Paeds · cardiology
Atrial septal defect and partial anomalous pulmonary venous return
Also known as atrial septal defect · ASD · secundum ASD · partial anomalous pulmonary venous return · PAPVR · partial anomalous pulmonary venous connection · PAPVC · scimitar syndrome
A fellowship approach to atrial septal defect and partial anomalous pulmonary venous return: the auscultatory signature of a wide fixed split second heart sound, the left-to-right shunt that silently loads the right ventricle, the echo that confirms and quantifies, and the device-versus-surgery closure decision that must be made before pulmonary vascular disease becomes irreversible.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A four-year-old is referred for an asymptomatic heart murmur heard at a preschool check; or a twelve-year-old presents with exertional dyspnoea and two episodes of pneumonia in a year; or a young woman in her twenties is investigated for new atrial fibrillation and is found to have a large secundum defect. The fellowship task in each is the same: confirm with echocardiography, quantify the shunt, exclude pulmonary vascular disease, and arrange closure before the right ventricle declares itself. [5] [1]
The four moves — Recognise, Confirm, Close, Protect
Overview & Definition
An atrial septal defect is a hole in the atrial septum that allows shunting between the atria, and partial anomalous pulmonary venous return is a drainage error in which one or more pulmonary veins empty into the systemic venous circulation instead of the left atrium. The two conditions are paired here because they produce the same haemodynamic problem — a left-to-right shunt that volume-loads the right heart — and because they so often coexist, particularly with sinus venosus defects. [5] [4]
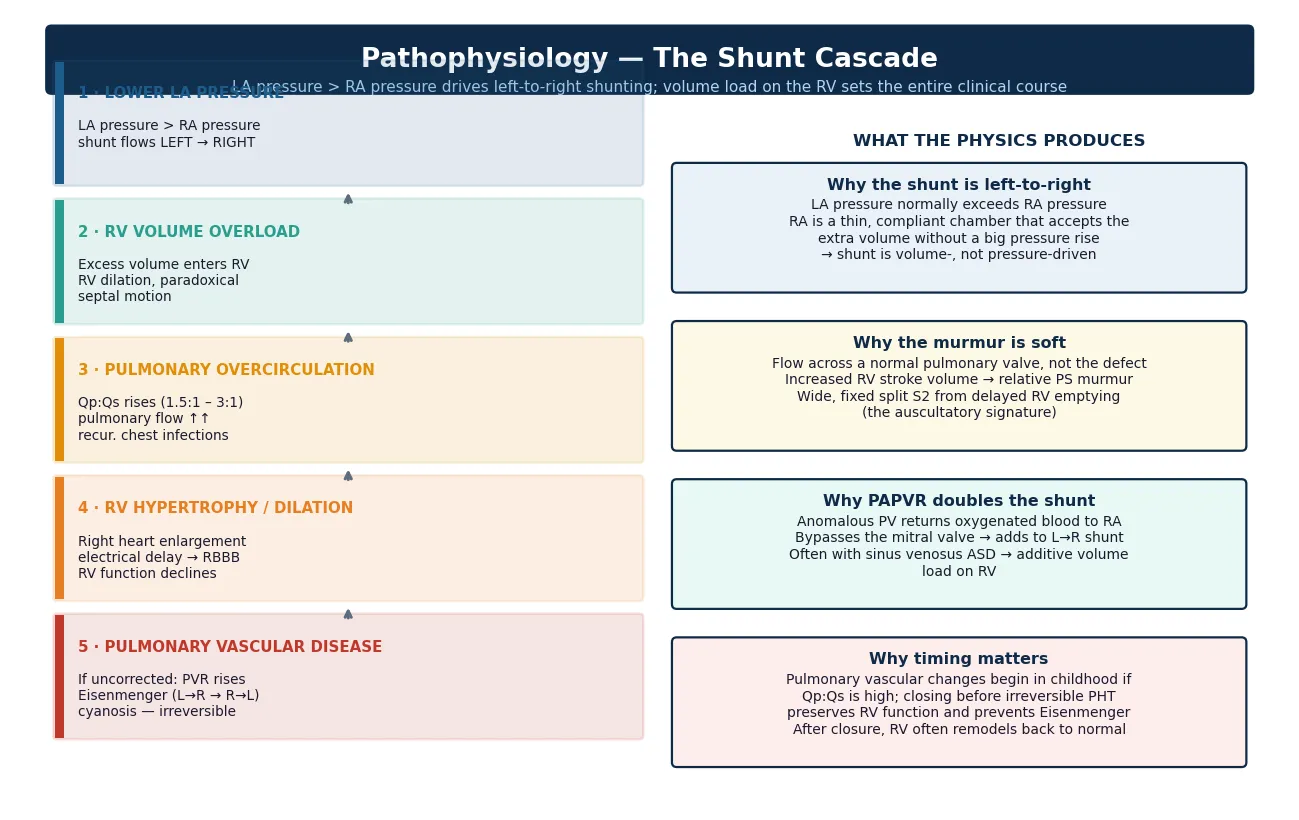
The fellowship framing turns on a single haemodynamic truth. Atrial septal defects are pressure-low, volume-high shunts, unlike the pressure-driven shunts of a ventricular septal defect. The right atrium is thin and compliant, so it accepts extra volume without a big pressure rise, the right ventricle dilates, and the pulmonary circulation is flooded with blood rather than pressure. This is why the disease is silent for so long, and why the damage accumulates insidiously. [5] [2]
The clinical importance of the condition comes from what happens if it is left untreated. A significant defect causes right ventricular dilation, exercise intolerance, recurrent respiratory infections, atrial arrhythmia, paradoxical embolism, and ultimately pulmonary vascular disease with Eisenmenger physiology. Closure of a significant defect in childhood or early adulthood prevents all of these, and the right ventricle usually remodels back to normal. The task is to find the defect, measure it, and close it in time. [1] [5]
Classification
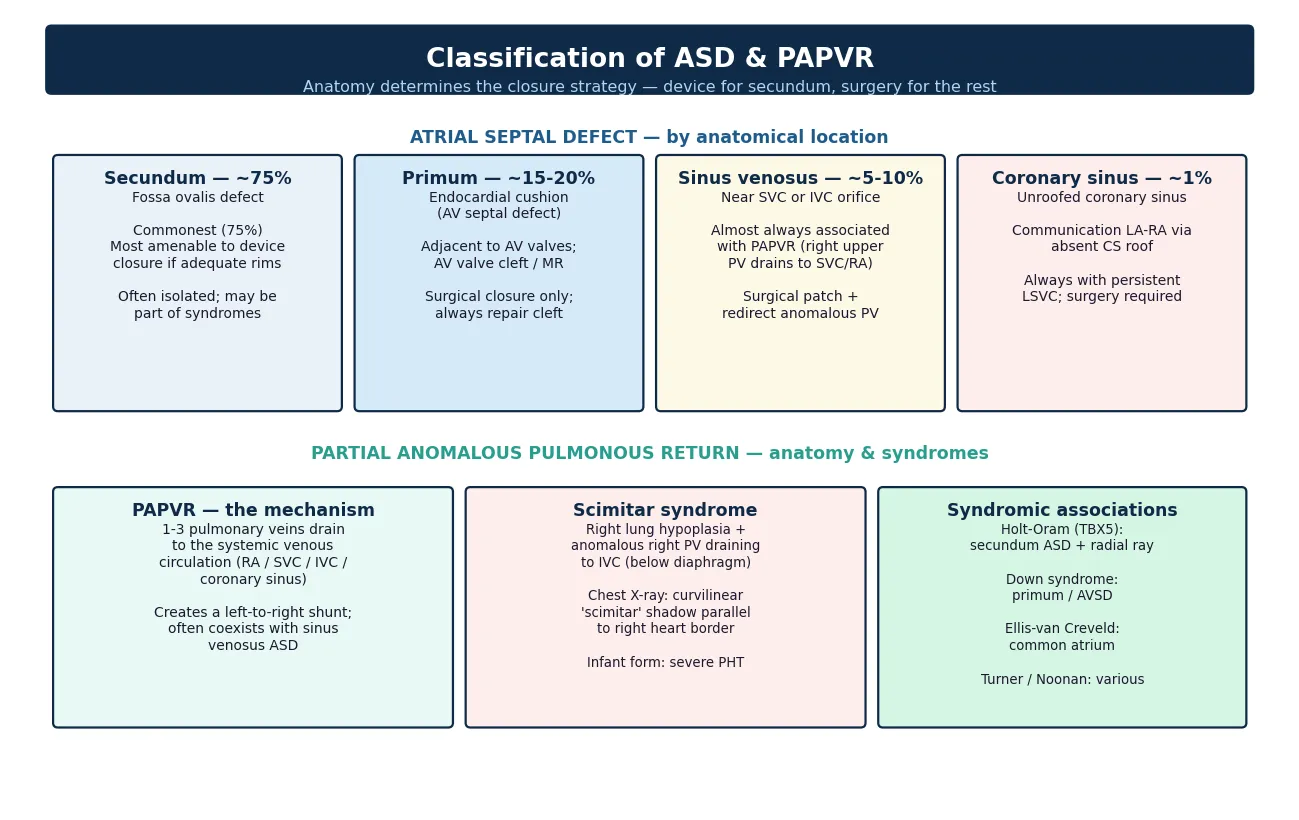
Classification of atrial septal defect rests on the anatomical location of the hole, because anatomy determines whether a device or surgery is the closure strategy. The secundum defect, in the fossa ovalis, accounts for about seventy-five per cent and is the only form reliably amenable to transcatheter device closure, provided the rims of surrounding atrial septal tissue are adequate. [5] [4]
The primum defect sits adjacent to the atrioventricular valves and is part of the atrioventricular septal defect spectrum, accounting for about fifteen to twenty per cent. It carries a cleft in the mitral or tricuspid valve that must be repaired at surgery, and it is never closed with a device. The sinus venosus defect, near the superior or inferior vena cava orifice, accounts for five to ten per cent and is almost always associated with partial anomalous pulmonary venous return — the right upper pulmonary vein drains into the superior vena cava or right atrium. The coronary sinus defect, or unroofed coronary sinus, is the rarest at about one per cent and coexists with a persistent left superior vena cava. [5] [4]
Partial anomalous pulmonary venous return is classified by where the anomalous vein drains. The commonest pattern is the right upper pulmonary vein draining to the superior vena cava, seen with sinus venosus defects. The left upper pulmonary vein may drain to the left innominate vein, and the scimitar syndrome pattern has the right pulmonary veins draining to the inferior vena cava below the diaphragm, alongside right lung hypoplasia. The anatomy is what decides the surgical approach, which is why precise imaging before theatre is non-negotiable. [7] [8]
Epidemiology & Risk Factors
Atrial septal defect is one of the commonest congenital heart lesions, accounting for roughly eight to ten per cent of all congenital cardiac defects, with a slight female predominance of about two to one. Isolated secundum defects occur in about one in fifteen hundred live births, and most are sporadic, although a family history of congenital heart disease raises the background risk two- to threefold. [4] [5]
The risk factors that matter for the fellowship answer are the syndromic associations, because they point the clinician toward the diagnosis and shape the genetic counselling. Holt-Oram syndrome, caused by TBX5 mutations, links secundum ASD with radial-ray upper limb abnormalities and should be looked for on every new secundum diagnosis. Down syndrome carries a high rate of atrioventricular septal defect, the primum end of the spectrum, and Ellis-van Creveld syndrome is associated with a common atrium. [9] [4]
Partial anomalous pulmonary venous return is found in about one in seven hundred individuals at autopsy, but it is clinically silent unless the shunt is large or it accompanies a sinus venosus defect. The infantile form of scimitar syndrome, presenting in the first months of life with heart failure and severe pulmonary hypertension, carries a mortality of up to forty-five per cent and behaves as a distinct high-acuity disease from the adult form. Recognising the infantile form and referring urgently is a must-not-miss skill. [7] [8]
Pathophysiology
The pathophysiology turns on the pressure difference between the two atria. Left atrial pressure normally sits at eight to ten millimetres of mercury, while right atrial pressure is two to five. That gradient drives blood from left to right across an atrial septal defect, volume-loading the right atrium, the right ventricle, and the pulmonary circulation, while the systemic output is relatively preserved. This is a volume-driven shunt, not a pressure-driven one, which explains why the pulmonary pressures stay low for years. [5] [4]
The right ventricle adapts to chronic volume load by dilating, which is the dominant feature on echocardiography. The dilated right ventricle bulges into the left ventricle, the interventricular septum moves paradoxically, and the electrical conduction through the dilated right heart slows, producing the right bundle branch block pattern on the electrocardiogram. None of this produces symptoms early, which is why the defect hides for decades. [5] [2]
The auscultatory findings follow directly from the volume load. The murmur is not the sound of blood crossing the defect — that flow is low-velocity and silent. The murmur is the sound of increased right ventricular stroke volume crossing a normal pulmonary valve, producing a soft, systolic ejection murmur at the upper left sternal edge. The wide, fixed, split second heart sound is the signature, caused by the right ventricle taking longer to empty against the increased pulmonary flow, so the pulmonary component of the second sound is delayed and does not vary with respiration. [5] [4]
The danger comes from the pulmonary vascular bed if the shunt is large and left untreated for years. Sustained over-circulation remodels the pulmonary arterioles, the pulmonary vascular resistance rises, and the shunt can reverse to right-to-left, producing Eisenmenger physiology with cyanosis. Once the resistance exceeds about eight Wood units with a bidirectional shunt, closure is contraindicated because the right ventricle needs the defect to decompress. This is why the timing of closure, in childhood or early adulthood, is the central decision. [1] [2]
Partial anomalous pulmonary venous return adds to the shunt because the anomalous vein returns oxygenated blood to the right atrium instead of the left. A single anomalous vein contributes a modest shunt, but several anomalous veins, or an anomalous vein combined with an atrial septal defect, can produce a shunt large enough to cause right ventricular dilation and pulmonary over-circulation. The sinus venosus defect and partial anomalous venous return are a single haemodynamic problem, which is why they are managed together. [7] [5]
Clinical Presentation
The presentation of an atrial septal defect depends entirely on the age and the size of the shunt, and the fellowship skill is to frame it as a spectrum from the asymptomatic child with an incidental murmur to the adult with atrial fibrillation or heart failure. Most children are entirely asymptomatic, and the diagnosis follows a preschool or school medical examination that picks up a murmur. [5] [4]
The symptomatic child presents with exertional dyspnoea, fatigue, or recurrent respiratory infections. The recurrent pneumonia or bronchitis is the pulmonary over-circulation making the child vulnerable to lower respiratory tract illness, and it is often the clue that shifts the clinician from reassurance to investigation. Failure to thrive is uncommon with an isolated atrial septal defect, and its presence should prompt a search for a larger or additional lesion. [4] [5]
The adult presentation reveals the untreated natural history. Atrial fibrillation or atrial flutter from atrial stretch is often the first sign, followed by exercise intolerance and right heart failure. Paradoxical embolism — a venous thrombus crossing the defect to cause a stroke — is a recognised and devastating complication. The lesson is that the asymptomatic child of today is the symptomatic adult of tomorrow, and the point of childhood closure is to prevent the adult presentation. [1] [4]
The infant with scimitar syndrome presents differently and urgently. The severe infantile form produces heart failure, severe pulmonary hypertension, and failure to thrive in the first months of life, and it carries a high mortality. The older child or adult with the milder form may be found incidentally on a chest radiograph showing the curvilinear scimitar shadow of the anomalous vein descending to the inferior vena cava. Recognising the infantile form and referring urgently is a distinct must-not-miss skill within the topic. [7] [8]
Differential Diagnosis
The differential splits into three questions. What else causes a soft pulmonary systolic murmur, what else causes right ventricular dilation, and what else causes recurrent respiratory infections in a child. The first and most important is the innocent pulmonary flow murmur, which is common and benign but lacks the wide fixed split second sound. [4] [5]
A pulmonary valve stenosis produces a louder ejection murmur at the upper left sternal edge, a systolic click, and a widely split second sound that varies with respiration, unlike the fixed split of an atrial defect. An atrioventricular septal defect produces a larger shunt with a mid-diastolic rumble from increased flow across the atrioventricular valves, and it is the diagnosis to exclude in a child with Down syndrome and a heart murmur. [5] [4]
A ventricular septal defect produces a holosystolic murmur at the lower left sternal edge, not an ejection murmur, and the second heart sound splits normally. The differential of right ventricular dilation includes pulmonary regurgitation, which gives a diastolic decrescendo murmur, and an Ebstein anomaly, which gives a systolic tricuspid regurgitation murmur and widely split second sound with severe right heart enlargement. [4] [2]
The clinical differential of recurrent respiratory infections includes asthma, immunodeficiency, and aspiration, but the atrial septal defect declares itself with the persistent auscultatory findings and the echocardiographic right heart dilation. The discriminating move is always the echocardiogram, because the auscultatory and clinical picture together raise the question, and the imaging closes it. [5] [1]
| Feature | Secundum ASD | Innocent flow murmur | Pulmonary stenosis | VSD |
|---|---|---|---|---|
| S2 | Wide, fixed split | Normal, varies with breath | Wide but varies | Normal |
| Murmur | Soft ejection, upper LSE | Short vibratory, lower LSE | Loud ejection + click | Holosystolic, lower LSE |
| RV | Dilated on echo | Normal | Hypertrophied | Normal or dilated LV |
| ECG | RBBB, RAD | Normal | RVH, RAD | Normal or LVH/LAE |
| Key clue | Fixed split S2 | Otherwise normal exam | Click + thrill | Holosystolic |
Clinical & Bedside Assessment
The recognition move runs off the auscultation. A child referred for a heart murmur earns a careful cardiovascular examination, and the question is whether the second heart sound is normal, widely split but varying, or widely and fixedly split. The wide fixed split is the finding that earns an echocardiogram, because it is the signature of an atrial-level shunt. [5] [4]
The history gathers the discriminators that shape the differential and the urgency. Ask about exertional symptoms, recurrent infections, and growth, because symptomatic disease or failure to thrive shifts the work-up toward a larger lesion. Ask about a family history of congenital heart disease, sudden death, or Holt-Oram syndrome, because the syndromic associations shape the genetic counselling. Ask about maternal diabetes, alcohol, or teratogen exposure, because these raise the background risk. [4] [9]
Examination is focused and systematic. Feel the precordium for a right ventricular impulse at the lower left sternal edge, and a pulmonary artery impulse at the upper left sternal edge. Auscultate for the soft systolic ejection murmur at the upper left sternal edge, the fixed split second heart sound, and occasionally a mid-diastolic flow rumble at the lower left sternal edge from increased flow across the tricuspid valve. Palpate the abdomen for hepatomegaly, which indicates right heart failure in advanced disease. [5] [4]
Inspect for syndromic features that point to a specific anatomy. Look for the triphalangeal thumb or radial-ray abnormality of Holt-Oram syndrome, the features of Down syndrome that point to an atrioventricular septal defect, and the polydactyly and nail dystrophy of Ellis-van Creveld syndrome. The general paediatrician's job is to recognise the murmur, refer for echocardiography, and flag the syndromic features that the cardiologist will need for the full work-up. [9] [4]
Investigations
Echocardiography is the single diagnostic investigation, and it answers every question the fellowship examiner will ask. Two-dimensional imaging shows the defect, its location, its size, and the surrounding rims of atrial septal tissue. Colour Doppler confirms the shunt and its direction. The right ventricular size, the pulmonary artery pressure estimated from the tricuspid regurgitation jet, and any associated lesions complete the picture. [5] [2]
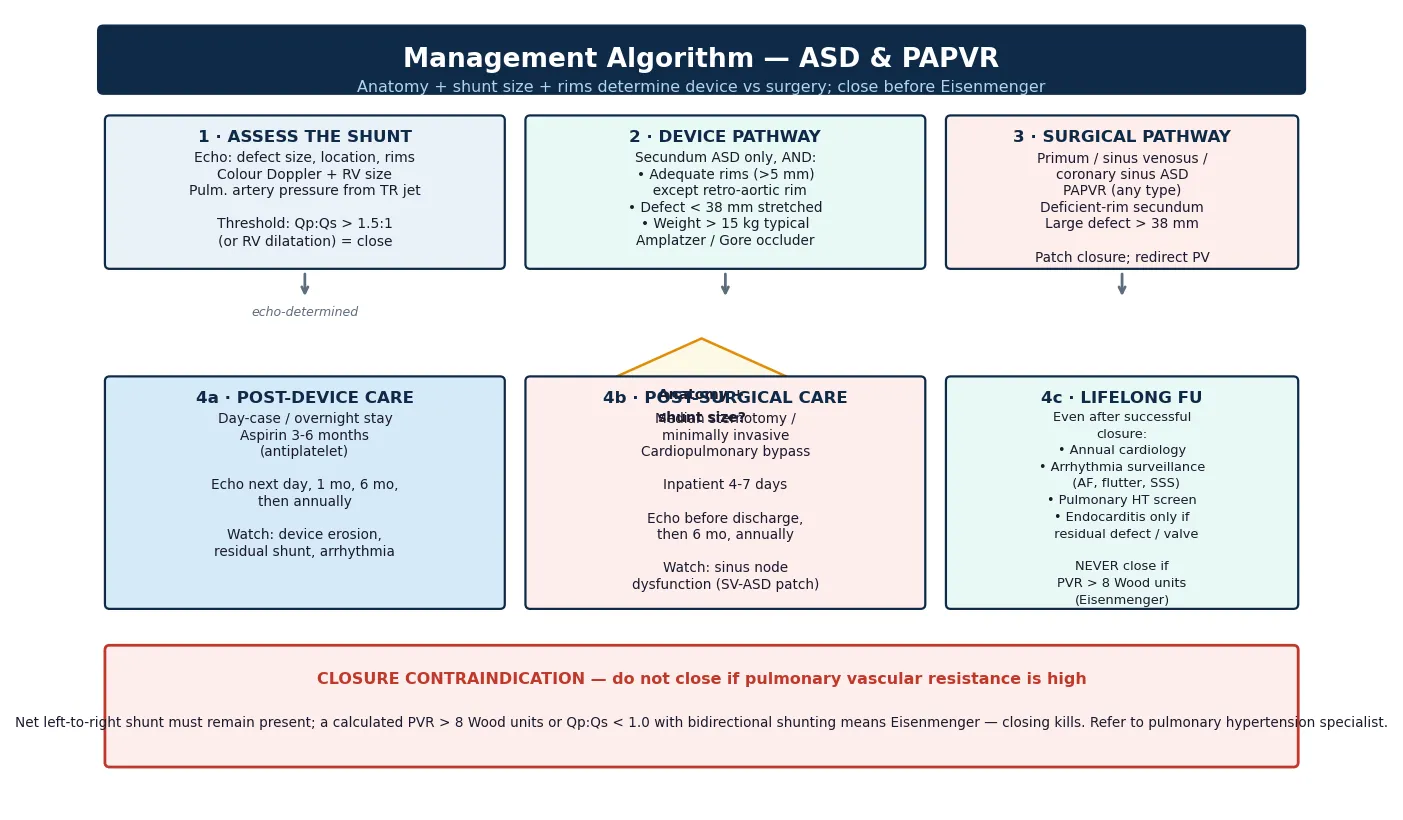
The shunt size is quantified as the ratio of pulmonary to systemic flow, the Qp to Qs ratio, and the threshold that earns closure is a ratio above 1.5 to 1, or right ventricular dilation on echocardiography regardless of the calculated ratio. A ratio below 1.5 with a normal-sized right ventricle can be observed, because the shunt is small and the long-term risk is low. The echo also determines device-versus-surgery, because the rims, the defect size, and the anatomy decide the closure strategy. [1] [6]
The electrocardiogram is supportive, showing a right bundle branch block pattern, right axis deviation in secundum defects, and a superior axis in primum defects. The chest radiograph shows cardiomegaly with right heart enlargement, increased pulmonary vascular markings, and a prominent main pulmonary artery. The scimitar syndrome radiograph shows the curvilinear anomalous vein parallel to the right heart border descending to the diaphragm, alongside a small right hemithorax. [4] [8]
Cardiac computed tomography or magnetic resonance imaging is indicated when the echocardiogram cannot fully define the anatomy, which is most often the case with sinus venosus defects and partial anomalous pulmonary venous return. The cross-sectional imaging maps the anomalous vein, its drainage site, and the relationship to the superior vena cava, and it is essential before surgery because the surgical plan depends on it. Cardiac catheterisation is reserved for measuring pulmonary vascular resistance when pulmonary hypertension is suspected, to decide whether closure is safe. [3] [7]
Management — Resuscitation
Resuscitation in atrial septal disease applies to two distinct situations. The first is the infant with severe scimitar syndrome who presents in heart failure and pulmonary hypertension, who needs oxygen, diuretics, inotropic support, and urgent referral to a congenital cardiac centre for definitive repair. The second is the rare adult with an undiagnosed large defect who presents in atrial arrhythmia or right heart failure, who needs rate control, diuresis, and anticoagulation while the closure decision is made. [7] [1]
For the infant with scimitar syndrome, the immediate priorities are oxygen supplementation to lower pulmonary vascular resistance, intravenous diuretics to reduce volume overload, and mechanical ventilation if respiratory failure supervenes. Prostaglandin is not indicated, because the ductus is not the problem. The referral to a congenital cardiac centre is urgent, because the infantile form carries a high mortality and definitive surgical repair or embolisation of the anomalous systemic arterial supply is the only durable solution. [8] [7]
For the older child or young adult, resuscitation is rarely needed because the disease is haemodynamically stable. The exception is the patient who presents in atrial fibrillation with a rapid ventricular response, who needs rate control with a beta-blocker or digoxin, anticoagulation with heparin or a direct oral anticoagulant, and electrical or chemical cardioversion once stable. The closure decision is then made once the rhythm is controlled and the pulmonary vascular status is assessed. [1] [2]
The general paediatrician's resuscitation role is to recognise the decompensated patient, stabilise them, and transfer to a centre with congenital cardiac expertise. Atrial septal defects are not duct-dependent lesions, so prostaglandin has no role, and thechild who is pink and stable does not need an emergency transfer. The emergency is the infant with scimitar syndrome and the adult with heart failure, and both need a centre that can do the definitive repair. [7] [4]
Management — Definitive & Stepwise
Definitive management is closure of the defect, and the strategy rests entirely on the anatomy as defined by echocardiography and, where needed, cross-sectional imaging. The threshold for closure is a pulmonary to systemic flow ratio above 1.5 to 1, right ventricular dilation, or symptomatic disease, and the contraindication is irreversible pulmonary vascular disease with a reversed shunt. [1] [5]
The secundum atrial septal defect with adequate rims is closed with a transcatheter device, the Amplatzer septal occluder or the Gore Cardioform device, typically as a day-case or overnight procedure under general anaesthesia and transoesophageal echocardiographic guidance. The requirements are a secundum defect in the fossa ovalis, rims of surrounding atrial septal tissue exceeding five millimetres except at the retro-aortic rim where a deficient rim is tolerated, and a stretched defect diameter under thirty-eight millimetres. Aspirin is given for three to six months for antiplatelet protection until the device endothelialises, and endocarditis prophylaxis is not needed beyond the first six months. [3] [6]
The non-secundum defects — primum, sinus venosus, and coronary sinus — and the partial anomalous pulmonary venous return, and the deficient-rim or very large secundum defect, are closed surgically. Surgery involves a median sternotomy, cardiopulmonary bypass, and direct suture or patch closure of the defect, with redirection of the anomalous pulmonary vein where present. The primum defect requires repair of the mitral valve cleft at the same operation. The sinus venosus defect with anomalous venous return requires a patch that redirects the anomalous vein through the defect into the left atrium, and care to avoid sinus node dysfunction from the patch near the superior vena cava. [2] [4]
The timing of closure is the central decision and earns the most marks. Closure in childhood or early adulthood, once the shunt meets the threshold and before pulmonary vascular disease develops, preserves the right ventricle and prevents the adult complications. Closure is contraindicated when the pulmonary vascular resistance exceeds about eight Wood units with a net right-to-left shunt, because the defect is acting as a pop-off for the right ventricle and closing it causes right heart failure. The decision rests on catheterisation when the echocardiographic pulmonary pressures are high. [1] [10]
Specific Subtypes & Scenarios
Sinus venosus atrial septal defect with partial anomalous pulmonary venous return is the subtype most often missed, and it deserves its own pathway. The defect sits near the superior vena cava orifice, the right upper pulmonary vein drains to the superior vena cava or right atrium, and the combined shunt is often large. Transthoracic echocardiography can miss the anomalous vein, so a sinus venosus defect or unexplained right ventricular dilation earns a cardiac CT or MRI. Closure is always surgical, with a patch redirecting the anomalous vein to the left atrium. [7] [5]
Scimitar syndrome is the most distinctive scenario and a fellowship favourite. The right pulmonary veins drain to the inferior vena cava below the diaphragm, the right lung is hypoplastic, and the chest radiograph shows the curvilinear scimitar shadow. The infantile form presents with heart failure, severe pulmonary hypertension, and a high mortality, and it often has an anomalous systemic arterial supply to the right lung from the aorta that adds a left-to-right shunt. The older form is milder and may be found incidentally. Management is surgical repair or embolisation of the anomalous systemic artery, and the infantile form is a surgical emergency. [7] [8]
The primum atrial septal defect and the atrioventricular septal defect are the endocardial-cushion spectrum and are commonest in Down syndrome. The defect sits adjacent to the atrioventricular valves, the mitral or tricuspid valve has a cleft that produces regurgitation, and closure is always surgical with repair of the valve cleft. A general paediatrician meeting a heart murmur in a baby with Down syndrome must exclude an atrioventricular septal defect, because the complete form produces a large shunt, pulmonary hypertension, and early heart failure. [4] [5]
Holt-Oram syndrome is the syndromic scenario that a fellowship answer should name. Caused by TBX5 mutations, it links a secundum atrial septal defect with triphalangeal thumbs and radial-ray upper limb abnormalities, inherited in an autosomal dominant pattern. Every child with a secundum atrial septal defect should have the hands examined, because the syndromic diagnosis shapes the genetic counselling and the family screening. The cardiac lesion is managed like any secundum defect, with device closure if the rims are adequate. [9]
Why the Qp to Qs ratio is the decision number
The Qp to Qs ratio measures the pulmonary to systemic flow, and it is the number that drives the closure decision. A ratio of 1.5 to 1 means half again as much blood flows through the lungs as through the body, which is the threshold above which the right ventricle dilates and the long-term complications accrue. A ratio above 2.0 is a large shunt that mandates closure. The ratio is calculated at catheterisation from the oxygen saturations, or estimated on echocardiography from the right ventricular size and the shunt width. The number exists to make the closure decision objective rather than gestalt-driven. [3] [1]
Complications & Pitfalls
The harm in atrial septal disease comes from two directions — the untreated disease that drives right heart failure, arrhythmia, and pulmonary vascular disease, and the complications of the closure itself. The fellowship answer names both, because the examiner wants to hear that closure is safe and effective but not without risk. [1] [5]
The untreated complications are the natural history. Right ventricular dilation progresses to right heart failure with hepatomegaly, peripheral oedema, and exercise intolerance, typically in the fourth or fifth decade. Atrial fibrillation and atrial flutter from atrial stretch are common and often the first presentation in adulthood. Paradoxical embolism, a venous thrombus crossing the defect to cause a stroke, is rare but devastating. Pulmonary vascular disease with Eisenmenger physiology is the end-state and is irreversible. [4] [2]
The complications of device closure are rare but serious. Device erosion into the aorta or atrial wall presents as chest pain, pericardial effusion, or tamponade, usually within days to weeks of the procedure, and it is more common with large devices and deficient aortic rims. Device thrombus, residual shunt, and atrial arrhythmia are the other device-specific risks, and they are the reason for follow-up echocardiography and aspirin for three to six months. Nickel allergy is a recognised but uncommon concern with the Amplatzer device. [3] [6]
The complications of surgical closure include sinus node dysfunction, particularly with the sinus venosus patch near the superior vena cava, post-pericardiotomy syndrome, residual shunt, and the general risks of cardiopulmonary bypass. The management pitfalls share a common root — closing a defect that should not be closed, missing an anomalous pulmonary vein at surgery, or failing to recognise the infantile form of scimitar syndrome. The safeguard is precise preoperative imaging and a centre with congenital cardiac expertise. [2] [7]
Prognosis & Disposition
The prognosis of a closed atrial septal defect is excellent, and a child whose defect is closed in childhood or early adulthood has a life expectancy close to the normal population. The right ventricle remodels back to normal size within months of closure, exercise tolerance returns, and the risk of the untreated complications — heart failure, arrhythmia, paradoxical embolism — falls dramatically. The single biggest predictor of outcome is the timing of closure, because the pulmonary vascular bed is preserved when closure happens early. [1] [5]
The residual risk is small but measurable and is the reason lifelong follow-up is recommended. Arrhythmia, particularly atrial fibrillation and atrial flutter, remains more common than in the general population even after closure, especially when closure is late. Pulmonary hypertension can persist or progress if closure happened after the vascular changes had begun, and it needs surveillance. These residual risks are the substance of the adult congenital follow-up that every closed child transitions into. [2] [10]
The general paediatrician owns the recognition and the referral, and the disposition is shared, structured care. Paediatric cardiology drives the closure decision, the procedure, and the early follow-up. The adult congenital cardiology service takes over at transition and provides the lifelong surveillance for arrhythmia and pulmonary hypertension. A named coordinator prevents the fragmentation that is the enemy of a lifelong follow-up plan, and the transition to adult care is structured and documented. [1] [4]
The prognosis of the untreated disease is the warning that justifies the whole topic. An atrial septal defect left untreated progresses to right heart failure, atrial arrhythmia, paradoxical embolism, and pulmonary vascular disease over decades, and the mortality is measurably higher than the closed population. The fellowship answer frames the prognosis in these honest terms — near-normal with early closure, and the natural history of a serious disease if left alone. [4] [5]
Special Populations
Atrial septal disease interacts with the child's social, cultural, and developmental context, and the same closure plan behaves differently across populations. Access to echocardiography, to a congenital cardiac centre, and to lifelong follow-up are the determinants of outcome, and a plan that is clinically correct but unattainable for a family is no plan at all. [1] [4]
Indigenous children in Australia and Aotearoa New Zealand may face later presentation through reduced access to primary care auscultation, echocardiography, and specialist referral, particularly in remote communities. The asymptomatic murmur that a routine examination would catch can be missed, and the disease declares itself later as the adult complications. Telehealth and outreach extend the diagnostic and follow-up net into communities that a clinic-based model would miss, and a low threshold to auscultate and refer is the safeguard. [4] [2]
Migrant, refugee, and asylum-seeking families may arrive with no documented echocardiogram and an uncertain cardiac history, and the atrial septal defect may not have been diagnosed in the country of origin. A careful history, a cardiovascular examination at the arrival health check, and an echocardiogram for any suspicious murmur or fixed split second heart sound are the foundations, and the results are communicated in the family's language with an interpreter. [4] [1]
Socioeconomic disadvantage shapes access to the device or the surgery, the transport to the cardiac centre, and the capacity to attend lifelong follow-up. The limiting step is often logistics — travel, accommodation near the cardiac centre, time off work — rather than the procedure itself. Structuring the closure and the follow-up around a coordinated visit, linking the family to transport and accommodation support, and using telehealth to reduce travel all improve engagement. The transition to adult congenital care is the point at which young people are most often lost to follow-up, and targeted support at that transition protects the long-term outcome. [1] [10]
Evidence, Guidelines & Regional Differences
The evidence base rests on the 2018 American Heart Association and American College of Cardiology guideline for the management of adults with congenital heart disease, the 2020 European Society of Cardiology guideline for adult congenital heart disease, and the 2008 ACC/AHA guideline that preceded them. These guidelines frame the closure thresholds, the device-versus-surgery decision, the contraindications, and the lifelong follow-up, and they are the operational standard for every congenital cardiac service. [1] [2]
The 2021 JACC guideline comparison of the American and European documents is a useful synthesis for the fellowship answer, because it highlights where the two guidelines converge and where they differ. Both endorse closure for a Qp to Qs ratio above 1.5 to 1, both recommend device closure for secundum defects with adequate rims, and both contraindicate closure in irreversible pulmonary vascular disease. The differences are in the detail of the follow-up intervals and the thresholds for pulmonary hypertension screening, which are areas of evolving practice. [10] [1]
The Feltes 2011 American Heart Association scientific statement on indications for cardiac catheterisation and intervention in paediatric cardiac disease remains the reference for the transcatheter approach, and the Geva 2014 Lancet review of atrial septal defects is the comprehensive single-source reference. The Alkashkari 2020 review of current practice in atrial septal defect occlusion frames the device approach and the outcomes, and the Aristizabal 2024 scimitar syndrome series frames the surgical management of that distinct entity. [3] [5] [6] [7]
Where the evidence is weak, a fellowship answer says so honestly. The optimal age for closure of a moderate secundum defect is not settled, with some centres closing in early childhood and others waiting until later. The long-term outcome of the newer Gore Cardioform device relative to the Amplatzer occluder is still accumulating. The management of the small asymptomatic defect with a Qp to Qs ratio below 1.5 is a genuine area of uncertainty, and the role of closure for migraine or paradoxical embolism in the absence of a large shunt is debated. Naming the uncertainty is a mark of intellectual honesty that examiners reward. [2] [10]
In Australia and Aotearoa New Zealand, atrial septal defects are managed according to the international guidelines, with paediatric cardiology in the major centres and shared care with general paediatrics and primary care across rural and remote regions. Transcatheter device closure is the standard for secundum defects with adequate rims, performed in the congenital cardiac centres in the capital cities, and surgical closure for non-secundum defects and partial anomalous venous return is performed by congenital cardiac surgeons. Telehealth extends the diagnostic and follow-up net into rural and remote communities, and the Cardiac Society of Australia and New Zealand provides the operational standard. Transition to adult congenital cardiology happens in the late teenage years through a structured handover. [1] [2]
Exam Pearls
A fellowship candidate answering on atrial septal defect and partial anomalous pulmonary venous return should land five anchor points and avoid three classic traps. The anchors are the framework examiners listen for, and the traps are where easy marks are lost. [5] [1]
Anchor one: recognise the auscultatory signature. A soft pulmonary ejection murmur with a wide, fixed, split second heart sound is the signature of a significant atrial septal defect. Never dismiss it as innocent. [4]
Anchor two: confirm with echocardiography. Echo shows the defect, the location, the size, the rims, the shunt, and the right ventricular size, and it decides device versus surgery. Cross-sectional imaging is added for sinus venosus defects and partial anomalous venous return. [5]
Anchor three: close before Eisenmenger. The closure threshold is a Qp to Qs ratio above 1.5 to 1 or right ventricular dilation, and the contraindication is irreversible pulmonary vascular disease. Catheterise if the pulmonary pressures are high. [1]
Anchor four: anatomy sets the strategy. Secundum with rims is device-closed; primum, sinus venosus, coronary sinus, and partial anomalous venous return are surgical. The mitral valve cleft is repaired with the primum defect. [2]
Anchor five: lifelong follow-up. Even after successful closure, arrhythmia surveillance and pulmonary hypertension screening continue, and the transition to adult congenital care is structured. [10]
The three traps to avoid are closing a defect with Eisenmenger physiology, missing the anomalous pulmonary vein in a sinus venosus defect, and forgetting the syndromic associations. Secundum defects account for seventy-five per cent, sinus venosus defects almost always carry partial anomalous venous return, the closure threshold is a Qp to Qs above 1.5 to 1, and aspirin is given for three to six months after device closure — the high-yield facts a candidate holds. [1] [7]
References
- [1]Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, Colman JM, Crumb SR, Dearani JA, Fuller S, Gurvitz M, Khairy P, Landzberg MJ, Saidi A, Valente AM, Van Hare GF. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol, 2019.PMID 30121239
- [2]Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, Diller GP, Lung B, Kluin J, Lang IM, Meijboom F, Moons P, Mulder BJM, Oechslin E, Roos-Hesselink JW, Schwerzmann M, Søndergaard L, Zeppenfeld K; ESC Scientific Document Group. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J, 2021.PMID 32860028
- [3]Feltes TF, Bacha E, Beekman RH 3rd, Cheatham JP, Feinstein JA, Gomes AS, Hijazi ZM, Ing FF, de Moor M, Morrow WR, Mullins CE, Taubert KA, Zahn EM. Indications for cardiac catheterization and intervention in pediatric cardiac disease: a scientific statement from the American Heart Association. Circulation, 2011.PMID 21536996
- [4]Warnes CA, Williams RG, Bashore TM, Child JS, Connolly HM, Dearani JA, del Nido P, Fasules JW, Graham TP Jr, Hijazi ZM, Hunt SA, King ME, Landzberg MJ, Miner PD, Radford MJ, Walsh EP, Webb GD. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol, 2008.PMID 19038677
- [5]Geva T, Martins JD, Wald RM. Atrial septal defects. Lancet, 2014.PMID 24725467
- [6]Alkashkari W, Alsubhi A, Alahmadi H, Alghamdi A, Al-Juhani S, Al-Halees Z, Al-Aklabi M, AlBugami S, Omair A, Arheden H, Cullen S, Qureshi SA. Current practice in atrial septal defect occlusion in children and adults. Expert Rev Cardiovasc Ther, 2020.PMID 32441165
- [7]Aristizabal AM, Sincleir C, Velasquez N, Jaramillo M, Aristizabal O, Sanchez D, Forero J, Zuleta C, Quintero D. Clinical characteristics, imaging findings, management, and outcomes of patients with scimitar syndrome at a tertiary care center. Int J Cardiovasc Imaging, 2024.PMID 38634941
- [8]Sehgal A, Loughran-Fowlds A, Chacko J, Fahl M. Scimitar syndrome. Indian J Pediatr, 2005.PMID 15812123
- [9]C S SL, Saya RP, Vasireddy A. Holt-Oram Syndrome With Atrial Septal Defect. Cureus, 2024.PMID 39156428
- [10]Egidy Assenza G, Cassini D, Pela G, Zambon S, Dall'Aglio A, Capuzzo C, Margheriti F, Pucci A, Faccioli L, Landolfi M, Bonvicini M, Placidi G, Gargiulo GD, Dallapiccola B, Pacileo G, Limongelli G. AHA/ACC vs ESC Guidelines for Management of Adults With Congenital Heart Disease: JACC Guideline Comparison. J Am Coll Cardiol, 2021.PMID 34736567