Paeds · cardiology
Hypertension in children
Also known as Paediatric hypertension · High blood pressure in children · Childhood hypertension · Elevated blood pressure in children · Secondary hypertension in children · Ambulatory blood pressure monitoring in children
Fellowship guide to hypertension in children: the AAP 2017 definition based on age, sex and height percentiles, the rule that elevated office blood pressure must be confirmed by ambulatory monitoring before a label is fixed, the search for a secondary cause (renal, renovascular, endocrine, coarctation) in any young or stage 2 child, and the threshold — left ventricular hypertrophy — at which drug therapy becomes mandatory.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The organising idea of this topic is that childhood hypertension is a diagnosis of confirmation, stratification and trigger, not of a single cuff reading. The American Academy of Pediatrics 2017 guideline reframed the field: it dropped the term prehypertension, introduced an elevated category, lowered the drug-treatment threshold, and made ambulatory monitoring the standard for confirmation. [1] Every step of the clinical pathway flows from that framework — measure, confirm, search for a cause, look for target-organ damage, and treat to a target. [7]
This page covers the measurement technique, the percentile-based classification, the primary-versus-secondary split, the work-up for target-organ damage, the lifestyle and pharmacological management, and the regional differences between the AAP and European Society of Hypertension approaches. It links to coarctation and chronic kidney disease leaves for the curable secondary causes that every candidate must be able to name. [3] [8]
Overview & Definition
Blood pressure in children is a continuous variable that rises with age, body size and pubertal maturation, so a reading that is normal for a tall sixteen-year-old is hypertensive for a small six-year-old. The definition is therefore percentile-based, anchored to normative data from healthy children. The 2017 AAP clinical practice guideline defines normal blood pressure as below the 90th percentile for age, sex and height (or below 120/80 mmHg for adolescents aged 13 years and older), elevated blood pressure as the 90th to below the 95th percentile (or 120/80 to below the blood-pressure-based threshold for adolescents), stage 1 hypertension as the 95th percentile to below the 95th percentile plus 12 mmHg, and stage 2 hypertension as at or above the 95th percentile plus 12 mmHg. [1]
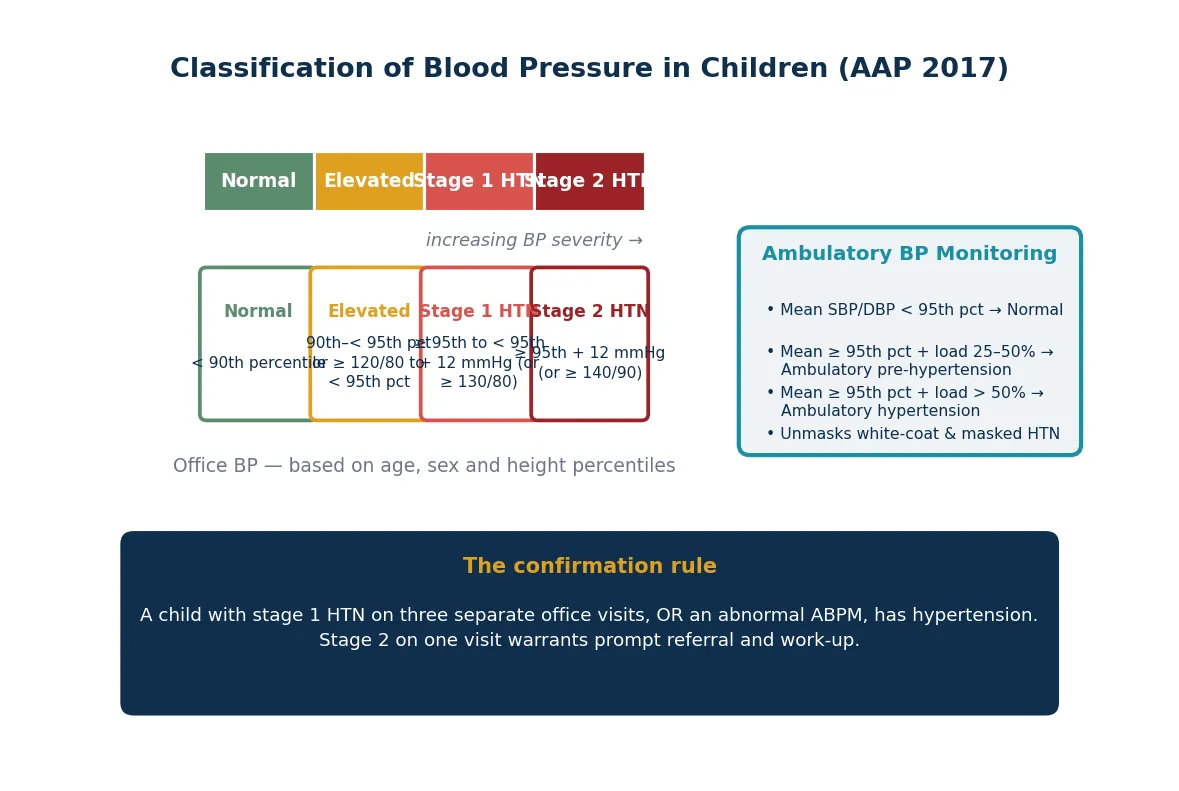
The practical corollary is that no child is labelled hypertensive on the basis of one reading. The diagnosis of office hypertension requires elevated or stage 1 readings on three separate occasions, or confirmation by 24-hour ambulatory blood pressure monitoring. A child with stage 2 readings is referred promptly and evaluated rather than watched. This rule protects children from the consequences of mislabelling — anxiety, restricted activity, insurance and employment effects — while ensuring that genuine disease is not missed. [1] [9]
Classification
The AAP 2017 classification replaced the earlier prehypertension category with two separate bands — elevated blood pressure and stage 1 hypertension — and aligned the adolescent (13 years and older) thresholds with the adult categories of 120/80 and 130/80 mmHg. The fourth report of 2004, which used a single prehypertension band from the 90th to below the 95th percentile, remains the historical reference and the basis of many normative tables. [2]
[1]Ambulatory blood pressure monitoring adds its own classification layer. Mean systolic or diastolic blood pressure below the 95th percentile is normal; a mean at or above the 95th percentile with a blood-pressure load (the proportion of readings above threshold) of 25 to 50 per cent is ambulatory pre-hypertension; and a mean at or above the 95th percentile with a load above 50 per cent is ambulatory hypertension. The monitoring study also distinguishes white-coat hypertension (elevated office, normal ambulatory) from masked hypertension (normal office, elevated ambulatory), a distinction that office readings alone cannot make. [3] [5]
Epidemiology & Risk Factors
The prevalence of childhood hypertension has risen over the last two decades, driven principally by the obesity epidemic. Population studies place the prevalence of sustained hypertension at around 3 to 5 per cent of children and adolescents, with elevated blood pressure in a further 10 to 15 per cent. The figure is higher among children with obesity, where prevalence approaches 10 per cent or more. A landmark study of electronic health records found that the majority of children with elevated blood pressure went undiagnosed, exposing the central practice failure that the 2017 guideline sought to correct. [4]
The risk factors for primary hypertension are the same as those for adult cardiovascular disease: obesity, a family history of hypertension, high dietary sodium, low physical activity, sleep disturbance and obstructive sleep apnoea. Secondary hypertension has a different epidemiology — it is concentrated in younger children, in those with known renal or cardiac disease, and in those presenting with stage 2 blood pressures — which is why the age and severity of presentation drive the intensity of the work-up. [7]
Pathophysiology
The blood pressure is the product of cardiac output and systemic vascular resistance, and sustained elevation reflects a sustained increase in one or both. In primary hypertension the mechanism is multifactorial: obesity-driven insulin resistance and hyperleukaemia, sympathetic nervous system overactivity, activation of the renin–angiotensin–aldosterone system, and impaired sodium excretion with endothelial dysfunction. No single defect explains it, which is why primary hypertension is a diagnosis of exclusion made after secondary causes are sought and excluded. [1]
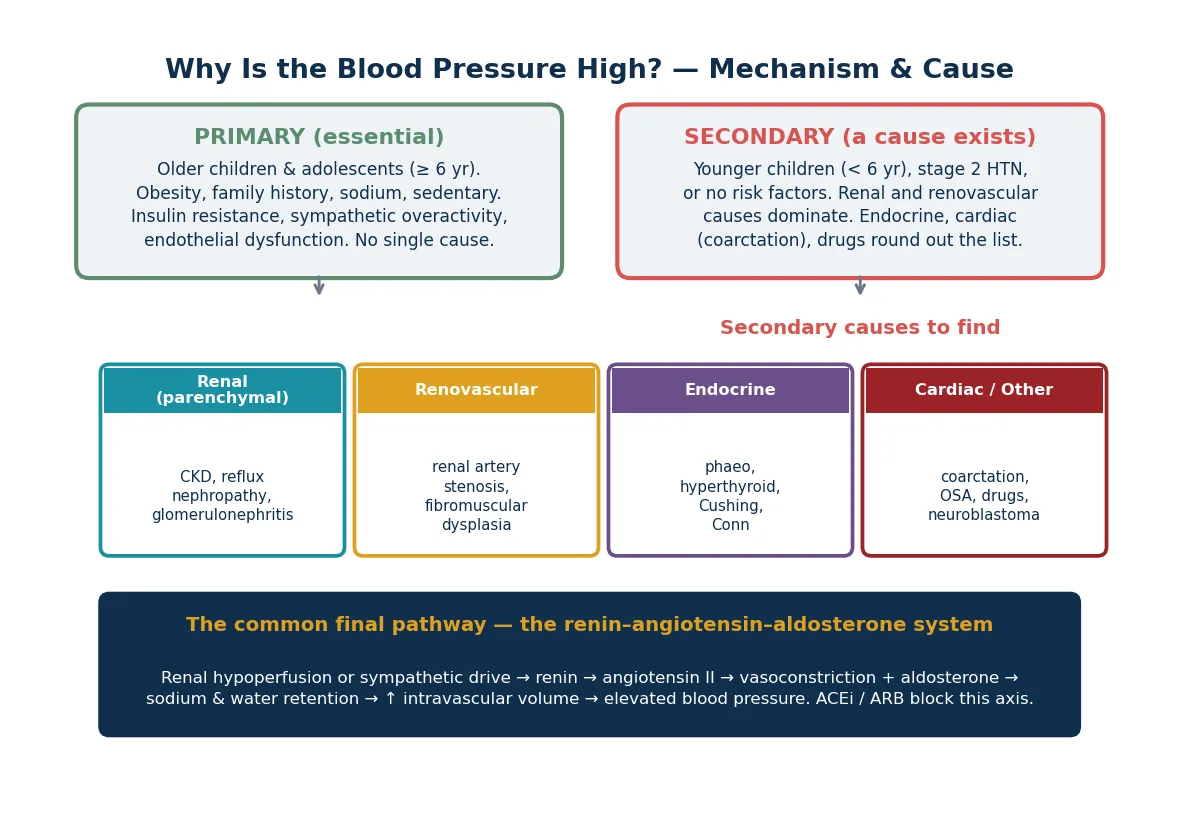
Secondary hypertension has a discrete mechanism tied to its cause. Renal parenchymal disease (chronic kidney disease, reflux nephropathy, glomerulonephritis) raises blood pressure through volume overload and renin release from ischaemic tissue. Renovascular disease (renal artery stenosis, fibromuscular dysplasia) causes renin-driven hypertension by perfusing a low-pressure kidney that signals volume depletion. Endocrine causes (phaeochromocytoma, mineralocorticoid excess, Cushing syndrome, hyperthyroidism) act through hormone-driven vasoconstriction or volume expansion. Coarctation of the aorta raises upper-body pressure by mechanical obstruction. The unifying therapeutic insight is that the renin–angiotensin–aldosterone system is the common final pathway for the two largest secondary groups — renal and renovascular — which is why angiotensin-converting-enzyme inhibitors and angiotensin-receptor blockers are first-line when the cause is renal. [8]
Clinical Presentation
Most children with hypertension are asymptomatic and are detected by screening — the reason the AAP guideline mandates annual blood pressure measurement from the age of three years at every routine visit, and at every visit from birth in children with risk factors. Symptomatic presentation falls on a spectrum from non-specific complaints to life-threatening hypertensive emergency. [1]
The history targets symptoms (headache, epistaxis, visual change, exercise intolerance, abdominal pain), lifestyle (diet, activity, sleep, screen time), family history (early cardiovascular disease, hypertension, renal disease), and the markers of secondary causes — failure to thrive, recurrent urinary tract infections, abdominal masses, limb cramping (suggesting coarctation), sweating and palpitation (suggesting phaeochromocytoma), and drug exposure (corticosteroids, sympathomimetics, oral contraceptives). [7]
The examination centres on four-limb blood pressure measurement. The cuff must cover 80 per cent of the upper arm; a cuff too small overestimates pressure. Measure the right arm first, then the legs. An arm-to-leg systolic gradient above 20 mmHg with weak or delayed femoral pulses identifies coarctation and earns an echocardiogram. The rest of the examination looks for the stigmata of secondary disease — oedema, abdominal bruit or mass, Turner phenotype, skin striae, thyromegaly — and for target-organ damage: fundoscopy for hypertensive retinopathy and a focused cardiac examination for left ventricular heave or a murmur. [9]
Differential Diagnosis
The first differential is not between diseases but between real and artefactual elevation. Cuff size error, anxiety, recent activity, caffeine and pain all raise blood pressure transiently. White-coat hypertension — elevated in the office but normal on ambulatory monitoring — accounts for up to half of referred children and must be excluded before any investigation or treatment. [5]
Once the elevation is confirmed, the differential is between primary and secondary hypertension. The age, the severity and the history divide them. [1]
Primary versus secondary hypertension: the clinical divide
The specific secondary causes to distinguish are renal parenchymal disease (the largest single group, suggested by abnormal urinalysis, raised creatinine or a small or scarred kidney on ultrasound), renovascular disease (suggested by abdominal bruit, severe or resistant hypertension, and renal-size asymmetry), coarctation (suggested by the four-limb gradient), endocrine causes (suggested by symptoms and signs of hormone excess), and drug-related or sleep-apnoea-related hypertension. The link to phaeochromocytoma and endocrine hypertension is covered in its own leaf. [8]
Clinical & Bedside Assessment
The bedside assessment begins with correct technique. The child should be seated and relaxed for at least five minutes, feet on the floor, arm supported at heart level, and the right size cuff (bladder covering 80 per cent of the arm circumference). Auscultation remains the reference standard; oscillometric devices are acceptable for screening but elevated readings must be confirmed by auscultation. [9]
The four-limb blood pressure check
Seat the child calmly for five minutes, right arm supported at heart level.
Measure the right arm with the correct cuff by auscultation.
Measure both legs (dorsalis pedis or posterior tibial, or popliteal with a large cuff).
Compare arm and leg systolic values: a leg systolic more than 10 mmHg below arm, or an arm-to-leg gradient above 20 mmHg, is coarctation until excluded.
Palpate femoral pulses: weak, absent or delayed (radio-femoral delay) reinforces coarctation.
The rest of the bedside assessment screens for the secondary causes and for target-organ damage. Look for growth parameters (failure to thrive points to systemic disease), the facies and habitus of syndromes (Turner, Cushing), abdominal masses (polycystic kidneys, hydronephrosis, neuroblastoma, Wilms tumour), an abdominal bruit (renovascular disease), peripheral oedema and pallor (renal disease), skin lesions (neurofibromas, café-au-lait spots suggesting renovascular disease; striae suggesting Cushing), and the cardiovascular signs of left ventricular hypertrophy or heart failure. Fundoscopy assesses hypertensive retinopathy, the clearest bedside evidence that the blood pressure is causing end-organ damage. [7]
Investigations
The investigation strategy is tiered: a screening first-line panel for every confirmed hypertensive child, a target-organ assessment, and a directed second-line work-up for the child in whom a secondary cause is suspected. [1]
[1]Echocardiography is the single most important target-organ investigation. Left ventricular hypertrophy (LV mass index above the 95th percentile) is present in 10 to 20 per cent of untreated hypertensive children, and its presence is an indication to start drug therapy regardless of the blood pressure category. Renal ultrasound with Doppler screens for structural renal disease (scarring, dysplasia, cysts, size asymmetry) and for renovascular stenosis, though Doppler has limited sensitivity in young children and small vessels. Ambulatory blood pressure monitoring is now the standard for confirming the diagnosis, defining the pattern (white-coat, masked, nocturnal) and assessing nocturnal dipping, a marker of target-organ risk. [5]
Management — Resuscitation
Hypertensive emergency — symptomatic stage 2 hypertension with end-organ effects such as encephalopathy, acute heart failure or renal failure — is the one resuscitation scenario in childhood hypertension. The goal is controlled reduction of blood pressure, not rapid normalisation. The maximal initial reduction is roughly one third of the planned total reduction in the first eight hours, because cerebral autoregulation has reset upward and abrupt correction risks ischaemic stroke and blindness. [11]
Intravenous options for hypertensive emergency include nicardipine as a continuous infusion, labetalol, and hydralazine, each titrated to effect in a monitored setting. Isradipine is oral only and is not an intravenous emergency agent. Oral agents have no place in true hypertensive emergency. The child is managed in a paediatric intensive care or high-dependency unit with continuous intra-arterial monitoring where feasible, and the underlying cause (often acute glomerulonephritis or a renovascular lesion) is investigated in parallel. [11]
Management — Definitive & Stepwise
The stepwise approach begins with confirmation and stratification and proceeds through lifestyle modification to drug therapy, with monitoring to a blood-pressure target. [1]
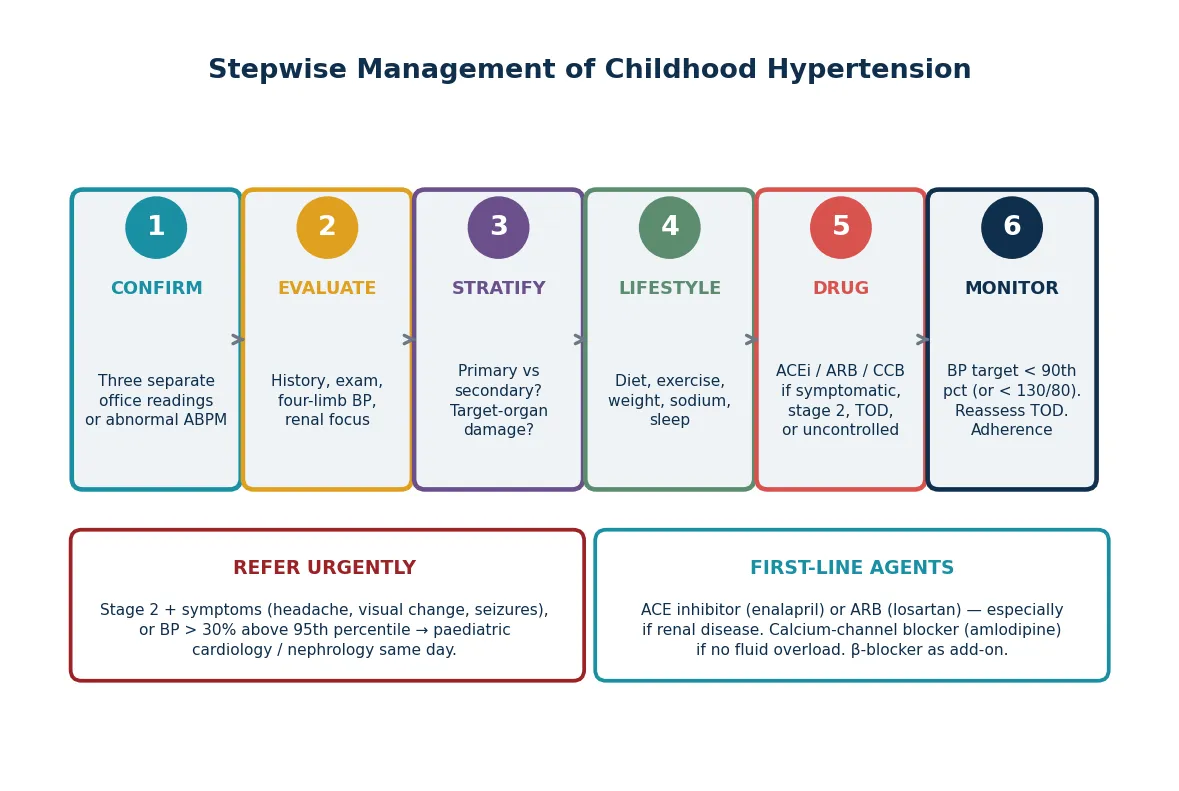
Lifestyle modification is the foundation of primary hypertension management and the first step for all children. It comprises the DASH-style diet (rich in fruit, vegetables and low-fat dairy, low in sodium), regular aerobic exercise, weight reduction in the overweight child, sodium restriction, and attention to sleep duration and screen-time habits. These measures alone normalise blood pressure in many children with mild primary hypertension and potentiate drug therapy in those who need it. [7]
Enalapril (ACE inhibitor — first line if renal disease)
Dose
0.08 mg/kg per day orally once daily, titrate to 0.6 mg/kg per day (max 40 mg/day)
Drug therapy is indicated for symptomatic hypertension, stage 2 hypertension, confirmed stage 1 hypertension with target-organ damage (especially left ventricular hypertrophy), diabetes or chronic kidney disease, and failure of a six-month lifestyle trial in stage 1 hypertension. The first-line agents are the angiotensin-converting-enzyme inhibitor (enalapril) or angiotensin-receptor blocker (losartan) when the cause is renal or renovascular, and the dihydropyridine calcium-channel blocker (amlodipine) when it is not, particularly in fluid-retaining states. Beta-blockers are effective but are now usually add-on therapy. The blood-pressure target is below the 90th percentile (or below 130/80 mmHg in adolescents), confirmed by ambulatory monitoring. [1] [8]
Specific Subtypes & Scenarios
Neonatal hypertension is a distinct entity, defined as systolic blood pressure above the 95th percentile for gestational age and postnatal age. The prevalence in neonatal intensive care units is 1 to 3 per cent, and the cause is almost always secondary — renal artery thromboembolism after umbilical artery catheterisation, renal venous thrombosis, congenital renal malformations, bronchopulmonary dysplasia, or medication (corticosteroids, caffeine). A palpable renal mass, an umbilical catheter history, or absent lower-limb pulses are key clues. Management begins with treating the cause and uses the same agent classes, dose-adjusted, with the involvement of a neonatologist and paediatric nephrologist. [12]
The young-child secondary-cause screen — RRECC
Hypertension in chronic kidney disease and on dialysis is the highest-risk subtype. Blood-pressure control is the single most important modifiable factor slowing the progression of renal disease and reducing cardiovascular mortality, which is the leading cause of death in children with end-stage kidney disease. Volume overload is the dominant mechanism, so salt restriction, fluid management and diuretics are central, with an ACE inhibitor or ARB for the renin component. Ambulatory monitoring is particularly valuable here because nocturnal hypertension and non-dipping are common and predict progression. [6]
Complications & Pitfalls
The complications of untreated childhood hypertension are target-organ damage in childhood and premature cardiovascular disease in adulthood. Left ventricular hypertrophy, increased carotid intima-media thickness, arterial stiffening and cognitive impairment are demonstrable in children with sustained hypertension, and the neurocognitive effects on attention, executive function and academic performance are increasingly recognised. These findings underpin the rationale for treatment in the asymptomatic child. [5] [10]
The common pitfalls are diagnostic and pharmacological. The diagnostic pitfalls are overdiagnosis (labelling on one reading, cuff-size error, ignoring white-coat hypertension), underdiagnosis (failing to screen, dismissing the reading as anxiety) and missing the secondary cause (not measuring four-limb blood pressure, not doing urinalysis or renal ultrasound in a young child). The pharmacological pitfalls are using the wrong first-line agent (a beta-blocker before an ACE inhibitor in renal disease), failing to monitor potassium and creatinine after starting an ACE inhibitor or ARB, and abrupt blood-pressure reduction in an emergency. [4]
Prognosis & Disposition
The prognosis of childhood hypertension depends on the cause and on control. Primary hypertension, well controlled by lifestyle and drug therapy, carries an excellent short-term prognosis and a markedly improved long-term cardiovascular outlook. Secondary hypertension has the prognosis of its underlying cause — surgically curable lesions (coarctation, unilateral renal artery stenosis) have an excellent outcome after correction, while chronic kidney disease carries the heavy cardiovascular burden of the renal disease itself. [6]
The disposition is shared care between the general paediatrician and a paediatric nephrologist or cardiologist. Children with primary hypertension can be managed in primary or general paediatric care with annual or biennial ambulatory monitoring and echocardiography. Children with secondary hypertension, stage 2 disease, hypertensive emergency, or complex chronic disease need subspecialty involvement from diagnosis. The transition to adult care in late adolescence is a high-risk period for loss to follow-up, and a structured handover that includes blood-pressure control status, target-organ assessment and the medication history is essential. [8]
Special Populations
Children with complex chronic conditions — chronic kidney disease, dialysis dependence, post-solid-organ transplant, and congenital heart disease — have a high prevalence of hypertension that interacts with their primary disease. In transplant recipients, calcineurin-inhibitor toxicity and steroid exposure drive hypertension; in congenital heart disease, coarctation repair survivors carry a lifelong re-coarctation and residual hypertension risk. These children need subspecialty-led, protocolised monitoring. [6]
Indigenous children in Australia and New Zealand, and children from migrant, refugee and socioeconomically disadvantaged backgrounds, carry a higher burden of the antecedents of primary hypertension — obesity, low birth weight, poor nutrition and reduced physical activity — and of the renal disease that drives secondary hypertension. Screening, early lifestyle intervention and equitable access to ambulatory monitoring and subspecialty care are the priority. The same equity principle applies to children in out-of-home care and youth justice settings, where missed health checks and psychosocial stress compound cardiovascular risk. [7]
Evidence, Guidelines & Regional Differences
The two dominant guidelines are the AAP 2017 clinical practice guideline and the European Society of Hypertension 2016 guideline (with its 2023 joint-statement update on measurement technique). They agree on the percentile-based definition, on ambulatory monitoring as the confirmation standard, and on the centrality of lifestyle modification and the renin–angiotensin–aldosterone system as a therapeutic target. They differ in detail: the AAP aligns adolescent thresholds with adult numbers (130/80 mmHg) and is more aggressive on drug-treatment thresholds, while the European guideline retains a slightly more conservative stance on pharmacological treatment in mild disease. [1] [3]
Controversies remain. The normative data underpinning the percentile tables were derived from a population that included overweight children, which may shift the thresholds upward; an ideal dataset would exclude overweight children, and updates are in progress. The role of home blood pressure monitoring (as distinct from ambulatory monitoring) is expanding but is less well validated in children than in adults. The long-term benefit of drug therapy in asymptomatic children with mild hypertension, demonstrated for surrogate endpoints (left ventricular mass, arterial stiffness), is still being established for hard cardiovascular endpoints. [7]
Exam Pearls
Three rules that mark a fellowship answer
The high-yield minutiae an examiner rewards: the cuff must cover 80 per cent of the arm; an elevated oscillometric reading must be confirmed by auscultation; the adolescent thresholds of 130/80 and 140/90 mmHg align with the adult numbers; left ventricular hypertrophy is the target-organ finding that triggers drug therapy; the maximal initial blood-pressure reduction in an emergency is 25 per cent in eight hours; and the renin–angiotensin–aldosterone system is the mechanism shared by the renal and renovascular causes, which is why ACE inhibitors and ARBs are first-line in renal disease. [1] [11]
References
- [1]Flynn JT; Kaelber DC; Baker-Smith CM; et al Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics, 2017.PMID 28827377
- [2]National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics, 2004.PMID 15286277
- [3]Lurbe E; Agabiti-Rosei E; Cruickshank JK; et al 2016 European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents. J Hypertens, 2016.PMID 27467768
- [4]Hansen ML; Gunn PW; Kaelber DC Underdiagnosis of hypertension in children and adolescents. JAMA, 2007.PMID 17712071
- [5]Kollias A; Dafni M; Poulidakis E; et al Out-of-office blood pressure and target organ damage in children and adolescents: a systematic review and meta-analysis. J Hypertens, 2014.PMID 25304469
- [6]Mitsnefes MM; Laskin BL; Dahhou M; et al Mortality risk among children initially treated with dialysis for end-stage kidney disease, 1990-2010. JAMA, 2013.PMID 23645144
- [7]Lurbe E; Litwin M; Pall D; et al Insights and implications of new blood pressure guidelines in children and adolescents. J Hypertens, 2018.PMID 29677052
- [8]Flynn JT; Kruger R; Brady TM; et al Practical approach to evaluate and manage hypertension in youth: an International Society of Hypertension position paper. J Hypertens, 2026.PMID 41674374
- [9]Lurbe E; Mancia G; Calpe J; et al Joint statement for assessing and managing high blood pressure in children and adolescents: Chapter 1. How to correctly measure blood pressure in children and adolescents. Front Pediatr, 2023.PMID 37138561
- [10]Hooper SR; Johnson RJ; Gerson AC; et al Overview of the findings and advances in the neurocognitive and psychosocial functioning of mild to moderate pediatric CKD: perspectives from the Chronic Kidney Disease in Children (CKiD) cohort study. Pediatr Nephrol, 2022.PMID 34110493
- [11]Miyashita Y; Peterson D; Rees JM; et al Isradipine for treatment of acute hypertension in hospitalized children and adolescents. J Clin Hypertens (Greenwich), 2010.PMID 21054771
- [12]Flynn JT Neonatal hypertension. J Med Liban, 2010.PMID 21462844