Paeds · allergy-and-immunology
Urticaria and angioedema
Also known as Hives · Nettle rash · Chronic spontaneous urticaria · Angio-oedema · Hereditary angioedema · CSU
A fellowship-grade approach to urticaria and angioedema in children: how to read a transient rash against the clock of six weeks, how to separate the common histamine-mediated majority from the rare but dangerous bradykinin-mediated minority, how to escalate treatment from second-generation antihistamines through omalizumab, and when angioedema of the larynx demands adrenaline or C1-inhibitor concentrate rather than another tablet.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a six-year-old who wakes with itchy pink lumps over her trunk. Each one moves and fades within hours, replaced by new ones elsewhere, and by morning she is back to normal skin. Her parents are frightened; the child is mostly annoyed. That picture — transient, migratory, intensely itchy wheals that individually resolve within twenty-four hours leaving normal skin — is urticaria, and recognising its rhythm is what separates it from every other childhood rash. [1] [5]
Urticaria is the appearance of wheals (raised, erythematous, oedematous papules or plaques with a pale centre), angioedema, or both. A wheal has three hallmarks: a raised central swelling of variable size surrounded by a reflex erythema, an associated itch — sometimes a burning sensation — and a fleeting nature, with the skin returning to normal within twenty-four hours. The driving event is mast-cell activation in the superficial dermis, with release of histamine and other mediators that produce vasodilation and extravasation of fluid. [1] [14]
Angioedema is the deeper sibling: swelling in the dermis, subcutaneous tissue or submucosa. It may accompany urticaria — as it does in about half of children with acute urticaria — or it may occur alone, and when it occurs alone the mechanism question changes entirely. Angioedema with wheals is almost always histamine-mediated. Angioedema without wheals may be bradykinin-mediated, and that single distinction changes the entire management. [1] [10]
The six-week clock is the other hinge. Acute urticaria lasts under six weeks and is overwhelmingly self-limiting, usually triggered by infection, drug or food in children. Chronic urticaria — defined as symptoms persisting or recurring on most days for six weeks or more — is further divided into chronic spontaneous urticaria (no identifiable external trigger) and chronic inducible urticaria (reproducibly triggered by a specific physical stimulus such as cold, pressure or dermographism). This time threshold is not arbitrary: it separates a condition that resolves on its own from one that needs a stepwise escalation plan and a search for mimics. [1] [4]
The numbers that frame the problem
Classification
The international urticaria guideline classifies the condition along two axes: duration and trigger. On the duration axis you separate acute (under six weeks) from chronic (six weeks or more). On the trigger axis you separate spontaneous (no external trigger) from inducible (a reproducible physical stimulus produces the wheal). These two axes combine to give every case a precise name, and the name tells you what to do next. [1] [14]
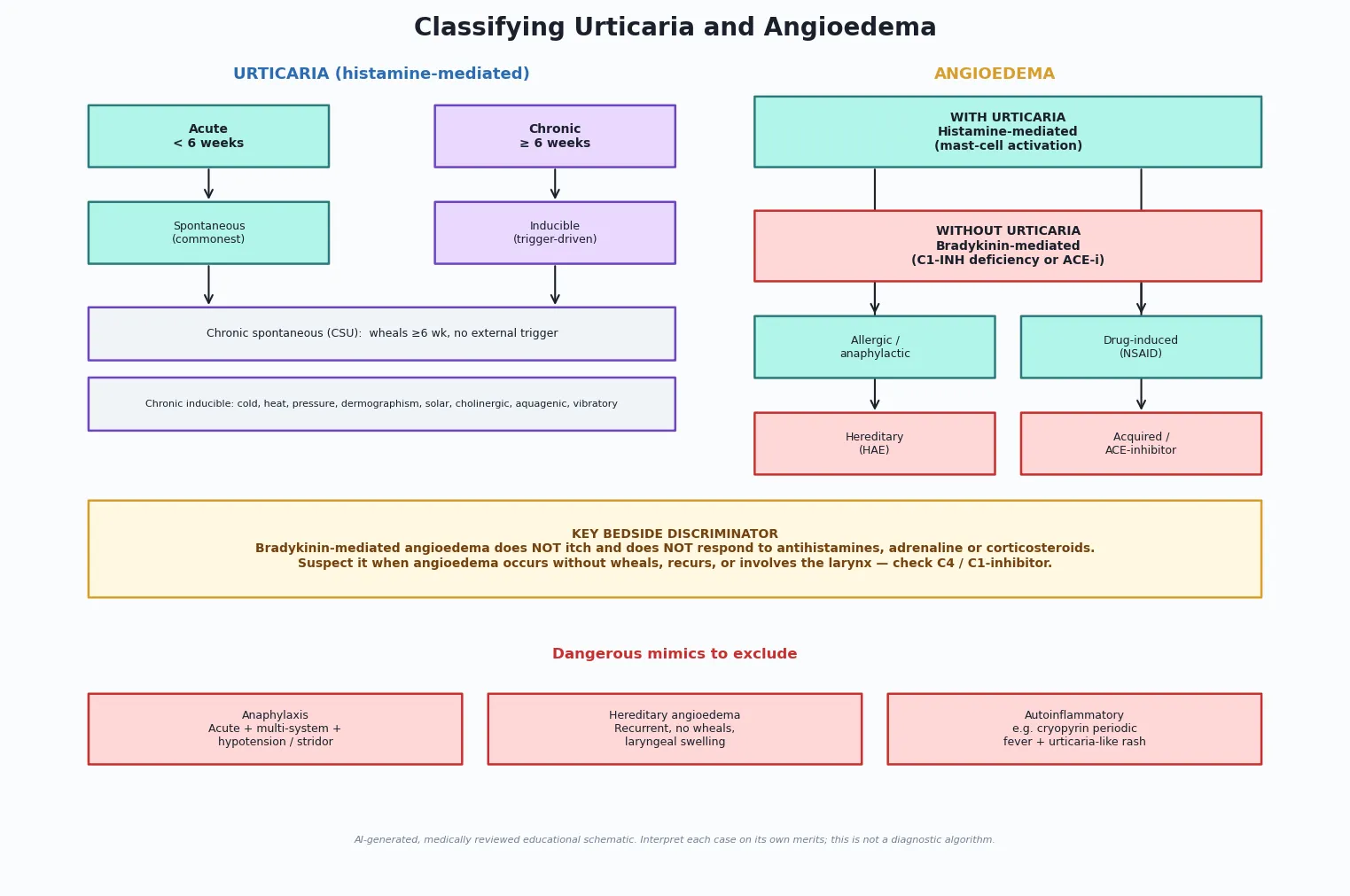
Chronic inducible urticaria is named for its trigger: symptomatic dermographism (wheals from a firm stroke of the skin), cold contact urticaria, delayed-pressure urticaria, solar urticaria, heat contact urticaria, cholinergic urticaria (wheals triggered by a rise in core body temperature), aquagenic urticaria, contact urticaria (wheals at the site of direct skin contact with a substance) and vibratory angioedema. Identifying an inducible trigger is useful because it focuses avoidance and because the response to antihistamines is often excellent. [1]
Angioedema sits in its own classification because the mechanism question overrides everything. When angioedema occurs together with wheals, it is histamine-mediated and follows the urticaria management. When it occurs without wheals, it may be bradykinin-mediated: hereditary angioedema (C1-inhibitor deficiency, types I and II, or normal-C4 hereditary angioedema with a factor XII mutation), acquired C1-inhibitor deficiency, or drug-induced (ACE-inhibitor or, less commonly, NSAID). The international hereditary angioedema guideline for paediatric patients sets the standard for diagnosis, on-demand treatment and prophylaxis in children. [9] [10]
Acute spontaneous (<6 wk)
The common presentation
- Triggered by infection (commonest in children), drug, food or idiopathic
- Self-limiting; usually resolves within days
- Second-generation antihistamine ± short course if severe
- Safety-net and review; antihistamines and steroids are symptomatic, not curative
Chronic spontaneous (≥6 wk)
Needs a stepwise plan
- No identifiable external trigger; autoimmune in a subset
- Stepwise: standard-dose antihistamine → up-titrate to 4× → omalizumab → specialist
- Screen for alarm features before accepting the label
- Most resolve within 1–5 years; quality of life impact is substantial
Chronic inducible
Trigger-driven
- Symptomatic dermographism, cold, delayed-pressure, solar, cholinergic, aquagenic
- Reproducible with the physical stimulus; confirm by provocation testing
- Avoidance + standard-dose antihistamine; up-titrate if needed
- Cold urticaria carries a drowning risk — warn about cold water swimming
Bradykinin-mediated angioedema
Rare, dangerous
- Hereditary angioedema (C1-INH deficiency) or acquired; ACE-inhibitor
- No wheals, no itch; laryngeal and GI involvement
- Does NOT respond to antihistamines, adrenaline or steroids
- C1-INH concentrate or icatibant for acute attacks; prophylaxis with lanadelumab or C1-INH
Epidemiology & Risk Factors
Acute urticaria is one of the commonest rashes a paediatric clinician will see: roughly one in six children experiences at least one episode, and the peak age is early childhood when viral infections are frequent. A Spanish paediatric emergency department cohort found that the commonest triggers in children presenting with acute urticaria were infections (often viral upper respiratory tract infections) and drugs — with antibiotics and NSAIDs prominent — while foods were identified far less often than parents expect. [5] [6]
Chronic urticaria is far less common in children than in adults. A global systematic review and meta-analysis estimated the point prevalence of chronic urticaria in children at well under one per cent, lower than the adult figure, with a female predominance emerging in adolescence. About a third of children with chronic urticaria have angioedema alongside their wheals, which raises the impact and the duration. [2]
Trigger categories in acute childhood urticaria
- Infection — viral upper respiratory tract infection is the single commonest identifiable trigger
- Drugs — beta-lactam antibiotics and NSAIDs lead the drug list
- Foods — over-estimated by families; a true food trigger is less common than parental concern implies
- Idiopathic — a substantial minority have no trigger identified despite thorough history
Risk factors for chronic disease
- Female sex (more prominent in adolescence and adulthood)
- Coexisting atopic disease in a subset, though chronic urticaria is not classically atopic
- Autoimmunity — a proportion have functional autoantibodies against IgE or the IgE receptor
- Thyroid autoimmunity — associated; thyroid function and antibodies are reasonable to check in refractory disease
Host and setting factors
- NSAID hypersensitivity exacerbates chronic spontaneous urticaria in a subset
- Stress and intercurrent illness worsen symptoms
- Cold-contact urticaria carries drowning risk — relevant for rural, remote and outdoor settings
- Health-literacy and access barriers delay specialist escalation for refractory disease
Hereditary angioedema is rare, with an estimated prevalence of about one in fifty thousand, and symptoms typically begin in childhood — the first attack often occurs in the first or second decade. Because the diagnosis is missed for years in many patients, a family history of unexplained swelling, abdominal pain or airway compromise is a high-yield clue. The dedicated paediatric hereditary angioedema guideline emphasises that children with recurrent angioedema without wheals should be screened with a C4 level, followed by C1-inhibitor antigenic and functional assays if low. [9] [10]
Pathophysiology
The wheal is the visible endpoint of mast-cell activation in the superficial dermis. When a mast cell degranulates, it releases histamine, platelet-activating factor, prostaglandin D2 and leukotrienes, which collectively produce vasodilation, increased vascular permeability and sensory nerve stimulation. Fluid leaks into the superficial dermis to form the wheal; the reflex erythema surrounds it; the itch drives the child to scratch. Because individual mast-cell activation events are transient, an individual wheal appears, grows, migrates and disappears within twenty-four hours — a feature no other common childhood rash shares. [1] [14]
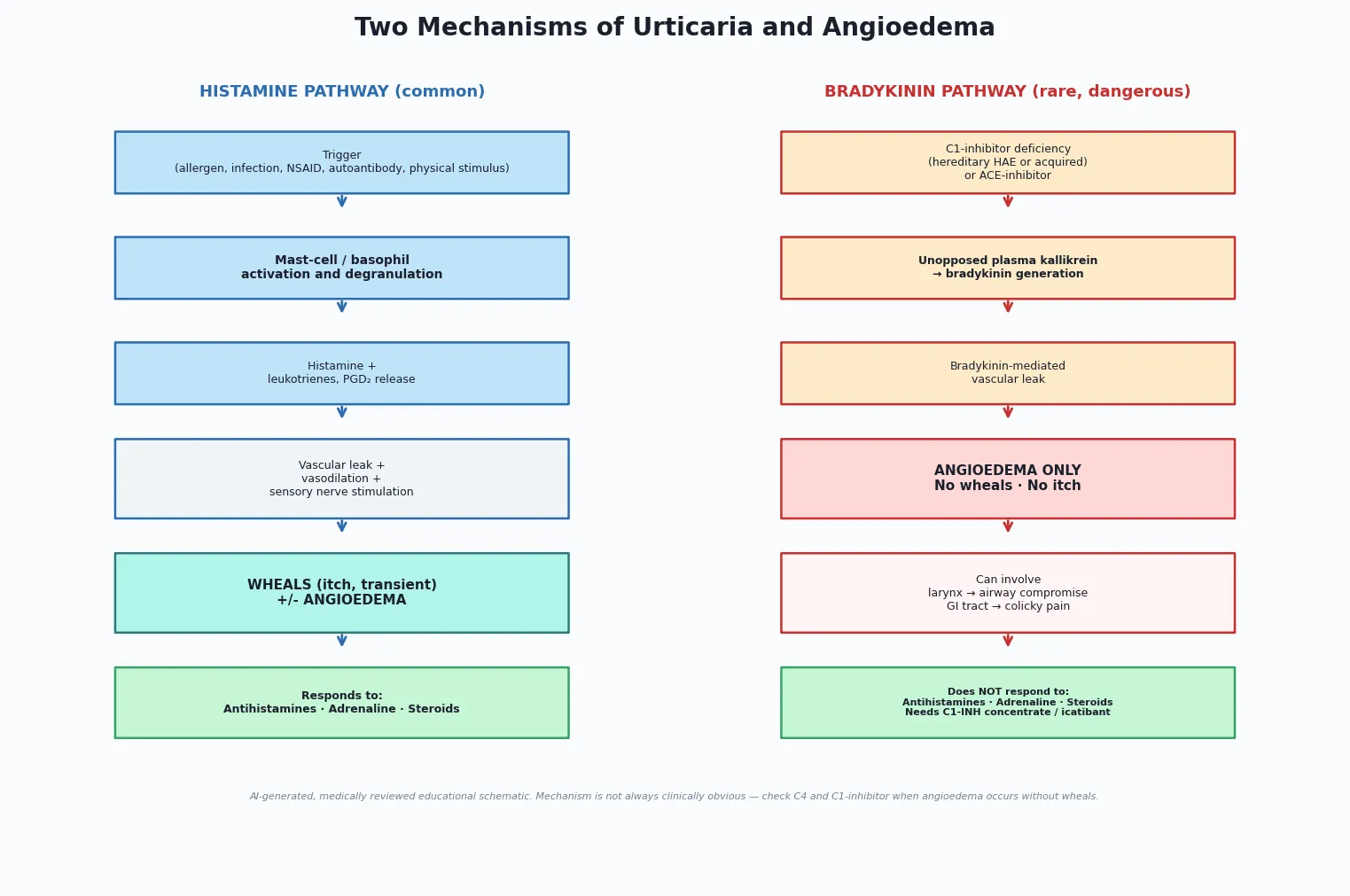
The trigger for mast-cell activation varies. In acute urticaria, infection (especially viral), drug (beta-lactams, NSAIDs) or food allergens cross-link IgE on the mast-cell surface or act through direct mast-cell activation. In chronic spontaneous urticaria, a substantial proportion of patients have functional autoantibodies directed against the high-affinity IgE receptor or IgE itself — an autoimmune mechanism that explains why the disease behaves like a chronic inflammatory condition and why it responds to immunomodulation in refractory cases. [1] [3]
The bradykinin pathway is entirely separate. In hereditary angioedema, a deficiency (type I) or dysfunction (type II) of C1-inhibitor allows unopposed plasma kallikrein activity, which cleaves high-molecular-weight kininogen to generate bradykinin. Bradykinin binds to vascular B2 receptors, producing deep-tissue angioedema without itch or wheals. The same endpoint can be reached through an ACE-inhibitor: by blocking bradykinin breakdown, the drug allows bradykinin to accumulate. This is why ACE-inhibitor angioedema and hereditary angioedema share the feature of antihistamine-resistance — the mediator is bradykinin, not histamine. [9] [10]
Understanding mechanism is not an academic exercise: it predicts treatment. Antihistamines block H1 receptors and so work only when histamine is the mediator. Adrenaline and corticosteroids suppress mast-cell activation and its consequences. None of these touch a bradykinin-driven attack. A child in laryngeal oedema from hereditary angioedema given repeated doses of adrenaline, antihistamines and hydrocortisone will not improve — and the time spent on those treatments is time the airway does not have. [9] [13]
Clinical Presentation
The presentation depends on which structure is involved and how fast it is evolving. A child with urticaria alone is itchy, uncomfortable and frightened, but not usually in danger. A child with angioedema of the lips and periorbital region is distressed and the family is alarmed, but the airway is usually intact. A child with angioedema involving the tongue, floor of mouth, or larynx is in immediate danger. Reading that gradient — skin, then face, then airway — is the clinical skill. [1] [13]
The wheal itself is the signature. Parents often describe "bites" or "bumps" that move around, appear and disappear over hours, and leave normal skin. Ask three questions of every wheal: does each individual lesion resolve within twenty-four hours (yes in urticaria), does it leave normal skin with no residual bruising or scale (yes in urticaria), and does it itch or burn (yes in urticaria). If any answer is no — the lesion lasts days, leaves bruising, or is painful rather than itchy — reconsider the diagnosis and look for urticarial vasculitis or another mimic. [1] [4]
| Presentation | What it means | What you do |
|---|---|---|
| Itchy migratory wheals, well child | Acute urticaria, almost certainly self-limiting | Antihistamine, identify trigger, safety-net, review |
| Wheals plus lip or facial swelling, no airway signs | Angioedema with urticaria — histamine-mediated | Antihistamine ± short-course steroid; observe for airway involvement |
| Tongue, floor-of-mouth or laryngeal swelling, stridor, drooling | Airway-compromising angioedema — emergency | IM adrenaline, airway team, secure airway; if bradykinin suspected, give C1-INH concentrate or icatibant |
| Wheals plus hypotension, respiratory distress or GI symptoms | Anaphylaxis | IM adrenaline, oxygen, fluid, observation; do not call it 'just urticaria' |
| Recurrent angioedema without wheals, intermittent abdominal pain | Possible hereditary angioedema | Check C4 and C1-inhibitor; allergy referral; emergency action plan |
| Daily wheals for six weeks or more | Chronic spontaneous urticaria | Stepwise plan; screen for alarm features; quality-of-life assessment |
Angioedema without urticaria deserves special attention because the first episode may be the one that compromises the airway. The swelling is non-pitting, non-dependent and not itchy. It may involve the face, limbs, genitals, or the gastrointestinal tract — where bradykinin-mediated bowel-wall oedema produces severe, colicky abdominal pain, sometimes with vomiting, that can be mistaken for a surgical abdomen. A family history of similar episodes, or of relatives needing intubation for swelling, is the clue that this is hereditary angioedema. [9] [10]
Chronic urticaria presents differently from acute disease: the child has wheals on most days for six weeks or more, often with angioedema, and the family is exhausted. The quality-of-life impact is comparable to that of a chronic skin disease, with sleep disruption, school absence and social embarrassment. Assessing the burden — not just the rash — is part of the consultation, because treatment intensity should track impact, not just appearance. [3] [4]
Differential Diagnosis
The differential has two layers: the differential of a "urticaria-like" rash that is not urticaria, and the differential of triggers and mimics within true urticaria. The first layer protects the child from a missed dangerous diagnosis; the second protects the family from unnecessary elimination diets and investigations. [1] [4]
The most important non-urticaria mimic is urticarial vasculitis, in which individual lesions last longer than twenty-four hours, are painful or burning rather than itchy, leave residual bruising or hyperpigmentation, and may be accompanied by systemic features such as fever, arthralgia and abdominal pain. Urticarial vasculitis is rare in children but demands different investigation and management, and it is the reason the twenty-four-hour rule for individual wheals exists. [1] [4]
Ordinary urticaria
- Individual wheals resolve within 24 h leaving normal skin
- Itchy, migratory, evanescent
- Responds to antihistamine
- No systemic features unless anaphylaxis
Urticarial vasculitis
- Lesions last >24 h, leave bruising or hyperpigmentation
- Painful or burning more than itchy
- May have fever, arthralgia, abdominal pain
- Needs skin biopsy and vasculitis work-up; do not treat as simple urticaria
Autoinflammatory rash
- Cryopyrin-associated periodic syndromes (CAPS): urticaria-like rash with fever from birth
- Rash is daily and non-pruritic or mildly pruritic, accompanies fever flares
- Associated with arthralgia, conjunctivitis, hearing loss
- IL-1 blockade is transformative; rheumatology and immunology referral
Other mimics
- Erythema multiforme — target lesions, mucosal involvement, often HSV-related
- Atopic dermatitis — eczematous, chronic, not transient wheals
- Viral exanthems — morbilliform, not evanescent or itchy in the same way
- Scabies, insect bites, mastocytosis (urticaria pigmentosa)
The autoinflammatory syndromes deserve a specific mention because their rash looks like urticaria but is not mast-cell-driven in the usual sense. In cryopyrin-associated periodic syndromes (familial cold autoinflammatory syndrome, Muckle-Wells syndrome, neonatal-onset multisystem inflammatory disease), a daily non-pruritic or mildly pruritic urticaria-like rash accompanies recurrent fever, arthralgia and conjunctivitis, often from early infancy. The EULAR/ACR points to consider guide the diagnosis and the IL-1 blockade that can transform the child's outlook. A baby with "urticaria" and fever is not having an allergic reaction — consider autoinflammation. [11] [12]
Clinical & Bedside Assessment
Begin with the wheal itself. Confirm the three defining features: transient (individual lesion under twenty-four hours), normal skin after resolution (no bruising or scale), and itchy. Ask the family to time how long a single wheal lasts and whether it leaves a mark — a photograph diary is invaluable because the rash is often absent by the time of consultation. Examine the skin for distribution, dermographism (lightly stroke the skin and watch for a wheal), and any features of a mimic such as fixed lesions, bruising or target lesions. [1] [4]
Take a structured history covering onset, duration, frequency, individual lesion lifespan, associated angioedema, itch quality, triggers (infection, drug, food, physical stimulus, stress), response to antihistamine, systemic features, and family history of swelling or allergy. The timeline matters: distinguish continuous disease from episodic, and date the first episode against the six-week threshold. Ask specifically about NSAID intake, new medications, recent illness, and — for angioedema — a family history of airway swelling or unexplained abdominal pain. [1] [5]
Bedside assessment of urticaria and angioedema
Confirm it is urticaria
Individual wheal under 24 h, normal skin after, itchy. If not, reconsider the diagnosis before treating as urticaria.
Grade the danger
Look for airway angioedema (stridor, drooling, voice change) and anaphylaxis (hypotension, respiratory distress). Treat before assessing further.
Split the pathway
Angioedema with wheals → histamine. Angioedema without wheals → consider bradykinin; check C4.
Identify the trigger and the clock
Acute (<6 wk): infection, drug, food. Chronic (≥6 wk): screen for alarm features before labelling.
Assess the impact
Sleep, school, quality of life — treatment intensity tracks impact, not just appearance.
Build the safety-net
What change brings them back, how urgently, and where — especially airway signs and anaphylaxis.
In the child with chronic disease, assess for alarm features that should prompt investigation beyond a diagnosis of chronic spontaneous urticaria: fever, weight loss, arthralgia, night sweats, lesions lasting over twenty-four hours, bruising, and a non-response to antihistamine. Their absence supports a confident clinical diagnosis of chronic spontaneous urticaria without extensive laboratory testing; their presence demands further work-up. [1] [4]
Investigations
Most children with acute or chronic spontaneous urticaria need no investigations at all. The diagnosis is clinical, and a battery of allergy tests in a child with chronic spontaneous urticaria is low-value: food-specific IgE panels in a child without a reproducible food-triggered history produce false positives, unnecessary elimination diets, and anxiety. The international guideline is explicit that routine allergy testing is not indicated in chronic spontaneous urticaria. [1] [4]
Rarely needed in ordinary urticaria
- Full blood count, CRP and ESR in straightforward acute or chronic spontaneous urticaria
- Allergy panels (specific IgE, skin prick) without a compatible history
- Thyroid function and thyroid antibodies in uncomplicated disease
- Complement studies when angioedema is always with wheals
Targeted and question-driven
- Thyroid function and antibodies in refractory chronic urticaria
- Stool for ova/cysts/parasites in endemic or relevant exposure settings
- Provocation testing for suspected inducible urticaria (ice cube, dermographometer)
- C4 and C1-inhibitor (antigenic and functional) for angioedema without wheals
Essential when a mimic is suspected
- Skin biopsy when lesions last >24 h or leave bruising (urticarial vasculitis)
- Inflammatory markers and autoinflammatory work-up for urticaria with fever from infancy
- Tryptase during an acute episode if mastocytosis or anaphylaxis is suspected
- Directed testing for systemic disease when alarm features are present
The single highest-yield laboratory test on this topic is the C4 level in a child with recurrent angioedema without wheals. A C4 is low during and between attacks in hereditary angioedema types I and II; a normal C4 effectively excludes these forms and is the screen that should precede specialist C1-inhibitor functional assay. The dedicated paediatric hereditary angioedema guideline provides the diagnostic algorithm and the on-demand treatment options by age and weight. [9] [10]
WHEALS
Management — Resuscitation
When urticaria or angioedema threatens the airway or the circulation, the management is resuscitation, not a rash work-up. Anaphylaxis presents with acute urticaria or angioedema alongside respiratory compromise, hypotension or persistent gastrointestinal symptoms, and it needs intramuscular adrenaline into the anterolateral thigh without delay, followed by oxygen, fluid and observation. The urticaria is the visible sign of the systemic event; treating the rash without giving adrenaline is the classic error. [13]
Laryngeal angioedema — stridor, drooling, voice change, dysphagia — is an airway emergency regardless of mechanism. For histamine-mediated angioedema, give intramuscular adrenaline early and call for airway support. For bradykinin-mediated angioedema (suspected hereditary angioedema), adrenaline is not the definitive treatment: the child needs C1-inhibitor concentrate or icatibant, and the airway team should be involved before the airway is lost. A child with known hereditary angioedema should carry an on-demand treatment and a written action plan. [9] [13]
The first minutes in an airway or circulation emergency
Recognise the emergency
Stridor, drooling, voice change or hypotension with urticaria or angioedema. Call for help and the airway team.
IM adrenaline
Weight-based intramuscular adrenaline into the anterolateral thigh for anaphylaxis or histamine-mediated airway swelling.
Oxygen, fluid, position
High-flow oxygen; IV fluid for hypotension; lay flat if shocked.
Identify the pathway
If known or suspected hereditary angioedema, give C1-inhibitor concentrate or icatibant — adrenaline is not definitive.
Secure the airway early
Involve anaesthetics or ENT before the airway is lost; do not wait.
Observe and plan
Observation period appropriate to the event; action plan and adrenaline autoinjector before discharge.
For non-anaphylactic acute urticaria with severe distress, a short course of oral corticosteroid (typically three to five days) can dampen the flare, but steroids are adjuncts, not first-line monotherapy, and should not replace the antihistamine or be extended into a prolonged taper that adds harm without benefit. [1] [4]
Management — Definitive & Stepwise
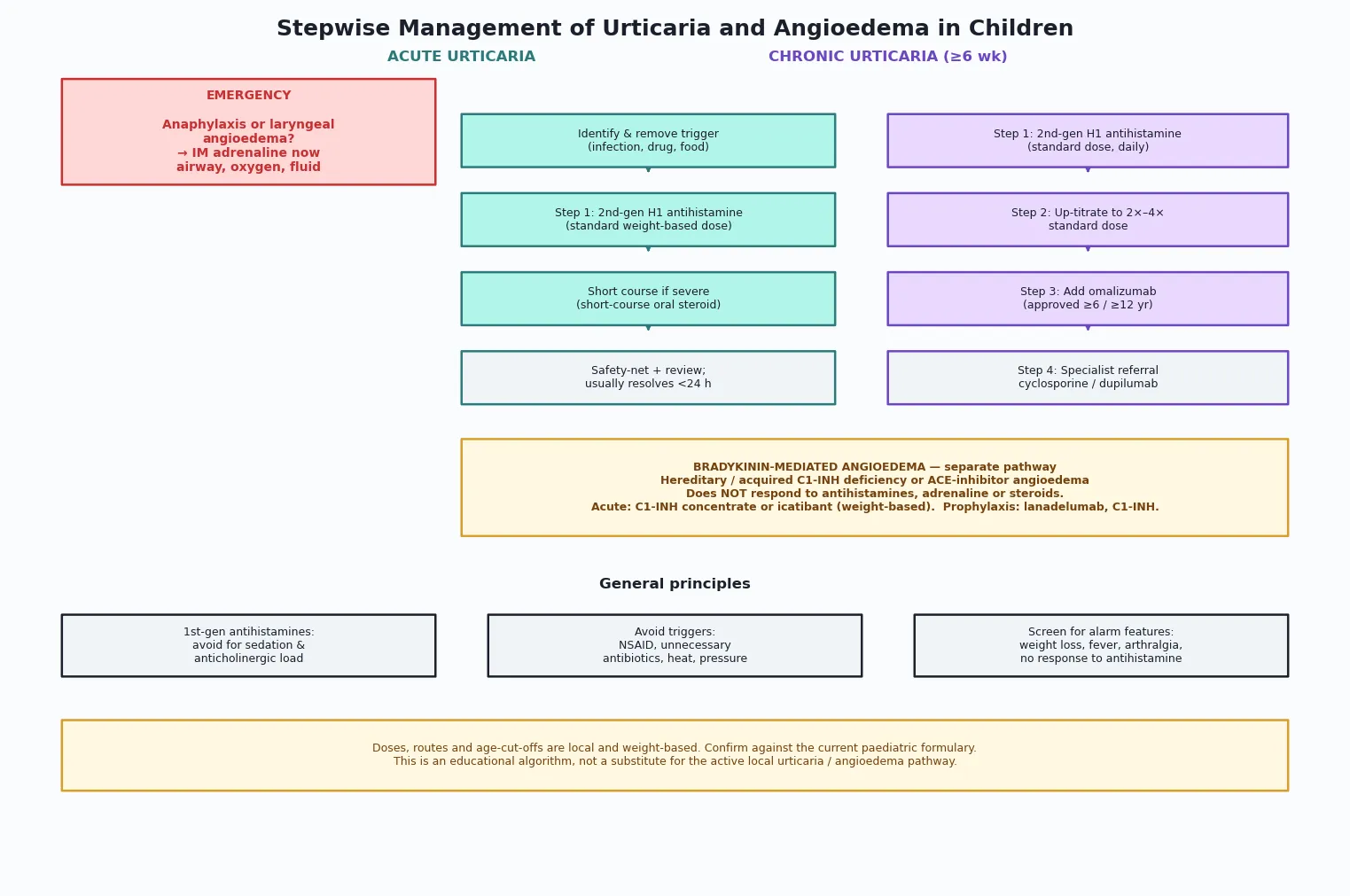
Once the child is safe, the stepwise plan follows the pathway classification. The international urticaria guideline defines a four-step ladder for chronic spontaneous urticaria, and the same first steps apply to acute disease when symptomatic. [1] [3]
Step 1 — standard-dose second-generation antihistamine
A non-sedating second-generation H1 antihistamine at the standard weight-based dose is the foundation. Cetirizine, levocetirizine, loratadine, desloratadine, fexofenadine and bilastine are all acceptable in children, with age-cut-offs varying by agent and jurisdiction. First-generation antihistamines (chlorphenamine, promethazine) are discouraged for routine use because of their sedative and anticholinergic burden and their impact on learning and sleep architecture. [1] [4]
Step 2 — up-titrate to four times the standard dose
If standard-dose therapy does not control symptoms within two weeks, the guideline recommends up-titrating the same second-generation antihistamine to two, then three, then up to four times the standard daily dose, before moving to an add-on biologic. This off-label up-titration is standard specialist practice, and it controls symptoms in a meaningful proportion of children who fail the standard dose — but it should be done with specialist input, documentation, and a plan for review and de-escalation. [1] [3]
Step 3 — omalizumab
For children whose symptoms are uncontrolled on up-titrated antihistamine, omalizumab — a monoclonal antibody against IgE — is the next step. The pivotal trials demonstrated that omalizumab is effective in chronic spontaneous urticaria, and it is licensed in this indication with age-cut-offs that vary by jurisdiction (commonly from age six or twelve). Omalizumab is given by subcutaneous injection at intervals determined by weight and total IgE, and it has transformed the management of refractory disease. [1] [7]
Step 4 — specialist immunomodulation
A small minority remain uncontrolled on omalizumab. Options include cyclosporine (an immunosuppressant that requires monitoring of blood pressure and renal function) and, increasingly, dupilumab, a monoclonal antibody against the interleukin-4 receptor alpha chain. Two phase-three randomised trials (LIBERTY-CSU CUPID) demonstrated that dupilumab reduces itch and wheal activity in chronic spontaneous urticaria, adding a second biologic option to the armamentarium. These steps are specialist-led and require referral to allergy, immunology or dermatology. [3] [8]
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne urticaria guideline provides parent- and clinician-facing guidance in the Victorian system. Omalizumab and dupilumab access is governed by the Pharmaceutical Benefits Scheme (PBS) in Australia and by PHARMAC in Aotearoa New Zealand, with specific authority criteria and age-cut-offs that must be verified against the current schedule. Local allergy and immunology services differ between states and between Australia and New Zealand, so confirm the active local referral pathway. [1] [3]
For inducible urticaria, avoidance of the trigger is the first principle, and a standard-dose second-generation antihistamine is usually effective — with up-titration if needed. In cold-contact urticaria, warn the family specifically about the risk of swimming in cold water, which has caused drowning; an adrenaline autoinjector and a written action plan are appropriate for severe cases. [1]
The bradykinin pathway — a separate treatment track
Hereditary angioedema is managed entirely differently and must not be lost in the antihistamine ladder. Acute attacks are treated with C1-inhibitor concentrate (plasma-derived or recombinant) or icatibant, a bradykinin B2-receptor antagonist, in weight-based paediatric doses. Long-term prophylaxis may use lanadelumab (a kallikrein inhibitor), C1-inhibitor concentrate, or — in selected cases — oral prophylactic agents. Every child with hereditary angioedema needs an on-demand treatment plan, a home supply where feasible, a medical-alert device, and education of the family and school. The dedicated paediatric hereditary angioedema guideline is the operative reference. [9] [10]
Omalizumab in chronic spontaneous urticaria
New England Journal of Medicine
Randomised, double-blind, placebo-controlled phase III trials (ASTERIA I, ASTERIA II, GLACIAL) of omalizumab in chronic spontaneous urticaria refractory to antihistamine
Key finding
Omalizumab significantly reduced itch and wheal activity versus placebo in patients uncontrolled on H1 antihistamine.
Practice change
Omalizumab became the licensed third-line (now Step 3) biologic for chronic spontaneous urticaria after antihistamine up-titration.
Dupilumab in chronic spontaneous urticaria (LIBERTY-CSU CUPID)
Journal of Allergy and Clinical Immunology
Two randomised, double-blind, placebo-controlled phase III trials of dupilumab in chronic spontaneous urticaria uncontrolled on standard-dose antihistamine
Key finding
Dupilumab reduced itch and wheal activity versus placebo, adding a second biologic option for refractory disease.
Practice change
Dupilumab expands the specialist toolkit for chronic spontaneous urticaria uncontrolled on antihistamine and omalizumab.
Specific Subtypes & Scenarios
The recognition logic is constant, but the subtype changes what you look for and how aggressively you act. Each scenario below keeps the danger-check first, then asks what is specific to that child. [1] [9]
Acute urticaria in the young child
- Often viral-triggered; self-limiting within days
- Standard-dose second-generation antihistamine; short course if severe
- Reassure: most do not progress to chronic disease
- Safety-net for airway and anaphylaxis signs
Anaphylaxis presenting as urticaria
- Acute urticaria with hypotension, respiratory or GI compromise
- IM adrenaline immediately; oxygen, fluid, observation
- Identify trigger; allergy referral; adrenaline autoinjector
- Do not treat the rash and miss the systemic event
Chronic spontaneous urticaria
- Daily wheals for ≥6 wk; screen for alarm features
- Stepwise ladder; up-titrate before biologic
- Assess quality of life; most resolve within 1–5 years
- Avoid routine allergy panels; targeted testing only
Cold-contact urticaria
- Wheals on cold exposure; confirm with ice-cube test
- Standard-dose antihistamine; up-titrate if needed
- Warn about cold-water swimming — drowning risk
- Adrenaline autoinjector for severe cases
Hereditary angioedema
- Recurrent angioedema without wheals; positive family history in most
- Low C4; confirm with C1-inhibitor antigenic and functional assay
- Acute: C1-INH concentrate or icatibant; prophylaxis with lanadelumab
- On-demand plan, medical-alert, family screening from childhood
ACE-inhibitor angioedema
- Angioedema without wheals; black African heritage over-represented
- Onset can be months after starting the drug
- Stop the ACE inhibitor; do not re-challenge; avoid ARB crossover cautiously
- Antihistamines and adrenaline are ineffective; supportive airway care
Autoinflammatory urticaria-like rash
- Daily non-pruritic rash with fever from infancy (CAPS spectrum)
- EULAR/ACR diagnostic points to consider; IL-1 blockade is transformative
- Rheumatology and immunology co-management
- Not an allergy — do not chase foods or give antihistamines alone
NSAID-exacerbated urticaria
- Wheals within hours of NSAID in a child with chronic urticaria
- Avoid NSAIDs; paracetamol is usually tolerated
- Cross-reactivity across non-selective NSAIDs is typical
- Consider COX-2 challenge under specialist supervision if NSAID needed
Complications & Pitfalls
Most harm on this topic comes from one of three errors: missing anaphylaxis or laryngeal angioedema behind a "rash", treating bradykinin-mediated angioedema with escalating doses of antihistamine, or over-investigating and over-restricting the diet of a child with straightforward chronic spontaneous urticaria. All three are preventable. [1] [9]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Calling anaphylaxis 'urticaria' | Adrenaline is delayed while the rash is treated | Look for airway and circulation involvement with every acute urticaria; give IM adrenaline if anaphylaxis criteria are met |
| Treating bradykinin angioedema with antihistamines | Escalating, futile treatment; airway is lost while waiting for a response | If angioedema has no wheals, check C4; give C1-INH concentrate or icatibant if hereditary angioedema is known or suspected |
| Over-testing chronic spontaneous urticaria | False-positive allergy panels, unnecessary elimination diets, parental anxiety | Diagnosis is clinical; avoid routine specific IgE panels without a compatible history |
| Missing urticarial vasculitis | Treated as simple urticaria while a systemic vasculitis progresses | Lesions >24 h, painful, bruising, or with systemic features → skin biopsy |
| Using first-generation antihistamines long-term | Sedation, anticholinergic load, impaired learning | Use non-sedating second-generation agents; reserve first-generation for brief sedative effect only |
| Not warning about cold-water swimming | Drowning in cold-contact urticaria | Specific safety advice and an adrenaline autoinjector for cold-contact urticaria |
| Withholding biologic escalation | Child lives with uncontrolled disease when omalizumab would control it | Up-titrate then refer for omalizumab; do not leave a child on sub-therapeutic antihistamine doses |
| Sending a child home without an action plan | The next attack is mismanaged | Written action plan, adrenaline autoinjector if indicated, safety-net content checked by teach-back |
Look actively for harm from treatment once the child is stable: sedation from first-generation antihistamines, weight gain and mood effects from prolonged corticosteroid courses, injection-site and systemic effects of biologics, and the psychological impact of an unnecessary elimination diet. The goal of chronic urticaria management is disease control and quality of life, not an impeccable panel of normal results. [1] [4]
Prognosis & Disposition
Most children with acute urticaria recover within days and never have another episode; a minority progress to chronic disease. The prognosis of chronic spontaneous urticaria in children is favourable overall: symptoms resolve in a majority within one to five years, though a subset persist into adulthood. The quality-of-life burden during active disease is substantial, and it should drive treatment intensity, not be dismissed. [2] [3]
Hereditary angioedema is lifelong, but with on-demand treatment, prophylaxis and family education, attacks are controllable and the risk of fatal airway oedema falls dramatically. Early diagnosis — ideally in childhood — is the single most important prognostic intervention, because it replaces years of misdiagnosis and ineffective treatment with a precise plan. Mortality from undiagnosed hereditary angioedema laryngeal attacks is real; with a correct action plan it is avoidable. [9] [10]
Discharge with safety-net
- Well child with acute urticaria, airway intact, no anaphylaxis
- Antihistamine, written action plan, clear safety-net content
- Named review point if not resolving or if features change
Observe or admit
- Angioedema involving the face but not the airway, for observation
- Anaphylaxis after initial stabilisation, for biphasic-risk observation
- Diagnostic uncertainty or social factors that impair safety-netting
Critical-care and specialist
- Airway-compromising angioedema needing airway protection
- Hereditary angioedema attack needing C1-INH concentrate or icatibant
- Refractory chronic urticaria for biologic escalation — allergy or immunology referral
A defensible discharge gives the family three things: a clear understanding of what the rash is and is not, a written action plan that names when and how to use an adrenaline autoinjector (if indicated) or seek emergency help for airway signs, and a named review or referral point. "Return if worried" is not enough. Check understanding with teach-back, document the plan, and connect the child to primary care and — for chronic or hereditary disease — to the relevant specialist service. [1] [4]
Special Populations
The standard of care is the same; what changes is the threshold to investigate, the intensity of prophylaxis, and the access to specialist escalation. In each group below, urticaria or angioedema is either higher-stakes or harder to manage than in an otherwise well child of the same age. [9] [10]
| Population | Why it matters | Adaptation in care |
|---|---|---|
| Known hereditary angioedema | Laryngeal attacks are life-threatening; attacks begin in childhood | On-demand C1-INH concentrate or icatibant; prophylaxis; medical-alert; family screening |
| Immunocompromised or transplant child | Drug interactions complicate antihistamine and biologic choice; infection triggers common | Multidisciplinary management; check interactions; lower threshold for specialist input |
| Indigenous and remote children | Delayed access to definitive care and to biologics; cold-contact urticaria drowning risk in some settings | Plan retrieval early; ensure action plan and adrenaline access; address access barriers |
| Migrant and refugee families | Language and health-literacy barriers; incomplete family history; may carry ACE-inhibitor from origin country | Professional interpreter; written plan in family language; elicit medication and family history carefully |
| Adolescents | Quality-of-life and adherence burden; transition to adult services | Engage the young person; address adherence and injection burden; plan transition |
| Socioconomic disadvantage | Cost of biologics and adrenaline autoinjectors; school action-plan access | Navigate subsidy schemes; ensure school access to adrenaline; advocacy |
Use a professional interpreter for any family with limited English proficiency during a clinical or safety-net conversation; communication access is a safety measure, not a courtesy. For Indigenous children and families, work with the local Aboriginal and Torres Strait Islander or Māori health service and recognise that delayed access to specialist care and biologics reflects structural factors the clinician can act on. [1]
Evidence, Guidelines & Regional Differences
What the evidence supports
The international urticaria guideline is the single most important reference on this topic. The 2022 EAACI/GA²LEN/EuroGuiDerm/APAAACI update reaffirmed the four-step treatment ladder — standard-dose antihistamine, up-titration to fourfold dose, omalizumab, then immunomodulation — and the definition of chronic disease as six weeks or more. The evidence for antihistamine up-titration and for omalizumab is strong; the evidence for older immunosuppressants such as cyclosporine is moderate; and dupilumab has added a second biologic with phase III trial support. [1] [3] [8]
The paediatric hereditary angioedema guideline translates the adult evidence into age- and weight-specific on-demand and prophylactic regimens, and emphasises that hereditary angioedema is a childhood-onset disease whose prognosis depends on early diagnosis and a precise action plan. The global systematic review quantified the prevalence of chronic urticaria in children as well under one per cent, putting the burden in context and cautioning against over-treatment of acute disease. [2] [9]
Jurisdictional implementation
Global and low-resource settings: access to biologics, C1-inhibitor concentrate and icatibant varies widely, so the management of refractory urticaria and hereditary angioedema depends on what is locally available. In settings without biologic access, up-titrated antihistamine and corticosteroid remain the backbone, and hereditary angioedema may rely on attenuated androgens (with attention to paediatric safety) or fresh-frozen plasma for acute attacks. Do not transplant a high-resource pathway uncritically where the rescue options differ. [1] [9]
Controversies and open questions
Three debates recur. First, the optimal speed of antihistamine up-titration in children — whether to go straight to fourfold or titrate stepwise — is still clinician-dependent; the guideline supports either, with documentation and review. Second, the role of routine thyroid screening in chronic spontaneous urticaria is not fully settled; most authors check thyroid function and antibodies in refractory disease, but not routinely in uncomplicated disease. Third, the place of dupilumab relative to cyclosporine in the fourth step is evolving as real-world paediatric experience accumulates. In each case, the named guideline is the operative standard and the local pathway is the deliverable. [1] [3] [8]
Exam Pearls
Define
- Urticaria = transient (<24 h) itchy wheals from mast-cell histamine
- Angioedema = deeper swelling; with wheals = histamine; without = consider bradykinin
- Six weeks separates acute from chronic
Danger
- Anaphylaxis = urticaria plus airway, circulation or GI compromise → IM adrenaline
- Laryngeal angioedema = stridor, drooling → airway emergency
- Bradykinin angioedema does not respond to antihistamines, adrenaline or steroids
Classify
- Acute spontaneous, chronic spontaneous, chronic inducible
- Angioedema: histamine-mediated (with wheals) vs bradykinin-mediated (without)
- Inducible types: dermographism, cold, pressure, solar, cholinergic, aquagenic
Investigate
- Diagnosis is clinical — avoid routine allergy panels in chronic spontaneous urticaria
- C4 is the screen for hereditary angioedema; confirm with C1-INH functional assay
- Lesions >24 h, bruising, painful → skin biopsy for urticarial vasculitis
Manage
- Step 1: standard-dose 2nd-gen antihistamine
- Step 2: up-titrate to 4× standard dose
- Step 3: omalizumab
- Step 4: cyclosporine or dupilumab under specialist
- Hereditary angioedema: C1-INH concentrate or icatibant; prophylaxis with lanadelumab
Boundaries
- Doses are local and weight-based — do not quote a universal dose
- Do not use first-generation antihistamines long-term
- Warn about cold-water drowning in cold-contact urticaria
- A daily rash with fever from infancy is not allergy — consider autoinflammation
“Confirm urticaria (wheal <24 h, itchy, normal skin) → check for airway and anaphylaxis danger → split the pathway (histamine vs bradykinin) → standard-dose antihistamine, then up-titrate, then omalizumab → bradykinin angioedema gets C1-INH concentrate or icatibant, not antihistamines → written action plan and safety-net on discharge.”
Viva: a four-year-old with acute itchy wheals after a viral illness
State that the individual wheals resolve within twenty-four hours leaving normal skin, which confirms ordinary acute urticaria — most likely viral-triggered, the commonest identifiable cause in this age group. Assess for airway or circulation involvement to exclude anaphylaxis, examine for angioedema, and identify any drug trigger (especially NSAIDs or antibiotics). Treat with a standard-dose second-generation antihistamine, give a short course of oral corticosteroid only if distress is severe, and discharge with a clear safety-net for airway and anaphylaxis signs. Reassure the family that most acute urticaria resolves within days and that routine allergy testing is not indicated. [1] [5]
Viva: recurrent facial swelling without a rash
This is angioedema without wheals, which raises the bradykinin pathway. Ask about family history of swelling, unexplained abdominal pain or airway events, and about ACE-inhibitor use. Check a C4 level — if low, proceed to C1-inhibitor antigenic and functional assays to confirm hereditary angioedema. State that this angioedema does not respond to antihistamines, adrenaline or corticosteroids; acute attacks need C1-inhibitor concentrate or icatibant, and long-term prophylaxis with lanadelumab or C1-inhibitor may be required. The child needs an on-demand treatment plan, a medical-alert device, and family screening. [9] [10]
SAQ: daily wheals for eight weeks in a school-age child
This meets the definition of chronic spontaneous urticaria — daily wheals for six weeks or more. First, screen for alarm features: individual lesions lasting over twenty-four hours, bruising, pain, fever, weight loss, arthralgia. Their absence supports a clinical diagnosis without extensive testing, and routine allergy panels are not indicated. Begin with a standard-dose second-generation antihistamine; if uncontrolled within two weeks, up-titrate to four times the standard dose; if still uncontrolled, refer for omalizumab. Assess quality of life and set expectations: most childhood chronic spontaneous urticaria resolves within one to five years. [1] [3]
References
- [1]Zuberbier T The international EAACI/GA²LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria Allergy, 2022.PMID 34536239
- [2]Fricke J Prevalence of chronic urticaria in children and adults across the globe: Systematic review with meta-analysis Allergy, 2020.PMID 31494963
- [3]Ensina LF Managing Chronic Urticaria in Children: An Update Current Allergy and Asthma Reports, 2025.PMID 40192928
- [4]Caffarelli C Management of chronic urticaria in children: a clinical guideline Italian Journal of Pediatrics, 2019.PMID 31416456
- [5]Marques-Mejías MA Acute urticaria in the pediatric emergency department: Management and possible triggers Annals of Allergy, Asthma & Immunology, 2020.PMID 31981615
- [6]Santa C Acute urticaria in children: from pediatric Emergency Department to allergology consultation at a Central Hospital European Annals of Allergy and Clinical Immunology, 2022.PMID 33944542
- [7]Maurer M Omalizumab for the treatment of chronic idiopathic or spontaneous urticaria New England Journal of Medicine, 2013.PMID 23432142
- [8]Maurer M Dupilumab in patients with chronic spontaneous urticaria (LIBERTY-CSU CUPID): Two randomized, double-blind, placebo-controlled, phase 3 trials Journal of Allergy and Clinical Immunology, 2024.PMID 38431226
- [9]Farkas H International Guideline on the Diagnosis and Management of Pediatric Patients With Hereditary Angioedema Allergy, 2026.PMID 41618059
- [10]Maurer M The international WAO/EAACI guideline for the management of hereditary angioedema-The 2021 revision and update Allergy, 2022.PMID 35006617
- [11]Hashkes PJ Autoinflammatory syndromes Pediatric Clinics of North America, 2012.PMID 22560579
- [12]Romano M The 2021 EULAR/American College of Rheumatology points to consider for diagnosis, management and monitoring of the interleukin-1 mediated autoinflammatory diseases Annals of the Rheumatic Diseases, 2022.PMID 35623638
- [13]Abrams EM Anaphylaxis Allergy, Asthma & Clinical Immunology, 2024.PMID 39654057
- [14]Zuberbier T The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria Allergy, 2018.PMID 29336054