Paeds · allergy-and-immunology
Latex allergy
Also known as Natural rubber latex allergy · NRL allergy · Latex hypersensitivity · Hevea brasiliensis allergy · Rubber allergy
A fellowship approach to natural rubber latex allergy in children: distinguish Type I IgE-mediated allergy (the dangerous form causing contact urticaria to intraoperative anaphylaxis) from Type IV contact dermatitis and irritant dermatitis; identify the high-risk child (spina bifida, multiple surgeries, atopy); explain the Hev b component framework and latex-fruit syndrome cross-reactivity; apply skin-prick, serum IgE and component-resolved diagnostics; manage with strict latex avoidance, latex-safe surgery protocols, and adrenaline where systemic risk exists; and understand the epidemiological decline driven by powder-free low-protein glove primary prevention across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A six-year-old with spina bifida develops generalised urticaria, wheeze and hypotension 40 minutes into an elective orthopaedic procedure. The anaesthetist has given no new drug since induction. That scenario — delayed intraoperative collapse in a high-risk child — is the archetype of latex anaphylaxis, and it is why every spina bifida patient is managed latex-safe until proven otherwise. [12] [17]
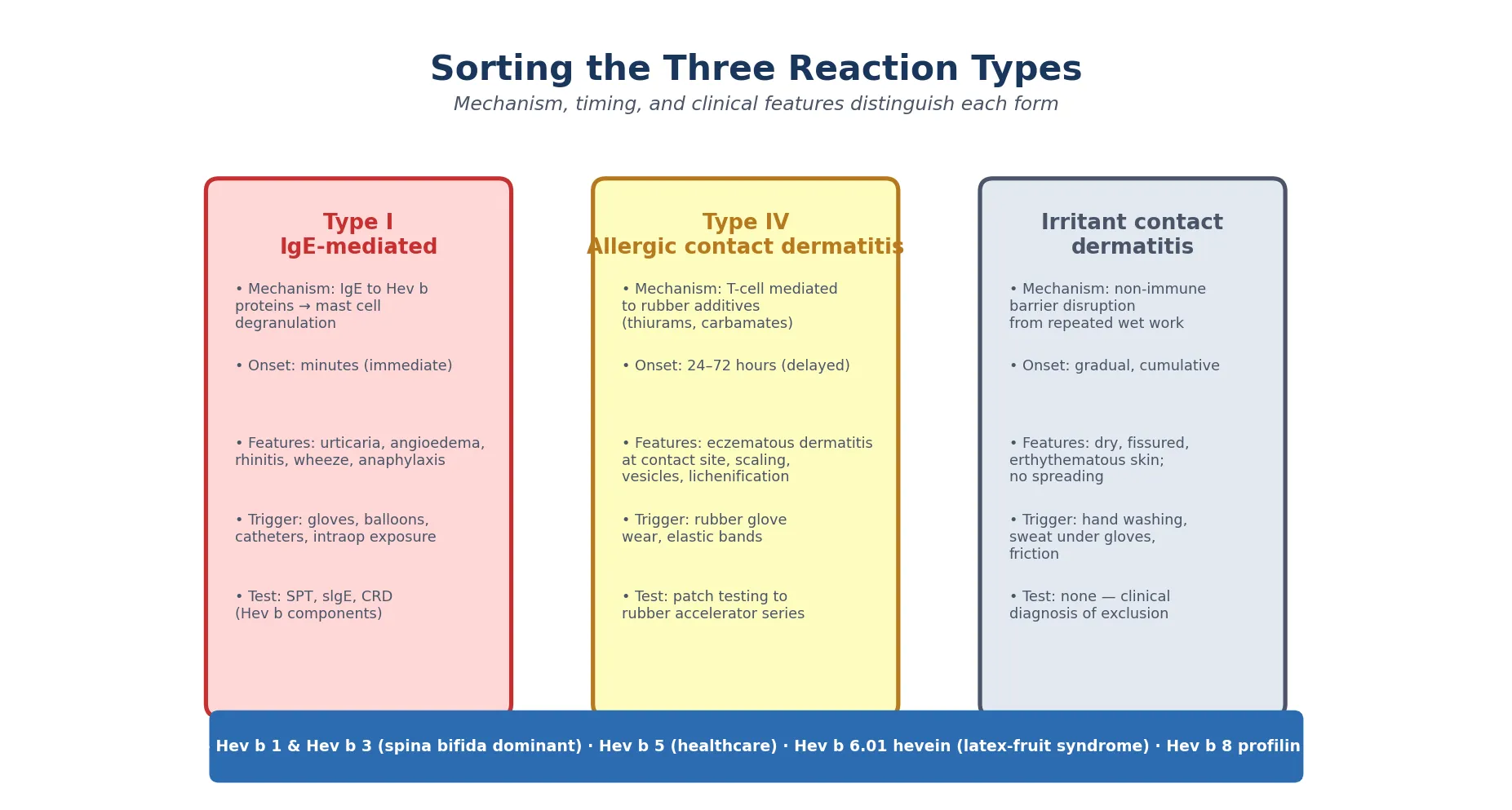
Natural rubber latex (NRL) allergy is an immune-mediated hypersensitivity reaction to proteins in the milky sap of the rubber tree Hevea brasiliensis. The term covers three distinct mechanisms, and confusing them is the commonest error in this topic. Type I is IgE-mediated: immediate, mast-cell-driven, and capable of causing urticaria, wheeze, and anaphylaxis. Type IV is T-cell-mediated allergic contact dermatitis, a delayed eczematous reaction to the chemical accelerators (thiurams, carbamates) added during rubber manufacture. Irritant contact dermatitis is non-immune barrier disruption from wet work and friction. [2] [3]
Only Type I is the dangerous form. It can kill a child on the operating table, which is why latex-safe protocols exist. The other two are chronic skin conditions that impair quality of life and barrier function but do not cause immediate life-threatening reactions. Holding that distinction makes the classification, the diagnosis, and the management fall into place. [1] [4]
The epidemiological backdrop shapes everything: latex allergy was epidemic in the late 1980s and 1990s, then fell sharply after healthcare systems switched to powder-free, low-protein gloves. It is now uncommon in low-risk populations but remains a live threat in the spina bifida, surgical, and previously-sensitised child. [9] [11]
Classification
Sort every child through two questions: what is the immune mechanism, and — if it is Type I — which Hev b component is driving the sensitisation? The answer to the first sets the management, and the answer to the second sets the risk. [2] [8]
By immune mechanism
The three forms of latex sensitivity are completely different diseases that share a trigger material. Type I IgE-mediated latex allergy fires within minutes of contact: contact urticaria at the exposure site, generalised urticaria, angioedema, rhinitis, wheeze, and in the worst case anaphylaxis with hypotension and cardiovascular collapse. The trigger is the latex protein itself. [1] [2]
Type IV allergic contact dermatitis presents 24 to 72 hours after exposure as an eczematous, well-demarcated eruption at the rubber-contact site — typically the dorsal hands under gloves or the wrists under elastic. The mechanism is T-cell-mediated delayed hypersensitivity to rubber accelerators and additives (thiurams, carbamates, mercaptobenzothiazole), not to latex protein. Patch testing to the rubber additive series, not latex protein testing, confirms it. [4]
Irritant contact dermatitis is non-immune: cumulative barrier disruption from wet work, sweating under gloves, hand washing, and friction. The skin is dry, fissured and erythematous, but there is no spreading, no vesiculation, and no immune mechanism. It is a diagnosis of exclusion. [3]
By Hev b component (for Type I)
The major IgE-reactive latex allergens are the Hev b proteins, named for Hevea brasiliensis. Knowing which component drives a child's sensitisation sorts genuine latex allergy from cross-reactive noise, and it guides whether non-latex-safe surgery may be acceptable. [8] [14]
Hev b 1 & Hev b 3
Genuine · high risk
- Rubber elongation factor and a homologous particle-bound protein
- Dominant sensitising allergens in spina bifida and multi-surgery children
- Reflect direct mucosal exposure to raw latex particles from catheters and gloves
- High clinical relevance — genuine latex allergy with anaphylaxis risk
Hev b 5
Genuine · high risk
- Acidic protein, major allergen in healthcare workers and children
- Associated with systemic reactions and latex-fruit syndrome overlap
- High clinical relevance — treat as genuine latex allergy
- Confirm with component-resolved diagnostics alongside Hev b 1
Hev b 6.01 (hevein)
Genuine · fruit cross-reactivity
- N-terminal hevein domain cross-reacts with plant class I chitinases
- Drives latex-fruit syndrome: banana, kiwi, avocado, chestnut, passion fruit
- High clinical relevance for both latex and fruit reactions
- Component testing identifies the cross-reactive mechanism
Hev b 8 (profilin)
Cross-reactive · low risk
- Profilin — ubiquitous actin-binding protein shared across pollens and plant foods
- Often represents pollen-driven cross-reactive sensitisation, not genuine latex allergy
- Low clinical reactivity — may tolerate latex exposure
- Monosensitised Hev b 8 patients may safely undergo non-latex-safe surgery (Quercia 2009)
Epidemiology & Risk Factors
Latex allergy tells a public-health success story. Prevalence rose steeply from the late 1980s through the mid-1990s as universal precautions drove massive glove use, peaked around the turn of the millennium, then fell sharply after healthcare systems adopted powder-free, low-protein gloves. [4] [9]
The decline was real and measurable. The German primary prevention study showed that switching to powder-free, low-protein gloves dramatically reduced sensitisation in healthcare workers — evidence that a supply-chain change could prevent allergy at population scale. The profile-shift paper documents the changing sensitisation pattern over 20 years, with declining overall prevalence but persistence in high-risk groups. [11] [9]
Risk concentrates in five groups. Children with spina bifida (myelomeningocele) and other neural tube defects are the single highest-risk population — historically 30 to 70 per cent were sensitised, because of repeated bladder catheterisations, multiple surgeries, and early heavy latex exposure from ventriculoperitoneal shunts and urological procedures. [5] [3]
Children with multiple surgical procedures (urological reconstructions, orthopaedic corrections, cardiac surgery) accumulate cumulative latex exposure that drives sensitisation. Long-term indwelling latex devices — catheters, tubes, VP shunts — maintain continuous mucosal contact. Atopy (eczema, asthma, allergic rhinitis) raises the background risk of latex sensitisation, and latex-fruit syndrome affects up to half of latex-allergic patients. [1] [6]
Pathophysiology
The conceptual core is IgE sensitisation through repeated exposure, then mast-cell degranulation on re-exposure — the same cascade that drives all Type I allergy, but with a specific set of proteins and a characteristic intraoperative catastrophe pattern. [2] [4]
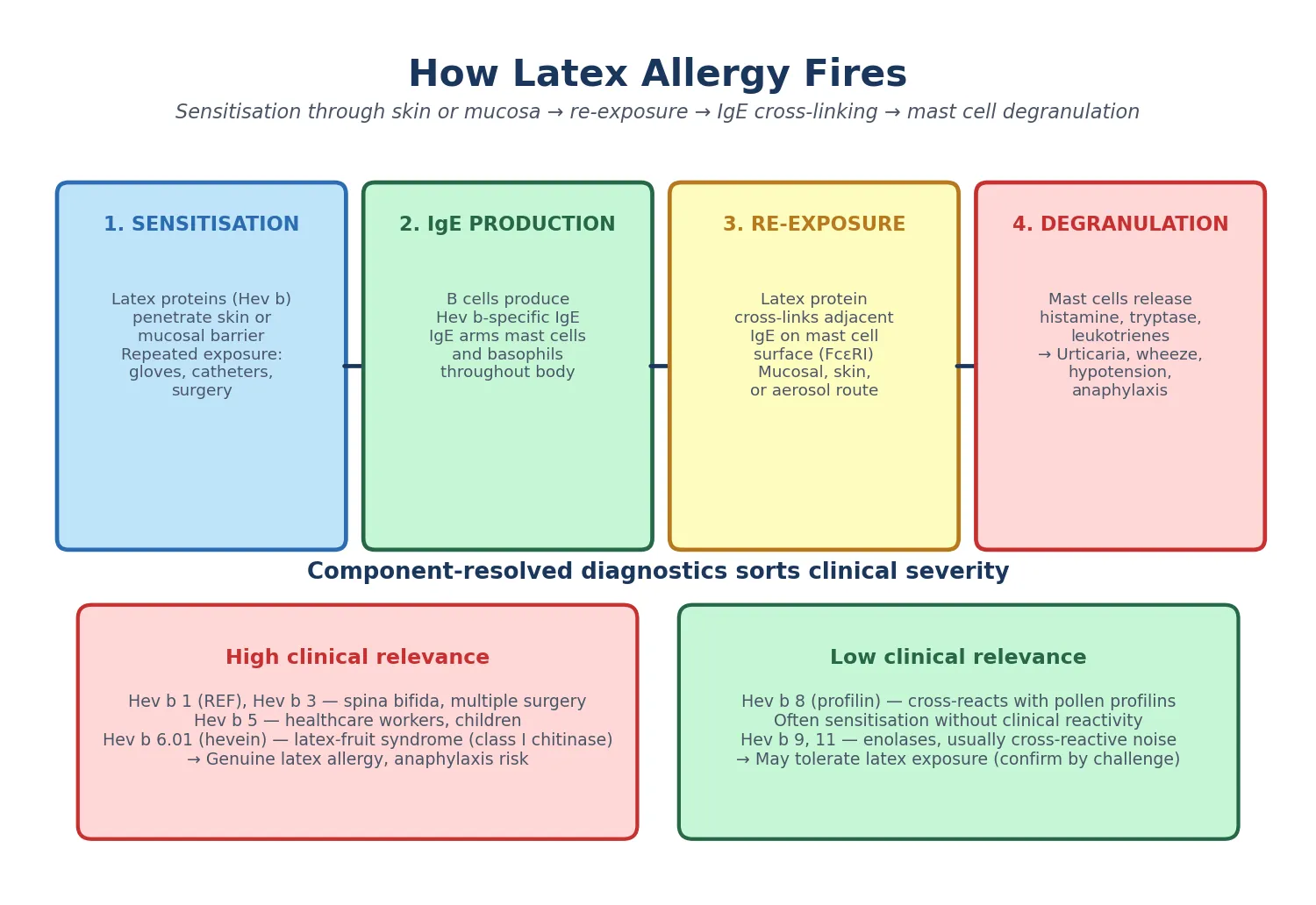
Sensitisation begins when latex proteins (Hev b allergens) penetrate the skin or a mucosal surface during repeated exposure. Antigen-presenting cells process the Hev b proteins and present peptides to T-helper-2 cells, which drive B-cell class-switching to Hev b-specific IgE production. The IgE then arms mast cells and basophils throughout the body by binding the high-affinity receptor Fc-epsilon-RI on their surface. The child is now sensitised but may be asymptomatic — and sensitisation is not the same as clinical allergy. [3] [8]
On re-exposure, multivalent latex protein cross-links adjacent IgE-Fc-epsilon-RI complexes on the mast cell surface, triggering degranulation with release of histamine, tryptase, prostaglandins and leukotrienes. The result is immediate urticaria, angioedema, bronchospasm, hypotension, and potentially full anaphylaxis. [1] [4]
The route of exposure shapes the clinical picture in ways that matter for the exam. Skin contact causes contact urticaria at the exposure site. Mucosal exposure — oral during dental work, vaginal, or surgical via the peritoneum and wound — drives rapid systemic absorption, which is the mechanism of intraoperative anaphylaxis. Aerosolised cornstarch glove-donning particles carrying latex protein cause airborne rhinitis and asthma, a problem largely eliminated by powder-free glove policies but still relevant when old or imported stock persists. [4] [11]
Latex-fruit syndrome arises because Hev b 6.01 (hevein) shares epitopes with class I chitinases in certain fruits — Pers a 1 in avocado, Cas s 1 in chestnut, and analogous defence proteins in banana, kiwi, passion fruit and tomato. IgE primed by latex cross-reacts with these plant proteins, producing allergic reactions to foods the child may never have linked to latex. [6] [7]
Hev b 8 (profilin) sensitisation represents a different, gentler pattern. Profilins are ubiquitous actin-binding proteins shared across pollens and plant foods, so Hev b 8 positivity often reflects broad cross-reactive sensitisation with low genuine latex clinical reactivity. This is why a child with only Hev b 8 positivity may tolerate latex exposure safely — a distinction that prevents unnecessary restriction and surgical over-precaution. [8] [10]
Clinical Presentation
Match the pattern to the mechanism. Each of the three forms of latex sensitivity has its own tempo, and reading the tempo tells you which disease you are dealing with. [1] [3]
Type I reactions present within minutes of latex contact. The spectrum runs from local contact urticaria at the exposure site (hands under gloves, lips after balloon blowing, oral mucosa after dental work) through generalised urticaria, angioedema, conjunctivitis, rhinitis and wheeze, to full anaphylaxis with hypotension and cardiovascular collapse. The timing is immediate — minutes, not hours. [2] [4]
Intraoperative anaphylaxis is the most feared presentation and historically made latex the leading cause of intraoperative anaphylaxis in children. It is the timing that discriminates: latex anaphylaxis typically occurs 30 to 60 minutes into the procedure, after mucosal absorption via the peritoneum or surgical wound. This is later than the immediate reactions caused by anaesthetic induction agents, neuromuscular blockers, or antibiotics, which fire within minutes of administration at induction. Any intraoperative cardiovascular event in a high-risk child after the first half-hour is latex until proven otherwise. [12] [17]
Airborne latex allergy presents as seasonal or occupational rhinitis, conjunctivitis and asthma, caused by inhalation of cornstarch glove-donning powder that has adsorbed latex protein. This was a major occupational health problem in the 1990s and is now largely eliminated by powder-free policies, but the mechanism is examinable. [4] [11]
Type IV allergic contact dermatitis presents 24 to 72 hours after exposure as an eczematous, pruritic, well-demarcated eruption at the rubber-contact site. Think dorsal hands under gloves, or wrists under elastic bands. Chronic cases show scaling, fissuring, vesiculation and lichenification. The delay and the eczematous morphology distinguish it from the immediate urticaria of Type I. [4]
Irritant contact dermatitis presents as dry, fissured, erythematous skin from cumulative barrier disruption by wet work, sweating under gloves, and friction. It is gradual, non-spreading, and lacks the vesicular phase of allergic dermatitis. [3]
The first systemic presentation in a child may be intraoperative anaphylaxis during an elective procedure, which is why preoperative latex-risk screening of spina bifida and multi-surgery children is mandatory. Never gamble on the first procedure. [5] [15]
Differential Diagnosis
The error is labelling any rubber-related skin problem as 'latex allergy' without separating the mechanism, or missing latex entirely when a child presents with food reactions or perioperative collapse. [1] [13]
| Finding | Prefer | Discriminators | Action |
|---|---|---|---|
| Immediate urticaria, wheeze or collapse with latex | Type I IgE latex allergy | Minutes onset; spina bifida or surgical history | Adrenaline; latex-safe environment |
| Eczema at glove-contact site, 24 to 72 h delay | Type IV contact dermatitis | Delayed; eczematous; rubber additives | Patch testing; accelerator-free gloves |
| Dry fissured hands from wet work | Irritant dermatitis | Non-immune; gradual; no spreading | Emollients; reduce wet work |
| Intraoperative collapse 30 to 60 min in | Latex anaphylaxis | Spina bifida, multi-surgery; delayed onset | IM adrenaline; latex-safe protocol |
| Collapse immediately after induction | Drug anaphylaxis (NMBAs, antibiotics) | Minutes after drug; at induction | IM adrenaline; drug allergy workup |
| Oral itch to raw apple, cooked tolerated | Pollen-food syndrome | Pollen-sensitised; raw only | History; component diagnostics |
The two hardest separations are perioperative and dietary. Intraoperatively, latex anaphylaxis is distinguished from drug-triggered anaphylaxis by the delayed onset (30 to 60 minutes versus immediate at induction), the spina bifida risk profile, and by serial tryptase plus latex-specific IgE. Dietary reactions to banana, kiwi, avocado and chestnut should prompt latex evaluation for latex-fruit syndrome, because the latex connection may be invisible to the family. [6] [7]
Distinguish latex allergy from other physical urticarias (cold, cholinergic, vibratory) by the reproducible latex-specific trigger, and from hereditary or acquired angioedema by the presence of urticaria and the temporal link to latex. [13]
Clinical & Bedside Assessment
In a suspected acute reaction, assessment is safety-first. Run an ABCDE approach and decide at the bedside whether this is localised (skin only) or systemic (airway, breathing, circulation involvement) — because that single distinction sets the immediate plan. [15]
Take a focused latex exposure history once the child is safe. Ask about gloves, balloons, rubber bands, condoms, dental dams, catheters, erasers, swimming caps, elastic in clothing, pacifiers and bottle nipples, and any recent surgical or dental procedure. The history is more diagnostic than any single test. [1] [3]
Establish the risk profile deliberately. Spina bifida or neural tube defect, the number of prior surgeries, any indwelling latex devices, atopic background (eczema, asthma, rhinitis), and any prior reactions to banana, kiwi, avocado or chestnut — these frame the pre-test probability and guide whether latex-safe precautions are needed before the results return. [5] [6]
Examine the hands for dermatitis (Type IV or irritant pattern), the skin for urticaria, and the respiratory system for wheeze. In the stable clinic patient, screen for atopic stigmata. Decide at the bedside whether the child needs latex-safe precautions for an upcoming procedure — any child with spina bifida or a convincing latex reaction history warrants a full latex-safe pathway until tests clarify. [1] [4]
Name the red flags explicitly so they are not missed: intraoperative cardiovascular collapse, rapid-onset generalised urticaria under anaesthesia, or any airway involvement. Each demands immediate adrenaline and a latex-safe environment. [12] [17]
Investigations
Tests support a compatible history; they never replace it. A positive latex-specific IgE or skin-prick in a child who tolerates latex is sensitisation, not clinical allergy, and acting on it alone causes over-restriction. [1] [9]
Skin-prick testing (SPT) with commercial latex extract is the most sensitive test for IgE-mediated latex allergy. It carries a small but real risk of systemic reaction, so it should be performed where resuscitation facilities are available, starting with a diluted extract. Availability of commercial latex SPT reagents varies by country. [2] [3]
Serum latex-specific IgE (ImmunoCAP) gives sensitisation data and is useful when SPT is unavailable or contraindicated. Sensitivity and specificity are good but not perfect, so use it as a pointer rather than a verdict. [1]
Component-resolved diagnostics (CRD) is the tool that sorts genuine latex allergy from cross-reactive noise. Using the ISAC microarray or singleplex recombinant Hev b components, it tells you which protein is driving the sensitisation. rHev b 1 and rHev b 3 indicate genuine sensitisation, dominant in spina bifida patients who have direct mucosal contact with raw latex particles. rHev b 5 indicates genuine allergy in healthcare workers and children. rHev b 6.01 links to latex-fruit syndrome through cross-reactivity with plant class I chitinases. rHev b 8 (profilin) often indicates low-risk cross-reactive sensitisation — and a child monosensitised to Hev b 8 may safely undergo surgery in a normal environment. [8] [10] [14]
Patch testing to the rubber additive series (thiuram mix, carba mix, mercapto mix) confirms Type IV allergic contact dermatitis to rubber accelerators — a completely separate mechanism from Type I latex allergy. A child can have both, and the patch test does not screen for IgE-mediated disease. [4]
Serum tryptase during an acute reaction supports the diagnosis of anaphylaxis; baseline serum tryptase screens for systemic mastocytosis as a cofactor for severe reactions. After an intraoperative event, serial tryptase (at 1 to 2 hours, 4 hours, and baseline at follow-up) is the investigation pathway that documents the mast-cell event and supports the allergy referral. [15] [16]
Provocation or use-testing (e.g. a finger-stall test with a latex glove) is rarely needed and carries risk. Reserve it for specialist centres when the history and standard tests are discordant. [2]
Management — Resuscitation
Any systemic feature is anaphylaxis until proven otherwise. Give IM adrenaline into the anterolateral thigh as the first drug, not an antihistamine, and call for help. Do not wait for IV access or a confirmatory test. [15]
Dose adrenaline by weight. A practical approach is roughly 0.01 mg/kg of 1:1000 (1 mg/mL) intramuscularly. Autoinjector doses map to this: 0.15 mg for smaller children (under about 20 kg) and 0.30 mg for larger children (about 20 kg and over). Repeat after five minutes if there is no response. [15] [16]
Remove the latex trigger immediately and eliminate any powdered latex gloves from the entire environment — not just the patient's direct contact, because aerosolised powder elsewhere in the suite can perpetuate the reaction. [4] [11]
[15]For local contact urticaria without systemic features, remove the latex, wash the area, give a non-sedating oral antihistamine, and observe for progression. Do not let the antihistamine delay adrenaline if any systemic feature appears. [1]
Risk-stratify disposition. Local-only reactions settle with observation, while systemic reactions, intraoperative anaphylaxis, and any child who needed adrenaline require at least six hours of observation and admission per anaphylaxis guidance. After an intraoperative event, follow the perioperative anaphylaxis investigation pathway with serial tryptase, specialist allergy referral, and documentation of the latex-safe requirement in the anaesthetic and surgical notes. [16] [17]
Management — Definitive & Stepwise
Once the acute event is settled, definitive management is a ladder that moves the family from the reaction to a safe, liveable latex-avoidance plan. [1] [5]
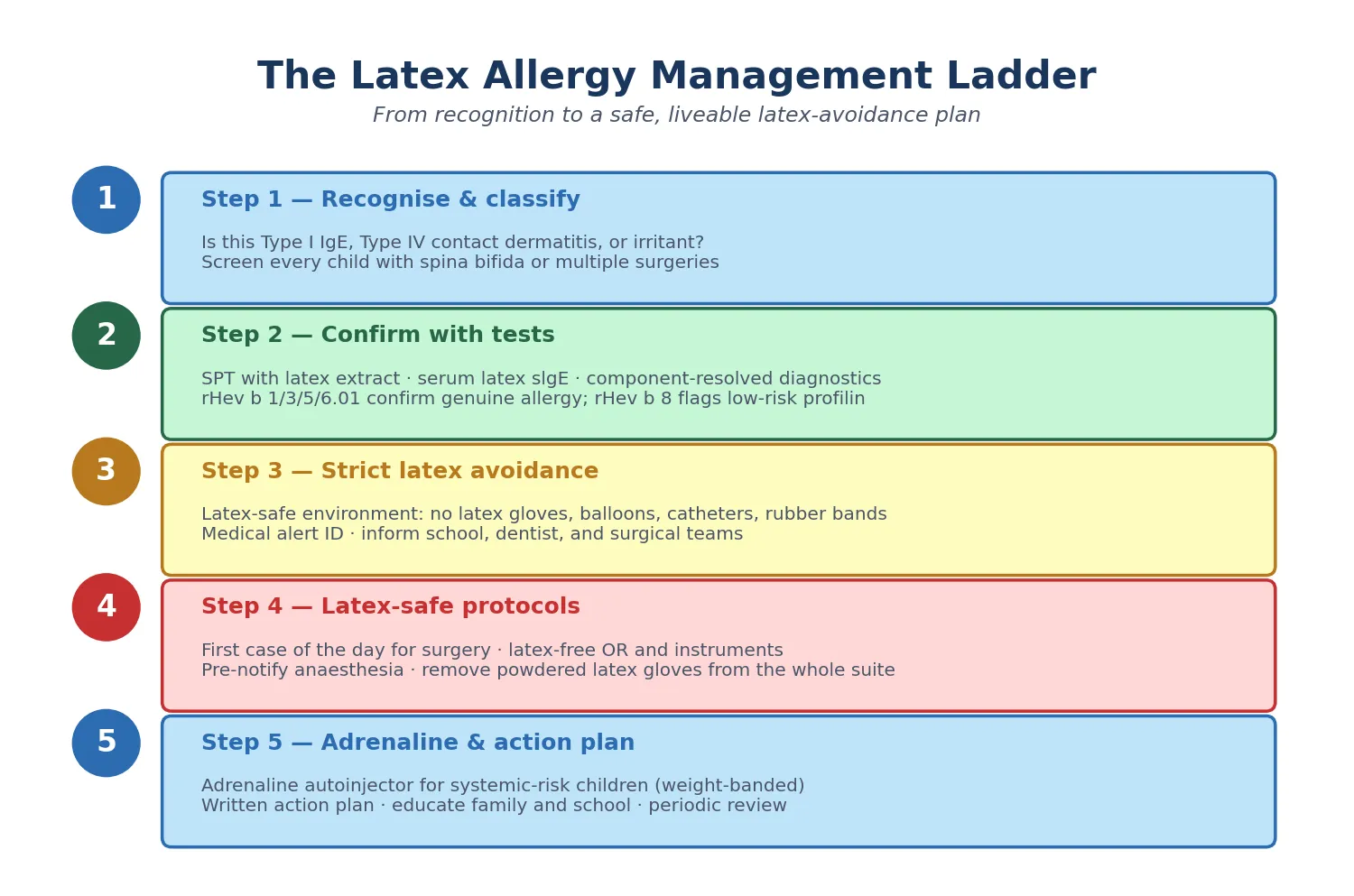
Step one — recognise and classify. Decide at the outset whether this is Type I IgE latex allergy, Type IV contact dermatitis, or irritant dermatitis. Screen every child with spina bifida or multiple surgeries for latex sensitisation, because the first systemic presentation may be intraoperative anaphylaxis. [5] [12]
Step two — confirm with tests. Combine the history with SPT, serum latex-specific IgE, and component-resolved diagnostics so the phenotype (genuine latex allergy vs Hev b 8 profilin-only cross-reactivity) is explicit and documented. Patch testing confirms Type IV contact dermatitis. [8] [10]
Step three — strict latex avoidance. This is the cornerstone. Replace latex gloves, catheters, and medical devices with latex-free alternatives. Avoid balloons, rubber bands, latex erasers, and latex-containing household items. The goal is complete elimination of latex contact, because even trace re-exposure can trigger a systemic reaction in a sensitised child. [1] [4]
Step four — latex-safe protocols. For any procedure, schedule the case first in the day, prepare a latex-free operating room, remove all powdered latex gloves from the suite (not just the patient's), use latex-free equipment and instruments, and ensure all staff are aware. The latex-safe protocol is an institutional commitment, not a bedside improvisation. [5] [11]
Step five — adrenaline and action plan. Provide a written anaphylaxis action plan (ASCIA in ANZ, BSACI or MedicAlert in the UK, FARE in the US) and a weight-banded adrenaline autoinjector for children with systemic-risk profiles or a history of anaphylaxis. Add medical alert identification (bracelet or card) and proactive notification of school, dentist, and all treating clinicians. [15] [16]
The five rungs after a latex reaction or risk identification
Recognise & classify
Type I, Type IV, or irritant? Screen spina bifida and multi-surgery children.
Confirm with tests
SPT + serum IgE + component-resolved diagnostics (Hev b 1, 3, 5, 6.01, 8).
Strict latex avoidance
Latex-free gloves, catheters, devices; avoid balloons and rubber bands.
Latex-safe protocols
First case of the day; latex-free OR; remove powdered gloves from the suite.
Adrenaline & action plan
Weight-banded autoinjector; action plan; medical alert; notify school and dentist.
Specific Subtypes & Scenarios
Different risk profiles and exposure scenarios produce different clinical pictures, and examiners probe these corners. [4]
Spina bifida and myelomeningocele is the highest-risk group and the archetype. Historically 30 to 70 per cent of these children were sensitised, because of repeated bladder catheterisations, multiple surgeries, and early heavy latex exposure from VP shunts and urological procedures. Screen all children with neural tube defects early, institute latex avoidance from birth if possible, and use full latex-safe protocols for all procedures. This is the single most examinable scenario. [5] [3]
Intraoperative anaphylaxis is the catastrophe you prevent. Latex causes reactions 30 to 60 minutes into surgery, later than drug triggers given at induction. Any intraoperative cardiovascular event in a high-risk child demands latex-safe management and adrenaline. After the event, follow the perioperative anaphylaxis pathway with serial tryptase and specialist referral. [12] [17]
Primary prevention of latex allergy (Allmers 2002)
Population: German healthcare workers exposed to natural rubber latex gloves
Key finding
Dramatic reduction in latex sensitisation and occupational latex allergy — evidence that a supply-chain change prevents allergy at population scale
Practice change
Primary prevention works: powder-free low-protein gloves are the single most effective intervention against latex allergy
Latex-fruit syndrome is the cross-reactivity scenario. Hev b 6.01 hevein cross-reacts with class I chitinases in banana, kiwi, avocado, chestnut, passion fruit, tomato and other foods. Up to half of latex-allergic patients react to at least one fruit, and the food reactions can be severe. Counsel families to be cautious with these foods and to avoid only those that cause reactions, as not all latex-allergic children react to every cross-reactive food. [6] [7]
Aerosolised latex allergy from cornstarch glove powder is now rare but mechanistically important. Powdered latex gloves aerosolise protein on cornstarch particles, causing airborne rhinitis and asthma. The lesson for the exam is that eliminating powdered gloves from the entire operating suite — not just the patient's direct contact — is part of a latex-safe protocol. [4] [11]
Type IV allergic contact dermatitis is the skin scenario. Patch-test confirmed allergy to rubber accelerators (thiurams, carbamates, mercaptobenzothiazole) is managed by avoidance of rubber additives and substitution with accelerator-free gloves, not by latex-protein avoidance. The two mechanisms can coexist in the same child. [4]
The Hev b 8-only (profilin) child is the low-risk scenario that prevents over-restriction. Component-resolved diagnostics shows only profilin sensitisation, which often represents cross-reactive pollen sensitisation with low genuine latex clinical reactivity. Some may safely undergo surgery in a non-latex-safe environment, as Quercia and colleagues demonstrated — but this decision belongs to a specialist, not the bedside. [8] [10]
Complications & Pitfalls
The most dangerous error is failing to anticipate intraoperative latex anaphylaxis in a high-risk child. Any child with spina bifida or multiple surgeries must be treated latex-safe until proven otherwise — never gamble on the first procedure. [5] [12]
Confusing Type I IgE latex allergy with Type IV contact dermatitis or irritant dermatitis is the commonest classification error. The management is completely different: latex-free environment plus adrenaline for Type I, accelerator-free gloves and emollients for Type IV, and barrier repair for irritant. Mistaking one for the other either withholds life-saving adrenaline or imposes unnecessary restriction. [1] [4]
Over-labelling based on Hev b 8 (profilin) sensitisation alone causes unnecessary restriction and surgical over-precaution. Profilin positivity often represents cross-reactive pollen sensitisation with low genuine latex clinical reactivity. Component-resolved diagnostics prevents this, but only if the result is interpreted, not just reported. [8] [10]
Missing latex-fruit syndrome in a child with unexplained food reactions to banana, kiwi or avocado is a quiet pitfall. The latex connection may be invisible to the family, so ask about cross-reactive foods in every latex-allergic child and, conversely, ask about latex exposure in any child with unexplained fruit reactions. [6] [7]
Relying on serum-specific IgE without confirming the clinical history is a recurrent trap. Sensitisation is not allergy, and a positive test in a child who tolerates latex does not justify latex avoidance or latex-safe surgery. [1] [9]
Failing to notify the school, dentist, and all treating teams results in accidental re-exposure during procedures. Latex allergy is a whole-of-life, whole-of-system management problem, and the medical alert and proactive notification are as important as the adrenaline device. [5] [15]
Finally, forgetting that powdered latex gloves elsewhere in the operating suite can aerosolise latex protein and trigger a reaction — even if the patient's own gloves are latex-free — undermines the latex-safe protocol. Eliminate powdered gloves from the suite, not just the bedside. [4] [11]
Prognosis & Disposition
With strict latex avoidance, most children with Type I latex allergy do well. Reactions are preventable by maintaining a latex-safe environment at every encounter, and the child who carries their medical alert, their adrenaline, and their knowledge of latex-safe requirements through life is a child who is protected. [1] [5]
The epidemiological trend is favourable. Universal adoption of powder-free, low-protein gloves has dramatically reduced new sensitisation in healthcare workers and the general population, and children with spina bifida who are managed with latex avoidance from early life show declining sensitisation rates — supporting primary prevention in this group. [9] [11]
Disposition follows the risk profile. Local reactions are managed with observation; systemic reactions and intraoperative anaphylaxis follow the anaphylaxis observation pathway — at least six hours, with admission for severe reactions or those needing more than one adrenaline dose. [15] [16]
Schedule periodic specialist review. Resolution of latex sensitisation can occur, but the child should maintain latex-safe precautions until tests and clinical history confirm tolerance. The quality-of-life burden — dietary restriction (latex-fruit foods), medical alert requirements, and the anxiety of avoiding a ubiquitous material — should be addressed proactively. [1]
Special Populations
Children with spina bifida and neural tube defects are the highest-risk group and the focus of the topic. Institute latex avoidance from birth, screen early with SPT and serum IgE, and treat every procedure as latex-safe. Coordinate with the spina bifida clinic and the neurosurgical, urological and orthopaedic teams so the latex-safe requirement travels with the child at every encounter. [5] [3]
Children with multiple surgical needs (urological reconstructions, orthopaedic procedures, cardiac surgery) accumulate cumulative latex exposure that drives sensitisation. Plan latex-safe pathways for every encounter, and screen before elective procedures so there are no surprises in the operating room. [1] [12]
Children with atopy (eczema, asthma, allergic rhinitis) carry higher background risk of latex sensitisation. Assess risk before procedures and counsel on latex-fruit foods, because the atopic child with latex allergy may have a complex dietary and inhalant allergy picture. [3] [13]
Adolescents transitioning to adult care need self-advocacy skills. Ensure they know their latex-safe requirements, carry adrenaline for systemic-risk profiles, and have a clear handover to adult allergy services. The transition is the point at which a well-managed child can be lost to follow-up and re-exposed. [1] [15]
For Aboriginal and Torres Strait Islander, Maori, migrant and refugee families, deliver culturally safe education, use trained interpreters, and address equity of access to latex-free medical supplies and adrenaline devices. Latex-safe supplies and adrenaline must be available regardless of geography or socioeconomic status. [5]
Rural and remote families face a narrower safety margin for a latex-allergic child undergoing surgery. Ensure regional hospitals stock latex-free equipment, provide a retrieval plan, and equip the systemic-risk child with a second adrenaline device and community education so the people around the child can act first. [15] [16]
Evidence, Guidelines & Regional Differences
The evidence base rests on a landmark primary prevention study, a maturing component-diagnostics literature, and a set of paediatric and surgical guidelines. Defending it is a viva staple. [4]
The German primary prevention study (Allmers 2002) demonstrated that switching to powder-free, low-protein gloves dramatically reduced latex sensitisation in healthcare workers. It is a landmark evidence-based public health intervention and the single most cited paper on latex allergy prevention. [11]
The profile-shift paper (Saleh 2019) documents the changing sensitisation pattern over 20 years, with declining overall prevalence but persistence in high-risk groups. It is the paper that explains why latex allergy is now uncommon in the general population but remains a live threat in spina bifida and surgical children. [9]
Component-resolved diagnostics for latex (Ebo 2010; Cardona 2016) underpin the shift from blanket 'latex allergy' labels to component-specific risk assessment. The key insight is that Hev b 1, 3 and 5 indicate genuine sensitisation, while Hev b 8 profilin often represents cross-reactive noise — and the Quercia 2009 study showed that patients monosensitised to Hev b 8 may safely undergo surgery in a non-latex-safe environment. [8] [14] [10]
The spina bifida latex allergy guidelines (Meneses 2020) codify lifelong latex-safe precautions for this population, and the intraoperative anaphylaxis landmark papers (Gold 1991; Pasquariello 1993) established the latex-anaphylaxis association that drives surgical latex-safe protocols. [5] [12] [17]
[4] [11] [16]Controversies remain. The role of latex immunotherapy (sublingual) is investigational and not routine, though early paediatric studies show immunologic modifications and some efficacy. The optimal use of component-resolved diagnostics in primary care is still maturing, and its cost and availability vary by region. And some older latex stocks and imported products remain a hazard despite powder-free policies, so vigilance is still needed. [4] [9]
Exam Pearls
S-L-A-T-E-X — what to ask in a suspected latex reaction
The high-yield rule is "IMMEDIATE not DELAYED, and SYSTEMIC not LOCAL" for Type I latex allergy: if the reaction is immediate after latex contact and any systemic feature is present, it is IgE-mediated latex allergy with anaphylaxis risk — give adrenaline and institute strict latex avoidance. If the reaction is delayed and eczematous, it is Type IV or irritant dermatitis — a completely different management. [2] [4]
References
- [1]Arasi S, Barni S, Caminiti L, et al Latex Allergy in Children. J Clin Med, 2023.PMID 38202131
- [2]Poley GE Jr, Slater JE Latex allergy. J Allergy Clin Immunol, 2000.PMID 10856135
- [3]Niggemann B, Breiteneder H Latex allergy in children. Int Arch Allergy Immunol, 2000.PMID 10705219
- [4]Raulf M The latex story. Chem Immunol Allergy, 2014.PMID 24925405
- [5]Meneses V, Parenti S, Burns H, et al Latex allergy guidelines for people with spina bifida. J Pediatr Rehabil Med, 2020.PMID 33285646
- [6]Blanco C Latex-fruit syndrome. Curr Allergy Asthma Rep, 2003.PMID 12542994
- [7]Wagner S, Breiteneder H The latex-fruit syndrome. Biochem Soc Trans, 2002.PMID 12440950
- [8]Ebo DG, Hagendorens MM, De Knop KJ, et al Component-resolved diagnosis from latex allergy by microarray. Clin Exp Allergy, 2010.PMID 20210809
- [9]Saleh MM, Forkel S, Schon MP, et al Profile Shift in Latex Sensitization over the Last 20 Years. Int Arch Allergy Immunol, 2019.PMID 30212836
- [10]Quercia O, Stefanini GF, Scardovi A, et al Patients monosensitised to Hev b 8 (Hevea brasiliensis latex profilin) may safely undergo major surgery in a normal (non-latex safe) environment. Eur Ann Allergy Clin Immunol, 2009.PMID 19877563
- [11]Allmers H, Schmengler J, Skudlik C Primary prevention of natural rubber latex allergy in the German health care system through education and intervention. J Allergy Clin Immunol, 2002.PMID 12170275
- [12]Gold M, Swartz JS, Braude BM, et al Intraoperative anaphylaxis: an association with latex sensitivity. J Allergy Clin Immunol, 1991.PMID 2005317
- [13]Cox AL, Eigenmann PA, Sicherer SH Clinical Relevance of Cross-Reactivity in Food Allergy. J Allergy Clin Immunol Pract, 2021.PMID 33429724
- [14]Cardona V, Ansotegui IJ Component-resolved diagnosis in anaphylaxis. Curr Opin Allergy Clin Immunol, 2016.PMID 26945180
- [15]Simons FE, Ardusso LR, Dimov V, et al World Allergy Organization Anaphylaxis Guidelines: 2013 update of the evidence base. Int Arch Allergy Immunol, 2013.PMID 24008815
- [16]Muraro A, Worm M, Alviani C, et al EAACI guidelines: Anaphylaxis (2021 update). Allergy, 2022.PMID 34343358
- [17]Pasquariello CA, Lowe DA, Schwartz RE Intraoperative anaphylaxis to latex. Pediatrics, 1993.PMID 8474820