Paeds · allergy-and-immunology
Peanut, tree-nut and seed allergy
Also known as Peanut allergy · Tree-nut allergy · Seed allergy · Nut allergy · Sesame allergy · Cashew allergy
Fellowship guide to peanut, tree-nut and seed allergy in children: IgE-mediated pathophysiology and storage-protein families, the HealthNuts natural-history data, diagnosis with skin-prick testing, specific IgE and component-resolved diagnostics, anaphylaxis recognition and adrenaline dosing, the LEAP trial and primary prevention through early introduction, oral immunotherapy, and the practicalities of avoidance, action plans and autoinjectors across ANZ and international practice.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Peanut, tree-nut and seed allergy together form the group of food allergies most likely to persist for life and to cause severe or fatal reactions in children. A child who reacts to a trace of peanut within minutes of eating it, with urticaria spreading across the face and a tightening throat, sits at the severe end of a spectrum that also includes the toddler with only lip swelling from cashew paste and the school-age child whose only problem is itchy mouth after a hazelnut cross-reacting with birch pollen. The clinician's job is to separate the dangerous, persistent, storage-protein-driven allergies from the milder cross-reactive and the non-IgE-mediated forms, and to do so without over-labelling children who are only sensitised. [8]
Peanut is a legume, not a nut, and its cross-reactivity with tree nuts is driven less by botanical kinship than by shared stable storage proteins that resist digestion and cooking. Tree nuts include walnut, cashew, hazelnut, almond, pecan, pistachio, Brazil nut and macadamia, while the major seed allergens are sesame, sunflower, poppy and mustard. Each carries distinctive allergen components — Ara h 2 in peanut, Ana o 3 in cashew, Ses i 1 in sesame — and knowing which components matter transforms a vague positive test into a meaningful clinical prediction. [9]
The single most important advance in this field is preventive. The LEAP trial showed that early, sustained consumption of peanut in high-risk infants reduced the later development of peanut allergy by roughly 80 per cent compared with avoidance, overturning decades of advice to delay allergenic foods. Alongside prevention, modern management pairs strict avoidance and adrenaline autoinjectors with the emerging option of oral immunotherapy, which desensitises rather than cures and must be weighed against its real risk of allergic reactions during treatment. [1]
Classification
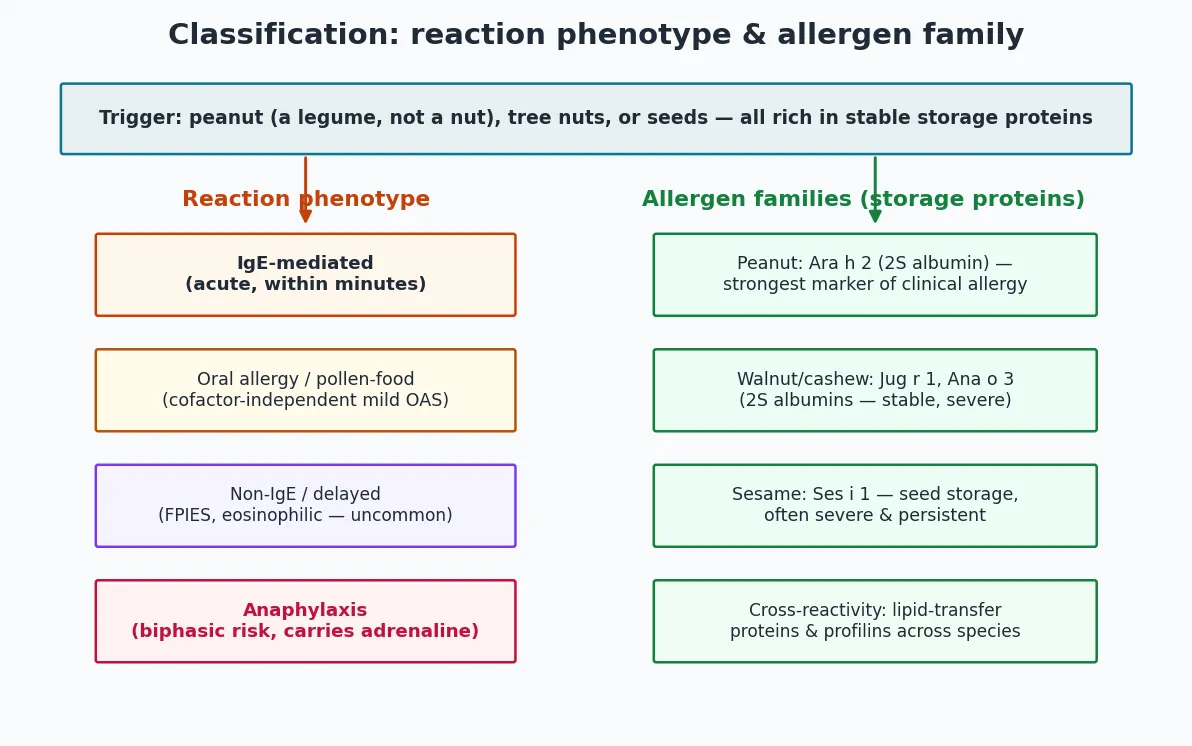
Classification runs along two axes: the immunological mechanism of the reaction and the molecular family of the offending allergen. The dominant phenotype is IgE-mediated and acute, with symptoms appearing within minutes to two hours of exposure and ranging from oral pruritus and urticaria through to anaphylaxis. A smaller and milder phenotype is the pollen-food or oral allergy syndrome, in which heat-labile proteins cross-react with airborne pollen and cause isolated oral symptoms, typically without systemic features. Non-IgE-mediated forms such as food protein-induced enterocolitis syndrome (FPIES) are uncommon with nut and seed triggers but do occur, presenting with delayed, repetitive vomiting and lethargy rather than immediate urticaria. [8]
The second axis is the allergen family, and here the storage proteins are decisive. The 2S albumins — Ara h 2 in peanut, Ana o 3 in cashew, Jug r 1 in walnut, Ses i 1 in sesame — are small, stable, digestion-resistant proteins that carry most of the clinical reactivity and the highest risk of severe reactions. Lipid transfer proteins and profilins, by contrast, are more often responsible for cross-reactivity across botanically unrelated foods and for the pollen-food syndrome. Recognising which component drives a child's sensitisation explains why one child with a positive peanut test tolerates peanut in baked goods while another reacts to a trace. [14]
[14]A practical point that examiners probe: peanut is a legume, yet a child allergic to peanut has a substantially increased chance of also being allergic to one or more tree nuts, not because of botanical closeness but because of shared epitopes and co-sensitisation. The reverse is also true. This is why a new tree-nut or seed allergy is best confirmed component by component rather than assumed from a single broad test, and why blanket "all nut" avoidance without evidence of clinical reactivity is a common error that harms nutrition and quality of life. [10]
Epidemiology & Risk Factors
Peanut allergy affects roughly 1 to 3 per cent of children in western populations, and tree-nut and seed allergies add a further burden, with cashew, walnut, hazelnut and sesame among the most common culprits. Prevalence has risen over the last two decades alongside the broader increase in allergic disease, and nut and seed allergies now account for the majority of food-induced anaphylaxis presentations to paediatric emergency departments. A repeated finding across countries is that peanut and tree-nut allergy are the foods most often implicated in fatal food anaphylaxis, with adolescents the highest-risk age group. [5]
Severity and persistence are not random. The strongest risk factors for a severe reaction are co-existing asthma, adolescence, a previous severe reaction, and a large allergen dose ingested away from home where adrenaline is unavailable. The presence of a storage-protein sensitisation, particularly Ara h 2, predicts a higher likelihood of clinical reactivity and severe symptoms than sensitisation to pollen-homologous components. Cashew allergy in young children deserves particular respect: population data show it produces anaphylaxis at least as often as peanut and frequently from very small exposures. [11]
The natural history differs sharply between foods. Peanut allergy resolves in only about one in five children by school age, and most persist for life, which is why a confirmed peanut allergy is managed as a long-term condition. Tree-nut and seed allergies resolve even less often, and cashew and walnut allergy are typically lifelong. These rates come from population-based cohort data such as HealthNuts, which tracked challenge-confirmed allergy through the first six years of life and showed that resolution, when it occurs, tends to happen early and is foreshadowed by falling specific IgE levels. [3]
Pathophysiology
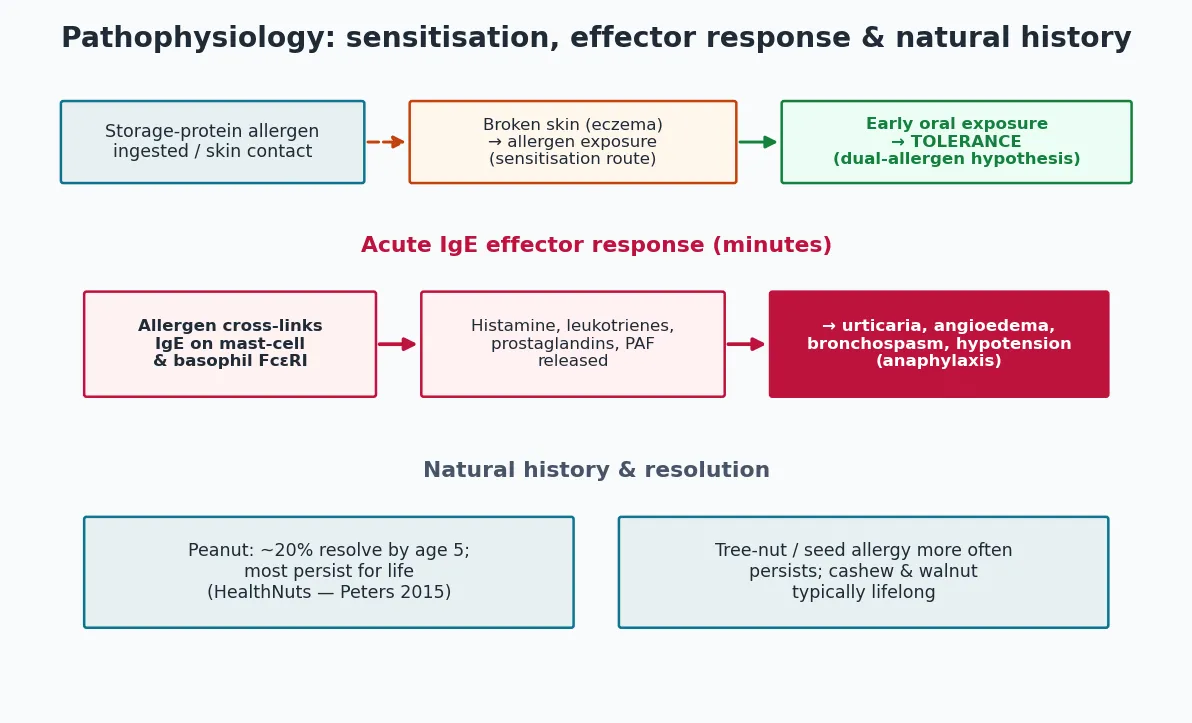
Sensitisation to a nut or seed storage protein classically begins away from the gut. The dual-allergen-exposure hypothesis holds that allergen reaching inflamed, broken skin — especially in an infant with eczema — drives the production of specific IgE and allergic sensitisation, while the same allergen reaching the gastrointestinal tract early in life promotes oral tolerance. This is the biological substrate of both the strong link between severe early eczema and peanut allergy and the success of early oral introduction as prevention. [8]
On re-exposure, the allergen cross-links allergen-specific IgE bound to the high-affinity FcεRI receptor on mast cells and basophils, triggering rapid degranulation. Histamine, leukotrienes, prostaglandins and platelet-activating factor are released into tissues and circulation, producing vasodilation, increased vascular permeability, bronchoconstriction and smooth-muscle spasm within minutes. The clinical translation is the familiar cascade of flushing, urticaria, angioedema, wheeze, vomiting, abdominal pain and hypotension — and, at its most severe, anaphylactic shock. [12]
The molecular stability of the offending protein governs the severity of this cascade. Storage proteins such as Ara h 2 resist gastric acid, digestive enzymes and heat, so a cooked, processed or trace exposure can still deliver enough intact protein to trigger a systemic reaction. Heat-labile pollen-homologous proteins, by contrast, are usually destroyed by cooking and by gastric transit, which is why the pollen-food syndrome seldom progresses beyond the mouth. Knowing this explains why a child reacts to raw but not roasted nuts, and why component testing refines risk assessment far better than whole-allergen testing alone. [14]
Persistence is immunological as much as clinical. Children whose peanut-specific IgE and Ara h 2 levels fall steadily over the first years of life are those most likely to outgrow the allergy, whereas stable or rising storage-protein IgE predicts lifelong disease. This trajectory is what makes serial specific IgE measurement and, where appropriate, supervised oral food challenge the rational basis for reassessment rather than a single test in isolation. [4]
Clinical Presentation
The history, not the laboratory, establishes the diagnosis in most cases. A typical IgE-mediated reaction begins within minutes of ingestion and unfolds over 30 minutes to two hours, with symptoms accumulating across organ systems. Cutaneous features — urticaria, flushing, angioedema of the lips, face or periorbital tissues, and pruritus — are the most common and earliest, but their absence does not exclude a serious reaction, and around one in five anaphylactic reactions have no skin features at all. [12]
Respiratory involvement is the most reliable warning of severity. Persistent cough, wheeze, stridor, hoarse voice, a sensation of throat tightness and dyspnoea signal impending airway compromise and should trigger adrenaline without waiting for hypotension. Gastrointestinal features — abdominal pain, repetitive vomiting and diarrhoea — are common in children and are easily mistaken for gastroenteritis, but in the context of a known or suspected allergen exposure they are a systemic feature. Cardiovascular collapse, pallor, floppiness and altered consciousness mark full anaphylaxis and demand immediate treatment. [13]
The pollen-food syndrome presents differently and more benignly: rapid-onset oral pruritus, tingling and mild lip or tongue swelling confined to the oropharynx after eating the raw cross-reactive food, often settling without treatment. Distinguishing it from a primary storage-protein allergy matters because the management is entirely different — the pollen-food syndrome is usually managed with avoidance of the raw trigger and antihistamines as needed, whereas a storage-protein allergy warrants an adrenaline autoinjector. [9]
Differential Diagnosis
The differential diagnosis for an apparent nut or seed reaction is broad, and the examiner will probe whether a clinician is anchoring on allergy without considering alternatives. The common pitfall is to equate any symptom after eating with IgE-mediated allergy, when the cause may be irritant, toxic, infective, or a different immunological mechanism. A careful temporal relationship to the food, reproducibility across exposures and objective signs on challenge are what separate true allergy from its mimics. [8]
[8]Two specific traps recur in paediatric practice. The first is the child labelled "nut allergic" on the basis of a positive blood test or skin-prick test alone, who has never reacted clinically and is in fact only sensitised; this overdiagnosis causes unnecessary restriction and anxiety and is resolved by a supervised oral food challenge. The second is cashew or pistachio allergy masquerading as a generic tree-nut allergy when in fact the cross-reactivity profile is specific, and other tree nuts may be safely eaten. A targeted, component-led approach lifts both traps. [10]
Clinical & Bedside Assessment
The bedside assessment begins and ends with the history, because no test substitutes for a careful account of the reaction. The clinician must establish the exact food, the dose, the time from ingestion to onset, every organ system involved, the setting, any cofactors such as exercise, NSAIDs, alcohol or intercurrent illness, and the response to any treatment given. A food-and-symptom diary for community reactions and a photograph of the packaging help when the trigger is uncertain, because the difference between a trace exposure and a full portion changes the risk profile. [8]
Examination during an acute reaction is goal-directed at identifying airway, breathing and circulatory compromise. Stridor, increased work of breathing, wheeze, oxygen desaturation, hypotension, pallor, altered consciousness and persistent vomiting are the features that meet anaphylaxis criteria and mandate adrenaline. Between reactions the examination is usually normal, though signs of co-existing atopy — eczema, allergic shiners, nasal obstruction, wheeze — are relevant because they quantify the child's atopic load and refine risk. [13]
The history also frames prevention for the next child in the family and for future siblings. An infant with severe eczema or egg allergy is precisely the high-risk group in whom early, supervised peanut introduction was shown in the LEAP trial to prevent allergy, so identifying these risk markers at routine infant checks is a clinical responsibility, not a laboratory exercise. [1]
Investigations
Diagnosis combines a compatible history with IgE-based testing, interpreted in the light of pre-test probability. Over-testing without a history is the cardinal error, because sensitisation without symptoms generates false positives and false restrictions. Skin-prick testing is quick, cheap and sensitive; a wheal of 3 mm or more greater than the negative control indicates sensitisation, and very large wheals raise the probability of clinical allergy but do not by themselves confirm it. [14]
Serum specific IgE quantifies sensitisation and is useful when skin testing is contraindicated, when antihistamines cannot be withheld, or when serial monitoring of trends is wanted. As with skin-prick testing, a positive result means sensitised, not allergic, and the likelihood of true clinical allergy rises with the titre. The decisive refinement is component-resolved diagnostics, which measures IgE against the individual allergen proteins rather than the whole extract. A positive Ara h 2, Ana o 3, Jug r 1 or Ses i 1 strongly predicts clinical reactivity and a higher risk of severe reaction, whereas Ara h 8 or profilin positivity points instead to pollen cross-reactivity and a milder phenotype. [14]
Diagnostic ladder for suspected nut or seed allergy
Take a structured reaction history (food, dose, timing, organ systems, cofactors)
Perform skin-prick testing to the suspected nut/seed (wheal ≥3 mm = sensitised)
Measure specific IgE and, if available, component IgE (Ara h 2, Ana o 3, Ses i 1)
Where the diagnosis remains uncertain or sensitisation without symptoms exists, arrange a supervised oral food challenge
Reassess periodically with serial specific IgE; re-challenge when titres fall
The supervised oral food challenge remains the gold standard and the tie-breaker when history and tests disagree. It is the only way to confirm a true clinical allergy when testing is equivocal, to establish a threshold dose, and to demonstrate that a child has outgrown the allergy. Because it can provoke a severe reaction, it must be performed in a controlled setting with trained staff and resuscitation equipment, and it is generally undertaken after a period of stable or falling specific IgE. [8]
Management — Resuscitation
When a child presents with an acute reaction, the first decision is whether this is anaphylaxis, because that determines whether adrenaline is given immediately or reserved. Anaphylaxis is a rapidly evolving, multi-system allergic reaction that compromises airway, breathing or circulation; once any of these is involved, intramuscular adrenaline into the anterolateral thigh is the first-line treatment and should not be delayed for investigation or a blood pressure reading. [12]
Adrenaline (epinephrine) — intramuscular
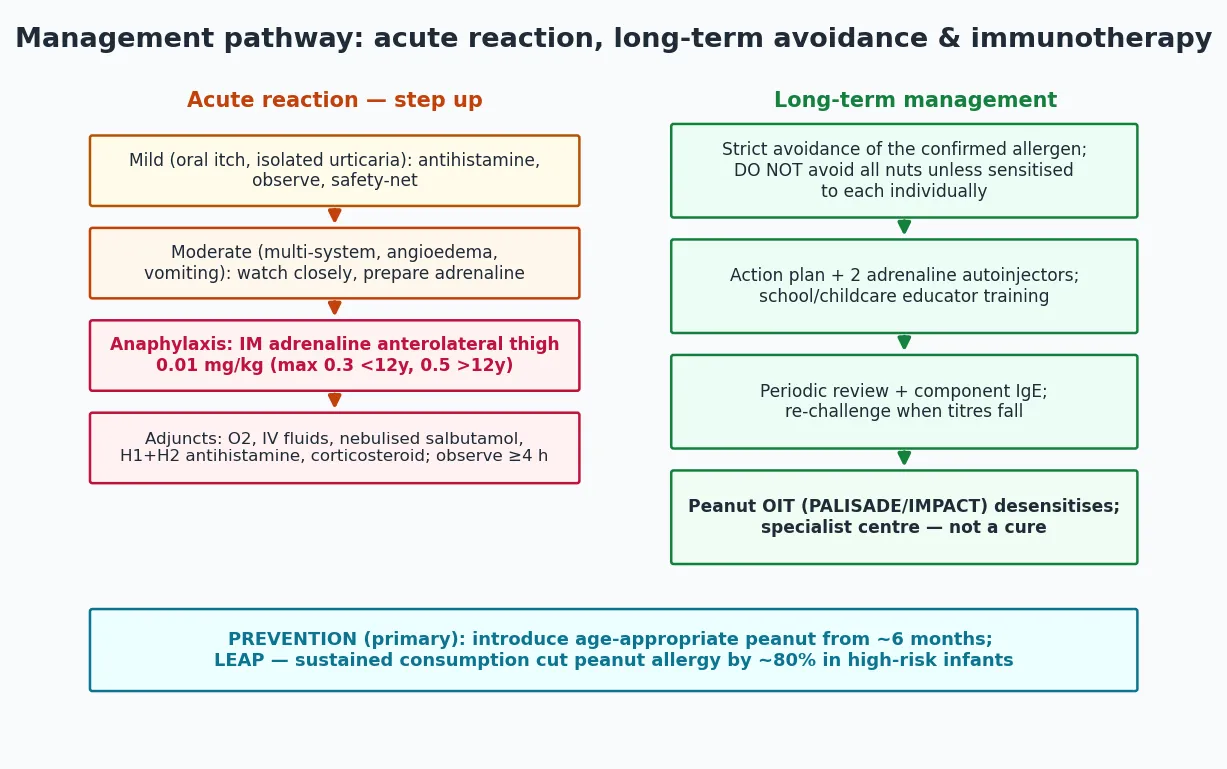
Adrenaline works through alpha-1 vasoconstriction to restore blood pressure and reduce angioedema, beta-2 bronchodilation to relieve wheeze, and stabilisation of mast cells to halt further mediator release. Dose errors and delays are the most common reason for a poor outcome, and giving it into the thigh rather than the arm or subcutaneously is essential for reliable absorption. Repeat doses may be needed within five minutes if features persist, and the dose is weight-based, administered intramuscularly, with autoinjector strengths chosen to approximate 0.01 mg per kilogram. [12]
Adjuncts support but never replace adrenaline. High-flow oxygen, intravenous fluid boluses for shock, nebulised salbutamol for persistent bronchospasm, and an H1-antihistamine for urticaria and pruritus are the standard additions; corticosteroids are commonly given to modulate late-phase inflammation but do not treat the acute episode and are not life-saving. Supine positioning with leg elevation (or left lateral in vomiting or pregnancy) improves venous return, and sitting a shocked child up can be fatal. [13]
Management — Definitive & Stepwise
Definitive management rests on three pillars: avoidance of the confirmed allergen, a written action plan with an adrenaline autoinjector, and ongoing education and review. Avoidance must be specific to the clinically reactive food, because blanket avoidance of all nuts when only one is allergic is unnecessarily restrictive and harms nutrition, growth and social participation. Reading labels, recognising precautionary "may contain" statements and educating the child and carers are the daily realities that prevent reactions. [9]
Every child with a confirmed IgE-mediated nut or seed allergy should have a written, personalised action plan that distinguishes mild and severe reactions and names the adrenaline dose, and should carry at least one adrenaline autoinjector, with two for those at higher risk or in remote settings. School and childcare staff must be trained in recognition and autoinjector use, and the child should wear medical identification. The plan is rehearsed regularly, because skill decay between reactions is a real and dangerous phenomenon. [15]
The anaphylaxis action plan — AIR
Oral immunotherapy has moved from research into selected practice for peanut allergy. The PALISADE trial of AR101 and the IMPACT trial in young children showed that graded oral exposure can desensitise the majority of treated children, raising the reaction threshold and reducing the risk from accidental exposure. The trade-off is real: treatment itself causes allergic reactions in a substantial minority, eosinophilic oesophagitis is a recognised complication, and desensitisation is not the same as sustained tolerance or cure. Immunotherapy is therefore a specialist-centred, shared-decision option rather than a blanket recommendation. [6]
Specific Subtypes & Scenarios
Peanut allergy is the prototype and the best studied. It is common, tends to persist, and is the food most often implicated in fatal anaphylaxis alongside tree nuts. Component testing changes practice here: a child sensitised to Ara h 2 carries a high risk of clinical allergy and severe reaction, while one sensitised only to Ara h 8 usually has a mild, pollen-related phenotype. Because roughly a fifth of children outgrow peanut allergy by school age, periodic reassessment with specific IgE and, where appropriate, challenge is part of good care. [3]
Cashew and walnut allergy deserve separate emphasis because they are frequently severe in young children. Population data show cashew causes anaphylaxis at least as often as peanut and often from very small doses, with Ana o 3 the key diagnostic component. Pistachio cross-reacts strongly with cashew, and the two are usually managed together, whereas other tree nuts may be tolerated and should be assessed on their own merits rather than assumed allergenic. Sesame allergy shares this severe, persistent profile and is now a declared major allergen in several jurisdictions, with Ses i 1 the dominant storage protein. [11]
The high-risk infant is a scenario in its own right and the one where prevention is possible. Severe eczema or egg allergy in infancy marks the group in whom early, supervised peanut introduction, sustained from around four to six months, prevented most peanut allergy in the LEAP trial. The addendum guidelines and ASCIA guidance operationalise this: test high-risk infants early, introduce peanut in an age-appropriate form under supervision if indicated, and maintain regular consumption. [1]
Complications & Pitfalls
The complications of nut and seed allergy range from the acute and life-threatening to the chronic and psychosocial. Acutely, anaphylaxis can be fatal, and biphasic reactions that recur four to 24 hours after apparent resolution can catch families and clinicians off guard, which is why observation after a significant reaction and clear safety-net advice are essential. Anxiety and reduced quality of life are pervasive among affected children and families, and over-restriction compounds this harm. [15]
The most common diagnostic pitfall is the over-interpretation of testing. A positive skin-prick or specific IgE result indicates sensitisation, not clinical allergy, and attaching an "allergic" label on a test alone can consign a child to years of unnecessary avoidance. The mirror-image error is to dismiss a convincing history because the test is negative, missing a genuine allergy that may have a component the standard extract does not capture. Both errors are corrected by returning to the history and, where indicated, the oral food challenge. [8]
Management pitfalls cluster around adrenaline. Delaying adrenaline for antihistamines or observation, giving it by the wrong route, prescribing a single autoinjector for a high-risk child, and failing to train carers are all recurring contributors to poor outcomes. On the avoidance side, over-labelling a child as "allergic to all nuts" when only one is reactive, and failing to reassess over time, are the errors that turn a manageable condition into an unnecessarily disabling one. [9]
Prognosis & Disposition
Peanut allergy resolves in only about a fifth of children by school age, and tree-nut and seed allergies resolve even less often, so the working assumption for a confirmed storage-protein allergy is persistence. Resolution, when it occurs, tends to be early and is predicted by falling specific IgE and a successful supervised challenge, after which the food is reintroduced and the autoinjector plan can be retired. Adolescence is the highest-risk period for fatal reactions, driven by risk-taking, inconsistent autoinjector carriage and uncontrolled asthma, and merits focused transitional care. [4]
Disposition after an acute reaction depends on severity and risk. A mild reaction that resolves fully can be observed briefly and discharged with safety-net advice and a review appointment, whereas anaphylaxis mandates a period of observation for biphasic recurrence, admission for those with severe features or asthma, and a clear plan for follow-up including an action plan, autoinjector prescription and referral to an allergy specialist. Every significant reaction is a trigger to review the child's plan, asthma control and autoinjector technique. [13]
In Australia and New Zealand, ASCIA provides the standardised action plans, autoinjector dose bands and school training that underpin community management, with two autoinjectors commonly recommended for those at higher risk or in remote settings. UK practice follows BSACI and NICE guidance with similar principles, North American practice follows the NIAID addendum and anaphylaxis parameters, and European practice follows EAACI guidance. The disease is the same; the dose bands, school laws and funding differ, so name the regional framework you are applying.
[9]Special Populations
Adolescents carry the highest risk of fatal food-induced anaphylaxis, a finding driven by risk-taking behaviour, inconsistent autoinjector carriage, alcohol and exercise cofactors, and uncontrolled asthma. Transitional care that gives the young person ownership of their plan, rehearses autoinjector use, addresses asthma aggressively and plans for eating out, travel and independence is a core part of management, and the plan should move with the patient into adult services. [5]
Children with complex or chronic disease — severe eczema, eosinophilic oesophagitis, or multiple food allergies — need coordinated care, because nut and seed allergy rarely exists in isolation. The infant with severe eczema is the prevention target of the LEAP paradigm, and identifying and acting on this risk early is a clinical duty. In migrant, refugee and remote communities, access to specialist services, autoinjectors and culturally appropriate education can be the limiting factor, and telehealth-supported shared care with local clinicians helps close the gap. [15]
Indigenous children in Australia and New Zealand share the rising burden of allergic disease seen in the wider population, and culturally safe, family-centred care that integrates allergy management with the child's broader health needs is the standard. The principles are identical to those for any child — accurate diagnosis, specific avoidance, a workable action plan and trained carers — delivered in partnership with primary care and, where relevant, Aboriginal and Torres Strait Islander health services. [9]
Evidence, Guidelines & Regional Differences
The evidence base has been transformed by randomised trials. The LEAP trial established that sustained early peanut consumption in high-risk infants reduced peanut allergy by roughly 80 per cent, and the EAT trial explored broader early introduction, with methodological debate about adherence but a consistent directional signal. The PALISADE and IMPACT trials established that oral immunotherapy desensitises, without proving sustained tolerance, and they defined the treatment-related reaction risk that families must weigh. Population cohort data from HealthNuts defined the natural history and resolution rates that frame prognosis. [2]
The NIAID addendum, ASCIA, BSACI and EAACI guidance now broadly converge: introduce allergenic solids, including peanut, from around six months (and from four to six months in high-risk infants with severe eczema or egg allergy, after testing where indicated), and maintain regular consumption. The era of blanket delayed introduction is over. The exact testing-then-introduction pathway for high-risk infants varies by region, so cite your local guideline at the exam.
[1]Controversies persist and examiners test them. Whether immunotherapy should be offered to all children or only those at highest risk, how to interpret precautionary "may contain" labelling, the role of component testing in routine practice, and the appropriate threshold for prescribing an autoinjector in a child with a mild phenotype are all live debates with no single right answer. The defensible position is to ground each decision in the child's individual risk — history, components, asthma, age, and access to care — and in the relevant regional guideline. [15]
Exam Pearls
A fellowship candidate should be able to walk an examiner from a reaction history through skin-prick testing and component diagnostics to an action plan, and then to defend the early-introduction prevention evidence with the LEAP data. Expect to be pushed on when to challenge rather than test, when to prescribe two autoinjectors, how to counsel a family about the risks of immunotherapy, and how to manage a teenager who does not carry their device. The answers are individualised to the child but grounded in the same evidence base. [9]
The recurring trap in written questions is the false equivalence of a positive test with a clinical allergy; the correct next step when sensitisation lacks symptoms is the oral food challenge, not lifelong avoidance. The recurring trap in clinical questions is delayed adrenaline; the correct first step in anaphylaxis is intramuscular adrenaline into the thigh, not an antihistamine, not observation, and not waiting for a blood pressure. Holding these two principles — challenge to confirm, adrenaline first — answers most of what the exam asks. [8]
References
- [1]Du Toit G, Roberts G, Sayre PH, Bahnson HT, Radulovic S, Santos AF, et al. (LEAP Study Team) Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med, 2015.PMID 25705822
- [2]Perkin MR, Logan K, Tseng A, Raji B, Ayis S, Peacock J, et al. (EAT Study Team) Randomized Trial of Introduction of Allergenic Foods in Breast-Fed Infants. N Engl J Med, 2016.PMID 26943128
- [3]Peters RL, Allen KJ, Dharmage SC, Tang ML, Koplin JJ, Ponsonby AL, et al. (HealthNuts) Natural history of peanut allergy and predictors of resolution in the first 4 years of life: a population-based assessment. J Allergy Clin Immunol, 2015.PMID 25725989
- [4]Peters RL, Koplin JJ, Gurrin LC, Dharmage SC, Wake M, Ponsonby AL, et al. (HealthNuts) The natural history of peanut and egg allergy in children up to age 6 years in the HealthNuts population-based longitudinal study. J Allergy Clin Immunol, 2022.PMID 35597613
- [5]Sicherer SH, Muñoz-Furlong A, Godbold JH, Sampson HA US prevalence of self-reported peanut, tree nut, and sesame allergy: 11-year follow-up. J Allergy Clin Immunol, 2010.PMID 20462634
- [6]Vickery BP, Vereda A, Casale TB, Beyer K, du Toit G, Hourihane JO, et al. (PALISADE Group) AR101 Oral Immunotherapy for Peanut Allergy. N Engl J Med, 2018.PMID 30449234
- [7]Jones SM, Shreffler WG, Pons L, Kulis M, Zoratti EM, Streif D, et al. (IMPACT) Efficacy and safety of oral immunotherapy in children aged 1-3 years with peanut allergy (IMPACT trial). Lancet, 2022.PMID 35065784
- [8]Boyce JA, Assa'ad A, Burks AW, Jones SM, Sampson HA, Wood RA, et al. (NIAID-Sponsored Expert Panel) Guidelines for the diagnosis and management of food allergy in the United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol, 2010.PMID 21134576
- [9]Stiefel G, Anagnostou K, Boyle RJ, Cale T, Clark A, Ewan P, et al. BSACI guideline for the diagnosis and management of peanut and tree nut allergy. Clin Exp Allergy, 2017.PMID 28836701
- [10]McWilliam VL, Koplin JJ, Walton J, Tang ML, Sheehan P, Ponsonby AL, et al. (HealthNuts) Patterns of tree nut sensitization and allergy in the first 6 years of life in a population-based cohort. J Allergy Clin Immunol, 2019.PMID 30171872
- [11]Brettig T, Remington BC, Kummeling L, Peters RL, Allen KJ, McWilliam V, et al. Cashew Allergy Prevalence and Sensitization in 1-Year-Old Infants. J Allergy Clin Immunol Pract, 2023.PMID 37481112
- [12]Shaker MS, Wallace DV, Golden DBK, Oppenheimer J, Bernstein JA, Campbell RL, et al. Anaphylaxis — a 2020 practice parameter update, systematic review, and Grading of Recommendations, Assessment, Development and Evaluation (GRADE). J Allergy Clin Immunol, 2020.PMID 32001253
- [13]Muraro A, Worm M, Alviani C, Cardona V, DunnGalvin A, González-Mancebo E, et al. EAACI guidelines: Anaphylaxis (2021 update). Allergy, 2022.PMID 34343358
- [14]Santos AF, Beyer K, Bindslev-Jensen C, Eigenmann PA, Fernández-Rivas M, Host A, et al. EAACI guidelines on the diagnosis of IgE-mediated food allergy. Allergy, 2023.PMID 37815205
- [15]Santos AF, Du Toit G, O'B Hourihane J, Togias A, Jones SM, Wood RA, et al. EAACI guidelines on the management of IgE-mediated food allergy. Allergy, 2025.PMID 39473345