Paeds · cardiology
Cardiovascular examination and murmur assessment
Also known as Paediatric cardiac auscultation · Heart murmur evaluation in children · Innocent vs pathological murmur · Paediatric precordial examination · Newborn cardiovascular assessment · Four-limb blood pressure and pulse oximetry screening
A fellowship approach to the paediatric cardiovascular examination and the heart murmur: perform a systematic inspection-palpation-auscultation sequence with four-limb blood pressure and pulse oximetry, recognise the benign fingerprint of an innocent murmur, identify the departures that mark a murmur as pathological, and resuscitate the duct-dependent neonate or the hypercyanotic spell before the echocardiogram confirms the lesion.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The mark goes to the candidate who treats the murmur as a question, not an answer. Most murmurs in children are innocent — found on a routine check in a thriving child, soft and short, and resolving with reassurance. The skill is not in naming every innocent murmur but in not missing the one that matters. The critical congenital heart lesion announces itself in one of two ways: cyanosis that does not correct with oxygen in the first days of life, or shock and acidosis as the duct closes. Both demand prostaglandin E1 before the anatomy is known, and both are missed most often because the murmur is quiet or absent at the worst moment. The cardiovascular examination is therefore an exercise in safe triage: recognise the benign fingerprint, recognise the red flags, and escalate. [2] [1]
Overview & Definition
The paediatric cardiovascular examination is a structured bedside assessment of a child's heart and circulation, performed to detect structural and functional heart disease and to characterise a murmur found incidentally. It has three inseparable parts: the general inspection of colour, breathing, growth and syndromic features, the focused palpation of the precordium and the peripheral and central pulses, and the systematic auscultation of the heart sounds and any added sounds in the five classical areas. The examination is incomplete without a four-limb blood pressure and a pulse oximetry reading taken in the right hand and a foot, because these two measurements alone detect the duct-dependent and shunt lesions that a stethoscope can miss. [1] [3]
A heart murmur is the sound of turbulent blood flow. Laminar flow is silent; when blood accelerates through a narrowing, crosses a shunt, or flows over a roughened surface, vortices form and the surrounding tissue vibrates, producing an audible murmur. The character of the murmur — its timing in the cardiac cycle, its location, its radiation, its intensity, and its quality — encodes the lesion that generated it. A fellow who reads the murmur by its character can predict the anatomy at the bedside, long before the echocardiogram confirms it. [6] [4]
The clinical importance of the examination sits in its prevalence. Murmurs are heard in up to half of all children at some point in childhood, and the overwhelming majority are innocent. The task of the clinician is therefore not to investigate every murmur but to separate, with the history and the bedside examination alone, the large benign majority from the small pathological minority that needs echocardiography and cardiology referral. Roughly one in a hundred and ten to one in a hundred and thirty infants is born with congenital heart disease, and a quarter of these have a critical lesion that presents in the neonatal period or early infancy — the population the examination and the pulse-oximetry screen exist to catch. [1] [2]
Classification
The classification that earns marks is the innocent-versus-pathological classification, because it converts the single finding of a murmur into a safe disposition. The benign majority share a recognisable fingerprint: a soft, short, systolic murmur of grade two or less, sitting at the left sternal edge, with normal first and second heart sounds, no radiation, and an asymptomatic child with normal pulses and a normal oxygen saturation. Any departure from this fingerprint — a louder, harsher, longer murmur, an abnormal heart sound, a thrill, a diastolic or continuous component, or any symptom or abnormal pulse — moves the murmur into the pathological column until proven otherwise. [1] [6]
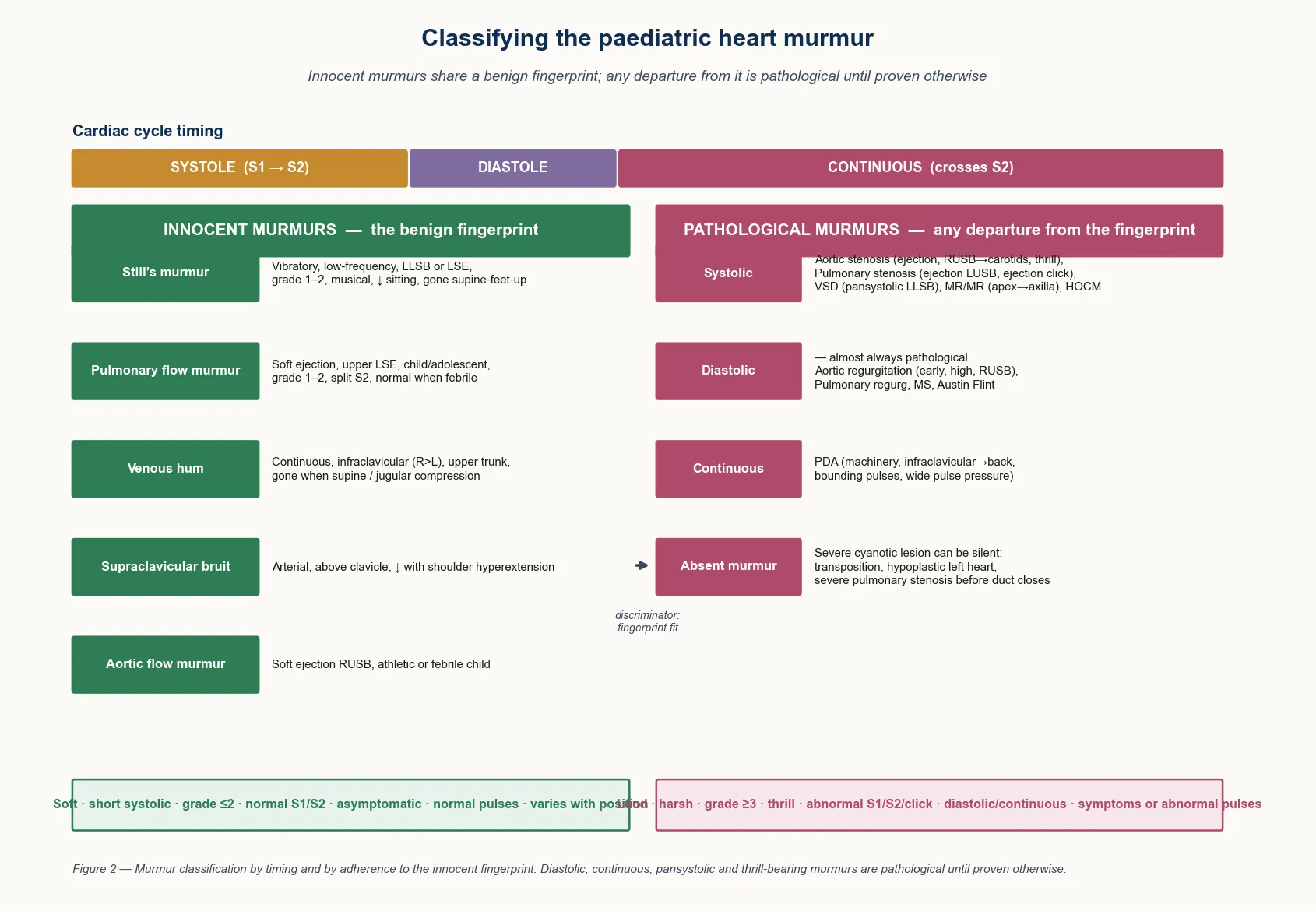
The innocent murmurs are the commonest murmurs of childhood and share a single mechanism — normal blood flowing at high velocity through a normal heart. The Still's murmur is the classic vibratory innocent murmur of early childhood, a low-frequency, musical, buzzing systolic sound best heard at the lower left sternal edge, that softens or disappears when the child sits forward. The pulmonary flow murmur is a soft ejection sound at the upper left sternal edge, common in febrile, anxious or athletic children. The venous hum is a continuous, soft murmur under the right clavicle, produced by flow in the jugular veins, that vanishes when the child lies flat or the jugular vein is compressed. The supraclavicular arterial bruit sits above the clavicle and softens with shoulder hyperextension. Each is recognised by its fit to the innocent fingerprint. [4] [5]
The pathological murmurs depart from the fingerprint in a way that points to the lesion. An ejection systolic murmur at the right upper sternal edge that radiates to the carotids, with a thrill and an ejection click, is aortic stenosis. An ejection systolic murmur at the left upper sternal edge with a click is pulmonary stenosis. A pansystolic murmur at the lower left sternal edge is a ventricular septal defect, and the same timing at the apex radiating to the axilla is mitral regurgitation. A continuous machinery murmur under the left clavicle, loudest in systole and bounding in quality, with a wide pulse pressure, is a patent ductus arteriosus. Any diastolic murmur in a child is, for practical purposes, always pathological. The fellow who maps timing to location to character can name the lesion at the bedside. [1] [5]
Epidemiology & Risk Factors
Heart murmurs are among the commonest findings in paediatric practice. A murmur is heard in around half of all children at some point during childhood, and the great majority are innocent — Still's murmur alone accounts for a large share of the systolic murmurs heard in pre-school and early school-age children. The prevalence peaks in the early school years, when routine checks and school-entry examinations surface murmurs that have been present but unnoticed. Congenital heart disease, by contrast, affects roughly eight to nine infants per thousand live births, and about a quarter of these infants have a critical lesion that declares itself in the neonatal period or early infancy. [1] [2]
The strongest risk factors for a pathological murmur are the company it keeps. A family history of congenital heart disease in a first-degree relative roughly doubles an infant's risk. Syndromic features on inspection carry a high yield: Down syndrome associates with atrioventricular septal defect and ventricular septal defect, Turner syndrome with coarctation of the aorta and bicuspid aortic valve, Noonan syndrome with pulmonary stenosis and hypertrophic cardiomyopathy, Williams syndrome with supravalvular aortic stenosis and peripheral pulmonary stenosis, and DiGeorge (22q11 deletion) with conotruncal anomalies including tetralogy of Fallot and interrupted aortic arch. A maternal history of diabetes, rubella, alcohol or teratogen exposure, or connective tissue disease, raises the background risk. [3] [8]
Recognition of the critical lesion is unevenly distributed across the population. In remote and Indigenous communities, and in migrant and refugee families, the interval between duct closure and presentation with shock or severe cyanosis can be shortened by distance from tertiary care, and the newborn pulse-oximetry screen may be the only chance to catch the lesion before collapse. A low threshold to measure four-limb blood pressure and pulse oximetry, and to start prostaglandin E1 on suspicion, is the equity response that closes the gap between a rural birth and a paediatric cardiology centre. [2] [11]
Pathophysiology
The pathophysiology of the murmur is the pathophysiology of turbulent flow. In the normal heart, blood moves in smooth, silent lamina. When a narrowing forces the same volume through a smaller orifice, the velocity rises, the flow breaks into vortices, and the surrounding tissue vibrates — the louder and harsher the turbulence, the greater the pressure gradient driving it. This is why a tight aortic stenosis produces a louder, harsher murmur than a mild one, and why the intensity of a murmur tracks the severity of the obstruction up to the point where the obstruction becomes so severe that flow falls and the murmur softens — the critical stenosis paradox the fellow should hold. [6] [1]
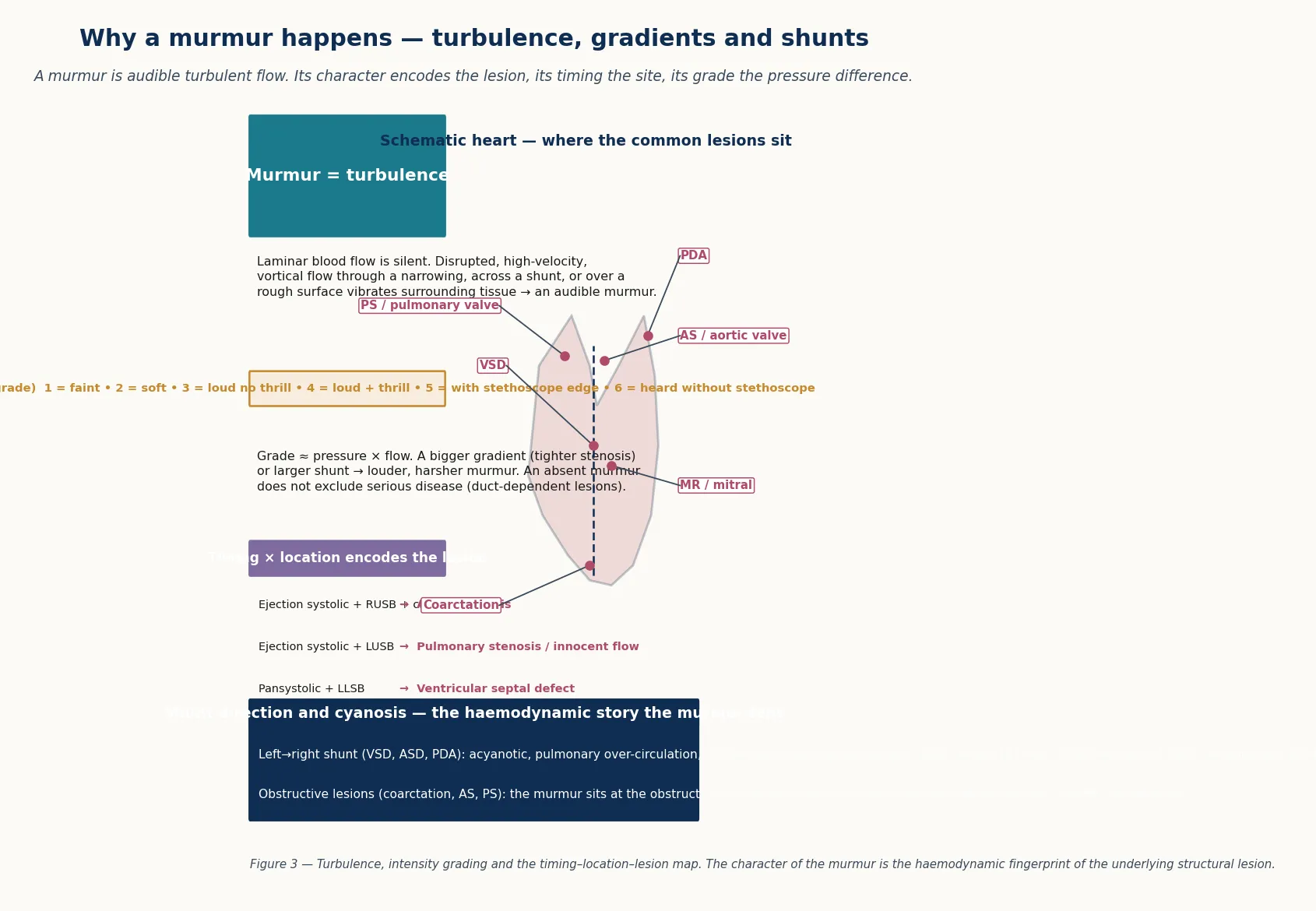
The timing of the murmur in the cardiac cycle encodes the site of turbulence. A systolic murmur sits between the first and second heart sounds: an ejection (crescendo-decrescendo) systolic murmur follows the pattern of ventricular ejection and points to a semilunar valve or an outflow-tract obstruction, while a pansystolic murmur that obscures the second sound points to flow from a high-pressure chamber to a low-pressure chamber throughout systole, as in a ventricular septal defect or mitral regurgitation. A diastolic murmur sits between the second and first heart sounds and points to flow into a ventricle during filling — aortic or pulmonary regurgitation, or mitral stenosis. A continuous murmur spans systole and diastole and points to a pressure gradient that persists through both, most classically a patent ductus arteriosus. [4] [6]
The haemodynamic consequences of the lesion drive the rest of the examination. A left-to-right shunt, as in a ventricular septal defect, overloads the pulmonary circulation, so the murmur is loud and the child may fail to thrive with recurrent respiratory infections. A right-to-left shunt, as in tetralogy of Fallot or transposition, desaturates the systemic blood, so the child is cyanotic and the murmur may be softer than expected because the obstruction limits outflow. An obstructive lesion, as in coarctation of the aorta, produces a pressure gradient that the body circumvents with collaterals, so the femoral pulses are weak and the blood pressure is high in the arms and low in the legs. The fellow who links the character of the murmur to the haemodynamics behind it can read the lesion from the bedside. [9] [8]
Clinical Presentation
The clinical presentation of a heart murmur falls into three archetypes that the fellow should be able to generate from the pathophysiology. The well child with an incidental murmur is the commonest: a thriving, asymptomatic child referred after a murmur is heard at a routine check, with a soft systolic sound at the left sternal edge, normal pulses, a normal saturation, and a fingerprint that fits an innocent murmur. The cyanotic neonate presents in the first hours to days of life with central cyanosis that does not correct with oxygen, tachypnoea, a varying murmur, and a low or falling saturation in the right hand or the foot. The acyanotic older infant or child presents with a loud, harsh or continuous murmur, often with a thrill, and sometimes with the stigmata of heart failure — sweating with feeds, tachypnoea, hepatomegaly, and failure to thrive. [1] [3]
The innocent murmur presents in its own characteristic ways. The Still's murmur is heard in children between two and seven years, a vibratory, buzzing, low-frequency systolic sound at the lower left sternal edge, softer when the child sits forward and louder when supine. The venous hum is heard in young children, a continuous soft sound under the right clavicle that disappears when the child lies flat or the ipsilateral jugular vein is compressed. The pulmonary flow murmur is heard at the upper left sternal edge in febrile or athletic children. Recognising these patterns in a well child with normal pulses and a normal saturation allows confident reassurance without echocardiography. [4] [7]
The pathological murmur presents with the symptoms of the underlying lesion. The infant with a ventricular septal defect presents with a pansystolic murmur at the lower left sternal edge and, if the defect is large, with heart failure over the first weeks as pulmonary vascular resistance falls and the shunt grows. The child with coarctation presents with weak or absent femoral pulses, an arm-to-leg blood-pressure gap, and sometimes hypertension or a murmur over the back. The child with tetralogy of Fallot presents with cyanosis and a systolic ejection murmur at the left sternal edge, and may have a hypercyanotic spell — a sudden deepening of cyanosis with irritability, tachypnoea and squatting. Each presentation carries its own red flag. [9] [8]
Why a hypercyanotic spell happens and why squatting helps
In tetralogy of Fallot, the right ventricular outflow obstruction fixes the resistance to pulmonary flow. Anything that lowers the systemic vascular resistance — crying, waking, fever, exertion — shunts more desaturated blood right-to-left across the ventricular septal defect, and the child becomes deeply cyanotic and distressed. Squatting, or the knee-to-chest position in an infant, raises the systemic vascular resistance, reduces the right-to-left shunt, and increases pulmonary blood flow, so the child self-corrects. This is why the knee-to-chest position is the first move in the hypercyanotic-spell bundle. [9] [12]
Differential Diagnosis
The differential depends on whether the child fits the innocent fingerprint or departs from it. For the well child with a fingerprint murmur, the practical differential is among the innocent murmurs themselves — Still's murmur against the pulmonary flow murmur, the venous hum and the supraclavicular bruit — distinguished by location, quality and the manoeuvres that abolish them. The discriminating move is always the same: confirm the normal heart sounds, the normal pulses, the normal four-limb blood pressure and the normal saturation, and document the fingerprint. [4] [7]
For the child whose murmur departs from the fingerprint, the differential runs by timing and location. An ejection systolic murmur at the right upper sternal edge radiating to the carotids is aortic stenosis; the same timing at the left upper sternal edge with an ejection click is pulmonary stenosis. A pansystolic murmur at the lower left sternal edge is a ventricular septal defect; the same timing at the apex radiating to the axilla is mitral regurgitation. An asymmetrical, harsh systolic murmur at the left lower sternal edge that increases with Valsalva is hypertrophic cardiomyopathy. A continuous machinery murmur under the left clavicle is a patent ductus arteriosus. Any diastolic murmur is, for practical purposes, pathological. [1] [5]
For the neonate, the differential of cyanosis is the differential that decides between the heart and the lungs. The hyperoxia test, though less used since the pulse-oximetry screen, helps in ambiguous cases: a saturation that does not rise on one hundred per cent oxygen points to a right-to-left shunt and a cyanotic cardiac lesion, while a rise points to a pulmonary cause. The key teaching point is that a cyanotic neonate with a normal or near-normal chest X-ray and a saturation that does not correct on oxygen has congenital heart disease until proven otherwise, and prostaglandin E1 is started before the echocardiogram. Differential cyanosis — a higher saturation in the right hand than in the foot — localises the right-to-left shunt to the duct, and reverse differential cyanosis points to transposition with pulmonary hypertension. [10] [2]
Clinical & Bedside Assessment
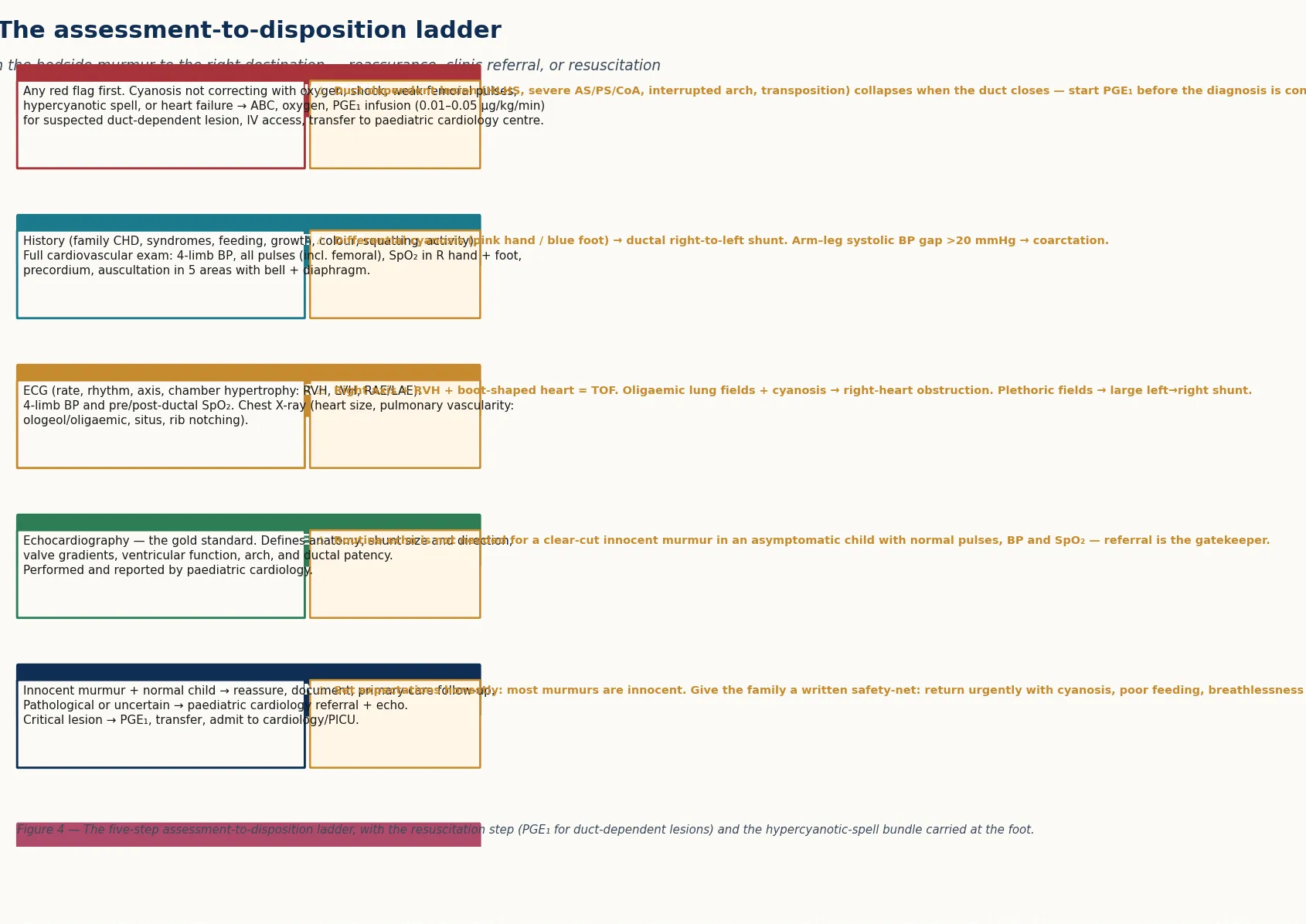
The bedside assessment has two speeds. In the cyanotic or shocked neonate, the immediate questions are the airway, the breathing, the circulation and the glucose, while the saturations and the blood pressure are measured and intravenous access is secured. A cyanotic infant who is not correcting on oxygen, or a collapsed infant with weak pulses and a metabolic acidosis, is a duct-dependent lesion until proven otherwise, and the assessment moves straight to prostaglandin E1 and transfer rather than waiting for the echocardiogram. In the elective presentation, the assessment is a careful history and a systematic examination that documents the features that will decide between reassurance and referral. [2] [11]
The examination sequence is fixed and the examiner listens for it in a short case. Begin with inspection: colour, work of breathing, the shape of the chest, the precordium for bulging or retraction, the fingers for clubbing, and the face and the hands for syndromic features. Move to palpation: the apex beat (site, diffuse or heaving), the right ventricular heave at the left sternal edge, any thrill over the precordium, the femoral and the brachial pulses together, and the abdomen for hepatomegaly. Then auscultate the five areas — aortic, pulmonary, Erb's point, tricuspid and mitral — first with the diaphragm for high-pitched sounds and then with the bell for low-pitched sounds, listening to the first and second heart sounds before any murmur. [1] [3]
The measurements that complete the examination are the ones that catch the lesions the stethoscope misses. Measure the blood pressure in the right arm and both legs to detect the arm-to-leg gap of coarctation or an interrupted arch; a systolic gap above twenty millimetres of mercury is significant. Measure the oxygen saturation in the right hand and a foot (pre- and post-ductal) to detect the ductal right-to-left shunt; a post-ductal saturation below ninety-five per cent, or a gap between the right hand and the foot above three per cent, warrants assessment for congenital heart disease. Plot the growth chart for failure to thrive, and take the feeding and exercise history for the stigmata of heart failure. The one-sentence problem representation that follows should name the child, the murmur's timing and location, and the red flags — for example, "a four-year-old with a soft systolic murmur at the left sternal edge, normal pulses and a normal saturation, fitting an innocent murmur." [3] [2]
Investigations
The investigation strategy is tiered and, in a child with a clear innocent murmur, may stop at the bedside. The first tier is the clinical fingerprint: a soft, short, systolic, grade-two-or-less murmur at the left sternal edge, with normal heart sounds, normal pulses, a normal four-limb blood pressure, a normal saturation, and an asymptomatic thriving child, needs no further investigation and is reassured and documented. The temptation to order an echocardiogram for every murmur drives cost and anxiety without improving outcome, because the recurrent-cardiology-evaluation data show that the great majority of these children are normal on echo. [7] [1]
The second tier settles the pathological or uncertain murmur. The electrocardiogram shows the rate, the rhythm, the axis and the chamber overload — right ventricular hypertrophy in tetralogy of Fallot and pulmonary stenosis, left ventricular hypertrophy in coarctation and aortic stenosis, and a superior axis in atrioventricular septal defect. The chest X-ray shows the heart size and the pulmonary vascularity: a boot-shaped heart with oligaemic lung fields in tetralogy of Fallot, a globular heart with plethoric fields in a large left-to-right shunt, and rib notching in older coarctation. The four-limb blood pressure and the pre- and post-ductal saturations are part of every work-up, not just the neonatal one. [3] [8]
The definitive test is the echocardiogram, performed and reported by paediatric cardiology. It defines the anatomy, the shunt size and direction, the valve gradients, the ventricular function, the aortic arch, and the ductal patency — everything needed to confirm the diagnosis and plan the management. The fellow's role is to recognise when to ask for it: the pathological murmur, the uncertain murmur, any red flag, or any abnormal first-tier test. The recognition that the echocardiogram is a cardiology investigation, requested through a referral rather than ordered as a screening test, is the disposition that protects the child and the service. [1] [4]
Management — Resuscitation
The resuscitation move is to keep the arterial duct open. A prostaglandin E1 (alprostadil) infusion at 0.01 to 0.05 micrograms per kilogram per minute reopens or maintains the duct in any neonate with a suspected duct-dependent lesion — hypoplastic left heart, severe aortic or pulmonary stenosis, coarctation or an interrupted arch, or transposition — and it is started before the echocardiogram confirms the anatomy. The common adverse effects are apnoea, hypotension, fever and irritability, so the child is monitored in a neonatal or paediatric intensive care setting and intubated early if apnoea develops. Securing intravenous access, giving oxygen, treating the metabolic acidosis, and transferring to a paediatric cardiology centre complete the resuscitation. [2] [11]
The hypercyanotic (tet) spell is the other resuscitation emergency in this topic, and it is treated with a bundle rather than a single drug. The knee-to-chest position raises the systemic vascular resistance and reduces the right-to-left shunt. High-flow oxygen reduces the hypoxic drive. An intravenous fluid bolus raises the preload. Morphine at around 0.1 milligrams per kilogram calms the child and reduces the sympathetic tone that drives the infundibular spasm. A vasoconstrictor such as phenylephrine raises the systemic vascular resistance and pushes blood into the lungs. A beta-blocker such as propranolol or esmolol relaxes the infundibular spasm. If the spell is refractory, prostaglandin E1, anaesthesia and surgery enter the ladder. The bundle is given together, not in sequence, and the child is admitted to a paediatric intensive care setting. [12] [9]
Resuscitation is not finished until the child is in the right place with the right team. The duct-dependent neonate is transferred to a paediatric cardiology centre on prostaglandin E1, intubated if apnoeic, with a clear handover that names the working diagnosis, the prostaglandin dose, the glucose and the acid-base status. The hypercyanotic spell is admitted to a paediatric intensive care setting with the cardiology team involved. The fellow who treats the resuscitation as a system — recognise, open the duct, bundle the spell, transfer — is the one who closes the gap between the bedside and the definitive care. [11] [2]
Management — Definitive & Stepwise
The definitive management of a murmur is, first and foremost, a decision: does this child need echocardiography and cardiology referral, or does this child need reassurance? For the child with a complete innocent fingerprint, the answer is reassurance, documentation, and primary-care follow-up. The data on recurrent cardiology evaluation for innocent murmurs show that the great majority of these children are normal on echo, that the echo adds cost and waiting without changing the outcome, and that the confident clinical call is both safer and more efficient. The written record should name the innocent murmur, the normal pulses and saturation, the safety-net, and the plan to return if symptoms develop. [7] [1]
For the child with a pathological or uncertain murmur, the definitive path is referral to paediatric cardiology and an echocardiogram. The management that follows is then the management of the underlying lesion — surgical or catheter repair of the structural defect, medical management of heart failure, or surveillance — and it is led by the cardiology team. The fellow's role at the point of referral is to give a clear, structured handover: the age, the murmur's timing and location, the red flags, the four-limb blood pressure and the saturation, and the working diagnosis. The structured handover is the single intervention that most reliably moves the child from the bedside to the right service. [1] [4]
The safety-net is the part of the management that closes the loop. Every family who leaves with a diagnosis of an innocent murmur is given a written instruction to return urgently if the child develops cyanosis, poor feeding, breathlessness, sweating with feeds, or poor growth — the symptoms that signal a lesion that was missed or that has progressed. The safety-net is not a hedge against a poor examination; it is the explicit contract that the benign call is reversible if the clinical picture changes. The fellow who frames the disposition around the safety-net, the structured referral, and the prostaglandin-for-the-duct-dependent-neonate rule earns the mark that separates a competent from a thoughtful candidate. [1] [7]
Specific Subtypes & Scenarios
The duct-dependent neonate is the scenario that the whole examination exists to catch. The lesion — hypoplastic left heart, severe aortic or pulmonary stenosis, coarctation or an interrupted arch, or transposition — is survivable in utero because the arterial duct carries the blood the heart cannot route, and the infant looks well at birth and collapses as the duct closes over the first hours to weeks. The presentation is cyanosis that does not correct with oxygen, or shock with a metabolic acidosis, and the murmur may be soft or absent. The management is prostaglandin E1, oxygen, intravenous access, correction of the acidosis and the glucose, and transfer to a paediatric cardiology centre. The pulse-oximetry newborn screen exists precisely to catch this infant before collapse. [2] [11]
Tetralogy of Fallot is the commonest cyanotic congenital heart lesion after the neonatal period, and the one most likely to present with a hypercyanotic spell. The four features — ventricular septal defect, overriding aorta, right ventricular outflow obstruction and right ventricular hypertrophy — produce a cyanotic child with an ejection systolic murmur at the left sternal edge that softens during a spell as less blood reaches the lungs. The spell is treated with the knee-to-chest bundle and, if refractory, with prostaglandin E1, anaesthesia and surgery. The long-term management is complete surgical repair in infancy, and the prognosis is excellent with modern surgery. [9] [12]
In Australia and New Zealand, coarctation is detected through the newborn examination, the pulse-oximetry screen, and the four-limb blood pressure that every fellow should perform at the baby check. The critical coarctation presents in the neonatal period with shock as the duct closes; the less severe forms present later with hypertension, a murmur over the back, or radio-femoral delay. Surgical repair is centralised to the paediatric cardiac centres, and the post-repair child is followed long-term for re-coarctation and hypertension. Naming the local pathway — the baby check, the four-limb blood pressure, the pulse-oximetry screen, and the retrieval partnership to the cardiac centre — earns the mark in a long case. [8]
The venous hum and the Still's murmur are the two innocent murmurs most often confused with a pathological lesion, and recognising them is the everyday skill of the general paediatrician. The venous hum is continuous and sits under the right clavicle, so it can be mistaken for a patent ductus arteriosus; the discriminator is that it vanishes when the child lies flat or the jugular vein is compressed, and the pulses and the saturation are normal. The Still's murmur is vibratory and low-frequency, and sits at the lower left sternal edge; it softens when the child sits forward, and it carries the innocent fingerprint throughout. The fellow who can demonstrate the manoeuvre that abolishes the venous hum earns the mark in a short case. [4] [5]
Complications & Pitfalls
The complications divide into those of the missed lesion and those of the over-investigated child. Missing the lesion is the serious harm: a duct-dependent neonate sent home as well, a coarctation labelled as a normal murmur at the baby check, or a hypercyanotic spell dismissed as a breath-holding attack. The protective moves are the four-limb blood pressure at every baby check, the pre- and post-ductal saturation, a low threshold to start prostaglandin E1, and a written safety-net for every child sent home with a murmur. Over-investigating the child is the lesser but real harm: an echocardiogram for every murmur drives cost, waiting-list pressure, and parental anxiety, without changing the outcome for the great majority who are normal on echo. [7] [2]
The cognitive traps that cost marks are four. First, treating an absent murmur as reassuring in a cyanotic or shocked neonate — the sickest duct-dependent lesions are the quietest. Second, missing coarctation because the femoral pulses felt present while the duct was open — the four-limb blood pressure is the catch. Third, ordering an echocardiogram reflexively for every innocent murmur, when a complete fingerprint and normal pulses and saturation allow confident reassurance. Fourth, forgetting the safety-net — the benign call is reversible only if the family knows the symptoms to return for. [1] [8]
The drug pitfalls sit with prostaglandin E1. The common adverse effects are apnoea, hypotension, fever and irritability, so the child is monitored in a neonatal or paediatric intensive care setting and intubated early if apnoea develops; the fever can be mistaken for sepsis, and the irritability for an underlying neurological problem, if the clinician forgets that these are expected effects of the drug. Prostaglandin E1 is also a gastric-artery vasodilator and can cause gastric-outlet obstruction in long-term use, though this is rarely an issue in the acute resuscitation. The fellow who names these effects when starting the infusion earns the mark for pharmacological competence. [11] [2]
Prognosis & Disposition
The prognosis of the innocent murmur is excellent: it is a feature of a normal heart, it resolves with growth in most children, and it carries no long-term cardiac risk. The child is reassured, documented, and followed in primary care, with a written safety-net for the symptoms that would prompt return. The disposition is the discharge, with a clear explanation to the family that a murmur is a sound and not a disease, that the heart is structurally normal, and that the child can do everything a child without a murmur can do. [7] [4]
The prognosis of the pathological murmur is the prognosis of the underlying lesion, and it has been transformed by modern paediatric cardiology and cardiac surgery. Most structural lesions are repaired surgically or by catheter in infancy or childhood, with survival into adulthood now the rule rather than the exception for almost every lesion. The duct-dependent neonate who reaches the cardiac centre on prostaglandin E1 has a good prognosis once the anatomy is defined and the repair is planned. The hypercyanotic spell that is bundled early has a good prognosis once the child reaches definitive surgical repair. The fellow who frames the prognosis around the lesion, the repair, and the long-term follow-up earns the mark. [9] [2]
The disposition for every child with a murmur is a clear, written plan that names the diagnosis, the red flags, the safety-net, and the follow-up. For the innocent murmur, the plan is reassurance and primary-care follow-up. For the pathological or uncertain murmur, the plan is referral to paediatric cardiology with an echocardiogram and a structured handover. For the critical lesion, the plan is prostaglandin E1, transfer to the cardiac centre, and admission to a paediatric intensive care setting. The structured, written plan is the single intervention that closes the gap between the bedside and the definitive care. [1] [11]
Special Populations
In remote and Indigenous communities, and in migrant and refugee families, the barriers to catching the critical lesion are concrete: distance from a paediatric cardiology centre, a delayed or absent newborn pulse-oximetry screen, and the narrow window between duct closure and collapse. The practical response is a four-limb blood pressure and a pre- and post-ductal saturation at every baby check, a low threshold to start prostaglandin E1 on suspicion, and a retrieval partnership with the regional cardiac centre. Recognising that the critical lesion in these settings is a systems problem rather than a clinical lapse — and designing the plan around the retrieval and the telehealth linkage — is the equity response that earns marks. [2] [8]
The newborn with a syndromic association is the population in whom a murmur should never be dismissed as innocent. Down syndrome, Turner syndrome, Noonan syndrome, Williams syndrome and 22q11 deletion each carry a high yield of structural heart disease, and the finding of a murmur (or the absence of one in a cyanotic infant) should prompt the echocardiogram rather than the reassurance. The child with a chromosomal or metabolic disorder under cardiology surveillance already is followed along a defined pathway, and the fellow's role is to know the pathway and to communicate with the cardiology team. [3] [8]
The adolescent with a murmur deserves a particular mention, because the presentations shift with age. The innocent pulmonary flow murmur of the athletic adolescent, the hypertrophic cardiomyopathy that announces itself with exercise-related syncope, and the coarctation or bicuspid aortic valve that surfaces through hypertension at a school check, are the moveable feasts of the teenage murmur. A murmur in an adolescent with exertional chest pain, syncope or a family history of sudden cardiac death is pathological until proven otherwise, and the echocardiogram and the cardiology referral are not optional. [5] [1]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric cardiovascular examination and murmur assessment is built on three strands. The first is the clinical-features literature that defines the innocent fingerprint and the yield of the bedside examination, anchored by the Ford and colleagues review of heart murmurs in children and the Hueckel and Leyland review of paediatric murmurs. The second is the newborn-cardiovascular-assessment literature that defines the duct-dependent lesion, the pulse-oximetry screen, and the prostaglandin-E1 resuscitation, anchored by the Singh and Lakshminrusimha review of perinatal cardiovascular physiology and the Fillipps and Bucciarelli review of cardiac evaluation of the newborn. The third is the lesion-specific literature that defines the anatomy and the management, anchored by the Law and colleagues review of coarctation, the Bailliard and Anderson review of tetralogy of Fallot, and the van Roekens and Zuckerberg review of the hypercyanotic crisis. [1] [2]
In Australia and New Zealand, the newborn cardiovascular assessment combines the clinical baby check (with a four-limb blood pressure and a femoral-pulse check), the pulse-oximetry screen at twenty-four to forty-eight hours, and a low threshold to start prostaglandin E1 and transfer to one of the paediatric cardiac centres. Echocardiography is centralised to the cardiac centres, and the structured referral and the retrieval partnership are the tools that close the gap for rural and remote infants. The fellow should name the local pathway in a long case — the baby check, the pulse-oximetry screen, the prostaglandin-E1 rule, and the retrieval to the cardiac centre. [3] [11]
The controversies that a higher-level candidate should hold are three. First, the role of the echocardiogram in the innocent murmur: the recurrent-cardiology-evaluation data argue against reflexive echo for a complete fingerprint, while the miss-rate of the rare lesion argues for a low threshold when the fingerprint is incomplete. Second, the place of the hyperoxia test in the era of the pulse-oximetry screen: largely historical, but still useful in the ambiguous case without a screen. Third, the timing of the newborn pulse-oximetry screen relative to early discharge: a screen before twenty-four hours has a higher false-positive rate but catches the earliest presenters. Holding these openly — rather than pretending the answers are settled — is the mark of a candidate who reads the literature rather than memorises it. [7] [2]
Exam Pearls
The six anchor points a fellowship candidate should land are these. First, the examination sequence: inspect, palpate the apex and the pulses together with the femorals, auscultate the five areas with bell and diaphragm, and always measure a four-limb blood pressure and a pre- and post-ductal saturation. Second, the innocent fingerprint: soft, short, systolic, grade two or less, left sternal edge, normal heart sounds, asymptomatic child, normal pulses and saturation. Third, the pathology rules: any diastolic, continuous or pansystolic murmur, any thrill, any grade three or louder, or any abnormal heart sound, symptom or pulse is pathological until proven otherwise. Fourth, the duct-dependent neonate: cyanosis that does not correct on oxygen or shock as the duct closes means prostaglandin E1 before the echo. Fifth, the coarctation rule: weak or absent femoral pulses with an arm-to-leg gap is coarctation until proven otherwise. Sixth, the hypercyanotic spell: knee-to-chest, oxygen, the bundle, and admission. [1] [2]
I.P.A.D. — the paediatric cardiovascular examination
The high-yield one-liners that earn the mark: most murmurs in children are innocent; the innocent murmur fits a fingerprint and the pathological murmur departs from it; an absent murmur does not exclude serious disease in a cyanotic neonate; the duct-dependent lesion is treated with prostaglandin E1 before the echocardiogram; coarctation is caught by the four-limb blood pressure and the femoral pulses; the hypercyanotic spell is bundled, not single-drug-treated. The fellow who can generate the whole topic from the single image of turbulent flow through a child's heart — and who lands each of these six anchor points — will pass the station. [4] [11] [9]
References
- [1]Ford B, Lara S, Park J. Heart Murmurs in Children: Evaluation and Management. Am Fam Physician, 2022.PMID 35289571
- [2]Singh Y, Lakshminrusimha S. Perinatal Cardiovascular Physiology and Recognition of Critical Congenital Heart Defects. Clin Perinatol, 2021.PMID 34353581
- [3]Fillipps DJ, Bucciarelli RL. Cardiac evaluation of the newborn. Pediatr Clin North Am, 2015.PMID 25836709
- [4]Hueckel RM, Leyland C. Pediatric Murmurs. Nurs Clin North Am, 2023.PMID 37536793
- [5]Naik RJ, Shah NC. Teenage heart murmurs. Pediatr Clin North Am, 2014.PMID 24267454
- [6]Poddar B, Basu S. Approach to a child with a heart murmur. Indian J Pediatr, 2004.PMID 14979389
- [7]Dalal NN, Dzelebdzic S, Frank LH, Clauss SB, Mott AR. Recurrent Cardiology Evaluation for Innocent Heart Murmur: Echocardiogram Utilization and Costs. Clin Pediatr (Phila), 2018.PMID 29993270
- [8]Law MA, Collier SA, Sharma S, Tivakaran VS. Coarctation of the Aorta. StatPearls, 2026.PMID 28613663
- [9]Bailliard F, Anderson RH. Tetralogy of Fallot. Orphanet J Rare Dis, 2009.PMID 19144126
- [10]Hipona FA, Sanyal SK. Differential cyanosis in congenital heart disease. J Pediatr, 1968.PMID 5638144
- [11]Johnson BA, Shepherd J, Bhombal S, Ali N, Friedland-Mewe D, Gruber PJ, et al. Special considerations for the stabilization and resuscitation of patients with cardiac disease in the Neonatal Intensive Care Unit. Semin Perinatol, 2024.PMID 39477714
- [12]van Roekens CN, Zuckerberg AL. Emergency management of hypercyanotic crises in tetralogy of Fallot. Ann Emerg Med, 1995.PMID 7832359