Paeds · allergy-and-immunology
Food allergy diagnosis and oral food challenge
Also known as Food allergy testing · Oral food challenge · DBPCFC · Food allergy workup · Component-resolved diagnostics
A fellowship-level approach to diagnosing food allergy in children: taking a structured reaction history, interpreting skin prick tests and serum specific IgE with their 95% predictive thresholds, using component-resolved diagnostics to refine risk, performing oral food challenge safely, and avoiding the harm of overdiagnosis from indiscriminate allergy panels.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Food allergy is one of the most common chronic conditions of childhood and one of the most frequently overdiagnosed. The diagnostic challenge is not detecting sensitisation — modern tests do that easily — but separating the child who will react on ingestion from the child who will not. A clinical history that does not fit the test result, or a test result without a supporting history, is the single most common reason for unnecessary dietary restriction, anxiety, and impaired quality of life. The paediatrician who masters the diagnostic pathway protects children both from the danger of a missed allergy and from the harm of a false label. [2]
This topic covers the full diagnostic journey: defining and classifying food allergic reactions, interpreting SPT and serum specific IgE with their predictive thresholds, applying component-resolved diagnostics, performing the oral food challenge safely, and navigating the regional guideline landscape from the NIAID consensus to the BSACI and ASCIA frameworks. [1][2]
Overview & Definition
A food allergy is an adverse health effect arising from a specific immune response that occurs reproducibly on exposure to a given food. The critical word is immune: this separates food allergy from food intolerance, which is a non-immunological adverse reaction (for example, lactose intolerance from lactase deficiency), and from toxic reactions (for example, scombroid fish poisoning from histamine). [1]
The NIAID-sponsored expert panel defined food allergy as "an adverse health effect arising from a specific immune response that occurs reproducibly on exposure to a given food," and the DBPCFC (double-blind placebo-controlled food challenge) as the gold standard for confirming it. Not every food-related symptom is an allergy; not every positive test means a clinical allergy exists. [1][2]
The diagnostic process follows a logical chain: first, does the history sound like an allergic reaction? Second, does testing show sensitisation to the implicated food? Third, when history and testing are discordant or inconclusive, does an oral food challenge reproduce symptoms under controlled conditions? Each step has a distinct evidentiary weight, and the paediatrician's job is to integrate them rather than rely on any single test in isolation. [5]
Classification
Food allergic reactions are classified by the immune mechanism driving them, because mechanism determines timing, clinical phenotype, and the appropriate diagnostic strategy. [1]
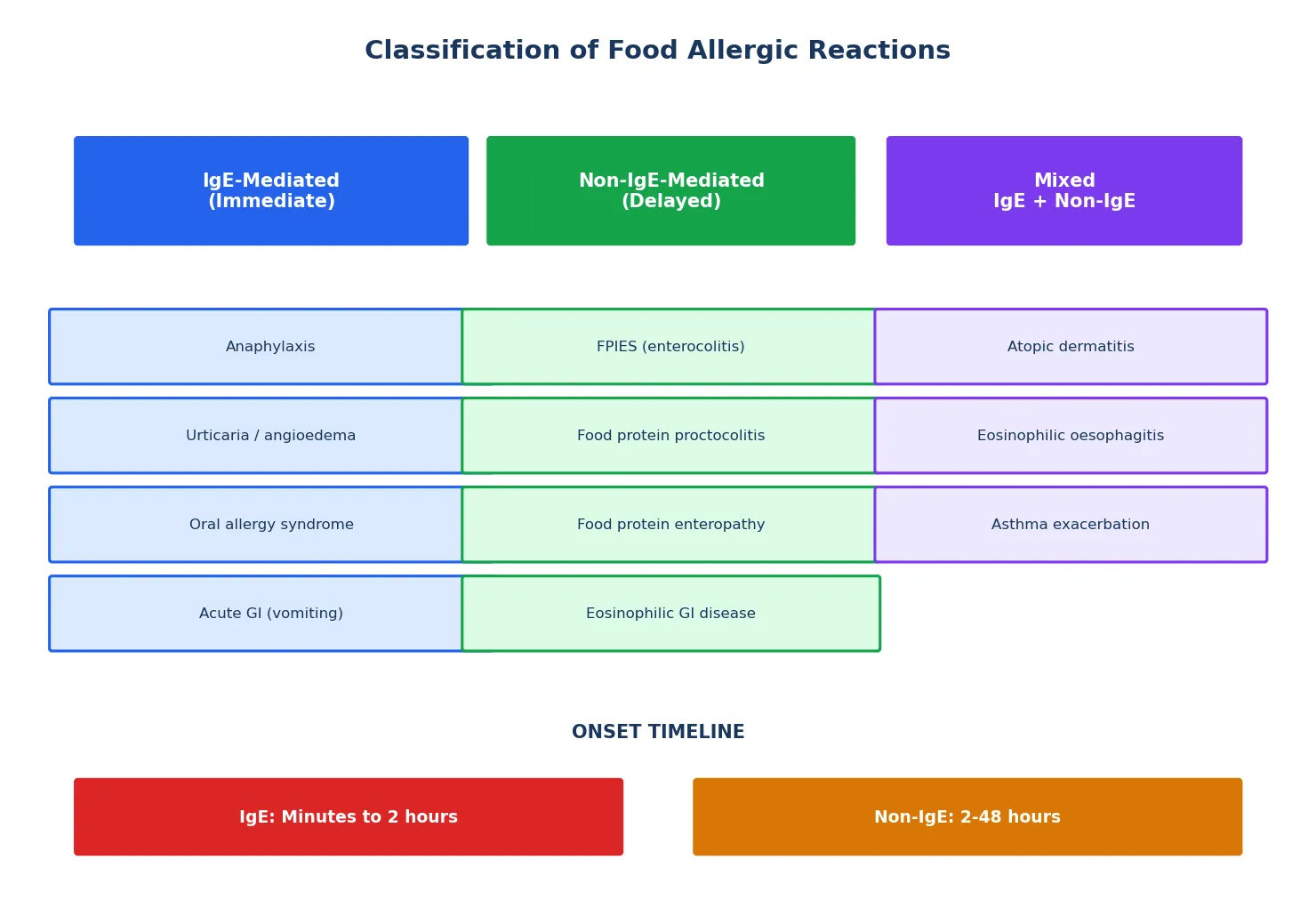
The IgE-mediated category is where SPT and specific IgE testing are most useful, and where the oral food challenge provides definitive confirmation. Non-IgE-mediated reactions — particularly FPIES — require a fundamentally different diagnostic approach: elimination followed by supervised re-challenge, with skin testing typically negative. The mixed category, encompassing atopic dermatitis and eosinophilic oesophagitis, is the most complex, because food triggers contribute to chronic inflammation but cannot be reliably identified by SPT or IgE alone. [1][12]
Epidemiology & Risk Factors
Food allergy is common, and its prevalence has risen significantly over the past two decades. The landmark Australian HealthNuts cohort study provided the first large-scale, challenge-proven prevalence data: among 12-month-old infants, challenge-proven peanut allergy affected approximately 3%, raw egg allergy approximately 9%, and sesame allergy approximately 0.8%. These figures, based on OFC rather than self-report or sensitisation alone, are substantially higher than older estimates and have been replicated across other populations. [8][11]
The European systematic review and meta-analysis by Spolidoro et al. (2023) confirmed that the "big eight" food allergens — cow's milk, egg, wheat, soy, peanut, tree nuts, fish, and shellfish — account for the vast majority of clinical food allergy, with cow's milk and egg being the most prevalent in young children and peanut, tree nuts, and seafood predominating in older children and adults. Regional variation is notable, reflecting dietary patterns and environmental exposures. [11]
The major risk factors for developing food allergy are well established. Severe atopic dermatitis in infancy is the strongest single predictor — the dual-allergen-exposure hypothesis proposes that cutaneous sensitisation through disrupted skin barrier precedes and predisposes to clinical allergy. A family history of atopy (parent or sibling with allergy, asthma, eczema, or allergic rhinitis) increases risk, as does early sensitisation detected on screening of high-risk infants. [2][6]
Pathophysiology
IgE-mediated food allergy develops in two phases: sensitisation and elicitation. Understanding both phases is essential for interpreting diagnostic tests correctly, because the tests detect the product of sensitisation (allergen-specific IgE on mast cells or in serum) but cannot, on their own, determine whether elicitation will occur on ingestion. [2]
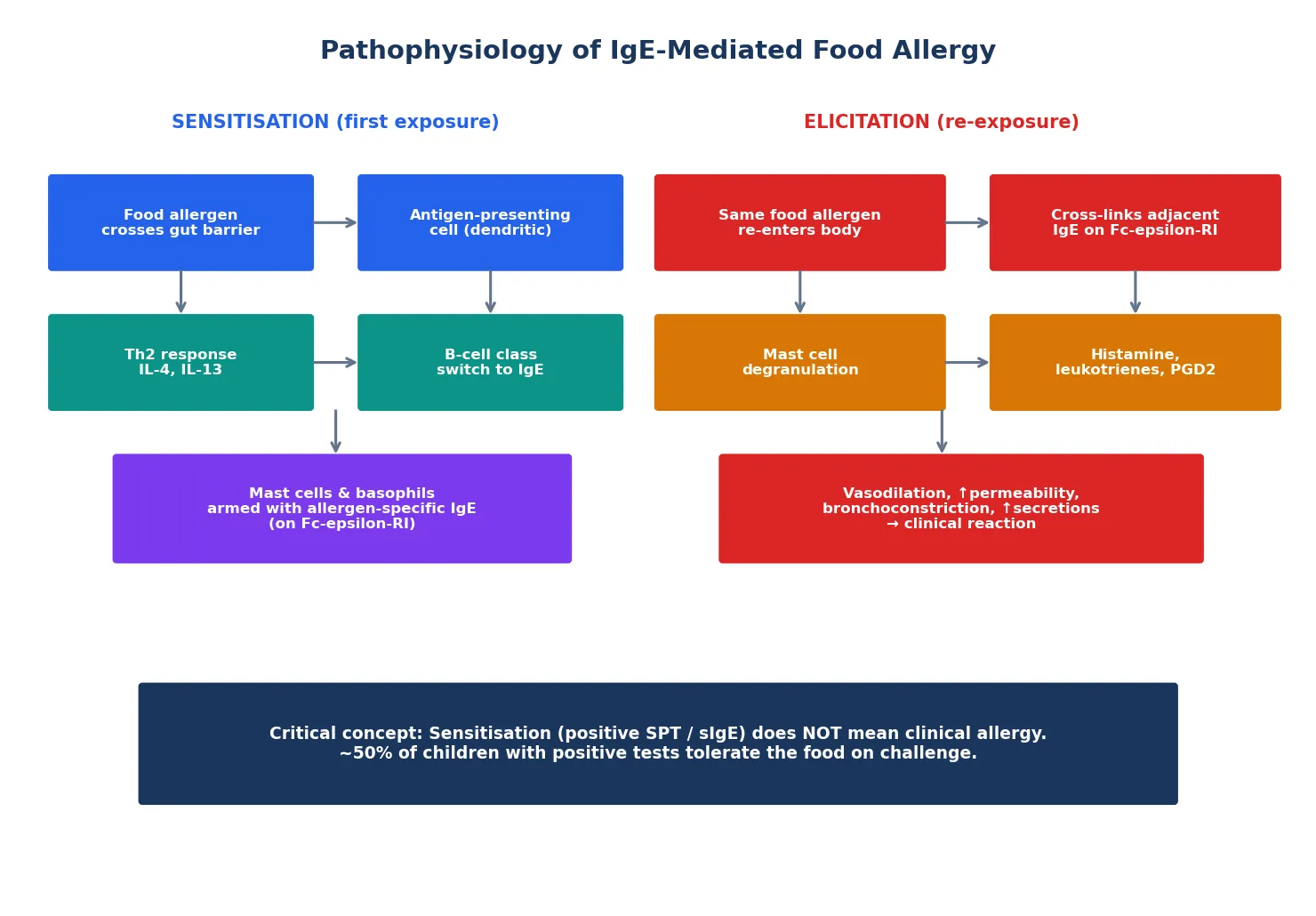
In the sensitisation phase, a food protein (the allergen) crosses the gut mucosal barrier and is taken up by antigen-presenting cells, particularly dendritic cells. These cells present allergen-derived peptides to naïve T-helper cells, skewing them toward a Th2 phenotype under the influence of cytokines such as IL-4 and IL-13. Th2 cells then direct B-cells to undergo class switching from IgM to IgE production specific to that food allergen. The resulting allergen-specific IgE binds to high-affinity Fc-epsilon-RI receptors on the surface of mast cells (in tissues) and basophils (in circulation). At this point, the child is sensitised — they have allergen-specific IgE detectable by SPT or serum testing — but may or may not react on ingestion. [2]
In the elicitation phase, re-exposure to the same food allergen causes it to cross-link adjacent allergen-specific IgE molecules on the mast cell surface. This cross-linking triggers mast-cell degranulation, releasing preformed mediators (histamine, tryptase, chymase) and generating newly synthesised mediators (leukotrienes, prostaglandin D2, platelet-activating factor). These mediators produce the clinical signs: vasodilation and increased vascular permeability (urticaria, angioedema, hypotension), bronchoconstriction (wheeze), increased mucus secretion (rhinitis), and smooth muscle contraction (cramping, vomiting, diarrhoea). The reaction typically begins within minutes of ingestion and peaks within 30 to 60 minutes. [2]
The critical insight for diagnosis is this: sensitisation is not allergy. Approximately 50% of children with a positive SPT or elevated serum specific IgE will tolerate the food without any reaction on oral food challenge. This is why testing without a supporting clinical history — the notorious "food allergy panel" — generates false positives that lead to unnecessary dietary avoidance, nutritional compromise, and psychological burden. [5]
Component-resolved diagnostics exploits the fact that food allergens are composed of multiple individual proteins (components), each with different clinical significance. For peanut, the component Ara h 2 (a 2S albumin storage protein) is strongly associated with systemic IgE-mediated reactions and has far higher diagnostic accuracy for clinical peanut allergy than whole-peanut extract IgE. The component Ara h 8 (a Bet v 1-homologue) cross-reacts with birch pollen and typically produces only oral allergy syndrome. This distinction explains why some children have large SPT wheals to whole peanut extract but tolerate peanut on challenge — they are sensitised to a cross-reactive component that does not cause systemic allergy. [2][5]
Clinical Presentation
A food allergic reaction can involve any combination of skin, gastrointestinal, respiratory, and cardiovascular systems. The clinical history is the single most important diagnostic tool — more so than any laboratory test — because it establishes whether the presentation is consistent with an IgE-mediated reaction at all, and whether the timing, dose, and reproducibility fit an allergic mechanism. [1][2]
IgE-mediated reactions are characterised by four history features: onset within minutes to two hours of ingestion, reproducibility (the reaction recurs on each exposure), a dose-dependent relationship (larger amounts tend to produce more severe reactions, though this is not absolute), and a constellation of symptoms involving at least one organ system. Typical IgE-mediated symptoms include urticaria, angioedema, pruritus, vomiting, abdominal pain, wheeze, stridor, cough, rhinitis, and — in anaphylaxis — hypotension and collapse. [1]
Non-IgE-mediated reactions present differently and are easily missed. FPIES (food protein-induced enterocolitis syndrome) produces delayed, profuse projectile vomiting 1 to 4 hours after ingestion, often with lethargy and pallor, and can mimic sepsis. Food protein proctocolitis presents with blood-streaked mucous stools in an otherwise well-appearing infant. Eosinophilic oesophagitis produces chronic dysphagia, food impaction, reflux unresponsive to proton pump inhibitors, and feeding difficulty. None of these conditions will reliably show positive SPT or specific IgE, and the history of delayed onset and chronicity is the key diagnostic clue. [12]
Atypical presentations deserve specific mention. Food-dependent exercise-induced anaphylaxis requires both food ingestion and exercise within a few hours to trigger a reaction, and the food is tolerated when the child is sedentary. Pollen-food (oral allergy) syndrome produces isolated oral itching and mild angioedema confined to the oropharynx, typically with raw fruits and vegetables in a child with pollen allergy; cooked forms are tolerated because heat denatures the cross-reactive proteins. These patterns are identified from the history, not from testing alone, and they change both the diagnostic and management strategy. [2]
Differential Diagnosis
The differential diagnosis of a suspected food allergic reaction is broad, and distinguishing mimics is essential to avoid both overdiagnosis and missed alternative diagnoses. [2]
The most dangerous diagnostic error is mistaking FPIES for sepsis — the profuse, delayed vomiting with lethargy and pallor can send a child down an aggressive intravenous antibiotic pathway before the dietary trigger is recognised. Conversely, mistaking sepsis for an allergic reaction delays life-saving antibiotic therapy. The history of food ingestion, the delay to onset, and the absence of fever are the key discriminators. [12]
A second dangerous error is mislabelling a vasovagal episode as anaphylaxis. Vasovagal syncope produces pallor, hypotension, and loss of consciousness — superficially resembling anaphylaxis — but lacks urticaria, pruritus, stridor, and bronchospasm, and the patient is typically bradycardic rather than tachycardic. The distinction matters because a food allergy label carries lifelong dietary and psychosocial consequences. [2]
Clinical & Bedside Assessment
The clinical assessment of a child with suspected food allergy begins and ends with the history. The physical examination, while important, rarely makes or breaks the diagnosis in isolation — its primary roles are to assess growth and nutritional status, identify signs of comorbid atopic disease, and exclude alternative diagnoses. [1]
Growth assessment is essential because dietary restriction imposed on the basis of a false positive test can cause faltering growth, calcium and vitamin D deficiency (from milk avoidance), and protein-calorie inadequacy (from multiple food avoidance). Every child with a food allergy label should have height and weight plotted on age-appropriate centile charts, and any downward trajectory should prompt urgent nutritional review. [5]
Atopic dermatitis severity should be assessed using a validated tool (SCORAD or EASI) because moderate-to-severe eczema is both the strongest risk factor for food sensitisation and a potential target for prevention strategies. The dual-allergen-exposure hypothesis proposes that early cutaneous exposure to food allergens through disrupted skin barrier drives Th2 skewing and IgE sensitisation, while early oral exposure promotes tolerance. This is the biological basis for the LEAP trial finding that early peanut introduction prevents allergy in high-risk infants. [3][6]
The skin examination should look for urticaria (distinguish from viral exanthem and dermatographism), angioedema (distinguish from hereditary angioedema by history and complement testing), and signs of chronic atopic dermatitis. The respiratory examination assesses for current wheeze and airway obstruction. The abdominal examination may reveal distension or tenderness suggesting a non-IgE-mediated GI process. [1]
Investigations
The diagnostic investigation of suspected food allergy proceeds in a structured, stepwise fashion. The principle is that no test should be ordered without a clinical history to direct it, and that each test has well-defined predictive values that must be interpreted in context. [1][5]
Skin Prick Test (SPT)
The skin prick test introduces a small amount of allergen extract into the epidermis using a lancet or prick device. If allergen-specific IgE is present on cutaneous mast cells, a wheal-and-flare reaction develops within 15 to 20 minutes. SPT is inexpensive, rapid, and has a high negative predictive value (a negative test makes clinical IgE-mediated allergy unlikely). However, its positive predictive value is modest — many sensitised children will tolerate the food. [1]
The SPT is interpreted by measuring the wheal diameter (the longest diameter plus the perpendicular diameter divided by two). The 95% positive predictive value (PPV) thresholds — the wheal size above which approximately 95% of children will react on challenge — have been established for common allergens. For peanut in young children, a wheal diameter of 8 mm or greater carries a 95% PPV; for egg, 7 mm; for cow's milk, 4 mm (in infants) to 8 mm (in older children). Wheal sizes of 3 mm or greater than the negative control are considered positive, but a 3-4 mm wheal has poor specificity for clinical allergy. [1][5]
Antihistamines must be withheld for 5 to 7 days before SPT, because they suppress the wheal-and-flare response and cause false negatives. The test uses a positive control (histamine) and a negative control (saline) to confirm that the skin is reactive and not dermatographic. SPT is safe in infants and children; systemic reactions are extremely rare. [1]
Serum Food-Specific IgE
Serum food-specific IgE (sIgE) measures circulating allergen-specific IgE antibodies by fluorescence enzyme immunoassay. It is reported in kU/L. Like the SPT, sIgE detects sensitisation, not clinical allergy, and must be interpreted with the clinical history. [2]
The 95% PPV thresholds for sIgE vary by food and age. Commonly cited values include: peanut 14 kU/L (95% PPV in children), egg 7 kU/L (young children), milk 15 kU/L, wheat 26 kU/L, and fish 20 kU/L. A rising sIgE level over time in a child with known allergy predicts lower likelihood of resolution, while a falling level predicts tolerance acquisition and may prompt a re-challenge. Importantly, these thresholds are population-derived and may not apply to every child; they are decision-support tools, not diagnostic absolutes. [1][5]
Component-Resolved Diagnostics (CRD)
Component-resolved diagnostics measures IgE antibodies to individual allergen proteins (components) rather than to whole-food extract. This refines the diagnostic accuracy beyond what SPT or whole-extract sIgE can achieve, because different components have different clinical significance. [2][5]
For peanut, the most clinically important component is Ara h 2 (2S albumin). IgE to Ara h 2 has substantially higher diagnostic accuracy for clinical peanut allergy than whole-peanut IgE, because it identifies children sensitised to a heat-stable storage protein that drives systemic reactions. In contrast, IgE to Ara h 8 (Bet v 1 homologue) indicates cross-reactivity with birch pollen and typically produces only oral allergy syndrome; these children often tolerate peanut on challenge. CRD with Ara h 2 can reduce the need for OFC in children with ambiguous whole-extract results. [5]
For egg, IgE to Gal d 1 (ovomucoid) predicts reactivity to both raw and cooked egg, whereas IgE to Gal d 2 (ovalbumin) is associated primarily with raw egg reactivity. This distinction matters because many egg-allergic children tolerate extensively heated (baked) egg, and Gal d 1 negativity may support a baked-egg challenge. For cow's milk, IgE to Bos d 8 (casein) is the most predictive component for persistent allergy, while IgE to Bos d 4 (alpha-lactalbumin) and Bos d 5 (beta-lactoglobulin) are more often associated with transient allergy that resolves. [2][5]
The Oral Food Challenge (OFC)
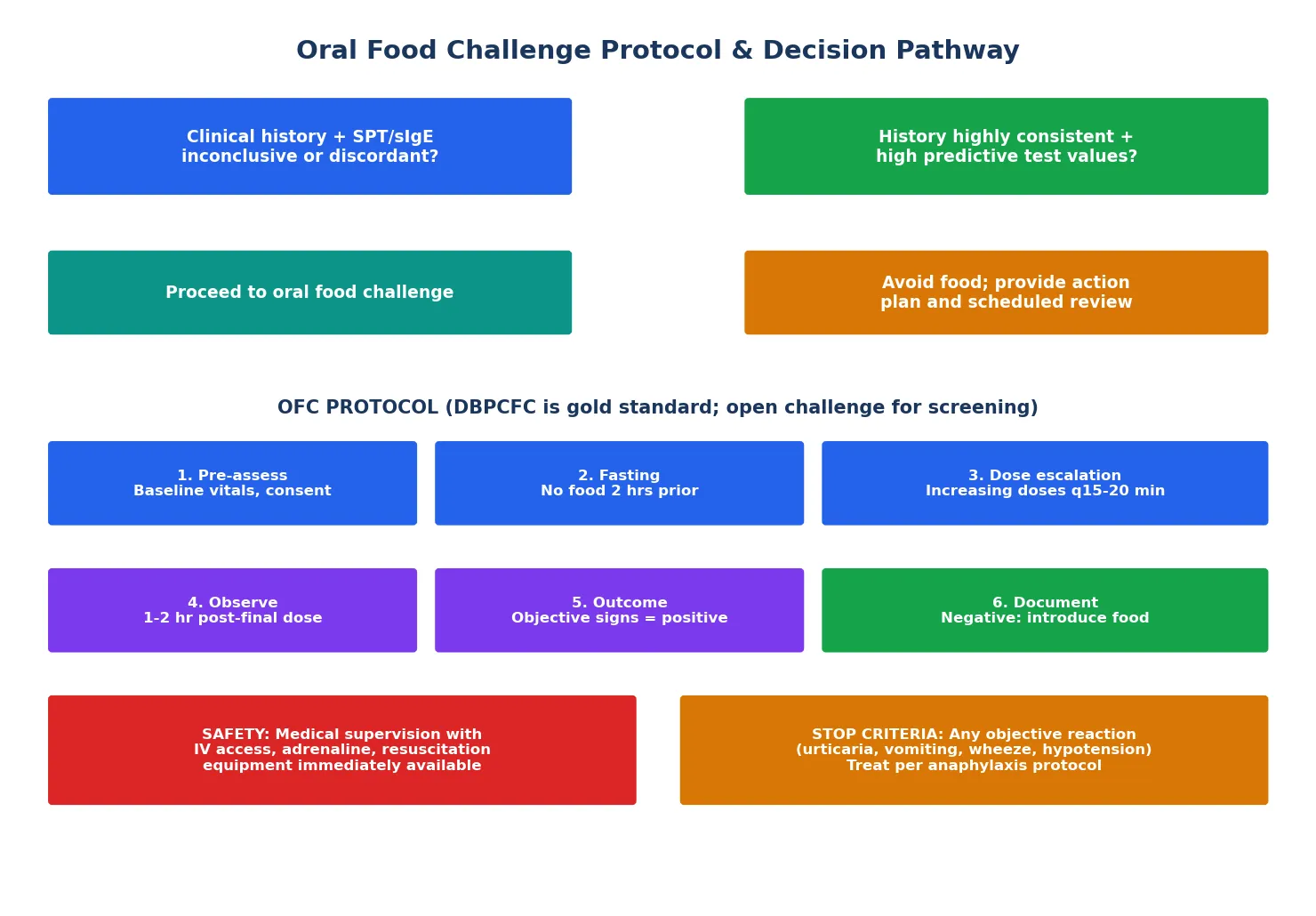
The oral food challenge is the gold standard for confirming or excluding clinical food allergy. It is indicated when the clinical history and test results are discordant, when sensitisation exists without a clear reaction history, when tolerance needs to be assessed (e.g., has the allergy resolved?), or when baked-milk or baked-egg tolerance needs to be determined. [1][4]
The double-blind placebo-controlled food challenge (DBPCFC) is the most rigorous format — neither the patient, family, nor supervising clinician knows whether the challenge dose contains the allergen or a placebo. It eliminates reporting bias and is the standard for research and for cases where subjective symptoms could confound the result. The single-blind placebo-controlled format hides the identity from the family and patient but not the clinician. The open challenge uses known allergen and is appropriate when the expected reaction would be objective and unambiguous; it is the most practical format for routine clinical use and for screening challenges in low-risk children. [4]
Management — Resuscitation
Oral food challenges carry a real risk of triggering an allergic reaction, including anaphylaxis. Approximately 10 to 15% of challenges produce a reaction requiring treatment, and severe reactions occur in a small but non-negligible proportion. The clinical environment must be prepared to manage anaphylaxis immediately. [4]
Before starting a challenge, the child must be assessed for contraindications. Uncontrolled asthma is the most important contraindication — a child with current wheeze, frequent symptoms, or recent oral corticosteroid use is at significantly higher risk of severe respiratory reactions. The challenge should be postponed until asthma is optimised. Other contraindications include acute illness (especially gastrointestinal or respiratory infection), uncontrolled severe eczema that would confound skin symptom interpretation, and a history of a recent severe reaction to the same food where the risk of a repeat reaction outweighs the diagnostic benefit. [4]
The challenge should be conducted in a setting with immediate access to resuscitation equipment, including adrenaline (epinephrine) for intramuscular injection, oxygen, nebulised bronchodilators, IV fluids, and antihistamines. Staff must be trained in paediatric anaphylaxis management. IV access should be established for high-risk challenges or when the history suggests a risk of severe reaction. [4]
Adrenaline (epinephrine) — IM
Dose
0.01 mg/kg of 1:1000 (1 mg/mL) concentration
The adrenaline dosing above follows standard paediatric anaphylaxis guidelines applied in the food challenge setting. [4][1]
If anaphylaxis occurs during challenge, the challenge is stopped immediately, IM adrenaline is administered, and the child is managed per the standard anaphylaxis protocol. After any reaction — mild or severe — the child must be observed for a minimum of 2 hours after the last dose and resolution of symptoms, because biphasic reactions can occur (though this is uncommon in challenge settings). [4]
Management — Definitive & Stepwise
The definitive diagnostic strategy integrates history, testing, and challenge into a stepwise pathway. The goal is to confirm or exclude clinical food allergy with the minimum necessary risk and intervention, and to avoid the harms of overdiagnosis and unnecessary dietary restriction. [1][5]
Step 1: Structured clinical history — Does the reaction sound like an IgE-mediated food allergy? (timing, reproducibility, symptoms, dose)
Step 2: Targeted SPT and/or serum specific IgE to the suspected food only — never a broad panel
Step 3: Interpret results against 95% PPV thresholds; if clearly diagnostic (high sIgE + convincing history), allergy is confirmed
Step 4: If ambiguous, apply component-resolved diagnostics (e.g., Ara h 2 for peanut) to refine the probability
Step 5: If still uncertain, proceed to oral food challenge (open for low-risk, DBPCFC for ambiguous or subjective symptoms)
Step 6: Counsel family on the result; arrange dietary introduction if negative; action plan and review if positive
The OFC Protocol in Detail
The standardised OFC protocol, as defined by the AAAAI-EAACI PRACTALL consensus, proceeds through escalating doses of the challenge food administered at fixed intervals. The total challenge dose is typically a serving-equivalent (for example, 4 to 8 grams of protein for peanut, 1 to 2 egg whites for egg, 100 to 200 mL of milk for cow's milk). [4]
The dose schedule starts with a small initial dose (approximately 1 to 5% of the total) and increases at 15 to 20 minute intervals, typically in 5 to 10 doses. Between each dose, the child is assessed for objective signs of reaction (urticaria, angioedema, vomiting, wheeze, cough, hypotension). Subjective symptoms alone (oral itch, nausea, refusal) warrant observation but may not require stopping the challenge. The challenge is terminated if any objective reaction occurs, if the total dose is reached without reaction (negative challenge), or if the family or clinician decides to stop for safety reasons. [4]
After the final dose — whether negative or after treatment of a reaction — the child is observed for 1 to 2 hours for delayed reactions. A negative challenge is followed by a recommendation to regularly include the food in the diet (home introduction within the following days to confirm ongoing tolerance). A positive challenge results in an allergy action plan, adrenaline autoinjector prescription if indicated, dietary advice, and a scheduled review to assess for resolution. [4][7]
Baked-Milk and Baked-Egg Tolerance
A significant proportion of children with IgE-mediated milk or egg allergy tolerate the food in extensively heated (baked) form, because the high temperature denatures the heat-labile allergenic proteins (ovalbumin, beta-lactoglobulin) while the food matrix (wheat) further reduces allergenicity. Assessing baked tolerance is an important diagnostic step because it expands the diet, improves nutrition, and accelerates the acquisition of full tolerance. A baked-milk or baked-egg challenge (using a standardised muffin or cake recipe) can be performed to determine whether the child can safely include baked products in their diet. [2][5]
SAFE
Specific Subtypes & Scenarios
Cow's milk protein allergy is the most common food allergy in infants and presents in both IgE-mediated (acute urticaria, vomiting, anaphylaxis) and non-IgE-mediated forms (proctocolitis, enteropathy, FPIES). The diagnostic approach differs by phenotype: IgE-mediated is diagnosed by SPT/sIgE and confirmed by OFC if needed, while non-IgE-mediated is diagnosed by elimination and re-challenge. Most milk allergy resolves by age 3 to 5, and the milk-specific IgE level and SPT wheal size are the best predictors of resolution. [2][5]
Peanut allergy is the most common cause of food-induced anaphylaxis in children and tends to persist — only approximately 20% resolve by age 5, though the HealthNuts natural history data showed higher resolution rates (approximately 22% by age 4) than previously believed. The diagnosis benefits most from component-resolved diagnostics: Ara h 2 positivity strongly predicts clinical allergy, while Ara h 8 positivity suggests cross-reactivity and likely tolerance. The 2017 NIAID addendum, based on the LEAP trial evidence, recommends early peanut introduction (4 to 6 months) in high-risk infants (severe eczema or egg allergy) after evaluation by testing or supervised feeding. [3][6][8]
Egg allergy resolves in the majority of children by school age. Many egg-allergic children tolerate baked egg, and a baked-egg challenge should be offered. The influenza vaccine can be safely administered to egg-allergic children without special precautions, because modern vaccine egg-protein content is negligible. [2][5]
Food-dependent exercise-induced anaphylaxis requires a careful history identifying that reactions occur only when food ingestion is followed by exercise within a few hours. The food (often wheat, celery, shellfish, or peach) is tolerated when the child does not exercise. Diagnosis requires a specific exercise-challenge protocol combined with food ingestion, performed under specialist supervision. [2]
Complications & Pitfalls
The most common diagnostic pitfall in paediatric food allergy is overdiagnosis from indiscriminate testing. A food allergy panel ordered without a supporting clinical history will produce multiple positive results in any atopic child, because sensitisation without clinical allergy is common. Each false positive becomes a dietary restriction, a school health plan, a label of "allergic child," and a source of anxiety. Studies have shown that children with food allergy labels have measurably reduced quality of life, comparable to other chronic childhood diseases. [5]
The second major pitfall is underdiagnosis of non-IgE-mediated reactions, particularly FPIES. A child who presents with delayed, profuse vomiting after milk or soy ingestion is often investigated for sepsis, gastroenteritis, or pyloric stenosis before FPIES is considered. The key diagnostic clue is the reproducible, delayed onset (1 to 4 hours) and the absence of fever or diarrhoea. FPIES is confirmed by supervised oral re-challenge after a period of elimination, because SPT and serum IgE are characteristically negative. [12]
The third pitfall is failing to reassess for resolution. Milk, egg, wheat, and soy allergies frequently resolve during childhood, but children labelled as allergic may never be re-challenged and may carry unnecessary restrictions into adolescence. Scheduled reassessment — by repeat SPT/sIgE monitoring every 1 to 2 years and oral re-challenge when levels suggest likely resolution — is an essential part of long-term management. [8]
During oral food challenge, complications include acute allergic reactions (urticaria, vomiting, wheeze, anaphylaxis), which occur in 10 to 15% of challenges. Severe reactions are uncommon but can occur, particularly in children with high pre-challenge sIgE, a history of previous severe reactions, or uncontrolled asthma. [4][7]
Prognosis & Disposition
The natural history of food allergy varies dramatically by food. Cow's milk, egg, wheat, and soy allergies typically resolve during childhood — approximately 50% of milk allergy resolves by age 5, and approximately 70% of egg allergy resolves by age 6. Peanut, tree nut, sesame, and seafood allergies are far more likely to persist, with peanut allergy resolving in only approximately 20% of children. [2][8]
Factors predicting tolerance acquisition include a falling SPT wheal size over time, a declining serum specific IgE level, and the component profile (e.g., sensitisation only to labile components predicts resolution). Factors predicting persistence include a large SPT wheal, a high and stable sIgE level, sensitisation to heat-stable storage proteins (Ara h 2, Gal d 1, Bos d 8), and a history of severe reactions. [5][8]
The HealthNuts study showed that food allergy — even when it resolves — is an important risk factor for childhood asthma, regardless of whether the food allergy persists. This finding underscores that food allergy is a marker of broader atopic susceptibility and that children with food allergy require ongoing surveillance for the development of asthma and allergic rhinitis. [8]
Disposition after diagnosis depends on the outcome. A negative challenge is followed by dietary introduction at home (with a written plan and advice on what to do if a delayed reaction occurs). A positive challenge is followed by dietary avoidance, an allergy action plan, an adrenaline autoinjector prescription (if there is risk of anaphylaxis), nutritional review, and a scheduled reassessment at 1 to 2 year intervals to test for resolution. [1][7]
Special Populations
Infants and very young children have the highest prevalence of food allergy and the highest likelihood of resolution. Their diagnostic testing requires age-specific interpretation — the 95% PPV thresholds are lower in infants than in older children, and a positive test in a 6-month-old has different implications than the same result in a 10-year-old. The LEAP trial and 2017 NIAID addendum have transformed the approach to infants at high risk (severe eczema, egg allergy), shifting from delayed introduction to early peanut introduction at 4 to 6 months. [3][6]
Children with severe atopic dermatitis require special consideration because they have both a higher pre-test probability of food allergy and lower predictive values for their tests. The extensive skin inflammation can drive polysensitisation, producing positive tests to multiple foods without clinical allergy to most of them. Testing should be directed by a history of acute reactions, not by eczema severity alone, and broad panels should be avoided. [2][6]
Children with eosinophilic oesophagitis (EoE) may have co-existing IgE-mediated food allergy, but the diagnostic and management strategies differ. EoE is diagnosed by endoscopic biopsy (showing 15 or more eosinophils per high-power field) and is managed with elimination diets guided by testing, elemental formula, or topical corticosteroids. Food allergy testing in EoE is adjunctive — SPT and sIgE may guide elimination diets but do not, on their own, identify all causative foods. [2]
Adolescents represent a high-risk group for fatal food-induced anaphylaxis, driven by risk-taking behaviour, reluctance to carry adrenaline autoinjectors, and the transition to independent eating. The diagnostic and management focus shifts toward empowerment, action plan adherence, and the transition to adult allergy services. [2]
Evidence, Guidelines & Regional Differences
The NIAID-sponsored guidelines (Boyce et al., 2010) provide the foundational US framework for food allergy diagnosis and management. They established the definitions, the role of SPT and sIgE, and the gold standard status of the DBPCFC. The 2017 NIAID addendum (Togias et al.) added the critical prevention recommendation based on the LEAP trial: infants with severe eczema or egg allergy should be evaluated for peanut allergy (by SPT or supervised feeding) at 4 to 6 months and offered early peanut introduction, because this reduces peanut allergy incidence by approximately 80%. [1][3][6]
The BSACI guidelines (UK, Stiefel et al., 2017) for peanut and tree nut allergy provide the UK framework, with similar diagnostic principles but region-specific guidance on challenge protocols and autoinjector provision. The UK National Health Service pathway emphasises specialist referral for suspected nut allergy and community management with action plans. [9]
The ASCIA guidelines (Australia) provide the ANZ framework. Australia has the highest documented food allergy prevalence in the world (HealthNuts data), and ASCIA guidelines emphasise early allergenic food introduction, no delayed introduction of allergens, and regular inclusion of allergens in the infant diet once introduced. ASCIA also provides the standardised action plans and autoinjector training resources used across Australian schools and childcare. [6]
ASCIA recommends introducing solid foods (including allergenic foods) from 4 to 6 months, without delay, and continuing regular exposure. This contrasts with older advice to delay introduction. The LEAP trial evidence and the HealthNuts prevalence data underpin this early-introduction strategy. Cow's milk or soy formula should not be used for allergy prevention; breastfeeding is recommended for at least 6 months. [6]
Current controversies include the role of oral immunotherapy (OIT) as a therapeutic option — it is not a diagnostic test but a treatment that induces desensitisation. The FDA and TGA approval of peanut OIT (Palforzia) has blurred the line between diagnosis and management, because OIT requires a confirmed diagnosis first and carries its own risk profile. Another controversy is the appropriate use of the basophil activation test (BAT) — a flow-cytometry-based functional assay that shows promise for improving diagnostic accuracy but is not yet widely available outside research settings. [5]
Exam Pearls
The exam favourite is the dual-allergen-exposure hypothesis: cutaneous sensitisation through disrupted skin barrier (atopic dermatitis) drives Th2 skewing and IgE production, while early oral exposure promotes tolerance. This is the biological basis for the LEAP trial — early peanut introduction prevents allergy — and explains why severe eczema is the strongest risk factor for food allergy. A candidate who can explain this mechanism, quote the SPT and sIgE thresholds, and describe the OFC protocol is well prepared for any food allergy viva. [2][3][6]
References
- [1]Boyce JA, Assa'ad A, Burks AW, et al. Guidelines for the diagnosis and management of food allergy in the United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol, 2010.PMID 21134576
- [2]Sicherer SH, Sampson HA Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J Allergy Clin Immunol, 2018.PMID 29157945
- [3]Du Toit G, Roberts G, Sayre PH, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med, 2015.PMID 25705822
- [4]Sampson HA, Gerth van Wijk R, Bindslev-Jensen C, et al. Standardizing double-blind, placebo-controlled oral food challenges: American Academy of Allergy, Asthma & Immunology-European Academy of Allergology and Clinical Immunology-PRACTALL consensus report. J Allergy Clin Immunol, 2012.PMID 23195525
- [5]Foong RX, Dantzer JA, Wood RA, et al. Improving Diagnostic Accuracy in Food Allergy. J Allergy Clin Immunol Pract, 2021.PMID 33429723
- [6]Togias A, Cooper SF, Acebal ML, et al. Addendum guidelines for the prevention of peanut allergy in the United States: Report of the National Institute of Allergy and Infectious Diseases-sponsored expert panel. Ann Allergy Asthma Immunol, 2017.PMID 28065802
- [7]Chan JCK, Peters RL, Koplin JJ, et al. Food Challenge and Community-Reported Reaction Profiles in Food-Allergic Children Aged 1 and 4 Years: A Population-Based Study. J Allergy Clin Immunol Pract, 2017.PMID 28283159
- [8]Peters RL, Allen KJ, Dharmage SC, et al. Natural history of peanut allergy and predictors of resolution in the first 4 years of life: A population-based assessment. J Allergy Clin Immunol, 2015.PMID 25725989
- [9]Stiefel G, Anagnostou K, Boyle RJ, et al. BSACI guideline for the diagnosis and management of peanut and tree nut allergy. Clin Exp Allergy, 2017.PMID 28836701
- [10]Perkin MR, Logan K, Marrs T, et al. Enquiring About Tolerance (EAT) study: Feasibility of an early allergenic food introduction regimen. J Allergy Clin Immunol, 2016.PMID 26896232
- [11]Spolidoro GCI, Ali MM, Amera YT, et al. Prevalence estimates of eight big food allergies in Europe: Updated systematic review and meta-analysis. Allergy, 2023.PMID 37405695
- [12]Leonard SA, Pecora V, Fiocchi AG, et al. Food protein-induced enterocolitis syndrome: a review of the new guidelines. World Allergy Organ J, 2018.PMID 29441147