Paeds · allergy-and-immunology
Insect-sting hypersensitivity
Also known as Hymenoptera venom allergy · Venom hypersensitivity · Bee and wasp sting allergy · Stinging-insect anaphylaxis · Venom immunotherapy indication
Fellowship topic on insect-sting (Hymenoptera venom) hypersensitivity in children: the reaction spectrum from normal local and large local reactions through cutaneous and systemic anaphylaxis; the culprits (honeybee, wasp and yellowjacket, ants including jack-jumper and fire ant); the IgE-mediated mast-cell and basophil mediator cascade; why baseline serum tryptase and clonal mast-cell disease mark out the severe reactor; the acute algorithm of early intramuscular adrenaline, positioning and fluids; the trigger-confirmation workup of venom-specific IgE, skin testing and component-resolved diagnostics; the decisive role of venom immunotherapy giving 90 to 98 per cent protection; and the discharge package of an adrenaline autoinjector, written action plan, medical identification and school education, citing the 2011 and 2023 practice parameters, the EAACI Hymenoptera venom allergy guideline, the Cochrane venom immunotherapy review, the predictors-of-severity tryptase study, and the paediatric venom allergy literature.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The venom rule — who gets what, and who gets VIT
Overview & Definition
Picture an eight-year-old playing barefoot in the garden who stands on a wasp, and within three minutes is rubbing an itchy swelling on her foot. Her mother watches and waits — most of the time, that is the whole story. Now picture the same child who, five minutes after the same sting, becomes flushed and wheezy, her lips swelling, before she goes grey and collapses in her mother's arms. The gap between those two pictures is the entire clinical problem of insect-sting hypersensitivity, and the fellowship task is to know which child is which, to treat the dangerous one immediately, and to make sure the dangerous one never has another dangerous sting. [8] [11]
Insect-sting hypersensitivity is the allergic, IgE-mediated response to the venom of stinging insects of the order Hymenoptera. The clinically important families are the bees (the honeybee Apis mellifera), the vespids (yellowjackets and wasps — Vespula and Polistes), and the ants (the jack-jumper Myrmecia in Australasia and the imported fire ant Solenopsis). Venom carries potent allergens — phospholipase, hyaluronidase, melittin, antigen 5 — and in a sensitised child these cross-link venom-specific IgE on mast cells and basophils to release the mediators of anaphylaxis. The reaction is graded by how far beyond the sting site it travels, because that grading is what predicts the next sting and what drives every management decision. [1] [3]
The clinical work splits into the two halves the examination always separates. The first is the acute event: recognise a systemic reaction, remove the embedded venom sac if a bee left one, give intramuscular adrenaline early and escalate if it does not resolve. The second is the long view: confirm which insect caused it, work out how severe the next sting might be, and — for any systemic reaction — offer venom immunotherapy, the one treatment that actually changes the natural history rather than just rescuing the next emergency. A candidate who stops at the adrenaline and forgets the immunotherapy has answered only half the question. [1] [4]
Classification
Insect-sting reactions are classified along two axes that each change what you do: by how far the reaction spread, and by which insect caused it. The spread axis is the one that matters at the bedside, because it alone predicts the next sting and alone determines whether the child needs an autoinjector and venom immunotherapy. The 2011 joint practice parameter, led by Golden and the stinging-insect working group, codified the four-step ladder that clinicians now use. A normal local reaction is swelling and redness confined to the sting site, under about ten centimetres, resolving within hours; it is what almost everyone gets and needs no special workup. A large local reaction extends beyond ten centimetres, often across a whole limb, grows over twenty-four to forty-eight hours, and resolves over days to a week. [1] [8]
The upper two rungs of the ladder are the systemic reactions, and these are the ones that change everything. A systemic cutaneous-only reaction is generalised urticaria, angioedema or itch that travels beyond the sting site but without any airway, cardiovascular or other organ involvement; it is low in mortality but still marks the child out as sensitised and warrants referral. A systemic anaphylactic reaction is the multi-organ event — skin together with airway obstruction, bronchospasm, hypotension or gastrointestinal symptoms — graded as Brown grade two or three, and it is the absolute indication for an adrenaline autoinjector and for venom immunotherapy. Large local reactions, by contrast, are not an indication for an autoinjector in isolation, because the risk of a future sting causing anaphylaxis in a child whose worst reaction was large-local is very low. [1] [6]
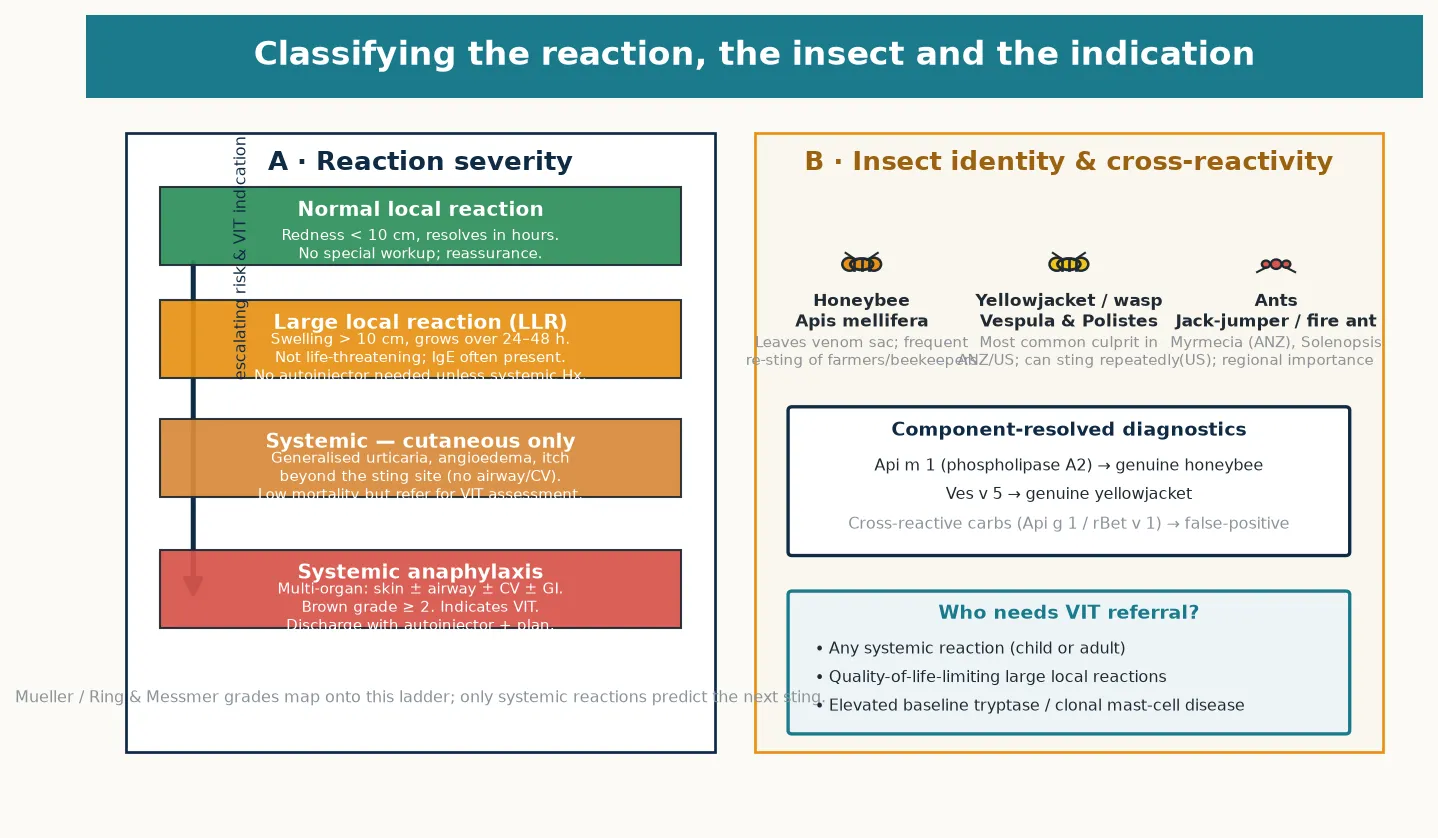
The second axis is the culprit insect, because identifying it directs both the diagnostic testing and the venom immunotherapy extract. The honeybee leaves its venom sac embedded in the skin and so tends to cause reactions in beekeepers and children who step barefoot on flowers; vespids — yellowjackets and paper wasps — are the commonest culprits in most temperate regions, nest near the ground and at picnics, and can sting repeatedly without dying; and the ants carry regional importance, with the jack-jumper ant a leading cause of sting anaphylaxis in south-eastern Australia and the imported fire ant a growing problem in the southern United States. Because venoms share some cross-reactive molecules, a child can test positive to several insects without true allergy to all of them — which is where component-resolved diagnostics (Api m 1 for genuine honeybee, Ves v 5 for genuine yellowjacket) separate the true double-positive from the cross-reactive artefact. [1] [11]
Epidemiology & Risk Factors
Where does insect-sting hypersensitivity sit in a paediatric practice? Most children will be stung many times and tolerate it. Sensitisation — the presence of venom-specific IgE — is common, detectable in perhaps three per cent or more of the general paediatric population by skin or blood testing, but only a small minority of sensitised children ever have a systemic reaction. The lifetime risk that a systemically reactive child will have another systemic reaction on a subsequent sting is meaningful — around thirty to sixty per cent for adults, and somewhat lower in children — and that residual risk is exactly what venom immunotherapy is designed to abolish. The point for the candidate is that sensitisation is common but systemic anaphylaxis is uncommon, so testing everyone who has ever been stung is not the task; testing and treating the child who has had a systemic reaction is. [8] [11]
The risk factors for a severe outcome are the ones the examiner wants named, because they stratify who needs the most aggressive prevention. The single best-validated predictor of sting-anaphylaxis severity is an elevated baseline serum tryptase: the European multicentre study by Ruëff and colleagues showed that the higher the baseline tryptase, the greater the chance of a severe systemic reaction to a sting. An elevated tryptase also points to clonal mast-cell disease — systemic mastocytosis — which is the syndrome of a pathologically expanded, hyper-reactive mast-cell clone driven by a KIT mutation; these patients have severe, sometimes skin-sign-absent sting anaphylaxis, often without any other allergy, and they need lifelong venom immunotherapy. [5] [9]
Other cofactors and amplifiers round out the risk profile. Poorly controlled asthma magnifies the bronchospasm of venom anaphylaxis exactly as it does food anaphylaxis, and optimising asthma control is part of the prevention package. Beta-blocker and angiotensin-converting-enzyme inhibitor therapy blunt the adrenaline response and, where they cannot be ceased, mark the patient out for glucagon and infusion strategies in refractory disease. Age matters in a particular way: although very young children can have systemic reactions, the natural history in children is somewhat more favourable than in adults, with a higher chance that a mild cutaneous systemic reaction will not progress — a nuance the paediatric venom literature has refined, though it never justifies withholding venom immunotherapy from a child with a clear systemic reaction. [11] [2]
Pathophysiology
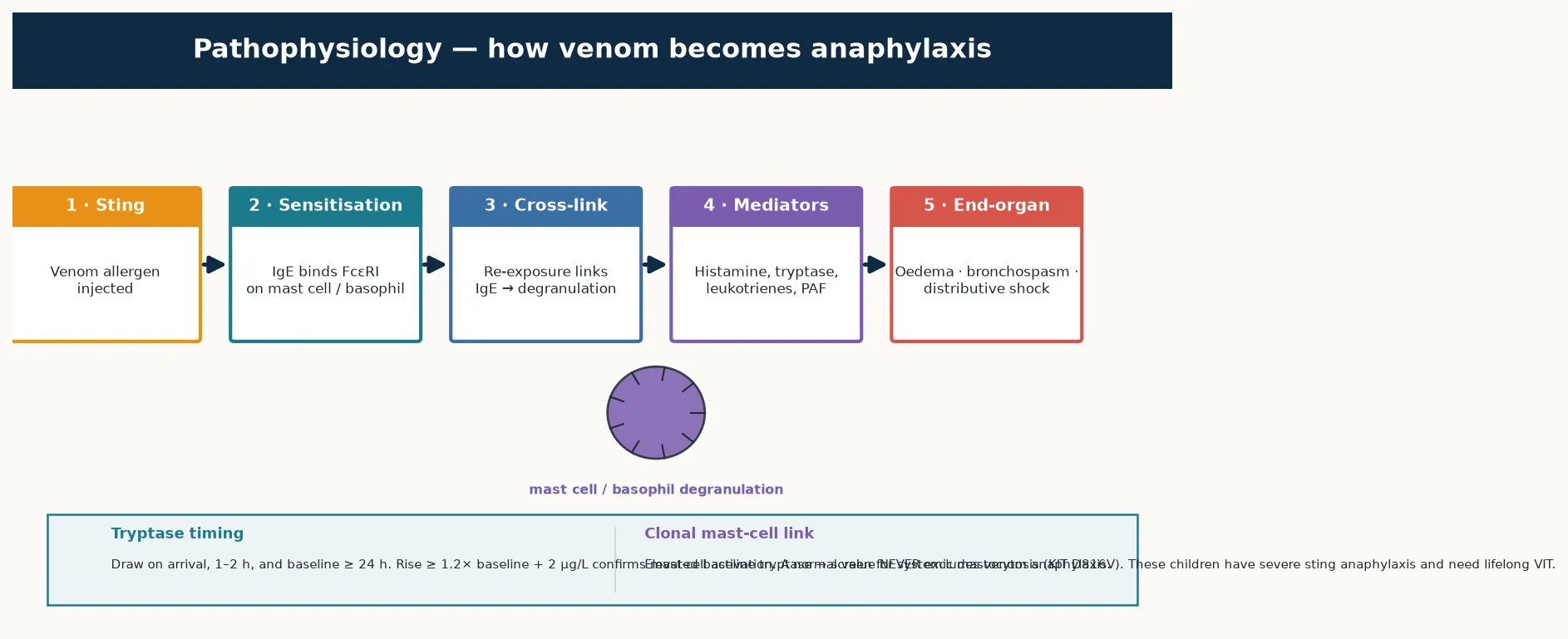
Why does a sting on the foot swell the throat and drop the blood pressure within minutes, and why does one drug reverse it? The answer is the IgE-mediated mast-cell and basophil cascade, and the way adrenaline maps onto every step of it. On first exposure, venom allergens are processed and presented, and a susceptible child makes venom-specific IgE that binds to the high-affinity Fc-epsilon-RI receptor on mast cells and basophils; the child is now sensitised but asymptomatic. On re-exposure — the next sting — the venom allergen cross-links the bound IgE, the receptor clusters, and the mast cell and basophil degranulate, releasing both preformed mediators (histamine, tryptase, heparin) and newly synthesised lipid mediators (leukotrienes, prostaglandins, platelet-activating factor). [8] [6]
These mediators produce the end-organ effects that define the clinical picture and that kill. Histamine and the lipid mediators increase vascular permeability, producing the angioedema that swells the lip and the larynx; they cause vasodilation, producing the flushing and the distributive shock; and they cause bronchospasm, producing the wheeze and the hypoxia. Platelet-activating factor is a particular villain whose level correlates with severity. The reason adrenaline is the perfect antidote is its receptor profile: alpha-1 stimulation vasoconstricts and reverses the oedema and the distributive shock, beta-2 stimulation bronchodilates and stabilises the mast cell membrane to curb further mediator release, and beta-1 stimulation supports the circulation. No other drug covers all three limbs, which is why antihistamines and steroids are adjuncts and never substitutes for adrenaline. [2] [8]
The large local reaction sits on the same pathway but at a different timescale, and understanding it prevents over-treatment. The mediators drive an IgE-mediated late-phase inflammatory response that recruits eosinophils and other cells over hours, producing the slowly enlarging, painful swelling that peaks at one to two days. It is dramatic but, because it is confined to the sting area and lacks systemic mediator spread, it is not life-threatening and does not need adrenaline. The same cascade, in a different balance and in a different patient, produces a large local swelling in one child and circulatory collapse in another — and the difference is often the mast-cell mass, which is why the baseline tryptase matters so much. [6] [8]
The clonal mast-cell link is the pathophysiological reason the severe reactor stands apart. In systemic mastocytosis, an aberrant mast-cell clone — usually carrying the KIT D816V mutation — expands and populates tissues with hyper-reactive mast cells; the baseline tryptase is high, and a sting can trigger a catastrophic, sometimes skin-sign-absent degranulation. These patients are over-represented among fatal and near-fatal sting reactions, they often have no other allergy to explain their history, and they are the group for whom venom immunotherapy is indicated for life. This is why the EAACI guideline and the practice parameters make baseline tryptase measurement part of the workup of every systemic sting reaction, and why an elevated value prompts a mast-cell workup. [9] [3]
Clinical Presentation
The presentation depends entirely on which rung of the ladder the child is on, and the skill is recognising the systemic reaction quickly and not over-treating the large local one. A normal local reaction is immediate pain, a small area of redness and swelling at the sting site, and resolution within hours; the family needs reassurance and simple first aid. A large local reaction develops more slowly — over the first day — as a progressively enlarging, firm, warm, painful swelling that extends well beyond the sting, sometimes across a whole limb, and may peak at twenty-four to forty-eight hours before resolving over several days; it is often mistaken for cellulitis, but its timeframe and the history of a sting distinguish it. [6] [11]
A systemic reaction begins minutes after the sting and involves organs remote from the site. The cutaneous-only systemic reaction is generalised urticaria, flushing, angioedema of the face or lips, and itch beyond the sting — no airway, no breathing, no circulation problem. The systemic anaphylactic reaction adds the dangerous features: rhinitis and a sensation of throat tightness, hoarseness, stridor and drooling from upper-airway oedema; cough, wheeze, tachypnoea and accessory-muscle use from bronchospasm; tachycardia, a narrowed pulse pressure, hypotension, pallor and collapse from distributive shock; and abdominal cramps, vomiting and diarrhoea from gut smooth-muscle contraction. Crucially — as in all anaphylaxis — up to a fifth of systemic sting reactions have no skin signs at all, so a child who collapses or wheezes minutes after a sting is in anaphylaxis until proven otherwise. [2] [7]
The features that change disposition are the red flags, and they are the same as for any anaphylaxis with a sting-specific twist. Stridor or throat closure signals impending airway obstruction from laryngeal oedema; marked wheeze or hypoxia signals severe bronchospasm that asthma will magnify; hypotension or collapse signals distributive shock; any reaction needing two adrenaline doses marks refractory disease; and a child known to have mastocytosis or on a beta-blocker is the severe-reactor phenotype who needs the lowest threshold for escalation. A child with a large local reaction and no systemic features can be managed at home with oral antihistamine and elevation; a child with any red flag needs admission, observation and a clear escalation plan. [2] [5]
Differential Diagnosis
The first differential is within the sting itself: is this a normal local, a large local, or a systemic reaction? The large local reaction is most often mistaken for cellulitis, and the distinction matters because cellulitis gets antibiotics and large local does not. Cellulitis develops over days rather than hours, is accompanied by systemic features of infection such as fever, and occurs without a clear sting or in a child who was already unwell; a large local reaction evolves within a day of a documented sting, is intensely itchy rather than uniformly painful, and lacks fever. When the sting history is clear and the swelling is the expected large local pattern, antibiotics are not needed and an oral antihistamine plus elevation is sufficient. [8] [11]
The systemic sting reaction must be distinguished from the non-allergic toxic effects of multiple stings. A child swarmed by bees and stung dozens of times can develop a toxic systemic illness — vomiting, diarrhoea, dizziness, even haemolysis and rhabdomyolysis from the cumulative venom load — that is not IgE-mediated and does not indicate venom immunotherapy. The history of a mass attack, the dose-related nature of the symptoms, and the absence of typical allergic features (urticaria, rapid progression) help separate toxicity from allergy, though the two can coexist and anaphylaxis can supervene on toxicity. A serum-sickness-like presentation days after a sting is also recognised and is managed supportively. [8] [6]
The other anaphylaxis mimics apply as in any collapse after an outdoor event. Vasovagal syncope produces pallor and brief loss of consciousness that recovers fully once supine, with bradycardia rather than tachycardia and no skin or respiratory involvement — and it is the commonest mimic after a frightening sting. A panic attack brings hyperventilation and paraesthesia without objective hypotension, hypoxia or skin signs. The decisive differentiator is the timeframe and the pattern: anaphylaxis progresses over minutes with multisystem involvement, while syncope resolves and panic lacks objective compromise. When the history is of a sting followed within minutes by multisystem involvement, treat as anaphylaxis first and rationalise later. [2] [7]
Clinical & Bedside Assessment
Assess simultaneously with treatment through the ABCDE approach, because the first minutes decide the outcome. The airway is threatened by laryngeal oedema — listen for stridor, drooling, a muffled voice and look for lip and tongue swelling. Breathing is compromised by bronchospasm — assess the rate, effort, wheeze and oxygen saturation, and remember that a silent chest is pre-arrest. Circulation fails through distributive shock — check the heart rate, blood pressure, capillary refill and level of consciousness, and feel for the warm, floppy peripheries of vasodilation rather than the cold peripheries of cardiogenic shock. The disability and exposure steps complete the picture and expose the sting site and any embedded venom sac. [2] [7]
Positioning is a treatment in itself, and it is often forgotten. Lie the child flat with the legs raised to support venous return — sitting a hypotensive child up can precipitate cardiac arrest from an empty vena cava. Sit the child up if respiratory distress dominates, and place an unconscious or vomiting child in the left lateral position. The embedded honeybee venom sac continues to inject venom, so remove it promptly by scraping sideways with a fingernail or the edge of a card rather than squeezing, which expels more venom. These manoeuvres take seconds and they matter. [2] [1]
The anchoring history runs in parallel with resuscitation and directs the later workup. Establish what stung the child and when, and how the symptoms progressed over minutes — a honeybee often leaves the sac, vespids sting repeatedly, and ant stings have characteristic patterns (the jack-jumper grips and stings repeatedly; fire ants produce clustered sterile pustules). Ask about prior reactions to stings, known venom allergy or immunotherapy, asthma and its control, and the medication list for beta-blockers and angiotensin-converting-enzyme inhibitors. Document whether an autoinjector was given, by whom and when, and record the time, number and timing of all adrenaline doses, the lowest blood pressure and oxygen saturation, and arrange the timed tryptase samples. [1] [3]
Investigations
Anaphylaxis from a sting is a clinical diagnosis and treatment must never wait for any test; the only acute supportive investigation is serum tryptase, and its sole role is to confirm mast-cell activation after the event and to set a baseline. Draw tryptase as soon as possible after the reaction, again at one to two hours (the peak), and at baseline at least twenty-four hours later; a rise to at least 1.2 times the baseline plus two micrograms per litre confirms mast-cell activation. A normal acute tryptase never excludes venom anaphylaxis — food reactions are often tryptase-normal, and venom reactions in mastocytosis can show a blunted rise — so never delay or deny treatment on the result. [2] [5]
The trigger-identification workup belongs in the allergy clinic, not the emergency department, and is done four to six weeks after the reaction so that allergen-specific IgE has had time to develop and the mast-cell activation of the acute event has settled. Two complementary tests are used. Venom-specific serum IgE detects IgE against honeybee, yellowjacket, wasp and (regionally) ant venoms, and is the first test when skin testing is impractical. Skin-prick testing, followed by intradermal testing at increasing dilutions if the prick is negative, is more sensitive and is the gold standard for confirming the culprit and for guiding the venom immunotherapy extract. [1] [3]
Baseline serum tryptase is measured at the workup visit for two reasons that the examiner will probe. First, it is the strongest predictor of severity — the Ruëff data showed that the higher the baseline tryptase, the greater the risk of a severe systemic reaction to a future sting, so it stratifies who most needs venom immunotherapy and who most needs careful build-up. Second, an elevated baseline tryptase (broadly, above about eleven and a half micrograms per litre, or a clearly rising value) points to clonal mast-cell disease and prompts a KIT D816V blood test, a bone-marrow assessment when indicated, and a plan for lifelong venom immunotherapy. Component-resolved diagnostics — Api m 1, Ves v 5 and others — separate genuine double-sensitisation from cross-reactive artefact when the standard tests are positive to several insects. [5] [9]
Management — Resuscitation
The acute management of systemic sting anaphylaxis is the same adrenaline-first algorithm as any anaphylaxis, applied without hesitation. Recognise the reaction and call for help. Remove the trigger — scrape away any embedded honeybee venom sac. Lie the child flat with legs raised (sit up if breathing is distressed, left lateral if unconscious). Give intramuscular adrenaline into the anterolateral thigh by weight band: 150 micrograms for a child of 7.5 to 20 kilograms (ASCIA), 300 micrograms for over 20 to 50 kilograms (or any child over about twelve years), and 500 micrograms for the larger adolescent, repeating every five minutes if there is no response. [2] [1]
Give high-flow oxygen for hypoxia or a saturation below ninety-four per cent, and give an intravenous crystalloid bolus of ten millilitres per kilogram for shock, repeated to twenty millilitres per kilogram. Add an inhaled bronchodilator for refractory wheeze that persists after adrenaline. Antihistamines, H2 blockers and corticosteroids are adjuncts for symptom control only — never a substitute for adrenaline and never a reason to delay it. The safety message is the same as for all anaphylaxis: intramuscular adrenaline in correct weight-banded doses is safe, and the risk of giving it when anaphylaxis is merely suspected is far smaller than the risk of withholding it from a child who has it. [2] [1]
Adrenaline (epinephrine) — intramuscular, anterolateral thigh
Management — Definitive & Stepwise
The definitive algorithm runs from the acute event through to five years of protection, and it has five linked steps. The first is the acute resuscitation above. The second is observation for the biphasic reaction — symptoms can recur one to seventy-two hours after apparent recovery, in around three to five per cent and higher in severe reactions — so apply a severity-graded decision: observe for at least six hours for a mild-moderate single-dose presentation with full recovery and good access, and admit overnight for any reaction needing two or more adrenaline doses, any severe or refractory reaction, poorly controlled asthma, beta-blocker therapy, mastocytosis or poor access to care. [2] [6]
The third step is trigger confirmation in the allergy clinic at four to six weeks: venom-specific IgE and skin testing to identify the culprit, a baseline tryptase to stratify severity and screen for mast-cell disease, and component-resolved diagnostics when double-positivity needs resolving. The fourth step — the distinctive fellowship content — is the venom immunotherapy decision. For any systemic reaction, whether cutaneous-only or anaphylactic, refer for venom immunotherapy using the relevant insect extract; the Cochrane review by Boyle and colleagues confirmed that it substantially reduces the risk of a systemic reaction to a subsequent sting, and the effect sizes translate to roughly ninety to ninety-eight per cent protection once maintenance is reached. [4] [1]
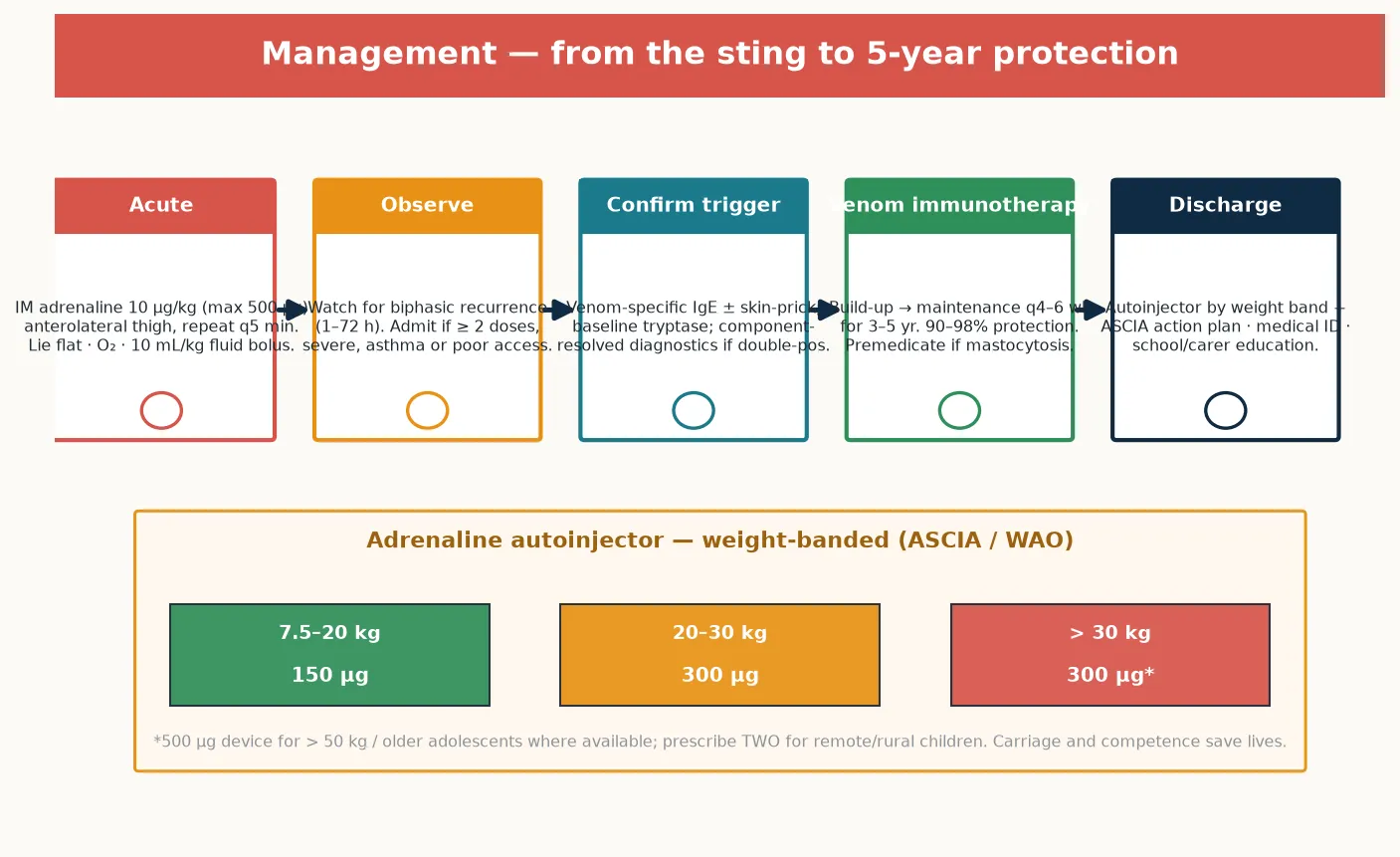
Venom immunotherapy itself is a build-up to a maintenance dose, then maintenance injections every four to six weeks for three to five years, and the candidate should know its shape. Conventional build-up takes several weeks to months; clustered, rush and ultrarush protocols reach maintenance in days and are used when rapid protection is needed, with antihistamine premedication to reduce reactions. The maintenance dose is typically 100 micrograms of the relevant venom — equivalent to about two stings — and once it is reached the protection is robust. Venom immunotherapy is indicated for any systemic reaction to a sting; it is generally not indicated for large local reactions alone in children, because the future risk of anaphylaxis is low, though quality-of-life burden can occasionally justify it. Premedication and a slower build-up are used for mastocytosis, where reactions to the immunotherapy itself are more likely. [3] [10]
The fifth step is the discharge prevention package, and it is non-negotiable. Every child treated for a systemic sting reaction leaves with one or two adrenaline autoinjectors by weight band, a written anaphylaxis action plan, medical identification, and a family and school who have been taught avoidance (footwear, avoiding nests and picnics, not flailing at flying insects) and how and when to use the device. The package is completed by the allergy-clinic referral for the workup and the venom immunotherapy decision, because the autoinjector rescues the next reaction but only venom immunotherapy prevents it. [2] [6]
Specific Subtypes & Scenarios
A few scenarios recur in the examination because each tests a different pitfall. The child with a single large local reaction and no systemic features is the commonest presentation and the test is restraint: reassure, give an oral antihistamine, elevate the limb, and do not prescribe an autoinjector or venom immunotherapy on the basis of the large local reaction alone — the future risk of anaphylaxis is low. Explain to the family what a systemic reaction would look like and what to do if one ever occurs, and offer an allergy review if reactions are frequent or burdensome. [1] [11]
The child with a systemic cutaneous-only reaction — generalised urticaria and angioedema after a sting, but no airway, breathing or circulation involvement — sits in a grey zone that the paediatric literature has refined. The risk of progression to a more severe reaction on a future sting is lower in children than in adults, and some guidelines allow observation rather than autoinjector prescription for a first, mild, cutaneous-only reaction in a young child with good access to care. The safe fellowship answer, however, is to refer all systemic reactions for venom assessment, to consider an autoinjector when access is poor or the family is anxious, and to offer venom immunotherapy when the family and clinician judge the protection worthwhile. [11] [3]
The child with systemic anaphylaxis and an elevated baseline tryptase — or known mastocytosis — is the severe-reactor scenario and the one the examiner uses to test depth. These children have a high risk of severe, skin-sign-absent sting anaphylaxis, they are over-represented in near-fatal and fatal cases, and the answer is lifelong venom immunotherapy, an adrenaline autoinjector, a tryptase-driven mast-cell workup (KIT D816V, and bone-marrow assessment when indicated), and a clear plan that the school and family understand. The child on a beta-blocker who has sting anaphylaxis is the refractory scenario: adrenaline may be blunted, glucagon is the antidote, and an adrenaline infusion with senior or PICU support is the escalation. [9] [2]
| Scenario | Acute | Long-term |
|---|---|---|
| Large local reaction only | Antihistamine, elevation, reassurance | No autoinjector / VIT; safety-net |
| Systemic cutaneous-only | Observe; adrenaline if any organ beyond skin | Refer; autoinjector if poor access; consider VIT |
| Systemic anaphylaxis | IM adrenaline now, repeat q5 min; fluids | Autoinjector + plan + VIT referral |
| Anaphylaxis + mastocytosis | Adrenaline early; expect no rash | Lifelong VIT, autoinjector, KIT workup |
| Anaphylaxis + beta-blocker | Adrenaline; add glucagon if refractory | Switch drug; infusion pathway; VIT |
Complications & Pitfalls
The single most important pitfall is the failure to recognise and treat a systemic reaction because the clinician waited for a rash, treated with antihistamine first, or mistook a sting collapse for a vasovagal event. Up to a fifth of systemic sting reactions have no skin signs, and in mastocytosis that proportion is higher still; a child who collapses or wheezes minutes after a sting is in venom anaphylaxis until proven otherwise. The corollary error is treating a large local reaction as if it were anaphylaxis — prescribing an autoinjector and frightening the family — which over-medicalises a non-life-threatening event and erodes trust. [2] [1]
The diagnostic pitfalls centre on timing and on cross-reactivity. Testing too early — in the first days after the reaction — can yield a false-negative because allergen-specific IgE has not yet risen; the workup belongs at four to six weeks. Cross-reactive carbohydrate determinants can produce false-positive IgE to several insects, and only component-resolved diagnostics (Api m 1, Ves v 5) separate the true double-positive from the artefact; getting this wrong means immunising against the wrong insect or against two when one would do. Missing an elevated baseline tryptase is the most consequential omission, because it both predicts severe recurrence and points to mastocytosis, whose management is qualitatively different. [5] [9]
The discharge pitfalls that set up the next reaction
Sending a child home without an autoinjector, a written action plan and an allergy referral; failing to measure a baseline tryptase; forgetting to arrange venom immunotherapy for a systemic reaction; and not educating the school and family in avoidance and device use — each of these is a recognised, avoidable contributor to recurrent and potentially fatal sting anaphylaxis. The autoinjector rescues the next reaction; venom immunotherapy prevents it; both must be in place. [2] [4]
Prognosis & Disposition
Most children who receive early adrenaline for a systemic sting reaction recover fully, and venom immunotherapy then transforms the long-term outlook. Once a maintenance venom immunotherapy dose is reached, the protection against a systemic reaction to a subsequent sting is roughly ninety to ninety-eight per cent, and after three to five years of maintenance many children can stop treatment with a sustained low risk — though those with mastocytosis or severe initial reactions are usually treated for life. The candidate should hold both numbers: the untreated residual risk of a systemic reaction on re-sting (thirty to sixty per cent in adults, lower in children), and the treated risk (a few per cent). [4] [3]
The disposition decision after the acute event is the severity-graded observation rule. Observe for at least six hours for a mild-moderate single-dose presentation that has fully recovered with good access to care. Admit overnight for any reaction needing two or more adrenaline doses, any severe or refractory reaction, poorly controlled asthma, beta-blocker or angiotensin-converting-enzyme inhibitor therapy, mastocytosis, or poor access to care; manage refractory shock or airway compromise in a high-dependency or PICU setting. Discharge is always with the prevention package: autoinjector, action plan, medical identification, allergy referral and school education. [2] [7]
Special Populations
Children with mastocytosis are the defining special population for venom hypersensitivity and the one the examiner uses to test whether the candidate knows the tryptase-mast cell link. They have a high baseline tryptase, an expanded hyper-reactive mast-cell mass, and a tendency to severe, often skin-sign-absent sting anaphylaxis; they may have no other allergy to explain their history. The management is lifelong venom immunotherapy, an adrenaline autoinjector, a KIT-driven workup, and explicit education that the absence of a rash does not exclude anaphylaxis. This single group distils the whole topic: measure the tryptase, recognise the clone, protect for life. [9] [3]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families, face particular regional and access realities. In Australasia the jack-jumper ant (Myrmecia) is a leading cause of sting anaphylaxis and has dedicated ant-venom immunotherapy programmes; fire ants are a regional issue in the southern United States. Address autoinjector cost and access barriers, deliver culturally safe education with trained interpreters, and ensure equity in the discharge equipment — a rural or remote child needs two devices and a competent family because retrieval is hours away. [11] [3]
Children with poorly controlled asthma, adolescents, and children in out-of-home care or school and childcare settings round out the populations who need tailored plans. Asthma magnifies bronchospasm and must be optimised; adolescents share the risk-taking and device-hesitancy that mark all allergy in this age group; and schools and carers must hold a copy of the action plan, be trained in the autoinjector, and have a clear sting-avoidance and emergency-response protocol. Children with complex chronic illness or on beta-blockade need individualised escalation plans with glucagon available where the beta-blocker cannot cease. [2] [7]
Evidence, Guidelines & Regional Differences
The evidence base for insect-sting hypersensitivity is unusually strong for an allergy topic, because venom immunotherapy is one of the best-studied desensitising treatments in medicine. The 2011 joint practice parameter (Golden, Moffitt, Nicklas and the stinging-insect working group) codified the reaction ladder, the testing strategy and the venom immunotherapy indications, and it remains the North American standard; the 2023 anaphylaxis practice parameter update (Golden, Wang, Waserman and colleagues) refreshed the adrenaline-first acute algorithm and the observation rules. The EAACI guideline on allergen immunotherapy for Hymenoptera venom allergy (Sturm, Varga, Roberts and colleagues, 2018) is the European standard, and Golden's successive reviews synthesise the epidemiology and natural history. [1] [2]
The Cochrane review by Boyle and colleagues established the efficacy of venom immunotherapy in reducing systemic reactions to subsequent stings, and the Ruëff European multicentre study established baseline tryptase as the strongest predictor of severity and the screen for clonal mast-cell disease — the two findings that most changed modern practice. The paediatric venom literature, including the Giovannini review of Hymenoptera venom allergy in children, refines the natural history in the young and supports venom immunotherapy in children with systemic reactions while cautioning against over-treatment of large local reactions. Severino's and Bilò's work on venom immunotherapy safety and the clonal mast-cell association complete the picture. [4] [5]
The regional differences are real and the examiner may probe them. In Australasia, ASCIA provides the action plans, autoinjector bands and the jack-jumper ant immunotherapy programmes; in the United Kingdom, NICE and the Resuscitation Council guide anaphylaxis assessment and the allergy referral; in North America, the joint practice parameter and the American Academy of Pediatrics guidance apply, with fire ant immunotherapy in the south. The convergence is the important point: everywhere, the acute algorithm is adrenaline first, intramuscular and early; everywhere, a systemic reaction triggers an allergy referral and a venom immunotherapy decision; everywhere, the discharge package is autoinjector, action plan and education. The controversies are narrower — the duration of venom immunotherapy in children, whether to immunise large local reactors for quality of life, and the optimal build-up protocol in mastocytosis. [3] [11]
Exam Pearls
Insect-sting hypersensitivity in one timeline
The high-yield points for the examination, distilled: a normal local reaction is under ten centimetres and hours; a large local reaction is over ten centimetres and one to two days; only systemic reactions predict the next sting and indicate venom immunotherapy. The culprits are honeybee (leaves the sac), vespid (yellowjacket and wasp, repeat stings) and ants (jack-jumper in Australasia, fire ant in the southern United States). Intramuscular adrenaline into the anterolateral thigh is 150 micrograms for 7.5–20 kg, 300 micrograms for >20–50 kg, 500 micrograms for larger adolescents (ASCIA weight bands; APLS also uses age bands), repeated every five minutes. [2] [11]
Baseline serum tryptase is the strongest predictor of severity and the screen for clonal mast-cell disease (KIT D816V); an elevated value means a severe-reactor phenotype and lifelong venom immunotherapy. Venom immunotherapy gives ninety to ninety-eight per cent protection once maintenance is reached, after three to five years of treatment; it is indicated for any systemic reaction and not for large local reactions alone. The discharge package is non-negotiable: adrenaline autoinjector by weight band, written action plan, medical identification, allergy referral, and family and school education. [4] [9]
References
- [1]Golden DB; Moffitt J; Nicklas RA; et al Stinging insect hypersensitivity: a practice parameter update 2011. J Allergy Clin Immunol, 2011.PMID 21458655
- [2]Golden DBK; Wang J; Waserman S; et al Anaphylaxis: A 2023 practice parameter update. Ann Allergy Asthma Immunol, 2024.PMID 38108678
- [3]Sturm GJ; Varga EM; Roberts G; et al EAACI guidelines on allergen immunotherapy: Hymenoptera venom allergy. Allergy, 2018.PMID 28748641
- [4]Boyle RJ; Elremeli M; Hockenhull J; et al Venom immunotherapy for preventing allergic reactions to insect stings. Cochrane Database Syst Rev, 2012.PMID 23076950
- [5]Ruëff F; Przybilla B; Biló MB; et al Predictors of severe systemic anaphylactic reactions in patients with Hymenoptera venom allergy: importance of baseline serum tryptase-a study of the European Academy of Allergology and Clinical Immunology Interest Group on Insect Venom Hypersensitivity. J Allergy Clin Immunol, 2009.PMID 19895993
- [6]Bilò MB; Tontini C; Martini M; et al Clinical aspects of hymenoptera venom allergy and venom immunotherapy. Eur Ann Allergy Clin Immunol, 2019.PMID 31594296
- [7]Vetander M; Helander D; Flodström C; et al Anaphylaxis and reactions to foods in children--a population-based case study of emergency department visits. Clin Exp Allergy, 2012.PMID 22417215
- [8]Golden DB Anaphylaxis to insect stings. Immunol Allergy Clin North Am, 2015.PMID 25841552
- [9]Bonadonna P; Scaffidi L Hymenoptera Anaphylaxis as a Clonal Mast Cell Disorder. Immunol Allergy Clin North Am, 2018.PMID 30007463
- [10]Severino M; Simioni L; Bonadonna P; et al Efficacy and safety of honeybee and wasp tyrosine-adsorbed venom immunotherapy. World Allergy Organ J, 2019.PMID 31768218
- [11]Giovannini M; Mori F; Barni S; et al Hymenoptera venom allergy in children. Ital J Pediatr, 2024.PMID 39707411
- [12]Golden DBK Update in stinging insect hypersensitivity. Allergy Asthma Proc, 2025.PMID 40958191