Paeds · cardiology
Bradyarrhythmias, heart block and pacing
Also known as Bradycardia · Atrioventricular block · AV block · Complete heart block · Congenital heart block · Heart block · Sinus node dysfunction · Sick sinus syndrome · Paediatric pacing · Pacemaker
Fellowship guide to bradyarrhythmias, atrioventricular block and cardiac pacing in children: how to read the slow rhythm on a 12-lead ECG, the anatomy of first-degree, Mobitz I, Mobitz II and third-degree block, why maternal anti-Ro antibodies scar the fetal AV node, the post-surgical AV block that will not recover, the stable-versus-unstable resuscitation fork, atropine and transcutaneous pacing, and the permanent pacemaker indications — including the 2021 PACES consensus, the ACCF/AHA/HRS and ESC pacing guidelines, epicardial versus transvenous versus leadless systems, and the lifelong care of the paced child.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the four-year-old brought in because she "tires on the trampoline and keeps needing to sit down." The GP hears a heart rate of forty-five and sends her to the emergency department, where the triage note reads "fit and healthy, likely athletic." That child carries the whole story of complete heart block: an abnormally slow rate dismissed as fitness, a slow ventricular escape rhythm holding her circulation together, and a single twelve-lead ECG that would change everything. Bradycardia in a child is never normal in the way that it can be in a conditioned adult athlete, and the question is always the same — where is the block, what caused it, and does she need a pacemaker. [4] [1]
A bradyarrhythmia is any pathologically slow heart rhythm — conventionally a rate below the age-adjusted normal range that is inadequate for the child's cardiac output. The two mechanisms are failure of impulse formation at the sinus node (sinus node dysfunction, sometimes called sick sinus syndrome in children) and failure of impulse conduction through the atrioventricular node or His-Purkinje system (atrioventricular block). The latter is the clinically important entity in paediatrics because it is the one that produces symptomatic, unpredictable bradycardia and carries a risk of sudden death when the escape rhythm fails. [4] [2]
The clinical importance of paediatric bradycardia rests on three facts. It is symptomatic: a slow rate in a child who needs a high cardiac output to grow and play shows up as fatigue, poor feeding, exercise intolerance, syncope, or heart failure rather than as a number on a monitor. It is under-recognised: a slow pulse is routinely attributed to fitness or to medications rather than investigated with an ECG, and the first presentation of complete heart block is sometimes a Stokes-Adams syncopal attack or sudden death. And it is treatable: the AV node and His-Purkinje system have a finite capacity to recover, but once the block is permanent, a pacemaker restores rate, abolishes symptoms, and prevents sudden death with excellent long-term outcomes. [5] [7]
Classification
The most useful way to classify a paediatric bradycardia is by the anatomical level of the problem — sinus node versus atrioventricular node — because the level determines the ECG appearance, the natural history, and the pacing threshold. A second layer classifies by aetiology, because congenital and post-surgical block behave very differently. [4] [2]
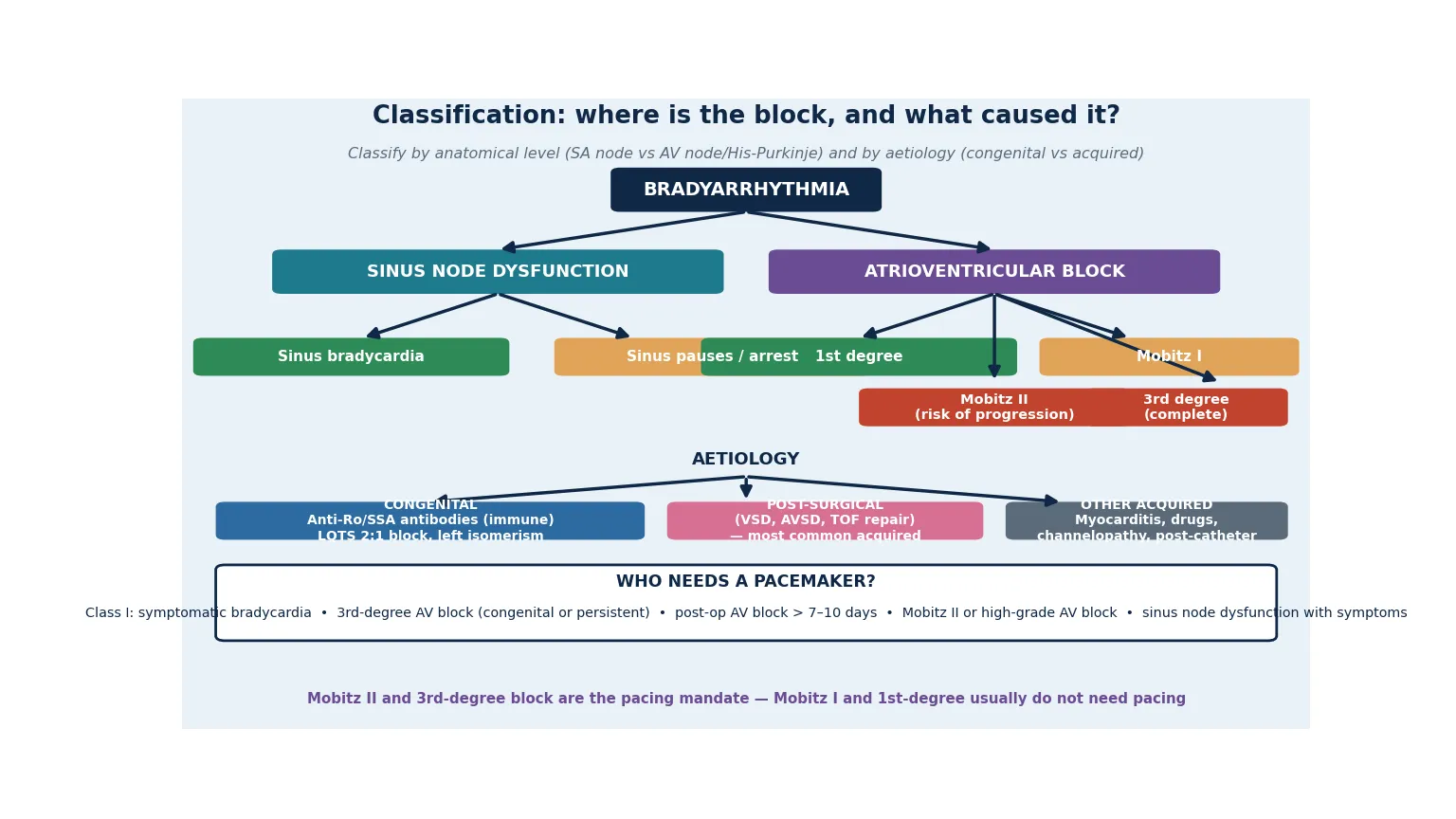
Atrioventricular block is graded by degree. First-degree AV block is a PR interval beyond the age-adjusted upper limit (broadly greater than the range for age, often quoted as greater than 200 milliseconds in older children) in which every atrial impulse still conducts. Second-degree AV block is intermittent failure of conduction and has two subtypes: Mobitz I (Wenckebach), in which the PR interval progressively lengthens until a beat is dropped, and Mobitz II, in which the PR interval is constant and one or more beats drop without warning. Third-degree (complete) AV block is total dissociation of atrial and ventricular activity, with the ventricles driven by a slow escape pacemaker below the block. [4] [2]
1st degree
PR prolonged, all conduct
- PR above age-adjusted range, every P followed by QRS
- Usually benign in isolation
- Does not need pacing
- Can progress if paired with other disease
- Exclude drugs and electrolytes
Mobitz I (Wenckebach)
PR lengthens, then drops
- Progressive PR prolongation until a dropped beat
- Usually at the AV node, narrow QRS
- Benign in children; often physiological
- No pacemaker unless symptomatic
- Seen during sleep, high vagal tone
Mobitz II
Constant PR, sudden drop
- Constant PR with suddenly dropped beats
- Often infranodal, wide QRS
- Real risk of progression to complete block
- Pacing indicated even if asymptomatic
- Distinct from Wenckebach — do not confuse
3rd degree (complete)
P and QRS dissociated
- Total AV dissociation, slow escape rhythm
- Congenital (anti-Ro) or post-surgical
- Pacing indicated when permanent
- Risk of syncope and sudden death
- Junctional escape (narrow) better than ventricular (wide)
Aetiology splits the paediatric population into three groups. Congenital complete heart block is dominated by immune-mediated disease, in which transplacental maternal anti-Ro/SSA (or anti-La) antibodies cross the placenta and damage the developing conduction tissue, and to a lesser extent by structural associations such as left atrial isomerism and levo-transposition of the great arteries. Post-surgical AV block is the commonest acquired form, complicating repair of ventricular septal defect, atrioventricular septal defect, and tetralogy of Fallot where sutures or patches sit close to the AV node and His bundle. A smaller third group covers myocarditis, infiltrative disease, drugs (digoxin, beta-blockers, calcium-channel blockers), and the channelopathies, of which long-QT syndrome presenting with 2:1 AV block in infancy is the prototype. [4] [6]
Epidemiology & Risk Factors
Congenital complete heart block affects approximately one in fifteen thousand to twenty thousand live births. The immune-mediated form accounts for the majority and is strongly linked to maternal connective tissue disease — systemic lupus erythematosus and Sjögren syndrome — through the passage of anti-Ro/SSA and anti-La antibodies across the placenta. Not every antibody-positive mother has a child with heart block: the recurrence risk in a subsequent pregnancy after one affected child is roughly fifteen to twenty per cent, and the overall risk in an antibody-positive pregnancy is about one to two per cent. [6] [9]
The numbers that anchor your viva
The highest-risk presentations cluster at the extremes of age and in the post-operative setting. Fetal complete heart block presenting in utero carries significant mortality, particularly when it is complicated by hydrops fetalis, and the neonate diagnosed in the nursery may have myocarditis of the antibody-mediated cardiomyopathy form alongside the conduction disease. Post-surgical AV block occurs in a small but important minority of repairs near the AV node, and the patient who has already had one cardiac operation for complex congenital heart disease is the one most likely to need a device. Children with inherited channelopathies, particularly long-QT syndrome with 2:1 AV block in infancy, and those with maternal antibody exposure, are the two groups most likely to present with bradycardia in the absence of surgery. [6] [10]
The most important risk stratification variable is whether the block is transient or permanent. Transient causes — drugs, electrolyte disturbance, acute myocarditis, early post-operative oedema — may resolve and do not in themselves mandate a device. Permanent causes — immune-mediated fibrosis, surgical transection, and the late post-operative block that has not recovered — do mandate pacing, because the slow escape rhythm that holds the child together today will not reliably hold forever. [4] [2]
Pathophysiology
The teaching model rests on a single concept: the heart's electrical impulse is normally generated at the sinus node, delayed at the atrioventricular node, and distributed through the His-Purkinje system, and disease at any of these points slows the rate or blocks conduction — the resulting slow ventricular escape rhythm is what the clinician hears as bradycardia and what the child experiences as low cardiac output. [4] [2]
In the dominant paediatric mechanism, immune-mediated congenital complete heart block, maternal immunoglobulin G anti-Ro/SSA (also called anti-SSA, the 52-kDa and 60-kDa Ro antigens) and anti-La antibodies cross the placenta from approximately sixteen weeks of gestation. The antibodies bind to the developing fetal conduction tissue — the AV node and the His-Purkinje system — where they trigger an inflammatory cascade, apoptosis, and ultimately fibrosis. Once scarred, the AV node does not conduct, the atria and ventricles beat independently, and a slow escape rhythm emerges from below the block. Because the damage is structural and permanent, immune-mediated block does not recover, and the child faces lifelong dependence on a pacemaker. The conduction tissue is most vulnerable between eighteen and twenty-four weeks of gestation, which is why fetal heart block typically declares on serial echocardiography in the second trimester in an anti-Ro positive pregnancy. [6] [9]
The escape rhythm is the concept that bridges the blocked conduction to clinical symptoms. Below the level of block, a subsidiary pacemaker takes over to keep the ventricles beating. A junctional escape rhythm arises from around the AV junction, produces a narrow QRS at roughly forty to sixty beats per minute, and is relatively reliable. A ventricular escape rhythm arises from below the His bundle, produces a wide QRS at twenty to forty beats per minute, and is slow and unstable. The slower and more distal the escape, the poorer the cardiac output and the higher the risk that the rhythm will fail altogether, producing a Stokes-Adams syncopal attack or sudden death. This is the whole justification for pacing a child with complete heart block — not to improve a number on the monitor, but to replace an unreliable escape rhythm with a dependable one before it fails. [5] [4]
[1] [2]The other mechanisms complete the picture. Post-surgical AV block reflects direct mechanical or ischaemic injury to the AV node or His bundle at the time of repair; the block may recover within days if it is oedematous, or persist permanently if the tissue is transected. Channelopathic block, most characteristically long-QT syndrome presenting in infancy with 2:1 AV block, occurs because the QT interval is so prolonged that alternate atrial impulses arrive while the ventricles are still refractory and are not conducted. Acquired reversible causes — digoxin toxicity, beta-blocker or calcium-channel-blocker excess, electrolyte disturbance, and acute myocarditis — impair AV nodal conduction acutely and may resolve when the insult is removed. Recognising the reversible causes matters because pacing a child with digoxin toxicity is the wrong operation. [4] [2]
Clinical Presentation
The presentation of a bradyarrhythmia in a child spans a wide spectrum, from the incidental finding on an ECG obtained for another reason, through exercise intolerance and fatigue, to syncope and sudden death. The age and context of presentation depend heavily on the aetiology. [4] [6]
In the fetus, congenital complete heart block presents as a persistent bradycardia detected on routine antenatal scanning or on serial echocardiography of an anti-Ro positive pregnancy, and may be complicated by hydrops fetalis when the slow rate cannot sustain adequate cardiac output. In the neonate and infant, complete heart block shows up as poor feeding, tachypnoea, mottling, or heart failure, and the slow rate may be the first clue on a routine postnatal check. Infants with antibody-mediated disease may also have a dilated cardiomyopathy from the same antibody injury to the myocardium, which compounds the heart failure and worsens the prognosis. [6] [10]
[1] [4]In the older child and adolescent, complete heart block or sinus node dysfunction presents as exercise intolerance, fatigue, presyncope or syncope — often during exertion, when cardiac output cannot rise to meet demand because the rate is fixed — and occasionally as seizures from cerebral hypoxia during a Stokes-Adams attack. Sinus node dysfunction in children is often seen after atrial surgery (for example, the Mustard or Senning repairs of transposition, or after Fontan) and presents with profound sinus bradycardia, sinus pauses, and junctional or atrial escape rhythms, sometimes alternating with atrial tachyarrhythmias in the so-called tachycardia-bradycardia syndrome. Post-operative AV block declares itself in the intensive care unit in the days after surgery, with the monitor showing dropped beats or complete dissociation. [4] [7]
| Clinical picture | What it implies | Act |
|---|
Differential Diagnosis
Build the differential in two layers: first, the causes of a slow heart rate that are not pathological AV block, and second, the causes of AV block that are reversible and must not be missed before committing a child to a device. The distinction matters because a reversible cause treated in time makes a pacemaker unnecessary. [4] [2]
The physiological and benign causes of a slow rate include the high vagal tone of sleep, breath-holding, and athletic conditioning, all of which produce sinus bradycardia or even Wenckebach that disappears with activity. Sinus bradycardia from hypothyroidism, hypothermia, and raised intracranial pressure must be considered and treated at the source. In the immediate newborn period, a slow rate is often sinus bradycardia from apnoea or from hypoxia rather than intrinsic conduction disease, and the resuscitation question is airway and oxygenation before it is cardiology. [4] [2]
Reversible AV block
- Drug toxicity — digoxin, beta-blockers, calcium-channel blockers, amiodarone
- Electrolyte disturbance — hyperkalaemia, hypokalaemia
- Acute myocarditis (often recovers)
- Early post-operative oedema (days 1–3)
- Hypoxia in the newborn (sinus bradycardia)
Sinus bradycardia mimics
- High vagal tone (sleep, breath-holding, athlete)
- Hypothyroidism, hypothermia
- Raised intracranial pressure
- Eating disorder with bradycardia
- Newborn apnoea / hypoxia
Permanent AV block
- Congenital immune CHB (anti-Ro fibrosis)
- Surgical transection of the His bundle
- Post-op block persistent beyond 7–10 days
- Long-QT syndrome with 2:1 block
- Progressive familial / genetic conduction disease
The key to resolving the differential is the twelve-lead ECG with a long rhythm strip, interpreted alongside the clinical context and a focused history of recent surgery, medication, maternal autoimmune disease, and family history. The ECG distinguishes sinus bradycardia (normal P wave morphology and PR, just slow) from AV block (abnormal conduction), and the degree and morphology of block — particularly the distinction between Mobitz I and Mobitz II, and the wide versus narrow QRS of the escape rhythm — guide both prognosis and pacing. A reversible cause identified in time is treated and the bradycardia resolves; a permanent cause identified in time is paced. The mistake to avoid is labelling a slow rate as benign without an ECG, or committing to a device before excluding digoxin toxicity. [4] [2]
Clinical & Bedside Assessment
Assessment runs from the history through the examination to a careful twelve-lead ECG with a long rhythm strip, because the diagnosis and the pacing decision hinge on the electrocardiogram and on whether the child is symptomatic. A child with a slow heart rate needs a focused cardiac assessment before the bradycardia is attributed to fitness, sleep, or medication. [4] [1]
The history targets the symptoms that make bradycardia pathologically significant: fatigue, poor feeding in the infant, exercise intolerance, dizziness, presyncope, and syncope — particularly during exertion, when a fixed slow rate cannot raise cardiac output. Ask about recent cardiac surgery (the post-operative setting is the single most common context for new AV block), medications (digoxin, beta-blockers, calcium-channel blockers, amiodarone), and a maternal history of systemic lupus erythematosus, Sjögren syndrome, or known anti-Ro antibodies. A family history of pacemaker implantation in early life, sudden death, or congenital heart disease raises the possibility of a genetic conduction disorder. The collateral history from parents and teachers is invaluable because the young child does not articulate fatigue as a cardiac symptom. [4] [6]
The examination looks for the haemodynamic consequences of the slow rate — pallor, mottling, cool peripheries, a low blood pressure, hepatomegaly and gallop rhythm of heart failure, and signs of reduced cerebral perfusion. The pulse is slow and may be irregular where beats are dropped. A cannon A wave may be visible in the jugular venous pulse in complete heart block, where the atria contract against a closed tricuspid valve. In the stable, well-perfused child, the examination may be normal apart from the bradycardia — and a normal examination does not exclude important block. [4] [1]
The ECG is read systematically. Confirm the rate is below the age-adjusted normal range. Measure the PR interval and decide whether every P wave conducts (first-degree block) or whether beats are dropped (second-degree). In second-degree block, decide whether the PR lengthens before the dropped beat (Mobitz I, Wenckebach — usually benign) or stays constant (Mobitz II — a pacing indication). In complete heart block, confirm that the P waves and QRS complexes are independent and assess the escape rhythm: a narrow QRS at forty to sixty beats per minute suggests a junctional escape, and a wide QRS at twenty to forty suggests a ventricular escape that is inherently less stable. [4] [2]
Investigations
The diagnostic strategy has three tiers: the resting twelve-lead ECG with a long rhythm strip to characterise the rhythm, ambulatory Holter monitoring to capture intermittent block or pauses, and echocardiography and ancillary testing to define the cause and exclude structural and reversible contributors. The goal is to confirm the rhythm, decide whether it is permanent or reversible, and determine whether a pacing indication is met. [4] [1]
The twelve-lead ECG with a long rhythm strip is the single most important investigation, and in complete heart block it is usually diagnostic. It defines the degree and morphology of block, the width and rate of the escape rhythm, and any associated abnormalities such as a prolonged QT (raising long-QT syndrome with 2:1 block) or signs of chamber hypertrophy from associated congenital heart disease. In a child with intermittent symptoms and a normal resting ECG, a twenty-four-hour (or longer) Holter monitor captures sinus pauses, dropped beats, or episodes of complete block that declare themselves only intermittently, and an exercise test may unmask rate-related block or confirm failure of the rate to rise with exertion. [4] [2]
Echocardiography excludes structural congenital heart disease (atrial septal defect, atrioventricular septal defect, left atrial isomerism, congenitally corrected transposition), assesses ventricular function — which may be impaired in antibody-mediated endocardial fibroelastosis or dilated cardiomyopathy — and detects the hydrops of fetal or neonatal heart failure. In the child with suspected immune-mediated block, maternal and infant antibody titres (anti-Ro/SSA and anti-La) are sent; in the post-operative child, serial ECGs document whether conduction is returning; and in any child, electrolytes, thyroid function, and a drug history exclude reversible contributors. A fluorine- or inflammation-based workup is reserved for suspected myocarditis, and electrophysiology study is rarely needed for diagnosis in children but may clarify the level of block when it is uncertain. [6] [4]
The standard diagnostic workup
12-lead ECG with a long rhythm strip — define the rate, the PR interval, the degree and morphology of block, and the escape rhythm (narrow vs wide QRS).
Ambulatory Holter monitoring (24–48 hours or longer) for intermittent block, sinus pauses, or the tachycardia-bradycardia pattern; exercise test for exertional symptoms.
Echocardiography — exclude structural congenital heart disease, assess ventricular function and endocardial fibroelastosis, detect hydrops or heart failure.
Maternal and infant anti-Ro/SSA and anti-La antibody titres if immune-mediated congenital block is suspected; maternal autoimmune history.
Electrolytes (potassium, calcium, magnesium), thyroid function, and a full medication review to exclude reversible causes (digoxin, beta-blocker, calcium-channel blocker).
Serial ECGs in the post-operative child to document whether conduction returns within the seven-to-ten-day decision window.
Cardiology referral for pacing decision against the 2021 PACES, ACCF/AHA/HRS and ESC indications.
Management — Resuscitation
The acute presentation of a bradycardic child follows the paediatric resuscitation algorithm, with one critical modification: the unstable bradycardic child is paced early, because the AV node that is blocked does not respond to atropine the way a slow sinus node does. The aim is to restore an adequate rate and cardiac output while the cause is found and definitive management planned. [1] [2]
Assess and support the airway, breathing, and circulation, attach cardiac monitoring, and obtain intravenous access. If the child is unstable — hypotensive, altered mental state, poor perfusion, or in heart failure — identify and treat reversible causes (hypoxia, hypoglycaemia, electrolyte disturbance, drug toxicity) using the standard approach, and treat the bradycardia. Atropine at 0.02 milligrams per kilogram (minimum 0.1 milligram, maximum 0.5 milligram per dose, may repeat) is effective for sinus bradycardia driven by high vagal tone, but it is unreliable for AV block and should not delay pacing when the rhythm is blocked. Epinephrine at 0.01 milligrams per kilogram intravenously supports the rate and blood pressure as a bridge to pacing. [1] [3]
SLOW-RATE
The definitive acute intervention for the unstable bradycardic child with AV block is pacing. Transcutaneous pacing through pacing pads on the chest is the fastest to deploy and is used as a bridge while transvenous access is obtained; transvenous pacing through a temporary wire into the right ventricle is more reliable and more comfortable and is the standard bridge to a permanent system. In the infant or the child with complex congenital heart disease where venous access is difficult, temporary epicardial pacing wires may be placed. While pacing is established, an isoprenaline or epinephrine infusion may hold the intrinsic rate and blood pressure, but pacing is the definitive bridge. The child is admitted to a high-dependency or intensive care bed with continuous monitoring pending the permanent pacing decision. [1] [3]
Management — Definitive & Stepwise
Definitive management is the decision to implant a permanent pacemaker, governed by guideline indications, and the choice of system — epicardial, transvenous, or leadless — tailored to the child's size, anatomy, and congenital heart disease. The 2021 PACES expert consensus, the ACCF/AHA/HRS device guidelines, and the ESC pacing guidelines are broadly concordant on the indications. [1] [2]
The Class I pacing indications in children are symptomatic bradycardia attributable to the rhythm; congenital third-degree AV block with a wide QRS escape, complex congenital heart disease, ventricular ectopy, or a ventricular rate below an age-defined threshold; persistent third-degree AV block of any cause; post-operative second- or third-degree AV block not resolved within seven to ten days of surgery; Mobitz II and high-grade AV block; and sinus node dysfunction with symptomatic bradycardia. In congenital complete heart block, asymptomatic infants and children are paced on rate and QRS criteria because the natural history without pacing includes syncope and sudden death — the Michaëlsson prospective study of adults with congenital complete block established that the unpaced course carries significant mortality, which underpins prophylactic pacing even in the apparently asymptomatic child. [5] [1]
The life arc of a child with complete heart block
The choice of pacing system follows the child. In infants and small children (broadly below approximately twenty to thirty kilograms, and whenever there is an intracardiac shunt or complex congenital heart disease that makes a transvenous lead risky), an epicardial system with leads placed on the surface of the heart at surgery is preferred because it avoids thromboembolic risk across a shunt and accommodates growth. In larger children and adolescents with a structurally normal heart or repaired congenital disease without residual shunt, a transvenous system with the lead passed via the subclavian vein to the right ventricular apex is standard and less invasive. Leadless pacemakers — fully intracardiac devices without transvenous leads — are an emerging option in selected older children and adolescents and address the long-standing problem of lead fracture and venous occlusion; the PACES collaborative study reported real-world experience with transcatheter leadless pacing in children. The atrium is paced where possible to preserve atrioventricular synchrony and reduce the long-term risk of pacing-induced cardiomyopathy, which is why dual-chamber or atrial-based pacing is favoured over single-chamber ventricular pacing in the child with an intact sinus node. [1] [12]
Lifelong surveillance is part of the disease. The paced child is reviewed regularly with device interrogation, lead impedance and threshold checks, and assessment of generator battery life; growth, activity, and lead-related complications (fracture, insulation breach, venous occlusion, infection) are monitored over decades. Fortescue and colleagues showed that patient, procedural, and hardware factors all contribute to pacemaker lead failures in paediatrics and congenital heart disease, which underpins the structured follow-up. The transitioning adolescent needs a planned handover to an adult congenital heart disease service, with counselling about sport, driving, and (for women with congenital block) pregnancy, which carries a recurrence risk of immune-mediated block if the mother herself is anti-Ro positive. [11] [7]
Specific Subtypes & Scenarios
Congenital complete heart block from maternal anti-Ro antibodies is the prototype paediatric bradyarrhythmia. It affects approximately one in fifteen thousand to twenty thousand live births, presents in the second trimester as fetal bradycardia or after birth as a slow rate, and is permanent because the fibrotic AV node does not recover. Management is a pacemaker when the rate, QRS width, or symptoms meet guideline thresholds, and the prognosis with pacing is excellent. The maternal pregnancy should be counselled about the fifteen to twenty per cent recurrence risk in a subsequent anti-Ro positive pregnancy, and serial fetal echocardiography from sixteen weeks is the surveillance strategy that detects first- and second-degree block — the stages at which transplacental treatment may be considered. [6] [9]
Post-surgical atrioventricular block is the commonest acquired form. It complicates repairs near the AV node and His bundle — ventricular septal defect, atrioventricular septal defect, and tetralogy of Fallot — and presents in the intensive care unit in the days after surgery. The decision rule is to maintain temporary pacing and to implant a permanent system if normal conduction has not returned by seven to ten days, because conduction that has not recovered by then is almost always permanent and carries a risk of late sudden death. This rule is one of the most examined facts in paediatric pacing and is common to the PACES, ACCF/AHA/HRS, and ESC documents. [1] [2]
Sinus node dysfunction in children is most often seen after extensive atrial surgery, classically the Mustard or Senning atrial switch for transposition and the Fontan procedure for single-ventricle physiology, and produces profound sinus bradycardia, sinus pauses, and junctional escape, sometimes alternating with atrial flutter or fibrillation in a tachycardia-bradycardia pattern. Management is atrial pacing for symptomatic bradycardia or pauses, often combined with antiarrhythmic control of the atrial tachyarrhythmia, and the long-term challenge is balancing rate support against tachycardia-induced cardiomyopathy. [4] [7]
Long-QT syndrome with 2:1 atrioventricular block is a distinctive infantile presentation in which the QT interval is so prolonged that alternate atrial impulses arrive during the ventricular refractory period and are not conducted, producing a functional 2:1 block and a slow rate. The mechanism is not conduction disease but extreme repolarisation prolongation, and the management is beta-blockade and genotype-specific care for the underlying channelopathy rather than pacing in isolation — though pacing may be needed if beta-blocker-related bradycardia aggravates the QT. Any infant with 2:1 AV block has long-QT syndrome until proven otherwise by a careful QT measurement. [4] [2]
Antibody-mediated fetal and neonatal heart block with cardiomyopathy represents the severe end of the immune spectrum, in which the same anti-Ro antibodies injure the myocardium and conduction tissue together, producing endocardial fibroelastosis, dilated cardiomyopathy, and a poor prognosis. Trucco and colleagues described the use of intravenous immunoglobulin and corticosteroids in maternal autoantibody-mediated cardiomyopathy, and the modern fetal strategy uses standardised transplacental anti-inflammatory treatment to try to halt progression of first- or second-degree block — though once third-degree block is established, treatment does not reverse it and pacing is inevitable. [10] [9]
Complications & Pitfalls
The complications of paediatric bradyarrhythmia are the consequences of the slow rate itself — syncope, heart failure, and sudden death from a failing escape rhythm — and the complications of pacemaker therapy over a lifetime. The 1995 prospective study by Michaëlsson established that adults with isolated congenital complete heart block followed without pacing had significant mortality from syncope and sudden death, which underpins the modern practice of prophylactic pacing even in the asymptomatic child. [5] [7]
On the device side, the complications are those of any implantable system amplified by decades of life and by growth. Lead failure — fracture, insulation breach, and dislodgement — is the commonest hardware problem in children, and Fortescue and colleagues identified patient age, procedural factors, and hardware characteristics as the determinants of lead failure in paediatrics and congenital heart disease. Venous occlusion and thrombosis across an intracardiac shunt are risks of transvenous systems, which is why epicardial leads are preferred in small children and in unrepaired shunts. Generator-site infection and endocarditis are serious and may require system extraction. Pacing-induced cardiomyopathy from chronic right ventricular apical pacing is a long-term concern that drives the preference for atrial-based or biventricular pacing where the anatomy allows. [11] [1]
The risks that drive management intensity
The common clinical pitfalls are: attributing a slow rate to athletic fitness or sleep without an ECG; confusing Mobitz I (benign) with Mobitz II (a pacing indication) on the ECG; relying on atropine for AV block and delaying pacing in the unstable child; waiting beyond seven to ten days for post-operative block to recover; missing a reversible cause (digoxin toxicity, electrolytes) before committing to a device; failing to recognise long-QT-related 2:1 block in an infant as a repolarisation disorder rather than conduction disease; and underestimating the psychosocial and activity burden of a lifelong device in a child. The non-clinical pitfall is failing to counsel an anti-Ro positive mother about recurrence risk and fetal surveillance in future pregnancies. [4] [2]
Prognosis & Disposition
With modern management, the prognosis of a child with complete heart block who receives an appropriate pacemaker is excellent. Pacing abolishes symptoms, prevents syncope and sudden death, and allows normal growth, schooling, and activity, with low long-term mortality and a good quality of life. The Michaëlsson prospective data, which documented the natural history without pacing, provide the historical counterfactual that justifies prophylactic pacing in the asymptomatic child with congenital block. [5] [7]
The prognosis is not uniform. Higher-risk features include fetal presentation (particularly with hydrops), associated antibody-mediated cardiomyopathy or endocardial fibroelastosis, complex congenital heart disease, a wide-QRS ventricular escape, and presentation in early infancy. The French nationwide cohort of late outcomes of congenital and childhood non-immune isolated atrioventricular block documented the long-term course and the ongoing risk of pacemaker need and cardiac events, reinforcing that even apparently isolated childhood block warrants lifelong surveillance. [8] [6]
Disposition is outpatient management under a specialist paediatric cardiology and pacing service, with the general paediatrician playing a critical role in recognising the slow rate, supporting the family through device implantation, and co-ordinating care during intercurrent illness. The paced child has regular device checks, lead and generator surveillance over decades, and activity guidance appropriate to the system. The transitioning adolescent receives a structured handover to an adult congenital heart disease service, with counselling on sport, driving, and the heritability of immune-mediated block in future pregnancies — a woman with anti-Ro positive congenital block has a recurrence risk in her own pregnancies and needs fetal echocardiographic surveillance from sixteen weeks. [1] [7]
Special Populations
The fetus with congenital complete heart block is managed by maternal-fetal medicine and fetal cardiology in partnership. Serial echocardiography from sixteen weeks in an anti-Ro positive pregnancy detects first- and second-degree block, the stages at which transplacental treatment with fluorinated corticosteroids or intravenous immunoglobulin may be considered to halt progression; once third-degree block is established the conduction disease is irreversible, and management shifts to supporting the fetal circulation, treating hydrops, and planning delivery and neonatal pacing. The Mawad cohort documented outcomes of antibody-mediated fetal heart disease with standardised transplacental anti-inflammatory treatment. [9] [6]
The neonate and infant with congenital complete heart block may be asymptomatic at rest because the junctional escape holds the circulation, but decompensates with intercurrent illness, feeds, or growth. Infants with low ventricular rates, wide-QRS escape, ventricular ectopy, complex congenital heart disease, or heart failure meet guideline criteria for early pacemaker implantation, usually with an epicardial system because of small size. Antibody-mediated cardiomyopathy compounds the picture and worsens prognosis. [6] [10]
The transitioning adolescent and young adult with a lifelong device faces adherence challenges, body-image and activity concerns, growth-related lead stress, and the handover to adult care. Structured transition — education about the device, self-management, sport and driving guidance, and a warm handover to an adult congenital heart disease service — is standard and is emphasised in the PACES consensus. Women with anti-Ro mediated congenital block need counselling that they carry a recurrence risk in their own pregnancies and require fetal echocardiographic surveillance. [1] [7]
Resource-limited and remote populations, including Indigenous, refugee, and rural communities, face diagnostic delays and limited access to fetal surveillance, paediatric pacemaker programmes, and lifelong device follow-up. Telehealth cardiology, a low threshold for ECG in any unexplained paediatric bradycardia, protocol-driven stabilisation of the unstable child with transcutaneous pacing as a bridge, and retrieval to a pacing centre are part of equitable practice. The global reality is that congenital heart block in many settings still presents as syncope or sudden death rather than as an antenatal or neonatal finding. [6] [3]
Evidence, Guidelines & Regional Differences
| Region | Key guideline | Pacing system preference | Leadless / emerging |
|---|
The controversies a candidate should be able to discuss are the threshold for pacing the asymptomatic infant with congenital complete block (rate and QRS criteria guide the decision, but practice varies at the boundary), the role of cardiac resynchronisation therapy in the paced child who develops pacing-induced cardiomyopathy, the place of leadless pacemakers as the technology matures in small children, the appropriate use of transplacental treatment (corticosteroid, intravenous immunoglobulin, hydroxychloroquine) for first- and second-degree fetal block, and the long-term management of the post-Fontan or post-atrial-switch patient with sinus node dysfunction who carries both bradycardia and atrial tachyarrhythmia. [1] [9]
Exam Pearls
References
- [1]Shah MJ, Silva JN, Czosek RJ, Bates S, Reinholtz K, et al. 2021 PACES Expert Consensus Statement on the Indications and Management of Cardiovascular Implantable Electronic Devices in Pediatric Patients. JACC Clin Electrophysiol, 2021.PMID 34794667
- [2]Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA 3rd, Freedman RA, et al. 2012 ACCF/AHA/HRS focused update incorporated into the ACCF/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol, 2013.PMID 23265327
- [3]Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J, 2013.PMID 23801822
- [4]Baruteau AE, Pass RH, Thambo JB, Behaghel A, Le Franc P, et al. Congenital and childhood atrioventricular blocks: pathophysiology and contemporary management. Eur J Pediatr, 2016.PMID 27351174
- [5]Michaëlsson M, Jonzon A, Riesenfeld T Isolated congenital complete atrioventricular block in adult life. A prospective study. Circulation, 1995.PMID 7634461
- [6]Eronen M, Siren MK, Ekblad H, Tikanoja T, Julkunen H, et al. Short- and long-term outcome of children with congenital complete heart block diagnosed in utero or as a newborn. Pediatrics, 2000.PMID 10878154
- [7]Eronen M Long-term outcome of children with complete heart block diagnosed after the newborn period. Pediatr Cardiol, 2001.PMID 11178669
- [8]Mycinski F, Baruteau AE, Bodeau C, Malot M, Gournay V, et al. Late outcomes of congenital and childhood non-immune, isolated atrioventricular block: a French nationwide retrospective cohort study. Europace, 2025.PMID 40067976
- [9]Mawad W, Jaeggi E, Hutter D, Friedberg MK, Stolarz K, et al. Outcome of Antibody-Mediated Fetal Heart Disease With Standardized Anti-Inflammatory Transplacental Treatment. J Am Heart Assoc, 2022.PMID 35001672
- [10]Trucco SM, Jaeggi E, Cuneo B, Moon-Grady AJ, Silverman E, et al. Use of intravenous gamma globulin and corticosteroids in the treatment of maternal autoantibody-mediated cardiomyopathy. J Am Coll Cardiol, 2011.PMID 21292131
- [11]Fortescue EB, Berul CI, Cecchin F, Walsh EP, Alexander ME Patient, procedural, and hardware factors associated with pacemaker lead failures in pediatrics and congenital heart disease. Heart Rhythm, 2004.PMID 15851146
- [12]Shah MJ, Karpawich PP, Bothe G, Shepard M, Bhaya M, et al. Transcatheter Leadless Pacing in Children: A PACES Collaborative Study in the Real-World Setting. Circ Arrhythm Electrophysiol, 2023.PMID 37039017