Paeds · allergy-and-immunology
Egg, wheat, soy, fish and shellfish allergy
Also known as Egg allergy · Wheat allergy · Soy allergy · Fish allergy · Shellfish allergy · Crustacean and mollusc allergy · Non-milk non-nut food allergy
Fellowship guide to paediatric egg, wheat, soy, fish and shellfish allergy: the signature allergen protein behind each food, IgE versus non-IgE mechanisms, skin-prick and specific-IgE interpretation, component-resolved diagnostics, the baked-egg ladder, oral food challenge as the gold standard, ASCIA anaphylaxis action plans and adrenaline autoinjector dosing, and the prognosis that separates the childhood-outgrown allergens (egg, wheat, soy) from the lifelong ones (fish, shellfish).
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who vomits and breaks out in hives twenty minutes after a slice of birthday cake, a teenager who collapses on a run two hours after a sandwich, and a toddler who is limp and pale four hours after scrambled egg are all describing the same phenomenon in different forms — an immune response to a specific food protein. Food allergy is an adverse health effect arising from a reproducible immune response that occurs on exposure to a given food, and it stands apart from food intolerance, which is non-immunological.[2]
This topic covers the five common paediatric allergens that are neither milk nor peanut and tree nut: egg, wheat, soy, fish and shellfish. Each carries a signature allergen protein, a characteristic age of onset, and a prognosis that examiners test deliberately. Egg, wheat and soy tend to begin in infancy and resolve through childhood, whereas fish and shellfish more often persist for life and carry a disproportionate share of severe reactions in adolescence and adulthood.[1]
The clinical skill is to move beyond "this child is allergic" to three sharper questions: which mechanism (IgE-mediated immediate, or non-IgE delayed), which component protein (heat-labile or heat-stable), and which prognosis (likely to resolve, or likely lifelong). The answers change the diet, the action plan, and the timing of re-challenge.[4]
Classification
The first decision point is whether the reaction is driven by IgE antibody, because that single distinction changes the investigation and the safety-net. IgE-mediated reactions come on within minutes to two hours of exposure and produce the familiar immediate phenotype of urticaria, angioedema, vomiting, wheeze and anaphylaxis; non-IgE, cell-mediated reactions come on hours later and show up as the delayed gastrointestinal syndromes such as food protein-induced enterocolitis syndrome (FPIES), eosinophilic oesophagitis and food protein-induced proctocolitis.[2]
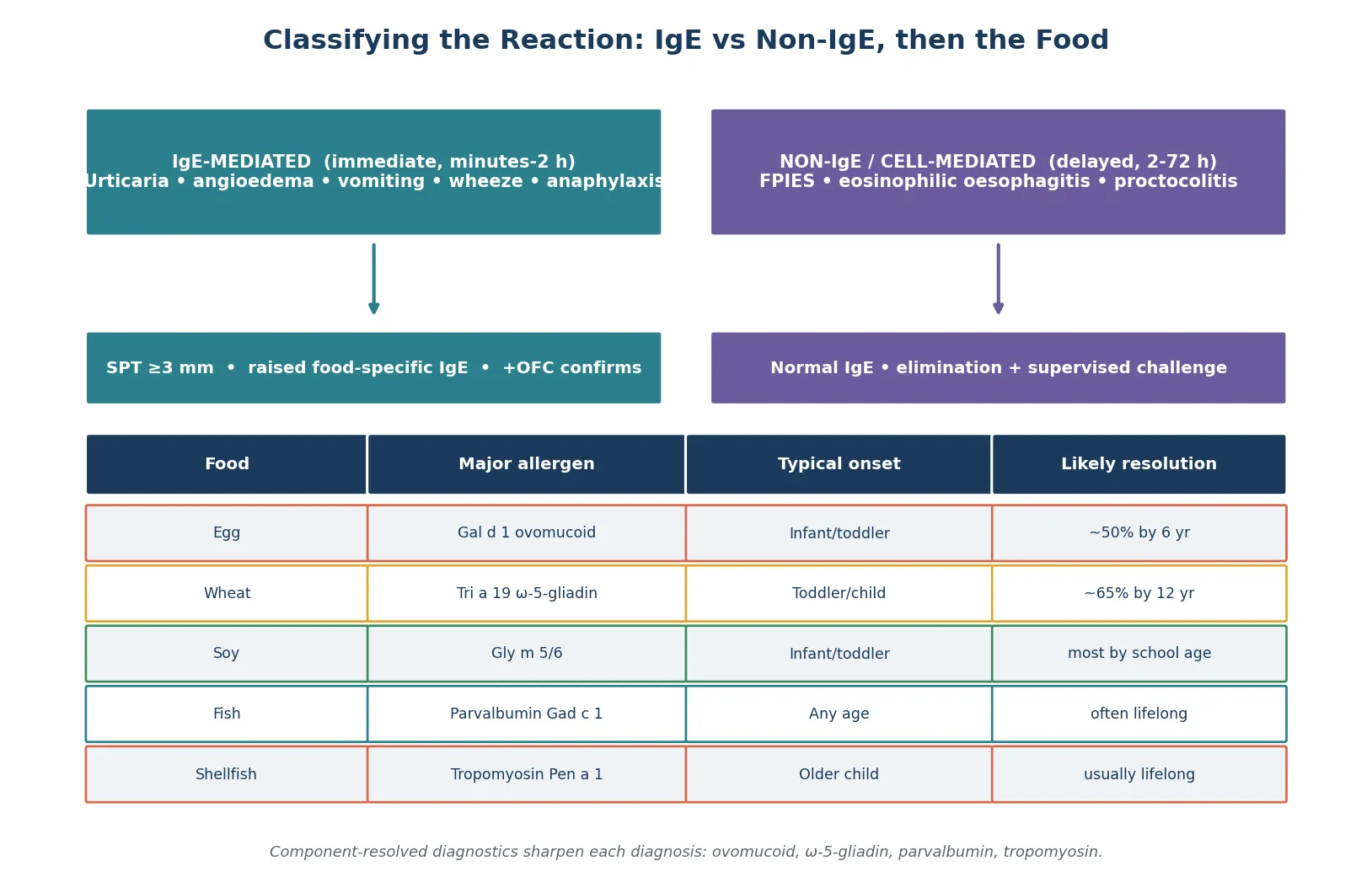
The second layer is the food itself and its dominant allergen. Each of the five foods owes its reactivity to a named protein whose heat-stability predicts how the child will react to cooked versus raw food. Egg reactivity centres on ovomucoid (Gal d 1), a heat-stable protein, and ovalbumin (Gal d 2), which is largely heat-labile; wheat immediate reactions are driven by omega-5-gliadin (Tri a 19); soy by the storage proteins Gly m 5 and Gly m 6; fish by parvalbumin (Gad c 1); and shellfish by tropomyosin (Pen a 1).[1]
The practical payoff of this classification is the baked-food question. A child whose allergy targets a heat-labile protein may tolerate the same food extensively baked — most famously the baked-egg and baked-milk ladders — whereas a child sensitised to a heat-stable protein such as parvalbumin or tropomyosin typically reacts to the food in every form, including well-cooked fish or shellfish.[14]
Epidemiology & Risk Factors
Egg allergy is the most common food allergy of early childhood after cow's milk. The HealthNuts population-based study in Melbourne used predetermined oral food challenge criteria in more than 2500 infants and found challenge-proven egg allergy in about 8.9 per cent of twelve-month-olds, a figure that transformed understanding of how common the condition really is when objectively confirmed rather than self-reported.[3]
Wheat, soy, fish and shellfish are less common in young children but each carries an epidemiological signature worth knowing. Wheat allergy affects roughly 0.1 to 1 per cent of children and tends to resolve, soy allergy is similarly uncommon and resolves early, while fish allergy (around 0.1 to 0.2 per cent) and shellfish allergy (up to around 2 per cent) are more prevalent in adults and, once established, often persist for life. Shellfish is in fact the most frequently reported food allergy in adults in the United States.[5]
The strongest risk factor for developing any food allergy is the presence of other atopic disease. Eczema in infancy, particularly early-onset moderate-to-severe eczema, markedly raises the risk of egg sensitisation and confirmed egg allergy, because inflamed skin allows allergen entry and the immune response that follows biases toward IgE production. The HealthNuts cohort confirmed that infants with early eczema had several-fold higher rates of challenge-proven egg allergy than those without.[15]
The strongest risk factor for a severe or fatal reaction once allergy is established is uncontrolled asthma. Children with food allergy and poorly controlled asthma carry the greatest risk of fatal food-induced anaphylaxis, a fact that makes asthma optimisation a core part of allergy management rather than a separate problem. Adolescents form the other high-risk group because of risk-taking behaviour, reluctance to carry an autoinjector, and away-from-home eating.[4]
Pathophysiology
IgE-mediated food allergy is a two-event disease, and understanding the two events makes both the diagnostic tests and the timing of reactions make sense. On first exposure, food protein taken up by antigen-presenting cells in the gut is presented to naive T cells, which under atopic conditions skew toward a T-helper-2 phenotype; the cytokines interleukin-4 and interleukin-13 then drive B-cell class-switching to IgE. The IgE binds to high-affinity Fc-epsilon receptors on mast cells and basophils, and the child is now sensitised without ever having had symptoms.[1]
The second event is re-exposure. When the same protein crosses the mucosa again, it cross-links adjacent IgE molecules on the mast-cell surface, triggering degranulation and the release of histamine, leukotrienes, prostaglandins and tryptase. These mediators produce the clinical phenotype within minutes to two hours: urticaria and angioedema in skin, vomiting and cramping in gut, wheeze and stridor in airway, and hypotension and collapse in the cardiovascular system.[2]
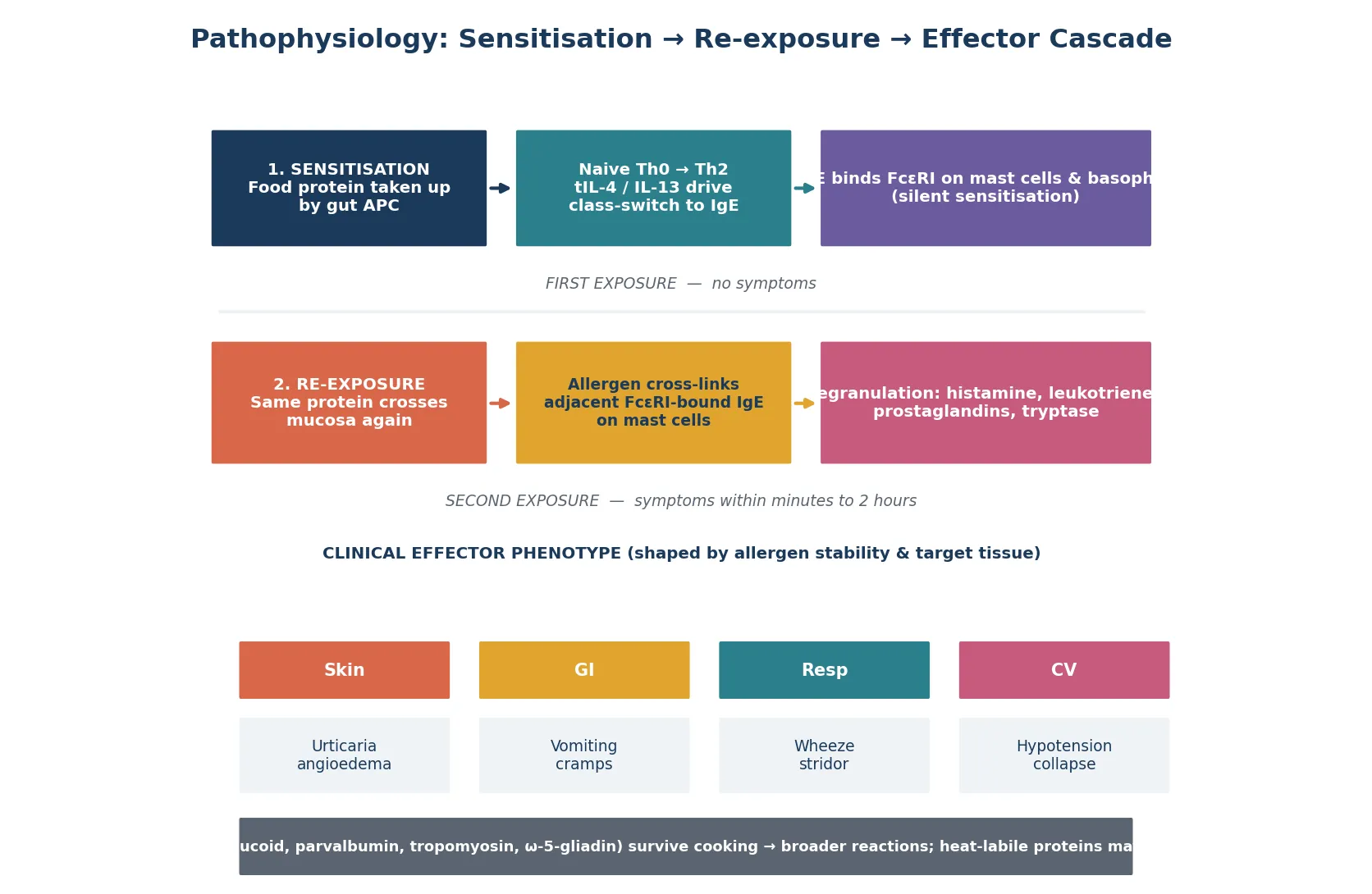
The heat-stability of the allergen protein governs whether cooking destroys it. Heat-labile proteins such as ovalbumin are largely destroyed by extensive baking, which is why many egg-allergic children tolerate egg in a cake or biscuit; heat-stable proteins such as ovomucoid, parvalbumin, tropomyosin and omega-5-gliadin survive cooking and provoke reactions to the food in any form. This single property explains both the baked-egg ladder and the persistence of fish and shellfish allergy.[14]
Non-IgE reactions follow a different mechanism. In FPIES, repeated exposure to a food protein such as egg, wheat or soy drives a T-cell-mediated response in the gut that, on re-exposure, produces delayed profuse vomiting, lethargy and pallor two to four hours later; in eosinophilic oesophagitis, chronic allergen exposure recruits eosinophils to the oesophageal mucosa, producing reflux-like symptoms, feeding difficulty and dysphagia. These reactions do not show on skin-prick or specific-IgE testing in the same way, which is the source of much diagnostic confusion.[4]
Clinical Presentation
A classic IgE-mediated reaction unfolds quickly and recognisably. Within minutes to two hours of eating the food, the child develops urticaria — raised, itchy, evanescent wheals that migrate — often with angioedema of the lips, periorbital tissue or face. Gastrointestinal symptoms of vomiting and abdominal cramping are common, and respiratory involvement shows as wheeze, stridor, cough or nasal congestion. The reaction can stall at the skin or escalate to anaphylaxis with hypotension, collapse and respiratory compromise.[2]
Each food has its own presentation patterns that an examiner will probe. Egg reactions most often begin in infancy through weaning or baked goods and classically involve the skin; wheat immediate reactions overlap but wheat is also the trigger for wheat-dependent exercise-induced anaphylaxis (WDEIA), in which collapse occurs during exercise one to four hours after wheat ingestion and is driven by omega-5-gliadin. Fish and shellfish reactions more often involve respiratory features and tend to be severe, because parvalbumin and tropomyosin are potent, heat-stable and cross-reactive across many species.[11]
The non-IgE presentations are different in tempo and demand a different line of questioning. FPIES produces delayed, repetitive vomiting with pallor and lethargy two to four hours after the food, sometimes progressing to dehydration and shock; there is no urticaria and no immediate collapse. Eosinophilic oesophagitis presents more insidiously with chronic reflux refractory to therapy, feeding aversion, vomiting and, in older children, food impaction. Food protein-induced proctocolitis presents as blood-streaked mucus stools in an otherwise well infant on a formula or breastfed diet containing the trigger.[4]
Atypical presentations deserve mention because examiners test them deliberately. A breastfed infant with eosinophilic proctocolitis reacts to trace protein in breastmilk; a child with oral allergy syndrome from soy cross-reacting with birch pollen (Gly m 4, a PR-10 protein) develops oral tingling with raw but not cooked soy; and a fish-allergic child may react to aerosolised allergen during fish cooking, a phenomenon that can mimic asthma. These atypical histories reward a careful food-and-symptom diary.[1]
Differential Diagnosis
The immediate-reaction differential turns on whether the symptom complex is allergic at all. Viral urticaria, which can last days and is non-migratory, serum-sickness-like reactions, contact urticaria from irritants, and histamine-releasing foods (such as strawberry or tomato) can all mimic IgE-mediated urticaria. The discriminating features are the timing (minutes to two hours), reproducibility, and the presence of a consistent food trigger confirmed on testing.[2]
For each food, specific non-allergic conditions enter the differential. Egg reactions must be separated from egg intolerance and from FPIES to egg; wheat allergy must be separated from coeliac disease (an autoimmune enteropathy against gluten, not an IgE reaction, with tissue transglutaminase antibodies and villous atrophy) and from non-coeliac gluten sensitivity; soy reactions overlap with soy-based formula intolerance; and fish reactions can be confused with scombroid fish poisoning, a histamine-mediated flushing reaction from spoiled dark-meat fish that responds to antihistamines rather than adrenaline.[11]
The delayed-GI-symptom differential is broad and includes gastroenteritis, intussusception, malrotation with volvulus, and metabolic causes of vomiting. FPIES is distinguished by its reproducibility on re-exposure to the same food, the absence of fever and diarrhoea in the acute episode, and the characteristic two-to-four-hour delay. A careful history of the timing relative to the food is the single most useful discriminator, and an elimination-and-supervised-reintroduction approach confirms the diagnosis.[4]
Clinical & Bedside Assessment
The history is the single most informative tool in food allergy, more than any single test. Build it around four questions: what exactly was eaten (read labels and recipes, ask about hidden ingredients such as egg as a glaze or fish sauce in a curry), how much was eaten, how quickly symptoms began, and what the symptoms were. A reproducible reaction within minutes to two hours of the same food, on more than one occasion, is highly suggestive of IgE-mediated allergy before any test is ordered.[13]
Examine for atopic stigmata and for signs of an acute reaction. Chronic eczema, particularly in the flexures, supports an atopic predisposition; look for current urticaria, angioedema, wheeze and signs of upper-airway obstruction if the child presents acutely. Between reactions the examination is often normal, which is itself an important finding — the absence of signs does not exclude allergy, because the reaction is provoked only on exposure.[2]
The synthesis for an exam long case is a one-sentence problem representation that names the trigger, the mechanism and the plan. A model statement is: "A two-year-old with moderate eczema who developed urticaria and vomiting twenty minutes after scrambled egg, with an egg-white specific IgE of 8 kU/L and a 5 mm skin-prick test, has IgE-mediated egg allergy and needs a baked-egg challenge, an ASCIA action plan, and a repeat specific-IgE trend to guide re-challenge timing." That sentence shows you have identified the food, classified the mechanism, and committed to a plan.[13]
The common assessment errors are worth naming because they cost marks and lives. Ordering a large screening panel of food-specific IgE tests without a matching history generates asymptomatic sensitisation and false-positive diets; failing to ask about exercise as a co-factor misses WDEIA; and accepting a parent's self-diagnosis of allergy without objective confirmation leads to unnecessary elimination diets and the nutritional and social harm that follow.[13]
Investigations
Skin-prick testing and serum food-specific IgE are the two front-line investigations, and neither alone confirms allergy — both measure sensitisation, which is the presence of IgE, not necessarily clinical reactivity. Skin-prick testing is cheap, rapid and performed on the volar forearm or back with commercial allergen extracts; a wheal of 3 mm or more above the negative control is positive. Serum food-specific IgE (ImmunoCAP) gives a quantitative result in kU per litre, and higher values carry a higher probability of true allergy for a given food.[2]
Component-resolved diagnostics sharpen the picture by measuring IgE against the individual allergen proteins rather than the whole-food extract. For egg, ovomucoid (Gal d 1) IgE predicts baked-egg reactivity and persistence better than whole-egg IgE; for wheat, omega-5-gliadin (Tri a 19) IgE identifies the WDEIA phenotype; and for fish and shellfish, parvalbumin and tropomyosin IgE confirm genuine allergy and predict cross-reactivity across species. This is the tool that moves a clinician from "egg allergic" to "ovomucoid-allergic and therefore likely baked-egg reactive and slower to resolve."[1]
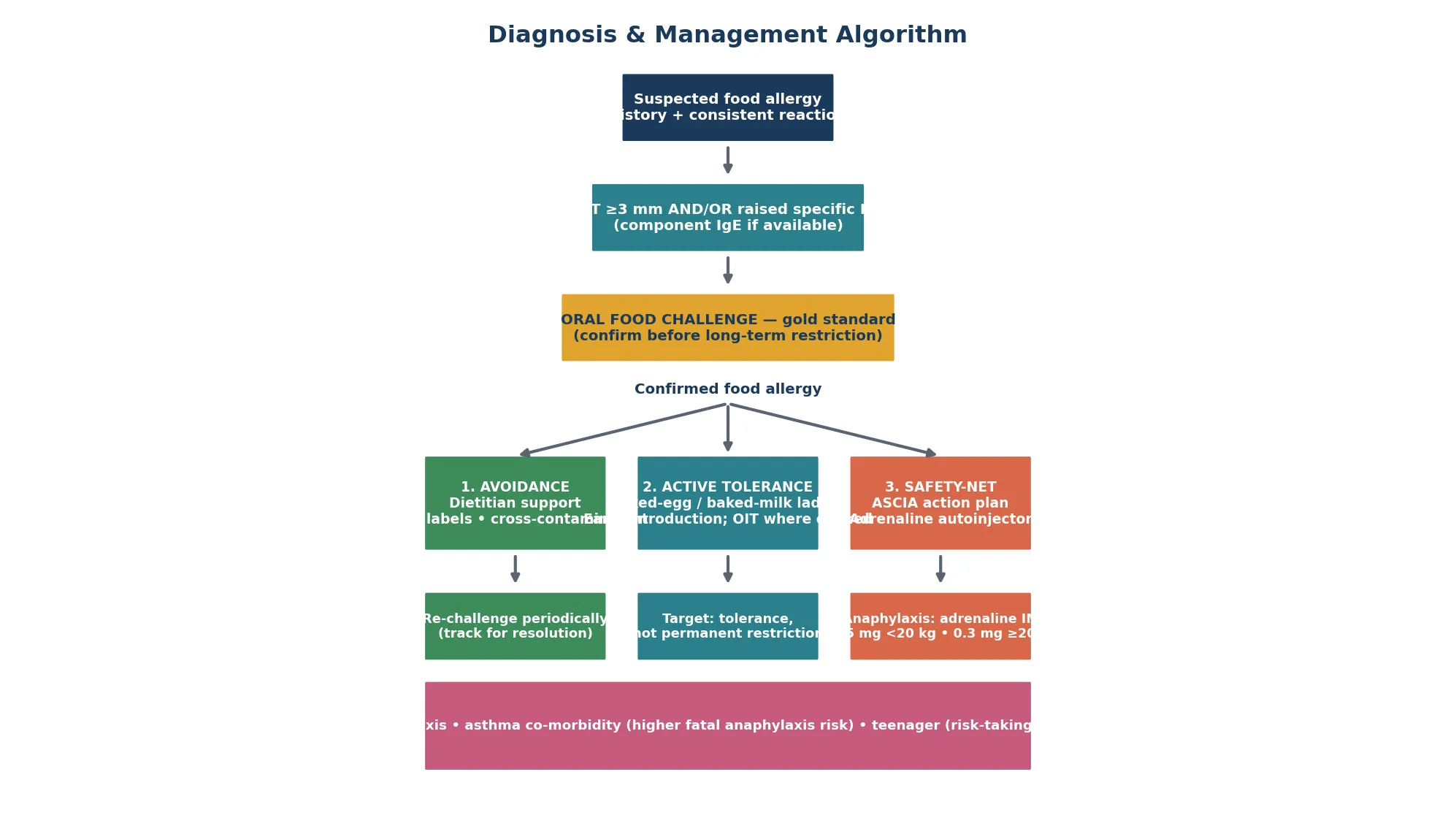
The oral food challenge is the gold standard and the only test that confirms clinical reactivity. It is performed under supervised medical supervision with incremental doses of the food, and it is indicated when the history and test results are inconclusive, when assessing whether a child has outgrown the allergy, or when introducing a baked-food ladder. The NIAID guidelines and the 2014 practice parameter both affirm the challenge as the reference standard, to be undertaken where resuscitation facilities are available.[13]
For non-IgE reactions the investigations differ. FPIES is confirmed by a consistent clinical history with resolution on elimination and recurrence on supervised oral challenge, with a normal specific-IgE and skin-prick test; eosinophilic oesophagitis requires upper endoscopy with biopsy showing 15 or more intraepithelial eosinophils per high-power field; and coeliac disease, the key wheat differential, is confirmed by tissue transglutaminase IgA in a child consuming gluten, with villous atrophy on biopsy. Choosing the right test for the suspected mechanism is the skill.[4]
Management — Resuscitation
The immediate priority in a child presenting with an acute allergic reaction is to recognise anaphylaxis and give adrenaline without delay. Anaphylaxis is defined by the rapid onset of skin or mucosal change together with respiratory compromise, hypotension, or gastrointestinal symptoms, or by involvement of two or more organ systems after a known allergen exposure. The treatment is intramuscular adrenaline into the anterolateral thigh, and the single most common error in fatal cases is delayed adrenaline.[2]
Dose adrenaline by weight. The standard weight-based intramuscular adrenaline dose is 0.01 mg per kilogram of 1:1000 adrenaline, with the practical autoinjector thresholds that the lower-dose device (0.15 mg) is used for children under 20 kg and the higher-dose device (0.3 mg) for children of 20 kg and over; repeat after five minutes if there is no response. Position the child supine with legs raised if hypotensive, give high-flow oxygen and intravenous fluid for shock, and arrange transfer to hospital because a biphasic reaction can recur four to thirty hours later.[2]
Adrenaline (intramuscular)
Dose
0.01 mg/kg of 1:1000 (1 mg/mL)
Adjuncts have a clear but secondary role. Antihistamines relieve urticaria and itch but do not treat airway, breathing or circulation compromise and must never delay adrenaline; bronchodilators treat persistent bronchospasm; corticosteroids have no role in the acute episode but are sometimes given to reduce the risk of a biphasic reaction, though evidence for this is limited. Fluid boluses of 10 mL per kilogram of isotonic crystalloid support the circulation in shock alongside adrenaline.[2]
After the acute episode the child must be observed, because a biphasic reaction — a recurrence of anaphylaxis without re-exposure — occurs in up to 5 to 15 per cent of cases, typically within hours of the first reaction but occasionally much later. A child treated for food-induced anaphylaxis needs a minimum observation period, an adrenaline autoinjector prescribed before discharge, training in its use, a written action plan, and follow-up with an allergy service.[13]
Management — Definitive & Stepwise
The long-term management of a confirmed food allergy rests on three pillars: allergen avoidance with dietetic support, active tolerance induction where appropriate, and a safety-net of an action plan and adrenaline. Avoidance sounds simple but is demanding in practice — it requires label-reading for hidden ingredients (egg as a glaze or binder, wheat in sauces, fish sauce in Asian cooking, soy in processed foods), attention to cross-contamination in shared kitchens and restaurants, and a dietetic review to ensure nutritional adequacy, particularly calcium, protein and energy when multiple foods are removed.[2]
Active tolerance induction is the modern frontier and is particularly relevant to egg. The baked-egg ladder introduces extensively heated egg in a matrix such as a well-baked cake or muffin, exploiting the heat-lability of ovalbumin; children who tolerate baked egg consume it regularly and many then progress toward tolerance of less-cooked egg over months to years, with cohort data suggesting that baked-egg consumption accelerates tolerance compared with strict avoidance. The same principle underpins the baked-milk ladder. Oral immunotherapy, validated most strongly for peanut by the PALISADE trial of AR101, is being extended to egg and other foods in specialist centres but remains a specialist, supervised intervention, not a routine community treatment.[14]
Confirm allergy
History + SPT/IgE; oral food challenge if doubt
Baked-food challenge
Supervised challenge to baked egg or wheat in matrix
Regular baked-food intake
If tolerated, daily baked food to build tolerance
Progress ladder
Advance to less-heated forms under guidance
Periodic re-assessment
Trend specific IgE and re-challenge to test for resolution
The safety-net pillar is non-negotiable for any child with a confirmed IgE-mediated allergy. Every such child needs a written, personalised anaphylaxis action plan — in Australasia the ASCIA action plan, in the United Kingdom the equivalent BSACI plan — and an adrenaline autoinjector prescribed if there is any history of a systemic reaction or if the child has asthma. Training the family, the child (age-appropriately), the school and any carers in autoinjector use and in recognising the early signs of a reaction is part of medical management, not an optional extra.[2]
Specific Subtypes & Scenarios
Egg allergy dominates paediatric practice and carries the richest management pathway. The HealthNuts cohort demonstrated that about half of children with challenge-proven egg allergy at age one had resolved by age six, and that resolution is faster in children who tolerate baked egg early. A child with a low or falling egg-white specific IgE, a small skin-prick wheal, and tolerance of baked egg is a strong candidate for a supervised challenge to assess resolution; a child with high ovomucoid IgE is more likely to be persistent and baked-egg reactive.[10]
Wheat allergy presents in three phenotypes that an examiner will ask you to separate. The most common is IgE-mediated immediate wheat allergy of childhood, which usually resolves by adolescence; the second is wheat-dependent exercise-induced anaphylaxis, an adolescent-or-adult phenotype driven by omega-5-gliadin and unmasked by exercise; the third is the non-IgE spectrum of eosinophilic oesophagitis and FPIES, both of which can be triggered by wheat. The Keet cohort found that about 65 per cent of wheat allergy resolved by twelve years.[7]
Soy allergy is characterised by early onset and early resolution. It is frequently seen in infants who react to soy-based formula or to soy introduced at weaning, and the natural-history study from Savage and colleagues found that approximately half of soy allergy had resolved by one year and that most children had outgrown it by school age. A particular trap is the Gly m 4 cross-reactivity with birch pollen, which produces oral symptoms with raw but not cooked soy in birch-sensitised children, a phenotype distinct from systemic soy allergy to storage proteins.[6]
Fish and shellfish allergy share the properties of heat-stable major allergens, broad cross-reactivity and a tendency to persist, but they differ in epidemiology and presentation. Fish allergy, driven by parvalbumin, often begins at any age and frequently persists; cross-reactivity across bony fish species means a child reactive to one fish is often reactive to others, though some tolerate certain species. Shellfish allergy, driven by tropomyosin, is the most common food allergy in adults, can involve both crustaceans and molluscs, and has a distinctive cross-reactivity with dust-mite tropomyosin — the "mite-shrimp syndrome" — in which a dust-mite-sensitised child reacts to shellfish on first exposure.[5]
[2]Complications & Pitfalls
Anaphylaxis is the most feared acute complication, and fatal food-induced anaphylaxis is concentrated in adolescents and young adults with known food allergy and co-existing asthma. The lessons from the fatal-case series are consistent: delayed adrenaline is the recurring theme, often compounded by asthma being treated with bronchodilators while the underlying anaphylaxis is missed, and by the absence or non-use of an adrenaline autoinjector. Optimising asthma control and ensuring the child and carers carry and can use the device are the two interventions that save lives.[4]
Nutritional and growth complications arise from unnecessary or over-broad elimination diets. Removing egg, wheat and soy simultaneously — or adding fish and shellfish — risks deficiency of protein, calcium, iron, energy and B vitamins, and children on multiple food restrictions need dietetic input and growth monitoring. The pitfall is the self-imposed or panel-driven diet that removes foods a child tolerates, based on sensitisation rather than confirmed clinical allergy; the corrective is to prove each allergy by challenge before restricting it long-term.[13]
The quality-of-life burden is substantial and under-recognised. Food allergy produces anxiety around eating, social isolation at school and restaurants, bullying, and parental hypervigilance, and adolescents in particular may engage in risk-taking such as not carrying the autoinjector or eating the food to "test" themselves. Addressing these in clinic, with an action plan the child understands and psychology support where needed, is part of definitive management.[1]
Specific food pitfalls deserve memorising. Egg can hide as a glaze on pastry or as lecithin (though lecithin is usually tolerated); wheat appears in sauces, soups and processed meats and is the WDEIA trigger; soy is ubiquitous in processed food and infant formula; fish allergen can aerosolise during cooking and contaminate shared oil; and shellfish shares tropomyosin with dust mite, producing unexpected first-exposure reactions. Each of these is a known exam stem.[11]
Prognosis & Disposition
The prognosis separates the five foods into two groups, and this distinction is the single most testable prognostic fact in the topic. Egg, wheat and soy are predominantly childhood allergies that usually resolve — about half of egg allergy clears by age six, about two-thirds of wheat allergy by adolescence, and most soy allergy by school age — whereas fish and shellfish allergy, once established, often persist for life. The practical consequence is that egg, wheat and soy warrant periodic re-testing and re-challenge to detect resolution, while fish and shellfish management is built around lifelong avoidance and safety-netting.[4]
For egg allergy specifically, the HealthNuts longitudinal data provide the modern reference. Peters and colleagues followed the population-based cohort to age six and confirmed that roughly half of challenge-confirmed egg allergy at age one had resolved, with baked-egg tolerance an early marker of the resolving group. The predictors of persistence are a larger skin-prick wheal, a higher egg-white specific IgE, and high ovomucoid IgE; these markers guide the timing of re-challenge.[10]
Disposition from an acute reaction depends on severity. Any child treated with adrenaline for anaphylaxis needs hospital observation for the biphasic window and discharge with an autoinjector, action plan and allergy follow-up. A child with a mild cutaneous reaction that settles can be observed and followed up in the community with testing and a plan. The long-term disposition is a structured allergy service that conducts periodic re-assessment, supervises challenges and baked-food ladders, and coordinates the school and family education.[13]
Special Populations
Infants and toddlers carry the highest burden of egg, wheat and soy allergy, and they are also the group most vulnerable to the nutritional effects of elimination. A young child on an egg-, wheat- and soy-free diet needs dietetic review for energy, protein, iron and calcium adequacy, and growth should be plotted at every visit. Early introduction of allergenic foods around six months, supported by the LEAP trial's demonstration that early peanut consumption prevents peanut allergy, has shifted practice toward early introduction of egg as well, under supervision for high-risk infants.[16]
Adolescents are the highest-risk group for fatal food-induced anaphylaxis because of risk-taking behaviour, inconsistent autoinjector carriage, away-from-home eating, and alcohol as a co-factor. The consultation with an allergic adolescent should explicitly address transition — ensuring the young person knows their allergens, carries and can use the autoinjector, reads labels, and has a plan for restaurants, parties and travel. Confidentiality, non-judgement and a written plan the adolescent owns are the tools.[4]
Children with disability and neurodiversity, and those with complex chronic or technology-dependent conditions, face additional barriers: restricted diets related to sensory selectivity, difficulty communicating early symptoms, and carers who may change shift. These children need an individualised action plan shared with all carers, attention to nutritional adequacy, and extra time for education. Migrant, refugee and asylum-seeker families may face language, labelling and access barriers, and an interpreter, written translated materials and a clearly explained action plan are essential.[13]
Children in out-of-home care and those from socioeconomically disadvantaged backgrounds may have inconsistent access to autoinjectors, school staff training, and specialist follow-up. The safeguarding question is whether the child's allergy management is supported across all their placements, and whether the autoinjector travels with the child. Social prescribing and advocacy for funded autoinjectors and dietetic support form part of equitable allergy care.[2]
Evidence, Guidelines & Regional Differences
The 2010 NIAID-sponsored expert-panel guidelines and the 2014 practice-parameter update remain the foundational documents for the diagnosis and management of food allergy, establishing the definitions, the role of skin-prick and specific-IgE testing, the oral food challenge as the gold standard, and the adrenaline-first treatment of anaphylaxis. The 2014 Sicherer and Sampson review synthesised the epidemiology, pathogenesis and treatment into the canonical reference that most contemporary guidance builds on.[1]
The natural-history evidence base is anchored by population-based cohorts. The HealthNuts study in Melbourne used predetermined challenge criteria in a population sample and established the true prevalence of egg allergy in infancy, and its longitudinal follow-up by Peters and colleagues to age six defined the resolution rates and predictors. The natural-history cohorts from Keet (wheat), Savage (soy) and Sicherer (egg) provided the resolution rates that guide re-challenge timing for each food.[4]
The prevention paradigm was transformed by the LEAP trial, which showed that early peanut consumption in high-risk infants reduced peanut allergy by about 80 per cent, prompting the 2017 NIAID addendum guidelines recommending early peanut introduction. The same principle of early introduction has been extended toward egg, though the evidence for egg is less conclusive than for peanut and supplementation with early cooked egg remains under guidance rather than mandate.[12]
Exam Pearls
Carry these single-testable facts into the written and clinical exam. Egg, wheat and soy are usually outgrown; fish and shellfish usually persist. The signature allergens are ovomucoid (egg), omega-5-gliadin (wheat), Gly m 5 and 6 (soy), parvalbumin (fish) and tropomyosin (shellfish). Heat-stable proteins (ovomucoid, parvalbumin, tropomyosin, omega-5-gliadin) survive cooking; heat-labile proteins may be tolerated baked. Skin-prick threshold is 3 mm; the oral food challenge is the gold standard.[1]
The five foods and their signature allergens — 'OWSFS'
Anaphylaxis treatment is intramuscular adrenaline into the anterolateral thigh, dosed 0.15 mg under 20 kg and 0.3 mg for 20 kg and over, repeated after five minutes. The single biggest error is delayed adrenaline, and the single biggest risk factor for fatal anaphylaxis is uncontrolled asthma. Antihistamines treat itch only and never substitute for adrenaline in anaphylaxis. Wheat-dependent exercise-induced anaphylaxis is omega-5-gliadin-driven and unmasked by exercise.[2]
Finally, the differential traps that examiners set: coeliac disease is autoimmune against gluten (tissue transglutaminase, not IgE); FPIES is cell-mediated and delayed; scombroid poisoning is histamine from spoiled fish and responds to antihistamines; and the over-interpreted screening panel produces asymptomatic sensitisation and harmful elimination diets. Knowing the mechanism of each condition is the key to choosing the right test and the right diet.[11]
References
- [1]Sicherer SH, Sampson HA Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol, 2014.PMID 24388012
- [2]Boyce JA, Assa'ad A, Burks AW, et al. Guidelines for the diagnosis and management of food allergy in the United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol, 2010.PMID 21134576
- [3]Osborne NJ, Koplin JJ, Martin PE, et al. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants. J Allergy Clin Immunol, 2011.PMID 21377036
- [4]Savage J, Sicherer S, Wood R The Natural History of Food Allergy. J Allergy Clin Immunol Pract, 2016.PMID 26968958
- [5]Sicherer SH, Munoz-Furlong A, Sampson HA Prevalence of seafood allergy in the United States determined by a random telephone survey. J Allergy Clin Immunol, 2004.PMID 15241360
- [6]Savage JH, Kaeding AJ, Matsui EC, Wood RA The natural history of soy allergy. J Allergy Clin Immunol, 2010.PMID 20226303
- [7]Keet CA, Matsui EC, Duguay G, Raha R, Lange L, Wood RA The natural history of wheat allergy. Ann Allergy Asthma Immunol, 2009.PMID 19492663
- [8]Savage JH, Courneya JP, Sterba PM, Macglashan DW, Saini SS, Wood RA The natural history of egg allergy in an observational cohort. J Allergy Clin Immunol, 2014.PMID 24636473
- [9]Peters RL, Dharmage SC, Gurrin LC, et al. The natural history and clinical predictors of egg allergy in the first 2 years of life: a prospective, population-based cohort study (HealthNuts). J Allergy Clin Immunol, 2014.PMID 24373356
- [10]Peters RL, Koplin JJ, Gurrin LC, et al. The natural history of peanut and egg allergy in children up to age 6 years in the HealthNuts population-based longitudinal study. J Allergy Clin Immunol, 2022.PMID 35597613
- [11]Cianferoni A Wheat allergy: diagnosis and management. J Asthma Allergy, 2016.PMID 26889090
- [12]Togias A, Cooper SF, Acebal ML, et al. Addendum guidelines for the prevention of peanut allergy in the United States: Report of the National Institute of Allergy and Infectious Diseases-sponsored expert panel. J Allergy Clin Immunol, 2017.PMID 28065278
- [13]Sampson HA, Aceves S, Bock SA, et al. Food allergy: a practice parameter update-2014. J Allergy Clin Immunol, 2014.PMID 25174862
- [14]Leonard SA Baked Egg and Milk Exposure as Immunotherapy in Food Allergy. Curr Allergy Asthma Rep, 2016.PMID 27002516
- [15]Koplin JJ, Peters RL, Allen KJ, et al. Cohort Profile: The HealthNuts Study: Population prevalence and environmental/genetic predictors of food allergy. Int J Epidemiol, 2015.PMID 25613427
- [16]Du Toit G, Roberts G, Sayre PH, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med, 2015.PMID 25705822