Paeds · cardiology
Cardiogenic shock and mechanical circulatory support
Also known as Cardiogenic shock · Pump failure · Low cardiac output syndrome · Mechanical circulatory support · Extracorporeal membrane oxygenation · Venoarterial ECMO · Ventricular assist device · Berlin Heart · ECPR
Fellowship guide to cardiogenic shock in children — the state where the heart cannot pump enough blood to perfuse the body, producing low cardiac output with congestion — and to the mechanical circulatory support that rescues the child who fails conventional therapy. The page covers the bedside distinction from other shock types, the cautious-fluid and inotrope resuscitation, the SCAI shock stages, the escalation to venoarterial extracorporeal membrane oxygenation and then a durable ventricular assist device, the four goals of support (bridge to recovery, transplant, candidacy and destination therapy), and the anticoagulation and complication burden of the devices.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The single idea that organises the topic is this: in cardiogenic shock the problem is the pump, so the answer is to support the pump while you find and fix the cause, and the device is what you reach for when drugs cannot. A child with fulminant myocarditis can arrest within hours of looking mildly unwell, and the intervention that reverses the course is not more fluid or a bigger inotrope dose — it is a machine that takes over the pumping. The discipline that saves these children is early recognition of the perfusion failure, restraint with fluid, and timely escalation to a centre that can deploy mechanical support. [9] [10]
This page covers the bedside distinction of cardiogenic shock from the other shock types, the pathophysiology that explains why the child spirals, the cautious-fluid and inotrope resuscitation, the SCAI shock stages, the escalation to extracorporeal membrane oxygenation and a ventricular assist device, and the anticoagulation and complication burden of the devices. It links to the myocarditis leaf for the commonest reversible trigger, the cardiomyopathies leaf for the durable-support substrate, and the duct-dependent congenital heart disease leaf for the neonatal prostaglandin rescue. [13] [1]
Overview & Definition
Cardiogenic shock is inadequate tissue perfusion caused by failure of the heart as a pump. The cardiac output falls, and because the ventricle cannot eject its filling volume, the pressures behind the heart rise. The child therefore shows two things at once: the forward signs of low flow (cold peripheries, weak pulses, a long capillary refill, oliguria and a rising lactate) and the backward signs of congestion (a raised jugular venous pressure, hepatomegaly, pulmonary oedema and a gallop rhythm). That combination — low output with congestion — is the bedside signature that separates cardiogenic shock from the other shock types. [2] [13]
The contrast matters because it changes the first action. In septic shock the child is often warm and the first move is to push in fluid. In cardiogenic shock the ventricle is failing, so pushing in fluid floods the lungs and the liver. The general paediatrician's job at the bedside is to spot the congestion, hold back on aggressive fluid, start an inotrope, and escalate the child who does not respond. [12] [11]
Mechanical circulatory support is the family of devices that take over the pumping function of the failing heart. They range from temporary devices that run for hours to weeks — venoarterial extracorporeal membrane oxygenation is the commonest — to durable ventricular assist devices that run for months to years while a child waits for transplant. Every device serves one of four goals: bridge to recovery, bridge to transplant, bridge to candidacy, or destination therapy. Fulminant myocarditis is the classic bridge to recovery; cardiomyopathy is the classic bridge to transplant. [6] [4]
Classification
You classify cardiogenic shock in two ways, and both change what you do. The first is the severity stage, which tells you how sick the child is and how urgently you must escalate. The second is the device category, which tells you what you can reach for when conventional support fails. The figure sets out both axes. [2] [6]
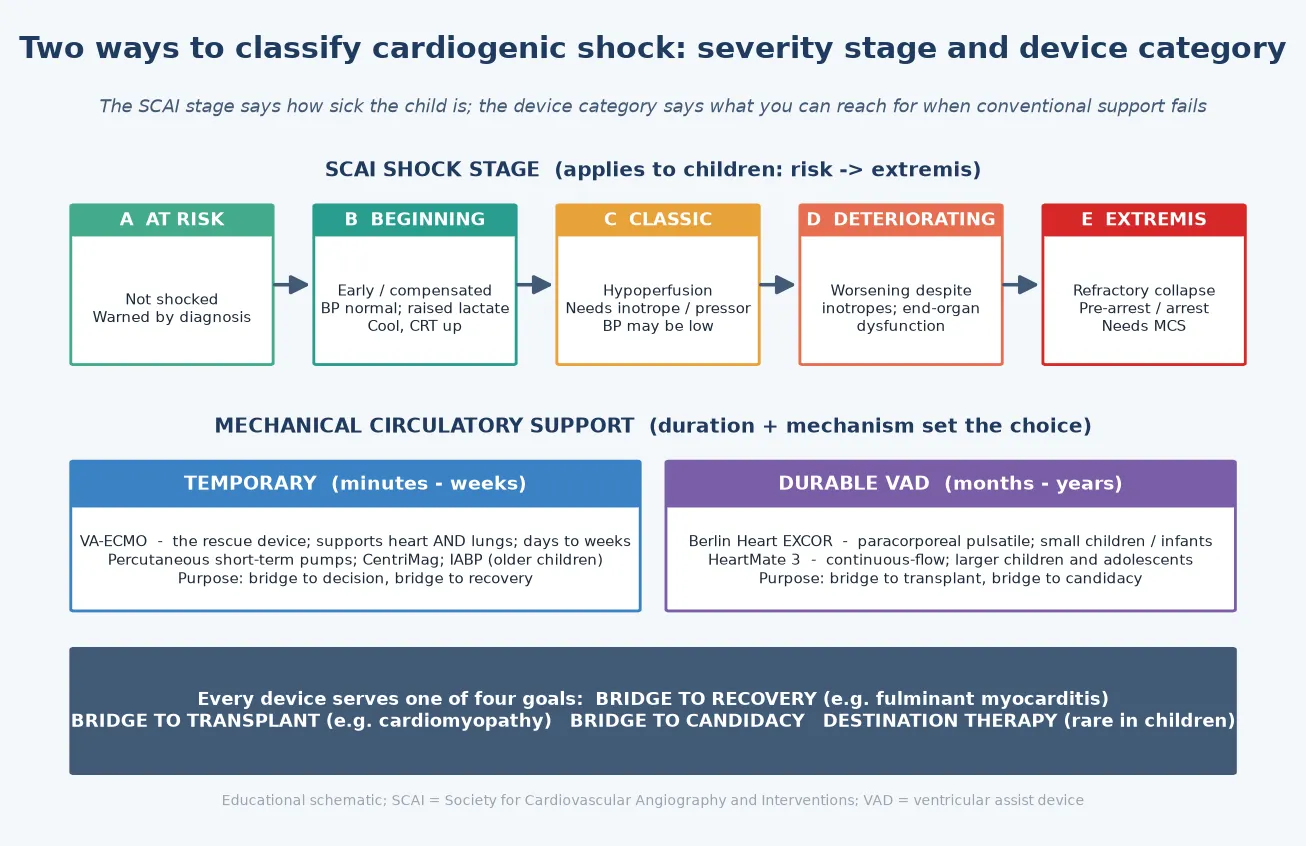
The severity axis comes from the SCAI classification, which the Society for Cardiovascular Angiography and Interventions developed for adults and which applies to children. Stage A is the child at risk — not yet shocked, but warned by the diagnosis, such as a child with myocarditis and a gallop. Stage B is the beginning of shock: compensated, with a normal blood pressure but early perfusion failure — a cool child with a rising lactate. Stage C is classic shock with overt hypoperfusion that needs an inotrope. Stage D is deterioration despite inotropes, with end-organ dysfunction. Stage E is extremis: refractory collapse, pre-arrest or arrest, needing mechanical circulatory support. The stages are a ladder, and the point of learning them is to climb it before the child reaches stage E. [2]
The device axis sorts support by how long it runs and how it works. Temporary support runs minutes to weeks and is dominated by venoarterial extracorporeal membrane oxygenation, which drains venous blood, oxygenates it, and returns it to the arterial system — so it supports both the heart and the lungs. Durable support runs months to years and means a ventricular assist device: the Berlin Heart EXCOR, a paracorporeal pulsatile pump, for small children and infants; a continuous-flow device such as the HeartMate 3 for larger children and adolescents. The choice between them is set by the child's size, the expected duration of support, and the goal. [6] [4]
Temporary support
- Runs minutes to weeks; venoarterial ECMO is the rescue device
- Supports both heart and lungs; drains venous, returns arterial blood
- Used as a bridge to decision, then to recovery
- Femoral or central cannulation; bedside or catheter-lab deployment
Durable VAD
- Runs months to years; allows rehabilitation and home discharge
- Berlin Heart EXCOR: paracorporeal pulsatile, for small children
- HeartMate 3: continuous-flow, for larger children and adolescents
- Used as a bridge to transplant or candidacy
Goals of support
- Bridge to recovery — fulminant myocarditis often recovers fully
- Bridge to transplant — cardiomyopathy is the usual substrate
- Bridge to candidacy — buy time until the child is listed
- Destination therapy — rare in children
Epidemiology & Risk Factors
Cardiogenic shock in children is uncommon but lethal when missed, and the causes cluster into a short list that the candidate must hold. The commonest reversible cause is fulminant myocarditis, in which a previously well child develops severe pump failure within days of a viral illness. Cardiomyopathy — dilated, and increasingly recognised genetic and metabolic forms — is the chronic substrate that decompensates into shock and usually needs a durable device and transplant. The post-cardiotomy child can fail to perfuse in the hours after cardiac surgery, the so-called low cardiac output syndrome. Sustained tachyarrhythmia and sepsis with myocardial depression complete the acute causes, and in the neonate the collapsed duct-dependent lesion is its own emergency. [13] [9]
The reason the epidemiology matters at the bedside is that the cause predicts the outcome and sets the goal of support. Fulminant myocarditis, despite its alarming presentation, often recovers near-normal function when the child is bridged with extracorporeal membrane oxygenation — so the device is a bridge to recovery. Cardiomyopathy usually does not recover, so the device is a bridge to transplant, and the scarcity of paediatric donor organs makes the durable ventricular assist device a necessary wait. The post-cardiotomy child is a bridge to myocardial recovery from the operative insult. Matching the cause to the goal is the skill. [15] [5]
Outcomes from paediatric cardiac extracorporeal membrane oxygenation depend on three things: the underlying diagnosis, the timing of deployment, and the centre's experience. Reversible causes do better than irreversible ones, and deploying support before irreversible liver and kidney failure sets in is the single biggest modifiable factor. Donor organ scarcity means that a meaningful proportion of children on durable support wait months, so the modern device must allow rehabilitation and even home discharge during the wait. [8] [3]
Pathophysiology
To understand why a shocked child spirals, picture the failing heart as a pump trapped in a feedback loop it cannot escape. The pump fails, so the cardiac output falls. The body reads the falling output as a threat and compensates the only way it knows how: it fires the sympathetic nervous system and the renin-angiotensin-aldosterone system. Heart rate rises, the blood vessels constrict, and the kidneys hold on to salt and water. Each of these was meant to protect the circulation — but each loads the failing ventricle further. The faster heart rate steals filling time, the vasoconstriction raises the afterload the weak ventricle must pump against, and the retained fluid floods the lungs and liver. Output falls further, the body compensates harder, and the spiral tightens. [13] [1]
The clinical face of the spiral is the combination of forward failure and backward failure. Forward failure is the low flow: the child becomes cold and mottled, the pulses weaken, the capillary refill lengthens, the urine output falls, the lactate rises, and a metabolic acidosis develops. Backward failure is the congestion: the failing left ventricle backs blood into the lungs and produces pulmonary oedema and respiratory distress, while the failing right ventricle backs blood into the systemic veins and raises the jugular venous pressure and the liver. The two travel together in cardiogenic shock, and their coexistence is what you look for at the bedside. [9] [13]
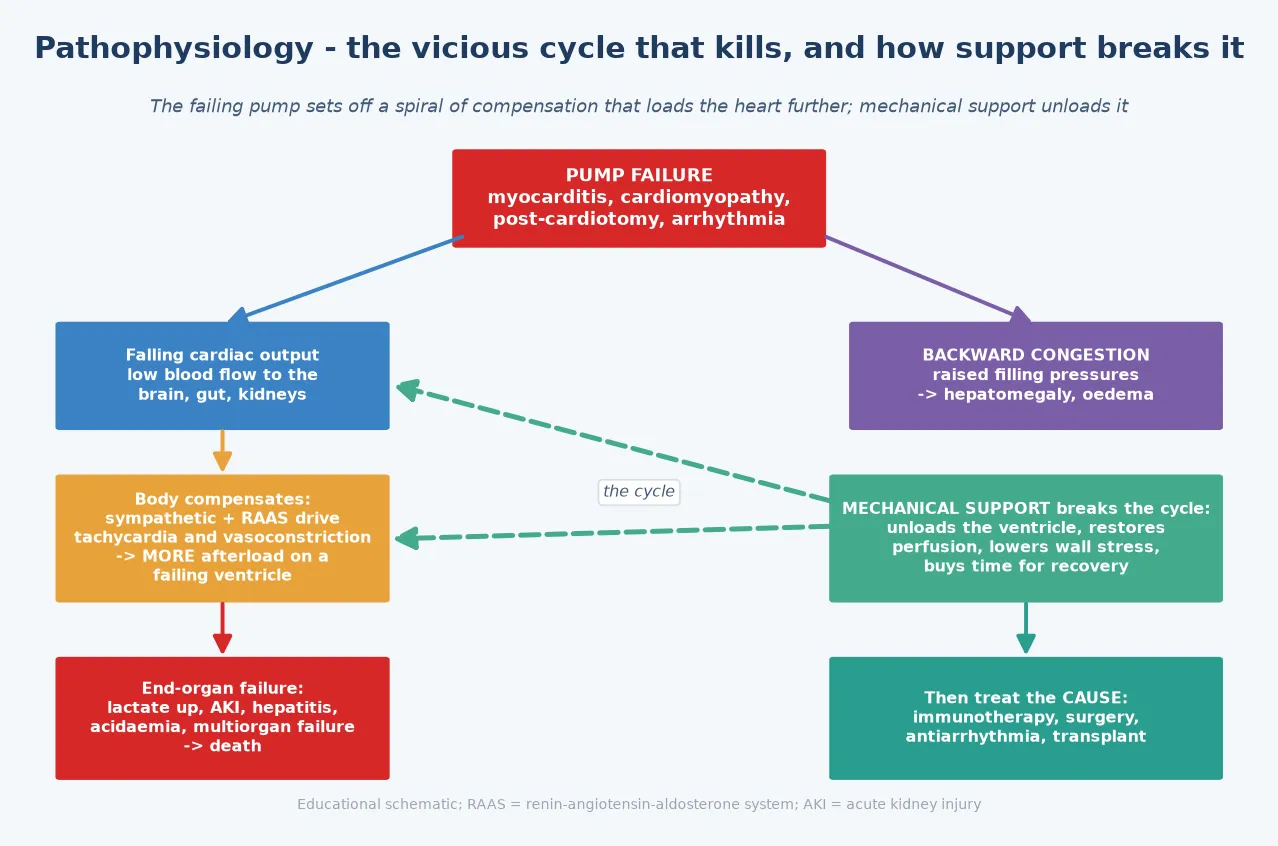
This is where mechanical circulatory support earns its place. The device does what the drugs cannot: it physically unloads the failing ventricle, takes over the pumping, restores systemic perfusion, and lowers the wall stress on the myocardium. The spiral stops, the end-organs reperfuse, and the heart is given time — to recover, in fulminant myocarditis, or to reach transplant, in cardiomyopathy. The drugs buy minutes; the device buys days to months. [7] [4]
One more point of physiology decides the bedside behaviour. A child can hold a normal blood pressure through a remarkable degree of shock, because intense vasoconstriction preserves the pressure even as the flow collapses. Hypotension is therefore a late and ominous sign, not an early one. The perfusion state — the skin, the pulses, the capillary refill, the urine output, the lactate — defines shock, and waiting for the blood pressure to fall before you act is the classic and dangerous error. [2] [14]
Clinical Presentation
The child in cardiogenic shock looks the way the physiology predicts: shut down, cold, and congested. Tachycardia is usually the first vital sign to change, followed by tachypnoea from the metabolic acidosis and the pulmonary congestion. The peripheries are cool and mottled, the pulses are weak and thready, and the capillary refill is prolonged beyond two seconds. The urine output falls — catheterise the child and measure it. The conscious level drifts, from irritability through lethargy to unresponsiveness. This is the compensated picture, and the blood pressure is often still normal. [9] [2]
Decompensation declares itself as the blood pressure finally falls, the lactate climbs, the metabolic acidosis worsens, and the peripheries become cold and white. The child is now in refractory territory, and every minute counts. The heart-failure signs sit alongside the shock signs and point to the cardiac cause: a third-heart-sound gallop, a liver enlarged edge, a raised jugular venous pressure, pulmonary crackles or grunting respiratory distress, and sometimes a murmur of structural or valvar disease. [13] [10]
The trigger tells you the cause. A viral prodrome followed by rapid collapse points to fulminant myocarditis. A child with a known cardiomyopathy who gets slowly worse over days is decompensating. A child who will not perfuse in the hours after cardiac surgery has post-cardiotomy low cardiac output syndrome. A sudden onset of instability with a rapid narrow-complex tachycardia points to a tachyarrhythmia. And a collapsed, pale, mottled neonate in the first days of life raises a duct-dependent congenital heart lesion until proven otherwise — a special case with its own rescue. [15] [1]
Differential Diagnosis
Shock has four mechanisms, and the bedside job is to work out which one this child has, because the first action differs for each. Distributive shock (septic, anaphylactic) is warm early, with a wide pulse pressure, and it responds to fluid boluses. Hypovolaemic shock (haemorrhage, severe dehydration) has no congestion and improves with volume. Obstructive shock (cardiac tamponade, tension pneumothorax, massive pulmonary embolism) needs relief of the mechanical obstruction. Cardiogenic shock has the congestion the others lack, and it does not tolerate fluid. The figure contrasts them at the bedside. [2] [9]
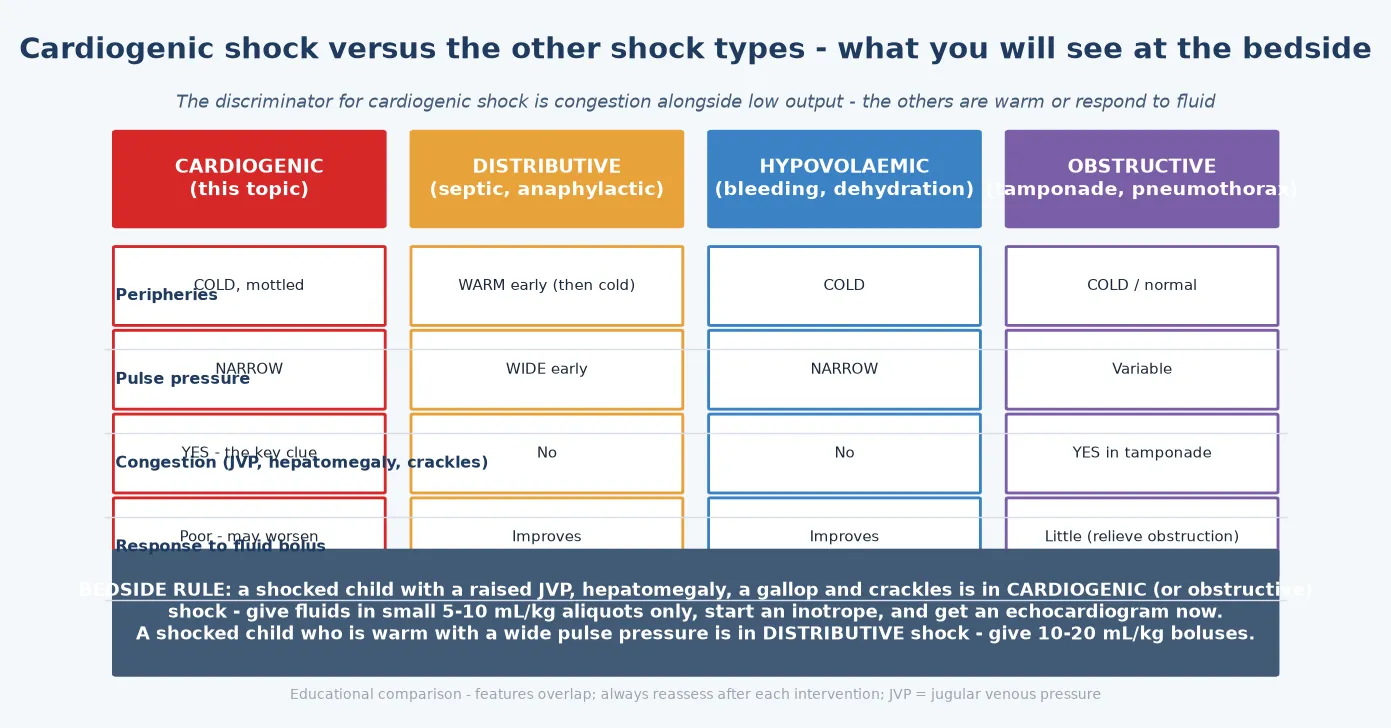
The discriminator that costs nothing is the jugular venous pressure and the liver. A shocked child with a raised venous pressure, an enlarged liver, a gallop and crackles is in cardiogenic shock (or obstructive, if tamponade is the cause). A shocked child who is warm and dry is in distributive shock, and the first move is fluid. Practising this one judgement — congested or not — is the highest-yield bedside skill in paediatric shock. [13] [12]
Before reaching for a device, exclude the causes that need a disease-specific rescue. A collapsed neonate with differential saturations or weak femoral pulses may have a duct-dependent lesion, and the rescue is prostaglandin E1 to reopen the ductus, not extracorporeal membrane oxygenation. A child with a pericardial effusion, a raised venous pressure, muffled heart sounds and pulsus paradoxus has tamponade, and the rescue is pericardiocentesis. A child in a sustained tachyarrhythmia needs cardioversion. Each of these is a treatment that relieves the shock without a machine, and missing them is a classic error. [1] [13]
Clinical & Bedside Assessment
The focused assessment rests on the paediatric assessment triangle and a disciplined look at perfusion. Look at the child first: the appearance, the work of breathing, and the colour of the skin tell you in seconds whether this is sick or not. Then measure the heart rate and the blood pressure with the correct cuff in all four limbs, feel the pulse volume and character, press and release the skin for the capillary refill, and note the skin temperature and any mottling. Catheterise the child and measure the urine output — it is the readout of renal perfusion. [9] [2]
Assess the end-organ perfusion directly. The conscious level, the urine output and the lactate are the three that matter, and the lactate trend is the single most useful marker that resuscitation is failing. A lactate that rises, or that fails to fall after an hour of treatment, is a red flag for refractory shock and should prompt escalation, not more of the same. The central venous oxygen saturation, if you have a line, should sit above sixty-five to seventy percent; a low value confirms inadequate oxygen delivery. [10] [12]
Then look for the heart. The gallop rhythm of a failing ventricle, the enlarged liver of systemic congestion, the raised jugular venous pressure, the pulmonary crackles of left-sided failure, and any murmur that points to a structural cause — these confirm that the shock is cardiogenic and sharpen the differential. Palpate the femoral pulses and compare the upper and lower limb blood pressures: weak femoral pulses or a pressure differential suggest coarctation or an interrupted arch, and in a collapsed neonate that means prostaglandin E1. [13] [1]
The discipline that protects the cardiogenic child is reassessment after every fluid bolus. Give five to ten millilitres per kilogram, then listen again for the gallop, feel again for the liver edge, and watch the oxygen saturation. New hepatomegaly, new crackles, a worsening gallop, or a falling saturation mark the point where further fluid is harmful. The failing ventricle drowns in volume, and the common iatrogenic injury in paediatric cardiogenic shock is the well-meaning bolus that floods the lungs. [12] [11]
Investigations
The bedside trio that anchors the diagnosis is the electrocardiogram, the chest radiograph and the echocardiogram. The electrocardiogram shows the rhythm and any ischaemic or axis change, and it catches the tachyarrhythmia that is the cause (or the consequence) of the shock. The chest radiograph shows the cardiomegaly and pulmonary oedema of pump failure and may reveal an alternative such as a tension pneumothorax. The echocardiogram is the key test: it defines the ventricular function, identifies a structural or valvar cause, excludes tamponade, and directly informs the decision about mechanical support. Get the echocardiogram early, at the bedside, before the child is moved. [1] [9]
The blood panel quantifies the perfusion failure and seeks the cause. Send a venous and an arterial blood gas for the lactate and the acid-base status — the lactate trend is the readout of resuscitation. Send troponin for myocardial injury and NT-proBNP for ventricular wall stress, electrolytes, renal and liver function (the end-organs), a full blood count, a coagulation screen, and blood cultures. In the right context, add a viral, metabolic and autoimmune screen, because the cause changes the goal of support. [9] [13]
Echocardiogram
- The key bedside test: ventricular function, structural cause, effusion
- Defines regional or global hypokinesis and valve regurgitation
- Guides the mechanical support decision (which side, which device)
- Directly informs cannulation strategy for ECMO
Lactate trend
- The single most useful marker of perfusion adequacy
- Rising or failing-to-fall lactate marks refractory shock
- Targeted by each step of the resuscitation
- Cheaper and faster than any imaging test
Cardiac catheterisation
- Measures filling pressures and cardiac index
- Confirms the haemodynamic indication for support
- Identifies pulmonary hypertension that changes device choice
- Reserved for the stable or supported child
The lactate trend and the central venous oxygen saturation are the dynamic markers that guide the adequacy of resuscitation, not a single blood pressure value. Cardiac catheterisation, in the child who is stable or already supported, measures the filling pressures and the cardiac index, confirms the haemodynamic indication for mechanical support, and identifies pulmonary hypertension that may change the device choice. The cause workup — viral polymerase chain reaction, metabolic studies, autoimmune serology — runs in parallel, because the cause sets whether the device is a bridge to recovery or to transplant. [10] [6]
Management — Resuscitation
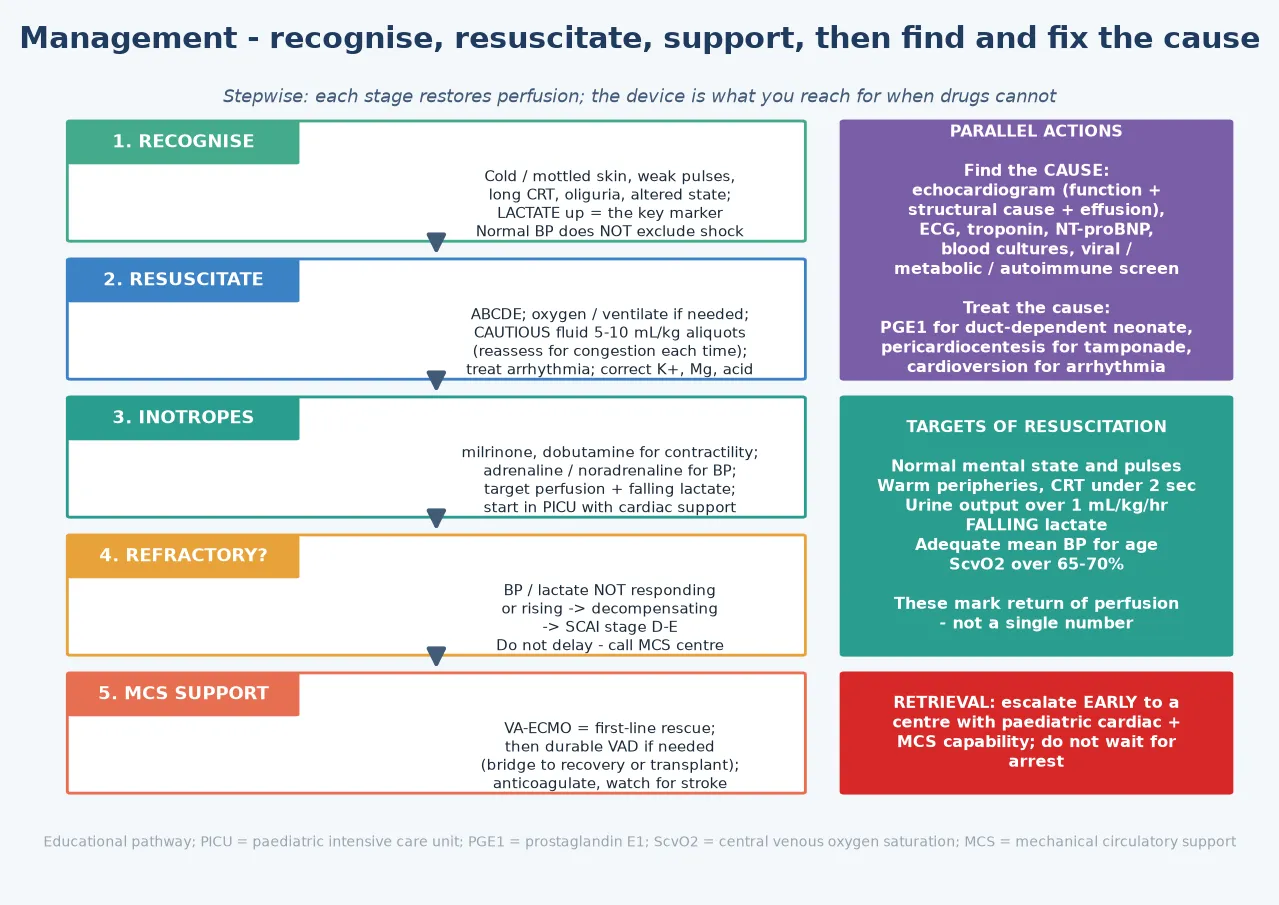
Resuscitation of the child in cardiogenic shock follows airway, breathing and circulation, with an honest judgement of how sick the child is. Give oxygen, support the airway and ventilate if the child is in respiratory failure or deep shock, and establish two reliable intravenous or intraosseous lines. From the first contact, make early contact with the paediatric intensive care and retrieval service, because these children deteriorate fast and the destination is a centre with cardiac and mechanical-support capability. [9] [10]
The fluid decision is where cardiogenic shock differs most from septic shock, and the candidate must hold the contrast. In septic shock you give ten to twenty millilitres per kilogram boluses. In cardiogenic shock you give five to ten millilitre per kilogram aliquots, and you reassess after each one for the signs of congestion — a new gallop, enlarging hepatomegaly, new crackles, a falling saturation. The failing ventricle cannot handle volume, and over-resuscitation converts a salvageable child into one drowned in pulmonary oedema. Treat the arrhythmia, correct the potassium and magnesium, and correct the acidosis. [12] [11]
Inotrope support drives the resuscitation of the low-output heart. Milrinone and dobutamine improve contractility and reduce afterload (they are inodilators), adrenaline and noradrenaline restore the blood pressure when it has fallen, and levosimendan, a calcium sensitiser, is an inodilator used in refractory low-output states. The agent and the dose are titrated to the perfusion state and the lactate trend, in a paediatric intensive care unit with cardiac monitoring. The aim is to restore perfusion, not to chase a pressure number. [11] [16]
When medical support fails to restore perfusion — the blood pressure or the lactate not responding despite adequate inotropes — the child is in refractory cardiogenic shock, and that is the trigger for mechanical circulatory support. The first-line device is venoarterial extracorporeal membrane oxygenation, deployed early. The evidence is consistent: earlier deployment, before irreversible end-organ failure, improves survival, and waiting for cardiac arrest before cannulating halves the chance of a good outcome. [10] [8]
Management — Definitive & Stepwise
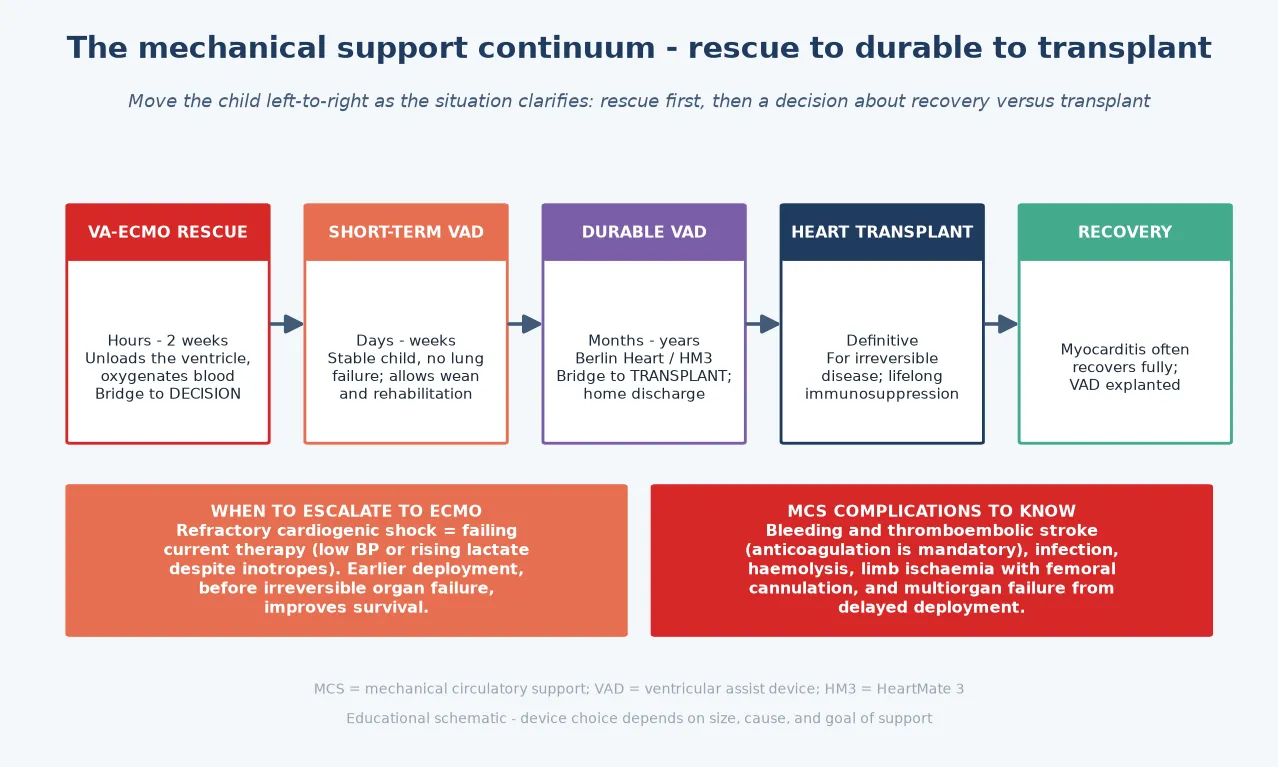
The definitive pathway is an escalation ladder, and the candidate must be able to climb it aloud. Recognise the shock. Resuscitate with oxygen, cautious fluid and arrhythmia control. Add inotropes in a paediatric intensive care unit. Identify refractory shock — failure to restore perfusion despite inotropes. Deploy venoarterial extracorporeal membrane oxygenation as the rescue. Then convert to a durable ventricular assist device for the child who needs longer support, and pursue recovery or transplant as the goal. The figure sets out the pathway with the parallel actions and the resuscitation targets. [6] [4]
The choice of durable device depends on the child's size and the expected course. The Berlin Heart EXCOR is a paracorporeal pulsatile pump, the device trialled in the prospective study of Fraser and colleagues, and it is the workhorse for small children and infants who are too small for an implanted continuous-flow pump. For larger children and adolescents, a continuous-flow device such as the HeartMate 3 is preferred because it is smaller, more durable, and allows the child to rehabilitate and go home while waiting for transplant. The match of device to child is a decision for the cardiac team, but the candidate must know the landscape. [3] [5]
Anticoagulation is mandatory for every mechanical support device, because blood in contact with artificial surfaces clots. It carries the twin risks that define the complication burden: bleeding and thromboembolic stroke. These are the dominant complications, alongside line and device infection, haemolysis, limb ischaemia from femoral cannulation, and multiorgan failure when deployment is delayed. Managing the anticoagulation is a daily intensive-care task, and the candidate must present the complication burden honestly when counselling a family. [7] [8]
Specific Subtypes & Scenarios
Fulminant myocarditis is the scenario that tests acute decision-making and the one most likely to appear in the exam. A previously well child develops severe pump failure and shock within days of a viral illness. The management is early venoarterial extracorporeal membrane oxygenation as a bridge to recovery, because the inflamed but acutely oedematous myocardium often recovers near-normal function once the storm is weathered. The pitfall is delaying support for biopsy confirmation; the recovery story does not apply to smouldering myocarditis that progresses to dilated cardiomyopathy. [15] [9]
Post-cardiotomy low cardiac output syndrome is the child who will not perfuse in the hours after cardiac surgery. The myocardium is stunned by the operative insult, and extracorporeal membrane oxygenation supports the circulation while it recovers. The prophylactic inotrope strategies reviewed by the Cochrane collaboration aim to prevent this state, but when it occurs, early support is the answer. [12] [8]
Cardiomyopathy decompensation is the chronic substrate that presents as acute shock. A child with known dilated cardiomyopathy, or one newly diagnosed, decompensates and needs a durable ventricular assist device as a bridge to transplant. The Berlin Heart EXCOR serves small children; a continuous-flow device serves larger children and adolescents, and allows rehabilitation and home discharge during the often-months-long wait for a donor organ. The candidate must frame the device as a bridge, not a destination, in the paediatric population. [3] [5]
The duct-dependent neonate and the disease-specific rescues must never be forgotten. A collapsed, pale neonate in the first days of life raises a duct-dependent congenital lesion, and the rescue is prostaglandin E1 to reopen the ductus. A child with tamponade needs pericardiocentesis, not a device. A child in a sustained tachyarrhythmia needs cardioversion. Each is a treatment that relieves the shock without mechanical support, and reaching for a machine when a drug or a needle was the answer is a failure of the differential. [1] [13]
Complications & Pitfalls
The untreated cardiogenic shock ends in multiorgan failure and death, which is why the single biggest modifiable factor is the speed of recognition and escalation. The complications of mechanical support itself are dominated by the anticoagulation burden: bleeding and thromboembolic stroke are the twin risks that define the device experience, alongside line and device infection, haemolysis, limb ischaemia from femoral cannulation, and multiorgan failure when deployment is delayed. A candidate who counsels a family must present these honestly. [7] [8]
The avoidable pitfalls cluster around three errors. Over-resuscitating with fluid floods the failing ventricle, worsens the pulmonary oedema and the right-heart strain, and is the commonest iatrogenic injury. Treating the blood pressure rather than the perfusion delays escalation, because a child can be in deep shock with a normal pressure until the end. Delaying mechanical support until irreversible organ failure halves the chance of survival, and so does missing a disease-specific rescue — prostaglandin for the duct-dependent neonate, pericardiocentesis for tamponade, cardioversion for the tachyarrhythmia — that does not need a device at all. [12] [10]
Prognosis & Disposition
The prognosis of paediatric cardiogenic shock is bimodal, and the candidate must hold both ends. When the cause is reversible — fulminant myocarditis, post-cardiotomy recovery — the child often survives to discharge with near-normal ventricular function, provided the support is deployed early. When the cause is irreversible — cardiomyopathy — the durable ventricular assist device bridges the child to transplant, and the prospective trial of the Berlin Heart EXCOR showed that the majority of supported children reach transplant. The outcome is worst when deployment is delayed into irreversible end-organ failure, or when the child arrests before cannulation. [8] [3]
Extracorporeal cardiopulmonary resuscitation — cannulating for extracorporeal membrane oxygenation during or immediately after cardiac arrest — is the last-chance rescue, and the systematic review evidence shows that a meaningful proportion of children survive to discharge, but far less than when support is deployed before arrest. This is the evidence behind the rule: escalate early, before the child arrests. [14] [10]
Disposition is a decision, not a location. Any child with refractory cardiogenic shock, or at high risk of deterioration, belongs in a paediatric cardiac intensive care unit with mechanical circulatory support and transplant capability. The general paediatrician's role is to recognise the shock early, begin the cautious resuscitation, and trigger the retrieval to such a centre without delay. In rural and remote areas, early telehealth coordination with the receiving cardiac centre and the retrieval service is part of the resuscitation, not an afterthought to it. [9] [13]
Special Populations
The neonate with a duct-dependent lesion is the special case where the rescue is a drug, not a device. A collapsed, pale, mottled neonate in the first days of life raises a ductal-dependent circulation until proven otherwise, and prostaglandin E1 reopens the ductus and restores systemic or pulmonary flow. Single-ventricle physiology needs special consideration if mechanical support is ever required, because the single ventricle and the shunt-dependent circulation change the cannulation strategy. [1] [13]
The child with complex congenital heart disease and the post-operative patient are the population in whom low cardiac output syndrome complicates the surgical course. Extracorporeal membrane oxygenation supports the circulation while the myocardium recovers from the operative insult, and the prophylactic inotrope strategies reviewed by the Cochrane collaboration aim to prevent the state. These children are managed in a cardiac intensive care unit with the surgical team embedded. [12] [8]
The adolescent with decompensated cardiomyopathy is on the pathway to a durable continuous-flow ventricular assist device and transplant. The continuous-flow devices allow rehabilitation and home discharge during the wait, which makes adherence and the transition to adult cardiac care central concerns. The candidate must frame the long support period as a time to optimise the child medically, nutritionally and psychologically for transplant. [3] [5]
The rural, remote and Indigenous child faces the dual burden of distance from a cardiac centre and the severity of the presentation. Early retrieval coordination, telehealth involvement of the receiving cardiac intensivist, and cultural support for the family are essential alongside the clinical resuscitation. The general paediatrician in a remote setting holds the child through the first critical hours, and the quality of that hold — the oxygen, the cautious fluid, the inotrope, the early call — sets the ceiling on what the cardiac centre can achieve. [9] [8]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric cardiogenic shock and mechanical circulatory support is anchored in several landmark documents. The SCAI clinical expert consensus statement on the classification of cardiogenic shock (Baran 2019) gives the severity stages that frame the escalation. The SCAI, ACC, HFSA and STS consensus on percutaneous mechanical circulatory support (Rihal 2015) sets the device principles and the four goals of support. The American Heart Association science advisory on chronic heart failure in children (Amdani 2024) frames the paediatric heart-failure substrate from which much shock arises. [2] [6]
The device evidence rests on the prospective trial of the Berlin Heart EXCOR paediatric ventricular assist device (Fraser 2012), the EXCOR North American experience (Fraser 2013, Almond 2011), the clinical practice guideline for extracorporeal circulation in cardiac and circulatory failure (Assmann 2022), and the paediatric extracorporeal membrane oxygenation outcomes data (Bembea 2023). The extracorporeal cardiopulmonary resuscitation systematic review (Esangbedo 2020) defines the last-chance rescue, and the fulminant myocarditis series (Feng 2026) shows the recovery outcome that makes early support worthwhile. [3] [14]
Regional practice aligns internationally on the cautious-fluid, early-escalation principle, but access shapes the reality. Australia and New Zealand run dedicated paediatric retrieval services (such as the perinatal and paediatric retrieval networks) that move the child to a cardiac extracorporeal membrane oxygenation centre, with telehealth coordination from the first call. The main controversies are the optimal timing of deployment, the choice of device in small children, the intensity of anticoagulation, and the equity of access to paediatric cardiac intensive care across remote and regional areas. [9] [10]
Exam Pearls
Hold one sentence for the viva: cardiogenic shock is low-output pump failure with congestion, treated with cautious fluid and inotropes and escalated to venoarterial extracorporeal membrane oxygenation when refractory; fulminant myocarditis is the commonest reversible cause and a bridge to recovery, while cardiomyopathy is a bridge to transplant. [2] [13]
State the frequently tested facts correctly. The SCAI stages run A to E, and stage E is the trigger for mechanical support. Fluid is five-to-ten millilitre-per-kilogram aliquots in cardiogenic shock, deliberately less than the ten-to-twenty of septic shock. The discriminator from other shock types is congestion alongside low output. Refractory shock — failure to restore perfusion despite inotropes — is the trigger for venoarterial extracorporeal membrane oxygenation, deployed early. The durable devices are the Berlin Heart EXCOR for small children and a continuous-flow device (HeartMate 3) for larger children. The four goals are bridge to recovery, transplant, candidacy and destination therapy. Anticoagulation is mandatory, and bleeding and stroke are the dominant complications. [12] [3]
The high-yield pairings: a child with a viral prodrome and rapid collapse has fulminant myocarditis (bridge to recovery); a known cardiomyopathy that decompensates needs a durable ventricular assist device (bridge to transplant); a collapsed neonate needs prostaglandin E1 for a duct-dependent lesion; a shocked child with a raised venous pressure, muffled heart sounds and pulsus paradoxus has tamponade (pericardiocentesis); a shocked child who is warm with a wide pulse pressure is in distributive shock (fluid boluses). These pairings do most of the diagnostic and management work in the written and clinical examinations. [1] [9]
References
- [1]Amdani S; Rossano JW; Wilmot I; et al Evaluation and Management of Chronic Heart Failure in Children and Adolescents With Congenital Heart Disease: A Scientific Statement From the American Heart Association. Circulation, 2024.PMID 38808502
- [2]Baran DA; Grines CL; Bailey S; et al SCAI clinical expert consensus statement on the classification of cardiogenic shock: This document was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), the Society for Cardiovascular Angiography and Interventions (SCAI), and the Society of Thoracic Surgeons (STS). Catheter Cardiovasc Interv, 2019.PMID 31104355
- [3]Fraser CD Jr; Jaquiss RD; Rosenthal DN; et al Prospective trial of a pediatric ventricular assist device. N Engl J Med, 2012.PMID 22873533
- [4]Fraser CD Jr; Jaquiss RD The Berlin Heart EXCOR Pediatric ventricular assist device: history, North American experience, and future directions. Ann N Y Acad Sci, 2013.PMID 23750961
- [5]Almond CS; Morales DL; Blackstone MH; et al Berlin Heart EXCOR Pediatric ventricular assist device Investigational Device Exemption study: study design and rationale. Am Heart J, 2011.PMID 21884857
- [6]Rihal CS; Naidu SS; Givertz MM; et al 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statement on the Use of Percutaneous Mechanical Circulatory Support Devices in Cardiovascular Care. J Card Fail, 2015.PMID 26036425
- [7]Assmann A; Boekstegers P; Brcic I; et al Use of extracorporeal circulation (ECLS/ECMO) for cardiac and circulatory failure -A clinical practice guideline. ESC Heart Fail, 2022.PMID 34811959
- [8]Bembea MM; Agus M; Akcan-Arikan A; et al Extracorporeal Membrane Oxygenation Characteristics and Outcomes in Children and Adolescents With COVID-19 or Multisystem Inflammatory Syndrome Admitted to U.S. ICUs. Pediatr Crit Care Med, 2023.PMID 36995097
- [9]Bhaskar P; Dhar R; Stephenson AL; et al Use of ECMO for Cardiogenic Shock in Pediatric Population. J Clin Med, 2021.PMID 33917910
- [10]Sachdev A; Chauhan S; Gupta D; et al Refractory pediatric cardiogenic shock: A case for mechanical support. Indian J Crit Care Med, 2016.PMID 27994387
- [11]Schranz D Pharmacological Heart Failure Therapy in Children: Focus on Inotropic Support. Handb Exp Pharmacol, 2020.PMID 31707469
- [12]Burkhardt BEA; Rücker G; Stiller B Inotropes for the prevention of low cardiac output syndrome and mortality for paediatric cardiac surgery patients. Cochrane Database Syst Rev, 2024.PMID 39588800
- [13]Rossano JW; Cherng An V; Lin KY; et al Heart failure in children: etiology and treatment. J Pediatr, 2014.PMID 24928699
- [14]Esangbedo ID; Biagas KV; Ma X; et al Pediatric Extracorporeal Cardiopulmonary Resuscitation: A Systematic Review. Pediatr Crit Care Med, 2020.PMID 32345933
- [15]Feng T; Zhao Y; Li L; et al Clinical outcomes of VA-ECMO in children with fulminant myocarditis: a single-centre case series. BMC Pediatr, 2026.PMID 42056983
- [16]Levin A Levosimendan. J Pediatr Intensive Care, 2013.PMID 31214430