Paeds · allergy-and-immunology
Food allergy management and prevention
Also known as Food allergy management · Food allergy prevention · Early allergen introduction · Adrenaline autoinjector prescribing · Food allergy in children
A fellowship approach to childhood food allergy: managing the child who reacts with avoidance, a written anaphylaxis action plan and weight-banded IM adrenaline; and preventing allergy forming through early, sustained allergen introduction built on the LEAP, LEAP-ON, EAT, PETIT and EAACI/NIAID guidance, across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old with egg allergy develops lip swelling and wheeze within minutes of a birthday cake. The two questions that follow define this topic: what do you do now, and what should you have done earlier to stop this child becoming allergic in the first place. Holding both answers at once is the fellowship skill. [5] [6]
A food allergy is an adverse immune-mediated reaction to a food protein. It is reproducible and immune-driven, which separates it from food intolerance (a non-immune mechanism such as lactase deficiency) and from simple food aversion. [5]
The mechanism matters because it changes everything that follows. IgE-mediated reactions are rapid, mast-cell driven, and can cause anaphylaxis within minutes. Non-IgE or mixed reactions are delayed, T-cell or eosinophil-driven, and are managed with diet rather than adrenaline. [6]
The single most useful framing for this topic is the manage versus prevent split. Management treats a child who already reacts. Prevention stops the allergy forming at all. The strongest prevention signal in modern paediatrics is early, sustained allergen introduction, which overturned the old advice to delay solids. [1] [4] [13]
Classification
Sort every child through two axes: which mechanism is driving the reaction, and whether you are managing an existing allergy or preventing a new one. [5]
By mechanism
IgE-mediated reactions appear within minutes to two hours. Think urticaria, angioedema, vomiting, and anaphylaxis with airway, breathing or circulation compromise. Peanut, tree nut, egg, milk, sesame and seafood are the classic rapid triggers. [6]
Non-IgE and mixed reactions are delayed, from hours to days. Examples are food-protein-induced enterocolitis syndrome (FPIES), food-protein-induced proctocolitis (blood and mucus in stool of a well infant with cow's-milk protein allergy), eczema flares, and eosinophilic oesophagitis. These rarely need adrenaline. [6] [7]
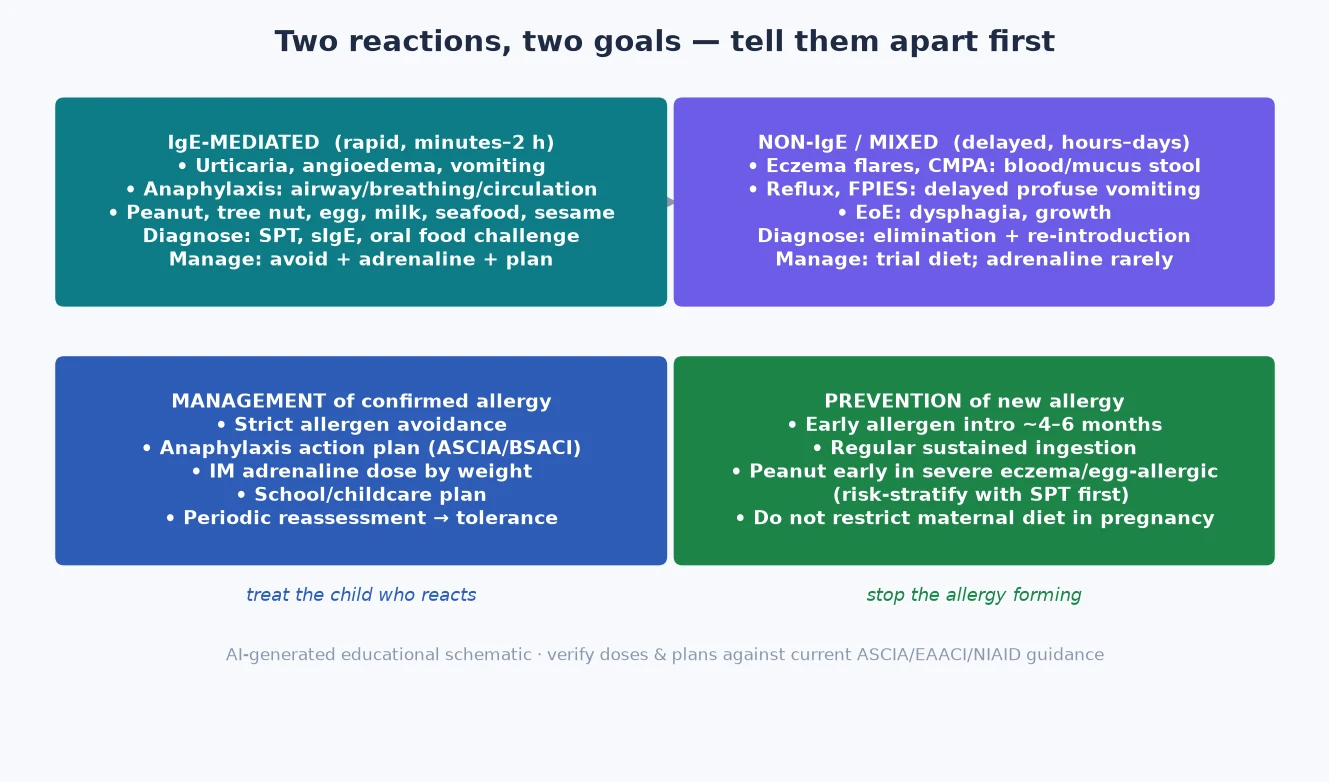
Read the figure like this: a child who reacts within minutes sits in the top-left quadrant — think adrenaline and an action plan. A well infant with blood-streaked stool sits in the top-right — think trial diet, not adrenaline. [6] [7]
IgE-mediated
Rapid · mast-cell
- Onset minutes to 2 hours
- Urticaria, angioedema, anaphylaxis
- Peanut, tree nut, egg, milk, seafood, sesame
- Diagnose: SPT, sIgE, oral challenge
- Manage: avoid + adrenaline + plan
Non-IgE / mixed
Delayed · T-cell / eosinophil
- Onset hours to days
- FPIES vomiting, proctocolitis, EoE, eczema flares
- Cow's milk, soy, oats, egg
- Diagnose: elimination + reintroduction
- Manage: trial diet; adrenaline rarely
Epidemiology & Risk Factors
Childhood food allergy affects roughly one in ten infants in high-income settings. Peanut, egg and cow's milk are the commonest childhood triggers, and the burden has risen over a generation. [6]
Risk concentrates where the skin barrier is broken. Severe early-onset eczema and existing egg allergy are the two strongest markers that an infant will develop peanut allergy — which is exactly the group the LEAP trial targeted for prevention. Family atopy adds further risk. [1] [4]
The natural history is more hopeful than families expect. Most children outgrow cow's-milk and egg allergy; peanut, tree-nut, seed and seafood allergy more often persist into later life. HealthNuts and older cohort data frame these resolution rates. [7] [12]
Mortality from food anaphylaxis is rare, but it clusters predictably: adolescents with co-existing asthma and delayed adrenaline use. That demographic drives much of the safety-net counselling in this topic. [6] [14]
Pathophysiology
The question "why does eating a food early stop you becoming allergic to it" is the conceptual core of prevention. The answer is the dual-allergen-exposure hypothesis. The same food protein can drive two opposite outcomes depending on the route it meets the immune system. [6]
Through broken skin (eczema), food protein drives IgE production and sensitisation. Through the gut, the same protein induces oral tolerance via regulatory T cells. So a baby with severe eczema who is not eating peanut can still become sensitised to it through the skin. Early oral exposure tilts the balance toward tolerance. [6] [10]
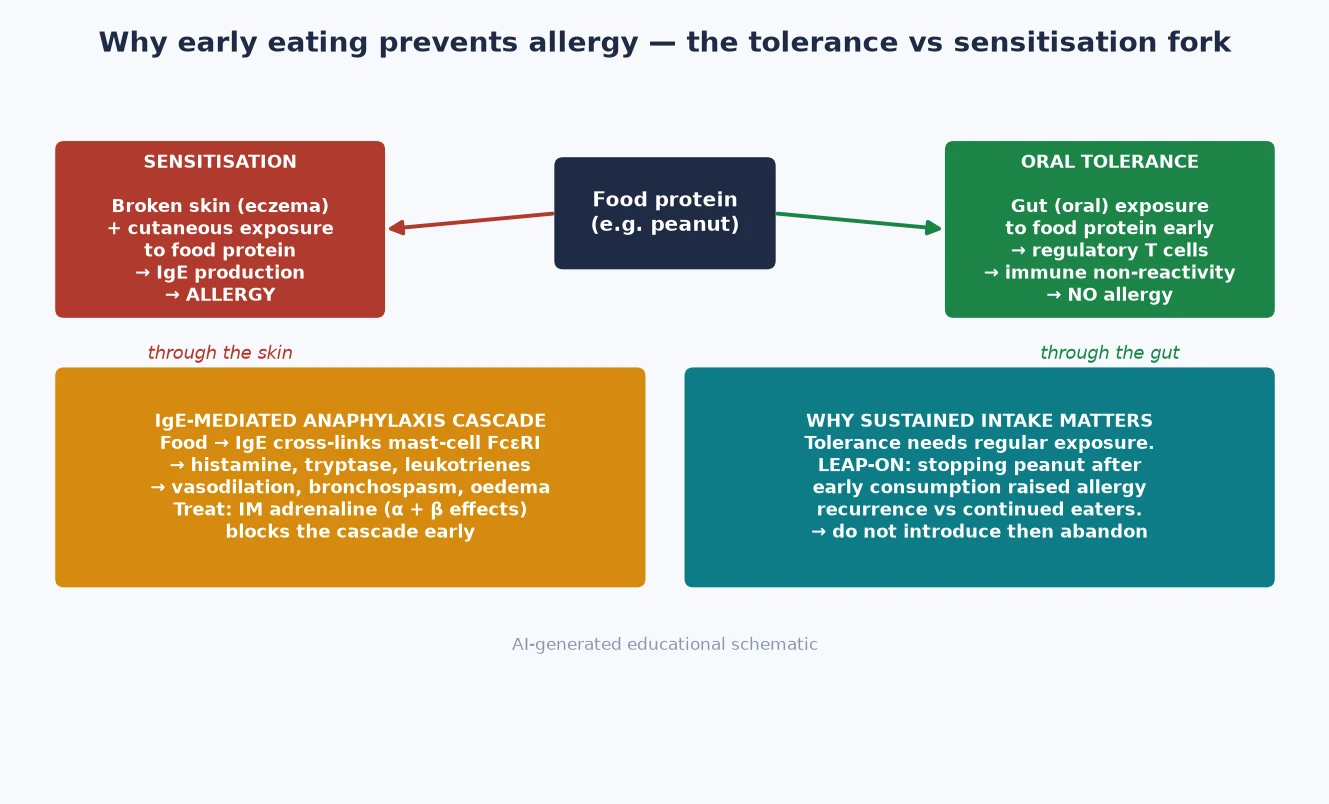
When sensitisation has already occurred, an IgE reaction unfolds as a cascade. Food protein cross-links IgE on the mast-cell FcεRI receptor. The cell degranulates, releasing histamine, tryptase and leukotrienes. The result is vasodilation, bronchospasm and mucosal oedema. [14]
This cascade is why IM adrenaline works and works early. Its alpha effect constricts vasculature and reduces oedema; its beta effect opens bronchi and stabilises mast cells. Waiting for an antihistamine while a child is wheezing and hypotensive is the classic exam error. [14]
Tolerance, once established, is not passive. The LEAP-ON study stopped peanut after a year of early consumption and showed that tolerance largely persisted — but allergy recurrence was higher than in children who kept eating peanut. The practical lesson is that introducing a food and then abandoning it leaves the door ajar. [2]
Clinical Presentation
Match the tempo to the mechanism. A rapid, multi-system reaction within minutes of a food is IgE-mediated until proven otherwise. [6]
Anaphylaxis is the emergency: airway swelling, wheeze or respiratory distress, hypotension or collapse, with or without urticaria and angioedema. Crucially, skin signs alone are not anaphylaxis — but anaphylaxis can also occur without skin signs, so the absence of a rash never excludes it. [6] [14]
Acute IgE reactions short of anaphylaxis include urticaria, angioedema, and rapid abdominal pain or vomiting after the trigger food. Onset is within minutes to two hours. [5]
Non-IgE presentations are slower and more deceptive. FPIES brings delayed, profuse, repetitive vomiting around one to four hours after a trigger. Cow's-milk protein proctocolitis shows as blood and mucus in the stool of an otherwise well infant. Eosinophilic oesophagitis causes dysphagia, reflux and growth failure. Eczema flares can track food exposure over days. [6] [7]
A reaction's severity can be amplified by cofactors: exercise (food-dependent exercise-induced anaphylaxis), NSAIDs, intercurrent infection, heat or alcohol in older teens. Ask about them whenever the history seems disproportionate to the dose eaten. [6]
Differential Diagnosis
The trap is labelling any post-food symptom as allergy. Separate immune reactions from mimics before restricting a child's diet. [5]
| Finding after eating | Prefer | Discriminators | Action |
|---|---|---|---|
| Multi-system collapse within minutes | IgE anaphylaxis | Onset minutes; airway/breathing/circulation | IM adrenaline immediately |
| Urticaria only, well between episodes | Acute urticaria (food, infection, drug) | No airway or circulation threat | Antihistamine; identify trigger |
| Flushing minutes after fish | Scombroid (histamine toxin) | Spoiled fish; responds to antihistamine | Supportive care; public-health report |
| Bloating, diarrhoea after dairy | Lactose intolerance | Non-immune; dose-related gut only | Lactase; no adrenaline |
| Brief collapse, pale, rapid recovery | Vasovagal syncope | No airway/breathing threat; good recovery | Lie flat; observe |
| Local oral itch to raw fruit | Oral allergy syndrome (pollen-food) | Cooked food tolerated; local only | Avoid raw trigger; confirm not progressing |
Separate coincidental illness from true food reaction by timing and plausibility. Urticaria the day after a vaccine is not a food allergy. A reaction within minutes of peanut is not coincidence. [6]
Clinical & Bedside Assessment
In a suspected acute reaction, assessment is resuscitation-first. Run an ABCDE approach and treat anaphylaxis as a clinical diagnosis — you do not need a blood test to give adrenaline. [14]
Take a focused trigger history once the child is safe. Ask what food, how much, the onset time, the exact symptoms, any treatment given, and any cofactors such as exercise or NSAIDs. The history is usually more diagnostic than any test. [5] [6]
For the high-risk infant in clinic, assess eczema severity and what the child already tolerates. Severe eczema plus egg allergy is the signal to risk-stratify before introducing peanut. [1] [4]
In chronic non-IgE allergy, examine growth and nutrition. A child on a restricted milk-free or multiple-food diet can slide into inadequate energy, calcium and vitamin D intake. Catching this is part of the assessment, not an afterthought. [6] [7]
Investigations
Tests support a compatible history; they do not replace it. A positive test in a child who tolerates the food is sensitisation, not allergy. [5] [6]
For IgE-mediated allergy, skin-prick testing (SPT) and serum specific IgE measure sensitisation. They are useful for risk stratification and tracking change over time, but a positive result alone never makes the diagnosis. Component-resolved diagnostics — such as Ara h 2 for peanut — help separate true allergy from cross-reactivity and predict persistence and severity. [6]
The oral food challenge is the gold standard. A supervised, graded ingestion confirms a diagnosis, demonstrates that a child has outgrown an allergy, and safely expands the diet. It is the test that unlocks dietary freedom. [5] [6]
In an acute reaction, tryptase drawn in the first one to two hours supports anaphylaxis and a baseline level between reactions screens for mastocytosis in severe or idiopathic cases. A normal tryptase never excludes anaphylaxis. [14]
Non-IgE workup relies on a trial of elimination with planned reintroduction — remove the suspected protein, document resolution, then reintroduce to confirm causation. Suspected eosinophilic oesophagitis needs endoscopy with biopsy, and FPIES is a clinical diagnosis confirmed by structured challenge. [6] [7]
Management — Resuscitation
When a child reacts, the first drug is adrenaline, not an antihistamine. [14]
Give IM adrenaline into the anterolateral thigh as the first step. Do not wait for intravenous access, antihistamines, or a confirmatory test. Lie the child flat with legs elevated if shocked, give high-flow oxygen, and use IV fluids for shock; a bronchodilator is adjunctive for bronchospasm. [14]
Dose adrenaline by weight. A practical approach is roughly 0.01 mg/kg of 1:1000 (1 mg/mL) intramuscularly. Autoinjector doses map to this: 0.15 mg for smaller children (under about 20 kg, roughly under six years) and 0.30 mg for larger children (about 20 kg and over, roughly six years and over). Repeat after five minutes if there is no response. [14]
Call for help and arrange retrieval early, especially in rural and remote settings where distance narrows the safety margin. Then observe for the biphasic reaction: at least six hours for moderate reactions, and admission for severe reactions, those needing more than one adrenaline dose, or any child with co-existing asthma. [14] [6]
Management — Definitive & Stepwise
Once the acute event is settled, definitive management is a ladder that takes the family from the reaction to a safe, liveable plan. [5] [6]
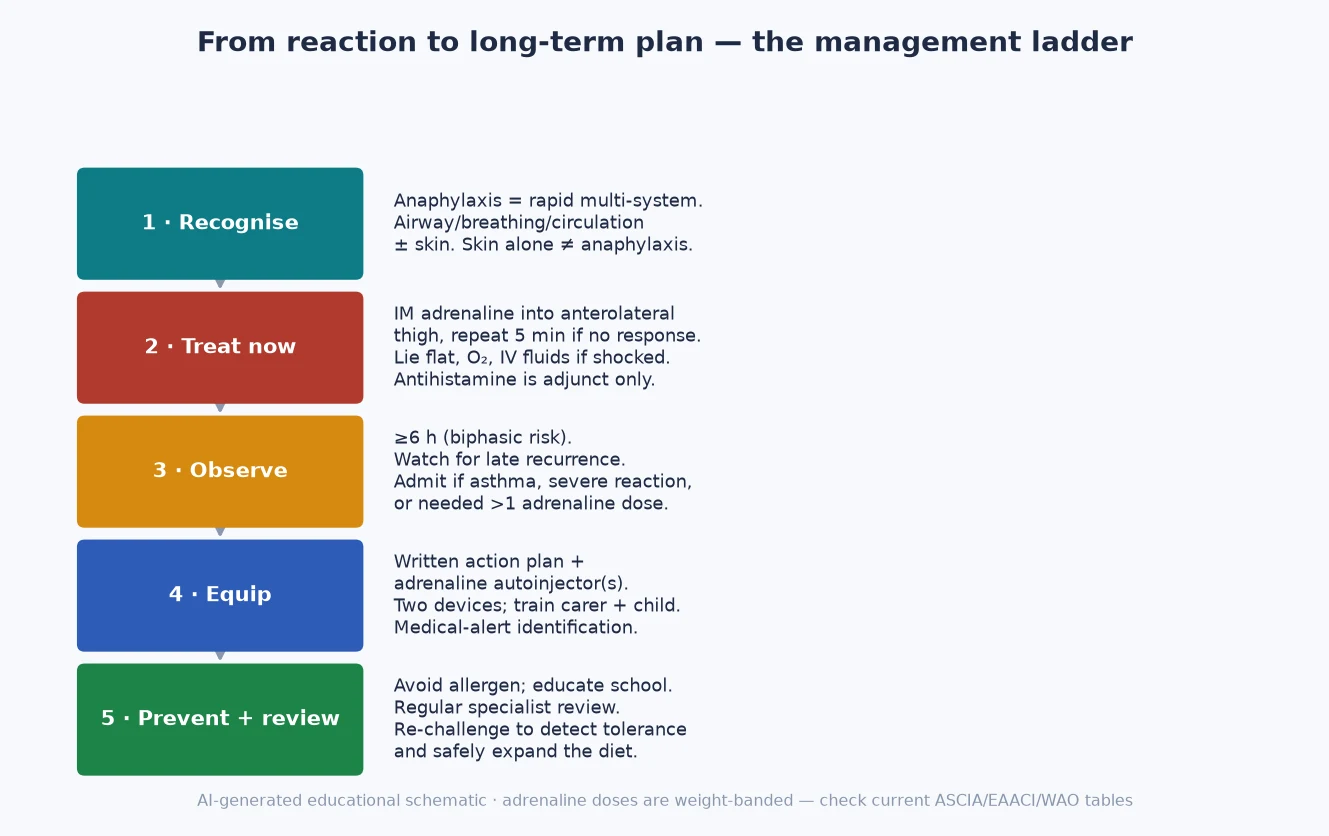
Step one — avoid the allergen. Teach label reading, cross-contamination, hidden sources and high-risk cuisines. The goal is precise avoidance of the confirmed trigger, not a blanket ban on foods the child tolerates. Over-restriction causes nutritional and social harm. [6]
Step two — a written action plan. Give the family a personalised anaphylaxis action plan (ASCIA in ANZ, BSACI/MedicAlert in the UK, FARE in the US) with the child's photo, allergen list, adrenaline dose and a step-by-step response. A plan that lives on a phone photo is a plan that gets used. [6]
Step three — adrenaline autoinjector(s). Prescribe by weight band. Two devices are recommended so the child is covered at home, school and away. Train the carer and an age-appropriate child, and check expiry at every review. [14]
Step four — educate the ecosystem. The school, childcare or sports club needs an anaphylaxis policy, trained staff, a meal-management plan and emergency drills. The child's safety depends on the people around them, not just the device in their bag. [6]
Step five — review and re-challenge. Because most milk and egg allergy resolves, arrange periodic specialist review and re-challenge to detect tolerance and safely expand the diet. In specialist centres, oral immunotherapy may be an option for selected children. [5] [6]
The five rungs after a confirmed reaction
Avoid the allergen
Label reading, cross-contamination, hidden sources — without over-restricting tolerated foods.
Written action plan
Photo, allergen, adrenaline dose, step-by-step response; ASCIA / BSACI / FARE format.
Adrenaline autoinjector(s)
Weight-banded dose; two devices; train carer and child; check expiry.
Educate the ecosystem
School/childcare anaphylaxis policy, trained staff, meal plan, emergency drills.
Review and re-challenge
Periodic reassessment to detect tolerance and safely expand the diet.
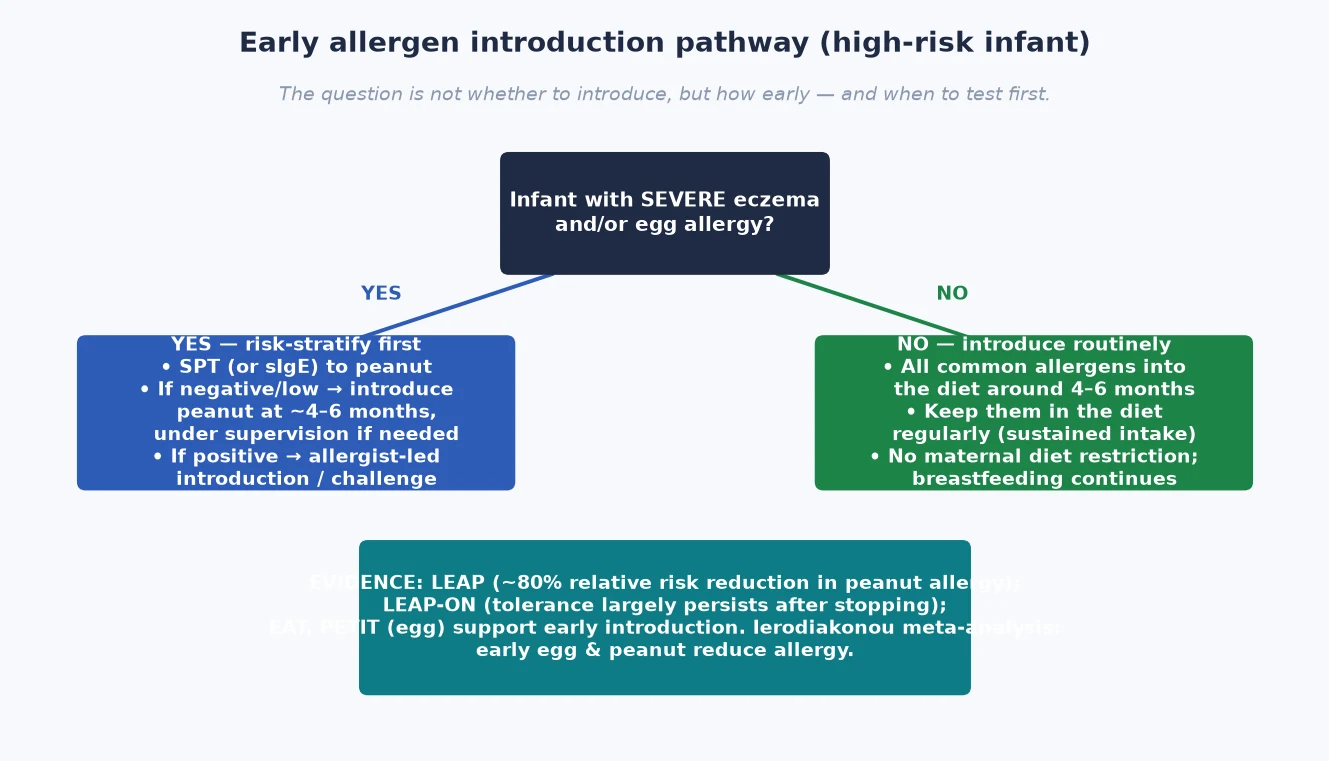
The prevention half of the topic sits alongside this ladder. Introduce common allergens around four to six months and keep them in the diet regularly. For the high-risk infant — severe eczema and/or egg allergy — risk-stratify with a skin-prick test first: introduce peanut early if the test is negative, and arrange specialist-led introduction if it is positive. Do not restrict the maternal diet during pregnancy or lactation, and keep breastfeeding. [1] [4] [13]
Specific Subtypes & Scenarios
Different foods behave differently, and examiners probe the corners. [6]
Peanut, tree-nut and seed allergy tend to persist and carry the highest anaphylaxis risk. Early introduction is the prevention priority; component testing (Ara h 2) refines the diagnosis. [1] [4] [12]
Egg and cow's-milk allergy are frequently outgrown. Tolerance to baked egg or baked milk expands the diet and is a marker of likely resolution, so confirm it rather than assuming strict avoidance forever. While milk is avoided, ensure calcium and vitamin D replacement. [7] [6]
FPIES presents with delayed, profuse vomiting around one to four hours after a trigger, often with pallor and lethargy. Acute management is supportive — IV fluids for dehydration and electrolytes — and adrenaline is not the treatment. A structured oral challenge guides reintroduction. [6]
Eosinophilic oesophagitis is a food-antigen-driven, eosinophil-predominant inflammation of the oesophagus. Management combines an elimination or elemental diet, a proton-pump inhibitor, and endoscopic follow-up with biopsy. [6]
Oral allergy syndrome (pollen-food syndrome) causes local oral itch to raw fruit or vegetable in a pollen-sensitised child. The cooked food is usually tolerated. The key teaching point is to confirm it is not progressing to systemic reactions, because systemic symptoms change the plan entirely. [6]
Complications & Pitfalls
The commonest error is over-diagnosis. A positive skin-prick or IgE in a child with no reaction history is sensitisation, not allergy. Acting on it alone condemns a child to an unnecessary restricted diet, family anxiety, and nutritional risk. [5] [6]
Delayed adrenaline is the most modifiable factor in fatal food anaphylaxis. Reaching for an antihistamine while a child has airway or circulation compromise is the single worst decision in this topic. [14] [6]
Over-restriction harms children too. Banning an entire food category, or removing foods the child tolerates, causes calcium and energy deficiency and social isolation. Aim for precise avoidance of the confirmed trigger. [6]
Missing the biphasic reaction by discharging too early is a recurrent exam trap — especially in the child with asthma or a severe initial reaction. Build the observation period into the plan. [14]
Two classification errors cost marks: confusing oral allergy syndrome with a systemic IgE allergy, and confusing FPIES (non-IgE, supportive care) with IgE anaphylaxis (adrenaline). Both lead to the wrong treatment. [6]
Finally, failing to risk-stratify before early peanut introduction in a severe-eczema or egg-allergic infant misses the prevention opportunity and the safety step in the same visit. [1] [4]
Prognosis & Disposition
The prognosis is more favourable than families fear for the common early-childhood allergens. The majority of children outgrow cow's-milk and egg allergy, often in the preschool years. Peanut, tree-nut, seed and seafood allergy persist more often, which is why they dominate the anaphylaxis and action-plan discussion. [7] [12]
Disposition after an acute reaction follows the risk profile. A child with a severe reaction, one who needed more than one adrenaline dose, one with co-existing asthma, or one far from emergency care is admitted and observed. A moderate, single-system reaction that resolves fully can be observed for at least six hours. [14] [6]
On the prevention side, early introduction is the strongest signal in the topic. The LEAP trial's roughly 80% relative reduction in peanut allergy is the result to quote. [1]
Quality of life, school participation and family anxiety are legitimate outcomes in their own right. A child who can attend a birthday party safely has a better outcome than one confined by fear. [6]
Special Populations
The high-risk infant is the centre of prevention. Severe eczema and/or egg allergy warrants a skin-prick test before introducing peanut; introduce early if the result is low or negative, and arrange specialist-led introduction if it is positive. [1] [4]
The adolescent and young adult sit at the peak of fatal food anaphylaxis. Risk-taking, eating away from home, and reluctance to carry or use a device all conspire here. Focus on self-carry, peer awareness, and a planned transition to adult allergy services. [6] [14]
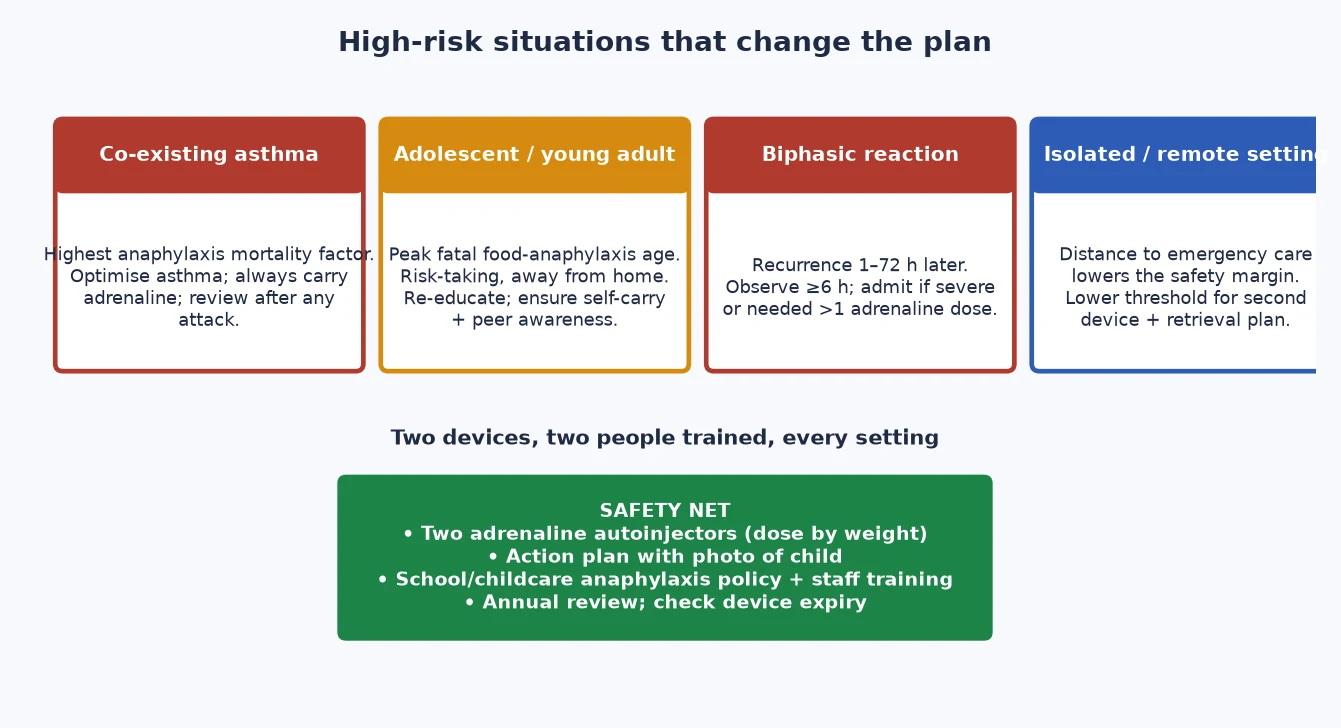
Co-existing asthma is the highest mortality factor in food anaphylaxis. Optimise the asthma, always ensure an adrenaline device is carried, and review after any asthma attack. [14]
Remote and rural families face a narrower safety margin because distance delays emergency care. Provide a second device, a retrieval plan, and community education so the people around the child can act first. [6]
Children with multiple food allergy or a heavily restricted diet need dietitian input for growth and micronutrient adequacy, especially calcium and vitamin D. [6] [7]
For Aboriginal and Torres Strait Islander, Māori, migrant and refugee families, deliver culturally safe education, use trained interpreters, and address equity of access to autoinjectors and specialist review. Out-of-home-care settings need a clearly designated carer responsible for the device and the plan. [6]
Evidence, Guidelines & Regional Differences
The evidence base has reversed in a decade, and defending that reversal is a viva staple. [4]
The LEAP trial (2015) randomised high-risk infants to early, sustained peanut consumption or avoidance. Early consumption cut peanut allergy by roughly 80% relative risk. [1]
LEAP-ON (2016) then stopped peanut for a year after the early-consumption arm. Tolerance largely persisted, though allergy recurrence was higher than in continued eaters — the basis for keeping the food in the diet. [2]
The EAT trial (2016) tested early introduction of six allergens in breast-fed infants. The intention-to-treat result was not significant, but per-protocol regular introduction reduced peanut and egg allergy. The takeaway is that adherence and sustained intake matter. [3]
LEAP — Learning Early About Peanut Allergy
Population: Infants 4–11 months with severe eczema and/or egg allergy
Key finding
~80% relative reduction in peanut allergy in the consumption arm
Practice change
Early sustained peanut introduction prevents peanut allergy in high-risk infants
The PETIT trial (2017) showed that a two-step egg introduction reduced egg allergy in high-risk infants with eczema. The Ierodiakonou JAMA meta-analysis (2016) provided moderate-certainty evidence that early egg and peanut introduction reduce allergy, and found no suggestion that early introduction increases autoimmune risk. [9] [8]
Guidelines have converged. The NIAID 2017 Addendum gives the risk-stratified peanut pathway. The EAACI 2021 guideline sets out food-allergy prevention in infants and young children. The older NIAID 2010 guidelines advised delaying allergens — that advice is now superseded, and a candidate who still quotes it will lose marks. [4] [13] [5]
[4] [13] [14]Controversies remain. The optimal dose and frequency of introduction are not fully defined. Oral immunotherapy is available in some specialist centres but carries risk and demands expertise. The role of component testing in primary care is still evolving. State the principle, name the guideline, and flag where the evidence is still maturing. [6]
Exam Pearls
A-F-A-C-T — the six steps after a confirmed food-allergy reaction
The high-yield prevention mnemonic is "EAT EARLY, KEEP EATING": introduce common allergens around four to six months, and sustain them in the diet — because tolerance needs regular exposure. [1] [2] [13]
References
- [1]Du Toit G Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med, 2015.PMID 25705822
- [2]Du Toit G Effect of Avoidance on Peanut Allergy after Early Peanut Consumption. N Engl J Med, 2016.PMID 26942922
- [3]Perkin MR Randomized Trial of Introduction of Allergenic Foods in Breast-Fed Infants. N Engl J Med, 2016.PMID 26943128
- [4]Togias A Addendum guidelines for the prevention of peanut allergy in the United States: Report of the NIAID-sponsored expert panel. J Allergy Clin Immunol, 2017.PMID 28065278
- [5]Boyce JA Guidelines for the diagnosis and management of food allergy in the United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol, 2010.PMID 21134576
- [6]Sicherer SH Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J Allergy Clin Immunol, 2018.PMID 29157945
- [7]Skripak JM The natural history of IgE-mediated cow's milk allergy. J Allergy Clin Immunol, 2007.PMID 17935766
- [8]Ierodiakonou D Timing of Allergenic Food Introduction to the Infant Diet and Risk of Allergic or Autoimmune Disease: A Systematic Review and Meta-analysis. JAMA, 2016.PMID 27654604
- [9]Natsume O Two-step egg introduction for prevention of egg allergy in high-risk infants with eczema (PETIT): a randomised, double-blind, placebo-controlled trial. Lancet, 2017.PMID 27939035
- [10]Fleischer DM Consensus Communication on Early Peanut Introduction and Prevention of Peanut Allergy in High-Risk Infants. Pediatr Dermatol, 2016.PMID 26354148
- [11]Obbagy JE Complementary feeding and food allergy, atopic dermatitis/eczema, asthma, and allergic rhinitis: a systematic review. Am J Clin Nutr, 2019.PMID 30982864
- [12]Peters RL Natural history of peanut allergy and predictors of resolution in the first 4 years of life: A population-based assessment. J Allergy Clin Immunol, 2015.PMID 25725989
- [13]Halken S EAACI guideline: Preventing the development of food allergy in infants and young children (2020 update). Pediatr Allergy Immunol, 2021.PMID 33710678
- [14]Simons FE World Allergy Organization Anaphylaxis Guidelines: 2013 update of the evidence base. Int Arch Allergy Immunol, 2013.PMID 24008815