Paeds · allergy-and-immunology
Oral allergy syndrome and pollen-food syndrome
Also known as Oral allergy syndrome · Pollen-food allergy syndrome · Pollen-food syndrome · PFAS · Birch-fruit syndrome · Cross-reactive food allergy
A fellowship approach to pollen-food allergy syndrome (oral allergy syndrome) in children: recognise the local oral reaction to raw fruit or vegetable in a pollen-sensitised child, explain the cross-reactive labile-versus-stable protein mechanism, use history plus fresh-food skin-prick and component-resolved diagnostics, counsel on keeping cooked forms while avoiding the raw trigger, and know when an adrenaline autoinjector is needed for the lipid-transfer-protein systemic-risk phenotype, across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A nine-year-old with spring hayfever bites into a raw apple and within a minute her lips tingle, her palate itches and her throat feels tight. She eats apple pie every week without trouble. That constellation — oral symptoms to the raw food only, in a pollen-sensitised child — is pollen-food allergy syndrome. [1] [2]
Pollen-food allergy syndrome (PFAS) is an IgE-mediated contact reaction, usually confined to the oropharynx, that follows raw plant-food exposure in a person sensitised to pollen. Oral allergy syndrome (OAS) is the older name, classically reserved for the local oral form; PFAS is now the preferred umbrella term because it acknowledges that some of these reactions go beyond the mouth. [2] [6]
The clinical hallmark is raw but not cooked. The cross-reactive proteins are fragile, so cooking, baking or canning denatures them and the food is tolerated. Holding that idea makes the mechanism, the diagnosis and the dietary advice fall into place. [1] [7]
The trap, and the fellowship discriminator, is the child whose reaction does not respect this rule. Symptoms beyond the mouth, or reactions to the cooked food, point away from classic PFAS and towards a heat-stable lipid transfer protein phenotype or a primary food allergy. [10] [12]
Classification
Sort every child through two questions: which cross-reactive protein is driving the reaction, and is that protein fragile or stable? The answer to the second question sets the risk. [2] [4]
By responsible protein family
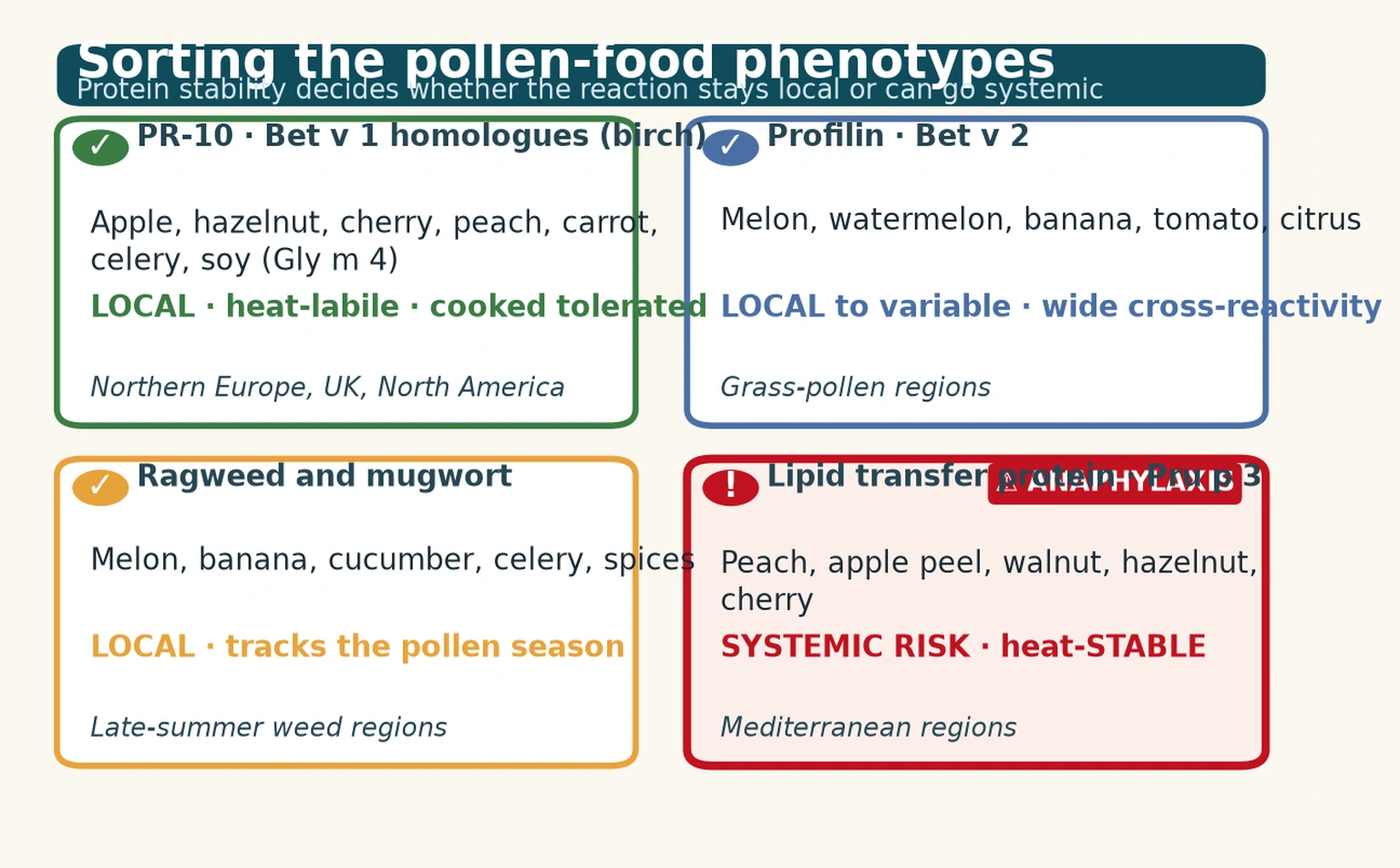
Birch-related (PR-10, Bet v 1 homologues) is the commonest phenotype in birch-endemic regions. Apple (Mal d 1), hazelnut (Cor a 1), cherry, peach, carrot, celery, pear, kiwi and soy (Gly m 4) cross-react with the major birch pollen allergen. Reactions are local and the cooked food is tolerated. [1] [7]
Profilin-mediated (Bet v 2) reactions cross-react across botanically unrelated foods — melon, watermelon, banana, tomato and citrus. Profilin is labile like the PR-10 proteins, so reactions are usually local, but the cross-reactivity is wide. [2] [9]
Ragweed and mugwort syndromes track the weed-pollen season. Ragweed drives reactions to melon, banana, cucumber and other Cucurbitaceae; mugwort cross-reacts with celery, carrot and spices, producing the celery-mugwort-birch-spice syndrome. [2] [6]
Lipid transfer protein (LTP, Pru p 3 in peach) is the systemic-risk outlier. LTP is heat-stable and digestion-stable, so it survives to be absorbed and can cause anaphylaxis. LTP allergy is Mediterranean-dominant and is regarded as a separate phenotype rather than classic PFAS. [10] [11]
By risk: labile versus stable
Labile PR-10 / profilin
Local · low risk
- Birch-related apple, hazelnut, cherry, soy; profilin melon, banana, citrus
- Heat- and digestion-labile — reaction confined to the mouth
- Cooked, baked or canned forms tolerated
- Manage: avoid raw trigger, keep cooked forms, antihistamine for breakthroughs
Stable LTP (Pru p 3)
Systemic · anaphylaxis risk
- Peach, apple peel, walnut, hazelnut; Mediterranean-dominant
- Heat- and digestion-stable — absorbed intact
- Reactions can occur to cooked food and can be systemic
- Manage: avoid all forms, adrenaline autoinjector, action plan
Epidemiology & Risk Factors
PFAS is the commonest food-allergy phenotype in adults and older children in pollen-rich regions, and it is substantially under-recognised in paediatric practice. It is uncommon in very young children because the child must first accumulate years of seasonal pollen sensitisation. [1] [9]
Prevalence rises steadily through the school-age and adolescent years. The dominant pollen in a region sets the dominant phenotype: birch drives PR-10 disease in Northern Europe, the United Kingdom and northern North America, while grass and weed pollen dominate elsewhere. [2] [6]
Risk concentrates in the atopic, pollen-sensitised child. Established allergic rhinitis (especially to birch), asthma, eczema and other food allergy all raise the likelihood, and adolescents bring extra risk through cofactors such as exercise and NSAID use. [1] [3]
Systemic-reaction risk has its own profile. Sensitisation to lipid transfer protein, a prior systemic reaction, cofactors (exercise, NSAIDs, infection, alcohol, an empty stomach), and foods eaten with the peel or in large amounts all raise the chance that a local reaction becomes systemic. [10] [11]
Pathophysiology
The conceptual core is cross-reactivity: the immune system, primed by inhaled pollen, mistakes a structurally similar food protein for the pollen and fires on the oral mucosa. [2] [5]
Primary sensitisation happens through the respiratory mucosa. The child inhales birch pollen, and the major birch allergen Bet v 1 drives production of pollen-specific IgE that arms mast cells throughout the body, including the oropharynx. [5] [9]
The food trigger shares that structure. Raw apple carries Mal d 1, a PR-10 protein that is a homologue of Bet v 1. When the raw apple touches the oral mucosa, Mal d 1 cross-links the pollen-specific IgE on mucosal mast cells, the cell degranulates, and histamine produces the immediate oral itch and angioedema. [4] [7]
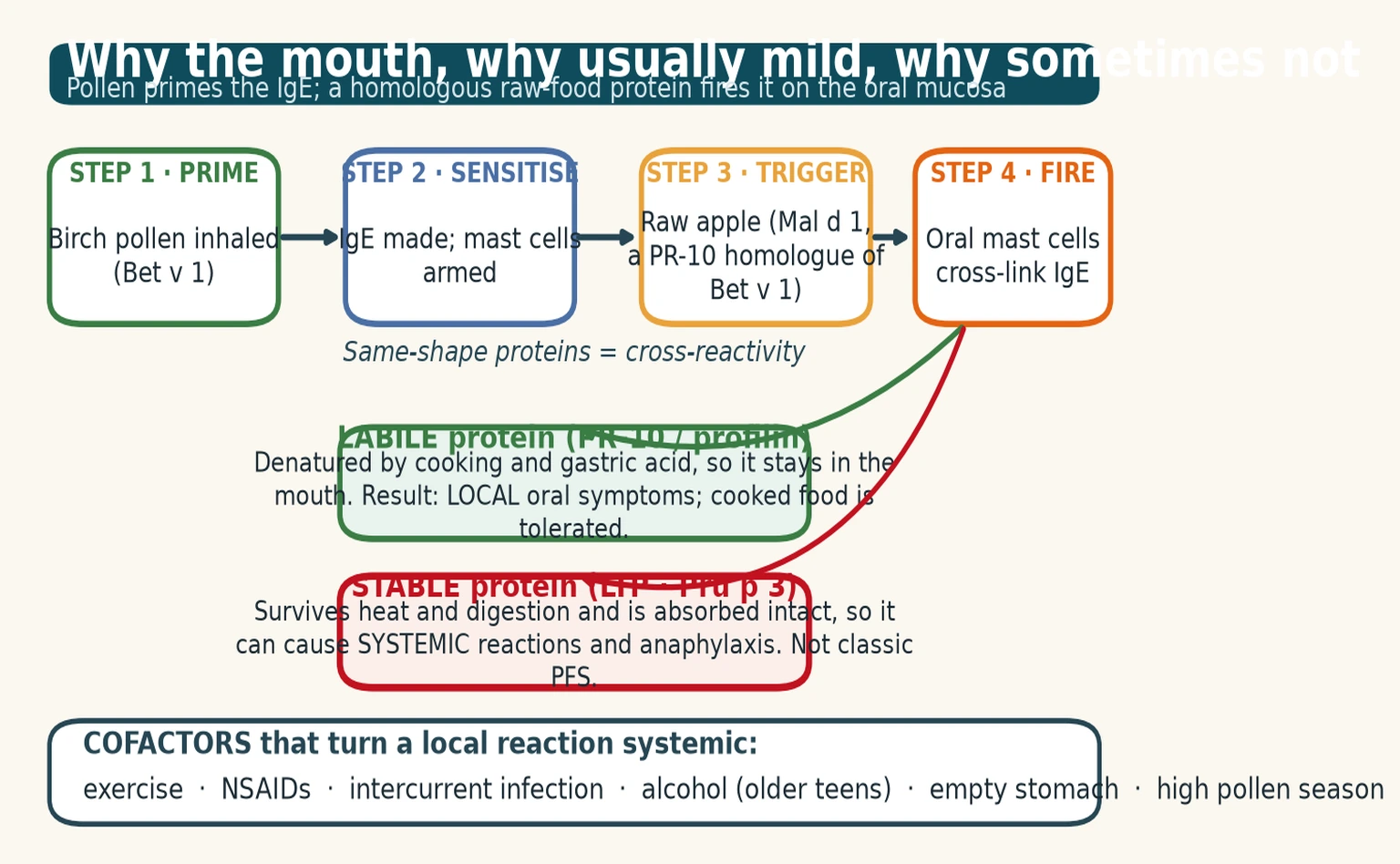
Protein stability is the whole story. Labile proteins — PR-10 and profilin — are denatured by heat and by gastric acid and digestion, so they never leave the oropharynx; that is why the reaction is local and the cooked food is tolerated. [7] [9]
Stable proteins behave differently. Lipid transfer protein (Pru p 3 in peach) resists cooking and digestion, reaches the circulation intact, and can trigger a systemic IgE response including anaphylaxis. This is why LTP allergy is classified apart from classic PFAS. [10] [11]
Cofactors amplify the cascade. Exercise, NSAIDs, intercurrent infection, alcohol and an empty stomach can all convert an otherwise local reaction into a systemic one, which is why a careful history of context matters as much as the food itself. [9] [12]
Clinical Presentation
Match the pattern to the mechanism. A rapid, local oral reaction to a raw plant food in a pollen-sensitised child is PFAS until proven otherwise. [1] [6]
Classic PFAS brings oral itching and tingling, angioedema of the lips, tongue or palate, throat tightness, throat clearing, ear itching and sometimes mild nausea, beginning within minutes of the food and settling quickly once it is removed. The picture is confined to the oropharynx. [2] [7]
The history is stereotyped and reproducible: the raw form provokes it, the cooked form does not, and the child is well between episodes. That reproducibility is itself diagnostic. [1] [8]
Systemic features change everything. Urticaria beyond the mouth, wheeze or respiratory distress, abdominal pain and vomiting, or hypotension and collapse, signal that the reaction has escaped the oropharynx and move the child into systemic-risk territory. [10] [13]
Ask about cofactors every time. Exercise, NSAIDs, intercurrent infection, alcohol (in older teens) and an empty stomach can turn a previously local reaction into a systemic one, and a high-pollen-season pattern points back to the sensitising pollen. [9] [12]
Differential Diagnosis
The error is labelling any post-food oral symptom as PFAS. Separate cross-reactive local reactions from the mimics before settling the plan. [2] [12]
| Finding after eating | Prefer | Discriminators | Action |
|---|---|---|---|
| Local oral itch to raw apple, cooked OK | PFAS (PR-10) | Pollen-sensitised; raw only; minutes | Avoid raw; keep cooked; antihistamine |
| Urticaria, wheeze or collapse | Systemic IgE / LTP / anaphylaxis | Beyond the mouth; may include cooked food | IM adrenaline; action plan |
| Reaction to banana, kiwi, avocado, chestnut | Latex-fruit syndrome | Latex sensitisation; often oral | Confirm latex IgE; avoid trigger |
| Flushing minutes after fish | Scombroid (histamine toxin) | Spoiled fish; responds to antihistamine | Supportive care; public-health report |
| Recurrent lip/tongue swelling, no itch | Angioedema (C1-inhibitor / ACE-i) | No urticaria; non-allergic | Stop ACE-i; screen complement |
| Dysphagia, reflux, slow onset | Eosinophilic oesophagitis | Not a contact reaction; delayed | Endoscopy with biopsy |
Two mimics cause the most confusion. Latex-fruit syndrome shares kiwi, banana, avocado and chestnut with PFAS, so confirm latex sensitisation to separate them. A primary food allergy to a stable storage protein reacts to the cooked food and can be severe — the opposite of classic PFAS. [8] [12]
Distinguish PFAS from non-allergic angioedema when there is no itch and no urticaria; hereditary or acquired C1-inhibitor deficiency and ACE-inhibitor angioedema are not IgE-mediated and need a different workup. [12]
Clinical & Bedside Assessment
In a suspected acute reaction, assessment is safety-first. Run an ABCDE approach and decide at the bedside whether this is local-only or systemic, because that single distinction sets the entire plan. [13]
Take a focused trigger history once the child is safe. Ask which food, raw versus cooked tolerance, the onset time, the exact symptoms, any prior systemic reaction, and any cofactors such as exercise or NSAIDs. The history is more diagnostic than any test. [1] [6]
Anchor the syndrome in pollen. Seasonal rhinitis or conjunctivitis, asthma and an atopic background frame the diagnosis and flag systemic risk; a child with no pollen sensitisation is less likely to have classic PFAS. [2] [3]
Examine the oropharynx acutely for angioedema or stridor, but in clinic also assess general atopic stigmata, growth and nutrition. An over-restricted diet causes real harm, and catching it is part of the assessment, not an afterthought. [12]
Name the systemic-risk signs explicitly so they are not missed: body urticaria, wheeze, abdominal pain, hypotension. Any one of them escalates the child out of the low-risk pathway and towards adrenaline. [10] [13]
Investigations
Tests support a compatible history; they never replace it. A positive test in a child who tolerates the food is sensitisation, not allergy, and acting on it alone causes over-restriction. [3] [12]
For skin-prick testing, commercial extracts are often falsely negative because the labile proteins degrade during manufacture. The fresh-food prick-prick test — prick the raw food, then prick the skin — is more sensitive for PR-10 and profilin reactions. [1] [8]
Serum specific IgE to whole foods gives sensitisation data only. It cannot separate cross-reactive PFAS from a primary food allergy, so use it as a pointer rather than a verdict. [2] [12]
Component-resolved diagnostics (CRD) is the tool that sorts the phenotypes. rBet v 1 and the food PR-10 components (Mal d 1, Cor a 1, Gly m 4, Ara h 8) indicate low-risk labile cross-reactivity; rBet v 2 flags wider profilin cross-reactivity; rPru p 3 flags systemic-risk lipid transfer protein allergy. Apply it within the EAACI Molecular Allergology User's Guide framework. [4] [5]
Confirm the sensitising pollen with coinhalant testing — pollen skin-prick or specific IgE — because it frames the syndrome and guides any future immunotherapy decision. [2] [6]
An oral food challenge is rarely needed in PFAS, but it settles genuine uncertainty, such as confirming cooked-form tolerance or excluding a primary allergy. Reserve it for a specialist centre. [8] [12]
Management — Resuscitation
Classic local PFAS is rarely an emergency. The immediate action is to stop eating the food, rinse the mouth, give an antihistamine for itch, and observe for any progression beyond the oropharynx. [1] [6]
Any systemic feature is anaphylaxis until proven otherwise. Give IM adrenaline into the anterolateral thigh as the first drug, not an antihistamine, and call for help. Do not wait for IV access or a confirmatory test. [13]
Dose adrenaline by weight. A practical approach is roughly 0.01 mg/kg of 1:1000 (1 mg/mL) intramuscularly. Autoinjector doses map to this: 0.15 mg for smaller children (under about 20 kg) and 0.30 mg for larger children (about 20 kg and over). Repeat after five minutes if there is no response. [13]
[13]For local reactions a non-sedating oral antihistamine relieves itch and angioedema, but it does not treat airway or circulation compromise, so never let it delay adrenaline in a systemic reaction. [9] [12]
Risk-stratify disposition. Local-only reactions settle at home, while systemic reactions, LTP-positive patients, and any child who needed adrenaline are observed for at least six hours and admitted per anaphylaxis guidance. [10] [13]
Management — Definitive & Stepwise
Once the acute event is settled, definitive management is a ladder that moves the family from the reaction to a safe, liveable plan. [1] [9]
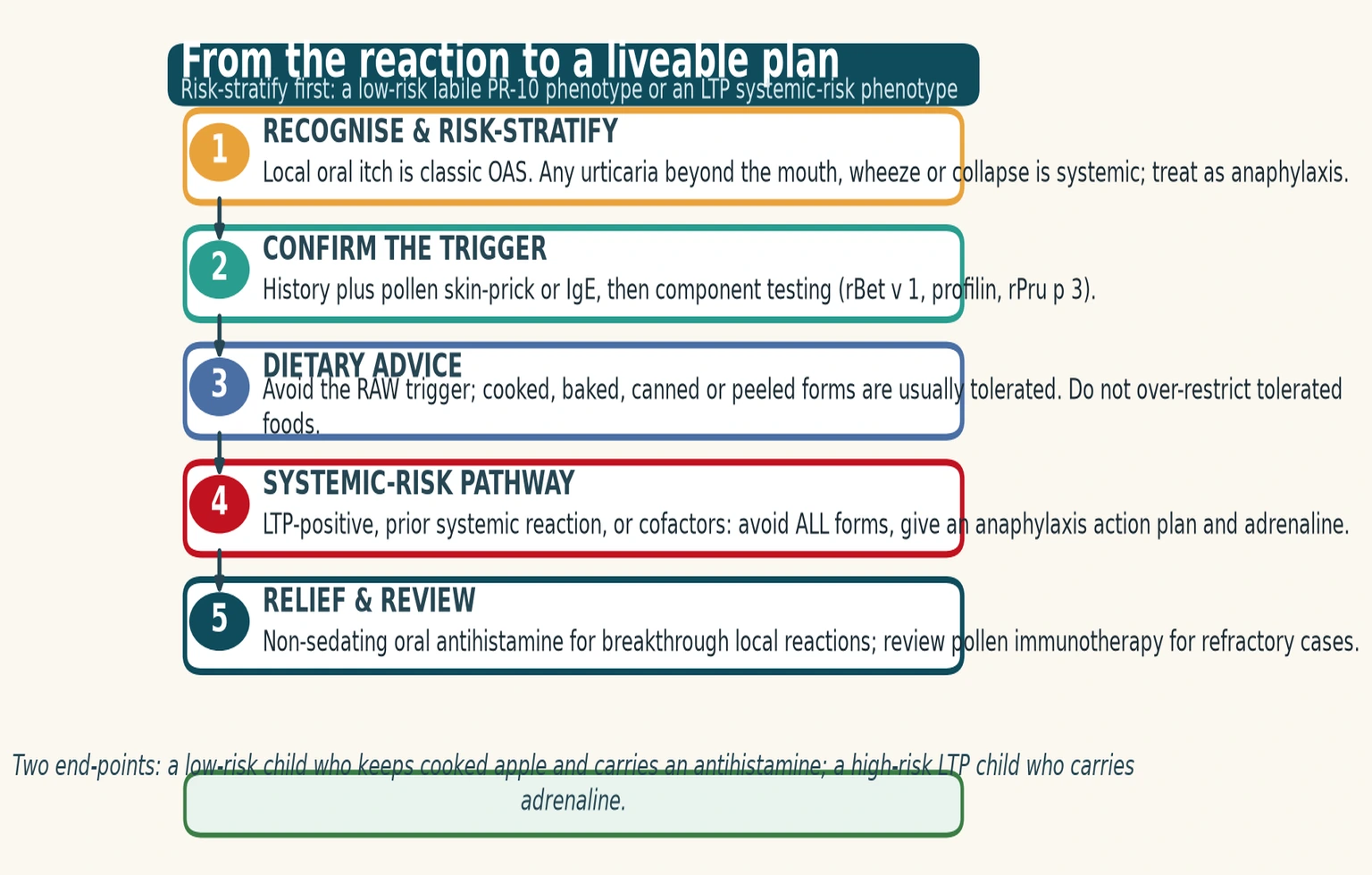
Step one — recognise and risk-stratify. Decide at the outset whether this is local-only PFAS or whether any systemic feature is present. That single decision routes the child to the antihistamine pathway or the adrenaline pathway. [10] [13]
Step two — confirm the trigger. Combine the history with pollen skin-prick or IgE and component-resolved diagnostics, so the phenotype (low-risk labile versus high-risk LTP) is explicit and documented. [4] [8]
Step three — dietary advice. For the low-risk phenotype, avoid the raw trigger and encourage cooked, baked, canned or peeled forms, which are usually tolerated. Peeling helps when the allergen concentrates in the skin, and the goal is precise avoidance of the raw trigger, not a blanket food ban. [1] [7]
Step four — the systemic-risk pathway. For the LTP-positive child, anyone with a prior systemic reaction, or when relevant cofactors apply, avoid the trigger in all forms and provide a written anaphylaxis action plan and a weight-banded adrenaline autoinjector. [10] [13]
Step five — relief and review. Give a non-sedating oral antihistamine for breakthrough local reactions, arrange periodic review (especially around adolescence), and consider pollen immunotherapy in selected, refractory cases. [9] [2]
The five rungs after a pollen-food reaction
Recognise & risk-stratify
Local-only or systemic? The answer routes antihistamine versus adrenaline.
Confirm the trigger
History + pollen SPT/IgE + component testing (Bet v 1, profilin, Pru p 3).
Dietary advice
Avoid the raw trigger; keep cooked, baked, canned or peeled forms.
Systemic-risk pathway
LTP or prior systemic reaction: avoid all forms, action plan, adrenaline.
Relief & review
Antihistamine for breakthroughs; review; consider pollen immunotherapy.
Specific Subtypes & Scenarios
Different pollens and proteins produce different syndromes, and examiners probe these corners. [2]
Birch-related (PR-10) PFAS is the prototype. Apple, hazelnut, cherry, peach, carrot, celery, pear, kiwi and soy (Gly m 4) cross-react with Bet v 1; reactions are local and cooked forms are tolerated. This is the phenotype a fellowship candidate is most often asked to explain. [1] [7]
Profilin-mediated (Bet v 2) reactions bridge unrelated botanical families. Melon, watermelon, banana, tomato and citrus all carry profilin, so a single sensitisation can produce wide cross-reactivity that looks more confusing than it is. [2] [9]
Ragweed and mugwort syndromes track the weed season. Ragweed drives melon, banana, cucumber and Cucurbitaceae in late summer; mugwort drives the celery-mugwort-birch-spice syndrome. Knowing the local pollen calendar sharpens the trigger list. [6] [2]
Lipid transfer protein allergy (Pru p 3) is the systemic-risk phenotype. Peach and other Rosaceae, walnut and hazelnut provoke reactions that can be severe and can occur with cooked food; it is Mediterranean-dominant and is classified apart from classic PFAS. [10] [11]
Pollen-food allergy syndrome in childhood (Mastrorilli 2019)
Population: Children with oral symptoms to raw plant foods and pollen sensitisation
Key finding
PFAS is common but under-recognised in children; the labile-versus-stable protein distinction sets the risk
Practice change
Recognise PFAS in school-age children, keep cooked forms, and reserve adrenaline for the systemic-risk phenotype
Latex-fruit syndrome is the look-alike to exclude. Kiwi, banana, avocado and chestnut cross-react with latex, so confirm latex sensitisation to separate it from PFAS before settling the dietary advice. [8] [12]
Watch for cofactor-dependent systemic reactions, which can masquerade as 'severe OAS'. A history of exercise, NSAIDs or alcohol before a systemic reaction should prompt a search for an LTP phenotype and a lower threshold for adrenaline. [9] [10]
Complications & Pitfalls
The most dangerous error is under-diagnosis — labelling a systemic reaction 'just OAS' and missing an LTP phenotype, a primary food allergy, or evolving anaphylaxis. Any feature beyond the mouth should reset the risk assessment. [10] [13]
Over-restriction is the other common harm. Banning cooked forms or tolerated foods causes nutritional deficiency (calcium, energy) and social isolation, and it is unnecessary for the labile phenotype where the cooked food is the dietary friend. [7] [12]
Relying on a negative commercial skin-prick extract to dismiss a convincing history is a recurrent trap. Labile proteins degrade in commercial extracts, so reach for the fresh-food prick-prick test. [1] [8]
Two classification errors cost marks. Confusing PFAS with latex-fruit syndrome (banana, kiwi, avocado, chestnut) misdirects the dietary advice, and confusing classic PFAS with a primary food allergy to a stable storage protein mislabels a severe child as mild. [8] [12]
Forgetting cofactors is a quiet pitfall. Exercise, NSAIDs, infection and alcohol can convert a local reaction into a systemic one, so ask about context whenever the history seems disproportionate to the food. [9]
Finally, two prescribing extremes both fail the child: failing to give adrenaline to a genuinely systemic-risk LTP patient, and over-prescribing adrenaline to every low-risk local OAS reaction. Risk-stratify, then prescribe to the phenotype. [10] [13]
Prognosis & Disposition
Classic labile PFAS is bothersome but low-risk. Reactions are local, brief and self-limiting once the food is removed, and the main burden is quality of life — dietary restriction, anxiety, and the social limits of eating out. [1] [6]
The LTP phenotype carries a different outlook. Heat-stable and absorbed intact, it carries a higher risk of systemic reactions and anaphylaxis, and it needs a correspondingly tighter plan with adrenaline and an action plan. [10] [11]
Symptoms often fluctuate with the pollen season and may improve with pollen immunotherapy in selected patients, so the trajectory is not fixed. [2] [9]
Disposition follows the risk profile. Local-only reactions are managed at home with dietary advice and an antihistamine, while systemic reactions follow anaphylaxis observation — at least six hours, with admission for the high-risk group. [10] [13]
Because new systemic features can appear over time, schedule periodic review, especially around adolescence when cofactors and risk-taking peak. A child who was once low-risk can change category, and the plan should change with them. [9] [12]
Special Populations
Young children are an uncommon but important group. PFAS needs prior years of pollen sensitisation, so it appears mainly from the school-age years onward; in a toddler with oral symptoms, reconsider a primary food allergy first. [1] [3]
Adolescents and young adults sit at the peak of cofactor-driven risk. Exercise, NSAIDs, alcohol and eating away from home can convert a previously local reaction into a systemic one, so address self-carry, peer awareness and a planned transition for the high-risk phenotype. [9] [13]
Children with multiple atopy — asthma, eczema and other food allergy — carry higher background risk and need more complex dietary counselling, so coordinate with the allergy and dietetic team and watch for nutritional gaps. [3] [12]
Region and pollen biology shape the phenotype. Birch-endemic regions drive PR-10 disease, the Mediterranean drives LTP disease, and ANZ is grass- and weed-dominant with relatively little birch — so tailor the trigger list to local pollen. [2] [6]
For Aboriginal and Torres Strait Islander, Māori, migrant and refugee families, deliver culturally safe education, use trained interpreters, and address equity of access to allergy services, component testing and adrenaline devices. [12]
Rural and remote families face a narrower safety margin for any systemic-risk child, so provide a second adrenaline device, a retrieval plan, and community education so the people around the child can act first. [13]
Evidence, Guidelines & Regional Differences
The evidence base rests on molecular allergology and a maturing paediatric literature, and defending it is a viva staple. [4]
The EAACI Molecular Allergology User's Guide (2016), and its 2.0 update (2023), underpin component-resolved diagnostics and the labile-versus-stable protein framework that lets you sort the phenotypes rationally. [4] [5]
Paediatric and general reviews of pollen-food allergy syndrome frame PFAS as a common but under-recognised childhood phenotype and stress the history-led, test-supported approach across the age span. [1] [9]
A key conceptual paper argues that lipid transfer protein allergy is not a classic pollen-food syndrome — a distinction that protects the systemic-risk child from being mislabelled as mild. [10]
Reviews of birch-related and fruit-and-vegetable allergy define the PR-10 cross-reactivity clusters and the clinical value of cooked-form tolerance, which is the diagnostic anchor of the whole topic. [7] [11]
[4] [10] [13]Controversies remain. The place of pollen immunotherapy for PFAS is evolving and not universally funded; the optimal use of component testing in primary care is still maturing; and regional pollen biology means the dominant phenotype varies by geography. State the principle, name the guideline, and flag where the evidence is still developing. [2] [9]
Exam Pearls
R-A-W-P-C — what to ask in a suspected pollen-food reaction
The high-yield rule is "RAW not COOKED, and LOCAL not SYSTEMIC": if both halves hold, you have classic low-risk PFAS and an antihistamine; if either breaks, escalate to component testing and adrenaline. [4] [9]
References
- [1]Mastrorilli C Pollen-Food Allergy Syndrome: A not so Rare Disease in Childhood. Medicina (Kaunas), 2019.PMID 31561411
- [2]Poncet P Update on pollen-food allergy syndrome. Expert Rev Clin Immunol, 2020.PMID 32691654
- [3]Sicherer SH Food Allergy from Infancy Through Adulthood. J Allergy Clin Immunol Pract, 2020.PMID 32499034
- [4]Dramburg S EAACI Molecular Allergology User's Guide 2.0. Pediatr Allergy Immunol, 2023.PMID 37186333
- [5]Matricardi PM EAACI Molecular Allergology User's Guide. Pediatr Allergy Immunol, 2016.PMID 27288833
- [6]Saunders S Oral allergy syndrome. Curr Opin Otolaryngol Head Neck Surg, 2015.PMID 25887974
- [7]Fernández-Rivas M Allergies to fruits and vegetables. Pediatr Allergy Immunol, 2008.PMID 19097271
- [8]Giovannini M Diagnosis and Management of Pollen Food Allergy Syndrome to Nuts. J Allergy Clin Immunol Pract, 2024.PMID 38280450
- [9]Kato Y Comprehensive review of pollen-food allergy syndrome: Pathogenesis, epidemiology, and treatment approaches. Allergol Int, 2025.PMID 39278756
- [10]Asero R Why lipid transfer protein allergy is not a pollen-food syndrome: novel data and literature review. Eur Ann Allergy Clin Immunol, 2022.PMID 34092069
- [11]Wolters P Lipid transfer protein allergy: characterization and comparison to birch-related food allergy. J Dtsch Dermatol Ges, 2022.PMID 36184811
- [12]Sicherer SH Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J Allergy Clin Immunol, 2018.PMID 29157945
- [13]Simons FE World Allergy Organization Anaphylaxis Guidelines: 2013 update of the evidence base. Int Arch Allergy Immunol, 2013.PMID 24008815