it is also the commonest false label, because the identical rash is produced by the viral illnesses for which the antibiotic was prescribed in the first place. [3] [9]
The severe delayed presentations are emergencies and permanent contraindications to re-challenge. Stevens-Johnson syndrome and toxic epidermal necrolysis present with mucocutaneous blistering, target lesions, skin pain, mucosal involvement and systemic symptoms. DRESS presents two to eight weeks after exposure with rash, fever, lymphadenopathy, eosinophilia and organ dysfunction. AGEP presents with sterile pustules and fever of acute onset. Any of these in the history means never re-challenge and refer to specialist allergy. [4] [11]
The confounded presentation is the one that dominates paediatric practice and tests the clinician most. A child is given amoxicillin for a viral upper-respiratory infection and develops a rash on day five. Is it viral, drug-related, or both? This is exactly the situation that generates false labels, and the correct response is a careful history and prospective documentation of the uncertainty — not reflex labelling. Distinguishing these presentations is the bedside skill this topic rewards. [10] [9]
Differential Diagnosis
The dominant mimic of drug allergy in children is the viral exanthem. Measles, rubella, roseola, erythema infectiosum, enterovirus and Epstein-Barr virus can all produce a rash indistinguishable from a maculopapular drug eruption, and they are the illnesses for which antibiotics are often prescribed. The distinguishing features are the timing relative to the illness, the morphology, the presence of a viral prodrome and fever, and whether the rash recurred on re-exposure — though re-exposure is rarely documented, which is precisely the problem. [3] [4]
An immediate drug reaction must be distinguished from anaphylaxis due to another trigger — food, insect sting or latex — that occurred coincidentally with drug exposure. The temporal relationship to the drug, the constellation of organ involvement, and a careful exposure history are decisive. In the perioperative setting, neuromuscular blocking agents and antibiotics both figure prominently, and the evaluation is best done by a specialist perioperative-allergy service. [7] [4]
Serum-sickness-like reaction must be distinguished from true serum sickness, vasculitis, post-streptococcal arthritis and juvenile idiopathic arthritis. It presents with rash (often annular or urticarial), fever and arthralgia days to weeks after a drug, classically cefaclor in young children. Non-allergic intolerance — gastrointestinal upset, headache — and pseudoallergy from direct mast-cell activation must be separated from immunologic allergy, because the management and the label differ. [4] [11]
Clinical & Bedside Assessment
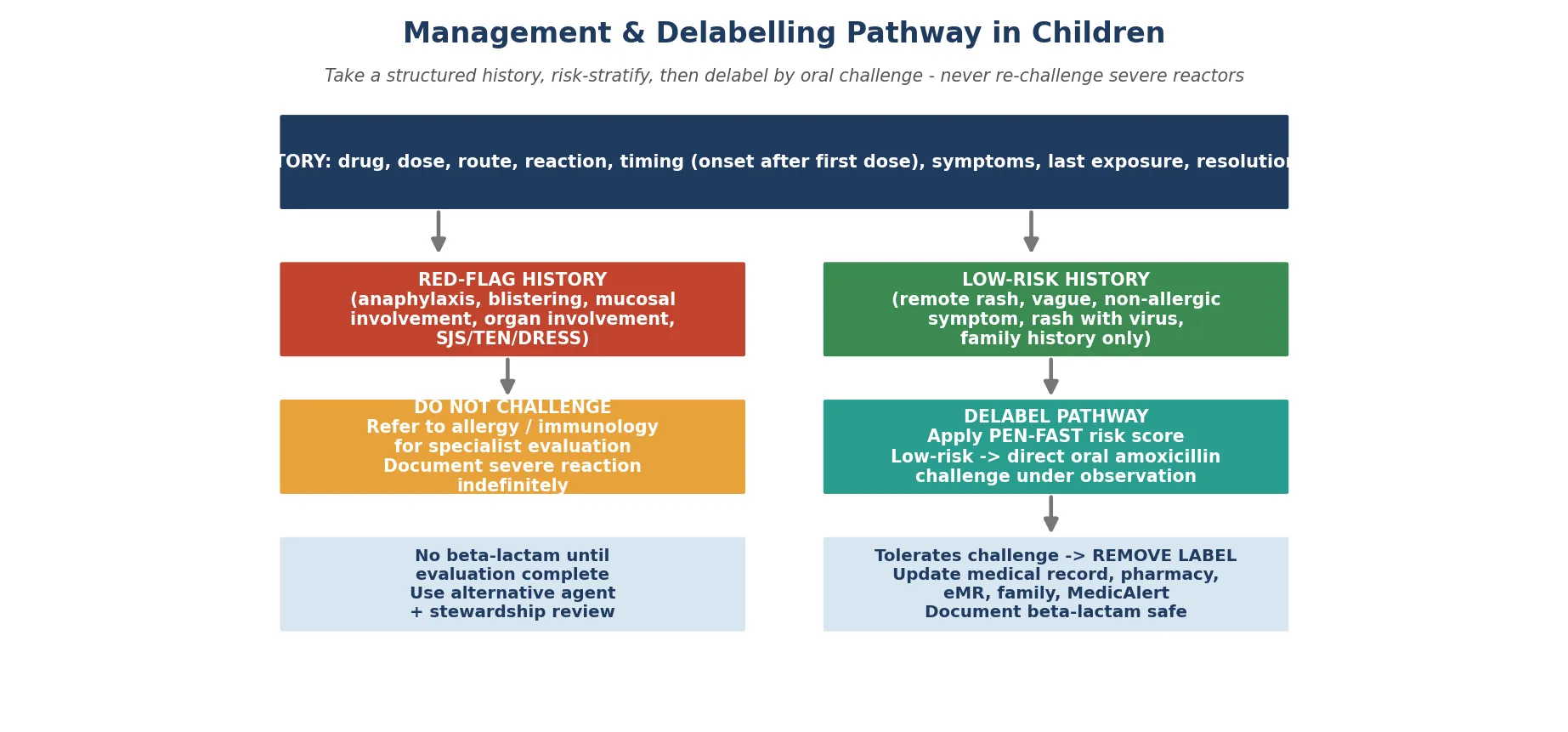
The assessment lives or dies on the history. Take a structured allergy history that captures the specific drug (brand and generic), the dose, route and indication, the exact reaction and its symptoms, the timing of onset relative to the first and last dose, whether the drug was stopped and what then happened, any co-illness (especially viral), previous tolerances and re-exposures, and a family history of allergy. Most of what you need to decide risk is in this history, and a vague history is itself a low-risk feature. [3] [2]
Identify the history red flags that mandate never-challenge and specialist referral. These are anaphylaxis, blistering or skin pain, mucosal involvement, multi-organ involvement, hepatic or renal dysfunction with rash, recurrence on re-exposure, and reactions under general anaesthesia. Any of these in the history closes the direct-challenge pathway and routes the child to a specialist allergy service. Recording these clearly protects the child for life. [4] [10]
Identify the low-risk history features that permit a delabelling or direct-challenge pathway: a remote or childhood-only reaction, a rash alone without systemic features, a vague or second-hand history, a known viral illness at the time, or a non-allergic symptom. These features, captured in validated rules such as PEN-FAST, identify the children in whom direct oral challenge is safe and efficient — and they describe most paediatric labels. [2] [1]
The examination matters most when a reaction is active. Look for urticaria, angiooedema, target lesions, blistering, mucositis, desquamation and pustules on the skin; assess the airway, work of breathing and circulation for anaphylaxis; and check for abdominal findings. For an inactive historical label, the examination confirms the child is well — the work is in the history and the records, not the stethoscope. Synthesise the assessment into a clear problem representation so the next step is obvious. [7] [3]
Investigations
Skin-prick testing looks for the IgE that drives immediate allergy. A prick is made through a drop of the major and minor determinants of penicillin (or the culprit beta-lactam), and the result is read at 15–20 minutes; a wheal 3 mm greater than the negative control is positive. Its limitation is that a negative result alone does not fully exclude IgE allergy, so in many cases skin testing is paired with drug provocation rather than relied upon in isolation. [5] [4]
Intradermal testing is more sensitive than skin-prick for immediate allergy and is also read at a delayed interval for Type IV reactions. Diaferio and colleagues showed that skin tests retain real diagnostic value in children with beta-lactam hypersensitivity, but that their number can be reduced — a practical point for the paediatric setting where minimising needle procedures matters. Serum-specific IgE (ImmunoCAP) to penicillin determinants is an adjunct of lower sensitivity and is never a standalone rule-out. [5] [4]
Drug provocation testing — the controlled, graded administration of the suspected drug under medical observation — is the reference standard. The diagnosis is established or excluded by the response to the actual drug, which is why a negative history plus a tolerated challenge is the most powerful evidence of all. A meta-analysis by Srisuwatchari and colleagues confirmed that direct drug provocation is safe in selected children with beta-lactam hypersensitivity, underpinning the modern direct-challenge pathway. [6] [12]
Interpretation follows directly. A negative evaluation — low-risk history, negative skin tests, tolerated drug provocation — confirms the label is false and the drug is safe, which is the basis for delabelling. A positive test or a reaction to challenge confirms true allergy and mandates avoidance, documentation and specialist follow-up. The investigation is not an end in itself; it exists to settle whether the label should stand or fall. [4] [10]
Management — Resuscitation
The resuscitation priority in drug allergy is anaphylaxis. Recognise it — airway, breathing or circulation compromise after a drug — and treat it immediately with intramuscular adrenaline (epinephrine) at 0.01 mg/kg (0.01 mL/kg of 1:1000, equivalent to 10 microgram/kg), repeated every five minutes as needed, into the anterolateral thigh, with airway support, oxygen, supine positioning and intravenous fluid resuscitation. Stop the suspected drug the moment an acute reaction begins. [7] [11]
For an acute urticarial or mild immediate reaction, stop the drug, give an oral or parenteral antihistamine, observe the child, and arrange definitive evaluation once the acute episode has resolved. The point of the acute encounter is to treat now and to set up the later evaluation that will determine whether the label stands. [4] [10]
Severe delayed reactions are emergencies in their own right. Stevens-Johnson syndrome, toxic epidermal necrolysis, DRESS and AGEP require immediate cessation of the culprit drug, supportive and specialist dermatology, burns or intensive-care management as the syndrome demands, and permanent contraindication to re-challenge. These children are never part of any delabelling pathway; they are referred to specialist allergy services for definitive documentation and cross-reactivity counselling. [4] [11]
Management — Definitive & Stepwise
The definitive management of an unverified label is the delabelling pathway, and it is best delivered as a stepwise algorithm. The steps are: take a structured history and risk-stratify; apply a validated clinical decision rule (PEN-FAST) and the low-risk criteria; for low-risk children, proceed to a direct oral amoxicillin challenge under observation; and on tolerance, remove the label and document it everywhere. Each step has a clear trigger and a clear output. [1] [3]
The risk-stratification tool is PEN-FAST, developed and validated by Trubiano and colleagues. The letters name the components: Penicillin allergy (scored by how long ago the reaction occurred), five years or less since the reaction (PEN-FAST timing item), Anaphylaxis, Severe skin reaction, and Treatment received. A PEN-FAST score of less than 3 identifies low-risk patients suitable for direct oral challenge without prior skin testing. This rule transformed penicillin-allergy evaluation from an allergist-only, skin-test-first process into an efficient pathway that trained clinicians can deliver. [2] [10]
The delabelling pathway in a low-risk child
Structured history — drug, dose, timing, symptoms, co-illness, re-exposure, family history; confirm low-risk features and no red flags
Apply PEN-FAST — a score under 3 supports direct oral challenge without prior skin testing
Direct oral amoxicillin challenge — single or graded dose under observation with anaphylaxis capacity
Tolerates challenge — remove the label and document across the electronic record, pharmacy, MedicAlert, family and GP
Communicate — explain to the family in plain language that the allergy was not real, and provide written confirmation
The direct oral challenge itself is a single or graded dose of oral amoxicillin given under medical observation, with rescue medication and anaphylaxis capacity available, for a defined observation period. The PALACE randomised trial by Copaescu and colleagues showed that a PEN-FAST-guided direct oral challenge was non-inferior to skin testing for low-risk penicillin allergy, and more efficient — the evidence that anchors direct challenge as the preferred pathway for the low-risk majority. [1] [2]
Vezir and colleagues demonstrated that direct oral provocation is safe even in children with non-immediate mild cutaneous reactions to beta-lactams, and Sillcox and colleagues extended the direct-graded-challenge approach to paediatric cephalosporin reactions. Together these studies place direct challenge at the centre of modern paediatric delabelling across the beta-lactam class, with skin testing reserved for selected or higher-risk contexts. [12] [14]
The final step — documentation — is where delabelling most often fails. Removing the label means updating the electronic medical record, the pharmacy record, MedicAlert where relevant, the family-held record and the medication list; counselling the family verbally and in writing; and communicating with the primary care provider. A label that survives in even one record will resurface at the next encounter, and the harm will return, so complete cross-system documentation is part of the treatment, not an afterthought. [10] [8]
The systems-level justification is antibiotic stewardship. Delabelling restores first-line beta-lactam therapy, reduces the use of broader-spectrum alternatives such as macrolides, fluoroquinolones and vancomycin, shortens admissions and lowers the burden of resistance and side-effects. This is why delabelling is increasingly embedded in stewardship programmes and why proactive evaluation of low-risk labels — not passive avoidance — is the recommended standard. [8] [9]
Specific Subtypes & Scenarios
Penicillin allergy is the prototype and the priority. It is the commonest label, the commonest false label, and the label whose removal delivers the greatest stewardship benefit. The amoxicillin-EBV rash is its classic false label, the PEN-FAST and direct-challenge pathway is its evaluation, and the message to families is that removing a false childhood label restores the safest, most effective antibiotic class for the rest of their lives. [3] [1]
Cephalosporin allergy in children is now understood through side-chain cross-reactivity rather than the older "10% cross-reactivity" figure, which is obsolete. Cross-reactivity between penicillin and cephalosporins is driven by shared side-chains — for example between amoxicillin and cefaclor, or amoxicillin and cephalexin — and is low for most modern cephalosporins. Sillcox and colleagues showed that direct graded oral challenge is a safe and effective way to assess paediatric cephalosporin reactions, supporting confident cephalosporin use and delabelling. [14] [13]
Severe delayed reactions — Stevens-Johnson syndrome, toxic epidermal necrolysis, DRESS and AGEP — form a distinct scenario with a single rule: never re-challenge. The culprit drug and structurally related drugs are permanently contraindicated, the child needs specialist evaluation, and the documentation must be explicit and lifelong. Confusing these with a benign rash is the most dangerous error in the topic. [4] [11]
Children with cystic fibrosis, oncology and complex chronic disease are a scenario in their own right because they need beta-lactams repeatedly and a false label is most costly to them. They are priority candidates for proactive delabelling, and the evaluation should be built into their chronic-disease pathway rather than left to a crisis. In the perioperative setting, antibiotic and neuromuscular-blocker reactions require coordination with anaesthesia and specialist perioperative-allergy services, distinguishing true allergy from direct mast-cell activation. [8] [7]
Complications & Pitfalls
The complications of carrying a false label are substantial and well quantified. A systematic review of penicillin-allergy testing outcomes in children, and a study of the impact of penicillin-allergy labels on children treated for outpatient respiratory infections, both show that labelled children receive broader-spectrum and more toxic antibiotics, have longer hospital stays, and carry higher rates of complications, resistance and healthcare cost than children without the label. The label is not benign; it is a recurring source of harm. [8] [9]
The cardinal pitfall is reflex labelling — recording any rash during a drug course as "allergy" without a structured history. This single habit is the engine of the false-label epidemic, and it is the most preventable error in paediatric allergy. The corollary pitfall is the amoxicillin-EBV rash recorded as penicillin allergy, which then persists for decades. Teaching clinicians to pause, take the history, and document uncertainty rather than a label is the intervention that matters most. [3] [10]
A second pitfall is over-reliance on a single negative test. Negative skin tests alone do not exclude penicillin allergy with certainty in every case, which is why the evaluation combines history, skin tests and drug provocation rather than leaning on one result. Treating a single negative skin test as definitive can give false reassurance. [5] [4]
The reverse pitfall is challenging a severe reactor. Re-exposure in Stevens-Johnson syndrome, toxic epidermal necrolysis, DRESS, AGEP or anaphylaxis can be fatal. The history red flags must be actively sought before any challenge pathway is contemplated, and the default for a severe history is never-challenge and specialist referral. Finally, delabelling without documentation is a pitfall in its own right: if the record is not updated in every system, the label resurfaces and the harm recurs. [4] [10]
Prognosis & Disposition
The prognosis of delabelling is excellent. Most low-risk children tolerate the direct oral challenge and are confirmed not allergic; once delabelled, they tolerate beta-lactams long-term and the label does not return. The gain is durable because removing the false label restores first-line therapy for the rest of the child's life — every future infection, every future admission, every future prescription benefits from the one-time evaluation. [8] [1]
The prognosis of true allergy is also more favourable than families assume. The majority of children with confirmed IgE-mediated penicillin allergy lose sensitivity over the years, so a specialist may re-evaluate even a remotely true allergy after an interval, using skin testing and challenge. True allergy is therefore not always permanent, though the severe delayed syndromes are. [5] [10]
For a positive challenge or confirmed severe allergy, the disposition is lifelong avoidance of the culprit and relevant cross-reactive drugs, MedicAlert documentation, family and carer education on recognition, an adrenaline autoinjector where the allergy is IgE-mediated, and specialist allergy follow-up. The safety-net for a delabelled child is that if a future beta-lactam course produces any reaction, the drug is stopped and the child reassessed — delabelling removes the unverified label, it does not guarantee lifetime tolerance in the rare event of new sensitisation. [7] [10]
The systems disposition matters as much as the clinical one. Delabelled status must be communicated to the general practitioner, pharmacist, hospital record, school and family so that the restoration of first-line therapy is realised at every future encounter. The disposition is only complete when the label has been removed everywhere it could do harm. [10] [8]
Special Populations
Children with cystic fibrosis, oncology and complex chronic disease are the priority delabelling candidates because their repeated beta-lactam need makes a false label most costly. Integrate delabelling into routine chronic-disease review rather than waiting for a crisis; the cumulative benefit across years of treatment is large, and these children are most harmed by defaulting to second-line agents. [8] [9]
For Indigenous and migrant or refugee families, ensure the evaluation is delivered with interpreters and in a culturally safe way, with clear written and verbal explanation of what delabelling means. The consequences of carrying a label are amplified when records are fragmented across services and languages, so clear communication and complete documentation protect these families disproportionately. [3] [11]
Adolescents transitioning to adult care should be delabelled before transfer so they do not carry a childhood label into adult prescribing. Address consent and the young person's own understanding of the label — a label acquired in infancy that they have never questioned can otherwise shape their adult care for decades. The transition visit is a natural opportunity to evaluate and remove. [10] [8]
In immunocompromised children, rash is common during therapy and is often non-allergic — driven by the drug, by infection, or by graft-versus-host disease. Avoid reflex labelling in this group and pursue a structured evaluation with the treating team, so that a child who needs beta-lactams for neutropenic sepsis is not denied them on the basis of a non-allergic rash. [11] [4]
Evidence, Guidelines & Regional Differences
The evidence base has matured rapidly. The PALACE randomised trial by Copaescu and colleagues established that a PEN-FAST-guided direct oral challenge is non-inferior to skin testing for low-risk penicillin allergy, anchoring direct challenge as the efficient modern pathway. The PEN-FAST development and validation study by Trubiano and colleagues provided the decision rule that makes risk stratification practical, and systematic reviews of paediatric penicillin-testing outcomes and direct drug-provocation safety supply the quantitative backbone for harm and safety. [1] [6]
The guidance landscape is concordant in principle and varied in operation. The Canadian Paediatric Society statement on beta-lactam allergy in the paediatric population sets a clear Canadian approach to evaluation and delabelling in children. The EAACI position paper on beta-lactam hypersensitivity diagnosis and the ESCMID clinical guideline on reported antibiotic allergy provide the specialist European framework and the newest international guidance, respectively. [3] [4]
Regional differences centre on who performs delabelling and how aggressively direct oral challenge is deployed. ANZ practice, supported by ASCIA and stewardship programmes, increasingly favours trained non-allergist delabelling and direct challenge for low-risk labels. North American practice, framed by the AAAAI/ACAAI and the Canadian Paediatric Society, similarly endorses direct challenge in low-risk children. European practice, shaped by EAACI and ESCMID, shares the principles and is converging on direct challenge, though the allergist-led model persists in some systems. The evidence is now strong enough that the direction of travel everywhere is toward proactive, low-risk direct delabelling. [1] [11]
PALACE (Copaescu et al., JAMA Intern Med 2023)
Population: Adults and adolescents with low-risk penicillin-allergy labels (PEN-FAST guided)
Comparator: Standard skin-test-first pathway
Key finding
Direct oral challenge was non-inferior to skin testing for safety and more efficient, supporting direct challenge as the preferred pathway for low-risk penicillin allergy
Exam Pearls
The one-liner for this topic is that more than nine in ten paediatric penicillin-allergy labels are false — the job is to verify, not to assume. Everything else flows from that single fact: the structured history, the PEN-FAST rule, the direct oral challenge, and the stewardship rationale. [3] [10]
The amoxicillin-EBV rash is the classic false label and the commonest source of a lifelong penicillin label. A maculopapular rash in a child with infectious mononucleosis given amoxicillin is the virus interacting with the drug, not an immunological penicillin allergy. Recording it as allergy without explanation is the single most preventable error in paediatric allergy. [3] [4]
The timing threshold is one hour. Immediate (within one hour) points to IgE and to skin-prick or intradermal testing; delayed (after one hour to days) points to T-cell and to drug provocation or delayed reading. The severity spectrum sets the safety of any challenge — mild rash is challengeable, anaphylaxis and the blistering syndromes never are. [4] [6]
Delabelling is incomplete until it is documented everywhere — the electronic record, pharmacy, MedicAlert, the family and the general practitioner. A label that survives in one system will resurface and the harm will return, so cross-system documentation is part of the treatment. And remember that adrenaline for drug-induced anaphylaxis is intramuscular, never dependent on an oral antihistamine alone. [7] [10]
References
- [1]Copaescu AM; Vogrin S; James F; et al Efficacy of a Clinical Decision Rule to Enable Direct Oral Challenge in Patients With Low-Risk Penicillin Allergy: The PALACE Randomized Clinical Trial. JAMA Intern Med, 2023.PMID 37459086
- [2]Trubiano JA; Vogrin S; Chua KYL; et al Development and Validation of a Penicillin Allergy Clinical Decision Rule. JAMA Intern Med, 2020.PMID 32176248
- [3]Wong T; Atkinson A; t'Jong G; et al Beta-lactam allergy in the paediatric population. Paediatr Child Health, 2020.PMID 32042244
- [4]Romano A; Atanaskovic-Markovic M; Barbaud A; et al Towards a more precise diagnosis of hypersensitivity to beta-lactams - an EAACI position paper. Allergy, 2020.PMID 31749148
- [5]Diaferio L; Chiriac AM; Leoni MC; et al Skin tests are important in children with β-lactam hypersensitivity, but may be reduced in number. Pediatr Allergy Immunol, 2019.PMID 30734416
- [6]Srisuwatchari W; Phinyo P; Chiriac AM; et al The Safety of the Direct Drug Provocation Test in Beta-Lactam Hypersensitivity in Children: A Systematic Review and Meta-Analysis. J Allergy Clin Immunol Pract, 2023.PMID 36528293
- [7]Grabenhenrich LB; Dölle S; Moneret-Vautrin A; et al Anaphylaxis in children and adolescents: The European Anaphylaxis Registry. J Allergy Clin Immunol, 2016.PMID 26806049
- [8]Kwok M; Heard KL; May A; et al Health outcomes of penicillin allergy testing in children: a systematic review. J Antimicrob Chemother, 2023.PMID 36879500
- [9]Joerger T; Taylor MG; Li Y; et al Impact of Penicillin Allergy Labels on Children Treated for Outpatient Respiratory Infections. J Pediatric Infect Dis Soc, 2023.PMID 36461664
- [10]Stone CA Jr; Trubiano J; Coleman DT; et al The challenge of de-labeling penicillin allergy. Allergy, 2020.PMID 31049971
- [11]Joean O; Sermet K; Ashkenazi-Hoffnung L; et al ESCMID clinical guidelines on the evaluation and management of a reported antibiotic allergy. Clin Microbiol Infect, 2026.PMID 41707748
- [12]Vezir E; Dibek Misirlioglu E; Civelek E; et al Direct oral provocation tests in non-immediate mild cutaneous reactions related to beta-lactam antibiotics. Pediatr Allergy Immunol, 2016.PMID 26619970
- [13]Misirlioglu ED; Guvenir H; Toyran M; et al Frequency of selective immediate responders to aminopenicillins and cephalosporins in Turkish children. Allergy Asthma Proc, 2017.PMID 28814358
- [14]Sillcox C; Gabrielli S; O'Keefe A; et al Assessing Pediatric Cephalosporin Allergic Reactions Through Direct Graded Oral Challenges. J Allergy Clin Immunol Pract, 2024.PMID 37832819
- [15]Sousa-Pinto B; Fonseca JA; Gomes ER Frequency of self-reported drug allergy: A systematic review and meta-analysis with meta-regression. Ann Allergy Asthma Immunol, 2017.PMID 28779998