Paeds · cardiology
Exercise evaluation and sports participation in heart disease
Also known as Sports participation in heart disease · Preparticipation cardiac screening · Exercise evaluation in the cardiac child · Athlete clearance in congenital and acquired heart disease · Mitchell sport classification · Eligibility and disqualification of the athlete with cardiac disease
Fellowship guide to exercise evaluation and sports participation for the child with heart disease: how to turn the clearance question into a stratified decision built on the cardiac lesion, the haemodynamic load of the sport (Mitchell dynamic x static classification), and the athlete's symptoms and family history; the red-flag exertional history that mandates a 12-lead ECG before clearance; the layered workup from the 14-point history and examination through ECG, echocardiography and cardiopulmonary exercise testing; the three eligibility tiers (cleared, individualised, disqualified) applied across the common substrates from innocent murmurs and repaired simple lesions through bicuspid aortic valve and repaired tetralogy to hypertrophic cardiomyopathy, the channelopathies, anomalous coronary artery and Marfan aortic disease; the AHA/ACC 2015 and ESC 2020 guideline consensus, the Italian ECG-screening evidence, annual re-evaluation of the growing athlete, and venue safety with a written emergency action plan and accessible AED.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the fourteen-year-old boy brought to your clinic by his parents because the school rugby coach needs a clearance form signed before the first trial. He has a bicuspid aortic valve picked up years ago on a murmur workup, and his father wants to know whether contact sport is safe. A week later a fifteen-year-old girl sits in front of you after collapsing during a cross-country run — she came around quickly, but her aunt died suddenly at forty-two. Both children are asking the same question, and the answer for each is different. The clearance decision is the whole of this topic: when to say yes, when to individualise, and when the honest answer is that competitive sport is not safe. [1] [2]
Exercise evaluation in heart disease is the structured preparticipation assessment that asks whether a child or adolescent with known or newly suspected cardiac disease can take part in competitive or recreational sport, and at what intensity. The question matters because sport is both a health good — cardiovascular, metabolic, mental-health, and social — and, for a small number of vulnerable hearts, the trigger that unmasks a fatal arrhythmia. The task is to identify that small group without denying the rest the benefits of exercise. [11] [14]
The decision rests on three legs that you should hold in mind whenever a clearance form arrives. First, the cardiac lesion and its haemodynamic severity: an innocent murmur and a hypertrophic cardiomyopathy are not the same problem. Second, the load of the intended sport, which the Mitchell grid classifies by its dynamic and static intensity. Third, the athlete's own symptoms and family history, which are the strongest predictors of risk and the features most often missed. Hold these three together and the tiered answer — cleared, individualised, or disqualified — usually follows. [1] [10]
Classification
The most useful classification for this topic is the Mitchell grid, because it lets you match the haemodynamic load of a sport to the severity of the cardiac lesion. Every sport can be placed somewhere on a three-by-three grid that crosses dynamic intensity with static intensity, and the cell the sport lands in tells you how much volume and pressure load it places on the heart. [1]
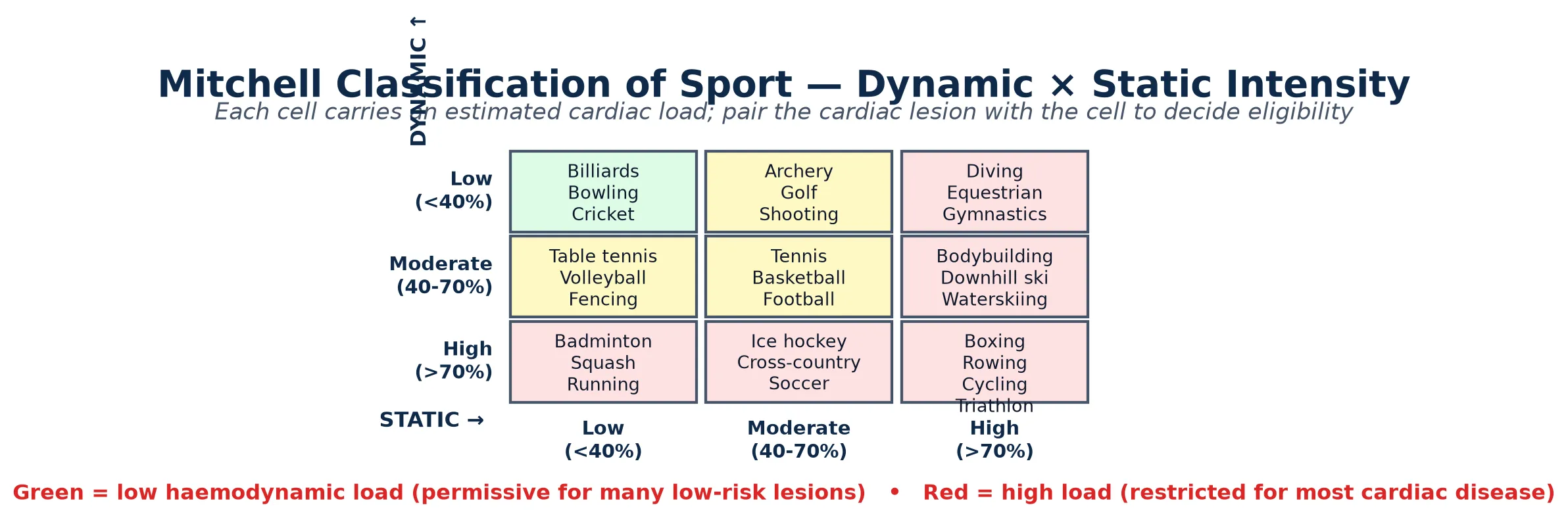
Dynamic intensity is the percentage of maximal oxygen uptake the sport demands — how high the cardiac output and heart rate are driven — so distance running and cycling are high-dynamic while billiards is low. Static intensity is the percentage of maximal voluntary contraction the sport demands — how high the blood pressure is driven — so weightlifting and gymnastics are high-static while cricket is low. The combination matters: a sport can be high in one and low in the other, and each axis stresses the heart differently. A child with a fixed obstruction tolerates high-static sport badly, while a child with limited cardiac reserve tolerates high-dynamic sport badly. [1] [10]
Low dynamic + low static
A-I cell
- Billiards, bowling, cricket, golf
- Lowest volume and pressure load
- Generally permissive for most stable cardiac lesions
- The starting point for the restricted athlete
High dynamic
running, cycling, soccer
- Drives cardiac output and heart rate
- Poorly tolerated with limited reserve or ischaemia
- Channelopathies and coronary anomalies unmasked here
- Cross-country, distance running, soccer
High static
weightlifting, gymnastics
- Drives blood pressure and afterload
- Poorly tolerated with outflow obstruction or aortic disease
- Weightlifting, wrestling, downhill skiing
- Bicuspid valve and Marfan root at risk here
The three eligibility tiers map onto this grid. A low-risk lesion can enter almost any cell. A moderate lesion is matched to a specific acceptable cell — often low-to-moderate on both axes, and away from collision. A high-risk lesion is excluded from competitive sport regardless of cell, because no competitive intensity is safe. The art of the clearance decision is pairing the lesion to the right cell, not applying a blanket ban. [1] [3]
Epidemiology & Risk Factors
Sudden cardiac death in young athletes is rare — about one event per fifty thousand to one hundred thousand athlete-years — but it is catastrophic, highly visible, and often preceded by warning symptoms that were missed or dismissed in the weeks beforehand. The rarity is what makes universal screening contentious; the warning symptoms are what make a careful history so powerful. [14] [13]
The substrates that kill young athletes differ by region and by screening intensity. In the United States, where systematic ECG screening is not universal, hypertrophic cardiomyopathy is the leading autopsy finding, with anomalous coronary artery and idiopathic left-ventricular hypertrophy also prominent. In countries with ECG-inclusive screening, the leading causes shift as more cardiomyopathies and channelopathies are detected before death. The lesson is that the substrate you miss depends on how hard you look. [14] [2]
The numbers that anchor your viva
Risk is amplified by male sex, by the intensity of competition, and crucially by the presence of symptoms. A prior exertional syncope, chest pain, or palpitation multiplies risk many-fold, as does a family history of sudden unexplained death before fifty in a first-degree relative. These are the features that separate the athlete who needs a form signed from the one who needs a workup. [13] [12]
Pathophysiology
The teaching model is simple: competitive sport places an acute haemodynamic and autonomic load on the heart, and a heart that is structurally or electrically abnormal handles that load badly. The cascade runs from substrate, through the exercise trigger, to arrhythmia and arrest. [3] [14]
During competitive exertion the body releases a catecholamine surge, the heart rate and cardiac output rise, the blood pressure climbs with the static component of the effort, and the myocardium demands more oxygen at exactly the moment electrolytes are shifting and dehydration is developing. For a normal heart this is well tolerated. For a vulnerable heart it is the moment of maximum stress. [6] [10]
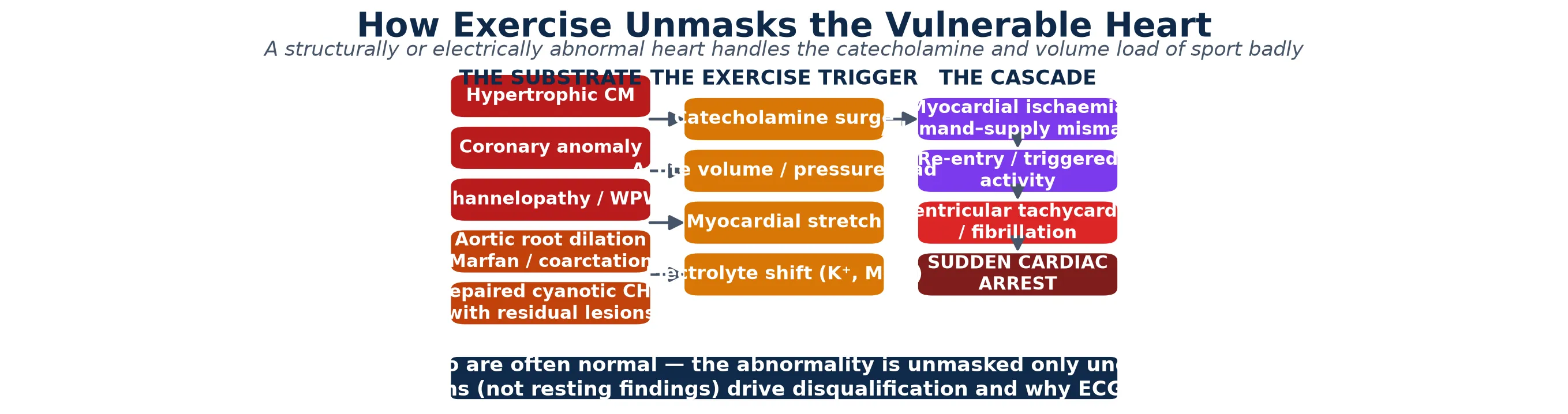
The failure mode depends on the substrate. In hypertrophic cardiomyopathy the thickened muscle demands more oxygen than a structurally abnormal vasculature can supply, and the small-vessel disease and dynamic outflow obstruction worsen the mismatch; the result is ischaemia that triggers ventricular arrhythmia. In an anomalous coronary artery the aberrant course — typically the artery taking an interarterial course between the aorta and pulmonary artery — kinks or is compressed during exertion, producing acute ischaemia. In the channelopathies the adrenergic surge destabilises an already prolonged or leaky repolarisation, generating torsades or polymorphic ventricular tachycardia. In aortic root disease the pressure load threatens dissection. [3] [6]
[8] [6]The implication for the clinician is direct. Resting findings are reassuring but they are not the whole story. The history of what happens during exertion is the most sensitive test you have, and a child who has collapsed during sport needs a workup that includes exercise testing, not just a resting ECG and a reassuring echocardiogram. [6] [10]
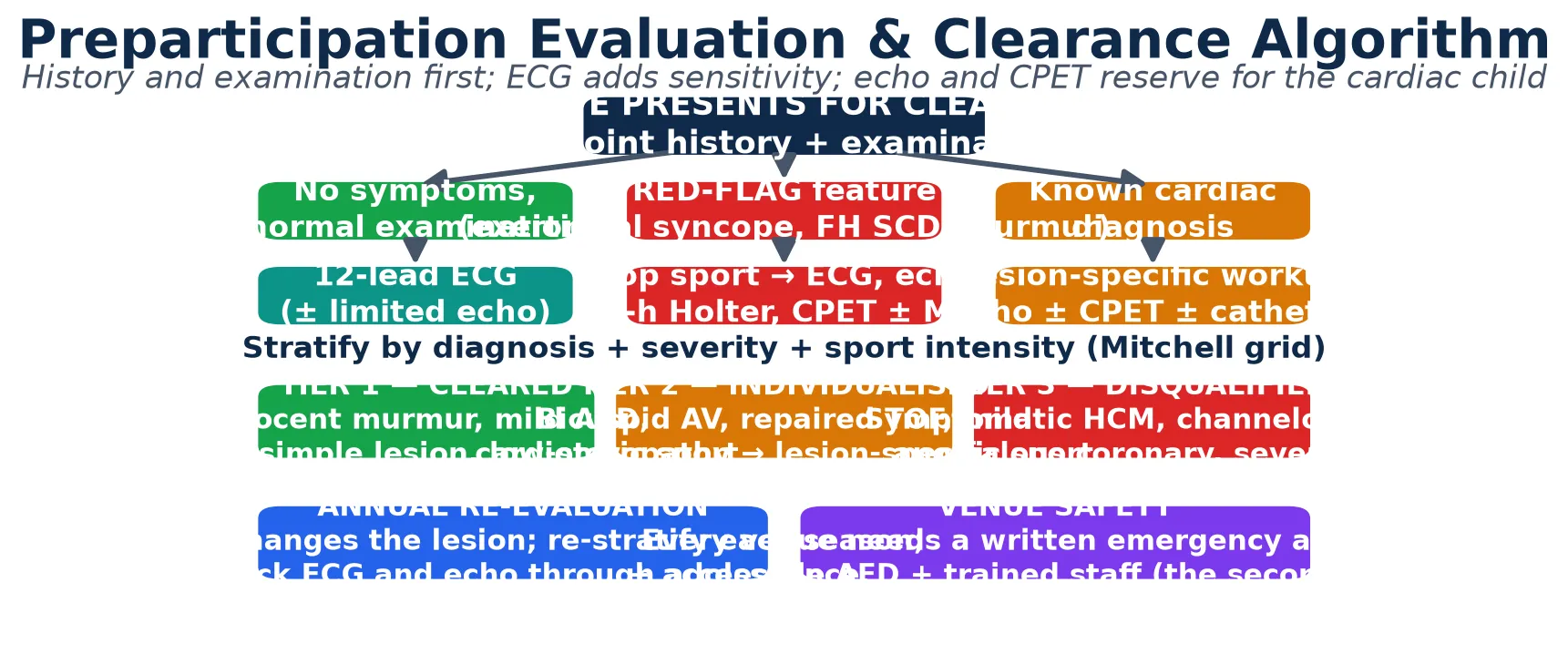
Clinical Presentation
The athlete arrives for clearance in one of three ways: asymptomatic and presenting only for the form; symptomatic with exertional chest pain, syncope, dyspnoea, or palpitations; or already known to carry a cardiac diagnosis, presenting to ask what is now permitted. Each pathway demands a different intensity of evaluation, but all three end at the same stratified decision. [2] [12]
The red-flag history is the heart of the assessment. Syncope or chest pain that occurs during exertion — not after it, not on standing — is the single most important warning, because it implies a cardiac rather than a vasovagal or situational cause. Exertional dyspnoea disproportionate to effort, unexplained fatigue, and palpitations that occur with exercise carry the same weight. A family history of sudden unexplained death before fifty in a first-degree relative is a red flag in its own right, as is a known channelopathy or cardiomyopathy in the family. [13] [8]
| Presentation | What it implies | Act |
|---|
Distinguish carefully between cardiac and benign presentations. Vasovagal syncope has a characteristic prodrome of warmth, nausea, and visual disturbance, occurs on standing or after the effort is over, and recovers quickly. Benign exercise-induced bronchoconstriction causes wheeze and cough after exercise, typically in the asthmatic child, and responds to a bronchodilator. The cardiac presentation is sudden, without prodrome, occurs mid-effort, and is the one that must never be dismissed. [12] [2]
Differential Diagnosis
The differential of an exertional symptom in a young athlete splits into benign causes that need reassurance and cardiac causes that need restriction. Getting this split right is the whole clinical task. [2] [10]
The benign causes are common and important to recognise. Exercise-induced bronchoconstriction produces wheeze, cough, and chest tightness that peaks five to ten minutes after exertion and responds to a bronchodilator. Vasovagal syncope has the prodrome and the situational triggers described above. Dehydration, heat illness, anaemia, deconditioning, and post-viral fatigue round out the list. None of these demand sport restriction once treated, but each must be distinguished from a cardiac cause by the history and, where indicated, the ECG. [11] [12]
Benign exertional symptoms
- Exercise-induced bronchoconstriction (post-exertional wheeze)
- Vasovagal syncope (prodrome, situational)
- Dehydration and heat illness
- Anaemia, deconditioning, post-viral fatigue
- Reassure and treat; no cardiac restriction
Cardiac causes requiring restriction
- Hypertrophic and other cardiomyopathies
- Channelopathies (long-QT, CPVT, Brugada)
- Anomalous coronary artery
- Aortic root disease (Marfan, bicuspid-related)
- Significant valvular disease and myocarditis
The cardiac causes are fewer but decisive. Hypertrophic cardiomyopathy, the channelopathies, an anomalous coronary artery, aortic root disease, significant valvular stenosis, and recent myocarditis are the diagnoses that change a clearance into a disqualification. The discriminator between benign and cardiac is the timing and reproducibility of the symptom with exertion, supported by the 12-lead ECG and, where indicated, echocardiography and exercise testing. A symptom that is reliably reproduced by exertion and relieved by rest is cardiac until proven otherwise. [3] [6]
Clinical & Bedside Assessment
Every clearance begins with the history and examination, because together they are the most sensitive screen available and they are the part most often done badly. The AHA 14-element personal and family history is the standard framework, and a focused five-minute cardiovascular examination completes the bedside assessment. [12] [2]
The history targets the exertional symptoms described above and a structured family history of sudden unexplained death, cardiomyopathy, channelopathy, Marfan syndrome, or surgery for congenital heart disease before fifty in a first-degree relative. Ask specifically about syncope, chest pain, dyspnoea, palpitations, and fatigue, and pin each symptom to its timing relative to exertion. The collateral history from a coach or parent is invaluable, because the athlete may minimise or under-report. [12] [13]
[2] [12]The examination looks for a pathological murmur — loud, harsh systolic, diastolic, or changing with position — radio-femoral delay suggesting coarctation, the marfanoid habitus, hypertension, and any sign of heart failure. An innocent murmur — soft, vibratory, short, sitting in the pulmonary area, vanishing on standing — is reassuring and clears the athlete without further testing if the history is clean. A pathological murmur or any red-flag finding stops clearance and triggers echocardiography. [2] [11]
Investigations
The diagnostic strategy is layered. Every athlete gets the history and examination; those with a red flag or a known cardiac diagnosis get a 12-lead ECG; and the symptomatic or complex child gets echocardiography, Holter monitoring, and cardiopulmonary exercise testing to define the lesion and unmask exertion-provoked abnormality. [2] [10]
The 12-lead ECG is the single most powerful test in the symptomatic athlete, but it must be interpreted with athlete-specific criteria, because athletic training produces benign changes — early repolarisation, isolated voltage criteria for left-ventricular hypertrophy, and T-wave inversion confined to the right precordial leads in some athletes — that overlap with disease. The International Recommendations for ECG Interpretation in Athletes were built precisely to reduce false positives without missing disease. Apply them, or refer to someone who does. [10] [13]
Echocardiography defines structure and severity in any known or suspected lesion, and is the test that resolves a pathological murmur, screens for hypertrophic cardiomyopathy, and measures the aortic root in the bicuspid valve and Marfan child. Holter monitoring captures paroxysmal arrhythmia in the child with intermittent palpitations. Cardiopulmonary exercise testing — the gold standard for functional capacity — unmask exertion-provoked ischaemia, exercise-induced arrhythmia such as CPVT, and any out-of-proportion limitation, and it sets a safe intensity ceiling for the child who is cleared but limited. [4] [11]
The standard preparticipation workup
14-element AHA personal and family history, pinned to exertional timing.
Focused cardiovascular examination: murmur, radio-femoral delay, marfanoid habitus, blood pressure.
12-lead ECG for any red flag, any abnormal finding, or any known cardiac diagnosis; interpret with athlete criteria.
Echocardiography to define structure and severity in a known or suspected lesion.
Holter monitoring for intermittent palpitations or suspected channelopathy.
Cardiopulmonary exercise testing to unmask exertion-provoked arrhythmia and set a safe ceiling.
Cardiac MRI or coronary CT if anomalous coronary artery, myocarditis, or arrhythmogenic cardiomyopathy is suspected.
Stratify into cleared, individualised, or disqualified; document and counsel; plan annual re-evaluation.
Where a coronary anomaly, myocarditis, or arrhythmogenic right-ventricular cardiomyopathy is suspected, cardiac magnetic resonance imaging and coronary CT angiography complete the workup. The intensity of the workup is proportional to the suspicion, and the threshold for referral to a specialist sports or congenital cardiology service is low for any red flag. [6] [4]
Management — Resuscitation
When the system fails and an athlete collapses on the field, the response in the first three to five minutes decides survival. The resuscitation is standard paediatric and adult life support with one emphasis: retrieve and use the AED as fast as possible, because early defibrillation is the single biggest determinant of survival in athlete sudden cardiac arrest. [9]
Recognise the collapse as cardiac — a sudden fall without contact, no responsive breathing, no pulse — and start the chain immediately: call for help, begin high-quality cardiopulmonary resuscitation, send someone for the automated external defibrillator, apply it, and follow its prompts. Do not wait for the ambulance to defibrillate, because survival falls by roughly ten per cent for every minute of delay to shock in a shockable rhythm. [9] [14]
SAVE-OUR-ATHLETE
The reason this belongs in a preparticipation topic is that resuscitation is a function of preparation, not luck. A venue with a written emergency action plan, a known and accessible AED, and staff trained to use it is the secondary line of defence behind screening. The clinician who signs clearances shares responsibility for ensuring that line exists. [9] [13]
Management — Definitive & Stepwise
Definitive management is the stratified clearance decision itself, and it has three tiers. The goal is not to prohibit sport — it is to permit the greatest safe activity, because the cardiovascular and mental-health benefits of exercise are real and the harms of unnecessary restriction are real too. [11] [10]
TIER 1 — Cleared
- Innocent murmur with clean history
- Repaired simple lesion (closed ASD, VSD, ligated PDA)
- Physiologically normal athlete
- All sports permitted; routine follow-up
TIER 2 — Individualised
- Bicuspid aortic valve without stenosis or root dilation
- Repaired tetralogy of Fallot, coarctation, Fontan
- Mild or treated cardiomyopathy
- Matched to an acceptable Mitchell cell; CPET may set the ceiling
TIER 3 — Disqualified
- Symptomatic hypertrophic cardiomyopathy
- Channelopathy (long-QT, CPVT)
- Anomalous coronary artery
- Severe aortic stenosis; Marfan with root dilation
- No competitive sport; leisure activity encouraged
The first tier is the cleared athlete. An innocent murmur with a clean history and a normal examination clears the athlete for all sports without further testing in most settings. A child with a repaired simple lesion — a closed atrial or ventricular septal defect or a ligated ductus with no residual shunt or pulmonary hypertension — is similarly cleared once echocardiography confirms the repair. These children should compete without restriction. [4] [11]
The second tier is the individualised athlete, and it is where most of the clinical judgement lives. The child with a bicuspid aortic valve is cleared if the valve is functionally normal and the aortic root is normal, but restricted from high-static sport if there is significant stenosis, regurgitation, or root dilation. The child with repaired tetralogy of Fallot or coarctation is usually cleared for low-to-moderate intensity sport, away from collision, after echocardiography and often cardiopulmonary exercise testing confirm good residual function. The principle is to match the lesion to an acceptable Mitchell cell, not to ban sport outright. [4] [5]
The season arc of a cardiac athlete
The third tier is disqualification from competitive sport, and it carries the diagnoses where no competitive intensity is safe. The symptomatic athlete with hypertrophic cardiomyopathy, any child with a channelopathy such as long-QT syndrome or catecholaminergic polymorphic ventricular tachycardia, the child with an anomalous coronary artery, the child with severe aortic stenosis, and the child with Marfan syndrome and an enlarged aortic root are all excluded from competitive sport. The decision is hard, and it must be delivered honestly, with a clear explanation, a plan for leisure activity, and attention to the psychosocial cost. Leisure activity is almost always possible and should be encouraged within the lesion's limits. [3] [8]
Specific Subtypes & Scenarios
The common scenarios deserve a direct answer, because they are the ones a candidate will be asked and the ones a clinician will face in clinic. Each maps onto the tiered framework, and the principle is always to match the lesion to the sport, not to default to a ban. [1] [4]
Innocent murmurs and the physiologically normal athlete clear for all sport once the history is clean and the examination reassuring. An innocent murmur — soft, vibratory, position-dependent, with no radiation and no other findings — needs no ECG in most settings, though an ECG is reasonable if any doubt remains. These children should never be restricted on the basis of the murmur alone. [2] [11]
Repaired congenital heart disease follows the lesion. Simple repairs — a closed atrial septal defect, ventricular septal defect, or ligated ductus with no residual shunt or pulmonary hypertension — clear for all sport once echocardiography confirms the result. Moderate repairs such as repaired tetralogy of Fallot, coarctation of the aorta, or a Fontan circulation are individualised: low-to-moderate intensity on both Mitchell axes, away from collision sport, and only after echocardiography and cardiopulmonary exercise testing confirm good residual function and no significant arrhythmia. [4] [11]
Bicuspid aortic valve clears the athlete when the valve is functionally normal and the aortic root is of normal size, but high-static sport is restricted when there is significant stenosis, regurgitation, or root dilation, because the pressure load threatens both the valve and the aorta. Serial echocardiography through growth guides the decision, and the root that grows disproportionately to body size tips the balance toward restriction. [4] [5]
Hypertrophic cardiomyopathy disqualifies the symptomatic athlete and most definitive diagnoses from competitive sport, because the risk of sudden death during exertion is substantially elevated and not abolished by treatment. Leisure activity within the lesion's limits is encouraged, and an implantable defibrillator is not a licence to return to competitive sport. The decision is delivered honestly, with family involvement and attention to the psychosocial cost. [3]
Channelopathies and the anomalous coronary artery disqualify the athlete from competitive sport, and both share the trap that the resting ECG and echocardiogram may be normal. The channelopathy — long-QT syndrome, catecholaminergic polymorphic ventricular tachycardia, or Brugada syndrome — is unmasked by exercise or epinephrine challenge, and the anomalous coronary artery by coronary imaging. Any child with exertional syncope and a normal resting workup needs exercise testing and, where indicated, coronary imaging before clearance is signed. [8] [6]
Marfan syndrome and aortic root disease restrict the athlete from high-static and collision sport because of the risk of aortic dissection under the pressure load, regardless of root size at presentation. Beta-blockade and serial root surveillance guide the decision, and the threshold for restriction is low because dissection is catastrophic. Low-dynamic, low-static activity is usually acceptable and is encouraged. [5]
Complications & Pitfalls
The catastrophic complication is sudden cardiac death during sport, and the commonest pitfall is the exertional symptom that was dismissed in the weeks before the event. The retrospective reviews of athlete deaths consistently find warning symptoms that were attributed to dehydration, asthma, fatigue, or effort and never investigated. A careful history is the cheapest and most powerful intervention available. [14] [13]
The second pitfall is the opposite error: over-restriction. Unnecessary disqualification removes the cardiovascular, metabolic, mental-health, and social benefits of exercise, may stigmatise the cardiac child, and is a harm in its own right. The goal is the greatest safe activity, and a child cleared for low-to-moderate sport is better served than a child banned from all sport on the basis of a lesion that would tolerate careful participation. [11] [10]
The pitfalls that cost marks and lives
Further pitfalls are technical. Relying on history and examination alone without an ECG misses most channelopathies and many cardiomyopathies. Over-calling benign athlete ECG changes — early repolarisation, isolated voltage criteria for hypertrophy — generates false positives and unnecessary disqualification if athlete-specific criteria are not applied. Failing to re-evaluate the growing athlete each season misses the changing root size, gradient, and channelopathy risk window through puberty. And signing a clearance without confirming that the venue has a written emergency action plan and an accessible AED leaves the secondary line of defence unattended. [10] [9]
Prognosis & Disposition
With appropriate stratification the vast majority of children with cardiac disease can participate in at least leisure and many competitive sports, and lead full and active lives. The clearance decision is not a binary yes or no; it is a matching of the lesion to the sport that protects the child while preserving as much normal activity as possible. [11] [4]
The high-risk athlete — the child with symptomatic hypertrophic cardiomyopathy, a channelopathy, or an anomalous coronary artery — is disqualified from competitive sport but is enrolled in lifelong cardiology surveillance, disease-specific treatment, and an individualised exercise prescription. Disqualification is the beginning of a care plan, not the end of activity; leisure exercise within limits is almost always possible and is encouraged for its health benefits. [3] [8]
Disposition is shared care. The paediatric cardiologist owns the eligibility decision and the surveillance; the general paediatrician owns the co-ordination, the growth and development monitoring, the mental-health support, and the annual re-evaluation each season. The transitioning adolescent moves to an adult sports or congenital cardiology service with a structured handover that carries the diagnosis, the clearance status, and the surveillance plan. [10] [3]
Special Populations
The adolescent in a growth spurt needs particular attention, because the channelopathy and cardiomyopathy risk window rises around puberty, the aortic root grows with body size in bicuspid valve and Marfan, and outflow gradients change. Re-stratify each season rather than relying on a clearance signed years earlier. [5] [3]
Children with repaired complex congenital heart disease — the single-ventricle Fontan circulation, repaired tetralogy of Fallot, repaired transposition — are individually cleared for low-to-moderate intensity sport, away from collision and away from high-static load, after echocardiography and cardiopulmonary exercise testing set a safe ceiling. Cardiopulmonary exercise testing is especially valuable in this group, because it quantifies the functional reserve that the lesion has left. [4] [11]
Rural and remote athletes, and Indigenous, refugee, and socioeconomically disadvantaged families, face diagnostic delays and limited access to echocardiography and cardiopulmonary exercise testing. Telehealth cardiology, protocol-driven workup, a low threshold for referral after any exertional symptom, and attention to venue emergency preparedness are part of equitable practice. The on-field collapse remains more common where screening is thin, which makes the written emergency action plan and accessible AED even more life-saving. [9] [10]
The transitioning athlete with a chronic lesion moves to adult sports or congenital cardiology with a structured handover. The handover carries the diagnosis, the clearance status, the permitted and prohibited sport cells, the surveillance plan, and the psychosocial context. Pregnancy, contraception, and the heritable nature of the lesion are addressed in transition for the conditions that carry them. [10] [5]
Evidence, Guidelines & Regional Differences
| Region | Screening model | ECG-inclusive? | Key reference |
|---|
The central controversy is the role of universal ECG screening. The Italian Veneto experience is the most cited evidence: mandatory ECG-inclusive screening was associated with an eighty-nine per cent reduction in sudden cardiac death among competitive athletes, and most of the reduction came from detecting cardiomyopathies and channelopathies before they killed. Against this stand the cost, the false-positive rate of an ECG read without athlete-specific criteria, and the infrastructure required. Australia and New Zealand have generally adopted targeted ECG screening — ECG for any red flag or known diagnosis — rather than universal screening, a position the Cardiac Society of Australia and New Zealand supports. [13] [12]
The second area of evolution is the move toward permitting more activity. The older tradition was the blanket ban for any cardiac diagnosis; the modern approach, reflected in both the AHA/ACC and ESC frameworks, is to individualise and to preserve the greatest safe activity, weighing the cardiac risk against the real harms of restriction and the athlete's and family's values. Shared decision-making is now part of the standard, and the psychosocial cost of disqualification is addressed alongside the surveillance plan. [10] [11]
Exam Pearls
References
- [1]Levine BD, Baggish AL, Kovacs RJ, Link MS, Maron BJ Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 1: Classification of Sports: Dynamic, Static, and Impact. J Am Coll Cardiol, 2015.PMID 26542656
- [2]Maron BJ, Levine BD, Washington RL, Baggish AL, Kovacs RJ, Maron MS Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 2: Preparticipation Screening for Cardiovascular Disease in Competitive Athletes. J Am Coll Cardiol, 2015.PMID 26542659
- [3]Maron BJ, Udelson JE, Bonow RO, Nishimura RA, Ackerman MJ, et al. Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 3: Hypertrophic Cardiomyopathy, Arrhythmogenic Right Ventricular Cardiomyopathy, and Other Cardiomyopathies. J Am Coll Cardiol, 2015.PMID 26542657
- [4]Van Hare GF, Ackerman MJ, Evangelista JK, Kovacs RJ, Myerburg RJ Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 4: Congenital Heart Disease. J Am Coll Cardiol, 2015.PMID 26542660
- [5]Braverman AC, Harris KM, Kovacs RJ, Maron BJ Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 7: Aortic Diseases, Including Marfan Syndrome. J Am Coll Cardiol, 2015.PMID 26542664
- [6]Thompson PD, Myerburg RJ, Levine BD, Udelson JE, Kovacs RJ Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 8: Coronary Artery Disease. J Am Coll Cardiol, 2015.PMID 26542666
- [7]Zipes DP, Link MS, Ackerman MJ, Kovacs RJ, Myerburg RJ, Page RL Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 9: Arrhythmias and Conduction Defects. J Am Coll Cardiol, 2015.PMID 26542670
- [8]Ackerman MJ, Zipes DP, Kovacs RJ, Maron BJ Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 10: The Cardiac Channelopathies. J Am Coll Cardiol, 2015.PMID 26542662
- [9]Link MS, Myerburg RJ, Estes NAM 3rd Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 12: Emergency Action Plans, Resuscitation, Cardiopulmonary Resuscitation, and Automated External Defibrillators. J Am Coll Cardiol, 2015.PMID 26542665
- [10]Pelliccia A, Sharma S, Gati S, Bäck M, Börjesson M, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J, 2021.PMID 32860412
- [11]Longmuir PE, Brothers JA, de Ferranti SD, Hayman LL, McCrindle BW, et al. Promotion of physical activity for children and adults with congenital heart disease: a scientific statement from the American Heart Association. Circulation, 2013.PMID 23630128
- [12]Maron BJ, Thompson PD, Ackerman MJ, Balady G, Berger S, et al. Recommendations and considerations related to preparticipation screening for cardiovascular abnormalities in competitive athletes: 2007 update. Circulation, 2007.PMID 17353433
- [13]Corrado D, Basso C, Pavei A, Michieli P, Schiavon M, Thiene G Trends in sudden cardiovascular death in young competitive athletes after implementation of a preparticipation screening program. JAMA, 2006.PMID 17018804
- [14]Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation, 2009.PMID 19221222