Paeds · cardiology
Acute rheumatic fever and rheumatic heart disease
Also known as acute rheumatic fever · ARF · rheumatic heart disease · RHD · Sydenham chorea · rheumatic carditis · post-streptococcal carditis
A fellowship approach to acute rheumatic fever and rheumatic heart disease: the child with a sore throat whose immune response scars a mitral valve for life, the Jones criteria that demand echo, the benzathine penicillin that prevents recurrence, and the disease-of-inequity reality that makes this a scourge of Indigenous Australia and the developing world rather than a closed chapter of Western medicine.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A nine-year-old Aboriginal boy in remote Northern Territory presents with a swollen, painful knee that migrated to the elbow over two days, a fever, and a new heart murmur; or a twelve-year-old girl of Pacific Islander background is admitted with dyspnoea and a harsh apical pansystolic murmur four weeks after a sore throat; or a teenager develops involuntary grimacing and writhing movements of the hands and face weeks after a febrile illness. The fellowship task in each is the same: apply the Jones criteria, confirm the streptococcal link with serology, request echocardiography, and commit to secondary prophylaxis. [3] [1]
The five moves — Suspect, Score, Scan, Strike, Sustain
Overview & Definition
Acute rheumatic fever is a delayed, nonsuppurative inflammatory disease that follows untreated group A streptococcal pharyngitis by two to three weeks, affecting the heart, joints, skin, and central nervous system. Rheumatic heart disease is the chronic, progressive, and largely irreversible damage to the cardiac valves — predominantly the mitral — that results from one or more episodes of acute rheumatic fever. The two are one disease viewed at different points in time. [5] [1]
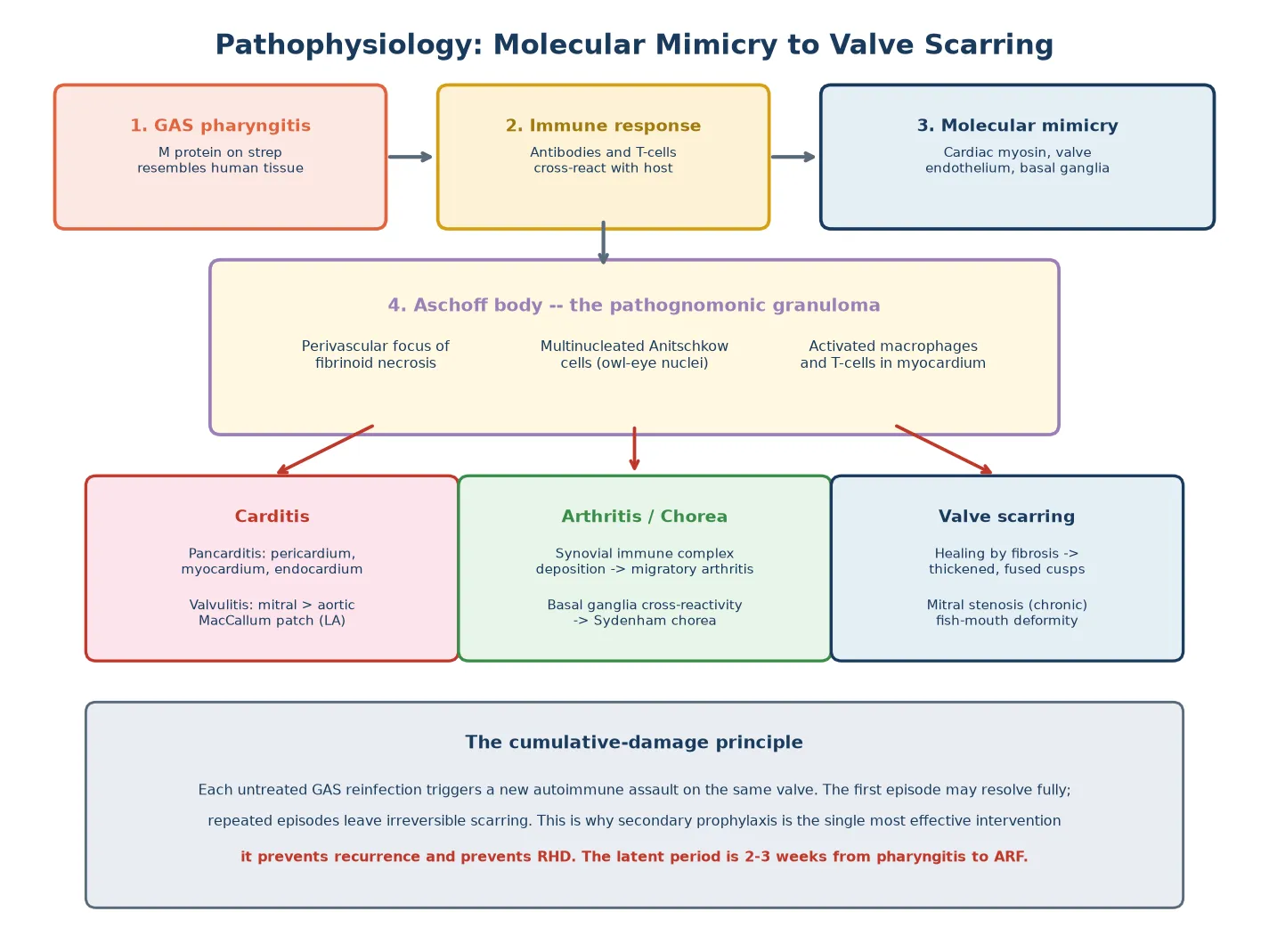
The fellowship framing rests on a single immunological truth. Group A streptococcal M proteins share antigenic similarity with human cardiac myosin, valvular endothelium, and the basal ganglia, so the antibodies and T cells raised against the streptococcus cross-react with host tissue. This molecular mimicry is the mechanism that turns a sore throat into a scarred mitral valve, and it is why the disease targets the heart rather than the throat. [5] [7]
The clinical importance comes from what happens if the disease is missed or undertreated. A single episode of acute rheumatic fever may resolve fully, but each recurrent episode driven by a new streptococcal infection cumulatively damages the valve, and established rheumatic heart disease carries a heavy burden of heart failure, atrial fibrillation, stroke, infective endocarditis, and premature death. The stakes are highest in pregnancy, where undiagnosed rheumatic heart disease remains a leading cause of maternal mortality in endemic regions. [8] [4]
Classification
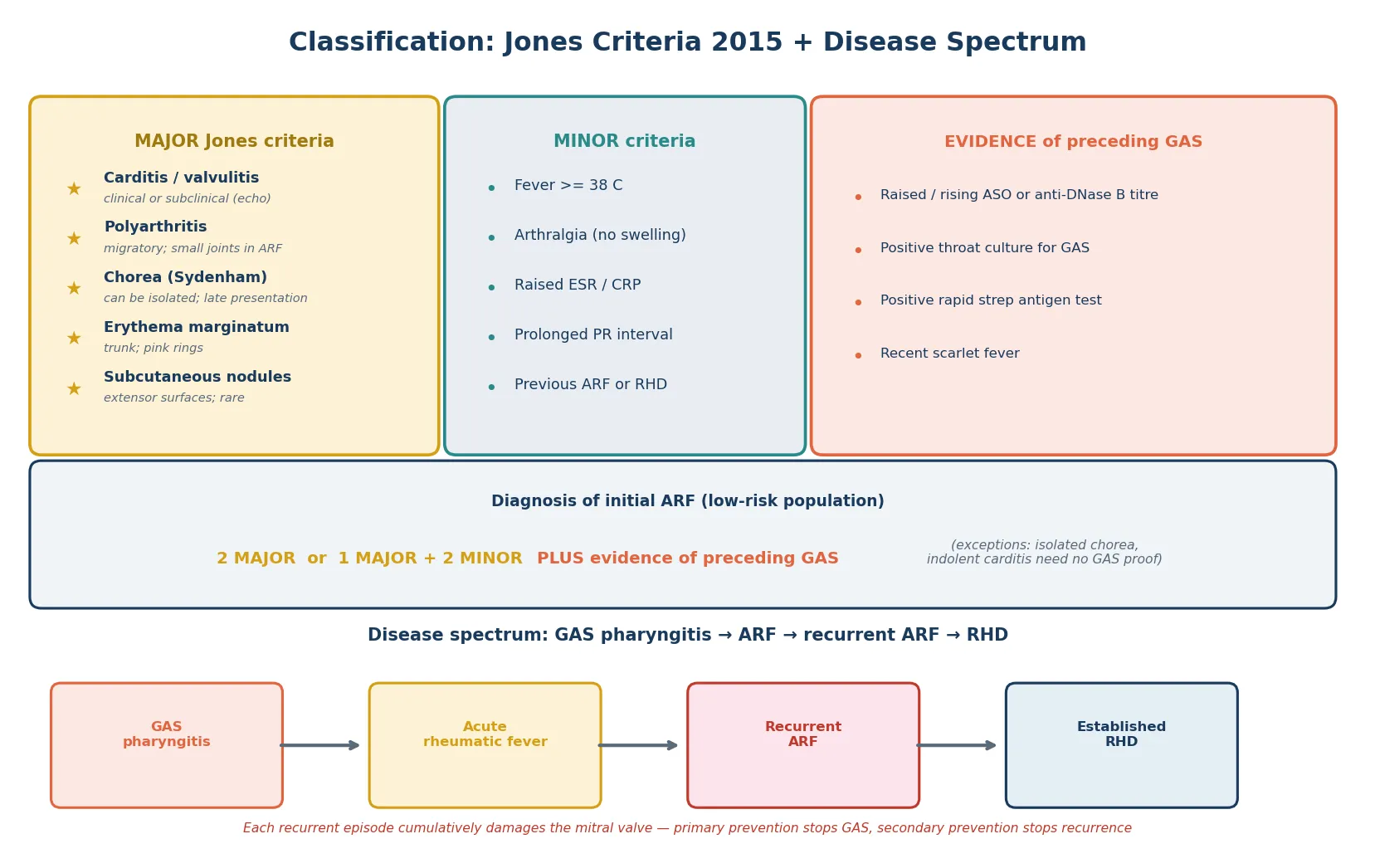
Classification of acute rheumatic fever rests on the revised Jones criteria, which separate the clinical manifestations into major and minor categories and require evidence of a preceding group A streptococcal infection to confirm the diagnosis. The 2015 American Heart Association revision introduced a critical change — subclinical carditis detected on echocardiography alone, without an audible murmur, now counts as a major criterion — because Doppler echocardiography is far more sensitive than the stethoscope for detecting valvulitis. [1]
The five major criteria are carditis or clinical or subclinical valvulitis, polyarthritis, chorea, erythema marginatum, and subcutaneous nodules. The four minor criteria are fever, arthralgia, raised acute-phase reactants (erythrocyte sedimentation rate or C-reactive protein), and a prolonged PR interval on the electrocardiogram, with a previous history of acute rheumatic fever or rheumatic heart disease also counting. For a first episode in a low-risk population, the diagnosis requires two major criteria or one major and two minor criteria, plus evidence of preceding group A streptococcal infection. [1]
The risk-stratified thresholds matter. In high-risk populations — including Indigenous Australians, Pacific Islanders, and those living in endemic regions — the criteria are more permissive: monoarthritis or polyarthralgia may substitute for polyarthritis, a lower temperature threshold applies, and a smaller PR prolongation counts. This acknowledges that the disease behaves differently where it is common, and it prevents the under-diagnosis that has historically disadvantaged high-risk children. The 2020 Australian guideline adopts these high-risk criteria across all of Australia and Aotearoa New Zealand, reflecting the endemic reality. [3] [1]
Epidemiology & Risk Factors
Acute rheumatic fever is overwhelmingly a disease of school-aged children, peaking between the ages of five and fifteen years, and it is vanishingly rare after the age of thirty. It follows untreated group A streptococcal pharyngitis in about three per cent of children who carry a rheumatogenic strain, and the global burden remains staggering — an estimated forty million people live with rheumatic heart disease worldwide, and the disease causes over three hundred thousand deaths each year. [7] [4]
The risk factors that matter for the fellowship answer are those of inequity and crowding. Overcrowded housing, poor sanitation, limited access to primary healthcare, and the social determinants of health are the engine of the disease, not the biology of the streptococcus. In Australia, the incidence of acute rheumatic fever among Aboriginal and Torres Strait Islander children in the Northern Territory is among the highest in the world — up to three hundred and fifty cases per one hundred thousand per year — while it is essentially zero in non-Indigenous children in the same cities. This is the sharpest epidemiological contrast in paediatrics, and it is the reason why rheumatic heart disease is framed as a disease of social determinants. [6] [3]
The disease persists in the Pacific Islands, sub-Saharan Africa, South Asia, and parts of Latin America, and it is re-emerging in pockets of socioeconomic disadvantage in wealthy nations. Migrant, refugee, and asylum-seeking children arriving from endemic regions may carry established rheumatic heart disease with no documented history, and the clinician in a tertiary centre must maintain a high index of suspicion. A family history of rheumatic heart disease and recurrent streptococcal infections further raise the individual risk. [7] [4]
Pathophysiology
The pathophysiology turns on molecular mimicry, in which the immune response raised against the group A streptococcal M protein cross-reacts with host tissues. Cardiac myosin shares antigenic epitopes with the M protein, and the antibodies and T cells that should target the streptococcus instead attack the heart. The valve endothelium, particularly the mitral valve, is especially vulnerable because the turbulent flow across the valve exposes its endothelium to the circulating immune response. [5] [7]
The histological hallmark is the Aschoff body, a perivascular focus of fibrinoid necrosis surrounded by multinucleated giant cells called Anitschkow cells, whose characteristic owl-eye nuclei are the pathognomonic finding. The Aschoff body is found in the myocardium, but the clinically important damage is to the valve leaflets, where the inflammatory process causes oedema, followed by healing with fibrosis and neovascularisation. The mitral valve is affected in the vast majority, followed by the aortic valve; the tricuspid and pulmonary valves are rarely involved. [5]
The acute valvulitis produces mitral regurgitation, because the inflamed, oedematous leaflets cannot coapt, and the elongated or ruptured chordae further impair closure. This acute regurgitation is what the stethoscope hears and what the echocardiogram measures. Over months and years, repeated episodes of inflammation and healing thicken, fuse, and retract the leaflets, transforming the acute regurgitation into the chronic stenosis of established rheumatic heart disease — the classic fish-mouth mitral valve. The MacCallum patch, an area of thickened endocardium in the left atrium where the regurgitant jet impinges, is a further chronic finding. [5] [1]
The extracardiac manifestations share the same autoimmune mechanism. The migratory polyarthritis results from immune complex deposition in the synovium, and the large joints are preferentially affected. Sydenham chorea, the neurological manifestation, results from cross-reactivity with the basal ganglia, specifically the caudate and subthalamic nuclei, and it can appear months after the streptococcal infection when the serological evidence has already faded. The skin manifestations — erythema marginatum and subcutaneous nodules — are the least common and the most transient. [5]
Clinical Presentation
The presentation begins with the streptococcal sore throat, which may be mild, unrecognised, or already resolved by the time the child presents with acute rheumatic fever. After a latent period of two to three weeks, the child develops fever and one or more of the major manifestations. Polyarthritis is the commonest presentation, seen in about seventy per cent of cases, and it is characteristically migratory, moving from one large joint to another over hours to days, with each joint inflamed for a brief period before the next is affected. [5] [1]
Carditis is the second commonest presentation and the most important, because it is the only manifestation that leaves permanent damage. It presents with a new heart murmur — classically the high-pitched apical pansystolic murmur of mitral regurgitation — accompanied by tachycardia out of proportion to the fever, a gallop rhythm, and signs of heart failure in severe cases. The pericardium may be involved, producing a friction rub or a pericardial effusion. The myocardium is histologically inflamed, but clinical myocardial dysfunction is rare without valvulitis, because the valve is the primary target. [5] [1]
Sydenham chorea is the most distinctive but least common presentation, occurring in about ten to fifteen per cent of cases and appearing weeks to months after the streptococcal infection. It presents with involuntary, purposeless, jerky movements of the face and limbs, emotional lability, and muscle weakness, and it may be unilateral. The chorea resolves over weeks to months, but because the streptococcal serology has often normalised by the time chorea appears, the diagnosis is made clinically and prophylaxis is started empirically. Erythema marginatum, the pink, serpiginous, expanding rash on the trunk, and subcutaneous nodules over the extensor surfaces are the rarest manifestations and are almost always seen alongside carditis. [5]
Which reassuring-sounding stories must never close the search for ARF? A well-looking child with a migratory arthritis and a faint murmur is not benign — the arthritis may settle overnight and the murmur may be dismissed, but the echo will show subclinical carditis. A child who has recovered from a sore throat and now has chorea is not a behavioural problem — the chorea is post-streptococcal and demands prophylaxis. And a pregnant young woman with exertional dyspnoea is not simply deconditioned — she may carry undiagnosed rheumatic heart disease that will declare itself in the haemodynamic load of pregnancy. [8] [3]
Differential Diagnosis
The differential diagnosis of a school-aged child with fever, arthritis, and a murmur is broad, and the fellowship skill is to distinguish acute rheumatic fever from its mimics using the Jones criteria and the streptococcal link. Reactive arthritis following a viral or bacterial infection produces a similar pattern but lacks the streptococcal serology and the carditis. Septic arthritis is monoarticular with a hot, swollen joint and a positive culture, and it is a single-joint emergency rather than a migratory phenomenon. [5]
Juvenile idiopathic arthritis enters the differential, but it produces a persistent, additive arthritis rather than a migratory one, and it lacks the streptococcal link and the characteristic rash of erythema marginatum. Systemic lupus erythematosus produces polyarthritis, a rash, and cardiac involvement, but the rash is malar rather than serpiginous, and the antinuclear antibody is positive. The streptococcal serology in rheumatic fever is the discriminator that resolves most of these. [5]
For the child presenting primarily with carditis, the differential includes infective endocarditis, Kawasaki disease, viral myocarditis, and congenital heart disease newly presenting. Infective endocarditis produces a murmur and fever but with positive blood cultures and vegetations on echo; Kawasaki produces coronary artery changes and a prolonged fever with a polymorphous rash; viral myocarditis produces a globally impaired ventricle without the valvular pathology. The echocardiogram, the streptococcal serology, and the clinical timecourse resolve the differential in nearly every case. [1]
Clinical & Bedside Assessment
The recognition move is to suspect acute rheumatic fever in any school-aged child with a sore throat followed by arthritis, a murmur, or chorea, and to perform a full cardiovascular and musculoskeletal examination. The history must establish the preceding sore throat, the time interval, the pattern of the arthritis, and the family and demographic context — Indigenous or Pacific Islander background, household crowding, and a family history of rheumatic heart disease all raise the pre-test probability and shift the clinician toward the high-risk criteria. [3] [1]
The bedside examination must assess each major criterion. Auscultate the heart for the high-pitched apical pansystolic murmur of mitral regurgitation radiating to the axilla, the early diastolic murmur of aortic regurgitation at the left sternal edge, a pericardial friction rub, and a gallop rhythm suggesting heart failure. Examine every joint for swelling, warmth, and limitation, and document the migratory pattern. Inspect the trunk for the serpiginous pink rings of erythema marginatum, palpate the extensor surfaces for subcutaneous nodules, and observe the child for the involuntary movements of chorea, which may be subtle and may be suppressed when the child is aware of being watched. [5]
Which examination findings must never be dismissed? Tachycardia out of proportion to the fever suggests carditis, because the inflamed myocardium drives the rate even when the temperature settles. A soft murmur in a child with polyarthritis is not incidental — it is the valvulitis that makes the diagnosis. And a child who cannot sit still, who grimaces and writhes, is not anxious — the chorea is the diagnosis, and it demands serology and prophylaxis even when the streptococcal titres have normalised. [5] [1]
Investigations
Echocardiography is the single most important investigation in suspected acute rheumatic fever, because the 2015 revision allows subclinical carditis — pathological valve regurgitation detected on Doppler echo without an audible murmur — to count as a major criterion. The echo assesses the mitral and aortic valves for the morphological changes of acute rheumatic carditis, including leaflet thickening, restricted motion, chordal elongation, and the pathological regurgitation that defines valvulitis. The World Heart Federation criteria provide a standardised framework for the echocardiographic diagnosis of both definite and borderline rheumatic heart disease. [2] [1]
The evidence of preceding group A streptococcal infection is required for the diagnosis of ARF (with the exceptions of chorea and indolent carditis). The antistreptolysin O titre is the most commonly used serological test, and a raised or rising titre confirms recent infection. Combining the ASO with an anti-DNase B titre increases the sensitivity, because some children mount a stronger response to one antigen than the other. A positive throat swab or rapid antigen test also confirms the streptococcal link, but a negative swab does not exclude the diagnosis, because the acute infection may have cleared by the time ARF presents. [1] [5]
The acute-phase reactants — erythrocyte sedimentation rate and C-reactive protein — are raised in most cases of ARF and count as minor criteria. The electrocardiogram may show a prolonged PR interval, which is a minor criterion, and it is essential if pericarditis is suspected. The chest radiograph may show cardiomegaly and pulmonary congestion in severe carditis. In established rheumatic heart disease, the echocardiogram quantifies the valve lesion, estimates the pulmonary artery pressure, and assesses the ventricular size and function, guiding the decision between medical management and valve intervention. [1] [5]
Management — Resuscitation
Resuscitation is rarely the primary need in acute rheumatic fever, because most children are haemodynamically stable, but severe carditis can present with acute heart failure that demands urgent treatment. The child with pulmonary oedema and a gallop rhythm needs oxygen, intravenous furosemide, and an inotrope if the ventricular function is impaired. Arrhythmia — particularly atrial fibrillation in the older child with established disease — requires rate control and anticoagulation. [3] [5]
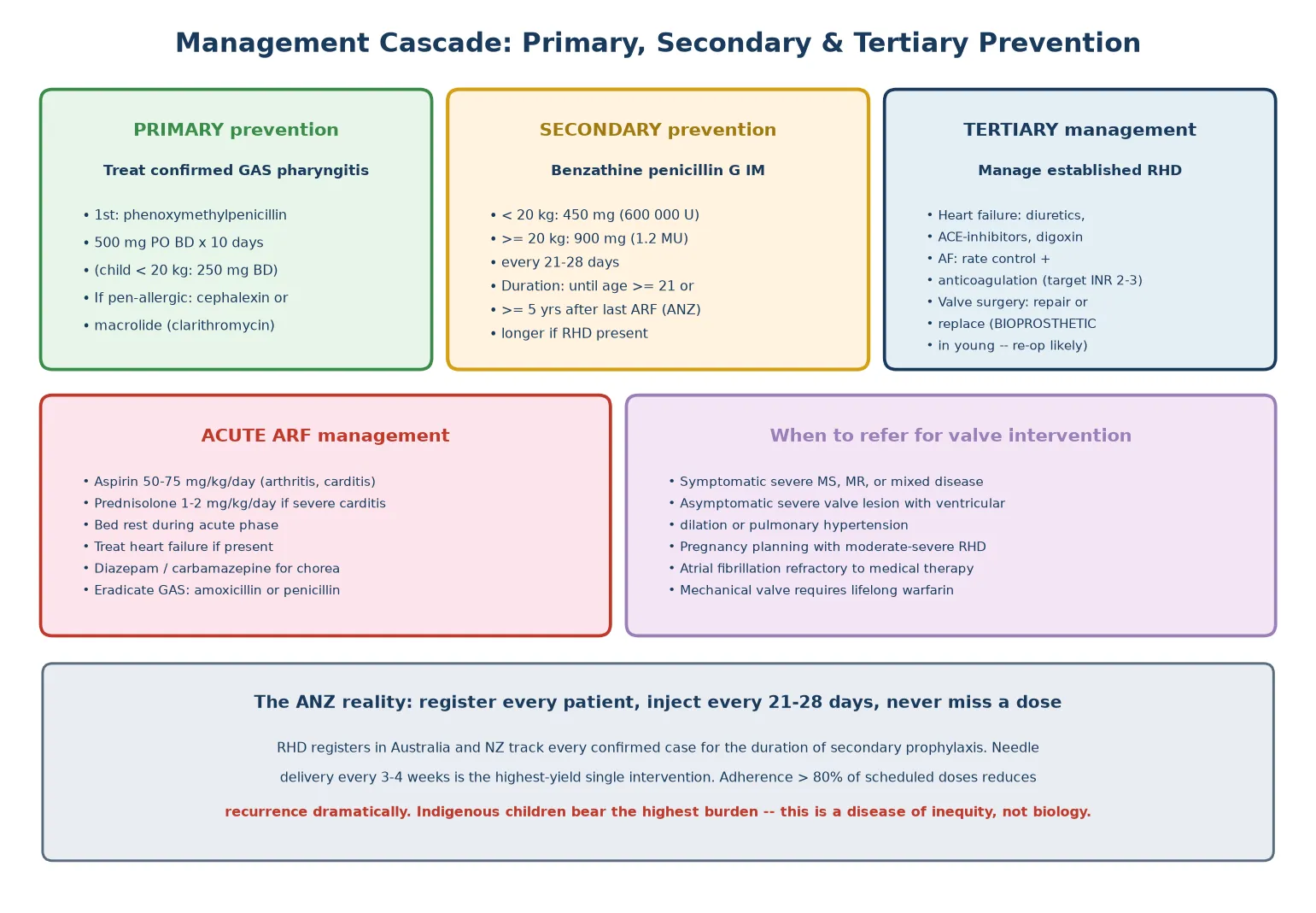
The acute episode is managed with bed rest during the active inflammatory phase, especially when carditis is present, and anti-inflammatory medication. Aspirin at fifty to seventy-five milligrams per kilogram per day is the standard treatment for arthritis and mild carditis, and it produces a dramatic response within twenty-four to forty-eight hours — a response so characteristic that it is itself a diagnostic clue. Severe carditis with heart failure is treated with corticosteroids, typically oral prednisolone at one to two milligrams per kilogram per day, although the evidence for a benefit over aspirin alone remains limited. [5] [3]
Chorea is treated symptomatically, because it is self-limiting over weeks to months. Diazepam or carbamazepine controls the movements, and a supportive, low-stimulation environment reduces the exacerbations. The echocardiogram is repeated at intervals to track the resolution of the valvulitis, and the child is counselled and prepared for the long-term secondary prophylaxis that is the central intervention. [5]
Management — Definitive & Stepwise
The definitive management of acute rheumatic fever is secondary prophylaxis with intramuscular benzathine penicillin G, given every twenty-one to twenty-eight days to prevent recurrent streptococcal infection and thereby prevent cumulative valve damage. This single intervention is the most effective action in the entire disease pathway, because it halts the progression from one episode of ARF to established rheumatic heart disease. The dose is four hundred and fifty milligrams (six hundred thousand units) for children under twenty kilograms and nine hundred milligrams (one point two million units) for those twenty kilograms and above. [3] [1]
The duration of secondary prophylaxis is a fellowship-critical detail. The 2020 Australian guideline recommends prophylaxis until at least the age of twenty-one for those with no established rheumatic heart disease, and for a minimum of five years after the last episode of ARF, whichever is longer. For those with established mild rheumatic heart disease, prophylaxis continues until at least age thirty-five or for ten years after the last episode, and for moderate to severe disease, prophylaxis may be lifelong. These durations reflect the cumulative-damage principle: the longer the child is protected, the lower the risk of recurrence and progression. [3]
Penicillin-allergic children are managed with oral penicillin V twice daily, or, if the allergy is severe, an oral macrolide such as erythromycin or clarithromycin. Oral prophylaxis is less effective than intramuscular because adherence is poorer, and the intramuscular route is preferred wherever feasible. Every child with confirmed ARF or RHD should be entered on the regional rheumatic heart disease register, because register-based recall and reminder systems are the backbone of effective prophylaxis programmes and they dramatically improve adherence. [3] [6]
For established rheumatic heart disease, the management is that of chronic valvular disease. Heart failure is treated with diuretics, angiotensin-converting enzyme inhibitors, and digoxin. Atrial fibrillation requires rate control and anticoagulation, with a target INR of two to three for mitral stenosis. Valve intervention — repair or replacement — is indicated for symptomatic severe disease, for asymptomatic severe valve lesions with ventricular dilation or pulmonary hypertension, and before pregnancy in women with moderate to severe RHD. Valve repair is preferred where feasible, and bioprosthetic valves are often chosen in young patients despite their limited durability, because mechanical valves demand lifelong warfarin with all its management challenges. [8] [3]
Specific Subtypes & Scenarios
Sydenham chorea presents a distinct subtype with a unique diagnostic challenge. The chorea appears weeks to months after the streptococcal infection, so the antistreptolysin O titre has often normalised, and the diagnosis is clinical. The chorea may be the sole manifestation, with no arthritis and no audible murmur, yet the child still has ARF and still requires secondary prophylaxis to protect the valve. The movements resolve over weeks to months, and the psychological distress of the involuntary movements is considerable — a supportive, validating approach is essential. [5] [1]
Subclinical carditis is the subtype created by the 2015 Jones revision, in which echocardiography detects pathological valvular regurgitation in a child with no audible murmur. This subtype matters because it is common and it was previously missed, leaving children unregistered and unprotected. A child presenting with polyarthritis and a normal stethoscope exam but a pathological echo has ARF — the subclinical carditis is the second major criterion — and the child is committed to the same secondary prophylaxis as the child with an audible murmur. [1] [2]
Pregnancy is the subtype that kills. Undiagnosed moderate to severe rheumatic heart disease declares itself under the haemodynamic load of pregnancy, when the increased blood volume and heart rate tip the stenotic mitral valve into pulmonary oedema. Rheumatic heart disease remains a leading cause of maternal mortality in endemic regions, and the fellowship skill is to assess and intervene before conception. A young woman with established RHD needs pre-pregnancy counselling, echocardiographic risk stratification, and valve intervention if the lesion is severe — because deferring to the first antenatal visit may be too late. [8]
The Indigenous Australian child is the subtype that defines the epidemiology. The incidence of ARF among Aboriginal and Torres Strait Islander children in remote communities is among the highest in the world, driven by household crowding, limited access to primary care, and the social determinants of health. The 2020 Australian guideline applies the high-risk Jones criteria across all of Australia and New Zealand, acknowledging that the standard thresholds would under-diagnose the children who bear the greatest burden. Environmental health interventions — housing, sanitation, access to primary care — are as much a part of management as the penicillin. [6] [3]
Complications & Pitfalls
The complications of untreated or recurrent acute rheumatic fever are those of established rheumatic heart disease: chronic mitral regurgitation progressing to mitral stenosis, atrial fibrillation from left atrial dilation, systemic embolism and stroke, infective endocarditis superimposed on the damaged valve, and progressive heart failure. Pregnancy compounds all of these, and maternal mortality remains significant in endemic regions. The complications are preventable with secondary prophylaxis, which is the central message of the fellowship answer. [8] [5]
The pitfall of under-diagnosis is the commonest error. A child with a migratory arthritis is sent home with analgesia, the faint murmur is dismissed, the echocardiogram is not requested, and the child is lost to follow-up until the next recurrence produces established disease. The pitfall of over-diagnosis is less common but real — diagnosing ARF in a child with reactive arthritis and a coincidental innocent murmur commits the child to years of unnecessary injections and anxiety. The streptococcal serology and the strict application of the Jones criteria prevent both errors. [1] [3]
The pitfall of suboptimal prophylaxis is the failure that perpetuates the disease. Intervals longer than twenty-eight days between benzathine penicillin injections are the commonest reason for recurrence, and poor adherence is the commonest reason for progression to RHD. The register, the recall and reminder system, and the community health partnership are the safeguards against this pitfall. The pitfall of the echocardiogram is the false reassurance of a single normal study — the echo is repeated if the clinical suspicion persists, because subclinical carditis can declare on a subsequent study. [9] [2]
The pitfall of valve surgery timing is operating too late or too early. Operating on an acutely inflamed valve during the active episode produces poor results, so the surgery is deferred until the inflammation has settled — but not deferred so long that the ventricle decompensates irreversibly. The choice between repair and replacement, and between mechanical and bioprosthetic valves, balances the durability of the valve against the burden of lifelong anticoagulation, and these decisions are made in a multidisciplinary congenital and valvular heart team. [8] [3]
Prognosis & Disposition
The prognosis of a single episode of acute rheumatic fever, treated early and protected with secondary prophylaxis, is excellent, with most children recovering fully and a significant proportion showing complete resolution of the carditis on follow-up echocardiography. The prognosis worsens with each recurrent episode, because each recurrence adds to the cumulative valve damage, and the child who experiences multiple episodes is the one who progresses to established RHD. This is why adherence to secondary prophylaxis is the single biggest predictor of outcome. [5] [3]
Established rheumatic heart disease carries a variable prognosis depending on the severity of the valve lesion and the access to surgical care. Mild disease, with mild mitral regurgitation and no stenosis, may remain stable for decades with prophylaxis and surveillance. Severe disease, with critical mitral stenosis or severe mixed disease, requires valve intervention and carries a significant long-term burden of reoperation, anticoagulation, and heart failure. The transition from paediatric to adult cardiology is a structured handover, because the young adult with RHD needs lifelong surveillance and the transition point is where loss to follow-up is highest. [3] [8]
The disposition is shared between the general paediatrician, who owns the recognition and the initial prophylaxis, the paediatric cardiologist, who owns the echocardiography and the valve assessment, and the primary care and community health team, who own the ongoing prophylaxis and the register. The family is counselled on the diagnosis, the duration of prophylaxis, the importance of adherence, and the signs that warrant urgent review — and the counselling is conducted in the family's language with an interpreter when needed. [3] [6]
Special Populations
Indigenous children in Australia and Aotearoa New Zealand bear the highest burden of rheumatic heart disease in the developed world, and the 2020 Australian guideline is built around this reality. The high-risk Jones criteria apply across the region, the register-based prophylaxis programme is the standard of care, and the environmental health interventions — housing, sanitation, primary care access — are recognised as fundamental to prevention. Cultural safety, community partnership, and the Indigenous health workforce are as much a part of the clinical answer as the penicillin. [6] [3]
Migrant, refugee, and asylum-seeking children may arrive with established rheumatic heart disease and no documented history, and the clinician in a tertiary centre must maintain a high index of suspicion. A routine health assessment of a newly arrived child from an endemic region should include a careful cardiovascular examination and, if any murmur or symptom is present, an echocardiogram. The family may have no records of prior episodes, and the disease may present for the first time as established mitral stenosis in adolescence or young adulthood. [7] [4]
Socioeconomic disadvantage is the thread that connects all high-risk populations. Household crowding facilitates the transmission of group A streptococcus; limited access to primary care delays the treatment of the sore throat and the recognition of the ARF; and the demands of secondary prophylaxis — a clinic visit every three to four weeks for years — fall hardest on the families with the least resources. The fellowship answer acknowledges the social determinants and advocates for the structural interventions — housing, primary care, the register — that prevent the disease at its root. [6] [3]
Pregnant young women with rheumatic heart disease are a special population at the highest risk. The haemodynamic load of pregnancy can precipitate heart failure, atrial fibrillation, and death in a woman with undiagnosed or undertreated disease. Pre-pregnancy counselling, echocardiographic risk stratification, and valve intervention before conception are the safeguards, and the transition to adult congenital and valvular care is structured to catch the young woman before the first antenatal visit. [8]
Evidence, Guidelines & Regional Differences
The 2015 American Heart Association revision of the Jones criteria, led by Gewitz, is the global standard for the diagnosis of acute rheumatic fever, introducing subclinical carditis as a major criterion and the risk-stratified thresholds. The 2012 World Heart Federation criteria, led by Reményi, standardised the echocardiographic diagnosis of rheumatic heart disease, separating definite and borderline disease and enabling screening and research. The 2020 Australian guideline, led by Ralph and published in the Medical Journal of Australia, is the standard for Australia and Aotearoa New Zealand, adopting the high-risk criteria across the region and providing the prophylaxis durations that frame the fellowship answer. [1] [2] [3]
The regional differences are stark and they matter for the fellowship answer. In Australia and New Zealand, the high-risk criteria are the default, the register is the standard, and the durations of prophylaxis extend to age twenty-one and beyond. In Western Europe and North America, where the disease is rare, the standard criteria apply and the index of suspicion is lower — which creates a pitfall for the clinician who treats a recently arrived migrant child with the standard thresholds. In sub-Saharan Africa and South Asia, where the disease is common, the resources for prophylaxis and surgery are limited, and the burden of disease is correspondingly high. [3] [7]
The controversies are few but real. The role of corticosteroids in severe carditis remains debated, with limited evidence of a benefit over aspirin alone. The role of echocardiographic screening in asymptomatic children in endemic regions has been advocated by the World Heart Federation but is not yet universally implemented, because the natural history of screen-detected borderline disease and the resources for follow-up remain uncertain. And the choice between mechanical and bioprosthetic valves in young patients remains a judgement call, balancing durability against the burden of anticoagulation. [9] [8]
Exam Pearls
The fellowship answer turns on five numbers. The latent period is two to three weeks from pharyngitis to ARF. The diagnosis needs two majors or one major and two minors plus evidence of GAS, with isolated chorea and indolent carditis exempt from the serology requirement. The prophylaxis is benzathine penicillin G every twenty-one to twenty-eight days, at four hundred and fifty milligrams under twenty kilograms and nine hundred milligrams above. The duration is until at least age twenty-one for no RHD, and longer for established disease. And the valve is the mitral in the vast majority, with the aortic second. [1] [3]
The examiner probes three traps. The first is the migratory arthritis mistaken for reactive or septic arthritis — the streptococcal serology and the echo resolve it. The second is the subclinical carditis missed on auscultation — the 2015 revision means the echo is diagnostic, so request it. The third is the chorea presenting months after the sore throat with a normal ASO — diagnose clinically, start prophylaxis, do not be dissuaded by the serology. [1] [5]
The examiner rewards the candidate who frames the disease as one of inequity. The incidence among Indigenous Australian children is among the highest in the world, and the 2020 guideline applies the high-risk criteria across the region. The environmental health interventions — housing, sanitation, primary care access — are as much a part of the answer as the penicillin. The register, the recall system, and the community partnership are the safeguards against the recurrence that drives progression. A candidate who shows this awareness demonstrates the systems thinking that the fellowship demands. [6] [3]
The five major Jones criteria — FEPCS
References
- [1]Gewitz MH, Baltimore RS, Tani LY, Sable CA, Taubert KA, Rowley AH, Shulman ST, Carapetis J, Burnette MH, Wilson W, Bolger A, Palevsky T, Baltimore RS, Beaton A, Ferrieri P, Gaur A, Grusd P, Maranhao M, Padilla M, Pyles L, Rose V, Sable C, Seo HS, Shah B, Taubert K, Tani L, Wald ER, Wilson W. Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association. Circulation, 2015.PMID 25908771
- [2]Reményi B, Wilson N, Steer A, Ferreira B, Kado J, Kumar K, Lawrenson J, Maguire G, Marijon E, Mirabel M, Mocumbi AO, Mota C, Paar J, Saxena A, Scheel J, Stirling J, Viali S, Balekundri VI, Wheaton G, Zühlke L, Carapetis J. World Heart Federation criteria for echocardiographic diagnosis of rheumatic heart disease--an evidence-based guideline. Nat Rev Cardiol, 2012.PMID 22371105
- [3]Ralph AP, Noonan S, Wade V, Currie BJ; RHDAustralia (ARF/RHD writing group), on behalf of the National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand. The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. Med J Aust, 2021.PMID 33190309
- [4]Watkins DA, Roth G. Global Burden of Rheumatic Heart Disease. N Engl J Med, 2018.PMID 29298146
- [5]Carapetis JR, McDonald M, Wilson NJ. Acute rheumatic fever. Lancet, 2005.PMID 16005340
- [6]Wyber R, Wade V, Anderson A, Roberts K, O'Donnell K, Grigg K, Peiris D, Carapetis J. Rheumatic heart disease in Indigenous young peoples. Lancet Child Adolesc Health, 2021.PMID 33705693
- [7]Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis, 2005.PMID 16253886
- [8]Liaw J, Walker B, Hall H, Coffey P, Zhang L, Wright A, Zühlke L, Stocks N, Thorsten Borgh M, Katzenellenbogen JM, Ralph AP. Rheumatic heart disease in pregnancy and neonatal outcomes: A systematic review and meta-analysis. PLoS One, 2021.PMID 34185797
- [9]Grimaldi A, Ammirati E, Mirabel M, Bland E, Marijon E, Rigo F, Celani G, Marzaro R, Spadotto I, Baritussio A, Iori M, Grisorio B, Vivenzio P, Ferrara I, Maggiore SM, Posteriori C, Macaluso S, Aloi F, D'Amico G, Canevelli M, Schirru G, Celentano A, Torosucco A, Martino B, Mirarchi G, Thiene G, Iliceto S, Tona F, Marcolongo R, Spagnolo A, Bottio T, Thiene G, Tarantini G, Gerosa G, Tarantini G, D'Amico G, Iliceto S, Marijon E, Jouven X, Celermajer DS, Tafflet M, Extramiana F, Caillet M, Bondonney D, Lung B, Vahanian A, Moatti N, Wilson N. Challenges of using ultrasounds for subclinical rheumatic heart disease screening. Int J Cardiol, 2013.PMID 23245797