Paeds · cardiology
Heart failure in infants and children
Also known as Heart failure in infants and children · Paediatric heart failure · Congestive heart failure in children · Infant heart failure · Cardiomyopathy with heart failure
Fellowship guide to heart failure as a clinical syndrome in infants and children: the volume-overload, pressure-overload and pump-failure mechanisms, the modified Ross severity grading, the neurohormonal vicious cycle, the infant presentation of tachypnoea and failure to thrive, echocardiographic assessment, acute resuscitation and chronic neurohormonal therapy, the carvedilol evidence, and escalation to the Berlin Heart EXCOR ventricular assist device and transplantation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Heart failure in a child is a clinical syndrome in which the heart cannot deliver enough blood to meet the body's metabolic demands, or can do so only at abnormally high filling pressures. It is not a single diagnosis: it is the end result of many different problems, and the whole skill of paediatric heart failure lies in finding the mechanism that is failing. [3]
Because cardiac output is the product of stroke volume and heart rate, anything that reduces stroke volume — a failing pump, a volume load that dilates the ventricle, or a pressure load that stiffens it — produces the same syndrome of poor perfusion and congestion. In adults heart failure is usually the consequence of coronary disease and a stiff, aging myocardium; in children it is usually the consequence of a structural congenital lesion or an intrinsic cardiomyopathy, which is why so much of childhood heart failure is surgically curable once the cause is found. [3] [4]
Classification
Heart failure in children is classified on two independent axes: how severe it is, and why the ventricle is failing. Both must be stated, because a class-IV infant with a repairable coarctation and a class-IV infant with a terminal cardiomyopathy are entirely different clinical problems that share only the label. [3] [5]
The severity axis uses the modified Ross classification, which translates the adult New York Heart Association functional classes into the language of infancy and childhood, where exertion is feeding and growth. Class I is no limitation and normal growth, with tachypnoea only on exertion. Class II is mild limitation, tachypnoea with feeds or exertion and some growth faltering. Class III is marked limitation, tachypnoea at rest, prolonged sweaty feeds, failure to thrive and marked hepatomegaly. Class IV is severe limitation, symptomatic at rest with a grey, mottled child, and cardiogenic shock is imminent. Ross's 2012 age-stratified revision refined the criteria across infancy and adolescence, and it remains the working bedside grading tool. [5]
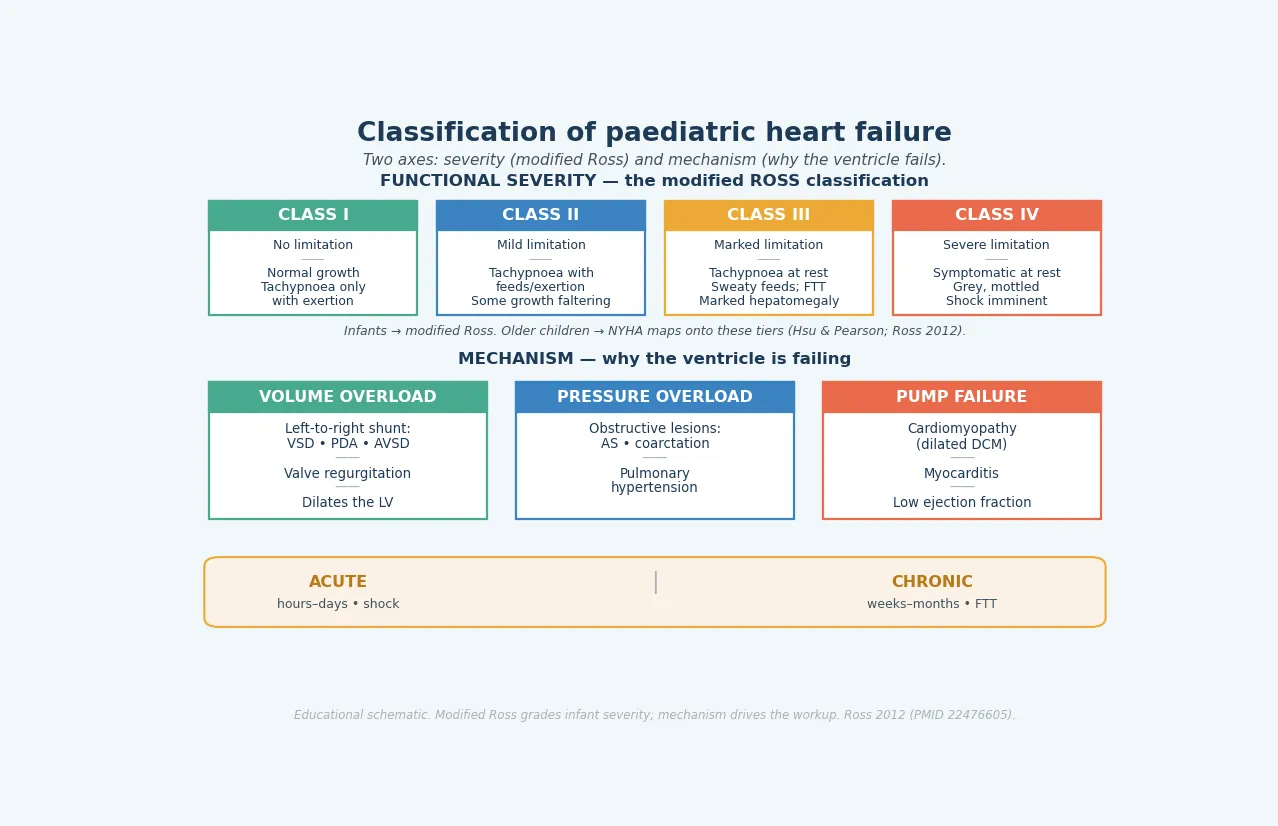
The mechanism axis names why the ventricle is failing. Volume overload comes from a left-to-right shunt (a ventricular septal defect, a patent ductus arteriosus, an atrioventricular septal defect) or from valvar regurgitation; the extra venous return floods and dilates the left heart. Pressure overload comes from an outflow obstruction (aortic stenosis, coarctation) or from pulmonary hypertension; the ventricle hypertrophies, becomes stiff, and fails first in diastole and then in systole. Pump failure comes from an intrinsic disease of the muscle — most often a dilated cardiomyopathy, or an acute myocarditis — in which contractility is lost and the ejection fraction falls. [3] [6]
Epidemiology & Risk Factors
Congenital heart disease is the commonest cause of heart failure in infants. Hoffman and Kaplan's landmark incidence review established that congenital heart disease affects roughly nine per thousand live births, and van der Linde's worldwide birth-prevalence meta-analysis confirmed a similar figure across populations. The lesions most likely to produce infant heart failure are the moderate-to-large left-to-right shunts (ventricular septal defect, patent ductus arteriosus, atrioventricular septal defect) and the obstructive lesions (coarctation, aortic stenosis), together with the duct-dependent lesions that collapse in the newborn period. [1] [2]
Outside the structural lesions, dilated cardiomyopathy is the commonest cardiomyopathy of childhood and the commonest reason for paediatric heart transplantation. The Pediatric Cardiomyopathy Registry has defined its epidemiology and prognosis, identifying elevated resting heart rate and progressive left ventricular remodelling as independent predictors of mortality. The acquired causes — myocarditis (often viral), Kawasaki disease with coronary involvement, anthracycline cardiotoxicity in oncology survivors, and tachycardia-induced cardiomyopathy from an uncontrolled supraventricular tachycardia — account for most of the remainder. [8] [9]
The risk factors therefore divide into the genetic and syndromic (trisomy 21 with atrioventricular septal defect, 22q11 deletion with conotruncal disease), the perinatal (prematurity with a patent ductus), the acquired (viral myocarditis, Kawasaki disease), and the iatrogenic (anthracycline exposure). The practical point is that the cause is usually identifiable, and once identified it is often treatable — which is the central optimism of paediatric heart failure. [1] [6]
Pathophysiology
Heart failure produces its syndrome through two failure modes that often coexist. Forward failure is the low-cardiac-output mode: the ventricle cannot eject enough blood, so perfusion falls and the child shows cool mottled skin, weak pulses, prolonged capillary refill, fatigue, poor feeding and growth failure. Backward failure is the raised-filling-pressure mode: blood dams up behind the failing ventricle, so the left side floods the lungs (tachypnoea, crackles, wheeze) and the right side congestes the venous system (hepatomegaly, raised venous pressure). In infants, hepatomegaly is the dominant backward-failure sign because peripheral oedema is unreliable. [3]
Whichever the initial insult — a shunt that overfills the ventricle, an obstruction that overstresses it, or a myocardium that cannot contract — the failing pump activates the same neurohormonal cascade. The sympathetic nervous system drives tachycardia and vasoconstriction to protect blood pressure; the renin-angiotensin-aldosterone system retains sodium and water to protect filling; antidiuretic hormone retains free water. Each of these briefly supports the cardiac output, which is why the child initially compensates and can look deceptively well. [3]
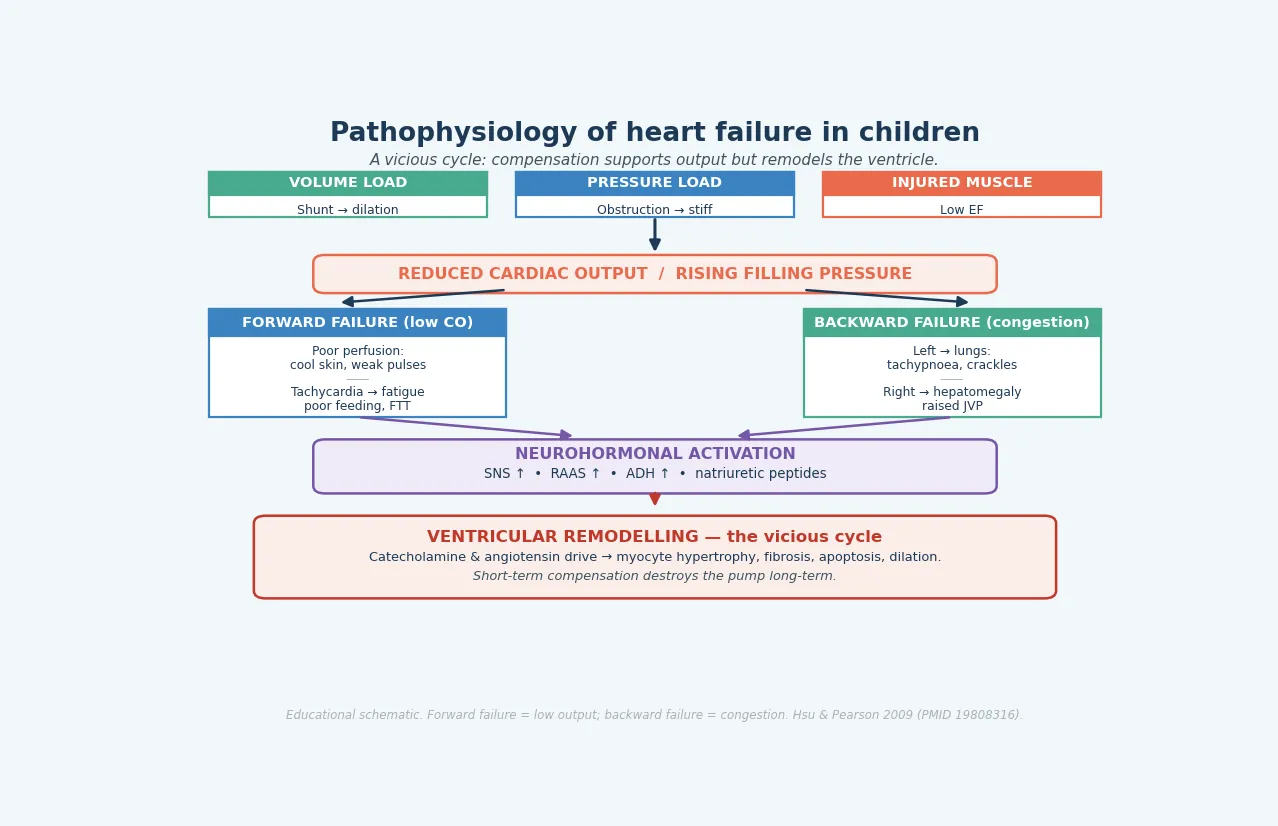
The trap is that this same neurohormonal activation, sustained over weeks and months, is exactly what destroys the ventricle. Chronic catecholamine and angiotensin drive produce myocyte hypertrophy, interstitial fibrosis, myocyte apoptosis and progressive chamber dilation — ventricular remodelling. The compensation that saved output in the short term becomes the disease in the long term. This single insight is the entire rationale for chronic neurohormonal therapy: an ACE inhibitor and a beta-blocker are given not to treat today's symptoms but to interrupt the remodelling cycle and protect the ventricle from the body's own response. [3] [4]
Clinical Presentation
The presentation of heart failure in a child is age-dependent, and recognising it depends on asking the right questions for the age. In an infant, exertion is feeding and growth, so heart failure shows itself as tachypnoea (especially with feeds), sweating during feeds, prolonged feeding time, poor weight gain crossing centiles downward, and recurrent lower respiratory infections. On examination there is a hyperactive precordium, a murmur of the underlying lesion, an apical mid-diastolic flow rumble if the shunt is large, a gallop rhythm in cardiomyopathy, and hepatomegaly as the backward-failure sign. [3] [6]
In an older child, exertion is exercise, so heart failure shows itself as exercise intolerance, fatigue, dyspnoea on exertion, abdominal pain from hepatic congestion, and poor growth. The history must probe what the child can no longer do — the sports they have dropped, the distance they can walk, the stairs they can climb — because exercise limitation is often the first and only symptom. A careful feeding and growth history is still essential, because growth failure may have preceded the symptomatic decline by months. [4]
Decompensated or low-output failure presents differently again: the child is grey and mottled, with cool peripheries, weak or thready pulses, prolonged capillary refill, marked tachycardia, oliguria and altered consciousness. This is the pre-shock or shock picture, and it is an emergency. The duct-dependent lesions add a specific newborn pattern: a well infant who collapses in the first days of life as the ductus closes, presenting with shock and poor perfusion rather than congestion, and requiring prostaglandin E1 within minutes. [3] [6]
Differential Diagnosis
The infant presenting with tachypnoea and poor feeding generates a broad differential, and the error is to anchor on the respiratory or the gastrointestinal system and miss the heart. The common alternatives are bronchiolitis and pneumonia (respiratory signs predominate, the liver is not enlarged, the chest radiograph shows focal changes rather than cardiomegaly), sepsis and metabolic acidosis (the child is systemically ill with a metabolic acidosis and a normal heart on echo), and anaemia (a flow murmur and pallor, but no cardiomegaly). A careful examination for hepatomegaly, a murmur and the character of the pulse, together with a chest radiograph and an echocardiogram, resolves most of these. [3] [6]
Within heart failure itself, the differential is the mechanism. A large left-to-right shunt gives a pansystolic murmur, a hyperactive precordium and an apical flow rumble. An obstructive lesion gives the murmur and blood-pressure pattern of the obstruction — absent femoral pulses and a pressure differential between the arms and legs in coarctation, an ejection murmur radiating to the neck in aortic stenosis. A cardiomyopathy gives a quiet precordium, a gallop rhythm and a displaced apex with no flow murmur. Acute myocarditis adds a viral prodrome and a rapid deterioration. [4]
The must-not-miss mimics are the ones that kill quickly if missed. A supraventricular tachycardia sustained over days produces a tachycardia-induced cardiomyopathy that resolves completely when the rhythm is controlled, so any infant with a heart rate at the upper limit of normal and heart failure needs an ECG. A duct-dependent lesion collapses when the ductus closes and is fatal without prostaglandin, so any newborn with shock and poor perfusion gets prostaglandin E1 while the echocardiogram is organised. Septic shock and an inborn error of metabolism can mimic cardiogenic shock, and a lactate, a septic screen and a metabolic panel are part of the first bloods. [3] [4]
Clinical & Bedside Assessment
Bedside assessment begins with growth, feeding and perfusion, because these quantify the haemodynamic weight of the failure better than any single sign. Plot the weight and height, and ask how the weight centiles have trended — a thriving infant who has crossed two centiles downward over weeks has significant failure until proven otherwise. Quantify the feeds: the volume per feed, the time taken, whether the child sweats, breathes fast or tires, and whether they ever go blue. Then assess perfusion with capillary refill, pulse volume and skin temperature, and palpate the liver edge, which is the most reliable backward-failure sign in an infant and the most reliable marker of response to therapy. [3] [6]
The cardiovascular examination then reveals the mechanism. Characterise the murmur (site, timing, quality, grade, radiation), feel the precordium for a hyperactive impulse or a right ventricular heave, locate the apex for displacement, listen to the second heart sound for a loud pulmonary component suggesting pulmonary hypertension, and take the blood pressure and four-limb pulses to detect coarctation. A gallop rhythm (a third heart sound) is the auscultatory signature of a failing ventricle and points to a cardiomyopathy or myocarditis rather than an overcirculation lesion. [4]
Severity is graded at the bedside with the modified Ross classification, which converts the clinical findings into a class I to IV that guides urgency and tracks response. A child who moves from class III to class II on therapy is improving; a child who moves from class II to class IV is deteriorating and needs escalation. The Ross score, the weight trend, the feed tolerance and the liver size together are the bedside dashboard of heart failure, and they are the measurements that should be documented at every review. [5]
Investigations
Echocardiography is the definitive investigation for paediatric heart failure and in most children it is the only cardiac imaging required. It defines the structural lesion, measures the chamber sizes, estimates the ventricular function and ejection fraction, estimates the pulmonary artery pressure from the tricuspid regurgitation jet and any shunt, assesses valve competence, and identifies a pericardial effusion or an intracardiac thrombus. In a child with suspected heart failure, the echocardiogram is the investigation that names the mechanism, and it should be obtained as soon as the diagnosis is entertained. [4] [6]
The electrocardiogram is supportive rather than diagnostic, but it is essential because it reveals the arrhythmias and the ischaemic and hypertrophic patterns that point to aetiology. A tachycardia-induced cardiomyopathy shows a sustained supraventricular tachycardia or pre-excitation; a dilated cardiomyopathy may show left ventricular hypertrophy with strain or a conduction abnormality; myocarditis can show non-specific ST and T changes, low voltages or, in fulminant disease, a normal ECG that belies a desperately sick heart; an obstructive lesion shows the voltage criteria for ventricular hypertrophy. The chest radiograph shows cardiomegaly, pulmonary venous congestion, pulmonary oedema and pleural effusion, though a normal heart size does not exclude heart failure, particularly in restrictive physiology. [4]
Blood tests support the diagnosis and the management. Troponin and NT-proBNP help to distinguish myocarditis and to grade severity and prognosis. A full blood count, electrolytes, renal and liver function, and a lactate assess the end-organ consequences of low output and guide diuretic and fluid therapy. A septic screen and a metabolic panel are part of the first bloods in any sick infant, because sepsis and inborn errors of metabolism can mimic cardiogenic shock. In the cardiomyopathies, genetic testing is increasingly part of the workup because it refines prognosis and family counselling. Cardiac MRI and, in selected cases, angiography add tissue characterisation and haemodynamic detail in the complex cardiomyopathies and myocarditis. [4] [9]
Management — Resuscitation
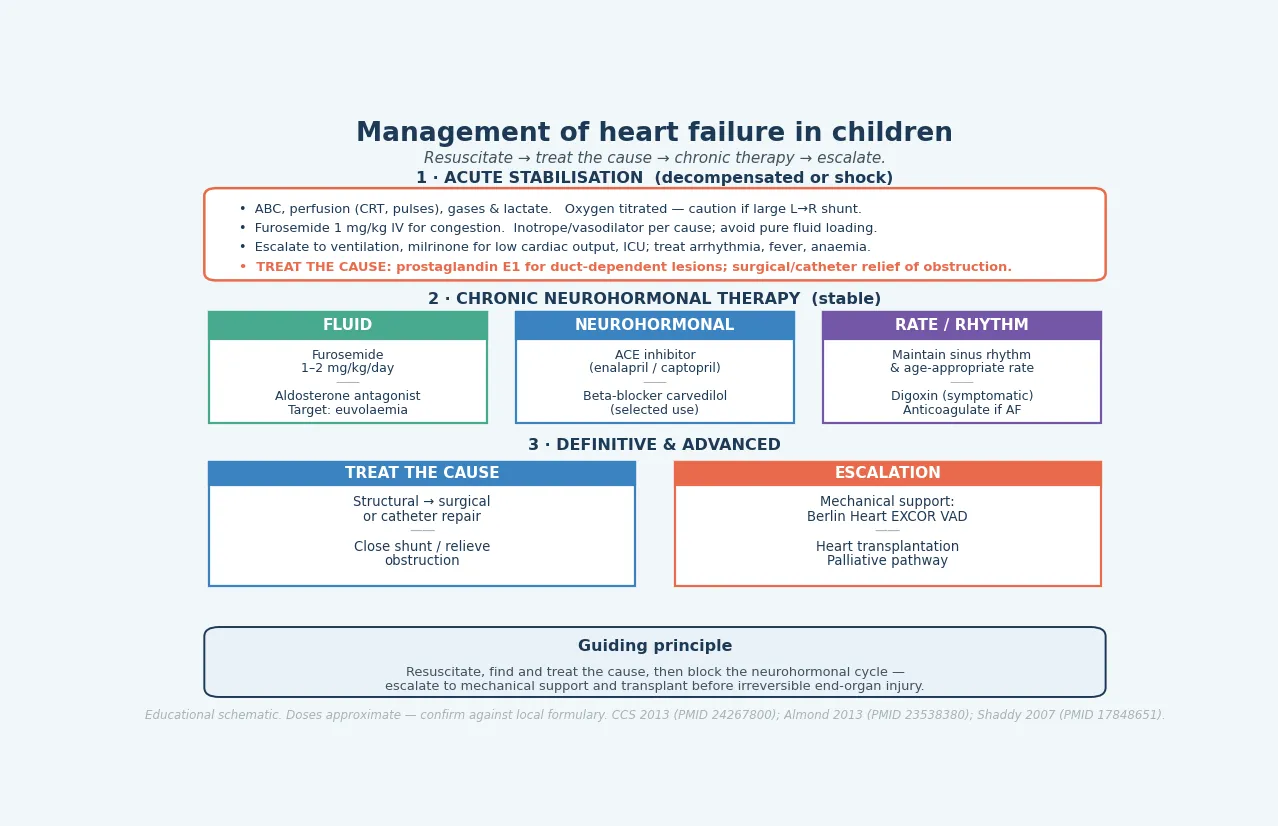
The resuscitation scenario is the infant or child presenting in decompensated heart failure or cardiogenic shock. The priority is to secure the airway and breathing, improve perfusion, relieve congestion, and treat the cause. Assess ABC, perfusion (capillary refill, pulse volume), work of breathing, and send a blood gas and lactate. Give oxygen, but titrate it to saturations and remember that in a large left-to-right shunt oxygen is a pulmonary vasodilator that can worsen the overcirculation. A loop diuretic such as furosemide 1 mg/kg intravenously relieves pulmonary congestion. Select the vasoactive agent by the cause: a low-output state may need an inotrope such as milrinone, while pure fluid loading is avoided because it worsens the failing ventricle. [3] [6]
Escalation is early and decisive. A child in respiratory failure needs non-invasive or invasive ventilation, which also reduces the work of breathing and the metabolic demand on the failing heart. A child with a low cardiac output that does not respond to the first measures needs milrinone and intensive-care admission, and consideration of mechanical circulatory support. Any arrhythmia, fever or anaemia that is driving the decompensation is treated promptly, because each can tip a compensated child into shock. [6]
Furosemide (acute decompensated paediatric heart failure)
Loading dose
1 mg/kg PO/IV
Maintenance dose
1–2 mg/kg/day in 1–2 divided doses
The single most important resuscitation principle is that acute therapy is a bridge to definitive treatment of the cause, not a substitute for it. The child with a duct-dependent lesion needs prostaglandin E1 within minutes. The child with a tachyarrhythmia needs rate or rhythm control. The child with an obstructive lesion needs surgical or catheter relief. The child with a shunt needs closure. Resuscitation buys the time to deliver the cure, and the cure is almost always the treatment of the underlying cause. [3] [6]
Immediate management of decompensated paediatric heart failure
Assess ABC, perfusion, work of breathing; send gas, lactate, tropanin, FBC, electrolytes, septic and metabolic screen
Titrate oxygen to saturations — caution with large left-to-right shunts
Give a loop diuretic (furosemide 1 mg/kg IV) for congestion
Select inotrope/vasodilator by cause (milrinone for low cardiac output); avoid pure fluid loading
Escalate to non-invasive/invasive ventilation and ICU as needed
Treat any arrhythmia, fever or anaemia driving the decompensation
Give prostaglandin E1 immediately if a duct-dependent lesion is suspected
Obtain urgent echocardiography to name the mechanism and guide definitive therapy
Management — Definitive & Stepwise
Definitive management follows the mechanism. For the volume-overload shunts, definitive therapy is closure of the shunt — surgical or transcatheter — once the infant has been stabilised and has grown enough for a safe repair, usually within the first year. For the pressure-overload obstructions, definitive therapy is relief of the obstruction: surgical repair or balloon dilatation of coarctation, surgical or balloon valvotomy for aortic stenosis. For the pump failures, definitive therapy is chronic neurohormonal treatment of the cardiomyopathy, with escalation to mechanical support and transplantation if it remains refractory. The unifying point is that most childhood heart failure is surgically curable because the cause is structural. [4] [6]
For the child with stable compensated chronic failure — typically a cardiomyopathy, or a child awaiting definitive surgery — chronic neurohormonal therapy is built on three legs. A loop diuretic (furosemide 1 to 2 mg/kg/day, with an aldosterone antagonist for synergy) controls congestion and aims for euvolaemia. An ACE inhibitor (enalapril or captopril) reduces afterload and interrupts the renin-angiotensin limb of the remodelling cycle. A beta-blocker (carvedilol) is added in selected cases to interrupt the sympathetic limb. Rate and rhythm control, digoxin for symptomatic chronic failure, and anticoagulation when there is atrial fibrillation or an intracardiac thrombus complete the regimen. [4] [6]
The carvedilol evidence is the part that examiners most often probe, because it is the point where paediatric and adult heart-failure medicine diverge. In adults, beta-blockers improve survival in chronic heart failure, so they were assumed to do the same in children. The Shaddy randomised controlled trial of carvedilol in children and adolescents with heart failure, however, found no overall benefit over placebo — the trial was in fact stopped for futility, and the placebo response was unusually high. The implication is not that beta-blockers are useless in children, but that their use is selective rather than universal, and the evidence base is weaker than in adults. [7]
The Shaddy carvedilol trial — the paediatric evidence examiners expect
The Pediatric Carvedilol Trial (Shaddy et al, JAMA 2007) randomised 161 children and adolescents with heart failure to carvedilol versus placebo. The trial found no significant difference in the primary composite outcome, and it was stopped early for futility. A high rate of improvement in the placebo arm partly explained the result. The takeaway for practice is that carvedilol is used selectively in children with chronic heart failure, on the strength of physiologic rationale and adult data, but without the survival evidence that underpins its use in adults. [7]
For the refractory pump failure that does not respond to maximal medical therapy, the escalation pathway is mechanical circulatory support followed by transplantation. The Berlin Heart EXCOR paediatric ventricular assist device is the established paracorporeal pulsatile pump used as a bridge to transplantation in children, including small infants. Almond and colleagues' cohort established its use across US children, documenting survival to transplant and the complications of stroke and infection that shape the decision. Heart transplantation is the definitive therapy for end-stage cardiomyopathy and for selected structural disease that cannot be repaired, with excellent medium-term survival but lifelong immunosuppression and surveillance. When transplantation is not an option, a palliative care pathway is developed with the family. [10] [4]
[6] [7] [10]Specific Subtypes & Scenarios
Heart failure from a large left-to-right shunt is the archetype of the infant presentation and the one an examiner most often expects in depth. The ventricular septal defect, the patent ductus arteriosus and the atrioventricular septal defect each flood the pulmonary circulation as the pulmonary vascular resistance falls over the first weeks, dilate the left heart, and present at four to eight weeks with tachypnoea, sweating with feeds, failure to thrive and hepatomegaly. The mechanism is a volume load, the murmur is pansystolic at the lower left sternal border with an apical flow rumble, and the cure is closure of the shunt. Medical therapy is a bridge to that closure. [3] [1]
Heart failure from dilated cardiomyopathy is the paradigm of the pump-failure mechanism and the commonest reason for paediatric heart transplantation. The child presents with a gallop rhythm, a displaced apex and poor growth or exercise intolerance, and the echocardiogram shows a dilated, thin-walled left ventricle with a low ejection fraction. The Pediatric Cardiomyopathy Registry has refined the prognosis: elevated resting heart rate and progressive left ventricular remodelling are independent predictors of mortality, which guides the intensity of therapy and the timing of transplantation listing. Genetic testing is increasingly part of the workup because many dilated cardiomyopathies have a genetic basis that carries family implications. [8] [9]
Acute myocarditis is the scenario that can deteriorate fastest. A previously well child, often after a viral prodrome, develops tachypnoea, a gallop and hepatomegaly and can progress to cardiogenic shock within hours. Troponin is typically elevated, the echocardiogram shows a globally impaired ventricle that may be only mildly dilated, and the ECG may be non-specific. Management is supportive — haemodynamic stabilisation, mechanical support if needed — with immunomodulation (intravenous immunoglobulin or steroids) used in selected centres. The outcome divides between full recovery and progression to a transplant-listed dilated cardiomyopathy, and the early phase is the most dangerous. [4]
Across Australia, New Zealand and the United Kingdom, paediatric heart failure is managed within tertiary paediatric cardiology networks that provide echocardiography, surgical and catheter intervention, and, in the national centres, mechanical circulatory support and transplantation. Rural and remote children are retrieved to the tertiary centre once heart failure is recognised, and shared-care follow-up is built around the local paediatrician and the cardiology team. The thresholds for transplantation listing and the protocols for mechanical support are set by the national paediatric cardiac service, and the family is supported through the transition to adult congenital or heart-failure care in adolescence. [6] [11]
Complications & Pitfalls
The complications of paediatric heart failure are the consequences of a failing pump sustained over time. Growth failure is nearly universal in the untreated infant, driven by the metabolic cost of the extra cardiac work and the anorexia of congestion. Recurrent respiratory infection follows from the pulmonary congestion. Arrhythmia — both atrial and ventricular — accompanies the dilated, fibrotic ventricle and is a mode of sudden death. Thromboembolism arises from stasis in the dilated chambers. End-organ injury — renal, hepatic, and neurological — follows sustained low output. Without treatment, the outcome is death; with modern therapy, the outcome is usually good because the cause is treatable. [3] [4]
The pitfalls are about recognition and about the misuse of therapy. The first is the diagnostic pitfall of attributing infant tachypnoea and poor feeding to reflux, bronchiolitis or feeding technique, and delaying echocardiography until the child is in shock. The second is the oxygen pitfall: giving indiscriminate high-flow oxygen to an infant with a large left-to-right shunt lowers pulmonary vascular resistance, increases the shunt and worsens the overcirculation. The third is the evidence pitfall: over-applying the adult carvedilol survival benefit when the paediatric trial was negative, or, conversely, withholding proven neurohormonal therapy on the grounds that one drug class lacks paediatric evidence. [3] [7]
Prognosis & Disposition
The prognosis of paediatric heart failure depends almost entirely on the mechanism and on whether the cause is treated. A structural lesion repaired in infancy, before the onset of fixed pulmonary vascular disease, has an excellent long-term outlook, with most children achieving normal growth, activity and quality of life. A dilated cardiomyopathy has a more guarded and more variable outlook: the Pediatric Cardiomyopathy Registry has shown that elevated resting heart rate and progressive left ventricular remodelling independently predict mortality, which is why these markers guide the intensity of therapy and the timing of transplantation listing. Acute myocarditis divides between full recovery and progression to a transplant-listed cardiomyopathy, with the fulminant presentation carrying the highest early risk. [8] [9]
Mechanical circulatory support and heart transplantation have transformed the prognosis of refractory failure. The Berlin Heart EXCOR ventricular assist device, established by the Almond cohort, provides effective bridging to transplantation in children including small infants, with documented survival to transplant and a defined complication profile of stroke and infection. Heart transplantation offers excellent medium-term survival for end-stage cardiomyopathy and selected unrepairable structural disease, at the cost of lifelong immunosuppression and surveillance. When transplantation is not an option, a palliative care pathway is built with the family around symptom control and quality of life. [10] [4]
Disposition follows the severity and the mechanism. Every child with confirmed or suspected heart failure is referred to paediatric cardiology for echocardiographic definition and a management plan. A compensated, stable child is followed in the outpatient clinic; a decompensated or refractory child is managed in a tertiary paediatric intensive care unit with access to mechanical support and transplantation. The infective endocarditis prophylaxis position is set by the 2021 American Heart Association statement, which restricts routine antibiotic prophylaxis to high-risk groups (prosthetic valves, prior endocarditis, selected complex unrepaired or repaired lesions), placing the emphasis on good oral hygiene and the prompt evaluation of unexplained fever. Adolescents with chronic failure or a transplanted heart are transitioned to adult congenital or heart-failure services through a structured handover. [12] [11]
Special Populations
The syndromic infant is the first special population. Trisomy 21 carries a high rate of atrioventricular septal defects; 22q11 deletion carries conotruncal disease and brings immunodeficiency, hypocalcaemia and airway anomalies that shape perioperative care. Each syndrome changes the counselling, the surveillance and sometimes the surgical timing, and a confirmed heart-failure lesion in a dysmorphic infant mandates a genetics assessment. [1]
The preterm infant is the second. Premature babies frequently have a patent ductus arteriosus that can produce a significant left-to-right shunt and a volume-load failure, and they may also have a cardiomyopathy of prematurity or a bronchopulmonary dysplasia-related right-heart load. Management balances the haemodynamic burden against the risks of medical (indomethacin, ibuprofen, paracetamol) and surgical closure in a small, fragile patient, and the threshold is set by the local neonatal and cardiology team. [6]
The adolescent with chronic heart failure or a transplanted heart is the third and the most complex. Adherence to a demanding medication regimen becomes the central issue, and the transition to adult care must be planned, structured and gradual. Contraception and pregnancy counselling are essential, because pregnancy carries substantial risk in a failing or a transplanted heart. Psychological support, school engagement and peer relationships are part of the care, because the burden of chronic disease in adolescence is as much psychosocial as it is cardiac. [11]
The rural or remote child is the fourth. Distance from the tertiary centre delays echocardiography and intervention, so the paediatric heart-failure strategy in rural and remote settings is built on a high index of suspicion in primary care, timely retrieval to a tertiary paediatric cardiology centre, and shared-care follow-up that keeps the child connected to both the local paediatrician and the cardiology team. [6]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric heart failure is anchored on a small set of seminal sources. The Hsu and Pearson two-part review (2009) established the modern framework for the history, pathophysiology, diagnosis and treatment of heart failure in children, and it remains the reference to cite for the syndrome as a whole. The Kantor Canadian Cardiovascular Society guidelines (2013) distilled the presentation, diagnosis and medical management into a practical framework that guides therapy. The Ross age-stratified revision (2012) refined the severity classification that bears his name. [3] [4] [5] [6]
The treatment evidence divides into the pharmacological and the mechanical. The pharmacological centrepiece is the Shaddy carvedilol randomised controlled trial (2007), which found no overall benefit of carvedilol in children and adolescents with heart failure — the paediatric counterpoint to the adult beta-blocker survival evidence, and the reason beta-blockade is selective rather than universal in children. The mechanical-support centrepiece is the Almond Berlin Heart EXCOR cohort (2013), which established the paediatric ventricular assist device as a bridge to transplantation in US children and defined its survival and complication profile. [7] [10]
The prognosis evidence comes from the Pediatric Cardiomyopathy Registry, which has defined the natural history of childhood cardiomyopathy in population-based cohorts. Rossano and colleagues (2020) showed that elevated resting heart rate is associated with worse survival in dilated cardiomyopathy, and Kantor and colleagues (2024) showed that progressive left ventricular remodelling independently predicts mortality. Together these markers — heart rate and remodelling — guide the intensity of therapy and the timing of transplantation listing. [8] [9]
The guideline landscape is completed by the 2020 European Society of Cardiology adult congenital heart disease guidelines, which frame the transition and lifelong care of the adolescent with repaired or unrepaired congenital disease, and by the 2021 American Heart Association infective endocarditis statement, which restricted routine antibiotic prophylaxis to high-risk groups and shifted the emphasis to oral hygiene and prompt fever evaluation. Across ANZ, the United Kingdom, Europe and North America, the consensus is uniform in principle: find and treat the cause, block the neurohormonal cycle, escalate to mechanical support and transplantation before irreversible injury, and transition the adolescent to lifelong adult care. [11] [12]
The single message that unifies regional practice is that most childhood heart failure is surgically curable because the cause is structural. The thresholds for closure versus surveillance, the device-versus-surgery decision, the listing criteria for transplantation, and the endocarditis-prophylaxis rules vary in detail by guideline body and centre, but the central strategy — find the mechanism, treat the cause, block the neurohormonal cycle, and escalate before irreversible injury — is uniform across high-resource settings. [6] [10] [11]
Exam Pearls
Heart-failure mechanism lanes — 'VPP-RAD'
References
- [1]Hoffman JI; Kaplan S The incidence of congenital heart disease. J Am Coll Cardiol, 2002.PMID 12084585
- [2]van der Linde D; Konings EE; Slager MA; Witsenburg M; Helbing WA; Takkenberg JJ; Roos-Hesselink JW Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol, 2011.PMID 22078432
- [3]Hsu DT; Pearson GD Heart failure in children: part I: history, etiology, and pathophysiology. Circ Heart Fail, 2009.PMID 19808316
- [4]Hsu DT; Pearson GD Heart failure in children: part II: diagnosis, treatment, and future directions. Circ Heart Fail, 2009.PMID 19808380
- [5]Ross RD The Ross classification for heart failure in children after 25 years: a review and an age-stratified revision. Pediatr Cardiol, 2012.PMID 22476605
- [6]Kantor PF; Lougheed J; Dancea A; McGillion M; Barbosa N; Chan W; Cherney DZ; Gandhi S; Holtby HM; Human DG; McCrindle BW; Prieur T; Conway J; Canadian Cardiovascular Society Presentation, diagnosis, and medical management of heart failure in children: Canadian Cardiovascular Society guidelines. Can J Cardiol, 2013.PMID 24267800
- [7]Shaddy RE; Boucek MM; Hsu DT; Boucek RJ; Sanders SP; Mineral S; Pahl E; Miyamoto SD; Tresed M; Pediatic Carvedilol Study Group Carvedilol for children and adolescents with heart failure: a randomized controlled trial. JAMA, 2007.PMID 17848651
- [8]Rossano JW; Kantor PF; Shaddy RE; Shi L; Lipshultz SE; Colan SD; Sleeper LA; Towbin JA; Jefferies JL; Everitt MD; Hsu DT; Wilkinson JD; Pediatric Cardiomyopathy Registry Elevated heart rate and survival in children with dilated cardiomyopathy: a multicenter study from the Pediatric Cardiomyopathy Registry. J Am Heart Assoc, 2020.PMID 32750307
- [9]Kantor PF; Shi L; Colan SD; Orav EJ; Mayer JE; Sleeper LA; Lipshultz SE; Pediatric Cardiomyopathy Registry Progressive left ventricular remodeling for predicting mortality in children with dilated cardiomyopathy: the Pediatric Cardiomyopathy Registry. J Am Heart Assoc, 2024.PMID 38214257
- [10]Almond CS; Morales DL; Blackstone EH; Turrentine MW; Imamura M; Massicotte MP; Jordan LC; Meyer DM; Das NA; Lorts A; Morales RS; Davies RR; Nikaidoh H; Muenzer JR; Rosenthal DN; Morell VO; Kanter KR; Mahle WT; Fraser CD Jr Berlin Heart EXCOR pediatric ventricular assist device for bridge to heart transplantation in US children. Circulation, 2013.PMID 23538380
- [11]Baumgartner H; De Backer J; Babu-Narayan SV; Budts W; Chessa M; Diller GP; Lung B; Kluin J; Lang IM; Meijboom F; Moons P; Mulder BJM; Oechslin E; Roos-Hesselink JW; Schwerzmann M; Sullebarger L; Van Hare GF; ESC Scientific Document Group 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J, 2020.PMID 33128054
- [12]Wilson WR; Gewitz M; Lockhart PB; Bolger AF; DeSimone DC; Koenig MJ; Sadhu Lohr J; Miro JM; Padera RF; Prendergast BD; Sexton DJ; Spelman DW; Tleyjeh IM; Van der Meer JTM; Westermann CJL; Whited W; Wojda TR; American Heart Association Prevention of Viridans Group Streptococcal Infective Endocarditis: A Scientific Statement From the American Heart Association. Circulation, 2021.PMID 33853363