Paeds · cardiology
Cardiac transplantation and ventricular assist devices
Also known as Cardiac transplantation and ventricular assist devices · Paediatric heart transplantation · Paediatric ventricular assist device · Berlin Heart EXCOR · Mechanical circulatory support in children · Bridge to transplant
Fellowship guide to cardiac transplantation and ventricular assist devices in children: when to escalate from medical heart-failure therapy to mechanical circulatory support, the Berlin Heart EXCOR and continuous-flow durable devices, the INTERMACS urgency profiles, bridge-to-transplant versus bridge-to-recovery strategy, donor allocation and transplant surgery, the denervated transplanted heart, lifelong immunosuppression and surveillance for rejection, cardiac allograft vasculopathy and post-transplant malignancy, and the family pathway through retrieval, listing and long-term follow-up.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Cardiac transplantation and ventricular assist devices are the two destinations for the child whose heart failure has become refractory to medical therapy. Transplantation replaces the failing pump with a donor heart; a ventricular assist device (VAD) is a mechanical pump that takes over the work of the ventricle, used to keep the child alive and to restore end-organ function until either the native heart recovers or a donor organ becomes available. Together they are the field of advanced paediatric mechanical circulatory support, and the skill is knowing when to leave medical therapy behind and when to commit to a device and a transplant pathway. [4]
The decision is built on a single principle: a child should be transplanted before irreversible injury to the pulmonary vascular bed, the kidneys or the liver. A ventricular assist device is the instrument that buys the time and reverses the end-organ damage so that the child arrives at transplantation in the best possible condition, and for a subset with myocarditis or a recoverable cardiomyopathy it is itself the cure. The Berlin Heart EXCOR is the established paracorporeal pulsatile pump used as a bridge to transplantation in children including small infants, and miniaturised continuous-flow devices now extend durable support to larger children and adolescents. [1] [11]
Classification
Advanced mechanical circulatory support in children is classified on three axes: the type of device, the urgency of the patient, and the strategic goal of the support. All three must be stated, because a profile-1 child on a durable Berlin Heart with a bridge-to-recovery strategy is a very different clinical problem from a profile-3 adolescent on a continuous-flow device with a bridge-to-transplant strategy. [11]
The device axis distinguishes short-term from durable support. Short-term devices — extracorporeal membrane oxygenation (VA-ECMO) and centrifugal pumps such as the CentriMag — are used for acute collapse, post-cardiotomy failure and as a rapid stabilising measure in the sickest children; they are not intended for weeks of support. Durable devices are designed for longer support and divide into the paracorporeal pulsatile Berlin Heart EXCOR, which has pump sizes small enough for neonates and infants, and the miniaturised implantable continuous-flow pumps used in larger children and adolescents. The child's size is the dominant determinant of device choice, because until recently there was no durable continuous-flow option for the smallest patients. [1] [11]
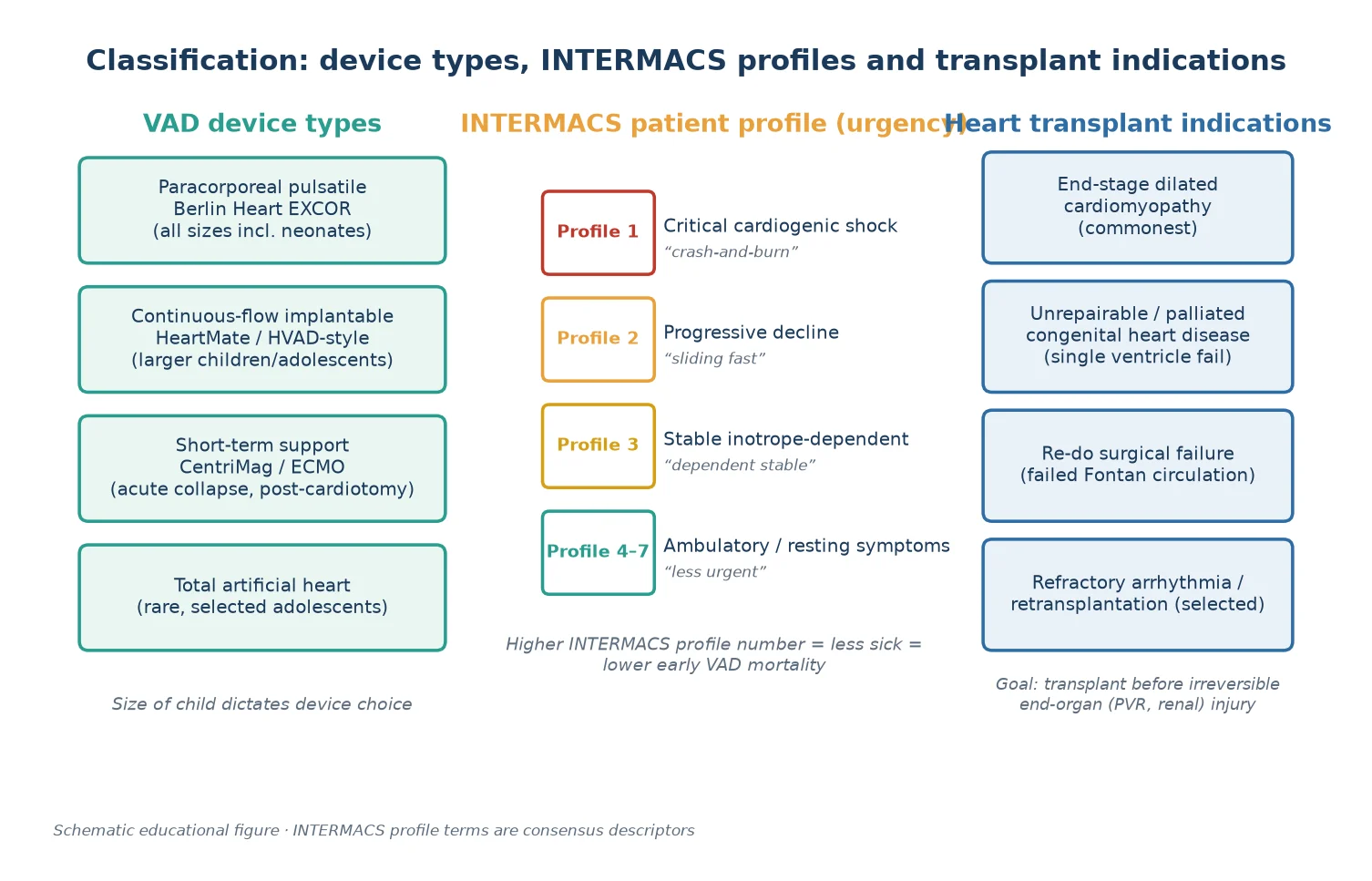
The urgency axis uses the INTERMACS patient profile, a consensus scale from 1 (critical cardiogenic shock, the 'crash-and-burn' patient with the highest early mortality on support) through 2 (progressive decline) and 3 (stable but inotrope-dependent) to the ambulatory profiles 4 to 7. The profile predicts how sick the child is, how urgently a device is needed, and the early mortality risk on support; the lower profiles justify short-term stabilisation with ECMO before a durable device. The strategic-goal axis names why the device is being placed: bridge to transplantation for most children, bridge to recovery for selected myocarditis and cardiomyopathy, bridge to candidacy for the child who needs end-organ recovery before listing, and destination therapy, which is uncommon in children. [2] [5]
Epidemiology & Risk Factors
The children who reach transplantation and ventricular assist devices are the refractory tail of paediatric heart failure. The epidemiology of acute decompensated heart failure in children, characterised by multicentre registry data, defines the population from which candidates are drawn: most are infants and young children with congenital heart disease or a cardiomyopathy. The commonest reason a child is listed for transplantation is a dilated cardiomyopathy, followed by congenital heart disease — most often the failing single-ventricle (Fontan) circulation — and then retransplantation and other causes. [6] [8]
The International Society for Heart and Lung Transplantation registry reports the global paediatric transplant population. Recipient characteristics shift with era and allocation policy: cardiomyopathy remains the dominant indication across age groups, but congenital heart disease accounts for a large share of infant transplants, reflecting the surgical complexity of the smallest patients. Survival after paediatric transplantation is excellent in the medium term, with a substantial proportion of recipients surviving beyond ten years, which is the central justification for the resource intensity of the pathway. [8]
The risk factors for needing a device or a transplant are the risk factors for refractory heart failure itself: a dilated cardiomyopathy with a low ejection fraction and progressive remodelling, an acute myocarditis that fails to recover, a failing Fontan circulation, and a re-do surgical patient in low output after complex congenital repair. The sickest candidates — INTERMACS profile 1 — carry the highest early mortality on support, which is why short-term stabilisation with ECMO is used to improve the child's condition before a durable device is committed. [3] [6]
Pathophysiology
The pathophysiology that drives a child onto a device and toward transplantation is the neurohormonal vicious cycle of advanced heart failure. The failing ventricle cannot generate adequate cardiac output, so the sympathetic nervous system, the renin-angiotensin-aldosterone system and antidiuretic hormone are activated to support blood pressure and filling. This briefly sustains output but chronically remodels the ventricle, producing myocyte hypertrophy, fibrosis and apoptosis, a falling ejection fraction, and progressive chamber dilation. Once medical therapy can no longer interrupt this cycle, the ventricle is refractory and mechanical support becomes necessary. [6]
A ventricular assist device interrupts the cycle mechanically rather than pharmacologically. The pump takes over the work of the ventricle, reducing wall stress and filling pressure, restoring forward cardiac output, and decompressing the dilated chamber. The downstream consequences are exactly what makes a device valuable: end-organ perfusion improves, the kidneys and liver recover, nutrition and growth resume, and crucially the pulmonary vascular bed may unload enough for the resistance to fall. For a child with myocarditis or a recoverable cardiomyopathy, the unloading itself allows the myocardium to heal and the device to be weaned; for the rest, it is the bridge to a donor organ. [1] [4]
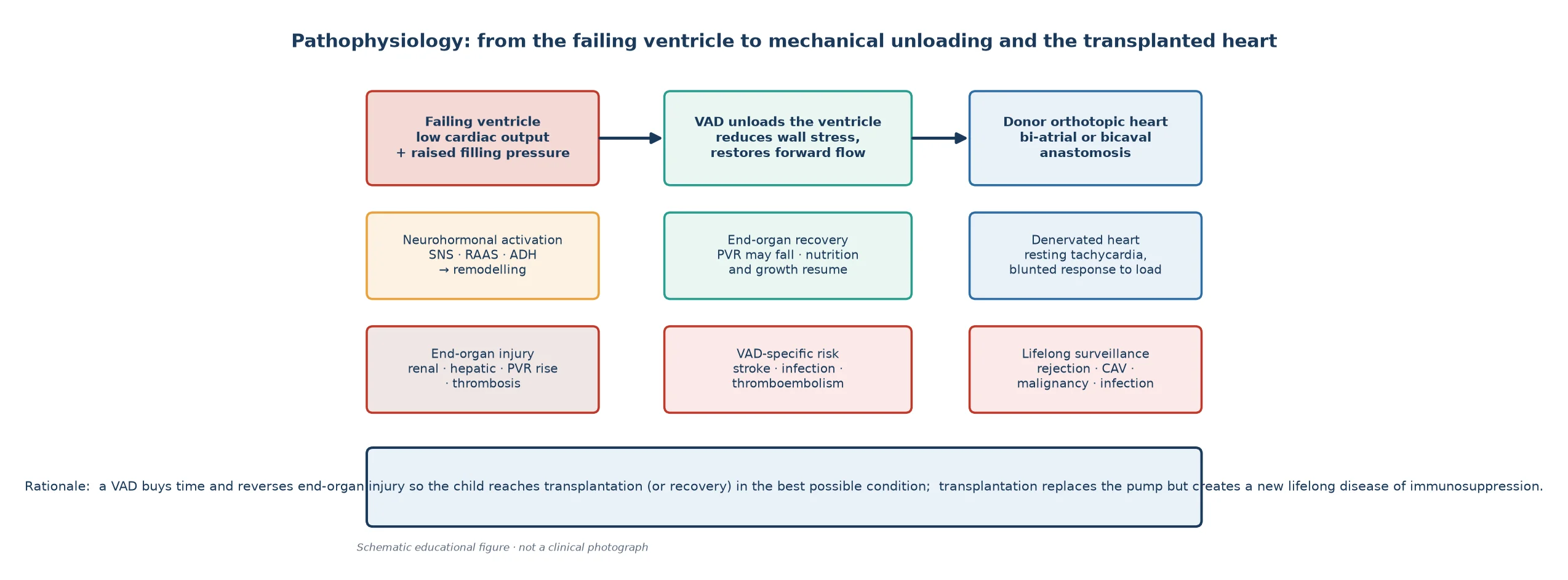
Transplantation replaces the failing pump but creates a new physiology. The donor heart is denervated, so it beats at a resting tachycardia and mounts a blunted chronotropic response to exercise, relying on circulating catecholamines rather than neural drive to raise output with exertion. The transplant recipient then lives with a new lifelong disease: immunosuppression to prevent rejection, which carries the risks of infection, cardiac allograft vasculopathy (a diffuse intimal proliferation of the graft vessels that is the leading cause of late graft loss), post-transplant malignancy (notably post-transplant lymphoproliferative disease), and the renal toxicity of calcineurin inhibitors. Understanding the denervated heart and the burden of immunosuppression is the core of long-term transplant follow-up. [4] [8]
Clinical Presentation
The child who needs advanced mechanical circulatory support presents with refractory heart failure — a syndrome that no longer responds to guideline medical therapy. The infant shows tachypnoea, sweating with feeds, failure to thrive and hepatomegaly despite a loop diuretic, an ACE inhibitor and caloric supplementation; the older child shows exercise intolerance, dyspnoea and poor growth that worsen despite optimised chronic therapy. The signal that escalation is needed is the persistence or progression of these signs on maximal treatment, particularly with emerging end-organ dysfunction. [6]
The sickest end of the spectrum is the INTERMACS profile 1 child in critical cardiogenic shock: grey, mottled, poorly perfused, with weak pulses, oliguria and a rising lactate, often already on one or more inotropes and deteriorating despite them. This child needs immediate short-term mechanical circulatory support — typically venoarterial extracorporeal membrane oxygenation — to restore perfusion and prevent irreversible end-organ death, before a durable device or transplantation can be considered. The profile 2 and 3 children are declining or stable on inotropes but not yet in extremis, and they are the candidates in whom a durable device is placed as a planned bridge. [3] [5]
The child already on a ventricular assist device presents differently. The pump and its driveline are visible and audible (a paracorporeal EXCOR clicks with each cycle), and the consultation shifts to device function, anticoagulation and complications. A new neurological sign on a device is a stroke until proven otherwise, a fever is line or pump infection until excluded, and any change in pump parameters or output may signal thrombosis or cannula obstruction. The transplanted child in long-term follow-up presents with the consequences of immunosuppression: fever may be rejection or opportunistic infection, exertional decline may be cardiac allograft vasculopathy, and a new lymphadenopathy or mass raises post-transplant lymphoproliferative disease. [2] [10]
Differential Diagnosis
The differential in advanced heart failure is the cause of the refractory pump failure, because the cause shapes whether recovery is possible and how urgently a device is needed. The common causes are dilated cardiomyopathy (the largest group, often genetic), acute myocarditis (potentially recoverable, so always considered for bridge-to-recovery), the failing Fontan circulation and other complex congenital disease, and re-do surgical low output. A tachycardia-induced cardiomyopathy from an uncontrolled supraventricular tachycardia is reversible and must be excluded before committing to a device — controlling the rhythm can cure the failure. [4] [6]
For the child who collapses, the differential of cardiogenic shock includes septic shock, myocarditis, a duct-dependent lesion in the newborn, and an inborn error of metabolism, all of which can mimic one another. The practical point is that any child in refractory shock with a poor cardiac output needs echocardiography to define the pump function and structural status, a lactate and septic and metabolic screen to exclude mimics, and a low threshold for short-term mechanical circulatory support if low output persists despite resuscitation. Stabilising first and diagnosing the cause in parallel is safer than waiting for certainty. [6]
The must-not-miss reversible causes that change the plan are three. First, a tachycardia-induced cardiomyopathy resolves with rate or rhythm control and should not reach a device. Second, an endocrine or metabolic cardiomyopathy (thyroid, electrolyte) may be correctable. Third, a recoverable fulminant myocarditis may be weaned from a device — which is why a bridge-to-recovery strategy is kept open for the myocarditis and selected cardiomyopathy presentations. Failing to identify a reversible cause commits a child unnecessarily to transplantation and lifelong immunosuppression. [4]
Clinical & Bedside Assessment
Bedside assessment of the child being considered for advanced support quantifies how refractory the failure has become and whether end-organ injury is emerging. Plot the weight and height and document the trend: a child still crossing centiles downward on maximal therapy, or failing to grow despite high-calorie feeds, is failing medical management. Assess perfusion with capillary refill, pulse volume and skin temperature, and palpate the liver edge as the most reliable marker of backward failure and of response to a device once it is in place. [6]
The cardiovascular examination reveals the underlying cause and the current haemodynamic state. Characterise the murmur, feel the precordium and locate the apex, listen for a gallop that signals a failing ventricle, and take the blood pressure and four-limb pulses to exclude a coarctation or obstructive lesion that might be surgically remediable rather than transplant-requiring. In the child already on a device, the assessment extends to the pump and driveline: confirm the device is cycling and producing adequate flow, inspect the cannula exit sites for infection, and check the anticoagulation record and the neurological status at every review. [2] [3]
Severity and candidacy are judged not at the bedside alone but at a multidisciplinary advanced heart-failure review. The team synthesises the clinical state, the serial echocardiographic function, the laboratory markers of end-organ function (renal, hepatic, the lactate), and the catheterisation data — above all the pulmonary vascular resistance — into a decision about listing for transplantation and the device strategy. The bedside role of the general paediatrician or registrar is to recognise refractory failure early, to escalate to the advanced centre, and to support the child and family through the assessment. [4] [8]
Investigations
Echocardiography is the central investigation throughout the pathway. Before a device it defines the structural lesion, the chamber sizes, the ejection fraction, the valve competence and an estimate of pulmonary pressure; during support it confirms that the device is unloading the ventricle adequately (the ventricle should be decompressed and the aortic valve may open intermittently depending on the support level); and after transplantation it monitors graft function and screens for rejection and pericardial effusion. A falling ejection fraction with progressive dilation on serial echoes is the marker of a ventricle moving toward refractory failure. [4] [8]
Cardiac catheterisation is essential for transplant candidacy because it measures the pulmonary vascular resistance. A fixed, high pulmonary vascular resistance predicts a high risk of donor right-heart failure after transplantation and, above a threshold, contraindicates orthotopic transplantation. Serial catheterisation is used to track resistance, and a ventricular assist device is often placed in part to unload the pulmonary circulation and bring the resistance back below the transplant threshold. Blood tests quantify end-organ function (renal, hepatic, full blood count), the lactate and acid-base status, and the virological and immunological profile that frames post-transplant immunosuppression. [4] [8]
Cross-sectional imaging and cardiac magnetic resonance add detail in selected cases — tissue characterisation in myocarditis or cardiomyopathy, and anatomical planning in complex congenital disease — and computed tomography is used to screen for cardiac allograft vasculopathy and to image the device and cannulae when complications are suspected. Tissue diagnosis matters acutely for rejection: endomyocardial biopsy remains the gold standard for diagnosing cellular rejection in the transplanted heart, and it is performed on a surveillance schedule in the first year and whenever rejection is suspected clinically. [8]
Management — Resuscitation
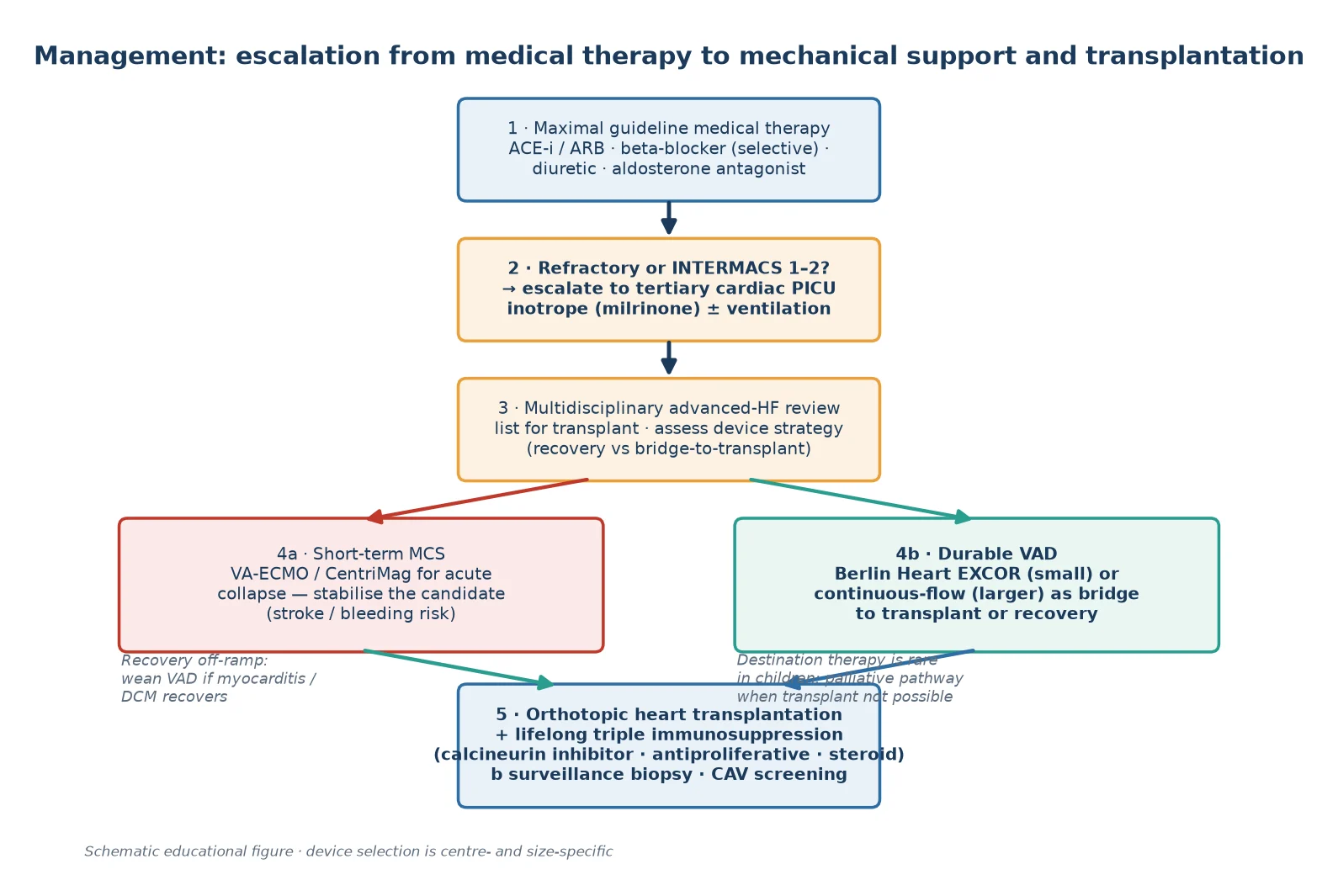
The resuscitation scenario is the child presenting in critical cardiogenic shock — the INTERMACS profile 1 patient — who is deteriorating despite inotropes. The priority is to secure the airway and breathing, restore perfusion, and move to short-term mechanical circulatory support before irreversible end-organ death. Assess ABC, perfusion and work of breathing, send a gas and lactate, and treat reversible drivers (arrhythmia, fever, anaemia) in parallel. Give oxygen, and select a vasoactive agent by the cause — milrinone for a low-output state — while avoiding indiscriminate fluid loading that worsens the failing ventricle. [6]
When low output persists despite resuscitation and inotropes, escalate to short-term mechanical circulatory support, most often venoarterial extracorporeal membrane oxygenation. VA-ECMO restores systemic perfusion and oxygenation rapidly and is the stabilising bridge used in the sickest children — the 'crash-and-burn' profile 1 patient — buying time to define the cause, to assess candidacy, and to decide between recovery, a durable device and transplantation. ECMO is not a destination: it carries its own risks of bleeding, thrombosis, infection and neurological injury, and the aim is to transition the recovering or listed child to a durable device or a transplant within days to a short number of weeks. [3] [5]
Heparin (anticoagulation on mechanical circulatory support)
Loading dose
Weight-based unfractionated heparin infusion titrated to institutional target (commonly 75 units/kg bolus then 20 units/kg/hour infusion, adjusted to anti-Xa or APTT)
Maintenance dose
Continuous infusion titrated to local anticoagulation protocol; transition to warfarin or antiplatelet therapy for durable support
The single most important resuscitation principle is that short-term support is a bridge to a decision, not a destination. The child stabilised on ECMO is assessed for recovery, for candidacy for a durable device, and for transplant listing, and is moved off ECMO — by recovery, by conversion to a durable VAD, or by transplantation — before ECMO complications accumulate. Indiscriminate or prolonged ECMO without an exit strategy is the failure mode to avoid. [5]
Immediate management of the child in critical cardiogenic shock
Assess ABC, perfusion, work of breathing; send gas, lactate, troponin, FBC, electrolytes, renal and hepatic function
Give titrated oxygen and select an inotrope by the cause (milrinone for low output); treat any arrhythmia, fever or anaemia
Escalate to short-term mechanical circulatory support (VA-ECMO) if low output persists despite inotropes
Obtain urgent echocardiography to define pump function and structural status
Treat reversible causes in parallel (rate control for tachyarrhythmia; exclude sepsis and metabolic disease)
Convene the advanced heart-failure team to assess recovery, durable-device candidacy and transplant listing
Define the ECMO exit strategy early: recovery, conversion to durable VAD, or transplantation
Management — Definitive & Stepwise
Definitive management is the durable ventricular assist device and transplantation pathway. Once a child is stabilised and judged refractory to medical therapy, the advanced heart-failure team decides the device strategy. For the smallest infants and children the durable option is the paracorporeal pulsatile Berlin Heart EXCOR, the device whose bridge-to-transplant role across US children was established by the Almond cohort. For larger children and adolescents, miniaturised continuous-flow implantable pumps are now the modern durable option, and they have changed the landscape by extending reliable longer-term support to patients who previously had no durable continuous-flow device. [1] [11]
The strategic goal of the device frames everything that follows. Bridge to transplantation is the most common strategy: the device keeps the child alive and reverses end-organ injury until a donor organ is available, and registry data show that a substantial majority of paediatric VAD recipients are successfully bridged to transplant. Bridge to recovery is reserved for myocarditis and selected cardiomyopathies in which the myocardium is expected to heal, allowing the device to be weaned and removed — this is the strategy that spares a child transplantation entirely. Bridge to candidacy is used for the child who needs end-organ recovery before listing is even possible, and destination therapy, common in adults, remains uncommon in children. [1] [5]
Transplantation is the definitive therapy. Allocation policy shapes waiting time and urgency: in the United States the 2016 paediatric heart allocation policy change altered waiting times and prioritisation, and registries track how such changes shift who is transplanted and how long candidates wait. The donor heart is implanted as an orthotopic graft, and the recipient then begins lifelong immunosuppression, typically a calcineurin inhibitor (tacrolimus or ciclosporin) together with an antiproliferative agent (mycophenolate or azathioprine) and a corticosteroid taper. When transplantation is not possible — because of irreversible pulmonary vascular disease, comorbidity or donor unavailability — a palliative care pathway is built with the family around symptom control and quality of life. [8] [12]
[1] [5]Specific Subtypes & Scenarios
The infant with a dilated cardiomyopathy on a Berlin Heart EXCOR is the archetype of the durable-bridge scenario. The child presents with refractory pump failure, is stabilised, and receives a paracorporeal pulsatile device sized to the patient; the device unloads the ventricle, restores nutrition and growth, and supports the child through the wait for a donor heart. The Berlin Heart EXCOR with ACTION post-approval surveillance data and the earlier Almond cohort established that the device can bridge infants and small children to transplantation, with the major limitation being its complication profile — above all stroke and infection. [1] [9]
Acute myocarditis is the scenario in which a bridge-to-recovery strategy must be kept open. A previously well child deteriorates rapidly to low output, is stabilised on short-term support or a durable device, and the ventricle — if it is going to recover — often does so over the first weeks of unloading. The decision to wean and explant the device, versus to proceed to transplantation, is made on serial echocardiographic recovery of function, and it is one of the most consequential judgements in paediatric mechanical support, because recovery spares the child a lifetime of immunosuppression. [4] [6]
The failing Fontan circulation is the most complex congenital scenario. A child who has undergone single-ventricle palliation develops a failing Fontan with protein-losing enteropathy, plastic bronchitis, arrhythmia or ventricular dysfunction, and transplantation is often the only durable solution. Mechanical support of the failing Fontan is technically demanding — the anatomy and the passive pulmonary circulation complicate device placement — and these children are among the highest-risk transplant candidates, which is why they are managed only in expert centres. Donor management to optimise the paediatric donor heart, summarised in international consensus guidance, is the other side of the equation: expanding the usable donor pool is central to shortening waiting times for these candidates. [4] [7]
Across Australia, New Zealand and the United Kingdom, paediatric heart transplantation and durable mechanical circulatory support are delivered through a small number of designated national centres, with retrieval networks that bring refractory children from regional and remote settings to the tertiary service. Listing thresholds, donor allocation and device protocols are set by the national cardiac and transplant services, and shared-care follow-up keeps the local paediatrician connected to the transplant team. In ANZ, donor organ availability and geographic distance shape waiting times and retrieval logistics, and adolescent transition to adult heart-failure and transplant care is planned and structured over the teenage years. [8] [11]
Complications & Pitfalls
The complications of mechanical circulatory support are the price of keeping a child alive on a device, and they dominate the experience of support. Stroke is the leading and most feared complication of the Berlin Heart EXCOR and other paediatric devices and a leading cause of death on support; the PediMACS stroke analysis quantified its burden and reinforced the centrality of anticoagulation management. Infection — of the driveline, the pump pocket or the bloodstream — is the other major morbidity, alongside bleeding from anticoagulation, haemolysis, pump thrombosis and the neurological and renal consequences of micro-thromboembolism. [2] [10]
The complications of transplantation are the consequences of a denervated graft and lifelong immunosuppression. Acute cellular and antibody-mediated rejection occur most often in the first year and are detected on surveillance endomyocardial biopsy and treated with augmented immunosuppression. Cardiac allograft vasculopathy — a diffuse, immunologically driven intimal proliferation of the graft vessels — is the leading cause of late graft loss and may present with silent ischaemia or sudden death, which is why transplanted children undergo lifelong surveillance. Post-transplant malignancy, notably post-transplant lymphoproliferative disease driven by Epstein-Barr virus, and the renal toxicity of calcineurin inhibitors complete the long-term burden. [4] [8]
The pitfalls are about timing and candidacy. The first is the timing pitfall: escalating too late, after irreversible end-organ or pulmonary vascular injury, when transplantation is no longer possible or outcomes are poor. The second is the candidacy pitfall: failing to exclude a reversible cause (a tachycardia-induced cardiomyopathy) before listing, or proceeding to transplantation when a bridge-to-recovery strategy would have allowed the myocardium to heal. The third is the anticoagulation pitfall: under-anticoagulation invites pump thrombosis and stroke, while over-anticoagulation invites catastrophic bleeding, and the narrow therapeutic window demands specialist management and a low threshold to investigate any change. [3] [10]
Prognosis & Disposition
The prognosis of paediatric heart transplantation is favourable in the medium term. International registry data show that a substantial proportion of paediatric recipients survive beyond ten years, with survival highest in recipients transplanted for cardiomyopathy and in stable (lower-INTERMACS) candidates. The graft carries a continuous attrition from cardiac allograft vasculopathy and the long-term consequences of immunosuppression, which is why lifelong surveillance and the eventual transition to adult transplant care are integral to the pathway. Retransplantation is an option for selected late graft failure but carries its own risks. [8]
The prognosis on a ventricular assist device is dominated by the complication profile and the urgency at implant. A stable, lower-INTERMACS child bridged electively with a durable device has substantially better survival to transplant than a profile-1 child placed on a device in extremis, which is why short-term stabilisation with ECMO before a durable device improves outcomes. Registry data from PediMACS and ACTION report survival to transplant across the supported population, and the post-approval surveillance of the Berlin Heart EXCOR has refined the understanding of its real-world performance and risks. [5] [9]
Disposition follows the severity. Every child with refractory or advanced heart failure is referred to a tertiary paediatric advanced heart-failure and transplant centre for assessment, device strategy and listing. A child on a device is managed in a tertiary paediatric intensive care or specialised cardiac unit with the multidisciplinary team; a transplanted child is followed lifelong in the transplant service, transitioning to adult care in adolescence. The general paediatrician's role is early recognition of refractory failure, timely retrieval to the tertiary centre, and shared-care follow-up that keeps the child connected to both the local team and the transplant service. [4] [8]
Special Populations
The infant is the first special population. The smallest patients need the smallest devices, and the Berlin Heart EXCOR is the durable option that reaches down to neonates, which is why infant support is concentrated in expert centres with the surgical and perfusion expertise to manage the smallest cannulae and pump sizes. The risks of stroke and infection are amplified in the smallest patients, and the waiting time for a size-matched donor organ can be long, which is why infant bridging is among the most resource-intensive work in paediatric cardiology. [1] [9]
The child with congenital heart disease — particularly the failing Fontan — is the second and the most complex. The abnormal anatomy complicates device placement and the single-ventricle physiology alters the haemodynamics of support, so these children are among the highest-risk candidates for both device and transplantation. A multidisciplinary assessment that includes the surgical anatomy, the pulmonary vascular bed and the systemic venous circulation is essential, and the decision to support or transplant is made only in expert centres. [4] [7]
The adolescent with a transplanted heart or a device is the third and the most complex for adherence and transition. The immunosuppression regimen is demanding and its non-adherence is a leading cause of late rejection and graft loss, which is why adherence support is central to adolescent care. The transition to adult heart-failure and transplant services must be planned, structured and gradual, with attention to contraception and pregnancy counselling, because pregnancy carries substantial risk in a transplanted or device-supported patient. Psychological support, school engagement and peer relationships matter as much as the cardiac care. [8] [11]
The rural or remote child is the fourth. Distance from the transplant centre delays assessment, device placement and follow-up, so the strategy in rural and remote settings is built on a high index of suspicion in primary care, timely retrieval to the tertiary centre, and shared-care follow-up that keeps the child connected to both the local paediatrician and the transplant team. Telehealth and structured transition of care reduce the burden of distance on these families. [8]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric mechanical circulatory support and transplantation is anchored on the multicentre registry cohorts and the annual international transplant registry reports. The Berlin Heart EXCOR bridge-to-transplant cohort (Almond 2013) established the device's role in US children and defined its survival and complication profile. The PediMACS registry reports — the first (Rosenthal 2016), the second (Blume 2018) and the fourth (Morales 2020) annual reports — have progressively defined the characteristics and outcomes of paediatric VAD recipients across the United States, and the PediMACS stroke analysis (Niebler 2021) quantified the burden of the dominant complication. [1] [2] [3] [5] [10]
The ACTION network and post-approval surveillance have refined the real-world performance of the devices. The Berlin Heart EXCOR and ACTION post-approval surveillance study report (Zafar 2021) added contemporary outcome data, and the registry-overview perspective (Lichtenstein 2021) framed the shift toward miniaturised continuous-flow pumps that is extending durable support to larger children and adolescents. The international thoracic organ transplant registry report (Singh 2021) remains the definitive source for the characteristics and survival of paediatric heart transplant recipients, and the donor-management consensus (Zimpfer 2020) addresses the other side of the equation — optimising the usable donor pool. [8] [9] [11]
The guideline and policy landscape is completed by studies of how allocation shapes the pathway. The 2016 United States paediatric heart allocation policy change altered waiting times and prioritisation, and the subsequent analysis (Williams 2022) quantified its effect on how long candidates wait and who is transplanted. Across ANZ, the United Kingdom, Europe and North America, the consensus is uniform in principle: declare refractory failure early, stabilise the sickest with short-term support, bridge with a durable device chosen by the child's size, transplant before irreversible end-organ injury, and transition the adolescent to lifelong adult care. The detail of allocation, listing and device protocols varies by region and centre, but the central strategy is shared. [12] [8]
The unifying message across high-resource settings is that advanced paediatric heart failure is managed by escalating from medical therapy to a device and transplantation before irreversible end-organ injury. What varies regionally is the donor pool, the allocation policy, the waiting time, the distance families must travel, and the specific devices available — all of which shape the practical experience of the pathway without changing the underlying strategy. [8] [11]
Exam Pearls
Advanced paediatric heart failure — 'DEVICE-BT'
References
- [1]Almond CS; Morales DL; Blackstone EH; Turrentine MW; Imamura M; Massicotte MP; Jordan LC; Meyer DM; Das NA; Lorts A; Morales RS; Davies RR; Nikaidoh H; Muenzer JR; Rosenthal DN; Morell VO; Kanter KR; Mahle WT; Fraser CD Jr Berlin Heart EXCOR pediatric ventricular assist device for bridge to heart transplantation in US children. Circulation, 2013.PMID 23538380
- [2]Rosenthal DN; Almond CS; Jaquiss RD; Peyton CE; Auerbach SR; Gomes KM; Blume ED; Pediatric Interagency Registry for Mechanical Circulatory Support (PediMACS) Adverse events in children implanted with ventricular assist devices in the United States: Data from the Pediatric Interagency Registry for Mechanical Circulatory Support (PediMACS). J Heart Lung Transplant, 2016.PMID 27197775
- [3]Blume ED; VanderPluym C; Lorts A; Baldwin JT; Rossano JW; Morales DLS; Cantor RS; Miller MA; Stoddard G; Jaquiss RDB; Rosenthal DN; Kilic A; Auerbach S; Bano M; Bates A; Checcchia P; Fynn-Thompson F; Kirklin JK; PediMACS Investigators Second annual Pediatric Interagency Registry for Mechanical Circulatory Support (PediMACS) report: Pre-implant characteristics and outcomes. J Heart Lung Transplant, 2018.PMID 28965736
- [4]D'Addese L; Boyle G; Spencer R; Gauvreau K; Fynn-Thompson F; Blume E Pediatric heart transplantation in the current era. Curr Opin Pediatr, 2019.PMID 31335745
- [5]Morales DLS; Rossano JW; VanderPluym C; Lorts A; Cantor R; Stoddard G; Adachi I; Almond CS; Bano M; Barta RJ; Bhalla A; Birks EJ; Boyle GJ; Cheng JK; Dreyer WJ; Essa N; Furnary AP; Gurung KJ; Hibino N; Huang JY; John MM; Kanter KR; Kister SE; Kon ZN; Liou A; Maeda K; McDiarmid TN; Mettler BA; Nussbaum DP; Penaranda C; Pigula F; Polito JW; Potapov EV; Schmitz JW; Schowengerdt KO; Smith RP; Thacker LR; Tsui SSL; Uluer AZ; Watkins B; Watson N; Wearden PD; Zwischenberger JB; Koehl DA Fourth Annual Pediatric Interagency Registry for Mechanical Circulatory Support (Pedimacs) Report. Ann Thorac Surg, 2020.PMID 33039359
- [6]Lasa JJ; Guffey D; Rogers RS; Minard CG; Shamszad P; Cabrera AG; Knott-Craig CJ; Goyia CM; Heinle JS; Jefferies JL; Price JF; Mott AR Epidemiology and Outcomes of Acute Decompensated Heart Failure in Children. Circ Heart Fail, 2020.PMID 32301336
- [7]Zimpfer D; Sabol F; Bonatti J; Colah S; De Robertis F; Dimopoulos K; Fiane AE; Gustafsson F; Hartyanszky I; Kaulfersch C; Kiaii B; Kolsrud LIL; Lamm P; Lund LH; Mohacsi P; Musial R; Oliva V; Pereda D; Potapov E; Rega F; Sá MPBO; Schmitto JD; Strüber M; Teutenberg JJ; Veres G; Waraich M; Zeriouh M; Zuckermann A; Sander M Pediatric donor management to optimize donor heart utilization. Pediatr Transplant, 2020.PMID 32198844
- [8]Singh TP; Cherikh WS; Chambers DC; Harhay MN; Hayes D Jr; Potena L; Sadavarte A; Zuckermann A; Khush KK; International Society for Heart and Lung Transplantation The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Twenty-fourth pediatric heart transplantation report - 2021; focus on recipient characteristics. J Heart Lung Transplant, 2021.PMID 34420853
- [9]Zafar F; Castleberry C; Khan MS; Mehta V; Bryant R III; Dreyer WJ; Adachi I; Fraser CD III; Morales DLS; Lorts A Berlin Heart EXCOR and ACTION post-approval surveillance study report. J Heart Lung Transplant, 2021.PMID 33579597
- [10]Niebler RA; Ghanayem N; VanderPluym C; Lorts A; Adachi I; Bryant R III; Cantor R; Koehl D; Menon S; Bano M; Fraser W; Lasa JJ; Marstein J; Mehta V; Rizwan R; Miller MA; Rosenthal DN; Conway J; Morales DLS Stroke in pediatric ventricular assist device patients-a pedimacs registry analysis. J Heart Lung Transplant, 2021.PMID 33824064
- [11]Lichtenstein KM; Schweiger M; VanderPluym C; Conway J; Schmidt D; Thompson L; Bano M; Zimpfer D Pediatric ventricular assist device registries: update and perspectives in the era of miniaturized continuous-flow pumps. Ann Cardiothorac Surg, 2021.PMID 34159114
- [12]Williams RJ; Taddeo P; Al-Aklabi M; Conway J; D'Astous J; Dipchand AI; L'Heureux A; Mertens L; Porepa LF; Rossano JW; Simpson KE; Singh TP; VanderPluym C; West LJ; McCrindle BW Pediatric heart transplant waiting times in the United States since the 2016 allocation policy change. Am J Transplant, 2022.PMID 34897984